

Abstract
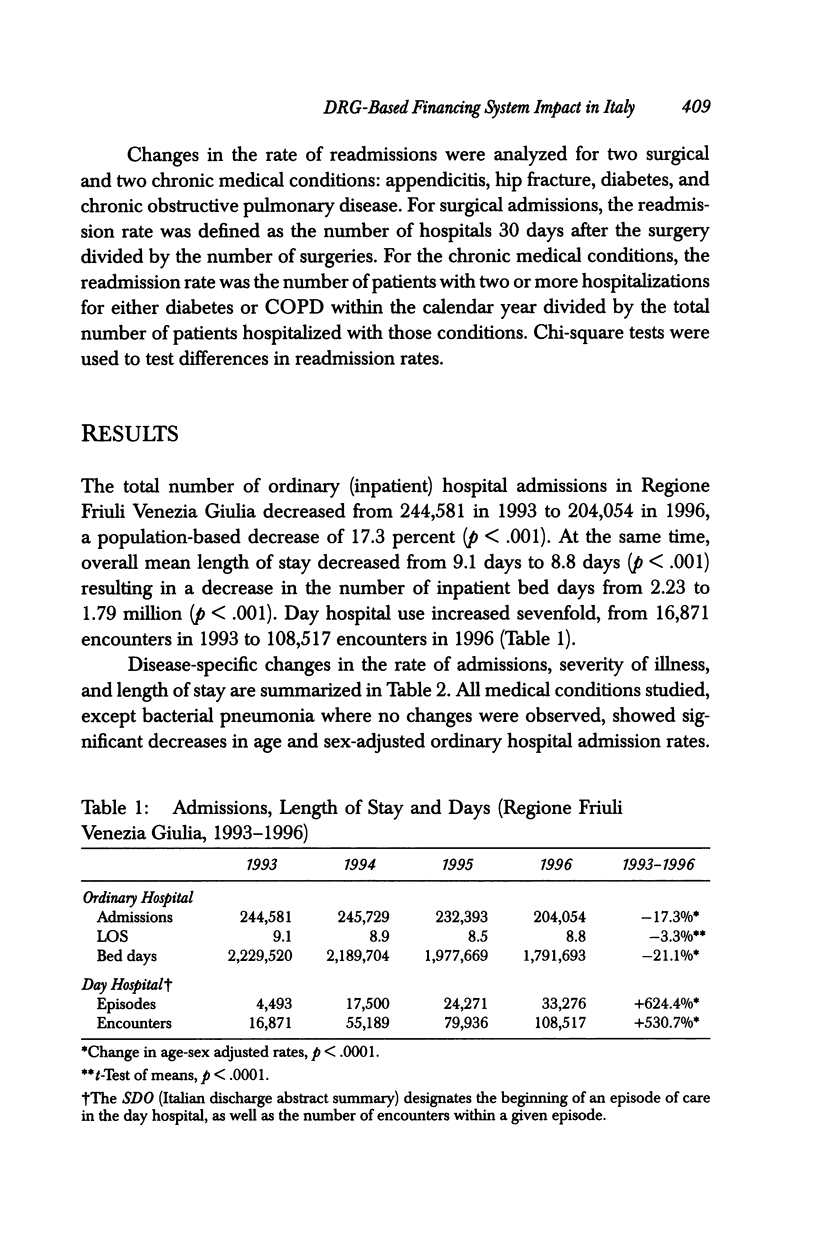
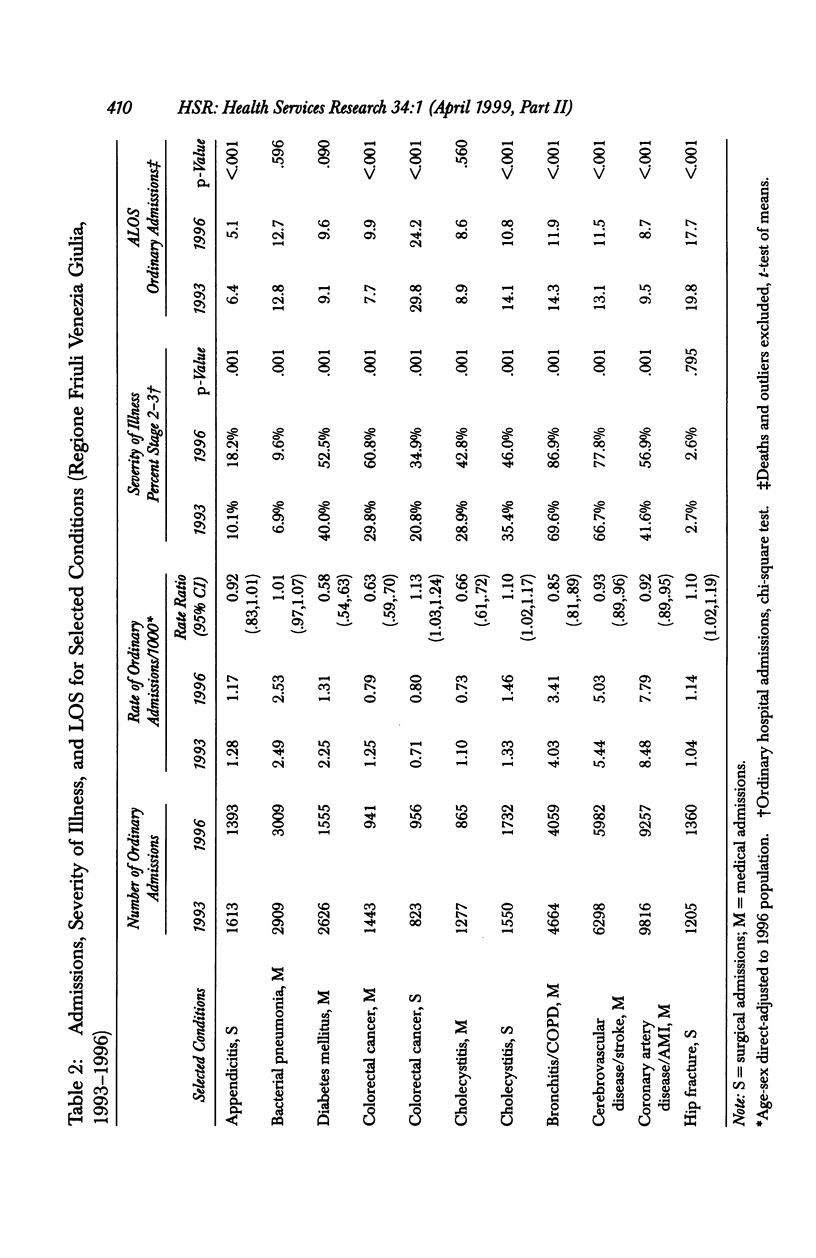
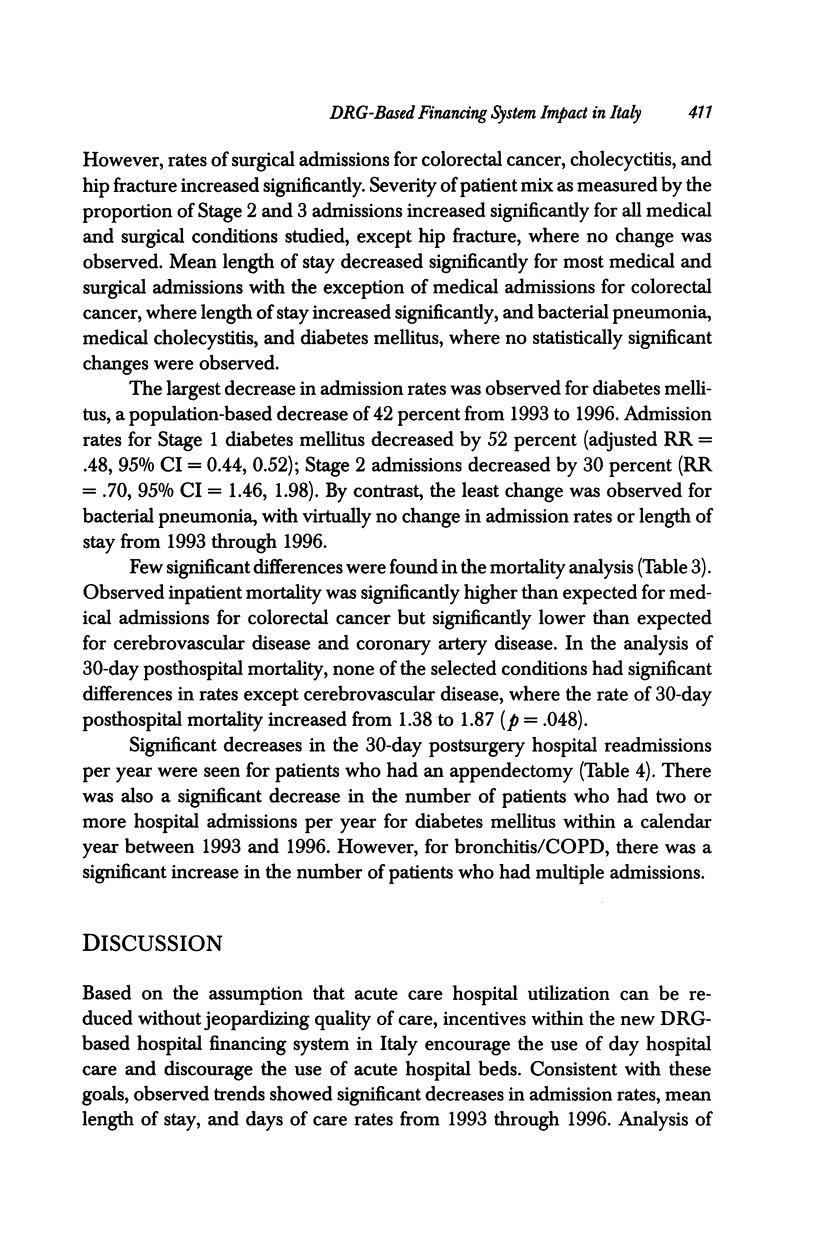
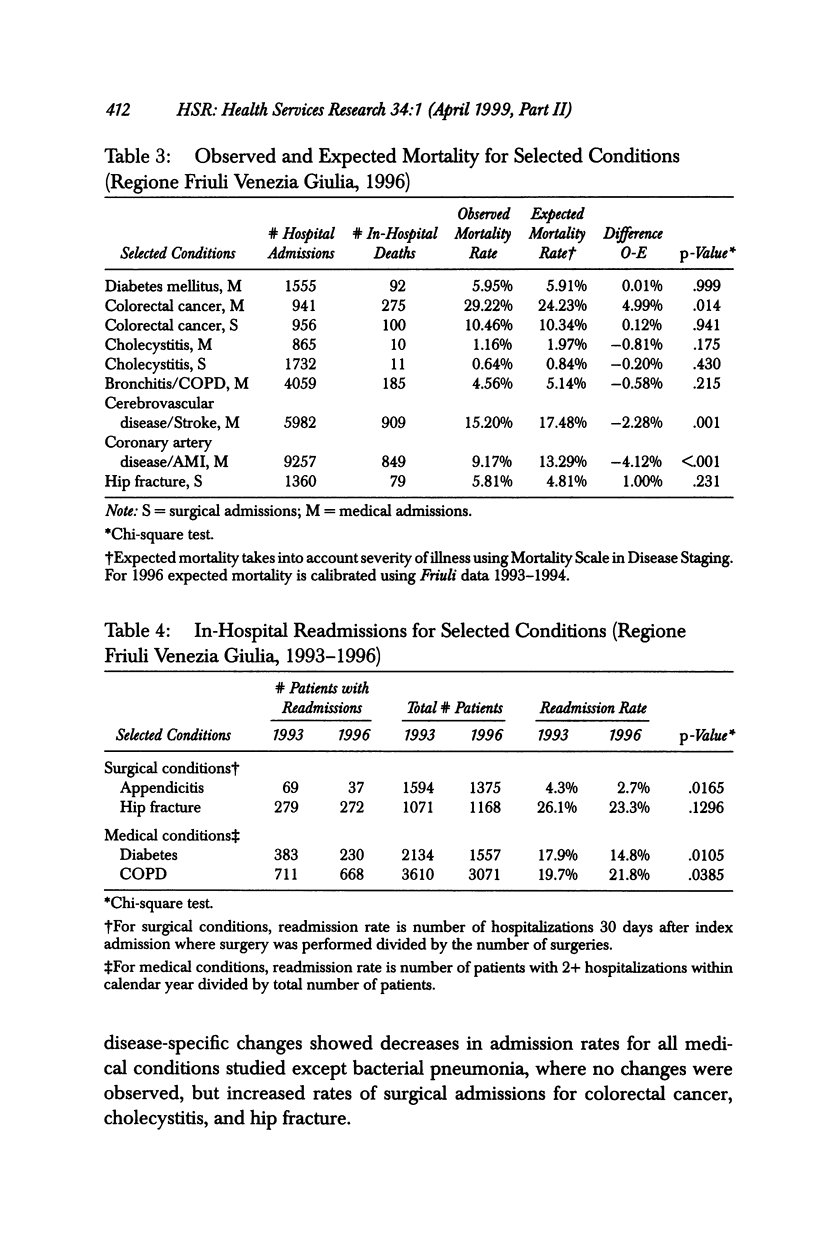
OBJECTIVE: To examine potential changes in quality of care associated with a recent financing system implementation in Italy: in 1995, hospital financing reform implemented in Italy included the introduction of a DRG-based hospital financing system with the goals of controlling the growth of hospital costs and making hospitals more accountable for their productivity. DATA SOURCES: Hospital discharge abstract data from 1993 through 1996 for all hospitals (N=32) in the Friuli-Venezia-Giulia region of Italy. Regional population data were used to calculate rates. STUDY DESIGN: Changes between 1993 and 1996 in hospital admissions, length of stay, mortality rates, severity of illness, and readmission rates were studied for nine common medical and surgical conditions: appendicitis, diabetes mellitus, colorectal cancer, cholecystitis, bronchitis/chronic obstructive pulmonary disease (COPD), bacterial pneumonia, coronary artery disease, cerebrovascular disease, and hip fracture. PRINCIPAL FINDINGS: The total number of ordinary hospital admissions decreased from 244,581 to 204,054 between 1993 and 1996, a population-based decrease of 17.3 percent (p<.001). The mean length of stay decreased from 9.1 days to 8.8 days, resulting in a 21.1 percent decrease in hospital bed days (p<.001). Day hospital use increased sevenfold from 16,871 encounters in 1993 to 108,517 encounters in 1996. The largest decrease in hospital admissions among study conditions was a 41 percent decrease for diabetes (from 2.25 per 1,000 in 1993 to 1.31 in 1996, p<.001). For eight of the nine conditions, severity of illness increased. Differences between severity-adjusted expected and observed in-hospital mortality rates were small. CONCLUSIONS: Observed trends showed a decrease in ordinary hospital admissions, an increase in day hospital admissions, and a greater severity of illness among hospitalized patients. There was little or no change in mortality and readmission rates. Administrative data can be used to track changes in patterns of care and to identify potential quality problems deserving further review.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bevan G., France G., Taroni F. Dolce vita. Health Serv J. 1992 Feb 27;102(5291):20–23. [PubMed] [Google Scholar]
- Hsia D. C., Ahern C. A., Ritchie B. P., Moscoe L. M., Krushat W. M. Medicare reimbursement accuracy under the prospective payment system, 1985 to 1988. JAMA. 1992 Aug 19;268(7):896–899. [PubMed] [Google Scholar]
- Kahn K. L., Keeler E. B., Sherwood M. J., Rogers W. H., Draper D., Bentow S. S., Reinisch E. J., Rubenstein L. V., Kosecoff J., Brook R. H. Comparing outcomes of care before and after implementation of the DRG-based prospective payment system. JAMA. 1990 Oct 17;264(15):1984–1988. [PubMed] [Google Scholar]
- McKee M., Aiken L., Rafferty A. M., Sochalski J. Organisational change and quality of health care: an evolving international agenda. Qual Health Care. 1998 Mar;7(1):37–41. doi: 10.1136/qshc.7.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers W. H., Draper D., Kahn K. L., Keeler E. B., Rubenstein L. V., Kosecoff J., Brook R. H. Quality of care before and after implementation of the DRG-based prospective payment system. A summary of effects. JAMA. 1990 Oct 17;264(15):1989–1994. [PubMed] [Google Scholar]
- Simborg D. W. DRG creep: a new hospital-acquired disease. N Engl J Med. 1981 Jun 25;304(26):1602–1604. doi: 10.1056/NEJM198106253042611. [DOI] [PubMed] [Google Scholar]
- del Favero A., Barro G., Vicari G., Rovelli F., Tognoni G., Bozzini L., Martini N., Pagliaro L., Remuzzi G. Health services: an Italian market. Lancet. 1996 Jul 20;348(9021):167–175. doi: 10.1016/s0140-6736(96)05024-6. [DOI] [PubMed] [Google Scholar]