

Abstract
Background
Suicide is a leading cause of death among post‐secondary students worldwide. Suicidal thoughts and planning are common among post‐secondary students. Previous reviews have examined the effectiveness of interventions for symptomatic individuals; however, many students at high risk of suicide are undiagnosed and untreated.
Objectives
We evaluated the effect on suicide and suicide‐related outcomes of primary suicide prevention interventions that targeted students within the post‐secondary setting.
Search methods
We searched the following sources up to June 2011: Specialised Registers of two Cochrane Groups, Cochrane Central Register of Controlled Trials, and nine other databases, trial registers, conference proceedings, and websites of national and international organizations. We screened reference lists and contacted authors of included studies to identify additional studies. We updated the search in November 2013; we will include these results in the review's next update.
Selection criteria
We included studies that tested an intervention for the primary prevention of suicide using a randomized controlled trial (RCT), controlled before‐and‐after (CBA), controlled interrupted time series (CITS), or interrupted time series (ITS) study design. Interventions targeted students within the post‐secondary setting (i.e. college, university, academy, vocational, or any other post‐secondary educational institution) without known mental illness, previous suicide attempt or self‐harm, or suicidal ideation. Outcomes included suicides, suicide attempts, suicidal ideation, changes in suicide‐related knowledge, attitudes and behavior, and availability of means of suicide.
Data collection and analysis
We used standardized electronic forms for data extraction, risk of bias and quality of evidence determination, and analysis. We estimated standardised mean differences (SMD) with 95% confidence intervals (CIs). We analysed studies by intervention type and study design. We summarized RCT effect sizes using random‐effects models meta‐analyses; and analysed statistical heterogeneity using the Chi2 test and I2 statistic. We described narratively the results from studies that used other study designs.
Main results
Eight studies met inclusion criteria. They were heterogeneous in terms of participants, study designs, and interventions. Five of eight studies had high risk of bias. In 3 RCTs (312 participants), classroom‐based didactic and experiential programs increased short‐term knowledge of suicide (SMD = 1.51, 95% CI 0.57 to 2.45; moderate quality evidence) and knowledge of suicide prevention (SMD = 0.72, 95% CI 0.36 to 1.07; moderate quality evidence). The effect on suicide prevention self‐efficacy in one RCT (152 participants) was uncertain (SMD = 0.20, 95% CI ‐0.13 to 0.54; low quality evidence). One CBA analysed the effects of an institutional policy that restricted student access to laboratory cyanide and mandated professional assessment for suicidal students. The incidence of student suicide decreased significantly at one university with the policy relative to 11 control universities, 2.00 vs. 8.68 per 100,000 (Z = 5.90; P < 0.05). Four CBAs explored effects of training 'gatekeepers' to recognize and respond to warning signs of emotional crises and suicide risk in students they encountered. The magnitude of effect sizes varied between studies. Gatekeeper training enhanced short‐term suicide knowledge in students, peer advisors residing in student accommodation, and faculty and staff, and suicide prevention self‐efficacy among peer advisors. There was no evidence of an effect on participants' suicide‐related attitudes or behaviors. One CBA found no evidence of effects of gatekeeper training of peer advisors on suicide‐related knowledge, self‐efficacy, or gatekeeper behaviors measured four to six months after intervention.
Authors' conclusions
We found insufficient evidence to support widespread implementation of any programs or policies for primary suicide prevention in post‐secondary educational settings. As all evaluated interventions combined primary and secondary prevention components, we were unable to determine the independent effects of primary preventive interventions. Classroom instruction and gatekeeper training increased short‐term suicide‐related knowledge. We found no studies that tested the effects of classroom instruction on suicidal behavior or long‐term outcomes. Limited evidence suggested minimal longer‐term effects of gatekeeper training on suicide‐related knowledge, while no evidence was found evaluating its effect on suicidal behavior. A policy‐based suicide intervention reduced student suicide, but findings have not been replicated. Our findings are limited by the overall low quality of the evidence and the lack of studies from middle‐ and low‐income countries. Rigorously designed studies should test the effects of preventive interventions on important health outcomes, including suicidal ideation and behavior, in varying post‐secondary settings.
Keywords: Humans; Education, Graduate; Suicidal Ideation; Suicide Prevention; Universities; Primary Prevention; Primary Prevention/methods; Randomized Controlled Trials as Topic; Secondary Prevention
Plain language summary
Prevention of suicide in university and other post‐secondary educational settings
Review question
We reviewed evidence about the effect of suicide prevention programs on post‐secondary students who are not known to be suicidal. We examined the effects of these programs on suicide, suicidal behavior, and knowledge and attitudes about suicide.
Background
Worldwide, suicide is a leading cause of death among post‐secondary students. Suicidal thoughts and planning are common among such students. However, fewer than half of students who report suicidal thoughts or other serious mental illness have received professional treatment. There is a need for suicide prevention programs that target students who are not already known to be suicidal ("primary prevention").
Study characteristics
We identified eight studies that were eligible for this Cochrane Review. All studies had both primary and secondary prevention components. That is, they targeted students known to be suicidal as well as those not known to be suicidal. We separately analysed the effects of classroom instruction, institutional policies, and gatekeeper training programs. Gatekeeper training programs train people to recognize and respond to warning signs of emotional crises or suicide risk in students they encounter. The evidence is current to June 2011.
Key results
Three studies, including 312 students, evaluated classroom instruction. Classroom instruction increases short‐term knowledge of suicide and suicide prevention. It may slightly enhance short‐term confidence in ability to prevent suicide. However, long‐term effects have not been studied. Effects of classroom instruction on suicidal behavior have also not been studied. One study evaluated an institutional policy. The policy restricted access to laboratory cyanide and required professional assessment for students who threatened or attempted suicide. The policy significantly reduced student suicides. These findings have not been tested in other post‐secondary institutions. Four studies, ranging from 53 to 146 participants, evaluated the effect of gatekeeper training programs. Gatekeeper training may lead to small‐to‐medium improvements in short‐term suicide‐related knowledge and confidence about being able to prevent suicide. We found no evidence that gatekeeper training improved short‐term attitudes toward suicide or long‐term knowledge or behaviors about suicide. The effect of gatekeeper training on suicide or suicidal behavior has not been evaluated.
Quality of evidence
The quality of evidence for short‐term knowledge of suicide and suicide prevention was moderate. For suicide prevention self‐efficacy, the quality of evidence was low. The quality of evidence was reduced because results were not similar across studies and there were not enough data.
Summary of findings
Summary of findings for the main comparison. Summary of findings for classroom‐based instructional programs.
| What are the effects of classroom‐based instructional programs on suicidal behavior and ideation, knowledge of suicide and suicide prevention, and suicide prevention self‐efficacy? | ||||
|
Patient or population: Post‐secondary undergraduate students Settings: Large public universities located in medium‐sized cities Intervention: Experiential and didactic suicide prevention programs Comparison: Non‐suicide related material or no treatment | ||||
| Outcomes | SMD (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments |
| Completed suicide at the end of active intervention | N/A | N/A | N/A | No studies were found that evaluated the effect of intervention on completed suicide among students. |
| Suicidal ideation at the end of active intervention | N/A | N/A | N/A | No studies were found that evaluated the effect of intervention on suicidal ideation among students. |
| Attempted suicide at the end of active intervention | N/A | N/A | N/A | No studies were found that evaluated the effect of intervention on attempted suicide among students. |
| Knowledge of suicide at the end of active intervention | 1.51 (0.57 to 2.45) | 312 (3 studies) | ⊕⊕⊕⊝ moderate1 | We downgraded the quality of evidence another level for unexplained, significant statistical heterogeneity, Chi2 = 22.60; P < 0.00001; I2 = 91%. We increased the quality of evidence by one level due to a large summary magnitude of effect. |
| Knowledge of suicide prevention at the end of active intervention | 0.72 (0.36 to 1.07) | 312 (3 studies) | ⊕⊕⊕⊝ moderate1 | We observed moderate statistical heterogeneity between studies. |
| Suicide prevention self‐efficacy at the end of active intervention | 0.20 (‐0.13 to 0.54) | 152 (1 study) | ⊕⊕⊝⊝ low1 | We downgraded the quality of evidence by another level for imprecision. |
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||
1Quality of evidence downgraded by one level for unblinded outcome assessment.
Background
Description of the condition
Suicide is the deliberate act of taking one's own life. The World Health Organization (WHO) has reported that globally, suicide is the third leading cause of death among young people aged under 25 years (Wasserman 2010). Although data on suicide rates among students in post‐secondary education (i.e. enrolled in a university or other post‐secondary educational institution), hereafter referred to as 'student', are limited especially in low‐income countries, available statistics suggest that student suicide is an important cause of death worldwide. Incidences of 6.5, 8.2, and 10.0 per 100,000 full‐time students per year (or per academic year) have been reported in the United States, Great Britain, and China, respectively (Schwartz 2006; Universities UK 2002; Xiangmin 2009). The incidence in Finland is 13.8 and 9.0 per 100,000 per year for male and female students, respectively (Niemi 1993). These data indicate that student suicide is a significant mental and public health problem.
Risk factors for suicide include hopelessness, lack of social support, mental disorders (e.g. mood, anxiety, substance abuse) and a history of suicidal plans, ideation, and attempts (Arria 2009). Among people who have died by suicide, an estimated 90% had a known psychiatric disorder and 60% had a mood disorder (Sher 2001). Among students, academic problems may also increase risk of suicide (Bernard 1982; Schotte 1982). Annually among U.S. students, an estimated 11.4% have suicidal ideation, 8.3% make a suicidal plan, and 1.7% attempt suicide (Barrios 2000). The high prevalence of risk factors for suicide among post‐secondary students highlights the need for suicide prevention interventions in this setting.
Description of the intervention
Programs have been developed and implemented in the post‐secondary educational setting to reduce the rate of suicide and associated risk factors among students (Gould 2009). Primary prevention (i.e. intervention before suicidal behavior occurs, or ideation is expressed; SPAN 2001) within this setting may include a wide range of interventions, such as educational curricula, school policies (e.g. to increase access to mental health care, or restrict access to lethal means), peer organizational programs (e.g. training peers to recognize people at risk), screening programs to identify risk factors for suicide, and social norming programs (e.g. targeting perceptions of how common or how acceptable suicidal behavior is among students). Other primary prevention strategies may aim, either through campaigns or other means, to reduce taboos that isolate individuals who experience suicidal thoughts and behaviors and inhibit them from disclosing or seeking help.
Why it is important to do this review
Because suicide is a leading cause of student death, preventive measures are needed. Numerous reviews have previously examined diverse interventions aimed at symptomatic individuals (i.e. secondary prevention of suicide) (Crawford 2007; Hall 2002; Hawton 1999; Hepp 2004; Linehan 1997; Tarrier 2008; van der Sande 1997). However, fewer than half of students who report suicidal ideation or other serious mental health issues have received any professional services or treatment (Eisenberg 2012; Verger 2010; Schweitzer 1995) while Gallagher 2009 found that 80% of students that completed suicide had never participated in counseling services on campus. Therefore, secondary prevention within the post‐secondary school setting is limited by the failure to identify many students at risk of suicide. Primary prevention interventions, targeted to the general student population, have the potential to prevent suicide among students not previously identified. Furthermore, post‐secondary educational institutions comprise large populations of young adults who are relatively easy to access for program delivery, potentially increasing cost efficiency. Although primary prevention of suicide in the school setting has been reviewed previously, these reviews did not include (or did not identify) studies in post‐secondary educational settings (Guo 2002; Guo 2003; Harden 2001; Hider 1998; Katz 2013; Mann 2005; Miller 2009; Ploeg 1999). Students in post‐secondary educational settings encompass an age group that is distinct from younger students in terms of their development, demographics, subjective perceptions, identity explorations, and risk behaviors (Arnett 2000), while post‐secondary settings comprise a new and potentially stressful environment (Schwartz 1990). In this Cochrane Review we will address this gap in knowledge by assessing the available evidence to identify effective methods of primary suicide prevention within the post‐secondary educational setting.
Objectives
To evaluate primary suicide prevention interventions that targeted students within the post‐secondary setting to determine their effect on suicide and suicide‐related outcomes.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials (RCT): prospective studies that compare two or more groups, in which there is random assignment of participants or clusters to the interventions utilizing a known randomization or pseudo‐randomization technique (e.g. random numbers table, computer generated randomization, coin flip) or a statement that subjects were assigned randomly without explanation of how;
Controlled before‐and‐after (CBA) studies: studies that compare two or more groups to which participants are assigned by an entity other than themselves, and in which pre‐test and post‐test outcomes are measured concurrently and are available for both groups;
Controlled interrupted time series (CITS) design studies: studies in which there are at least three observations of the outcome measure both before and after a specific point in time when the intervention is implemented, from both the intervention group or area and concurrently at least one external comparison group or area, and in which an entity other than the participants determines which group or area receives the intervention;
Interrupted time series (ITS) design: studies in which there are at least three observations of the outcome measure both before and after a specific point in time when the intervention is implemented.
Types of participants
Students that attended a post‐secondary educational institution (e.g. college, university, community college, academy, or vocational or any other higher or post‐secondary educational institution) were a principal target of the intervention. We included studies that also targeted or collected data on faculty or staff in post‐secondary educational institutions as long as students were a principal target of the intervention. Students could be full‐time or part‐time, in any year of study, and live either on or off campus. We excluded individual apprenticeships unless they were part of matriculation in a vocational school. Also, we excluded studies solely targeting participants with a diagnosed mental health disorder or previous suicide attempt or self‐harm, or known suicidal ideation.
Types of interventions
We included any intervention that: a) targeted students without known suicidal risk (i.e. primary prevention), b) had the prevention of suicide as one of its primary purposes, and c) was delivered in the post‐secondary educational setting in any country. Examples of interventions included classroom‐based instructional programs, restricted access to lethal means (e.g. firearms), peer support programs, screening to identify suicide risk factors before development of suicidal ideation or behavior (e.g. substance abuse), and suicide awareness campaigns (CDC 1994). We excluded intervention programs that focused solely on early detection of suicidal ideation or planning and therapeutic interventions for known suicide risk, such as anti‐depressant medication (secondary prevention) and interventions to ameliorate the consequences of suicide attempts or other suicidal behavior (tertiary prevention) (SPAN 2001).
Types of outcome measures
Primary outcomes
Our primary outcomes of interest were:
Completed suicide; and
Suicide attempt, which we defined as self‐injury with intent to die, as opposed to non‐suicidal self‐injury (Lloyd‐Richardson 2007).
We excluded assisted suicide because the type and focus of interventions for this outcome are likely to differ from those for non‐assisted suicide, and there is disagreement ‐‐ political, legal, and social ‐‐ about whether it is an appropriate prevention target.
Secondary outcomes
Secondary outcomes included suicidal ideation (i.e. thoughts, preparation, and planning), changes in knowledge and attitudes (e.g. knowledge of suicide or suicide prevention, suicide prevention self‐efficacy/self‐expectation, and attitudes toward suicide), changes in behavior including help‐seeking (e.g. use of mental health services) and helping others at risk (e.g. "gatekeeper" behavior), and lethal means availability.
When studies had multiple outcome measures of the same construct, we selected one outcome measure based on a predetermined hierarchy described elsewhere (Data extraction and management).
Search methods for identification of studies
In order to reduce publication and retrieval bias we did not restrict our search by language, date, or publication status.
Electronic searches
Using methods described elsewhere (Goss 2007), we developed a sensitive, database‐neutral search strategy to search electronic databases. We searched the following databases after adaptation of the free‐text search strategy to include subject headings (e.g. MeSH) specific to each database (Appendix 1):
Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library) (Issue 2, July 2011);
Cochrane Injuries Group Specialised Register (18 July 2011);
Cochrane Depression, Anxiety & Neurosis Group Specialised Registers (25 July 2011);
MEDLINE (OvidSP) (1948 to 2011 June Week 4);
Embase (Elsevier) (pre‐1966 to July 2011);
CINAHL (Cumulative Index to Nursing and Allied Health Literature) (1960 to 12 July 2011);
PsycINFO (OvidSP) (1806 to 2011 June Week 4);
ISI Web of Science: Social Science Citation Index (SSCI) 1974 to 2011;
Dissertation Abstracts International (1816 to 2011);
ERIC (Education Resources Information Center) (pre‐1966 to 2011);
NIH RePORTER (Research Portfolio Online Reporting Tools Expenditures and Results) (projects still active as of 29 June 2011);
Suicide Information and Education Collection (SIEC) database (November 2011).
We limited the literature search of the Suicide Information and Education Collection (SIEC) database to studies of suicide and suicidal behaviors, searching initially for any suicide interventions, then within this subset using terms such as post‐secondary, college, university, and higher education.
We used lateral search functions such as "related articles" or "cited by" for each included study.
Searching other resources
We reviewed bibliographies of all included studies to identify additional relevant citations. We also handsearched the following journals from 1970 (or initial publication, as shown) through 2008:
Acta Psychiatrica Scandinavica;
Archives of General Psychiatry;
British Journal of Psychiatry;
Crisis: The Journal of Crisis Intervention and Suicide Prevention (2005‐);
JAMA‐Journal of the American Medical Association;
Journal of American College Health (1982‐);
Journal of Consulting and Clinical Psychology;
Journal of the American Academy of Child and Adolescent Psychiatry;
Psychological Reports;
Suicide and Life‐Threatening Behavior (1971‐).
Although some of these journals are already being handsearched by Cochrane groups, our broader inclusion criteria for study design necessitated additional handsearching.
We sought gray literature (Conn 2003) through electronic databases, as listed above, by contacting study authors, and by screening reference lists of included studies. We also contacted or searched electronic resources (e.g. websites) of the following organizations:
American Association of Suicidology;
American Foundation for Suicide Prevention;
Australian Indigenous HealthInfoNet;
Australian Institute for Suicide Research and Prevention;
Beijing Suicide Research and Prevention Center;
Centre for Suicide Research (Denmark);
European Network for Suicidology;
International Association for Suicide Prevention;
Menzies School of Health Research (Australia);
National Prevention of Suicide and Mental Ill‐Health (Karolinska Institutet, Sweden);
National Centre for Suicide Research and Prevention (University of Oslo, Norway);
University of Oxford Centre for Suicide Research (United Kingdom);
World Health Organization (SUPRE).
Data collection and analysis
Selection of studies
Two review authors (CH, CG or VT) independently screened titles and abstracts using selection criteria for eligible study designs, participants, and interventions. We obtained the full‐text articles of studies that met inclusion criteria or that both review authors could not definitely exclude. If eligibility remained unclear after full‐text review, we contacted the study authors for clarification. If an otherwise eligible study did not report collecting eligible outcome measures, we asked the study author to provide any unpublished outcomes data. If the two review authors were unable to agree about study eligibility after full‐text review and discussion, a third review author (CD) reviewed the full‐text to determine eligibility. We recorded and managed individual study information, including year, design, intervention type and population, using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at University of Colorado Denver (Harris 2009). REDCap is a secure, web‐based application designed to support data capture for research studies, providing an intuitive interface for validated data entry; audit trails for tracking data manipulation and export procedures; automated export procedures for seamless data downloads to common statistical packages; and procedures for importing data from external sources (Harris 2009).
Data extraction and management
Two review authors (CH and CG) independently extracted information on study design, intervention type and characteristics, participants, setting, methods, outcomes, and results from all eligible studies and managed this data using Microsoft Excel. We contacted study authors for missing information. CH entered data into Review Manager and CG reviewed data entry for accuracy and completeness. If disagreement persisted following discussion, CD made a final determination.
Assessment of risk of bias in included studies
CH and CG independently assessed risk of bias using criteria developed by the Cochrane Effective Practice and Organisation of Care (EPOC) review group (EPOC 2009). If the two review authors disagreed, a third review author (CD) resolved the dispute. We assigned each methodological quality criterion one of the following ratings: low risk, unclear risk, or high risk. Operational definitions of these methodological quality criteria ratings vary by the specific quality criteria. How these ratings are defined for each criterion can be found elsewhere (EPOC 2009).
The criteria to determine the methodological quality of RCTs and CBAs were as follows:
Adequacy of sequence generation;
Allocation concealment;
Completeness of outcome data;
Participant blinding;
Selective outcome reporting;
Other potential internal and external threats to validity.
The criteria to determine the methodological quality of CITS and ITS are described elsewhere (EPOC 2009).
To summarize the quality of evidence, we used the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach. CH and CG independently assessed the evidence of outcomes across included studies. CD resolved disputes. We used the GRADE criteria for increasing or downgrading the quality level of the body of evidence for each outcome in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2008) and the McMaster (http://cebgrade.mcmaster.ca/) GRADE learning modules. We only applied the GRADE approach to evidence from RCTs, in which outcomes were meta‐analysed. We summarized the quality of evidence from non‐randomized studies narratively.
We used the following operational criteria for downgrading ratings based on heterogeneity and imprecision and upgrading ratings due to large magnitude of effect. We downgraded quality grades by one level if there was significant heterogeneity (i.e. I2 statistic ≥ 50% with P < 0.10 using the Chi2 test) between studies that could not be explained by such factors as subgroup analyses. Following recommendations by McMaster, we downgraded quality ratings by one level if an SMD 95% confidence interval (CI) contained both 0.0 (i.e. no effect) and 0.50, which we considered to be a meaningful effect. Using Cohen 1988's guidelines for interpreting SMD, we increased quality ratings by one level based on a large magnitude of effect if the SMD > 0.80.
For RCTs, we assigned the body of evidence for each outcome one of the following quality ratings, or N/A if no evidence was available:
High: further research is very unlikely to change our confidence in the estimate of effect;
Moderate: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate;
Low: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate;
Very low: we are very uncertain about the estimate.
Measures of treatment effect
We extracted and analysed dichotomous and continuous outcomes. Continuous data were analysed with means and standard deviations (SD) where available or as calculated using other estimates (e.g. from t‐tests, F‐tests, or exact P values). As the included studies used different scales, we estimated standardized mean difference (SMD) values using Review Manager's formula based on Hedges' g which adjusts for small sample bias. We used 95% CIs for individual study and summary estimates. For dichotomous outcomes, we converted odds ratios to SMD using the Cox logit formula (Sánchez‐Meca 2003).
Unit of analysis issues
For clustered studies with unit of analysis issues (Drabek 1991; Holdwick 2000; Tompkins 2009), we extracted data on sample size, average cluster size, and SDs by intervention group. We then corrected the group SDs for clustering using a published interclass correlation coefficient (ICC) of 0.07 (Jacobson 2011).
Dealing with missing data
We asked study authors to provide any missing summary data, or failing that, data to derive the required summary data. If they were unable to provide this, we attempted to derive the data from other reported study statistics. If we could not obtain or derive the data, we analysed the study narratively.
Where included studies did not state that results were reported using an intention‐to‐treat analysis for primary outcomes, we contacted study authors to request the necessary data. In the event of non‐response, we analysed results as reported.
Assessment of heterogeneity
We analysed statistical heterogeneity using the Chi2 test and I2 statistic (Higgins 2003). As detection of heterogeneity has low power with a small numbers of studies, we used an alpha of P ≤ 0.10 (Dickersin 1992). We considered statistical heterogeneity to be significant if the I2 statistic was ≥ 50% with a P value < 0.10, and moderate if only one of the two criteria was met. We also examined study participants, interventions (within broadly categorized types – see Data synthesis below), and outcomes for evidence of clinical heterogeneity (i.e. variability across studies in participants, interventions, or outcomes studied (Section 9.5.1 of Higgins 2008)). We described these characteristics in the Characteristics of included studies tables. We examined clinical variations in subgroup and sensitivity analyses.
Assessment of reporting biases
To reduce reporting bias, we searched for studies without publication or language restrictions, and asked the authors of included studies for any data collected but not reported. Given the small number of included studies, we did not use funnel plots to assess bias.
Data synthesis
We grouped studies according to intervention type and study design (randomized or not). All comparisons were between intervention and control groups (placebo or no intervention). We considered both statistical and clinical heterogeneity within each intervention type.
For each outcome we calculated weighted means and SDs. For main analyses, we combined multiple different intervention groups in two RCTs (Abbey 1990; Holdwick 2000) and, in one CBA (Shipley 2003), combined results from two groups that received the same (mandatory) intervention but had been divided for reporting purposes into "voluntary" and "involuntary" participants based on reported likelihood at baseline of voluntary participation in gatekeeper training. One RCT (Abbey 1989) provided combined means and SDs for two intervention groups, and we analysed the data as such. Where appropriate data were available, we conducted sensitivity analyses comparing controls to each different intervention group in two RCTs (Abbey 1990; Holdwick 2000) and to the "voluntary" and "involuntary" groups separately in one CBA (Shipley 2003).
One CBA (Pasco 2012) created and used the Suicide Intervention Training Assessment (SITA), a 14‐item instrument that measures self‐efficacy, reported as 14 individual results. As the items were directionally and conceptually similar, we calculated overall weighted mean estimates and pooled SDs for SITA results for both intervention and control groups.
In one RCT (Abbey 1989), we used the reported t‐statistics and group means and sample sizes to calculate intervention and control group SDs for two outcomes measured by the Knowledge of Suicide Test (KOST) and Suicide Intervention Response Inventory (SIRI), assuming equality of variances between groups. Because the KOST was also used in a subsequent RCT with a similar intervention and student population (Abbey 1990), we pooled the SDs.
Using an average cluster size extracted from the respective included study and ICC = 0.07 (Jacobson 2011), we corrected group SDs of clustered studies that had not accounted for clustering, and re‐analysed the data.
For one CBA (Shipley 2003) that used a binary measure of "knowledge of suicide", we converted the odds ratio to SMD using the Cox logit formula (Sánchez‐Meca 2003). The original pre‐ and post‐test results (odds ratios) are displayed in a Forest plot. The converted results are described in the text.
Among three CBAs that implemented a delayed intervention control group (Drabek 1991; Pasco 2012; Tompkins 2009), we only extracted and analysed control group data collected concurrently with post‐test measures for the intervention groups, before the controls received the intervention.
We calculated SMD values for all analyses because of the heterogeneous scales used to measure each construct. Where the direction of a scale was dissimilar from other measures, i.e. a decrease indicated improved outcome (Scale 3 ‐ Suicide and Suicide Prevention Questionnaire (SSPQ) (Holdwick 2000), Suicide Opinion Questionnaire – Acceptability Factor (SOQ‐AF) (Drabek 1991), and SIRI‐2 (Pasco 2012)), we multiplied the mean values of intervention and control groups by ‐1. We did not modify group SDs.
For RCT studies, we conducted random‐effects model meta‐analyses using inverse variance techniques to estimate SMD at post‐test between intervention and control groups.
For CBA studies, we reported individual study effect sizes without summary estimates. Insufficient data were provided to calculate mean change score SDs and correlation coefficients for intervention and control groups. As a result, we calculated SMD and 95% CIs based on post‐test results only. This approach may bias SMD as participants were not randomly allocated to intervention and control groups; however, analysis comparing baseline measures between intervention and control groups revealed no statistically significant differences.
We performed analyses in Review Manager and used an alpha value of 0.05 for statistical significance throughout this review.
We used Cohen's guidelines for interpreting SMD (small = 0.20; medium = 0.50; and large = 0.80) (Cohen 1988). For our review, an SMD of zero translates to there being no evidence of an effect from the suicide prevention intervention relative to the comparison group. The higher the SMD, the more efficacious is the intervention in enhancing the respective outcome. A negative SMD means that the suicide prevention intervention had a negative effect on the outcome relative to the comparison group (Faraone 2008). Post‐test comparisons of suicide‐related outcomes immediately following active intervention are considered "short‐term". If a later follow‐up evaluation occurred, the findings are considered "longer‐term".
Subgroup analysis and investigation of heterogeneity
Due to a lack of data on demographics, housing status (i.e. whether living on or off campus), and student workload (full vs. part‐time) and lacked study heterogeneity for level of study and institution type, we were unable to conduct subgroup analyses for relevant outcomes using random‐effects models (Borenstein 2009) as proposed. Although we proposed a subgroup analysis involving attrition (follow‐up > 80% vs. < 80%), no RCT had follow‐up < 80%. In a post hoc exploration of heterogeneity among studies of classroom instructional programs, we examined subgroups according to outcome measure used.
Sensitivity analysis
Although we proposed sensitivity analyses based on allocation concealment and randomization sequence generation, these quality parameters were similar across the three RCT studies we included in meta‐analyses. In post‐hoc sensitivity analyses, we tested the influence on suicide‐related outcomes of differing intervention groups and 'voluntary' versus 'involuntary' participant groups.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies tables.
We included eight eligible studies in this review and identified one ongoing study that met our inclusion criteria (5R01MH083740).
Results of the search
See Figure 1.
1.

PRISMA study flow diagram.
This review fully incorporates the results of searches conducted up to November 2011. We identified a further 13 documents in a search update we conducted in November 2013. However, we have not yet incorporated these into the review and will be addressed in the next review update. See Studies awaiting classification for details.
Our electronic search strategy yielded 49,503 records (CENTRAL = 775; CINAHL = 2182; Cochrane Injuries Group Specialised Register = 21; Dissertation Abstracts International = 1283; EMBASE = 9490; ERIC = 2482; MEDLINE = 12,670; NIH RePORTER = 195; PsycINFO = 12,057; SSCI = 7674; Cochrane Depression, Anxiety and Neurosis Group Specialised Register = 469 and SIEC = 205). Using forward, backward and lateral search functions on eligible studies, and screening reference lists of potentially eligible studies, we identified 47 additional records. Screening websites of national and international organizations and agencies (Searching other resources), and conference proceedings revealed no additional studies. Of 27,449 unique records, we deemed 290 potentially eligible. We examined 287 full‐text documents; we could not find the full‐text of three records and we excluded these records based on available information. Nine studies, including one ongoing study (5R01MH083740), were eligible. Also, we identified one of the nine studies (Pasco 2012) through author contact after the electronic search date. The authors of all but one study (Drabek 1991) provided additional information or data.
Included studies
We included eight completed studies: four published journal articles (Abbey 1989; Joffe 2008; Pasco 2012; Tompkins 2009) and four dissertations (Abbey 1990; Drabek 1991; Holdwick 2000; Shipley 2003). All contributed analysable outcome data. The three RCTs randomized a total of 312 students to relevant study arms. We have listed the details of the included studies in the Characteristics of included studies section.
Study designs
The eight included studies consisted of three RCTs (Abbey 1989; Abbey 1990; Holdwick 2000) and five CBAs (Drabek 1991; Joffe 2008; Pasco 2012; Shipley 2003; Tompkins 2009). Our searches did not yield any CITS or ITS studies. One RCT (Holdwick 2000) and one CBA (Drabek 1991) allocated participants by session date, and another CBA examined institutions that did and did not receive the experimental intervention (Tompkins 2009). One CBA (Joffe 2008) examined outcomes in twelve universities that were similar in location, size, and educational mission before (1975 to 1983) and after (1984 to 2004) one of the universities implemented the intervention.
Settings and populations
One study (Shipley 2003) was set in Australia and all others took place in the United States. All studies involved four‐year degree granting colleges or universities. Study participants included students enrolled in a psychology course (Abbey 1989; Abbey 1990; Holdwick 2000; Joffe 2008; Shipley 2003), peer advisors (i.e. students, generally in their third or fourth year at university, that reside and oversee peers within university student accommodation, plan social activities, and may serve as a mediator to interpersonal conflict or offer counsel to students dealing with personal issues) (Pasco 2012; Tompkins 2009), and faculty and staff (Drabek 1991).
Interventions
All interventions included both primary and secondary suicide prevention components. The three RCTs evaluated one to four week classroom‐based instruction involving suicide‐related lectures and handouts (Abbey 1989; Abbey 1990; Holdwick 2000). One RCT also included suicide vignettes (Abbey 1989) and another featured modeling and role‐play (Abbey 1990). Primary prevention components included empathetic listening, lethal means restriction (e.g. firearms), and prevention of risk factors for suicide (e.g. substance abuse). Secondary prevention components included instruction on intervening with suicidal peers and enhancing self help‐seeking if suicidal. One CBA (Joffe 2008) evaluated an institutional policy restricting access to laboratory cyanide (primary prevention) and mandating four professional assessment sessions for students threatening or exhibiting suicidal behavior (secondary prevention). The other four CBAs examined training "gatekeepers" ‐ those who are strategically positioned to recognize and refer students at risk for suicidal ideation or behavior‐ including fellow students (Shipley 2003), faculty and staff (Drabek 1991), and peer advisors (Pasco 2012; Tompkins 2009). The gatekeeper is trained to ask the student with suicide warning signs about the presence of suicidal thoughts and feelings, encourage them to seek help, and refer them to local resources to obtain needed help. Programs included Campus Connect training for peer advisors (Pasco 2012), "Question, Persuade, and Refer" training for students (Shipley 2003) and peer advisors (Tompkins 2009), respectively, and an experiential and didactic training program for faculty and staff (Drabek 1991). Gatekeeper training programs comprised one session lasting from one to three hours and generally including training in active listening (primary prevention) and in self‐efficacy and skills for responding to emotional distress or crisis (primary prevention) and suicidal threats or behavior (secondary prevention), as well as information on local mental health and crisis services.
Outcomes
Following data extraction, CH, CG, CD, and Dr. Jeffrey Gliner (see Acknowledgements) independently generated an outcome construct categorization scheme. We agreed final categorization through discussion and consensus, and measured six constructs in the included studies:
Completed suicide;
Knowledge of suicide;
Knowledge of suicide prevention;
Suicide prevention self‐efficacy;
Attitudes toward suicide;
Gatekeeper behavior.
Gochman 1997 describes self‐efficacy as a main determinant of behavioral self‐prediction (i.e. "I will perform this action"). Self‐expectation is interpreted as an individual's estimated likelihood of performing specific future behaviors. Despite the slight difference in definition, we combined self‐expectation with self‐efficacy for analytic purposes. No included studies evaluated intervention effects on suicide attempts or threats, suicidal ideation, help‐seeking behavior, or lethal means availability.
When studies collected and provided adequate data for multiple measures of primary or secondary outcomes of interest, we selected only one of those measures for analysis based on the following predetermined hierarchy applied independently by two review authors (CH and CG). We abstracted or determined study information for the hierarchy criteria through the index study or other documents, such as a validation study, by two review authors independently (CH and CG). We resolved any disagreements by discussion and referral to a third review author (CD) if necessary. We applied the following hierarchy to each measure with sufficient data for meta‐analysis:
Validity (i.e. degree to which an instrument measures what it intends to measure – operationalized as measures of construct, content, or face validity (Sushil 2010));
Specificity (i.e. extent to which the instrument only measures the construct of interest);
Reliability (i.e. repeatability and consistency);
Completeness of data (e.g. percent of missing data);
Objectivity (e.g. observed by study personnel) versus subjectivity (e.g. self‐reported);
Frequency of implementation within the included studies (i.e. of two equivalent measures, the one more frequently used);
Similarity of content between instruments (i.e. the most relevant outcome construct as determined by review authors; if review authors disagreed, we implemented the next level of the hierarchy);
Random selection if measures were still equivalent after steps 1 to 7.
After application of the hierarchy, we selected the following outcome measures with associated instruments and used them in this review:
Knowledge of suicide:
KOST (Abbey 1989);
KOST (Abbey 1990);
Recognition of Suicide Lethality Scale (RSL) (Drabek 1991);
Suicide Information Test (SIT) (Holdwick 2000);
Mental Health Literacy Scale 1‐item Questionnaire (Shipley 2003).
Knowledge of suicide prevention:
SIRI (Abbey 1989);
Suicide‐Related Vignette Questionnaire (Abbey 1990);
Assessment of Appropriate Responses Scale (AARS) (Drabek 1991);
Scale 2 ‐ SSPQ (Holdwick 2000);
SIRI‐2 (Pasco 2012);
Mental Health Literacy Scale 4‐item Questionnaire (Shipley 2003);
-
Question, Persuade, and Refer Quiz (Tompkins 2009)
Self‐evaluation of knowledge item.
Suicide prevention self‐efficacy:
Scale 3 ‐ SSPQ (Holdwick 2000);
SITA (Pasco 2012);
Generalized Self‐Efficacy Scale (Shipley 2003);
-
Question, Persuade, and Refer Quiz (Tompkins 2009)
Gatekeeper efficacy item.
Attitudes toward suicide:
SOQ‐AF (Drabek 1991);
Attitude Scale 8‐item Questionnaire (Shipley 2003).
Gatekeeper behaviors:
-
Question, Persuade, and Refer Quiz (Tompkins 2009);
Question, Persuade, and Refer behaviors item.
One study measured completed suicide (Joffe 2008).
Excluded studies
Of 290 potentially eligible studies, we excluded 282 studies. We have listed the reasons for exclusion of a small sample of these studies, representing our general reasoning for exclusion (see Characteristics of excluded studies).
Risk of bias in included studies
We successfully contacted authors of all but one included study (Drabek 1991) to obtain complete information on risk of bias. Nevertheless, some risk of bias criteria remained unclear because insufficient information was obtained.
Figure 2 shows a summary of the aggregate and Figure 3 the individual risk of bias criteria and their ratings. We have given detailed descriptions of these assessments in the Characteristics of included studies table.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
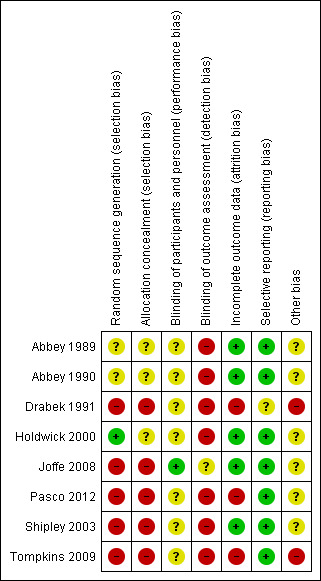
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
One clustered RCT (Holdwick 2000) was rated at low risk of selection bias based on random sequence generation. The other two RCTs (Abbey 1989; Abbey 1990) were unclear. Allocation concealment was unclear due to insufficient information in all three RCTs. Random sequence generation and allocation concealment for non‐randomized studies (Drabek 1991; Joffe 2008; Pasco 2012; Shipley 2003; Tompkins 2009) were deemed at high risk of selection bias.
Blinding
In seven studies, the risk of performance bias based on blinding of participants and personnel was unclear due to insufficient information and the risk of detection bias was high because appropriate blinding of outcome assessment was not implemented. However, participant blinding in classroom instruction and gatekeeper training interventions may not be possible. In the remaining CBA (Joffe 2008), the risk of performance bias was low because the outcome (i.e. suicide) was unlikely to be influenced by a lack of blinding and the potential for detection bias in this study was unclear.
Blinding was attempted in two studies, but deemed insufficient. In a clustered RCT (Holdwick 2000), participants and study personnel were blinded to the research hypotheses but the data assessors were not. In a CBA (Pasco 2012), participants were blinded to research hypotheses but study personnel and data assessors were not.
Incomplete outcome data
All three RCTs were judged to be at low risk of bias as outcomes data were missing for 0% (Abbey 1989), 3% (Abbey 1990), and < 10% (Holdwick 2000) of participants, respectively. Three CBAs (Drabek 1991; Pasco 2012; Tompkins 2009) were at high risk of attrition bias: outcomes data were missing for 23% to 25% (Pasco 2012) and 26% (Drabek 1991) of participants, respectively, in two studies, while the third CBA (Tompkins 2009) purposely reduced the control sample for follow‐up evaluation to alleviate burden on subjects, resulting in 39% missing outcome data. Two CBA studies were at low risk of bias: Joffe 2008 measured the cumulative incidence of student suicide as a primary outcome, while Shipley 2003 had between 1.4% and 2.9% missing outcome data for three outcomes, and 15.9% for another.
Selective reporting
Seven studies were at low risk of reporting bias. Although none had protocols available for review, each study author confirmed that the published report had all expected outcomes, including those that were pre‐specified. We were unable to contact the investigators of one CBA (Drabek 1991) to confirm pre‐specified outcomes, rendering a judgement of unclear risk of bias.
Other potential sources of bias
Three RCTs had no other biases noted. In one clustered CBA (Tompkins 2009), administrators of each institution selected their own group assignment. This may bias the study if differences in suicide‐related factors between campuses influenced choice of study group. This is also a potential concern in Drabek 1991, where investigators allocated participants to intervention or control groups based on session date, after participants chose which session to attend. However, in neither instance did the participants themselves select their group assignment. In another CBA (Joffe 2008), an intervention to enhance help‐seeking behavior was implemented for a three‐month period before the index suicide‐related institutional policy was implemented. Although the study authors concluded it did not increase the number of contacts with social workers or psychologists, it is unclear how it may have influenced the results. One clustered CBA (Tompkins 2009) showed that baseline knowledge of suicide resources was greater among control compared to treatment participants, and different testing formats between the groups were used during the post‐test phase. Another CBA (Shipley 2003) had different source populations for intervention and control groups, resulting in significant differences in age, gender and ethnicity between groups.
Effects of interventions
See: Table 1
We analysed the effects of intervention stratified by intervention type and whether randomized or not. All comparisons were between intervention and placebo or no intervention control groups. We meta‐analysed results from three RCTs testing classroom‐based instruction (Abbey 1989; Abbey 1990; Holdwick 2000) and analysed five CBA studies narratively.
Using available data (Methods ‐ Data synthesis), in one RCT (Abbey 1989), we calculated intervention and control group SDs for two outcomes, knowledge of suicide (measured by the KOST) and knowledge of suicide prevention (measured by the SIRI). More conservative pooled SDs were used for the main analysis (Analysis 1.1), since sensitivity analysis (Analysis 5.1) revealed that the statistical significance of the test for knowledge of suicide did not differ using assumed equality of variance between intervention and control groups as compared to using the estimated pooled SDs between the two similar studies.
1.1. Analysis.

Comparison 1 Classroom instruction: knowledge of suicide, Outcome 1 Post‐test differences in knowledge of suicide at the end of active intervention.
5.1. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 1 Sensitivity analysis (Abbey 1989, KOST ‐ equality of variance): post‐test differences in knowledge of suicide at the end of active intervention.
Classroom‐based instructional programs
Knowledge of suicide
Classroom instruction greatly increased short‐term knowledge of suicide in three RCTs (SMD = 1.51, 95% CI 0.57 to 2.45) with significant quantitative heterogeneity (Chi2 = 22.60; P < 0.00001; I2 = 91%; Analysis 1.1). Sensitivity analyses comparing experiential and didactic suicide prevention programs (Abbey 1990) respectively, to controls, revealed a slightly greater effect from didactic education (SMD = 1.74, 95% CI 0.56 to 2.93; Analysis 5.3) compared to experiential intervention (SMD = 1.35, 95% CI 0.41 to 2.28; Analysis 5.2). A direct comparison between the two intervention groups suggested that didactic intervention significantly enhanced short‐term knowledge of suicide relative to experiential (Analysis 4.1). Additional sensitivity analyses comparing each of two different intervention groups, an education‐based suicide prevention program (EB‐SP) and a motivational‐enhancement suicide prevention program (ME‐SP) (Holdwick 2000), respectively, to controls, revealed no statistically significant differences, with SMD = 1.50 (95% CI 0.55 to 2.46, Analysis 5.4) and SMD = 1.54 (95% CI 0.64 to 2.43, Analysis 5.5) for the two interventions, respectively. Post‐hoc exclusion of Holdwick 2000, which used a different outcome measure than did the other two RCTs, reduced but did not eliminate statistical heterogeneity (Chi2 test = 4.44; P = 0.04; I2 statistic = 77%; Analysis 5.6).
5.3. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 3 Sensitivity analysis (Abbey 1990, lecture and handouts vs. control): post‐test differences in knowledge of suicide at the end of active intervention.
5.2. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 2 Sensitivity analysis (Abbey 1990, modeling and role play vs. control): post‐test differences in knowledge of suicide at the end of active intervention.
4.1. Analysis.

Comparison 4 Experimental group comparison for classroom instruction: post‐test differences at the end of active intervention, Outcome 1 Abbey 1990, lecture and handouts vs. modeling and role play: post‐test differences in knowledge of suicide at the end of active intervention.
5.4. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 4 Sensitivity analysis (Holdwick 2000, education‐based suicide prevention program vs. control): post‐test differences in knowledge of suicide at the end of active intervention.
5.5. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 5 Sensitivity analysis (Holdwick 2000, motivational‐enhancement suicide prevention program vs. control): post‐test differences in knowledge of suicide at the end of active intervention.
5.6. Analysis.

Comparison 5 Sensitivity analyses for classroom instruction: knowledge of suicide, Outcome 6 Post‐hoc sensitivity analysis (exclusion of Holdwick 2000): assessment of statistical heterogeneity.
Knowledge of suicide prevention
In three RCTs, classroom instruction increased short‐term knowledge of suicide prevention (SMD = 0.72, 95% CI 0.36 to 1.07) with moderate statistical heterogeneity (Chi2 test = 3.98; P = 0.14; I2 statistic = 50%; Analysis 2.1). Sensitivity analyses comparing experiential and didactic suicide prevention programs (Abbey 1990), respectively, to controls, revealed no differences in effect or significance, with SMD = 0.70 (95% CI 0.35 to 1.06; Analysis 6.1) and SMD = 0.72 (95% CI 0.35 to 1.10; Analysis 6.2) for the two interventions, respectively. Furthermore, comparing the education‐based suicide prevention program and the motivational‐enhancement suicide prevention program (Holdwick 2000), respectively, to controls revealed no differences in effect or significance, with SMD = 0.71 (95% CI 0.33 to 1.10; Analysis 6.3) and SMD = 0.75 (95% CI 0.45 to 1.04; Analysis 6.4), respectively. Post‐hoc exclusion of Holdwick 2000 eliminated heterogeneity (Chi2 = 0.01; P = 0.94; I2 = 0%) (Analysis 6.5).
2.1. Analysis.

Comparison 2 Classroom instruction: knowledge of suicide prevention, Outcome 1 Post‐test differences in knowledge of suicide prevention at the end of active intervention.
6.1. Analysis.

Comparison 6 Sensitivity analyses for classroom instruction: knowledge of suicide prevention, Outcome 1 Sensitivity analysis (Abbey 1990, modeling and role play vs. control): post‐test differences in knowledge of suicide prevention at the end of active intervention.
6.2. Analysis.

Comparison 6 Sensitivity analyses for classroom instruction: knowledge of suicide prevention, Outcome 2 Sensitivity analysis (Abbey 1990, lectures and handouts vs. control): post‐test differences in knowledge of suicide prevention at the end of active intervention.
6.3. Analysis.

Comparison 6 Sensitivity analyses for classroom instruction: knowledge of suicide prevention, Outcome 3 Sensitivity analysis (Holdwick 2000, education‐based suicide prevention program vs. control): post‐test differences in knowledge of suicide prevention at the end of active intervention.
6.4. Analysis.

Comparison 6 Sensitivity analyses for classroom instruction: knowledge of suicide prevention, Outcome 4 Sensitivity analysis (Holdwick 2000, motivational‐enhancement suicide prevention program vs. control): post‐test differences in knowledge of suicide prevention at the end of active intervention.
6.5. Analysis.

Comparison 6 Sensitivity analyses for classroom instruction: knowledge of suicide prevention, Outcome 5 Post‐hoc sensitivity analysis (exclusion of Holdwick 2000): assessment of statistical heterogeneity.
Suicide prevention self‐efficacy
One RCT (Holdwick 2000) demonstrated a small, non‐significant increase in short‐term suicide prevention self‐efficacy among students who received the education‐based or motivational‐enhancement suicide prevention program compared to control students (SMD = 0.20, 95% CI ‐0.13 to 0.54; Analysis 3.1). Sensitivity analyses comparing education‐based suicide prevention programs and motivational‐enhancement suicide prevention programs to controls a somewhat greater effect size from the motivational‐enhancement suicide prevention program (SMD = 0.30, 95% CI ‐0.09 to 0.69; Analysis 7.2) than from the education‐based suicide prevention program (SMD = 0.09, 95% CI ‐0.30 to 0.48; Analysis 7.1), but effects did not differ significantly when the experimental groups were directly compared (Analysis 4.2).
3.1. Analysis.

Comparison 3 Classroom instruction: suicide prevention self‐efficacy, Outcome 1 Post‐test differences in suicide prevention self‐efficacy at the end of active intervention.
7.2. Analysis.

Comparison 7 Sensitivity analysis for classroom instruction: suicide prevention self‐efficacy, Outcome 2 Sensitivity analysis (Holdwick 2000, motivational‐enhancement suicide prevention program vs. control): post‐test differences in self‐efficacy at the end of active intervention.
7.1. Analysis.

Comparison 7 Sensitivity analysis for classroom instruction: suicide prevention self‐efficacy, Outcome 1 Sensitivity analysis (Holdwick 2000, education‐based suicide prevention program vs. control): post‐test differences in self‐efficacy at the end of active intervention.
4.2. Analysis.

Comparison 4 Experimental group comparison for classroom instruction: post‐test differences at the end of active intervention, Outcome 2 Holdwick 2000, motivational‐enhancement suicide prevention program vs. education based‐suicide prevention program: post‐test differences in self‐efficacy at the end of active intervention.
Policy‐based interventions
Completed suicide
One Midwestern US university implemented a multi‐component policy intervention involving means restriction and mandatory assessment for suicidal behavior (Joffe 2008). Before policy implementation (1980 to 1983), no evidence of a difference in the cumulative incidence of suicide was detected between the intervention institution and 11 comparable control institutions, 7.89 vs. 7.07 per 100,000 (Z = 0.33; P > 0.05). Afterward (1984 to 1990), the cumulative incidence of suicide was significantly lower at the intervention university relative to control universities, 2.00 vs. 8.68 per 100,000 (Z = 5.90; P < 0.05). Additionally, the cumulative incidence of student suicide was significantly lower at the intervention institution following implementation (2.00 (after) vs. 7.89 (before) per 100,000; Z = 2.32; P < 0.05), whereas the control institutions showed no evidence of a reduction (8.68 (after) vs. 7.07 (before) per 100,000; Z = 1.57; P > 0.05).
Gatekeeper training programs
There was no evidence of differences in suicide‐related baseline measures between intervention and control groups (Analysis 8.1; Analysis 8.2; Analysis 8.3; Analysis 8.4; Analysis 8.5; Analysis 8.6). Also, no statistically significant differences were found in suicide‐related baseline measures of "voluntary" versus "involuntary" student participants (designated according to baseline self‐reported motivation to participate, though all the students were required to participate) in a Question, Persuade, and Refer workshop (Shipley 2003) (Analysis 10.1; Analysis 10.2; Analysis 10.3; Analysis 10.4). Post‐test comparisons of the effects of gatekeeper interventions are described below.
8.1. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 1 Baseline measures of knowledge of suicide (continuous).
8.2. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 2 Baseline measures of knowledge of suicide (dichotomous).
8.3. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 3 Baseline measures of knowledge of suicide prevention.
8.4. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 4 Baseline measures of suicide prevention self‐efficacy.
8.5. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 5 Baseline measures of attitudes toward suicide.
8.6. Analysis.

Comparison 8 Gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 6 Baseline measures of gatekeeper behaviors.
10.1. Analysis.

Comparison 10 Experimental group comparisons, gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 1 Baseline measures of knowledge of suicide (Shipley 2003 ‐ dichotomous).
10.2. Analysis.

Comparison 10 Experimental group comparisons, gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 2 Baseline measures of knowledge of suicide prevention (Shipley 2003).
10.3. Analysis.

Comparison 10 Experimental group comparisons, gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 3 Baseline measures of suicide prevention self‐efficacy (Shipley 2003).
10.4. Analysis.

Comparison 10 Experimental group comparisons, gatekeeper training programs: baseline measures of suicide‐related outcomes, Outcome 4 Baseline measures of attitudes toward suicide (Shipley 2003).
Knowledge of suicide
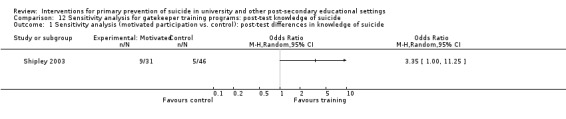
A gatekeeper training program (Drabek 1991) featuring experiential and didactic components administered to faculty and staff increased short‐term knowledge of suicide relative to no training (SMD = 0.86, 95% CI 0.28 to 1.44; Analysis 9.1). A two to three hour gatekeeper workshop delivered to students (Shipley 2003) also suggested an increase in short‐term knowledge of suicide among trained students relative to those who did not receive training (SMD = 0.63, 95% CI ‐0.02 to 1.28; original result: OR = 2.84, 95% CI 0.97 to 8.29); however, this finding was not statistically significant (Analysis 9.2). Sensitivity analyses revealed that when compared to students who received no training, students who expressed motivation to volunteer for the Question, Persuade, and Refer workshop had greater increases in short‐term knowledge of suicide (SMD = 0.73, 95% CI 0.001 to 1.47; original result: OR = 3.35, 95% CI 1.00 to 11.25; Analysis 12.1) than did those who did not express motivation to volunteer (SMD = 0.55, 95% CI ‐0.18 to 1.27; original result: OR = 2.46, 0.75 to 8.09; Analysis 12.2). However, a direct comparison between 'voluntary' and 'involuntary' participants showed no statistically significant difference in post‐test outcome (Analysis 11.1).
9.1. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 1 Post‐test differences in knowledge of suicide (continuous).
9.2. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 2 Post‐test differences in knowledge of suicide (dichotomous).
12.1. Analysis.
Comparison 12 Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide, Outcome 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in knowledge of suicide.
12.2. Analysis.

Comparison 12 Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide, Outcome 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in knowledge of suicide.
11.1. Analysis.

Comparison 11 Experimental group comparisons, gatekeeper training programs: post‐test of suicide‐related outcomes, Outcome 1 Post‐test differences in knowledge of suicide (Shipley 2003).
Knowledge of suicide prevention
One Question, Persuade, and Refer workshop delivered to students (Shipley 2003) increased short‐term knowledge of suicide prevention (SMD = 0.64, 95% CI 0.28 to 0.99; Analysis 9.3). Sensitivity analyses suggested that compared to students who received no treatment, 'voluntary' participants had a greater increase in short‐term knowledge of suicide prevention (SMD = 1.04, 95% CI 0.58 to 1.49; Analysis 13.1) than did 'involuntary' participants (SMD = 0.38, 95% CI ‐0.01 to 0.77; Analysis 13.2). A direct comparison between 'voluntary' and 'involuntary' Question, Persuade, and Refer workshop participants showed significantly greater short‐term knowledge of suicide prevention among 'voluntary' participants (SMD = 0.65, 95% CI 0.20 to 1.10; Analysis 11.2). No evidence of an effect was observed from gatekeeper training delivered to faculty and staff (Drabek 1991) (SMD = 0.06, 95% CI ‐0.50 to 0.61; Analysis 9.3) while a moderate effect was detected when delivered to peer advisors (Pasco 2012) (SMD = 0.46, 95% CI ‐0.06 to 0.98; Analysis 9.3). Question, Persuade, and Refer training delivered to peer advisors in another study (Tompkins 2009) suggested no evidence of an effect on longer‐term knowledge of suicide prevention (SMD = 0.13, 95% CI ‐0.20 to 0.46; Analysis 9.3).
9.3. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 3 Post‐test differences in knowledge of suicide prevention.
13.1. Analysis.

Comparison 13 Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide prevention, Outcome 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in knowledge of suicide prevention.
13.2. Analysis.

Comparison 13 Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide prevention, Outcome 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in knowledge of suicide prevention.
11.2. Analysis.

Comparison 11 Experimental group comparisons, gatekeeper training programs: post‐test of suicide‐related outcomes, Outcome 2 Post‐test differences in knowledge of suicide prevention (Shipley 2003).
Suicide prevention self‐efficacy
The Campus Connect program delivered to peer advisors (Pasco 2012) demonstrated a large increase in short‐term suicide prevention self‐efficacy (SMD = 0.78, 95% CI 0.24 to 1.31), while another gatekeeper training program (Shipley 2003) showed a small, non‐statistically significant effect (SMD = 0.24, 95% CI ‐0.11 to 0.59; Analysis 9.4). Sensitivity analyses (Shipley 2003) suggested a small, non‐statistically significant difference in short‐term suicide prevention self‐efficacy among both "voluntary" and "involuntary" student participants compared to students who received no training, with SMD = 0.12 (95% CI ‐0.30 to 0.55; Analysis 14.1) and SMD = 0.32 (95% CI ‐0.08 to 0.71; Analysis 14.2), respectively. A direct comparison between 'voluntary' and 'involuntary' participants showed no statistically significant difference in post‐test outcome (Analysis 11.3). Question, Persuade, and Refer training delivered to peer advisors (Tompkins 2010) showed no evidence of an effect on longer‐term suicide prevention self‐efficacy (SMD = 0.15, 95% CI ‐0.18 to 0.48; Analysis 9.4).
9.4. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 4 Post‐test differences in suicide prevention self‐efficacy.
14.1. Analysis.

Comparison 14 Sensitivity analysis for gatekeeper training programs: post‐test suicide prevention self‐efficacy, Outcome 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in suicide prevention self‐efficacy.
14.2. Analysis.

Comparison 14 Sensitivity analysis for gatekeeper training programs: post‐test suicide prevention self‐efficacy, Outcome 2 Sensitivity analysis (involuntary participation vs. control): post‐test differences in suicide prevention self‐efficacy.
11.3. Analysis.

Comparison 11 Experimental group comparisons, gatekeeper training programs: post‐test of suicide‐related outcomes, Outcome 3 Post‐test differences in suicide prevention self‐efficacy (Shipley 2003).
Attitudes toward suicide
A gatekeeper training program administered to faculty and staff (Drabek 1991) and a Question, Persuade, and Refer workshop given to students (Shipley 2003) demonstrated no evidence of an effect on short‐term attitudes toward suicide, with SMD = 0.06 (95% CI ‐0.50 to 0.61) and SMD = 0.06 (95% CI ‐0.28 to 0.41) respectively (Analysis 9.5). Sensitivity analyses (Shipley 2003) displayed a slight, non‐statistically significant difference in effect between "voluntary" and "involuntary" participation when compared to students who received no treatment, SMD = 0.21 (95% CI ‐0.23 to 0.64; Analysis 15.1) and SMD = ‐0.04 (95% CI ‐0.43 to 0.35; Analysis 15.2), respectively. A direct comparison between 'voluntary' and 'involuntary' participants showed no statistically significant difference in post‐test outcome (Analysis 11.4).
9.5. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 5 Post‐test differences in attitudes toward suicide.
15.1. Analysis.

Comparison 15 Sensitivity analysis for gatekeeper training programs: post‐test attitudes towards suicide, Outcome 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in attitudes towards suicide.
15.2. Analysis.

Comparison 15 Sensitivity analysis for gatekeeper training programs: post‐test attitudes towards suicide, Outcome 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in attitudes towards suicide.
11.4. Analysis.

Comparison 11 Experimental group comparisons, gatekeeper training programs: post‐test of suicide‐related outcomes, Outcome 4 Post‐test differences in attitudes towards suicide (Shipley 2003).
Gatekeeper behavior
Among peer advisors who received a Question, Persuade, and Refer training compared to no training (Tompkins 2009), no evidence of a longer‐term effect on suicide‐related gatekeeper behavior was found (SMD = ‐0.01, 95% CI ‐0.34 to 0.32; Analysis 9.6).
9.6. Analysis.

Comparison 9 Gatekeeper training programs: post‐test measures of suicide‐related outcomes, Outcome 6 Post‐test differences in gatekeeper behaviors.
Discussion
Summary of main results
Our review identified eight eligible, completed studies, only one of which provided any data on completed suicides, our primary outcome. The lack of studies examining health outcomes is an important finding that demonstrates a major gap in the research literature. Seven studies assessed only indirect measures, including suicide‐related knowledge, attitudes, and self‐reported gatekeeper behavior. As these measures have neither been directly linked to health outcomes, nor indirectly linked to health outcomes through correlation with previously validated measures, it is unclear whether observed changes in the measures will result in reductions in suicidal behavior or completed suicide. While completed suicides are rare, non‐fatal suicidal behavior (i.e. suicide attempts) is more common and therefore potentially feasible to measure in intervention studies. As such studies become available, combining them quantitatively through meta‐analysis may provide sufficient power to assess intervention effects on this important health outcome.
This review aimed to summarize the best available evidence on interventions for the primary prevention of suicide in post‐secondary settings. However, all of the included studies evaluated interventions targeting students at both the primary and secondary prevention levels. Hence we were unable to determine the independent effect of primary preventive interventions on suicide‐related outcomes.
The studies were heterogeneous in terms of participants, study designs, and interventions. As specified in our protocol (Harrod 2011), the main effects identified in the included studies are described according to the type of intervention implemented (see below). We have presented results, GRADE ratings, and associated comments from studies of classroom‐based instructional programs can be found in Table 1. Results from studies of gatekeeper training programs can be found in Table 2. We did not summarize results from the single study evaluating institutional policy in a table.
1. Findings for gatekeeper training programs (non‐randomized studies).
| What are the effects of gatekeeper training programs on suicidal behavior and ideation, knowledge of suicide and suicide prevention, suicide prevention self‐efficacy, attitudes toward suicide and gatekeeper behavior? | ||
|
Patient or population: Post‐secondary students, faculty and staff Settings: Public and private universities located in urban and rural settings Intervention: Campus Connect and Question, Persuade, and Refer gatekeeper training programs and workshops Comparison: Delayed treatment control groups or no treatment | ||
| Outcomes | SMD (95% CI) | Number of participants (studies) |
| Completed suicide at the end of active intervention | N/A | N/A |
| Suicidal ideation at the end of active intervention | N/A | N/A |
| Attempted suicide at the end of active intervention | N/A | N/A |
| Knowledge of suicide at the end of active intervention | 0.86 (0.28 to 1.44) 0.63 (‐0.02 to 1.28) |
53 (1 study) 116 (1 study) |
| Knowledge of suicide prevention at the end of active intervention | 0.06 (‐0.50 to 0.61) 0.46 (‐0.06 to 0.98) 0.64 (0.28 to 0.99) 0.13 (‐0.20, 0.46)† |
53 (1 study) 65 (1 study) 136 (1 study) 146 (1 study) |
| Suicide prevention self‐efficacy at the end of active intervention | 0.78 (0.24 to 1.31) 0.24 (‐0.11 to 0.59) 0.15 (‐0.18 to 0.48)† |
64 (1 study) 136 (1 study) 146 (1 study) |
| Attitudes toward suicide at the end of active intervention | 0.06 (‐0.50 to 0.61) 0.06 (‐0.28, 0.41) |
53 (1 study) 134 (1 study) |
| Gatekeeper behavior at the end of active intervention | ‐0.01 (‐0.34 to 0.32)† | 146 (1 study) |
†Post‐test outcomes measured at four to six months follow‐up.
Classroom‐based instructional programs
In three RCTs, totaling 312 students (Abbey 1989; Abbey 1990; Holdwick 2000), classroom instruction featuring experiential and didactic components greatly increased short‐term knowledge of suicide and also improved knowledge of suicide prevention, but had little or no evidence of an effect on short‐term suicide prevention self‐efficacy (Table 1). In one RCT (Abbey 1990), a large, statistically significant difference was detected between experiential and didactic classroom instruction on students' short‐term knowledge of suicide, suggesting that didactic intervention may be more beneficial (Analysis 4.1). Although differences were not statistically significant (Analysis 4.2), motivational enhancement programs may improve students' short‐term suicide prevention self‐efficacy more than education‐based instruction. None of the RCTs tested long‐term effects of the instructional interventions nor the effects on suicidal behavior or completed suicides among students. Differing outcome measures may have contributed to observed statistical differences in results between studies, as exclusion of one trial (Holdwick 2000) that used a different instrument from the other two (Abbey 1989; Abbey 1990) reduced or eliminated these differences for knowledge‐related outcomes.
Policy‐based intervention
An institutional policy restricting access to lethal means and mandating students who threaten or attempt suicide to receive four sessions of professional assessment (with threat of dismissal from the institution for failure to comply) (Joffe 2008) significantly reduced the cumulative incidence of suicide relative to 11 comparable control institutions. It was not possible to differentiate the effect of means restriction from the effects of mandatory professional assessment as both interventions were implemented during the same time period.
Gatekeeper training programs
Gatekeeper training programs delivered to students, peer advisors, and faculty and staff yielded diversity in the statistical significance and magnitude of effects (Table 2) in four CBAs (Drabek 1991; Pasco 2012; Shipley 2003; Tompkins 2009). A 1.5‐hour gatekeeper training program (Drabek 1991) delivered to faculty and staff significantly enhanced short‐term knowledge of suicide, as did a two to three hour Question, Persuade, and Refer gatekeeper training workshop (Shipley 2003) delivered to students. A three‐hour Campus Connect program (Pasco 2012) given to peer advisors suggested that the intervention improved short‐term suicide prevention self‐efficacy, and that experiential and didactic training was superior to didactic training alone. In one clustered CBA (Tompkins 2009), there was no evidence of improvements in knowledge, attitudes or behavior four to six months after a one hour Question, Persuade, and Refer training for peer advisors. Intervention duration appeared to influence results, as effects sizes for short‐term knowledge of suicide prevention and self‐efficacy were apparently greater for interventions of longer (Pasco 2012; Shipley 2003) versus shorter duration (Drabek 1991; Tompkins 2009). Additionally, in one CBA (Shipley 2003), "voluntary" participation in a Question, Persuade, and Refer workshop (determined by self‐reported motivation to participate at baseline) was generally associated with enhanced suicide‐related outcomes compared to "involuntary" participation, relative to students who did not participate.
Overall completeness and applicability of evidence
Our objective was to evaluate the effects of a broad range of post‐secondary primary prevention suicide interventions on suicide‐related outcomes. However, the body of evidence was incomplete in several areas. The evidence regarding the effect of primary suicide prevention programs in post‐secondary institutions on the most important health outcomes is limited to one study reporting completed suicides. We were unable to assess the effect of any intervention on suicidal attempts, threats, or ideation or help‐seeking behavior since no identified studies evaluated these outcomes. Only one CBA tested the influence of a suicide‐related institutional policy, which has yet to be replicated. We did not identify any ITS or CITS studies. Such designs would have been most applicable to policy interventions; only one identified study evaluated this type of intervention. Hence evidence regarding policy effects is lacking. Only one study (Joffe 2008) examined long‐term outcomes, and all but two assessed outcomes only immediately after intervention. Therefore, whether improvements in knowledge or attitudes persist over time is unknown. Furthermore, none of the instructional or gatekeeper interventions lasted more than a few weeks or hours, respectively. Whether greater effects would be seen with more intensive or longer‐term interventions has not been evaluated. Lack of data prevented our conducting relevant subgroup analyses to examine modification of intervention effects by class status, gender, residence on versus off campus, or other characteristics.
Due to the lack of diversity in the source populations, the generalizability of our findings may be limited. Only undergraduates taking psychology courses at their respective institutions enrolled in the classroom‐based instructional programs being tested. These results may not be externally valid across disciplines since psychology students may have been more eager, trained, or attentive to the intervention, leading to more beneficial effects on suicide‐related outcomes. Some of the gatekeeper interventions involved training of peer advisors in campus housing, which may have limited applicability to students living off campus or to non‐residential campuses. For example, among nearly 250 national universities in the US, nearly two‐thirds of the undergraduate population, on average, lives off campus (Haynie 2013). The included studies provided little or no information about their samples in terms of sociocultural characteristics that have been associated with differences in suicide risk, such as sex, race, or ethnicity (Liu 2013). Primary prevention interventions that target the general majority population may not be culturally relevant to minority students, potentially reducing their effectiveness in such subgroups, thereby exacerbating existing health disparities. Results may not be generalizable to students in graduate or professional schools. The gatekeeper training programs were delivered to more diverse participants, suggesting greater generalizability. However, seven of eight studies were conducted in the United States, and all were implemented in high‐income countries. As stated by Bertolote 2004, "Since suicide is intrinsically affected by sociocultural factors, there is no safe indication that what has worked somewhere will work elsewhere". It is unclear whether these results can be generalized to other systems of higher education, particularly outside the United States, or to low‐ or middle‐income countries.
Quality of the evidence
All included studies demonstrated high risk of bias on at least one criterion, and either high or unclear risk of bias on the majority of risk of bias criteria.
Two RCTs (Abbey 1989; Abbey 1990) had unclear risk of bias regarding selection biases; and only one RCT (Holdwick 2000) had known methods for random sequence generation, but it lacked adequate information regarding allocation concealment. The most significant limitation of the CBAs is the lack of randomization, which renders these studies vulnerable to selection biases and thus questionable internal validity. However, for a CBA to be eligible for this review, the participants could not self‐select treatment or control status, and all outcomes had to be assessed concurrently, removing the potential for secular changes influencing the results. These inclusion criteria likely increased the quality of evidence.
We independently rated outcomes for RCTs using the GRADE approach (Table 1). Only classroom‐based instructional programs were evaluated with RCTs; therefore, suicide‐related knowledge and suicide prevention self‐efficacy were rated, whereas no evidence was available to rate the body of evidence for the key health outcomes of completed suicide, suicide attempt and suicidal ideation, which were not assessed by RCTs.
The quality of the body of evidence for classroom instruction interventions on suicide‐related knowledge and suicide prevention self‐efficacy received ratings of low to moderate. In general, the high risk of bias of the studies evaluating institutional policy intervention and gatekeeper training programs substantially reduced the quality of the body of evidence for studied outcomes. When taking into account the strengths and limitations of the quality of evidence provided by these studies, the overall body of evidence does not permit robust conclusions regarding the objectives of this review. We have described the quality of evidence by intervention type in detail below.
Classroom‐based instructional programs
Knowledge of suicide
The quality of the body of evidence for knowledge of suicide was moderate based on three RCTs that included 312 participants. We downgraded the quality of evidence by one level based on risk of selection, performance, and detection biases and another for unexplained heterogeneity between studies. We upgraded the quality of evidence by one level based on a large magnitude of effect. We did not downgrade for indirectness of evidence, lack of precision, or high probability of publication bias.
Knowledge of suicide prevention
The quality rating for knowledge of suicide prevention was moderate based on three RCTs, totaling 312 participants. We decreased the quality of evidence by one level due to risk of selection, performance, and detection biases. We downgraded the quality of evidence by another level for statistical imprecision. However, we did not downgrade for unexplained heterogeneity, indirectness of evidence, or high probability of publication bias.
Suicide prevention self‐efficacy
The quality of the body of evidence for suicide prevention self‐efficacy was rated as low, based on one RCT including 152 participants. We downgraded the quality of evidence by one level due to the potential for selection, performance, and detection biases. We downgraded an additional level for imprecision. We did not downgrade the quality of evidence based on unexplained heterogeneity, indirectness of evidence, or high probability of publication bias.
Regardless of outcome, the direction of effects for all classroom‐based instructional programs indicated that the intervention was beneficial relative to the control. However, the magnitude of effect varied, with significant heterogeneity observed for knowledge of suicide (Analysis 1.1) and moderate heterogeneity for knowledge of suicide prevention (Analysis 2.1).
Policy‐based interventions
Completed suicide
One study examined effects of a policy intervention on suicide within 12 universities. The study lacked randomization and other methodological quality criteria (Figure 3), which reduced the quality of evidence. The quality of evidence for effect of the institutional policy on completed suicide was likely unaffected by indirectness of evidence, lack of precision, or high probability of publication bias. Evaluation of the multi‐component institutional policy has yet to be replicated. Demonstrating the effect of the policy at other post‐secondary institutions would support external validity.
Gatekeeper training programs
Despite the limitations of the studies evaluating gatekeeper training programs, primarily due to study design (CBAs) with consequent high risk of bias, the direction of effects for suicide‐related outcomes was consistent across studies. However, the magnitude of effects observed in the individual CBAs ranged from small to large, suggestive of statistical heterogeneity, for short‐term outcomes (Table 2), while only one study, a CBA, evaluated longer‐term outcomes and showed no evidence of an effect (Table 2). The quality of the body of evidence from gatekeeper training programs for each of these outcomes was likely not affected by indirectness of evidence or high probability of publication bias, but may be reduced by imprecision as the CBAs ranged from only 53 to 146 participants in each study.
Potential biases in the review process
A significant strength of our review are the comprehensive searches of multiple bibliographic databases and diverse sources of gray literature, without date, publication, or language restrictions. Furthermore, of the 290 records that were deemed potentially eligible, we were only unable to obtain the full‐text articles of three studies. This comprehensive search likely mitigated publication and other potential biases related to the review process. Nevertheless, it is possible that our search strategy did not identify every eligible study, which may introduce bias.
Our review methods, which included a duplicate assessment of study eligibility, hierarchy selection, categorization scheme, entered data, risk of bias, and GRADE ratings, as well as a third assessment if disagreement occurred, likely alleviated bias.
We conducted our initial electronic searches in November 2011. We performed an updated electronic search in November 2013. We have not incorporated potentially eligible studies identified through the updated search (Characteristics of studies awaiting classification) into the results of this review. The lag period since the last literature search incorporated into the results of this review is a potential source of bias.
In one RCT (Abbey 1989), the group SDs for knowledge of suicide were not given and could not be obtained directly; therefore, we used conservative methods to estimate them, which may have biased the effect size towards the null. Some included studies used multiple intervention groups (Abbey 1990; Holdwick 2000) or provided intervention group data separately according to self‐reported baseline information (Shipley 2003), which we combined for main analyses. Significant differences between intervention groups were not detected, but combining them may have biased effect sizes towards or away from the null compared to analyses using individual intervention groups. We detected significant differences between students motivated and not motivated to participate in a Question, Persuade, and Refer workshop compared to controls who received no intervention, for two outcomes. When these two groups were combined for main analyses, the effect size for knowledge of suicide prevention was statistically significant (P = 0.0004), while effect on knowledge of suicide was marginally significant (P = 0.06). We have therefore also reported the individual effects of the Question, Persuade, and Refer workshop participants according to their voluntary motivation, compared to controls (Analysis 12.1; Analysis 12.2; Analysis 13.1; Analysis 13.2; Analysis 14.1; Analysis 14.2; Analysis 15.1; Analysis 15.2) as well as direct comparisons between the two motivational groups (Analysis 11.1; Analysis 11.2; Analysis 11.3; Analysis 11.4).
We used a published, conservative ICC to correct group SDs for clustering; this adjustment may have biased some results towards or away from the null depending on the true ICC.
In general, data availability was problematic, which prevented analyses of CBAs using mean gain scores. Because only post‐test differences were analysed for CBAs and the participants were not randomized at baseline, differences may exist between intervention and control groups. Although none of the baseline measures were significantly different between groups (Analysis 8.1; Analysis 8.2; Analysis 8.3; Analysis 8.4; Analysis 8.5; Analysis 8.6), bias could still be introduced based on attenuated or increased group means at baseline.
Agreements and disagreements with other studies or reviews
We found no other systematic reviews evaluating primary prevention of suicide in the post‐secondary educational setting. However, existing reviews have addressed similar types of interventions in other settings and, despite different inclusion criteria, have reached generally similar conclusions in terms of the geographic distribution of study populations, strength of the body of evidence, intervention effects, and research needs.
Classroom‐based instructional programs
A number of systematic reviews previously evaluated the effect of classroom‐based instruction for suicide awareness and prevention delivered in the educational setting, although none identified studies in post‐secondary educational institutions (Guo 2002; Harden 2001; Hider 1998; Katz 2013; Mann 2005; Miller 2009; Ploeg 1999). Nearly all reviews limited their searches to English‐language literature, and most to published studies, while all included a wider range of study designs, particularly cohort studies, than our review. Like our review, the majority of identified studies in other reviews were from the United States, with most of the rest from other high‐income English‐speaking countries. Previous reviews concluded that classroom‐based curricular programs may improve suicide‐related knowledge, awareness and attitudes, mental health indicators (e.g. stress), and problem‐solving skills or coping strategies. Several also noted some evidence that programs focused on raising awareness of suicide resulted in harmful effects on suicide‐related attitudes, hopelessness, and coping (Guo 2002; Hider 1998; Ploeg 1999). Previous reviews found few methodologically sound, controlled evaluations overall, and few or no high‐quality studies evaluating intervention effects on suicidal ideation or behavior. Katz 2013 reported that there was moderate quality evidence of a reduction in suicide attempts among secondary education students after one universal awareness and education program, Signs of Suicide (SOS), but only three‐month follow‐up was available and the evaluation has not been replicated. Other reviews concluded that there was insufficient evidence to either support or not to support curriculum‐based suicide prevention programs in schools targeted to the general population at average risk. All reviews identified a need for methodologically sound studies of classroom‐based curricula that assess long‐term suicide‐related behavioral outcomes including attempts and completions.
Lethal means restriction
No other systematic reviews have evaluated means restriction in the post‐secondary setting. A meta‐review by Crowley 2004 identified three systematic reviews that considered the evidence on limiting access to suicide means among youths, and found a lack of studies evaluating effects on suicide rates. There was some evidence in support of the restriction of acetaminophen packet size for reduction of fatal overdoses. However, these three reviews are over 15 years old and are unlikely to reflect current literature. CDC 2003 evaluated laws restricting firearms and found insufficient evidence to determine the effectiveness of any of the firearms laws or combinations of laws reviewed on violent outcomes. Another systematic review (Mann 2005) found that suicide may be reduced by restriction of lethal means, including firearm control legislation, detoxification of domestic gas, restrictions on the prescription and sale of barbiturates, changing the packaging of analgesics to blister packets, and construction of barriers at jumping sites, among other means. Similarly, a systematic review (Cox 2013) found that restricting access to means in places commonly used for suicide reduced suicide and usually did not result in substitution of other locations. However, nearly all of these interventions were evaluated using ecological studies. Further, these types of means restriction may or may not be applicable to the post‐secondary educational setting. Consistent with previous reviews, we found in one study (Joffe 2008) that lethal means restriction (when combined with a policy mandating professional assessment after suicide attempts) was associated with reduced suicide rates.
Gatekeeper training programs
Mann 2005 identified two cohort studies evaluating multilevel gatekeeper training programs conducted in military settings, both of which reported reduced suicide rates. It is unclear, however, whether these findings can be generalized to post‐secondary educational settings, and the risk of bias of these two observational studies was not examined. Two other systematic reviews that evaluated gatekeeper training programs limited searches to studies published in English, included observational studies, and neither identified nor included any studies in post‐secondary settings. Isaac 2009 evaluated gatekeeper training programs delivered in any setting while Katz 2013 reviewed school‐based programs. As in our review, both reviews found few high quality studies evaluating gatekeeper training. The majority of studies in both reviews were from the US or Canada, with the rest from other high‐income countries. These two reviews, like ours, concluded that gatekeeper training had positive effects on knowledge, attitudes, and self‐efficacy, but evidence was lacking on persistence of these changes long‐term and on effects of training on gatekeeper behavior and suicidal behavior. The review authors identified research needs for high‐quality evaluations of long‐term effects of gatekeeper training programs on suicidal ideation and behavior.
Other interventions
Reviews of other types of interventions implemented outside the post‐secondary educational setting have identified screening as a strategy that has promise but needs further evaluation to determine effectiveness for preventing suicide among the general population. A review of English‐language studies by the US Preventive Services Task Force (O'Connor 2013) found that screening tools used in mental health settings were reasonably accurate in identifying adults at‐risk of suicide; however the conclusions could not be extended to the general population due to a lack of studies in primary care settings. Evidence about the effectiveness of screening in preventing suicide or suicide attempts was insufficient. Another systematic review of English‐language, quasi‐experimental studies of communities in Japan with high suicide rates found reductions in the incidence of suicide following implementation of community depression screening, referral, and health education, although the quality of the included studies was not assessed (Oyama 2008). One systematic review (Mann 2005) concluded that physician education reduced suicide among patients, but the quality of studies was not assessed.
Authors' conclusions
Implications for practice.
A variety of interventions for the primary prevention of suicide, including classroom instruction, gatekeeper training programs, and campus‐wide policies, have been evaluated in the post‐secondary educational setting. There was no evidence evaluating the effects of brief classroom‐based instructional programs or gatekeeper training programs on suicidal behavior. Such programs did increase short‐term knowledge of suicide and suicide prevention, and gatekeeper training may also improve suicide prevention self‐efficacy, but there was substantial heterogeneity among the studies and no evidence of long‐term improvements in knowledge or attitudes. An institutional policy intervention consisting of lethal means restriction and mandated professional assessment of suicidal students was shown to decrease the incidence of suicide in one controlled study that has not been replicated. All included studies had methodological deficiencies that increased the risk of bias. Given the small number of studies identified, the use of proxy measures in nearly all included studies, and the generally low quality of the body of evidence, we conclude that there is insufficient evidence to support widespread implementation of any of the studied programs or policies for the primary prevention of suicide in post‐secondary educational settings.
Implications for research.
While many populations of young adults other than post‐secondary students are also at high risk of suicide, university campuses offer unique access to a high‐risk population and important potential opportunities for primary prevention through curricular changes, social norming, and campus policies. New research is needed that evaluates the effects of educational and training programs for the primary prevention of student suicide on suicidal intent and behavior. While some evidence suggests that such programs may result in short‐term improvements in suicide‐related knowledge and self‐efficacy in the student population, evidence linking these changes to reductions in suicidal behavior within the student population is lacking. Further, there is a dearth of well‐designed and controlled studies with long‐term follow‐up, which are necessary to determine whether any observed changes persist.
Additional studies are needed that evaluate the effects of institutional policies that attempt to reduce student suicide. Only one CBA study evaluated an institutional policy, which has not been replicated. Further study is needed to attempt to replicate the findings with more rigorously designed trials and to evaluate other types of institutional policies that may mitigate suicide risk.
None of the identified studies focused solely on primary prevention of suicide. This is not necessarily a deficiency, since the integration of more population‐based approaches with clinical strategies may have a greater overall impact than either in isolation (Bertolote 2004). Nevertheless, it is important to examine the effectiveness and cost‐effectiveness of different strategies alone and in combination, in order to determine the best and most efficient approaches to preventing suicide in this high‐risk population.
Only one of the eight included studies was conducted outside of the United States. Additional research is needed to examine the effects of suicide prevention programs in post‐secondary institutions located in other high‐income countries, as well as in low‐ and middle‐income countries throughout the world.
Acknowledgements
Eryn Callihan, Rammohan Kummathi, and Sarah Morehouse conducted hand searching. Dustin Currie retrieved full‐text documents and Vedavani Tiruveedhula conducted handsearching, retrieved full‐text documents, and performed initial screens of titles and abstracts. Dr. Jeffrey Gliner (now retired) made substantive contributions to the planning of the data analysis and categorization of outcome measures, and critically reviewed the protocol.
Appendices
Appendix 1. Search strategy
Cochrane Injuries Group Specialised Register
suicide* or “domestic gas” or “gun control” or “firearm training” or “intervention skills” or “troubled peers” or “bereavement group” or “vehicle exhaust”
Cochrane Depression, Anxiety and Neurosis Group Specialised Register
*suicid*
“domestic gas”
“gun control”
“firearm training”
“intervention skills”
“troubled peers”
“bereavement group”
“vehicle exhaust”
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8
Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library)
MeSH descriptor: [Suicide] this term only
MeSH descriptor: [Suicide, Attempted] this term only
MeSH descriptor: [Suicidal Ideation] this term only
suicides (Word variations have been searched)
#1 or #2 or #3
MeSH descriptor: [Mass Screening] this term only
MeSH descriptor: [Community Mental Health Services] explode all trees
MeSH descriptor: [Preventive Health Services] explode all trees
MeSH descriptor: [Primary Prevention] explode all trees
MeSH descriptor: [Public Health Administration] explode all trees
MeSH descriptor: [Public Health] explode all trees
MeSH descriptor: [Education] explode all trees
#6 or #7 or #8 or #9 or #10 or #11 or #12
#5 and #13
"suicide risk" (Word variations have been searched)
"suicide prevention" (Word variations have been searched)
"suicide news" (Word variations have been searched)
"suicide awareness" (Word variations have been searched)
"suicide survivors" (Word variations have been searched)
"suicide rates" (Word variations have been searched)
"suicide warning signs" (Word variations have been searched)
#15 or #16 or #17 or #18 or #19 or #20 or #21
"teenage suicide" (Word variations have been searched)
"youth suicide" (Word variations have been searched)
#23 or #24
"effects of suicide" (Word variations have been searched)
"firearms for suicide" (Word variations have been searched)
#26 or #27
"troubled peers" (Word variations have been searched)
"bereavement group" (Word variations have been searched)
#29 or #30
"domestic gas" (Word variations have been searched)
"vehicle exhaust" (Word variations have been searched)
#32 or #33
"gun control" (Word variations have been searched)
"firearm training" (Word variations have been searched)
"intervention skills" (Word variations have been searched)
#35 or #36 or #37
#4 or #14 or #22 or #25 or #28 or #31 or #34 or #38
suicide (Word variations have been searched)
gassing (Word variations have been searched)
trends (Word variations have been searched)
guns (Word variations have been searched)
#40 and (#41 or #42 or #43)
#39 or #44
MEDLINE (OvidSP)
suicide/ or suicidal ideation/ or suicide, attempted/
suicides.mp.
Mass Screening/
exp *Community Mental Health Services/
*Preventive Health Services/
exp *Public Health/
exp *Public Health Administration/
exp *Education/
*Primary Prevention/
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9
(suicide adj (warning signs or risk* or prevent* or news or awareness or survivor* or rate*)).mp.
((youth or teenage* or 'effects of' or 'firearms for') adj suicide).mp.
bereavement group.mp.
troubled peers.mp.
3 or 4 or 5 or 6 or 7 or 8 or 9
2 and 15
13 or 14
domestic gas.mp.
vehicle exhaust.mp.
18 or 19
gun control.mp.
firearm training.mp.
intervention skills.mp.
21 or 22 or 23
1 or 11 or 12 or 16 or 17 or 20 or 24
suicide.mp.
gassing.mp.
trends.mp.
guns.mp.
27 or 28 or 29
26 and 30
25 or 31
Animals/
Humans/
33 not (33 and 34)
32 not 35
PsycINFO (OvidSP)
suicides
suicide/ or suicidal ideation/ or suicide, attempted/
“mass screening”/
exp *”community mental health services”/
*”preventive health services”/
*”primary prevention”/
exp *”public health”/
exp *education/
or/ 3‐8
2 and 9
“suicide risk”
“suicide warning signs”
“suicide prevention”
“suicide news”
“suicide awareness”
“suicide survivors”
“suicide rates”
or/ 11‐17
“teenage suicide”
“youth suicide”
or/ 19‐20
“effects of suicide”
“firearms for suicide”
or/ 22‐23
“bereavement group”
“troubled peers”
or/ 25‐26
“domestic gas”
“vehicle exhaust”
or/ 28‐29
“gun control”
“firearm training”
“intervention skills”
or/ 31‐33
1 or 10 or 18 or 21 or 24 or 27 or 30 or 34
suicide
gassing
trends
guns
36 and (37 or 38 or 39)
35 or 40
animals/
humans/
42 not (42 and 43)
41 not 44
EMBASE (Elsevier)
suicides
‘suicide’/mj or ‘suicidal ideation’/mj or ‘suicide, attempt’/mj
‘mass screening’/exp
‘mental health service’/exp/mj
‘preventive health service’/exp/mj
‘primary prevention’/mj
‘public health service’/exp/mj
‘public health’/exp/mj
‘health education’/exp/mj
‘education’/exp/mj
or/ 3‐10
2 and 11
‘suicide risk’
‘suicide warning signs’
‘suicide prevention’
‘suicide news’
‘suicide awareness’
‘suicide survivors’
‘suicide rates’
or/ 13‐19
‘teenage suicide’
‘youth suicide’
‘effects of suicide’
‘firearms for suicide’
or/ 21‐24
‘bereavement group’
‘troubled peers’
or/ 26‐27
‘domestic gas’
‘vehicle exhaust’
or/ 29‐30
‘gun control’
‘firearm training’
‘intervention skills’
or/ 32‐34
1 or 12 or 20 or 25 or 28 or 31 or 35
‘suicide’
gassing
trends
guns
37 and (38 or 39 or 40)
36 or 41
animals/lim
42 and 43
42 not 44
ERIC (CSA Illumina)
KW= suicides
DE=suicide
DE= prevention
DE= public health
DE= health education
DE= education
DE= mental health
3 or 4 or 5 or 6 or 7
2 and 8
KW= “suicide risk”
KW= “suicide prevention”
KW= “suicide news”
KW= “suicide warning signs”
KW= “suicide awareness”
KW= “suicide survivors”
KW= “suicide rates”
10 or 11 or 12 or 13 or 14 or 15 or 16
KW= “teenage suicide”
KW= “youth suicide”
18 or 19
KW= “effects of suicide”
KW= “firearms for suicide”
21 or 22
KW= “bereavement group”
KW= “troubled peers”
24 or 25
KW= “domestic gas”
KW= “vehicle exhaust”
27 or 28
KW= “gun control”
KW= “firearm training”
KW= “intervention skills”
30 or 31 or 32
1 or 9 or 17 or 20 or 23 or 26 or 29 or 33
KW= suicide
KW= gassing
KW= trends
KW= guns
35 and (36 or 37 or 38)
34 or 39
ISI Web of Knowledge: Social Sciences Citation Index (SSCI)
TS= suicides
TS= suicide
TS= risk
TS= prevention
TS= news
TS= awareness
TS= survivors
TS= rates
3 or 4 or 5 or 6 or 7 or 8
2 adj 9
TS= gassing
TS= trends
TS= guns
11 or 12 or 13
2 and 14
TS= “teenage suicide”
TS= “youth suicide”
TS= “effects of suicide”
TS= “firearms for suicide”
16 or 17 or 18 or 19
TS= “bereavement group”
TS= “troubled peers”
21 or 22
TS= “domestic gas”
TS= “vehicle exhaust”
24 or 25
TS= “gun control”
TS= “firearm training”
TS= “intervention skills”
TS= “suicide warning signs”
27 or 28 or 29 or 30
1 or 10 or 15 or 20 or 23 or 26 or 31
Dissertations & Theses (ProQuest)
suicides
“suicide risk”
“suicide warning signs”
“suicide prevention”
“suicide news”
“suicide awareness”
“suicide survivors”
“suicide rates”
2 or 3 or 4 or 5 or 6 or 7 or 8
“teenage suicide”
“youth suicide”
“effects of suicide”
10 or 11 or 12
“bereavement group”
“troubled peers”
14 or 15
“domestic gas”
“vehicle exhaust”
17 or 18
“gun control”
“firearm training”
“intervention skills”
20 or 21 or 22
1 or 9 or 13 or 16 or 19 or 23
suicide
trends
guns
27 and (28 or 29)
24 or 28
NIH RePORTER (National Institutes of Health, US Dept of Health & Human Services)
suicides
“suicide risk”
“suicide warning signs”
“suicide prevention”
“suicide news”
“suicide awareness”
“suicide survivors”
“suicide rates”
2 or 3 or 4 or 5 or 6 or 7 or 8
“teenage suicide”
“youth suicide”
10 or 11
“effects of suicide”
“firearms for suicide”
13 or 14
“bereavement group”
“troubled peers”
16 or 17
“domestic gas”
“vehicle exhaust”
19 or 20
“gun control”
“firearm training”
“intervention skills”
22 or 23 or 24
1 or 9 or 12 or 15 or 18 or 21 or 25
suicide
gassing
trends
guns
27 and (28 or 29 or 30)
26 or 31
SIEC Database (Centre for Suicide Prevention)
College and university students
Educational institutions
Inservice education
Befrienders International
community development
social isolation
social integration
social support
bereavement groups
bereavement programs
Samaritans
Survivor groups
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 in Subject Terms
(book or chapter or government document or information kit or manuscript or newsclipping or pamphlet or proceedings or review or thesis) in Publication Type
13 and 14
CINAHL (EBSCO)
suicides
suicide/ or suicidal ideation/ or suicide, attempted/
“health screening”/
exp *“community mental health services”/
exp*“preventive health care”/
exp *“public health administration”/
exp *“public health”/
exp *education/
3 or 4 or 5 or 6 or 7 or 8
2 and 9
“suicide risk”
“suicide warning signs”
“suicide prevention”
“suicide news”
“suicide awareness”
“suicide survivors”
“suicide rates”
11 or 12 or 13 or 14 or 15 or 16 or 17
“teenage suicide”
“youth suicide”
19 or 20
“effects of suicide”
“firearms for suicide”
22 or 23
“bereavement group”
“troubled peers”
25 or 26
“domestic gas”
“vehicle exhaust”
28 or 29
“gun control”
“firearm training”
“intervention skills”
31 or 32 or 33
1 or 10 or 18 or 21 or 24 or 27 or 30 or 34
suicide
gassing
trends
guns
36 and (37 or 39 or 40)
35 or 40
Data and analyses
Comparison 1. Classroom instruction: knowledge of suicide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Post‐test differences in knowledge of suicide at the end of active intervention | 3 | 312 | Std. Mean Difference (IV, Random, 95% CI) | 1.51 [0.57, 2.45] |
Comparison 2. Classroom instruction: knowledge of suicide prevention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Post‐test differences in knowledge of suicide prevention at the end of active intervention | 3 | 312 | Std. Mean Difference (IV, Random, 95% CI) | 0.72 [0.36, 1.07] |
Comparison 3. Classroom instruction: suicide prevention self‐efficacy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Post‐test differences in suicide prevention self‐efficacy at the end of active intervention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 4. Experimental group comparison for classroom instruction: post‐test differences at the end of active intervention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Abbey 1990, lecture and handouts vs. modeling and role play: post‐test differences in knowledge of suicide at the end of active intervention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Holdwick 2000, motivational‐enhancement suicide prevention program vs. education based‐suicide prevention program: post‐test differences in self‐efficacy at the end of active intervention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 5. Sensitivity analyses for classroom instruction: knowledge of suicide.
Comparison 6. Sensitivity analyses for classroom instruction: knowledge of suicide prevention.
Comparison 7. Sensitivity analysis for classroom instruction: suicide prevention self‐efficacy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis (Holdwick 2000, education‐based suicide prevention program vs. control): post‐test differences in self‐efficacy at the end of active intervention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis (Holdwick 2000, motivational‐enhancement suicide prevention program vs. control): post‐test differences in self‐efficacy at the end of active intervention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 8. Gatekeeper training programs: baseline measures of suicide‐related outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Baseline measures of knowledge of suicide (continuous) | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Baseline measures of knowledge of suicide (dichotomous) | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Baseline measures of knowledge of suicide prevention | 4 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Baseline measures of suicide prevention self‐efficacy | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 Baseline measures of attitudes toward suicide | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Baseline measures of gatekeeper behaviors | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 9. Gatekeeper training programs: post‐test measures of suicide‐related outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Post‐test differences in knowledge of suicide (continuous) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Post‐test differences in knowledge of suicide (dichotomous) | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Post‐test differences in knowledge of suicide prevention | 4 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Post‐test differences in suicide prevention self‐efficacy | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 Post‐test differences in attitudes toward suicide | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Post‐test differences in gatekeeper behaviors | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 10. Experimental group comparisons, gatekeeper training programs: baseline measures of suicide‐related outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Baseline measures of knowledge of suicide (Shipley 2003 ‐ dichotomous) | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Baseline measures of knowledge of suicide prevention (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Baseline measures of suicide prevention self‐efficacy (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Baseline measures of attitudes toward suicide (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 11. Experimental group comparisons, gatekeeper training programs: post‐test of suicide‐related outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Post‐test differences in knowledge of suicide (Shipley 2003) | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Post‐test differences in knowledge of suicide prevention (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Post‐test differences in suicide prevention self‐efficacy (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Post‐test differences in attitudes towards suicide (Shipley 2003) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 12. Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in knowledge of suicide | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in knowledge of suicide | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 13. Sensitivity analysis for gatekeeper training programs: post‐test knowledge of suicide prevention.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in knowledge of suicide prevention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in knowledge of suicide prevention | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 14. Sensitivity analysis for gatekeeper training programs: post‐test suicide prevention self‐efficacy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in suicide prevention self‐efficacy | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis (involuntary participation vs. control): post‐test differences in suicide prevention self‐efficacy | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 15. Sensitivity analysis for gatekeeper training programs: post‐test attitudes towards suicide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis (motivated participation vs. control): post‐test differences in attitudes towards suicide | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis (unmotivated participation vs. control): post‐test differences in attitudes towards suicide | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abbey 1989.
| Methods | RCT, stratified randomization (by gender). | |
| Participants | 73, 18 to 22 year old non‐suicidal undergraduate students who had not received prior crisis intervention, 68% female. Florida State University, USA. | |
| Interventions | Intervention 1: 4 weeks of individual study of suicide intervention handouts and 3 lectures during weeks 2 to 3 related to the handouts, supplemented by question and answer sessions. Intervention 2: 4 weeks of individual study of suicide intervention handouts. Control: Three non‐suicide related lectures during weeks 2 to 3. |
|
| Outcomes | Knowledge of appropriate crisis response (25‐item Suicide Intervention Response Scale (SIRI) (self‐report, scored by number of correct responses)); suicide awareness knowledge (30 multiple‐choice question, self‐report, KOST and 10 question, self‐report Suicide Prevention Questionnaire (SPQ) (11‐point Likert scale, ‐5 "strongly disagree" to +5 "strongly agree"); all 3 outcomes measured week 1 (pre‐test) and week 5 (post‐test). Suicide‐Related Vignette scores (individual score given to each of the five vignettes). Vignettes measured during week 4 and 5. | |
| Notes | Pre‐ and post‐test reliability for the SIRI was 0.68 and 0.76, respectively. Pre‐ and post‐test reliability for the KOST was 0.53 and 0.72, respectively. Pre‐ and post‐test reliability for the SPQ was 0.74 and 0.82, respectively. Percent agreement for suicide‐related vignettes based on pre‐determined scoring criteria between undergraduates and "experts" was 0.89. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random sequence generation was not explained. "Participants were randomly assigned to 1 of 3 treatment conditions, which were controlled for gender: an individual‐study group; a control group; and an individual‐study‐plus‐lecture group." |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Insufficient information. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 73/73 analysed participants provided sufficient data for analyses. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the study author stated that the published reports include all expected outcomes, including pre‐specified outcomes (written communication 26 June 2012). |
| Other bias | Unclear risk | ‐ |
Abbey 1990.
| Methods | RCT, stratified randomization (by gender). | |
| Participants | 90 (87 analysed) non‐suicidal undergraduate students who had not received prior crisis intervention, 61% female, mean age = 21.92 years. Florida State University, USA. | |
| Interventions | Intervention ‐ 1: Modeling and role play, 2 1‐hour and 15 minute sessions during week 2 Intervention ‐ 2: Suicide related lecture and handouts, 2 1‐hour and 15 minute sessions during week 2 Control: Received non‐suicide related coursework to complete on their own during week 2 |
|
| Outcomes | Simulated Suicidal Interactions (SSI), scored 8 (A+) to 1 (C‐), with confederates playing students at the Psychology Clinic who had not yet seen a therapist, 30 multiple‐choice question, self‐report, KOST (see above), Suicide Related Vignette scores (individual score given to each of the five vignettes). KOST measured in Week 3; SSI measured in Week 4, vignettes measured in weeks 3 to 5. | |
| Notes | Agreement for rating Simulated Suicidal Interactions was 92%. Reliability for the KOST was 0.72. Percent agreement for suicide‐related vignettes, based on pre‐determined scoring criteria between two PhD psychologists with expertise in suicide intervention, was 0.83. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random sequence generation was not explained. "Participants were randomly assigned to one of three treatment conditions, controlled for gender." |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Insufficient information regarding blinding of study personnel. "Students were informed that the class would be divided into thirds, with each division receiving the information about issues concerning adolescents. They were admonished to respect the research taking place and not discuss out of class the various issues being presented in their respective groups...students took an 'Interaction Questionnaire' in which they were asked to indicate their perception of purpose of the experiment". Data for two students who correctly determined the purpose of the experiment were excluded from the study. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 87/90 analysed participants provided sufficient data for analyses. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports include all expected outcomes, including those that were pre‐specified (written communication 26 June 2012). |
| Other bias | Unclear risk | ‐ |
Drabek 1991.
| Methods | CBA (clustered by session date). | |
| Participants | 48 (33 analysed) faculty members with full‐time appointments, aged 27 to 66 years. 24 (20 analysed) student‐service personnel, aged 25 to 56 years. University of South Dakota, USA. |
|
| Interventions | Intervention: 90‐minute suicide prevention program with didactic and experiential components (i.e. discussion regarding case scenarios of at‐risk students; 19 faculty and 14 student‐service personnel). Delayed treatment control group: same intervention delayed until after completion of initial post‐tests (14 faculty and 6 student‐service personnel). |
|
| Outcomes | 10‐item (5‐point Likert scale, 1 "strongly agree" to 5 "strongly disagree") SOQ‐AF, 13‐item Recognition of Suicide Lethality Scale (RSL), 33‐item (true/false) Quiz on Knowledge of Suicide (QKS), 18‐item Assessment of Appropriate Responses Scale (AARS). All outcomes measured pre‐intervention and 1 week post‐intervention (or comparable timing for delayed treatment controls). | |
| Notes | Reliability for the SOQ‐AF was 0.79. Cronbach's alpha for the RSL was 0.65. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Not used. |
| Allocation concealment (selection bias) | High risk | Not used. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Insufficient information provided. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 53/72 participants provided sufficient data for analyses; reasons for dropout were not reported. |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information provided. |
| Other bias | High risk | Participants were assigned to a group by the investigators based on the session date that they self‐selected to attend. |
Holdwick 2000.
| Methods | RCT (clustered by session date). | |
| Participants | 168 (152 analysed), 18 to 42 year old undergraduates (mean age = 21.34 years), 63% female. University of Arkansas, USA. | |
| Interventions | Intervention ‐ 1: Education‐based suicide prevention program, didactic seminar based on six components, 1‐hour initial experimental session, followed by a 2‐hour experimental session 1 week later Intervention ‐ 2: Motivational‐enhancement suicide prevention program, didactic seminar based on six components; presented using techniques consistent with motivational interviewing. , 1 hour initial experimental session, followed by a 2‐hour experimental session 1 week later Control: Received no intervention. |
|
| Outcomes | Knowledge of suicide and knowledge of suicide prevention, and likelihood to seek help in times of distress (3 scales from 40‐item modified Attitude Towards SSPQ (m‐SSPQ) (scored 14 to 84 for scale 1; 17 to 102 for scale 2; 3 to 18 for scale 3); knowledge of suicide (28‐item modified‐Suicide Information Test (m‐SIT) (scored 27 to 162), Intention to intervene (4 Suicide Vignette Simulations assessed by Behavioural Interventions Questionnaire (scored 11 to 66)). All outcomes measured pre‐ and immediately post‐intervention (1 week after pre‐test for control group). | |
| Notes | Reliability for the m‐SIT was 0.71. Three subscales of the SSPQ assessed knowledge of suicide, knowledge of suicide prevention, and likelihood to seek help in times of distress; reliability was 0.70, 0.80, and 0.78, respectively. Reliability for the four vignettes ranged from 0.70 to 0.77. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer random number generator, randomized to treatment or control within a given session date (written communication 02 July 2012). |
| Allocation concealment (selection bias) | Unclear risk | Students were enrolled in courses before randomization occurred and the investigators and study personnel were unaware of assignment before study entry (written communication 02 July 2012). |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants and study personnel were blinded to the research hypotheses (written communication 02 July 2012). |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Baseline characteristics were not significantly different between those with and without missing data, 152/168 participants were analysed and appropriate adjusted analyses were conducted (e.g. analysis of covariance). |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports include all expected outcomes, including those that were pre‐specified (written communication 02 July 2012). |
| Other bias | Unclear risk | ‐ |
Joffe 2008.
| Methods | CBA study, before (1980 to 1983) and after (1984 to 1990) intervention. | |
| Participants | 12 universities roughly similar in their Midwestern USA location, size, and educational mission. 345,963 average enrolment years before intervention and 342,963 average enrolment years after intervention. | |
| Interventions | Intervention: Campus policy intervention, in which students who threaten or attempt suicide must attend four sessions of professional assessment. If students failed to complete the four mandated sessions, they would be withdrawn from the post‐secondary institution. Control: 11 Midwestern institutions without the index policy. |
|
| Outcomes | Annual standardized mortality rates for completed suicide (per 100,000 enrolled students per year). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Not used. |
| Allocation concealment (selection bias) | High risk | Not used. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding was not done, but the outcome measurement was not likely to be influenced by lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Standardized mortality rates were used for outcome measures. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports included all expected outcomes, including those that were pre‐specified (written communication, 15 June 2012). |
| Other bias | Unclear risk | Initially, an "invite and encourage" program occurred concurrently with the suicide‐related institutional policy. The program attempted to increase the percent of students meeting with social workers and psychologists following a suicide threat or attempt. It lasted for 3‐months and was deemed ineffective because the number of contacts with social workers and psychologists did not increase. It is unclear how this program influenced the policy intervention as it provided the interventionists with direct contact with suicidal students. The university also self‐selected the intervention to be delivered to their students. |
Pasco 2012.
| Methods | CBA study | |
| Participants | 85 (64 to 65 analysed) peer advisors, mean age of 19 years, 54% female. Syracuse University, USA. | |
| Interventions | Intervention: Campus Connect gatekeeper training program in the standard 3‐hour format including didactic informational presentations, experiential exercises and role playing. Delayed treatment control group: Campus Connect program using a modified 1.5‐hour format with didactic information presentations only, and delayed (following post‐tests) experiential and role playing exercises. |
|
| Outcomes | Knowledge of appropriate crisis response (25‐item, 7‐point Likert scale, ‐3 "highly inappropriate" to +3 "highly appropriate"), self‐report, Suicide Intervention Response Scale ‐ 2 (SIRI‐2); self‐efficacy for suicide‐ and crisis‐related knowledge and skills (14‐item, 10‐point scale, 1 = "not at all true" to 10 = "very true"), self‐report, SITA. Outcomes measured pre‐intervention and immediately post‐intervention. | |
| Notes | The SITA questionnaire was generated by the investigators of the study to measure self‐efficacy among participants. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Not used. |
| Allocation concealment (selection bias) | High risk | Not used. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants were blind to the research hypotheses, but study personnel were not (written communication, 19 June 2012). |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 65/85 participants provided sufficient data for analyses; reason for dropout were not reported. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports include all expected outcomes, including those that were pre‐specified (written communication, 18 June 2012). |
| Other bias | Unclear risk | ‐ |
Shipley 2003.
| Methods | CBA study | |
| Participants | 138 participants (85 gatekeeper participants; mean age 23.65 years (range 18 to 52 years), 42% female; and 53 control participants, mean age 21.34 (range 18 to 52 years), 68% female). University of Canberra. Australia. Gatekeeper participants were all education or nursing students participating in tutorial classes; control participants were recruited from introductory psychology classes. | |
| Interventions | Intervention: 2 to 3 hour gatekeeper workshop, based on the Question, Persuade, and Refer program, with experiential and educational components Control: Received no treatment |
|
| Outcomes | 10‐item Self‐efficacy Scale (4‐point Likert scale, 1 "not at all true" to 4 "exactly true"), 4‐item Mental Health Literacy Scale (7‐point Likert scale, 1 "very unlikely/strongly disagree" to 7 "very likely/strongly agree"), 1‐item Knowledge of Suicide Scale (correct/incorrect), 8‐item Attitude Scale (7‐point Likert scale, varying responses from negative to positive), 5‐item Perceived Behavioural Control Scale (7‐point scale, 1 "strongly disagree/very difficult/no control" to 7 "strongly agree/very easy/complete control"), 6‐item Behavioural Intention Scale (7‐point Likert scale, 1 "strongly disagree/very unlikely" to "strongly agree/very likely"). Outcomes measured pre‐intervention and immediately post‐intervention, or 2 hours after pre‐test for control group. | |
| Notes | Cronbach's alpha for the self‐efficacy scale was 0.83 (pre‐test) and 0.88 (post‐test); mental health literacy was 0.58 (pre‐test) and 0.78 (post‐test); attitude scale was 0.88 (pre‐test) and 0.94 (post‐test); Perceived Behavioural Control Scale was 0.72 (pre‐test) and 0.79 (post‐test); and Behavioural Intentions Scale was 0.94 (pre‐test) and 0.96 (post‐test). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Not used. |
| Allocation concealment (selection bias) | High risk | Not used. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Investigators did not use (written communication, 31 July 2012). |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Missing outcome data balanced in numbers across intervention groups, but reasons for missing data are not reported. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports include all expected outcomes, including those that were pre‐specified (written communication, 31 July 2012). |
| Other bias | Unclear risk | Different sources of participants were used for control vs. intervention groups (different baseline characteristics ‐ age, gender, ethnicity), but outcomes at baseline did not differ. |
Tompkins 2009.
| Methods | CBA study, clustered by post‐secondary institution. University administrators self‐selected whether school peer advisors would receive intervention, waitlist, or no intervention. | |
| Participants | 240; 146 peer advisors (4 to 6 month follow‐up) from six private institutions located in rural and urban areas of the Pacific Northwest USA; 83% Caucasian, 59% female, mean age of 20 years. | |
| Interventions | Intervention: 1‐hour Question, Persuade, and Refer gatekeeper training administered by a certified Question, Persuade, and Refer trainer. Waitlist Control: Question, Persuade, and Refer gatekeeper training provided after follow‐up assessment. Control: Received no treatment. |
|
| Outcomes | 14‐item Question, Persuade, and Refer quiz assessing knowledge, efficacy, and self‐reported gatekeeper behaviors. Outcome measure administered immediately pre‐ and post‐intervention and 4 to 6 months for intervention group and at baseline and 4 to 6 months for control participants. | |
| Notes | Pre‐ and post‐tests were administered at different times to intervention and control groups. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Not used. |
| Allocation concealment (selection bias) | High risk | Not used. Administrators at two schools self‐selected their peer advisors to receive training, three chose to serve as control groups and one school chose to be a waitlist control group. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Investigators did not use (written communication, 18 June 2012). |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were self‐reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 146/240 peer advisors provided sufficient data for analyses at 4 to 6 months. There was differential attrition between the groups at 4 to 6 months follow‐up. Among the intervention group participants, those with greater pre‐test knowledge were more likely to drop out. |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but the author states that the published reports include all expected outcomes, including those that were pre‐specified (written communication, 18 June 2012) |
| Other bias | High risk | Baseline characteristics were compared and demographics were similar between groups, but knowledge of resources was significantly greater among control compared to the intervention group. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Balk 1993 | Principal investigator stated that the intervention was not intended to prevent suicide (Written communication, 05/29/2012). |
| Buelow 2001 | Did not implement an eligible study design. |
| Knox 2003 | Intervention was not implemented within the post‐secondary educational setting to subjects that attended or were employed by the institution. |
| Manning 2011 | Did not implement an eligible study design. |
| Richards 2008 | Did not implement an eligible study design. |
| Seguin 1990 | Did not implement an eligible study design. |
| Suldo 2010 | Intervention was not implemented within the post‐secondary educational setting to subjects that attended or were employed by the institution. |
| Sun 2011 | Principal target of the intervention was patients, not post‐secondary students. |
| Tompkins 2010 | Principal target of the intervention was youth, not post‐secondary students. |
| White 1984 | Not a primary prevention intervention. |
Characteristics of studies awaiting assessment [ordered by study ID]
Basilico 2012.
| Methods | RCT |
| Participants | Approximately 2100 students ages 14 to 24 years in seven countries in the European Union |
| Interventions | Intervention 1: interactive website targeted at adolescents and young adults in the age group 14 to 24 years; Intervention 2: a set of published guidelines for media outfits that target young audiences |
| Outcomes | Lifestyles, values and attitudes, psychological well‐being, familiar relationship, and friendship |
| Notes |
Bender 2012.
| Methods | Not yet assessed |
| Participants | Not yet assessed |
| Interventions | Screening program for suicide risk |
| Outcomes | Suicide implicit association task (S‐IAT) to measure iatrogenic effects |
| Notes |
Cascamo 2013.
| Methods | Not yet assessed |
| Participants | Students enrolled in a rural community college in the northwestern United States |
| Interventions | One‐hour presentation of the gatekeeper suicide prevention training program called Question Persuade and Refer |
| Outcomes | The Inventory of Attitudes toward Seeking Mental Health Services (IASMHS) was used to assess willingness to intervene with individuals at risk of suicide and attitudes toward the utilization of mental health services |
| Notes |
Cooper 2011.
| Methods | Not yet assessed |
| Participants | 142 students attending a university in the northeastern United States |
| Interventions | University‐based suicide prevention outreach program |
| Outcomes | Self‐harm, stress, anxiety, depression, alcohol consumption, therapy‐seeking |
| Notes |
Doane 2011.
| Methods | CBA |
| Participants | 167 college students. United States. |
| Interventions | Video‐based cyberbullying prevention program |
| Outcomes | Knowledge about cyberbullying, attitudes towards cyberbullying, reports of cyberbullying behavior, perceptions of others' attitudes towards cyberbullying, perceptions of others' cyberbullying behavior. |
| Notes |
Douglas 2012.
| Methods | Not yet assessed |
| Participants | Counseling students in the United States |
| Interventions | Intervention 1: suicide risk assessment game; Intervention 2: suicide risk assessment game and evaluation‐focused discussion groups |
| Outcomes | Counselor self‐efficacy related to suicide assessment (Counselor Suicide Assessment Survey); counseling skill related to suicide assessment and intervention (SIRI‐2) |
| Notes |
Freeman‐Schulze 2012.
| Methods | Not yet assessed |
| Participants | Students attending a university in the northeastern United States |
| Interventions | Six‐week peer suicide prevention training program, aimed at training to students to identify friends in need and refer them for help |
| Outcomes | Not yet assessed |
| Notes |
Jacobson 2012.
| Methods | RCT |
| Participants | Social work students |
| Interventions | Gatekeeper training program |
| Outcomes | Not yet assessed |
| Notes |
Kim 2011.
| Methods | Controlled clinical trial |
| Participants | 58 college students in Korea |
| Interventions | Weekly program sessions aiming to reduce depression and suicidal ideation |
| Outcomes | Suicidal ideation, depression |
| Notes |
Mallory 2011.
| Methods | Not known |
| Participants | Not known |
| Interventions | Not known |
| Outcomes | Not known |
| Notes | Grant application. Not known if the study was carried out. |
Perryman 2011.
| Methods | Not yet assessed |
| Participants | Undergraduate males with same‐sex preference who are at‐risk for suicide in the United States |
| Interventions | Integrative person‐centered counseling intervention using Rogers' person‐centered approach, bibliotherapy and group discussion activities |
| Outcomes | Not yet assessed |
| Notes |
Peters 2013.
| Methods | CBA |
| Participants | First‐semester university students in three freshman dormitories at a large private university in the United States |
| Interventions | Intervention: on‐line psycho educational prevention program, SocialConnections, which integrates interpersonal skills from cognitive behavioral therapy, dialectical behavior therapy, and interpersonal therapy to target interpersonal challenges. Control: on‐line sleep program |
| Outcomes | Depression, loneliness, empathy, and social skills |
| Notes |
Zisook 2012.
| Methods | Not yet assessed |
| Participants | Not yet assessed |
| Interventions | Not yet assessed |
| Outcomes | Not yet assessed |
| Notes |
Characteristics of ongoing studies [ordered by study ID]
5R01MH083740.
| Trial name or title | Prevention of suicidality in college students: A common core process approach |
| Methods | RCT |
| Participants | 18 to 20 year old first‐year post‐secondary students |
| Interventions | Intervention: Acceptance and Commitment Therapy (ACT) Control: didactic course on adjustment to the psychological challenges of college life |
| Outcomes | Experiential avoidance, psychological, behavioral, health, and academic problems that are known to predict suicidality, and the frequency or severity of suicidality, self‐injury, suicide attempts, ER visits, and other risky behaviors |
| Starting date | 2008 |
| Contact information | |
| Notes | 720 participants are randomly allocated in three annual waves of 240 students each to receive either ACT or control condition |
Differences between protocol and review
We intended to review interventions for the primary prevention of suicide, and to exclude interventions that targeted persons at known risk of suicide. However, no studies implemented primary preventive interventions in isolation. We included studies as long as there was any primary prevention component to the intervention, even if secondary prevention components were also included. Classifications of primary and secondary preventive interventions were in accordance with the definitions from the Suicide Prevention Action Network (SPAN 2001). In the Cochrane Protocol (Harrod 2011), the statistical model approach for meta‐analysis was unspecified. We chose to use a random‐effects model for relevant analyses because we determined that the studies were drawn from populations that varied from each other in ways that could impact treatment effect. We intended to conduct meta‐analyses of CBA data, but due to concerns about high risk of bias and low quality of evidence, we instead chose to report individual study SMDs and summarize these results narratively. We planned subgroup analysis to explore heterogeneity on a range of sociodemographic, institutional, and methodological characteristics but were unable to do so due to lack of data for some characteristics and lack of heterogeneity for others. We conducted a post‐hoc sensitivity test of statistical heterogeneity based on study instruments, which we had not included in our protocol. Although we did not include details in our protocol about how we would assign ratings for the quality of the body of evidence for a given outcome, our approach, which used standard methods from the Cochrane Handbook and McMaster GRADE learning modules, was decided before ratings were assigned to outcomes and the methodology was detailed in the review.
Contributions of authors
CD, CG, and LS conceived the study. CH, CG, and CD designed the protocol. CH drafted the protocol and all authors critically reviewed and revised the protocol for important intellectual content. CH designed a hierarchy selection for multiple outcomes and CD and CG reviewed and revised the criteria. CH and CG screened titles and abstracts and extracted data from eligible studies, and CD resolved disputes. CD, CG, and CH all contributed to the generation of an outcome categorization scheme. CH entered data for analytic purposes and CG reviewed and revised them. CH and CD developed the analysis plan. CH conducted the analyses and CG and CD reviewed and revised them. CH and CG rated risk of bias criteria and quality of evidence using the GRADE approach and CD resolved disputes. CH drafted the review and all review authors critically evaluated and revised the review for important intellectual content.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Centers for Disease Control and Prevention (CDC), US Department of Health and Human Services (DHHS), USA.
This review was supported by Colorado Injury Control Research Center Grant Number R49/CCR811509 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the review authors and do not necessarily represent the official views of the CDC.
Declarations of interest
CH: None known.
CG: None known.
LS: None known.
CD: None known.
New
References
References to studies included in this review
Abbey 1989 {published data only}
- Abbey KJ, Madsen CH Jr, Polland R. Short‐term suicide awareness curriculum. Suicide and Life‐Threatening Behavior 1989;19(2):216‐27. [DOI] [PubMed] [Google Scholar]
Abbey 1990 {published data only}
- Abbey KJ. Suicide intervention training: Role playing versus lecture methods for college students [PhD dissertation]. Tallahassee, FL: Florida State University, 1990. [Google Scholar]
Drabek 1991 {published data only}
- Drabek GA. Training gatekeepers: Evaluation of a suicide prevention training program for university faculty and selected staff members [PhD dissertation]. Vermillion, SD: University of South Dakota, 1991. [Google Scholar]
Holdwick 2000 {published data only}
- Holdwick DJ. The effects of two educational interventions on college students' knowledge of suicide and reported intentions to prevent suicide. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000; Vol. 61, issue 3‐B:1‐145.
Joffe 2008 {published data only}
- Joffe P. An empirically supported program to prevent suicide in a college student population. Suicide and Life‐Threatening Behavior 2008;38(1):87‐103. [DOI] [PubMed] [Google Scholar]
Pasco 2012 {published data only}
- Pasco S, Wallack C, Sartin RM, Dayton R. The impact of experiential exercises on communication and relational skills in a suicide prevention gatekeeper‐training program for college resident advisors. Journal of American College Health 2012;60(2):134‐40. [DOI] [PubMed] [Google Scholar]
Shipley 2003 {published data only}
- Shipley M. Suicide intervention training and education in a university setting: Effects of training intensity and voluntary motivation [Master thesis]. Bruce, ACT ‐ Australia: University of Canberra, 2003. [Google Scholar]
Tompkins 2009 {published data only}
- Tompkins TL. The short‐term effectiveness of a suicide prevention gatekeeper training program in a college setting with residence life advisers. Journal of Primary Prevention 2009;30(2):131‐49. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Balk 1993 {published data only}
- Balk DE, Tyson‐Rawson K, Colletti‐Wetzel J. Social support as an intervention with bereaved college students. Death Studies 1993;17(5):427‐50. [Google Scholar]
Buelow 2001 {published data only}
- Buelow G, Range LM. No‐suicide contracts among college students. Death Studies 2001;25(7):583‐92. [DOI] [PubMed] [Google Scholar]
Knox 2003 {published data only}
- Knox KL, Litts DA, Talcott GW, Feig JC, Caine ED. Risk of suicide and related adverse outcomes after exposure to a suicide prevention programme in the US Air Force: cohort study. British Medical Journal 2003;327(7428):1376. [DOI] [PMC free article] [PubMed] [Google Scholar]
Manning 2011 {published data only}
- Manning J, Vandeusen K. Suicide prevention in the dot com era: Technological aspects of a university suicide prevention program. Journal of American College Health 2011;59(5):431‐3. [DOI] [PubMed] [Google Scholar]
Richards 2008 {published data only}
- Richards D, Tangney B. An informal online learning community for student mental health at university: a preliminary investigation. British Journal of Guidance & Counselling 2008;36(1):81‐97. [Google Scholar]
Seguin 1990 {published data only}
- Seguin MR, Sylvaine G, Francois VT. Suicide prevention in a college setting: Is it possible?. Psychologie Medicale 1990;22(5):381‐3. [Google Scholar]
Suldo 2010 {published data only}
- Suldo S, Loker T, Friedrich A, Sundman A, Cunningham J, Saari B, et al. Improving school psychologists' knowledge and confidence pertinent to suicide prevention through professional development. Journal of Applied School Psychology 2010;26(3):177‐97. [Google Scholar]
Sun 2011 {published data only}
- Sun F‐K, Long A, Huang X‐Y, Chiang C‐Y. A quasi‐experimental investigation into the efficacy of a suicide education programme for second‐year student nurses in Taiwan. Journal of Clinical Nursing 2011;20(5‐6):837‐46. [DOI] [PubMed] [Google Scholar]
Tompkins 2010 {published data only}
- Tompkins TL, Witt J. The short‐term effectiveness of a suicide prevention gatekeeper training program in a college setting with residence life advisers. Journal of Primary Prevention 2009;30(2):131‐49. [DOI] [PubMed] [Google Scholar]
White 1984 {published data only}
- White WC, Rubenstein AS. Crisis intervention on campus. Crisis Intervention 1984;12(2):42‐54. [Google Scholar]
References to studies awaiting assessment
Basilico 2012 {published data only}
- Basilico F, Carli V, Iosue M, D'Aulerio M, Domenico A, Recchia L, et al. Internet and the media for the prevention of suicide among European youngs. European Psychiatry 2012;27(Suppl 1):P‐1410. [Google Scholar]
Bender 2012 {published data only}
- Bender TW. Screening for suicide in an adult population: An analysis of iatrogenic risk [PhD dissertation]. Tallahassee, FL: Florida State University, 2012. [Google Scholar]
Cascamo 2013 {published data only}
- Cascamo JA. Gatekeeper suicide prevention training and its impact on attitudes toward help seeking [PhD dissertation]. Minneapolis, MN: Walden University, 2013. [Google Scholar]
Cooper 2011 {published data only}
- Cooper TM. Effectiveness of an internet‐based mental health outreach program in encouraging use of mental health services by traditional and nontraditional college students [PhD dissertation]. Newton, MA: Massachusetts School of Professional Psychology, 2011. [Google Scholar]
Doane 2011 {published data only}
- Doane AN. Testing of a brief Internet cyberbullying prevention program in college students [PhD dissertation]. Norfolk, VA: Old Dominion University, 2011. [Google Scholar]
Douglas 2012 {published data only}
- Douglas KA. Enhancing learning outcomes through evaluation of serious gaming: A mixed methods study [PhD dissertation]. West Lafayette, IN: Purdue University, 2012. [Google Scholar]
Freeman‐Schulze 2012 {published data only}
- Freeman‐Schulze R. Suicide prevention on a college campus: An in‐depth look at the students' experiences in a peer education program [PhD dissertation]. Boston, MA: Boston University, 2012. [Google Scholar]
Jacobson 2012 {published data only}
- Jacobson JM, Osteen PJ, Sharpe TL, Pastoor JB. Randomized trial of suicide gatekeeper training for social work students. Research on Social Work Practice 2012;22(3):270‐81. [Google Scholar]
Kim 2011 {published data only}
- Kim GH, Kim K, Park H. Outcomes of a program to reduce depression. Western Journal of Nursing Research 2011;33(4):560‐76. [DOI] [PubMed] [Google Scholar]
Mallory 2011 {published data only}
- Mallory NA. Suicide prevention assessment for community college students: A grant proposal [PhD dissertation]. Long Beach, CA: California State University, Long Beach, 2011. [Google Scholar]
Perryman 2011 {published data only}
- Perryman JC. Gay university undergraduate males at risk for suicide: An integrative person‐centered bibliotherapy approach to prevention [PhD dissertation]. Moraga, CA: Saint Mary's College of California, 2011. [Google Scholar]
Peters 2013 {published data only}
- Peters HO. Social connections: Internet prevention of loneliness and depression in first year university students [PhD dissertation]. Palo Alto, CA: Palo Alto University, 2013. [Google Scholar]
Zisook 2012 {published data only}
- Zisook S, Downs N, Moutier C, Clayton P. College students and suicide risk: prevention and the role of academic psychiatry. Academic Psychiatry 2012;36(1):1‐6. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
5R01MH083740 {published data only}
- 5R01MH083740. Prevention of suicidality in college students: a common core process approach. projectreporter.nih.gov/project_info_details.cfm?aid=8270526&icde=17545604 (accessed 09 January 2013).
Additional references
Arnett 2000
- Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. American Psychologist 2000;55(5):469‐80. [PubMed] [Google Scholar]
Arria 2009
- Arria AM, O'Grady KE, Caldeira KM, Vincent KB, Wilcox HC, Wish ED. Suicide ideation among college students: A multivariate analysis. Archives Suicide Research 2009;13(3):230‐46. [DOI] [PMC free article] [PubMed] [Google Scholar]
Barrios 2000
- Barrios LC, Everett SA, Simon TR, Brener ND. Suicide ideation among US college students. Associations with other injury risk behaviours. Journal of American College Health 2000;48(5):229‐33. [DOI] [PubMed] [Google Scholar]
Bernard 1982
- Bernard JL, Bernard ML. Factors related to suicidal behavior among college students and the impact of institutional response. Journal of College Student Personnel 1982;23:409‐13. [Google Scholar]
Bertolote 2004
- Bertolote JM. Suicide prevention: at what level does it work?. World Psychiatry 2004;3(3):147‐51. [PMC free article] [PubMed] [Google Scholar]
Borenstein 2009
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta‐Analysis. 1st Edition. Chichester: Wiley, 2009. [Google Scholar]
CDC 1994
- Centers for Disease Control and Prevention. Programs for the prevention of suicide among adolescents and young adults; and suicide contagion and the reporting of suicide: Recommendations from a national workshop. Morbidity and Mortality Weekly Report 1994;43(6):1‐18. [PubMed] [Google Scholar]
CDC 2003
- Centers for Disease Control and Prevention. First reports evaluating the effectiveness of strategies for preventing violence: early childhood home visitation and firearms laws: findings from the Task Force on Community Preventive Services. MMWR 2003;52(No. RR‐14):11‐19. [PubMed] [Google Scholar]
Cohen 1988
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd Edition. Hillsdale, NJ: Lawrence Erlbaum Associates, 1988. [Google Scholar]
Conn 2003
- Conn V, Valentine J, Cooper H, Rantz M. Grey literature in meta‐analyses. Nursing Research 2003;52(4):256‐61. [DOI] [PubMed] [Google Scholar]
Cox 2013
- Cox GR, Owens C, Robinson J, Nicholas A, Lockley A, Williamson M, et al. Interventions to reduce suicides at suicide hotspots: a systematic review. BMC Public Health 2013;13(214):1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Crawford 2007
- Crawford MJ, Thomas O, Khan N, Kulinskaya E. Psychosocial interventions following self‐harm: systematic review of their efficacy in preventing suicide. British Journal of Psychiatry 2007;190:11‐17. [DOI] [PubMed] [Google Scholar]
Crowley 2004
- Crowley P, Kilroe J, Burke S. Youth suicide prevention: Evidence briefing. http://www.nice.org.uk/niceMedia/documents/suicidePO.pdf 2004.
Dickersin 1992
- Dickersin K, Berlin JA. Meta‐analysis: State‐of‐the‐science. Epidemiologic Reviews 1992;14:154‐76. [DOI] [PubMed] [Google Scholar]
Eisenberg 2012
- Eisenberg D, Hunt J, Speer N. Help seeking for mental health on college campuses: review of evidence and next steps for research and practice. Harvard Review of Psychiatry 2012;20(4):222‐32. [DOI] [PubMed] [Google Scholar]
EPOC 2009
- Cochrane Effective Practice and Organisation of Care (EPOC) Review Group. 'Risk of Bias' guidelines. https://epoc.cochrane.org/sites/epoc.cochrane.org/files/uploads/Suggested%20risk%20of%20bias%20criteria%20for%20EPOC%20reviews.pdf (accessed 15 October 2014).
Faraone 2008
- Faraone SV. Interpreting estimates of treatment effects: implications for managed care. Pharmacy and Therapeutics 2008;33(12):700‐11. [PMC free article] [PubMed] [Google Scholar]
Gallagher 2009
- Gallagher RP. National Survey of Counseling Center Directors. Arlington, VA: International Association of Counseling Services, 2009. [Google Scholar]
Gochman 1997
- Gochman DS. Handbook of Health Behavior Research I: Personal and Social Determinants. 1st Edition. New York: Springer, 1997. [Google Scholar]
Goss 2007
- Goss C, Lowenstein S, Roberts I, DiGuiseppi C. Identifying controlled studies of alcohol‐impaired driving prevention: designing an effective search strategy. Journal of Information Science 2007;33(2):151‐62. [Google Scholar]
Gould 2009
- Gould M, Klomek AB, Batejan K. The role of schools, colleges and universities in suicide prevention. In: Wasserman D, Wasserman C editor(s). Oxford Textbook of Suicidology and Suicide Prevention: a global perspective. Oxford: Oxford University Press, 2009:551‐62. [Google Scholar]
Guo 2002
- Guo B, Harstall C. Efficacy of Suicide Prevention Programs for Children and Youth. http://www.ihe.ca/documents/suicide_prevention.pdf (accessed 05 August 2013).
Guo 2003
- Guo B, Scott A, Bowker S. Suicide prevention strategies: Evidence from systematic reviews. http://www.ihe.ca/documents/suicide_prevention_strategies_evidence.pdf (accessed on 01 September 2010).
Hall 2002
- Hall K, Day P. Suicide prevention topic 1: What kind of follow‐up is needed to reduce the risk of repeated suicide attempts/suicide?. http://nzhta.chmeds.ac.nz/publications/topic1.pdf (accessed on 01 September 2010).
Harden 2001
Harris 2009
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic Data Capture (REDCap) ‐ A metadata‐driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics 2009;42(2):377‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Harrod 2011
- Harrod CS, Goss CW, Stallones L, Gliner JA, DiGuiseppi C. Interventions for primary prevention of suicide in the post‐secondary educational setting. Cochrane Database of Systematic Reviews 2011, Issue 11. [DOI: 10.1002/14651858.CD009439] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hawton 1999
- Hawton KKE, Townsend E, Arensman E, Gunnell D, Hazell P, House A, et al. Psychosocial and pharmacological treatments for deliberate self harm. Cochrane Database of Systematic Reviews 1999, Issue 4. [DOI: 10.1002/14651858.CD001764] [DOI] [PMC free article] [PubMed] [Google Scholar]
Haynie 2013
- Haynie D. 10 national universities where most students live on campus. http://www.usnews.com/education/best‐colleges/the‐short‐list‐college/articles/2013/06/18/10‐national‐universities‐where‐most‐students‐live‐on‐campus (accessed 18 June 2013).
Hepp 2004
- Hepp, U, Wittmann L, Schnyder U, Michel K. Psychological and psychosocial interventions after attempted suicide. Crisis 2004;25(3):108‐17. [DOI] [PubMed] [Google Scholar]
Hider 1998
- Hider P. Youth suicide prevention by primary healthcare professionals: A critical appraisal of the literature. New Zealand Health Technology Assessment 1998; Vol. Report 4:1‐115.
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. British Medical Journal 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2008
- Higgins JPT, Green S (editors). The Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Isaac 2009
- Isaac M, Elias B, Katz LY, Belik SL, Deane FP, Enns MW, et al. Gatekeeper training as a preventative intervention for suicide: a systematic review. Canadian Journal of Psychiatry 2009;54(4):260‐8. [DOI] [PubMed] [Google Scholar]
Jacobson 2011
- Jacobson CM, Marrocco F, Kleinman M, Gould MS. Restrictive emotionality, depressive symptoms, and suicidal thoughts and behaviors among high school students. Journal of Youth and Adolescence 2011;40(6):656‐65. [DOI] [PubMed] [Google Scholar]
Katz 2013
- Katz C, Bolton SL, Katz LY, Isaak C, Tilston‐Jones T, Sareen J, et al. A systematic review of school‐based suicide prevention programs. Depression and Anxiety 2013;30(10):1030‐45. [DOI] [PubMed] [Google Scholar]
Linehan 1997
- Linehan MM. Behavioral treatments of suicidal behaviours: Definitional obfuscation and treatment outcomes. Annals of the New York Academy of Sciences 1997;836:302‐28. [DOI] [PubMed] [Google Scholar]
Liu 2013
- Liu RT, Kraines MA, Puzia ME, Massing‐Schaffer M, Kleiman EM. Sociodemographic predictors of suicide means in a population‐based surveillance system: findings from the National Violent Death Reporting System. Journal of Affective Disorders 2013;151(2):449‐54. [DOI] [PubMed] [Google Scholar]
Lloyd‐Richardson 2007
- Lloyd‐Richardson EE, Perrine N, Dierker L, Kelley ML. Characteristics and functions of non‐suicidal self‐injury in a community sample of adolescents. Psychological Medicine 2007;37(8):1183‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mann 2005
- Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, et al. Suicide prevention strategies: a systematic review. JAMA 2005;294(16):2064‐74. [DOI] [PubMed] [Google Scholar]
Miller 2009
- Miller DN, Eckert TL, Mazza JJ. Suicide prevention programs in the schools: a review and public health perspective. School Psychology Review 2009;38(2):168‐88. [Google Scholar]
Niemi 1993
- Niemi T, Lönnqvist J. Suicides among university students in Finland. Journal of American College Health 1993;42(2):64‐6. [DOI] [PubMed] [Google Scholar]
O'Connor 2013
- O'Connor E, Gaynes BN, Burda BU, Soh C, Whitlock EP. Screening for and treatment of suicide risk relevant to primary care: a systematic review for the U.S. Preventive Services Task Force. Annals of Internal Medicine 2013;158(10):741‐54. [DOI] [PubMed] [Google Scholar]
Oyama 2008
- Oyama H, Sakashita T, Ono Y, Goto M, Fujita M, Koida J. Effect of community‐based intervention using depression screening on elderly suicide risk: a meta‐analysis of the evidence from Japan. Community Mental Health Journal 2008;44(5):311‐20. [DOI] [PubMed] [Google Scholar]
Ploeg 1999
- Ploeg J, Ciliska D, Brunton G, MacDonnell J, O'Brien MA. The effectiveness of school‐based curriculum suicide prevention programs for adolescents. http://www.ephpp.ca/PDF/1999_Adolescent%20Suicide%20Prevention.pdf (accessed on 01 September 2010).
Review Manager [Computer program]
- The Nordic Cochrane Centre. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, 2008.
Schotte 1982
- Schotte DE, Clum GA. Suicide ideation in a college population: A test of a model. Journal of Consulting and Clinical Psychology 1982;50(5):690‐6. [DOI] [PubMed] [Google Scholar]
Schwartz 1990
- Schwartz AJ, Whitaker LC. Suicide among college students: Assessment, treatment, and intervention. In: Blumenthal SJ, Kupfer DJ editor(s). Suicide Over the Life Cycle: Risk Factors, Assessment, and Treatment of Suicidal Patients. Washington, DC: American Psychiatric Press Inc, 1990:303‐40. [Google Scholar]
Schwartz 2006
- Schwartz AJ. College student suicide in the United States: 1990‐1991 through 2003‐2004. Journal of American College Health 2006;54(6):341‐52. [DOI] [PubMed] [Google Scholar]
Schweitzer 1995
- Schweitzer R, Klayich M, McLean J. Suicidal ideation and behaviours among university students in Australia. Australian and New Zealand Journal of Psychiatry 1995;29(3):473‐9. [DOI] [PubMed] [Google Scholar]
Sher 2001
- Sher L, Oquendo MA, Mann JJ. Risk of suicide in mood disorders. Clinical Neuroscience Research 2001;1:337‐44. [Google Scholar]
SPAN 2001
- SPAN USA, Inc. Suicide prevention: Prevention effectiveness and evaluation. http://www.sprc.org/sites/sprc.org/files/library/prevtoolkit.pdf (accessed 06 May 2013).
Sushil 2010
- Sushil S, Verma N. Questionnaire validation made easy. European Journal of Scientific Research 2010;46(2):172‐8. [Google Scholar]
Sánchez‐Meca 2003
- Sánchez‐Meca J, Marín‐Martínez F, Chacón‐Moscoso S. Effect‐size indices for dichotomized outcomes in meta‐analysis. Psychological Methods 2003;8(4):448‐67. [DOI] [PubMed] [Google Scholar]
Tarrier 2008
- Tarrier N, Taylor K, Gooding P. Cognitive‐behavioral interventions to reduce suicide behaviour: a systematic review and meta‐analysis. Behavior Modification 2008;32(1):77‐108. [DOI] [PubMed] [Google Scholar]
Universities UK 2002
- Universities UK. Reducing the risk of student suicide: Issues and responses for higher education institutions. http://www.healthyuniversities.ac.uk/uploads/files/uuk_scop_report__reducing_risk_of_student_suicide.pdf 2002.
van der Sande 1997
- Sande R, Buskens E, Allart E, Graaf Y, Engeland H. Psychosocial intervention following suicide attempt: a systematic review of treatment interventions. Acta Psychiatrica Scandinavica 1997;96(1):43‐50. [DOI] [PubMed] [Google Scholar]
Verger 2010
- Verger P, Guagliardo V, Gilbert F, Rouillon F, Kovess‐Masfety V. Psychiatric disorders in students in six French universities:12‐month prevalence, comorbidity, impairment and help‐seeking. Social Psychiatry and Psychiatric Epidemiology 2010;45(2):189‐99. [DOI] [PubMed] [Google Scholar]
Wasserman 2010
- Wasserman D, Wasserman C. The Oxford Textbook of Suicidology and Suicide Prevention: A Global Perspective. 1st Edition. Oxford: Oxford University Press, 2010:109‐10. [Google Scholar]
Xiangmin 2009
- Xiangmin DU, Hongyun S. Research on the reason of college students committing suicide based on the impact of Chinese culture. International Conference on Education Management and Engineering. 2009:781‐7.