

Abstract
Epidemiological studies suggest that 10–15% adults meet the present criteria for the diagnosis of insomnia disorder; however, there may be geographical variations. Untreated insomnia disorders have a number of adverse health consequences in addition to economic burden caused by it. Available guidelines mention that CBT-I should be preferred over hypnotics. However, several patients of chronic insomnia are not candidate for CBT-I and for them, hypnotics are the only answer. This paper reviews the literature to answer following questions: What is the current understanding regarding place of hypnotics for in management of insomnia disorder? How many patients misuse or abuse hypnotics, especially benzodiazepines, as commonly believed? Do we have data from human studies regarding low-dose benzodiazepine dependence? What does hypnotics produce—withdrawal insomnia, rebound insomnia or end of dose phenomenon? Are adverse effects of benzodiazepines worse than other psychotropic medications? Is prescription of hypnotics more troublesome than untreated insomnia disorder? Available literature suggests that there is an unreasonable negative bias attached to the use of hypnotics. Only a sub-set of patients who are prescribed hypnotics, meet the criteria for “dependence” in long term. Other patients either discontinue it (as insomnia remits) or change to occasional use (since insomnia may be relapsing remitting disorder), or continue using it in low dose (since insomnia reappears as hypnotics are discontinued, similar to increase in blood sugar after hypoglycemics are discontinued). Meta-analysis shows that adverse effects of hypnotics are comparable to that of other psychotropic medications. Considering the consequences and risks associated with untreated insomnia disorder, even long-term use of hypnotics is justified, however with the careful watch that patients are not increasing the dose. This approach is especially important in geographical areas where trained CBT-I therapists are not available.
Keywords: Chronic insomnia, Hypnotics, Long-term use, Dependence
Introduction
Insomnia disorder or chronic insomnia is one of the highly prevalent sleep disorders with significant morbidity. Treatment of insomnia has been one of the highly debated topics, since treatment outcome is often sub-optimal, from the perspectives of the treating doctor as well as that of the patient [39]. Several guidelines are available for the management of acute and chronic insomnia among adult patients mentioning different therapeutic approaches [4, 40, 42, 47, 50]. Recommendations are also available that addressing the management of insomnia disorder in specific age groups, i.e., children and elderly [6, 30]. These documents mention two different approaches for the management of insomnia- pharmacological and non-pharmacological. Non-pharmacological management of insomnia includes use of multi-model cognitive behaviour therapy for insomnia (CBT-I, while a number of pharmacological agents are also mentioned [4, 40, 42, 50]. During past 20 years, a significant advancement has been achieved in pharmacological approaches to manage insomnia disorder [47]. As of today, myriad medications are available for management of insomnia disorder that are categorized to different classes based upon their pharmacodynamic properties, e.g., benzodiazepines, non-benzodiazepine hypnotics, anti-histamines, sedating antidepressants, sedating antipsychotics and dual orexin receptor antagonists [47], Asnis et al. 2010).
Most of the guidelines mentioned above advocate that CBT-I should be the preferred method for addressing insomnia, while pharmacotherapy may be used for short-term treatment only, i.e., 4–8 weeks, that too, when CBT-I is not available. Arguments mentioned to avoid pharmacotherapy for insomnia including development of tolerance, dependence, and other adverse effects that may occur with hypnotics—benzodiazepines (BZD) and benzodiazepine receptor antagonists (BZRA) [42, 50]. Term “hypnotics” will be used to denote these classes of medications in present paper.
The current paper was conceptualized because of the apparent reluctance of physicians in prescribing hypnotics. Common apprehensions against the use of hypnotics are abuse potential, fear of inducing dependence and facing disapproval by the peers. In this paper, we intend to review issues viz., efficacy, cost, adherence, adverse effects especially abuse and dependence related to hypnotics when they are used for management of insomnia disorder.
Search strategy and selection criteria
This is a narrative review regarding use of hypnotics for the management of insomnia disorder. Hence, narrative reviews, systematic reviews, meta-analysis and guidelines were searched using terms “chronic insomnia”, “cognitive behavior therapy for insomnia”, “hypnotics”, “pharmacotherapy” in PubMed and Google scholar. However, for some specific sections (e.g., low-dose hypnotic dependence), systematic reviews and meta-analysis were not available. For these sections, individual papers were searched with an attempt of include latest available evidence.
Hypnotics: Why to avoid?:
With the above-mentioned background, following sections will try to find out why hypnotics remain under-used in the management of insomnia disorder.
Definitions
To understand the intricacies of the enigma of hypnotics, familiarization with the common diagnostic entities used in contemporary classificatory systems and the issues arising from them is essential.
Abuse, misuse as well as dependence, all three terms have often been used interchangeably in relation to hypnotics. According to standard definition, dependence is characterized by three pharmacological properties—tolerance, withdrawal, and craving [1]. On the other hand, misuse pertains to the use of medication for therapeutic purpose which is not conforming to the medical or legal guidelines. Lastly, abuse refers to use of hypnotics for non-therapeutic purpose, primarily for the recreation [54, 69]. Thus, misuse may clinically present as long-term use of medication than intended but to achieve therapeutic effect, but is not synonymous with abuse and dependence.
Abuse
Laboratory as well as epidemiological evidence suggest that benzodiazepines have relatively lower abuse potential. Similar to anxiety disorder, subjects with insomnia symptoms and healthy controls do not prefer hypnotics over placebo [45]. Reinforcement is important for continuation of substance for recreational purpose. However, reinforcing effects have been found only among patients having anxiety, insomnia and moderate alcohol consumption, especially among poly substance users [16]. Whether the reinforcement was obtained from the relief of symptoms or the recreation could not be addressed in this paper. A systematic review reported that frequency of hypnotic “misuse” (where “misuse” denotes both abuse as well as misuse corroding to definitions used in this paper) was found to vary between five occasions in past year to 1–2 days in a month [66]. Most of the times, hypnotics were consumed for relieving anxiety and sleeplessness [66]. Hypnotics, for the recreational purpose, were almost always used by persons consuming other substances—particularly opioids [66]. Recent data regarding hypnotics suggest that 1 year prevalence of hypnotic abuse is just 1.2% and only 0.24% patients abused both BZDs and BZRAs [22]. Abuse of hypnotics was related to illicit use of other drugs such as opioids and stimulants [22]. Interestingly, such low prevalence was observed even though, in this population-based study, subjects were prescribed hypnotics for a variety of reasons, including psychiatric disorders [22]. Taken together, available evidence suggest that contrary to common belief, even in at-risk population, only a small number use hypnotics for recreational purpose. Moreover, most of the data regarding abuse potential of hypnotics emerges from case reports and animal studies.
Misuse/long-term use
Data regarding misuse of hypnotics is also available. Approximately, 14% subjects diagnosed as having insomnia disorder continue to use hypnotics even after 1 year, which was associated with hyperarousal that manifested as anxiety and daytime sleeplessness [38]. Takaesu et al. [59] reported that nearly half of the subjects with insomnia disorder needed hypnotics by 6 months which was related to higher scores (> 13.5) on Pittsburg Sleep Quality Index. However, in these subjects, hypnotics were required to relive symptoms, not for the recreational purpose.
Misuse of hypnotics is also common among subjects with other psychiatric disorders, not only insomnia. A long-term study assessed hypnotic use in a population consisting of patients with a variety of psychiatric disorders reported that nearly 70% subjects use hypnotics sparingly (< 30 defined daily doses/year) and only 20% require it for long term (> 180 defined daily dose/year) [49]. A recent study followed 3981 subjects for 1 year after their first prescription of hypnotics. This study reported that 70% subjects discontinued hypnotics after 3 months and only 10% continued hypnotics for 1 year which was related to concomitant antidepressant therapy and older age, factors that increase likelihood of disturbed sleep [11]. Most common pattern seen in long-term hypnotic use was “low and stable doses taken either occasionally or daily for years” while dose escalation was seen in merely 1–2% of subjects [27].
These evidence suggest that long-term use of hypnotics among subjects with insomnia disorder is likely to be related to underlying pathophysiology rather than craving. Moreover, it supports the fact that hypnotics were continued for obtaining therapeutic benefit, similar to long-term therapy with anti-hypertensive and hypoglycemics. In either case, symptoms of primary disease are likely to recur when medications are discontinued.
Tolerance
Soldatos et al. [55] reviewed the tolerance of hypnotics among patients with insomnia and, reported that tolerance was observed with triazolam but not with midazolam and zolpidem. In this review, tolerance was defined as reduction in total sleep time and increase in sleep onset latency. It was reported that with intermediate and long-term use of triazolam, sleep onset latency was increased from baseline for 0.5 min and 5.4 min, respectively, and total sleep time reduced by 19.9 min and 26 min, respectively [55]. However, this was not observed with other hypnotics. Whether change in these values are clinically significant and whether they represent progression of disease (insomnia disorder) are questions that remain to be explored. A systematic review suggested that benzodiazepine doses remain stable over long-term use (6 months to an year), suggesting absence of tolerance in human [27]. An increment of the hypnotic doses (> 720 defined daily doses/year) was observed in merely 0.5% new hypnotic users in a study spanning 10 years [49]. These data show the absence of tolerance with hypnotics. An 8-month-long zolpidem trial also suggests that tolerance to hypnotic action does not develop even after chronic use among subjects having chronic insomnia, as commonly believed [44]. Similar results were shown by Green et al. [15] who reported that most of the patients having insomnia disorder did not increase the dose of hypnotics, however, continued low-dose use in long term. Thus, the scientific literature does not support evidence of tolerance to hypnotics among human subjects.
Withdrawal
One of the important components of dependence is withdrawal symptoms. Data regarding withdrawal symptoms arising from the use of therapeutic doses of hypnotics are insufficient to be considered significant. Most of the studies suggest that persons with insomnia disorder only complain of sleep disturbance when they do not take hypnotics (during withdrawal), rather than a withdrawal “syndrome” having additional symptoms other than insomnia, as seen during alcohol dependence.
“Rebound insomnia’ is different from ‘withdrawal insomnia’ as former denotes worsening of symptoms compared to baseline after discontinuation of hypnotics, while the latter can be understood as occurrence of symptoms due to the absence of pharmacological effect of medication upon discontinuation of medication [23]. Rebound insomnia has been considered as manifestation of withdrawal (though mistakenly) in earlier reports [24]. Data regarding rebound insomnia are inconsistent and even when it occurs, it is usually short-lasting (1–2 nights) [45]. However, Hajak et al. [18] reported that rebound insomnia was observed on hypnotic discontinuation a quarter of subjects having insomnia. However, in this study, rebound was defined as severity of night time and daytime symptoms that was assessed using visual analog scale, hence, influence of stress arising out of “insomnia” cannot be ruled out. Risk of rebound appears to be high with short acting medications like triazolam compared to long-acting medications viz., flunitrazepam, especially among non-responders to treatment [14, 18]. Thus, there is a need to carefully distinguish these entities. Phenomenon similar to “withdrawal insomnia” is routinely observed with other classes of medications, e.g., anti-inflammatory, anti-hypertensive, antipsychotic and antiepileptics, to name a few. Moreover, we could not identify any study citing “withdrawal syndrome” among patients with insomnia disorder, who often use hypnotics in low dose.
Dependence
The concept of benzodiazepine dependence is unique and not just ‘dependence’ which has been modeled upon the Griffith Edwards model of ‘alcohol dependence’ [58]. It has been conceptualized as dependence without tolerance. In this regard, it needs to be understood that long-term usage of benzodiazepines is not synonymous with benzodiazepine dependence. In fact, a kind ‘slow-onset’ long-term benzodiazepine substitution has also been described though clinical evidence is yet to come. The main behavioural correlates are drug seeking behaviour manifested by doctor shopping and obtaining multiple prescriptions [3]. Also, it needs to be understood that benzodiazepines cannot be compared to the classic substances of abuse like cocaine and opioids in the different animal models [26]. When pretreated with alcohol and other substances, the reinforcing properties of benzodiazepines are greater, but not when they are used in isolation. Benzodiazepines do influence the dopamine secretion in the ventral tegmental area as shown in the classic studies by Tan et al. [61].
In this regard, it is important to note that long-term use does not amount to dependence though the risk is more for certain vulnerable groups like older age (> 65 years), prescription by a psychiatrist, regular use, use of a high dose, and concomitant prescription of psychotropic drugs [60].
Low-dose benzodiazepine dependence
Research advocating benzodiazepine usage has collimated with that which cautions against it. The scientific views for long-term low-dose use have been synonymous with the term low-dose dependence [8, 63]. It has been disputed since neuro-adaptive changes were never required nor sufficed for the criteria for dependence [5, 51]. There were anecdotal reports stating that discontinuing benzodiazepines was a challenge in clinical practice. Systematic qualitative approach to the problem informed us of the phenomenon of non-cooperation by non-compliance from subjects treated with long-term therapeutic doses [29]. It placed the term with an evidence base that disseminated the reference and its usage in later works [56–58] (Table 1). But this information should be seen in perspectives of information presented in Sects. 3.1.1 to 3.1.4.
Table 1.
Studies that evaluated low-dose long-term benzodiazepine usage and withdrawal syndrome
| References | Sample size | Age | Drug dose | Duration of use | Type of study | Outcome |
|---|---|---|---|---|---|---|
| [8] |
Subjects—20 Healthy Controls—19 |
Mean age—40.10 years | Diazepam mean 16.2 mg SD (11.5) | Mean—72 months (9–198) | Double-blind placebo controlled | Withdrawal syndrome present |
| [48] | 40 | Middle aged | 0.5–2 times recommended dose of: Bromazepam/Brotizolam/Diazepam/Flunitrazepam/Flurazepam/Lorazepam/Midazolam/Nitrazepam/Oxazepam/Temazepam/Triazolam | > 6 months | Cross-sectional observational | Withdrawal present |
| [37] | 20 | N/A |
Diazepam 10–30 mg Lorazepam 1–7.5 mg Clobazam 30 mg |
1–16 years | Double-blind Placebo controlled | Withdrawal Syndrome present |
| [19] | 143 | Mean age—48 years |
Flunitrazepam 1–2 mg Nitrazepam 5–10 mg |
3 months prior; 13 weeks during trial |
Double-blind randomized placebo-controlled trial | No withdrawal syndrome |
| [28] | 24 | Mean age—54 years | Diazepam 10–30 mg/day | Mean 5 years (1–12 years) | No withdrawal syndrome | |
| [41] | 180 |
Age range 21–65 years (mean N/A) |
Diazepam 15–40 mg/day |
6–22 weeks in trial Previous use (none, < 8 months, > 8 months) |
Double Blind | Limited results |
| [64] | 40 | N/A |
Lorazepam 4 mg (mean dose) Diazepam 10 mg (mean dose) |
3–6 years | Double-blind placebo controlled | Limited results |
| [63] | 41 | Mean age—41 years | Diazepam 5–20 mg | > 6 months | Double blind | Limited results |
| [9] | 39 | Mean age—30 years | Diazepam 30–40 mg | 5 months | Double-blind placebo controlled | Limited results |
Animal studies
Self-administration experiments in rhesus monkeys indicated that the animals did derive positive effects from receiving benzodiazepines and would actively seek further administration, although to a lesser extent than with barbiturates [12, 70]. When these experiments were continued over several weeks, the monkeys not only failed to increase their self-administration but actually reduce it by an amount not explainable by pharmacokinetic factors alone [71]. An animal study on rats, comparing the differences between chronic high- and low-dose chlordiazepoxide demonstrated that there are similar signs of withdrawal between the two groups with statistically significant differences in the intensity of withdrawal symptoms. A conformational change in the receptors or receptor-coupled counter-adaptive changes were proposed as underlying mechanisms (Guarino et al. [17]). Thus, animal studies failed to show the recreational effect, tolerance and continuation of medication over long period.
Human studies
The dissimilitude of overestimating sleep while being medicated and the awareness of sleep disturbance upon discontinuation was the discernment for inability to discontinue long-term therapeutic doses of benzodiazepines [48]. This could easily be explained by hyperarousal occurring in parallel process model of insomnia [43, 46]. This model also shows why most of the patients suffering from chronic insomnia would continue hypnotics in long term.
Risk of fall and fracture
A recent meta-analysis reported increased risk of fractures but not falls among patients taking zolpidem, however, study was not able differentiate whether these events were related to drugs or to the effects of insomnia [62]. Interestingly, not only hypnotics, but also antipsychotics as well as antidepressants increase risk of fall among elderly in different settings, although specific pathophysiologic mechanisms are yet to be elucidated. Among the psychotropics, the odds ratio of falls in the elderly was 2.02 (1.85–2.20) for the selective serotonin reuptake inhibitors, higher than that for benzodiazepines which was 1.42 (1.81–1.27) [52]. Risk of fracture in the elderly who were prescribed benzodiazepines was 1.34 (CI 1.24–1.45) which is lower than that of antidepressants 1.60 (CI 1.38–1.86) and antipsychotics 1.59 (CI 1.27–1.98) [60]. At-risk population for fall and fractures are those on high doses of hypnotics and having co-prescribed psychotropic medications [7]. These observations contradict the claims of increased falls and fractures just by use of hypnotics.
Worsening of OSA and depression of respiration
A meta-analysis suggests that even among patients with obstructive sleep apnea (OSA), BZRAs in therapeutic doses do not worsen OSA [72]. As of now, there is no substantial evidence that hypnotics depress respiration [7]. In fact, a Cochrane review showed that benzodiazepines do not have any significant deterioration in the clinical severity of OSA as measured by apnea–hypopnea index (AHI) [31]. On the contrary this review suggested that Z group of drugs like eszopiclone 3 mg significantly decreased AHI compared to placebo. However, studies included in this review had small sample size with short duration [31]. A recent population-based retrospective case–control study showed that there was a statistically significant association between recent benzodiazepine use and adverse respiratory effects in patients with OSA which persisted even after multivariate adjustment. However, this study was done in a predominantly Taiwanese ethnicity, suffered from the bias of retrospective methodology and could not conclude about the ‘causality’ of benzodiazepine use and adverse respiratory effects [67]. Thus, as of now, it appears that benzodiazepines do not worsen OSA in therapeutic doses.
Mortality
A recent longitudinal study spanning 20 years reported that hypnotics increased mortality in short term (within 2 years of prescription); however, results were confounded by inclusion of subjects with cancer and cardiovascular disorders. Further, causal relationship appeared with the comorbidity rather than with BZD/BZRAs; further causality could not be established as other medications with hypnotic property also increased mortality [20]. A meta-analysis reported that hypnotic users had 43% greater chances of mortality than non-users, however, age of the subjects ranged from 18 to 102 years and subjects in the included studies had other medical disorders, inducing the bias in the results [34]. Another meta-analysis showed that hypnotics in fact reduce the risk of mortality from cardiac diseases, especially in Asian population [25]. On the other hand, initial insomnia and non-refreshing sleep have been found to increase odds for all causes mortality and mortality from cardiovascular diseases [13]
Motor vehicular accidents
Both experimental and epidemiological studies show that hypnotics increase risk of accidents. However, data regarding critical dose of medications associated with risk, pharmacological properties that increase the risk and identifying “population at risk” is sparce [7]. Another controversy is whether the accidents occur due to the effect of the BZD or the effect of the insomnia disorder itself, which if left untreated induces cognitive deficits and psychomotor slowing [67].
Why hypnotic therapy is denounced for the management of insomnia?
A number of factors play a role why hypnotics are avoided in the management of insomnia disorder. First, despite having optimal literature regarding neurobiological basis of insomnia disorder and adverse health consequences of untreated insomnia disorder, it is still not considered as a medical disorder [33]. Second, addictive potential of hypnotics has been disproportionately highlighted in a number of meta-analysis and guidelines, however, scientific backing for the claim appears dodgy [42, 53]. It has been stated correctly in a previous report that “addictive potential of benzodiazepines has been catastrophized” [10]. Reappearance of symptoms after reduction of dose or discontinuation of medication is a common phenomenon in a number of diseases. Many physicians fail to realize that insomnia is a chronic disorder, similar to diabetes mellitus or hypertension and, hence, requires long-term treatment. Discontinuation of antihypertensives and hypoglycemics leads to increase in blood pressure and blood sugar, respectively, similarly, discontinuation of hypnotics would lead to re-appearance of insomnia [10]. Unfortunately, this has been mistakenly labeled as withdrawal insomnia or ‘rebound insomnia’ [53]. A paper from Perlis et al. is worth mentioning here in this regard. They advocated that considering the night-to-night variability in insomnia, long-term intermittent hypnotic therapy should be explored as an option [35]. Such strategy could reduce direct and indirect costs related to insomnia. Third, besides other reasons, hypnotic prescription was considered to be influenced by industry pressure, for which data were not provided [33]. Most of the benzodiazepines are cheap and industry has lost interest in promoting them. While discouraging the use of hypnotics for chronic insomnia, especially in developing and third world countries, benefits and risks must be assessed carefully (Fig. 1) [2, 32, 68]. These factors are important and worthy of scientific investigation in the future.
Fig. 1.
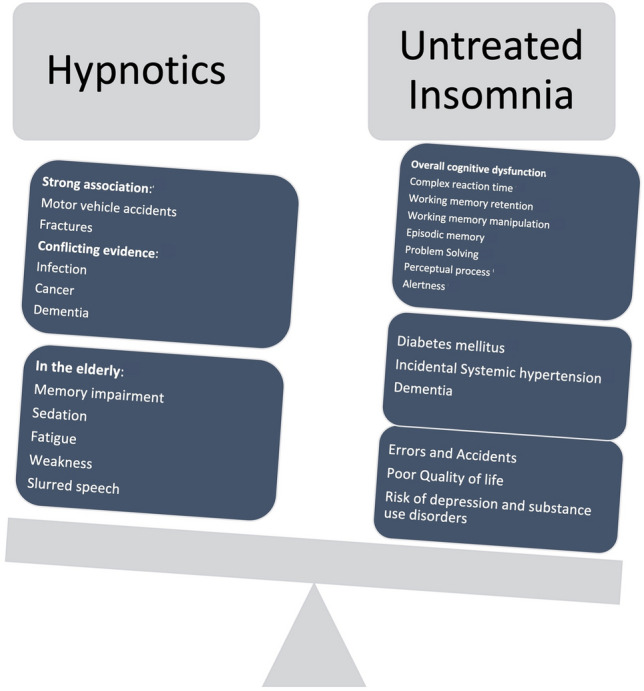
Comparison of harms associated with use of hypnotics and untreated insomnia
Conclusion
Recently, the United States FDA has cautioned about the addiction potential of BZDs [65]. However, as a reaction to it, clinicians should not err on the side of restricting benzodiazepines thereby and allowing the patients to suffer from the consequences of untreated chronic insomnia. CBT-I has many limitations in terms of candidature, adherence, cost of treatment, adverse effects and is mostly not available in most parts of the world especially low- and middle-income countries. Considering these issues, benzodiazepines are the only available option and it should be prescribed to all deserving patients. Here, one needs to perform a balancing act, treating who needs to be treated and at the same time protecting the vulnerable population, e.g., patients having comorbid substance use disorder [21, 36].
Author contributions
RG conceived the study. TJ and AP searched literature. AB and RG reviewed it. RG and TJ prepared first draft. AB and AP critically reviewed it and provided scientific content to bring it to final shape.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declarations
Conflict of interest
Authors do not have any conflict of interest to disclose.
Ethics approval
This is a review article and hence does not require approval from IEC.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5. Arlington: American Psychiatric Association; 2013. [Google Scholar]
- 2.Anothaisintawee T, Reutrakul S, Van Cauter E, et al. Sleep disturbances compared to traditional risk factors for diabetes development: systematic review and meta-analysis. Sleep Med Rev. 2016;30:11–24. doi: 10.1016/j.smrv.2015.10.002. [DOI] [PubMed] [Google Scholar]
- 3.Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. 2005;18:249–255. doi: 10.1097/01.yco.0000165594.60434.84. [DOI] [PubMed] [Google Scholar]
- 4.Asnis GM, Thomas M, Henderson MA. Pharmacotherapy treatment options for insomnia: a primer for clinicians. Int J Mol Sci. 2016 doi: 10.3390/ijms17010050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ballenger JC. Medication discontinuation in panic disorder. J Clin Psychiatry. 1992;53:26–31. [PubMed] [Google Scholar]
- 6.Bloom HG, Ahmed I, Alessi CA, et al. Evidence-based recommendations for the assessment and management of sleep disorders in older persons. J Am Geriatr Soc. 2009;57:761–789. doi: 10.1111/j.1532-5415.2009.02220.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Brandt J, Leong C. Benzodiazepines and Z-drugs: an updated review of major adverse outcomes reported on in epidemiologic research. Drugs R D. 2017;17:493–507. doi: 10.1007/s40268-017-0207-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Busto U, Sellers EM, Naranjo CA, Cappell H, Sanchez-Craig M, Sykora K. Withdrawal reaction after long-term therapeutic use of benzodiazepines. N Engl J Med. 1986;315(14):854–9. doi: 10.1056/NEJM198610023151403. [DOI] [PubMed] [Google Scholar]
- 9.Covi L, Lipman RS, Pattison JH, et al. Length of treatment with anxiolytic sedatives and response to their sudden withdrawal. Acta Psychiatr Scand. 1973;49:51–64. doi: 10.1111/j.1600-0447.1973.tb04398.x. [DOI] [PubMed] [Google Scholar]
- 10.El-Guebaly N, Sareen J, Stein MB. Are there guidelines for the responsible prescription of benzodiazepines? Can J Psychiatry. 2010;55(11):709–714. doi: 10.1177/070674371005501104. [DOI] [PubMed] [Google Scholar]
- 11.Enomoto M, Kitamura S, Tachimori H, et al. Long-term use of hypnotics: analysis of trends and risk factors. Gen Hosp Psychiatry. 2020;62:49–55. doi: 10.1016/j.genhosppsych.2019.11.008. [DOI] [PubMed] [Google Scholar]
- 12.Findley JD, Robinson WW, Peregrino L. Addiction to secobarbital and chlordiazepoxide in the rhesus monkey by means of a self-infusion preference procedure. Psychopharmacologia. 1972;26:93–114. doi: 10.1007/BF00422097. [DOI] [PubMed] [Google Scholar]
- 13.Ge L, Guyatt G, Tian J, Pan B, Chang Y, Chen Y, Li H, Zhang J, Li Y, Ling J, Yang K. Insomnia and risk of mortality from all-cause, cardiovascular disease, and cancer: systematic review and meta-analysis of prospective cohort studies. Sleep Med Rev. 2019;48:101215. doi: 10.1016/j.smrv.2019.101215. [DOI] [PubMed] [Google Scholar]
- 14.Gillin JC, Spinweber CL, Johnson LC. Rebound insomnia: a critical review. J Clin Psychopharmacol. 1989;9(3):161–172. doi: 10.1097/00004714-198906000-00002. [DOI] [PubMed] [Google Scholar]
- 15.Green A, Bensky M, Kemer L, Stein O, Dagan Y. Do chronic hypnotics users truly develop tolerance. J Insomn Sleep Disord. 2019;1(1):102. [Google Scholar]
- 16.Griffiths RR, Weerts EM. Benzodiazepine self-administration in humans and laboratory animals–implications for problems of long-term use and abuse. Psychopharmacology. 1997;134(1):1–37. doi: 10.1007/s002130050422. [DOI] [PubMed] [Google Scholar]
- 17.Guarino J, Boisse N, Gay M. Differentiation of high versus low dose chronic benzodiazepine dependence in the rat. In: Problems of drug dependence: proceedings of the annual scientific meeting, the College on Problems of Drug Dependence, Inc. US Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute on Drug Abuse, 1988; p 330.
- 18.Hajak G, Clarenbach P, Fischer W, Rodenbeck A, Bandelow B, Broocks A, Rüther E. Rebound insomnia after hypnotic withdrawal in insomniac outpatients. Eur Arch Psychiatry Clin Neurosci. 1998;248(3):148–156. doi: 10.1007/s004060050032. [DOI] [PubMed] [Google Scholar]
- 19.Hartelius H, Larsson A-K, Lepp M, et al. A controlled long-term study of flunitrazepam, nitrazepam and placebo, with special regard to withdrawal effects. Acta Psychiatr Scand. 1978;58:1–15. doi: 10.1111/j.1600-0447.1978.tb06915.x. [DOI] [PubMed] [Google Scholar]
- 20.Hedström AK, Hössjer O, Trolle Lagerros Y, et al. Short- and long-term mortality following hypnotic use. J Sleep Res. 2020 doi: 10.1111/jsr.13061. [DOI] [PubMed] [Google Scholar]
- 21.Hirschtritt ME, Olfson M, Kroenke K. Balancing the risks and benefits of benzodiazepines. JAMA. 2021;325(4):347–348. doi: 10.1001/jama.2020.22106. [DOI] [PubMed] [Google Scholar]
- 22.Hockenhull J, Black JC, Haynes CM, et al. Non-medical use of benzodiazepines and Z-drugs in the United Kingdom. Br J Clin Pharmacol. 2020 doi: 10.1111/bcp.14397. [DOI] [PubMed] [Google Scholar]
- 23.Kales A, Scharf MB, Kales JD. Rebound insomnia: a new clinical syndrome. Science. 1978;201:1039–1041. doi: 10.1126/science.684426. [DOI] [PubMed] [Google Scholar]
- 24.Kales A, Soldatos CR, Bixler EO, et al. Rebound insomnia and rebound anxiety: a review. Pharmacology. 1983;26:121–137. doi: 10.1159/000137794. [DOI] [PubMed] [Google Scholar]
- 25.Kim YH, Kim HB, Kim DH, Kim JY, Shin HY. Use of hypnotics and the risk of or mortality from heart disease: a meta-analysis of observational studies. Korean J Intern Med. 2018;33(4):727–736. doi: 10.3904/kjim.2016.282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kuhn BN, Kalivas PW, Bobadilla AC. Understanding addiction using animal models. Front Behav Neurosci. 2019;13:262. doi: 10.3389/fnbeh.2019.00262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kurko TAT, Saastamoinen LK, Tähkäpää S, et al. Long-term use of benzodiazepines: definitions, prevalence and usage patterns—a systematic review of register-based studies. Eur Psychiatry. 2015;30:1037–1047. doi: 10.1016/j.eurpsy.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 28.Laughren TP, Battey Y, Greenblatt DJ, et al. A controlled trial of diazepam withdrawal in chronically anxious outpatients. Acta Psychiatr Scand. 1982;65:171–179. doi: 10.1111/j.1600-0447.1982.tb00838.x. [DOI] [PubMed] [Google Scholar]
- 29.Linden M, Bär T, Geiselmann B. Patient treatment insistence and medication craving in long-term low-dosage benzodiazepine prescriptions. Psychol Med. 1998;28:721–729. doi: 10.1017/S0033291798006734. [DOI] [PubMed] [Google Scholar]
- 30.Malow BA, Byars K, Johnson K, et al. A practice pathway for the identification, evaluation, and management of insomnia in children and adolescents with autism spectrum disorders. Pediatrics. 2012;130(Suppl):S106–S124. doi: 10.1542/peds.2012-0900I. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mason M, Cates CJ, Smith I. Effects of opioid, hypnotic and sedating medications on sleep-disordered breathing in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2015 doi: 10.1002/14651858.CD011090.pub2. [DOI] [PubMed] [Google Scholar]
- 32.Meng L, Zheng Y, Hui R. The relationship of sleep duration and insomnia to risk of hypertension incidence: a meta-analysis of prospective cohort studies. Hypertens Res. 2013;36:985–995. doi: 10.1038/hr.2013.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Moloney ME, Konrad R, Zimmer CR. The medicalization of sleeplessness: a public health concern. Am J Public Health. 2011;101:1429–1433. doi: 10.2105/AJPH.2010.300014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Parsaik AK, Mascarenhas SS, Khosh-Chashm D, Hashmi A, John V, Okusaga O, Singh B. Mortality associated with anxiolytic and hypnotic drugs—a systematic review and meta-analysis. Aust N Z J Psychiatry. 2016;50(6):520–533. doi: 10.1177/0004867415616695. [DOI] [PubMed] [Google Scholar]
- 35.Perlis M, Gehrman P, Riemann D. Intermittent and long-term use of sedative hypnotics. Curr Pharm Des. 2008;14:3456–3465. doi: 10.2174/138161208786549290. [DOI] [PubMed] [Google Scholar]
- 36.Petursson H, Lader MH. Withdrawal from long-term benzodiazepine treatment. Br Med J. 1981 doi: 10.1136/bmj.283.6292.643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Petursson H, Lader MH. Benzodiazepine dependence. Br J Addict. 1981;76(2):133–45. doi: 10.1111/j.1360-0443.1981.tb00218.x. [DOI] [PubMed] [Google Scholar]
- 38.Pillai V, Cheng P, Kalmbach DA, et al. Prevalence and predictors of prescription sleep aid use among individuals with DSM-5 insomnia: the role of hyperarousal. Sleep. 2016;39:825–832. doi: 10.5665/sleep.5636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Pillai V, Roth T, Roehrs T, Moss K, Peterson EL, Drake CL. Effectiveness of benzodiazepine receptor agonists in the treatment of insomnia: an examination of response and remission rates. Sleep. 2017;40(2):zsw044. doi: 10.1093/sleep/zsw044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pinto LR, Jr, Alves RC, Caixeta E, et al. New guidelines for diagnosis and treatment of insomnia. Arq Neuropsiquiatr. 2010;68:666–675. doi: 10.1590/S0004-282X2010000400038. [DOI] [PubMed] [Google Scholar]
- 41.Rickels K, Case WG, Downing RW, Winokur A. Long-term diazepam therapy and clinical outcome. JAMA. 1983;250(6):767–771. doi: 10.1001/jama.1983.03340060045024. [DOI] [PubMed] [Google Scholar]
- 42.Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26:675–700. doi: 10.1111/jsr.12594. [DOI] [PubMed] [Google Scholar]
- 43.Riemann D, Spiegelhalder K, Feige B, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev. 2010;14:19–31. doi: 10.1016/j.smrv.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 44.Roehrs T, Roth T. Hyperarousal in insomnia: pre-sleep and diurnal cortisol levels in response to chronic zolpidem treatment. Sleep Med. 2019;61:52–56. doi: 10.1016/j.sleep.2019.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Roehrs T. Rebound insomnia: its determinants and significance. Am J Med. 1990;88:39S–42S. doi: 10.1016/S0002-9343(13)80001-0. [DOI] [PubMed] [Google Scholar]
- 46.Roth T, Roehrs T, Pies R. Insomnia: pathophysiology and implications for treatment. Sleep Med Rev. 2007;11:71–79. doi: 10.1016/j.smrv.2006.06.002. [DOI] [PubMed] [Google Scholar]
- 47.Sateia MJ, Buysse DJ, Krystal AD, et al. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13:307–349. doi: 10.5664/jcsm.6470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Schneider-Helmert D, et al. Why low-dose benzodiazepine-dependent insomniacs can’t escape their sleeping pills. Acta Psychiatr Scand. 1988;78:706–711. doi: 10.1111/j.1600-0447.1988.tb06408.x. [DOI] [PubMed] [Google Scholar]
- 49.Schonmann Y, Goren O, Bareket R, et al. Chronic hypnotic use at 10 years—does the brand matter? Eur J Clin Pharmacol. 2018;74:1623–1631. doi: 10.1007/s00228-018-2531-4. [DOI] [PubMed] [Google Scholar]
- 50.Schutte-Rodin S, Broch L, Buysse D, et al. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4:487–504. doi: 10.5664/jcsm.27286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sellers EM, Ciraulo DA, DuPont RL, et al. Alprazolam and benzodiazepine dependence. J Clin Psychiatry. 1993;54:64–75. [PubMed] [Google Scholar]
- 52.Seppala LJ, Wermelink AMAT, de Vries M, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: II. Psychotropics. J Am Med Dir Assoc. 2018;19(371):e11–371.e17. doi: 10.1016/j.jamda.2017.12.098. [DOI] [PubMed] [Google Scholar]
- 53.Sirdifield C, Chipchase SY, Owen S, et al. A systematic review and meta-synthesis of patients’ experiences and perceptions of seeking and using benzodiazepines and Z-drugs: towards safer prescribing. Patient. 2017;10:1–15. doi: 10.1007/s40271-016-0182-z. [DOI] [PubMed] [Google Scholar]
- 54.Smith SM, Dart RC, Katz NP, et al. Classification and definition of misuse, abuse, and related events in clinical trials: ACTTION systematic review and recommendations. Pain. 2013;154:2287–2296. doi: 10.1016/j.pain.2013.05.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Soldatos CR, Dikeos DG, Whitehead A. Tolerance and rebound insomnia with rapidly eliminated hypnotics: a meta-analysis of sleep laboratory studies. In: Database of Abstracts of Reviews of Effects (DARE): quality-assessed reviews [Internet]. 1999. York (UK): Centre for Reviews and Dissemination (UK); 1995. Available from: https://www.ncbi.nlm.nih.gov/books/NBK67701/. [PubMed]
- 56.Soyka M, Queri S, Küfner H, Rösner S. Where are 1.9 million drug addicts hiding? Neurologist. 2005;76(1):72–77. doi: 10.1007/s00115-004-1828-y. [DOI] [PubMed] [Google Scholar]
- 57.Soyka M. Abuse of, and dependence on, medically prescribed drugs. In: Henn F, Sartorius N, Helmchen H, Lauter H, editors. Contemporary psychiatry. Berlin: Springer; 2001. [Google Scholar]
- 58.Soyka M. Treatment of benzodiazepine dependence. N Engl J Med. 2017;376:1147–1157. doi: 10.1056/NEJMra1611832. [DOI] [PubMed] [Google Scholar]
- 59.Takaesu Y, Komada Y, Asaoka S, et al. Factors associated with long-term use of hypnotics among patients with chronic insomnia. PLoS ONE. 2014 doi: 10.1371/journal.pone.0113753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Takeshima N, Ogawa Y, Hayasaka Y, et al. Continuation and discontinuation of benzodiazepine prescriptions: a cohort study based on a large claims database in Japan. Psychiatry Res. 2016;237:201–207. doi: 10.1016/j.psychres.2016.01.040. [DOI] [PubMed] [Google Scholar]
- 61.Tan KR, Brown M, Labouébe G, et al. Neural bases for addictive properties of benzodiazepines. Nature. 2010;463:769–774. doi: 10.1038/nature08758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Treves N, Perlman A, Kolenberg Geron L, et al. Z-drugs and risk for falls and fractures in older adults-a systematic review and meta-analysis. Age Ageing. 2018;47:201–208. doi: 10.1093/ageing/afx167. [DOI] [PubMed] [Google Scholar]
- 63.Tyrer P, Owen R, Dawling S. Gradual withdrawal of diazepam after long-term therapy. Lancet. 1983;321(8339):1402–1406. doi: 10.1016/S0140-6736(83)92355-3. [DOI] [PubMed] [Google Scholar]
- 64.Tyrer P, Rutherford D, Huggett T. Benzodiazepine withdrawal symptoms and propranolol. Lancet. 1981;317(8219):520–522. doi: 10.1016/S0140-6736(81)92861-0. [DOI] [PubMed] [Google Scholar]
- 65.US Food and Drug Administration . FDA requiring boxed warning updated to improve safe use of benzodiazepine drug class. US FDA; 2020. [Google Scholar]
- 66.Votaw VR, Geyer R, Rieselbach MM, McHugh RK. The epidemiology of benzodiazepine misuse: a systematic review. Drug Alcohol Depend. 2019;1(200):95–114. doi: 10.1016/j.drugalcdep.2019.02.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Wang S-H, Chen W-S, Tang S-E, et al. Benzodiazepines associated with acute respiratory failure in patients with obstructive sleep apnea. Front Pharmacol. 2019;9:1513. doi: 10.3389/fphar.2018.01513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Wardle-Pinkston S, Slavish DC, Taylor DJ. Insomnia and cognitive performance: a systematic review and meta-analysis. Sleep Med Rev. 2019;48:101205. doi: 10.1016/j.smrv.2019.07.008. [DOI] [PubMed] [Google Scholar]
- 69.World Health Organization . Lexicon of alcohol and drug terms. World Health Organization; 1994. [Google Scholar]
- 70.Yanagita T, Takahashi S. Dependence liability of several sedative-hypnotic agents evaluated in monkeys. J Pharmacol Exp Ther. 1973;185(2):307–316. [PubMed] [Google Scholar]
- 71.Yanagita T. Dependence-producing effects of anxiolytics. In: Hoffmeister F, Stille G, editors. Psychotropic agents. Handbook of experimental pharmacology (continuation of Handbuch der experimentellen Pharmakologie), vol 55/2. Berlin: Springer; 1981. [Google Scholar]
- 72.Zhang XJ, Li QY, Wang Y, et al. The effect of non-benzodiazepine hypnotics on sleep quality and severity in patients with OSA: a meta-analysis. Sleep Breath. 2014;18:781–789. doi: 10.1007/s11325-014-0943-7. [DOI] [PubMed] [Google Scholar]