

Abstract
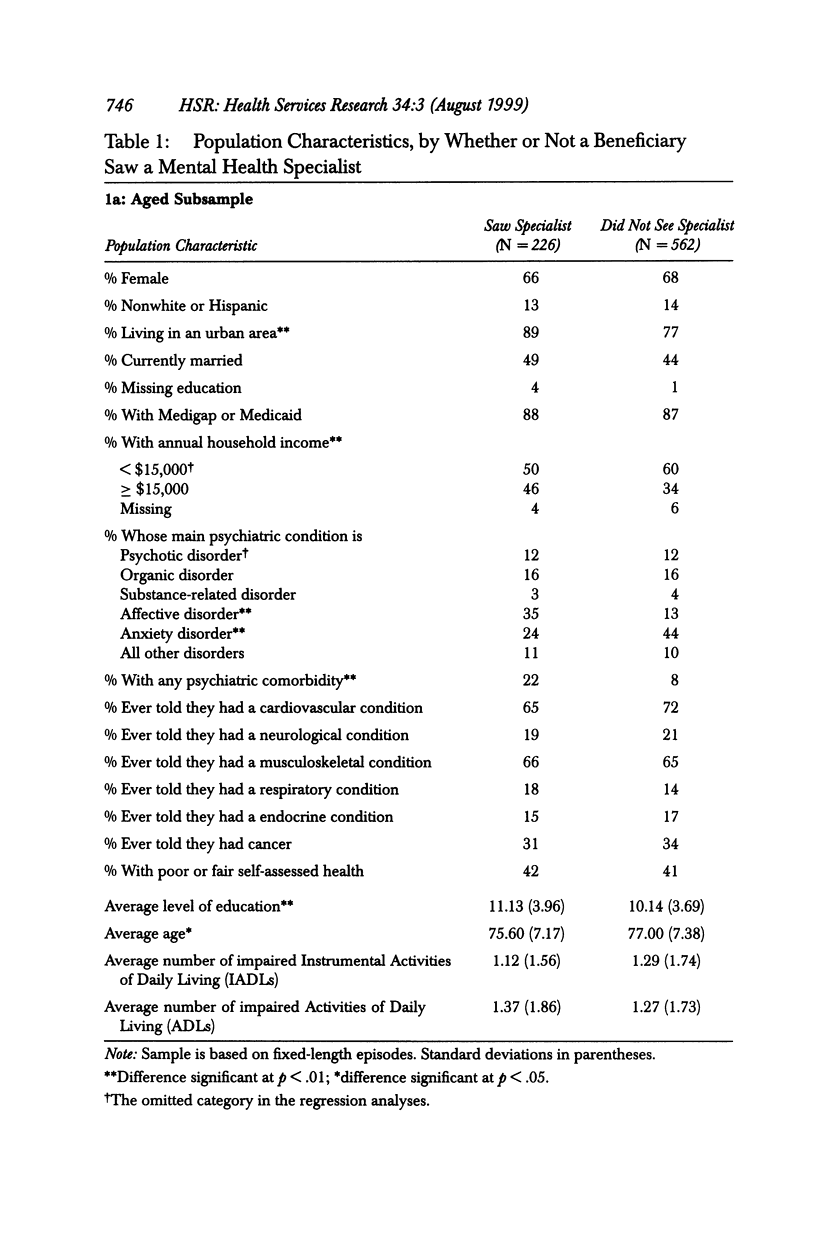
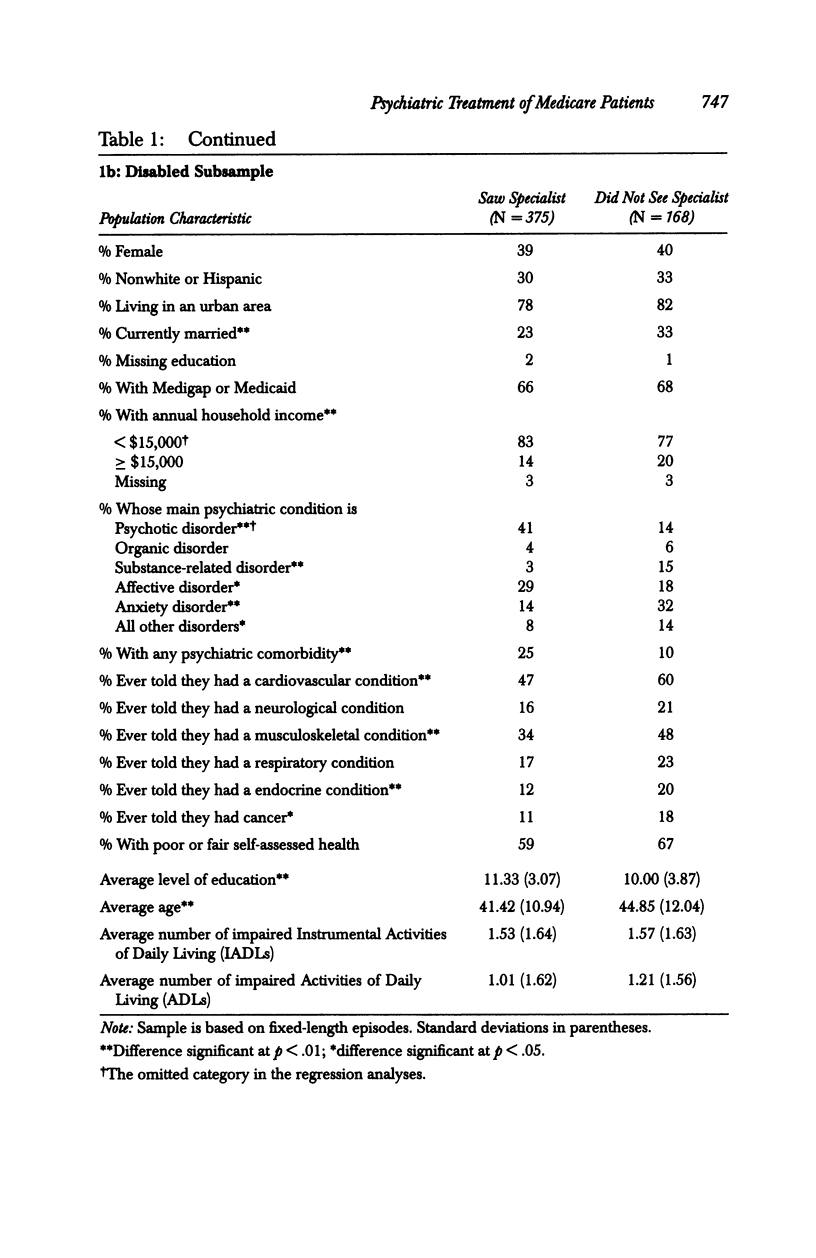
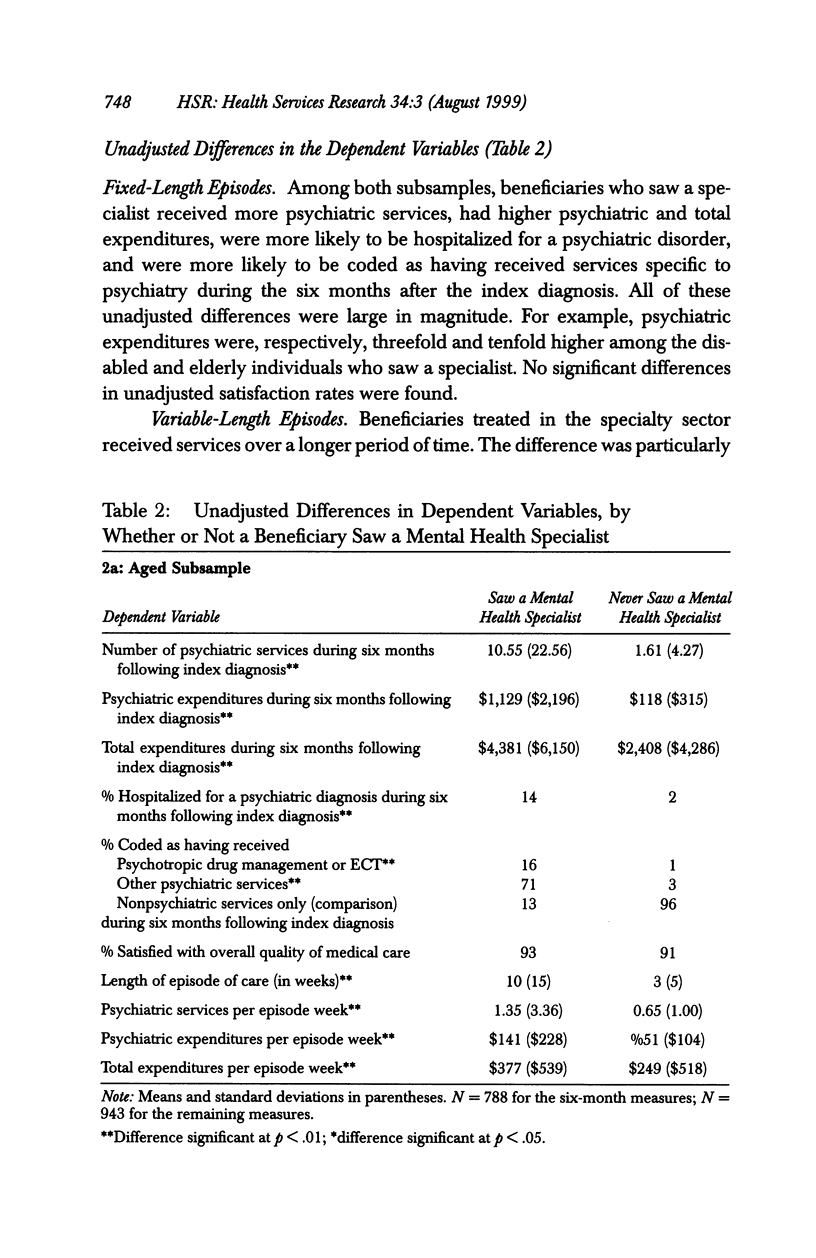
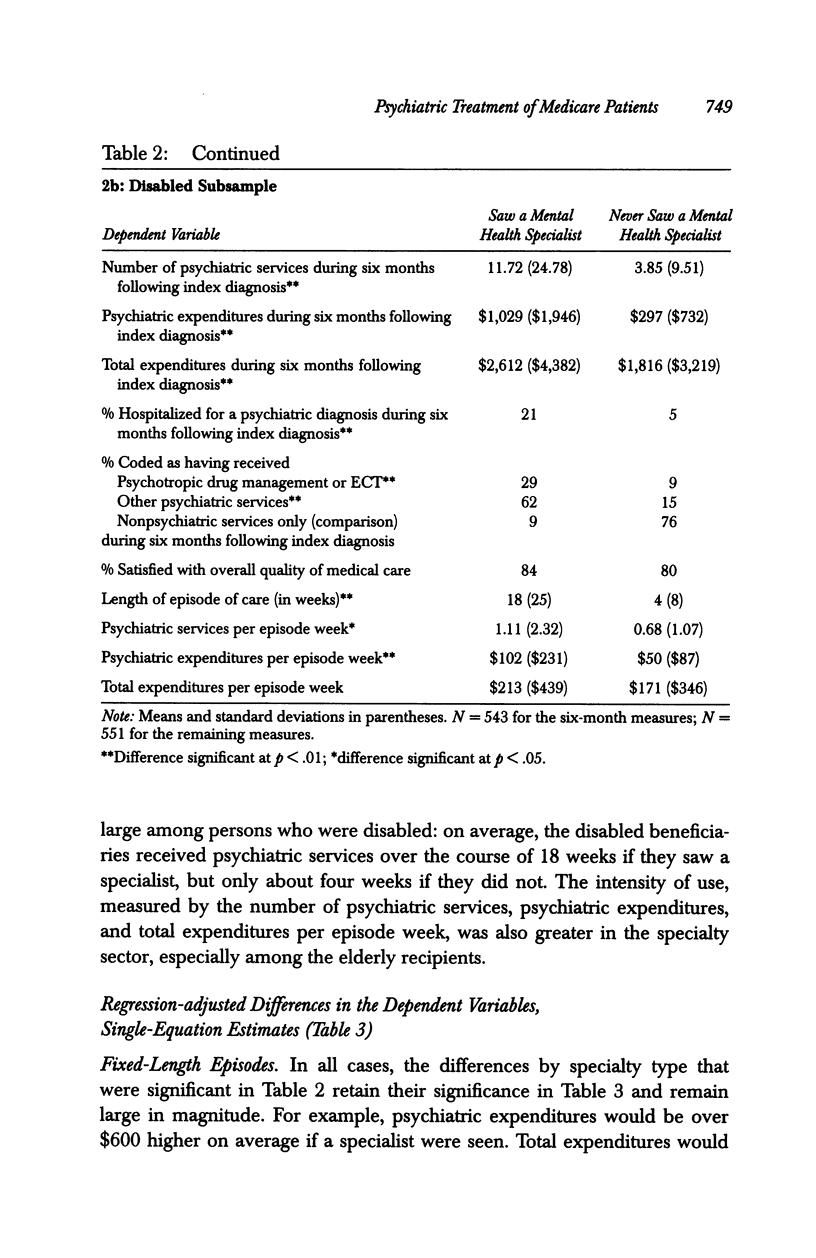
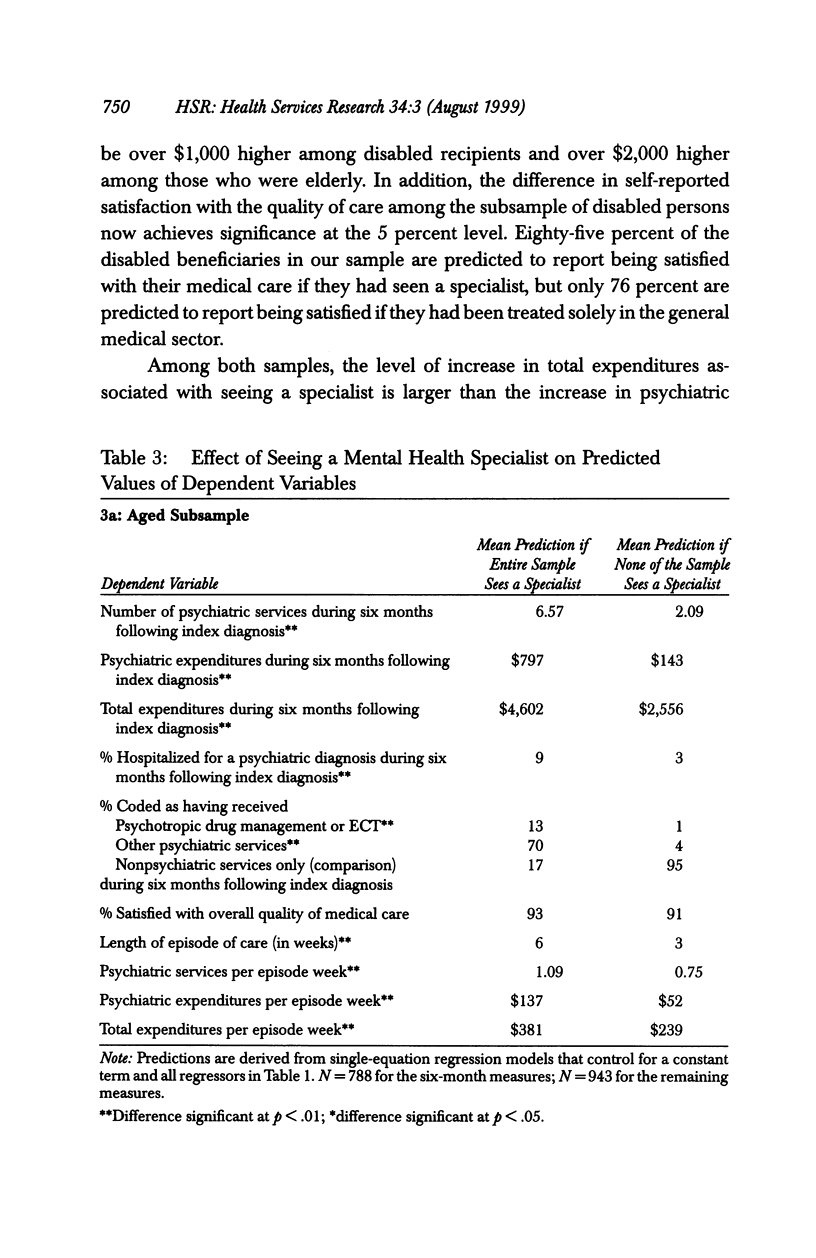
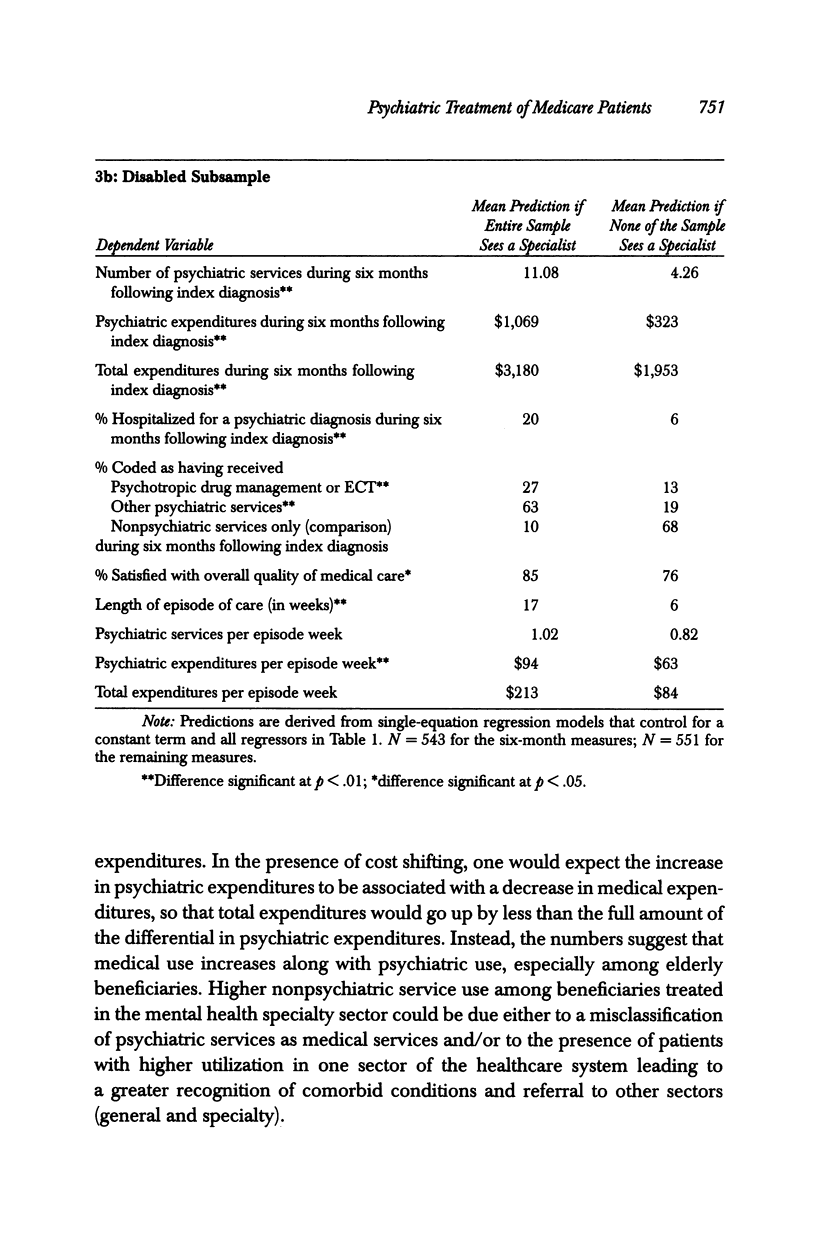
OBJECTIVE: To examine differences between the general medical and mental health specialty sectors in the expenditure and treatment patterns of aged and disabled Medicare beneficiaries with a physician diagnosis of psychiatric disorder. DATA SOURCES: Based on 1991-1993 Medicare Current Beneficiary Survey data, linked to the beneficiary's claims and area-level data on provider supply from the Area Resources File and the American Psychological Association. STUDY DESIGN: Outcomes examined included the number of psychiatric services received, psychiatric and total Medicare expenditures, the type of services received, whether or not the patient was hospitalized for a psychiatric disorder, the length of the psychiatric care episode, the intensity of service use, and satisfaction with care. We compared these outcomes for beneficiaries who did and did not receive mental health specialty services during the episode, using multiple regression analyses to adjust for observable population differences. We also performed sensitivity analyses using instrumental variables techniques to reduce the potential bias arising from unmeasured differences in patient case mix across sectors. PRINCIPAL FINDINGS: Relative to beneficiaries treated only in the general medical sector, those seen by a mental health specialist had longer episodes of care, were more likely to receive services specific to psychiatry, and had greater psychiatric and total expenditures. Among the elderly persons, the higher costs were due to a combination of longer episodes and greater intensity; among the persons who were disabled, they were due primarily to longer episodes. Some evidence was also found of higher satisfaction with care among the disabled individuals treated in the specialty sector. However, evidence of differences in psychiatric hospitalization rates was weaker. CONCLUSIONS: Mental health care provided to Medicare beneficiaries in the general medical sector does not appear to substitute perfectly for care provided in the specialty sector. Our study suggests that the treatment patterns in the specialty sector may be preferred by some patients; further, earlier findings indicate geographic barriers to obtaining specialty care. Thus, the matching of service use to clinical need among this vulnerable population may be inappropriate. The need for further research on outcomes is indicated.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Andersen S. M., Harthorn B. H. The recognition, diagnosis, and treatment of mental disorders by primary care physicians. Med Care. 1989 Sep;27(9):869–886. doi: 10.1097/00005650-198909000-00003. [DOI] [PubMed] [Google Scholar]
- Callies A. L., Popkin M. K. Antidepressant treatment of medical-surgical inpatients by nonpsychiatric physicians. Arch Gen Psychiatry. 1987 Feb;44(2):157–160. doi: 10.1001/archpsyc.1987.01800140067009. [DOI] [PubMed] [Google Scholar]
- Cooper-Patrick L., Crum R. M., Ford D. E. Characteristics of patients with major depression who received care in general medical and specialty mental health settings. Med Care. 1994 Jan;32(1):15–24. doi: 10.1097/00005650-199401000-00002. [DOI] [PubMed] [Google Scholar]
- Fortney J., Rost K., Zhang M. A joint choice model of the decision to seek depression treatment and choice of provider sector. Med Care. 1998 Mar;36(3):307–320. doi: 10.1097/00005650-199803000-00008. [DOI] [PubMed] [Google Scholar]
- Fowles J. B., Lawthers A. G., Weiner J. P., Garnick D. W., Petrie D. S., Palmer R. H. Agreement between physicians' office records and Medicare Part B claims data. Health Care Financ Rev. 1995 Summer;16(4):189–199. [PMC free article] [PubMed] [Google Scholar]
- Frank R. G., Kamlet M. S. Economic aspects of patterns of mental health care: cost variation by setting. Gen Hosp Psychiatry. 1990 Jan;12(1):11–18. doi: 10.1016/0163-8343(90)90032-8. [DOI] [PubMed] [Google Scholar]
- Gerber P. D., Barrett J., Barrett J., Manheimer E., Whiting R., Smith R. Recognition of depression by internists in primary care: a comparison of internist and "gold standard" psychiatric assessments. J Gen Intern Med. 1989 Jan-Feb;4(1):7–13. doi: 10.1007/BF02596483. [DOI] [PubMed] [Google Scholar]
- German P. S., Shapiro S., Skinner E. A. Mental health of the elderly: use of health and mental health services. J Am Geriatr Soc. 1985 Apr;33(4):246–252. doi: 10.1111/j.1532-5415.1985.tb07111.x. [DOI] [PubMed] [Google Scholar]
- Horgan C. M. Specialty and general ambulatory mental health services. Comparison of utilization and expenditures. Arch Gen Psychiatry. 1985 Jun;42(6):565–572. doi: 10.1001/archpsyc.1985.01790290047005. [DOI] [PubMed] [Google Scholar]
- Katz S. J., Kessler R. C., Lin E., Wells K. B. Medication management of depression in the United States and Ontario. J Gen Intern Med. 1998 Feb;13(2):77–85. doi: 10.1046/j.1525-1497.1998.00022.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keeler E. B., Manning W. G., Wells K. B. The demand for episodes of mental health services. J Health Econ. 1988 Dec;7(4):369–392. doi: 10.1016/0167-6296(88)90021-5. [DOI] [PubMed] [Google Scholar]
- Kessler L. G., Steinwachs D. M., Hankin J. R. Episodes of psychiatric utilization. Med Care. 1980 Dec;18(12):1219–1227. doi: 10.1097/00005650-198012000-00007. [DOI] [PubMed] [Google Scholar]
- Kessler R. C., McGonagle K. A., Zhao S., Nelson C. B., Hughes M., Eshleman S., Wittchen H. U., Kendler K. S. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994 Jan;51(1):8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Knesper D. J., Pagnucco D. J., Wheeler J. R. Similarities and differences across mental health services providers and practice settings in the United States. Am Psychol. 1985 Dec;40(12):1352–1369. doi: 10.1037//0003-066x.40.12.1352. [DOI] [PubMed] [Google Scholar]
- Leaf P. J., Bruce M. L., Tischler G. L., Freeman D. H., Jr, Weissman M. M., Myers J. K. Factors affecting the utilization of specialty and general medical mental health services. Med Care. 1988 Jan;26(1):9–26. doi: 10.1097/00005650-198801000-00002. [DOI] [PubMed] [Google Scholar]
- Leaf P. J., Livingston M. M., Tischler G. L., Weissman M. M., Holzer C. E., 3rd, Myers J. K. Contact with health professionals for the treatment of psychiatric and emotional problems. Med Care. 1985 Dec;23(12):1322–1337. doi: 10.1097/00005650-198512000-00002. [DOI] [PubMed] [Google Scholar]
- Lurie N., Popkin M., Dysken M., Moscovice I., Finch M. Accuracy of diagnoses of schizophrenia in Medicaid claims. Hosp Community Psychiatry. 1992 Jan;43(1):69–71. doi: 10.1176/ps.43.1.69. [DOI] [PubMed] [Google Scholar]
- Mechanic D. Treating mental illness: generalist versus specialist. Health Aff (Millwood) 1990 Winter;9(4):61–75. doi: 10.1377/hlthaff.9.4.61. [DOI] [PubMed] [Google Scholar]
- Ormel J., Van Den Brink W., Koeter M. W., Giel R., Van Der Meer K., Van De Willige G., Wilmink F. W. Recognition, management and outcome of psychological disorders in primary care: a naturalistic follow-up study. Psychol Med. 1990 Nov;20(4):909–923. doi: 10.1017/s0033291700036606. [DOI] [PubMed] [Google Scholar]
- Regier D. A., Goldberg I. D., Taube C. A. The de facto US mental health services system: a public health perspective. Arch Gen Psychiatry. 1978 Jun;35(6):685–693. doi: 10.1001/archpsyc.1978.01770300027002. [DOI] [PubMed] [Google Scholar]
- Regier D. A., Narrow W. E., Rae D. S., Manderscheid R. W., Locke B. Z., Goodwin F. K. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry. 1993 Feb;50(2):85–94. doi: 10.1001/archpsyc.1993.01820140007001. [DOI] [PubMed] [Google Scholar]
- Robbins J. M., Kirmayer L. J., Cathébras P., Yaffe M. J., Dworkind M. Physician characteristics and the recognition of depression and anxiety in primary care. Med Care. 1994 Aug;32(8):795–812. doi: 10.1097/00005650-199408000-00004. [DOI] [PubMed] [Google Scholar]
- Schulberg H. C., Saul M., McClelland M., Ganguli M., Christy W., Frank R. Assessing depression in primary medical and psychiatric practices. Arch Gen Psychiatry. 1985 Dec;42(12):1164–1170. doi: 10.1001/archpsyc.1985.01790350038008. [DOI] [PubMed] [Google Scholar]
- Schurman R. A., Kramer P. D., Mitchell J. B. The hidden mental health network. Treatment of mental illness by nonpsychiatrist physicians. Arch Gen Psychiatry. 1985 Jan;42(1):89–94. doi: 10.1001/archpsyc.1985.01790240091010. [DOI] [PubMed] [Google Scholar]
- Sherbourne C. D., Wells K. B., Hays R. D., Rogers W., Burnam M. A., Judd L. L. Subthreshold depression and depressive disorder: clinical characteristics of general medical and mental health specialty outpatients. Am J Psychiatry. 1994 Dec;151(12):1777–1784. doi: 10.1176/ajp.151.12.1777. [DOI] [PubMed] [Google Scholar]
- Simon G. E., VonKorff M. Recognition, management, and outcomes of depression in primary care. Arch Fam Med. 1995 Feb;4(2):99–105. doi: 10.1001/archfami.4.2.99. [DOI] [PubMed] [Google Scholar]
- Stewart A. L., Sherbourne C. D., Wells K. B., Burnam M. A., Rogers W. H., Hays R. D., Ware J. E., Jr Do depressed patients in different treatment settings have different levels of well-being and functioning? J Consult Clin Psychol. 1993 Oct;61(5):849–857. doi: 10.1037//0022-006x.61.5.849. [DOI] [PubMed] [Google Scholar]
- Sturm R., Meredith L. S., Wells K. B. Provider choice and continuity for the treatment of depression. Med Care. 1996 Jul;34(7):723–734. doi: 10.1097/00005650-199607000-00005. [DOI] [PubMed] [Google Scholar]
- Sturm R., Wells K. B. How can care for depression become more cost-effective? JAMA. 1995 Jan 4;273(1):51–58. [PubMed] [Google Scholar]
- Von Korff M., Shapiro S., Burke J. D., Teitlebaum M., Skinner E. A., German P., Turner R. W., Klein L., Burns B. Anxiety and depression in a primary care clinic. Comparison of Diagnostic Interview Schedule, General Health Questionnaire, and practitioner assessments. Arch Gen Psychiatry. 1987 Feb;44(2):152–156. doi: 10.1001/archpsyc.1987.01800140058008. [DOI] [PubMed] [Google Scholar]
- Wells K. B., Burnam M. A., Camp P. Severity of depression in prepaid and fee-for-service general medical and mental health specialty practices. Med Care. 1995 Apr;33(4):350–364. doi: 10.1097/00005650-199504000-00003. [DOI] [PubMed] [Google Scholar]
- Wells K. B., Hays R. D., Burnam M. A., Rogers W., Greenfield S., Ware J. E., Jr Detection of depressive disorder for patients receiving prepaid or fee-for-service care. Results from the Medical Outcomes Study. JAMA. 1989 Dec 15;262(23):3298–3302. [PubMed] [Google Scholar]
- Wells K. B., Katon W., Rogers B., Camp P. Use of minor tranquilizers and antidepressant medications by depressed outpatients: results from the medical outcomes study. Am J Psychiatry. 1994 May;151(5):694–700. doi: 10.1176/ajp.151.5.694. [DOI] [PubMed] [Google Scholar]
- Wells K. B., Manning W. G., Jr, Duan N., Newhouse J. P., Ware J. E., Jr Cost-sharing and the use of general medical physicians for outpatient mental health care. Health Serv Res. 1987 Apr;22(1):1–17. [PMC free article] [PubMed] [Google Scholar]