

Abstract
Objective
The impact of poor sleep on tinnitus has been mainly attributed to central processes. There is an association between sleep disorders and hearing loss, but whether hearing levels mediate the association between sleep disorders and tinnitus is unknown. This study investigates the association between sleep characteristics, tinnitus, and hearing loss.
Study Design
Cross‐sectional.
Setting
National Health and Nutrition Examination Survey (NHANES).
Methods
Study cohort includes 9693 adults (≥20 years) from the NHANES 2005 to 2018 who completed audiometric testing and questionnaires on tinnitus and sleep characteristics. Multivariable regression analyses were performed to quantify associations between sleep characteristics, tinnitus, and hearing loss.
Results
In this cohort, 29% (95% confidence interval [CI]: 28%‐31%) reported trouble sleeping and 9% (95% CI: 8%‐10%) reported being diagnosed with sleep disorders. Negative sleep characteristics (less hours of sleep, diagnosis of a sleep disorder, trouble sleeping, or OSA symptoms) were not associated with audiometry‐measured hearing loss in multivariable models adjusted for demographics and comorbidities but were significantly associated with bothersome tinnitus. This association remained significant without substantial attenuation in multivariable models additionally adjusting for hearing levels: sleeping <8 h/day (vs ≥8) (odds ratio [OR]: 1.28 [95% CI: 1.08‐1.52]), trouble sleeping (OR: 1.78 [95% CI: 1.45‐2.19]), diagnosis of sleep disorders (OR: 1.57 [95% CI: 1.14‐2.15]), and report of OSA symptoms (OR: 1.42 [95% CI: 1.08‐1.88]).
Conclusion
Negative sleep characteristics were associated with tinnitus while there was no clinically meaningful association between sleep and hearing loss. Our findings suggest that the relationship between poor sleep and tinnitus is likely contributed by central processes without a major role of mediation via the peripheral auditory system.
Keywords: hearing loss, NHANES, sleep, tinnitus
Tinnitus is a phenomenon of perceiving sound in the absence of external stimuli. There exists significant heterogeneity across tinnitus etiology, severity, and impact, highlighting its multifaceted nature. Due to this heterogeneity, there is no singular mechanism that fully explains tinnitus, nor is there a universally effective treatment. Severe tinnitus can have a negative impact on daily functioning, quality of life, and mental health. 1 , 2 , 3 , 4 , 5 Tinnitus imposes a significant economic burden on healthcare, with direct and indirect costs in the United States exceeding $15 billion annually. 6 In 2020, more than 2.3 million US veterans received compensation for tinnitus‐related claims—for a total cost believed to be more than $2.75 billion. 6 , 7 , 8
Sleep disorders are strongly linked to tinnitus. Disrupted sleep is a well‐established risk factor for worsening the distress caused by tinnitus. 9 Conversely, bothersome tinnitus itself is a risk factor for poor sleep quality, creating a vicious cycle. 10 Prior studies have demonstrated that various negative sleep characteristics are significantly associated with tinnitus. Chronic tinnitus patients are more likely to report insomnia, poor sleep efficiency, and sleep quality. 10 , 11 , 12 Furthermore, insomnia has been associated with tinnitus and some studies have found links between increased intensity of tinnitus and impaired sleep quality. 13 , 14 Studies have also shown that the prevalence of obstructive sleep apnea (OSA) is higher among tinnitus patients. 15 Given these significant correlations, there have been efforts to understand the mechanistic pathways linking tinnitus and sleep disorders and to manage them in conjunction based on shared strategies such as cognitive behavior therapy. 16 Various mechanisms have been proposed to explain these links, mainly via central auditory pathway such as hyperarousal of the sympathetic nervous system in limbic and autonomic brain activities exacerbating the intolerance of tinnitus. 17
Recently, there has been emerging evidence indicating the association between sleep disorders and hearing loss. 18 Patients with a diagnosis of OSA were found to have higher rates of audiometry‐measured hearing loss based on population‐based and clinic‐based cohorts. 19 , 20 , 21 , 22 Ischemic damage to the cochlea secondary to periods of apnea during sleep has been proposed as one of the underlying mechanisms. 23 , 24 These findings demonstrate the potential role of hearing loss as a mediator of the association between sleep disorders and tinnitus via peripheral auditory pathway. However, no prior studies have investigated the association between sleep‐related characteristics and tinnitus with audiometry‐measured hearing loss as a potential mediator.
In this study, we examined the association between sleep characteristics, tinnitus, and hearing loss based on a large population‐based cohort of US adults. We particularly assessed the role of objectively measured hearing thresholds as a potential mediator of associations between negative sleep characteristics and tinnitus.
Methods
Study Population
The analytic cohort was comprised of 9693 participants from the National Health and Nutrition Examination Survey (NHANES) who were 20 years of age or older and who had complete data on tinnitus, audiometric assessment, sleep, and related demographic characteristics. The NHANES is an ongoing program of studies designed to assess the health, functional, and nutritional status of the noninstitutionalized, civilian US population. Each of the sequential, cross‐sectional study cycles in NHANES uses a stratified, multistage probability sampling design to survey a sample of the US population with selective oversampling of low‐income individuals, racial minorities, and older adults. Sampling weights allow for analyses that account for the complex survey design and yield results that are generalizable to the US population. NHANES cohorts from 2005 to 2006, 2011 to 2012, 2015 to 2016, and 2017 to 2018 were included excluding cohorts with audiometry data on pediatric participants. The study underwent review by the University of Minnesota Institutional Review Board and was deemed exempt (#00015174).
Sleep‐Related Variables
Five sleep‐related variables were defined through NHANES: sleep hours as a continuous variable, sleep hours as a binary variable, sleep disorder diagnosis, trouble with sleeping, and OSA symptoms. Participants were asked the number of hours of sleep they usually get at night in integers (SLD010H and SLD012). This served as our sleep hours variable. Because of the recommended sleep duration in young adults, adults, and older adults, we analyzed sleep duration continuously and binarily (≥8 and <8 hours). 25 Participants were asked if they had ever been told by a doctor that they had a sleep disorder (SLQ060) or if they had ever told a doctor that they had trouble sleeping (SLQ050). Positive answers for these questions indicated a “sleep disorder diagnosis” and “trouble with sleeping,” respectively. Participants were asked how often they had snored while they slept (SLQ030) and how often they snorted, gasped, or stopped breathing in the past 12 months (SLQ040). Additionally, they were asked how many times they felt excessively or overly sleepy during the day in the past month (SLQ120). Possible answers for all three questions were never, rarely (1‐2 times per week), occasionally (3‐4 times per week), or frequently (≥5 times per week). Individuals who answered “occasionally” or “frequently” to all three questions were determined to be positive for “obstructive sleep apnea symptoms” in our analysis as in prior literature. 26 Data on OSA symptoms was available in a subset of the cohort (NHANES 2005‐2006, 2016‐2017, 2017‐2018, n = 4651). Sample weights were adjusted for this subgroup analysis for the presence of OSA symptoms to account for the changes in study cohort.
Audiometric Assessment and Tinnitus
Audiometric assessment was performed by trained examiners based on the established NHANES protocols. 27 A trained examiner determined the air conduction hearing threshold for each unaided ear in a sound‐isolated room in the mobile examination center. Testing was conducted according to a modified Hughson‐Westlake procedure using the automated testing mode of the audiometer (Model AD 226; Interacoustics). Quality assurance and control were established through daily calibration of equipment and monitoring of ambient noise levels using a sound level meter. Thresholds were measured twice at 1 kHz in each ear as an additional quality measure, and audiometry was repeated if there was a greater than 10‐dB discrepancy between the threshold measurements. Speech‐frequency pure‐tone average (PTA) was calculated for each ear based on thresholds at 0.5, 1, 2, and 4 kHz. Audiometry‐measured hearing loss was defined as speech‐frequency PTA at 25 dB HL or greater in better hearing ear as defined by the World Health Organization. 28 Tinnitus was defined as answering “yes” to the question as in prior literature: In the past 12 months, have you been bothered by ringing, roaring, or buzzing in your ears or head that lasts for 5 minutes or more? 29 , 30 , 31 Sensitivity analyses were performed defining audiometry‐measured hearing loss based on high‐frequency thresholds (PTA at 3, 4, 6, and 8 kHz as defined in prior study) given the significant association between high‐frequency hearing loss and tinnitus. 32
Other Study Variables
Data on demographics, medical history, noise exposure history, and depression were obtained from interviews. Sex was included as a binary variable. Race/ethnicity was grouped as white (non‐Hispanic white), black (non‐Hispanic black), Hispanic (Mexican American or other Hispanic), or other. Education was categorized in three groups (<12th grade, high school graduate, or some college or more). Household income was reported in five categories (<$20,000, $20,000‐$44,999, $45,000‐$74,999, ≥$75,000, unknown). Insurance status was included as a binary variable for analyses and further descriptive categories were provided (none, private insurance, Medicare, Medicaid, or unknown). Medical history variables include smoking (never, former, current), diabetes (based on self‐reported diagnosis and/or current use of insulin or other diabetic medications), hypertension (told by physician on two or more visits about hypertension diagnosis), cardiovascular disease (congestive heart failure, coronary artery disease, angina pectoris, or myocardial infarction), and stroke (self‐reported history). Occupational noise exposure (“Have you ever had a job where you were exposed to loud noise for five or more hours a week?”—yes or no), and recreational noise exposure (“Outside of a job, have you ever been exposed to very loud noise or music for five or more hours a week?”—yes or no) was also included. Depression was defined by a Patient Health Questionnaire‐9 (PHQ‐9) score ≥10 as in prior literature. 33
Statistical Analyses
Complex sampling design was accounted for by using sample weights according to the National Center for Health statistics guidelines in all analyses, except for the data presented in Table 1. 34 The population prevalence of the five sleep variables were estimated with 95% confidence intervals (CIs) in the overall cohort, individuals without tinnitus, and individuals with tinnitus. Logistic regression analysis was used to examine the association between the sleep variables and tinnitus. Multivariable regression models were adjusted for age, demographic factors, medical history, and noise exposure sequentially. Linear and logistic regression analyses were used to examine the association between sleep variables and hearing loss as continuous and binary (<25 and ≥25 dB HL) variables, respectively. Statistical significance was set at P < .05, two‐tailed. All analyses were conducted using Stata software (version 16.1; StataCorp.).
Table 1.
Study Participant Characteristics, NHANES 2005‐2018 (n = 9693)
| Sleep hours | ||||
|---|---|---|---|---|
| Overall | ≥8 hours | <8 hours | ||
| Characteristics | n = 9693 | n = 4112 | n = 5581 | P value |
| Mean age, years (SD) | 51.7 (18.7) | 52.5 (19.7) | 51.1 (17.9) | <.001 |
| Sex, n (%) | ||||
| Female | 4782 (49.3) | 2173 (52.9) | 2609 (46.8) | <.001 |
| Race, n (%) | ||||
| White | 4012 (41.4) | 1847 (44.9) | 2165 (38.8) | <.001 |
| Black | 2185 (22.5) | 752 (18.3) | 1433 (25.7) | <.001 |
| Hispanic | 2213 (22.8) | 999 (24.3) | 1214 (21.8) | <.001 |
| Other | 1283 (13.2) | 514 (12.5) | 769 (13.8) | <.001 |
| Education, n (%) | ||||
| Less than high school | 2159 (22.3) | 984 (23.9) | 1175 (21.0) | .001 |
| High school graduate | 2200 (22.7) | 948 (23.0) | 1252 (22.4) | .001 |
| Some college or more | 5334 (55.0) | 2180 (53.0) | 3154 (56.5) | .001 |
| Income, n (%) | ||||
| <$20,000 | 1811 (18.7) | 789 (19.2) | 1022 (18.3) | .006 |
| $20,000‐$44,999 | 2500 (25.8) | 1095 (26.6) | 1405 (25.2) | .006 |
| $45,000‐$74,999 | 1685 (17.4) | 692 (16.8) | 993 (17.8) | .006 |
| ≥$75,000 | 2292 (23.6) | 908 (22.1) | 1384 (24.8) | .006 |
| Unknown | 1405 (14.5) | 628 (15.3) | 777 (13.9) | .006 |
| Health insurance, n (%) | ||||
| None | 1763 (18.2) | 749 (18.2) | 1014 (18.2) | <.001 |
| Private | 3681 (38.0) | 1346 (32.7) | 2335 (41.8) | <.001 |
| Medicare | 2509 (25.9) | 1228 (29.9) | 1281 (23.0) | <.001 |
| Medicaid | 987 (10.2) | 472 (11.48) | 515 (9.2) | <.001 |
| Unknown | 753 (7.8) | 317 (7.7) | 436 (7.8) | <.001 |
| Smoking, n (%) | ||||
| Never | 5380 (55.5) | 2346 (57.1) | 3034 (54.4) | .004 |
| Former | 2522 (26.0) | 1066 (25.9) | 1456 (26.1) | .004 |
| Current | 1791 (18.5) | 700 (17.0) | 1091 (19.5) | .004 |
| Diabetes, n (%) | 1498 (15.4) | 667 (16.2) | 831 (14.9) | .073 |
| Hypertension, n (%) | 3570 (36.8) | 1509 (36.7) | 2061 (36.9) | .815 |
| Cardiovascular disease, n (%) | 928 (9.6) | 403 (9.8) | 525 (9.4) | 0.515 |
| Stroke, n (%) | 403 (4.2) | 191 (4.6) | 212 (3.8) | .039 |
| Occupational noise exposure, n (%) | 3408 (35.2) | 1347 (32.8) | 2061 (36.9) | <.001 |
| Recreational noise exposure, n (%) | 1308 (13.5) | 510 (12.4) | 798 (14.3) | .007 |
| Major depressive disorder, n (%) | 559 (5.8) | 224 (5.5) | 335 (6.0) | .247 |
Results
The overall study cohort consisted of 9693 adults who participated in the 2005 to 2018 NHANES (4782 women [49.3%] and 4911 men [50.7%]; mean [SD] age, 51.7 [18.7] years). Unweighted participant characteristics are summarized in Table 1. In this representative cohort of US adults, the mean sleep hours were 7.3 (SD 1.5) and 57% [95% CI: 56%‐58%] reported sleeping less than 8 hours. 29% [95% CI: 28%‐31%] reported trouble sleeping, 9% [95% CI: 8%‐10%] reported being diagnosed with sleep disorders, and 22% [95% CI: 20%‐24%] reported OSA symptoms. Figure 1 represents the prevalence of negative sleep characteristics for the overall study cohort and by presence and absence of bothersome tinnitus. The prevalence of sleep disorders, trouble sleeping, and OSA symptoms were higher in adults who reported having bothersome tinnitus.
Figure 1.
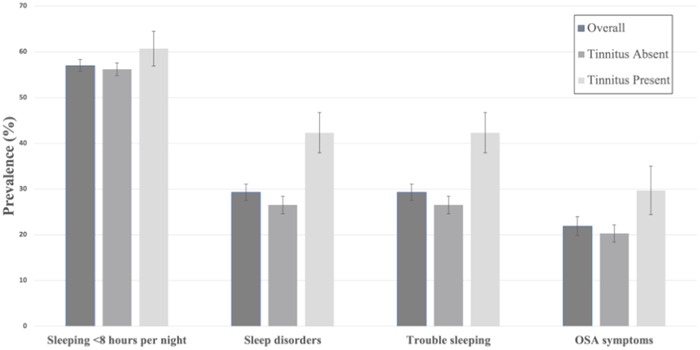
Prevalence of negative sleep characteristics for the overall cohort and by presence of bothersome tinnitus in the past 12 months. Sleep Hours: Participants were asked the number of hours of sleep they usually get at night on weekdays or workdays in integers. Sleep Disorders: Answering “yes” to “Have you ever been told by a doctor or other health professional that you have a sleeping disorder?” Trouble Sleeping: Answering “yes” to “Have you ever told a doctor or other health professional that you have trouble sleeping?” OSA symptoms: Answering “occasionally” or “frequently” to all three of the following questions; “In the past 12 months, how often did you snore while you were sleeping?” “In the past 12 months, how often did you snort, gasp, or stop breathing while you were sleeping?” and “In the past month, how often did you feel excessively or overly sleepy during the day?” OSA, obstructive sleep apnea.
Table 2 summarizes findings from the univariable and multivariable logistic regression analyses examining the associations between sleep‐related variables and tinnitus. Negative sleep characteristics were significantly associated with bothersome tinnitus in the crude model. These associations remained significant across all sleep‐variables in multivariable models adjusting for hearing levels, demographics, medical comorbidities, history of noise exposure, and depression (model 3). In these models, sleeping less than 8 hours per night was associated with 28% (95% CI: 8%‐52%) increased risk of bothersome tinnitus than sleeping more than 8 hours per night. Reporting trouble with sleeping was associated with 78% (95% CI: 45%‐119%) increased risk of bothersome tinnitus. Report of OSA symptoms was associated with 42% (95% CI: 8%‐88%) increased risk of bothersome tinnitus.
Table 2.
Logistic Regression Analysis Examining the Association Between Sleep Variables and Bothersome Tinnitus
| Odds ratio (95% CI) | P value | |
|---|---|---|
| Sleep hours (continuous) | ||
| Crude modela | 0.92 (0.87‐0.97) | .003 |
| Multivariable model | ||
| Model 1 | 0.91 (0.86‐0.96) | <.001 |
| Model 2 | 0.91 (0.86‐0.95) | <.001 |
| Model 3 | 0.92 (0.88‐0.97) | .002 |
| Model 4 | 0.93 (0.89‐0.98) | .004 |
| Sleep hours (binary; ≥8 h (reference) vs. <8 h) | ||
| Crude modela | 1.21 (1.02‐1.43) | .028 |
| Multivariable model | ||
| Model 1 | 1.30 (1.10‐1.55) | .003 |
| Model 2 | 1.31 (1.10‐1.55) | .002 |
| Model 3 | 1.28 (1.08‐1.52) | .005 |
| Model 4 | 1.25 (1.05‐1.49) | .012 |
| Sleep disorder diagnosis | ||
| Crude modela | 2.05 (1.56‐2.68) | <.001 |
| Multivariable model | ||
| Model 1 | 1.97 (1.48‐2.61) | <.001 |
| Model 2 | 1.88 (1.40‐2.451) | <.001 |
| Model 3 | 1.57 (1.14‐2.15) | .006 |
| Model 4 | 1.55 (1.13‐2.13) | .007 |
| Trouble with sleeping | ||
| Crude modela | 2.04 (1.69‐2.44) | <.001 |
| Multivariable model | ||
| Model 1 | 1.97 (1.62‐2.40) | <.001 |
| Model 2 | 1.98 (1.63‐2.40) | <.001 |
| Model 3 | 1.78 (1.45‐2.19) | <.001 |
| Model 4 | 1.73 (1.43‐2.10) | <.001 |
| Obstructive sleep apnea symptoms | ||
| Crude modela | 1.66 (1.32‐2.09) | <.001 |
| Multivariable model | ||
| Model 1 | 1.65 (1.28‐2.13) | <.001 |
| Model 2 | 1.57 (1.22‐2.04) | .001 |
| Model 3 | 1.42 (1.08‐1.88) | .015 |
| Model 4 | 1.41 (1.08‐1.84) | .013 |
Model 1: adjusted for age, hearing levels. Model 2: adjusted for age, hearing levels, and other demographic factors (sex, race, education, income, health insurance). Model 3: adjusted for age, hearing levels, demographic factors, medical history (smoking, diabetes, hypertension, cardiovascular disease, stroke), occupational and recreational noise exposure, and depression. Model 4: adjusted for all variables in model 3 except hearing levels (excluding hearing levels as a covariate).
Crude model: unadjusted crude model.
Table 3 summarizes findings from the univariable and multivariable logistic and linear regression analyses examining the associations between sleep‐related variables and audiometry‐measured hearing loss. Hearing loss was defined in two ways, as a continuous variable and as a binary variable (speech frequency PTA in better hearing ear <25 vs ≥25 dB HL). When considering hearing loss as a continuous variable, a history of sleep disorder diagnosis and report of trouble with sleeping were associated with increased hearing thresholds in the crude model (β = 2.25, 95% CI: 0.78‐3.73; β = 1.55, 95% CI: 0.77‐2.33). In multivariable models adjusting for demographics, medical comorbidities, and noise exposure, there was no statistically significant association between a history of sleep disorder diagnosis and hearing loss (β = 0.12, 95% CI: −1.13‐1.37). While the association between report of trouble with sleeping and hearing loss remained statistically significant, the effect size remained small without clinically meaningful differences in hearing thresholds (β = −0.69, 95% CI: −1.37‐0). Similarly, there were no significant associations between sleep‐related characteristics and hearing loss when hearing loss was defined as a binary variable (<25 vs ≥25 dB HL) in multivariable models. Sensitivity analysis was performed defining hearing loss based on high‐frequency thresholds (continuous and binary variables). Findings from the sensitivity analysis demonstrated no changes in statistical significance, effect size, or directionality of these associations (data not shown).
Table 3.
Linear and Logistic Regression Analysis Examining the Association Between Sleep Variables and Hearing Loss
| Linear regression | Logistic regression | |||
|---|---|---|---|---|
| HL continuously (dB) | HL binary (<25 vs ≥25 dB) | |||
| β‐coefficients (95% CI) | P value | Odds ratio (95% CI) | P value | |
| Sleep hours (continuous) | ||||
| Crude modela | 0.23 (−0.06‐0.53) | .114 | 1.05 (1.00‐1.11) | .069 |
| Multivariable model | ||||
| Model 1 | 0.15 (−0.04‐0.34) | .122 | 0.97 (0.91‐1.03) | .297 |
| Model 2 | 0.12 (−0.05‐0.30) | .170 | 0.98 (0.92‐1.04) | .512 |
| Model 3 | 0.15 (−0.03‐0.33) | .095 | 0.98 (0.92‐1.05) | .631 |
| Sleep hours (binary; ≥8 h (reference) vs <8 h) | ||||
| Crude modela | −1.26 (−2.03 to −0.49) | .002 | 0.78 (0.67‐0.90) | .001 |
| Multivariable model | ||||
| Model 1 | −0.67 (−1.27 to −0.44) | .036 | 1.01 (0.83‐1.23) | .11 |
| Model 2 | −0.50 (−1.06‐0.05) | .073 | 0.99 (0.82‐1.19) | .879 |
| Model 3 | −0.53 (−1.08‐0.02) | .058 | 0.98 (0.80‐1.18) | .803 |
| Sleep disorder diagnosis | ||||
| Crude modela | 2.25 (0.78‐3.73) | .003 | 1.15 (0.83‐1.61) | .389 |
| Multivariable model | ||||
| Model 1 | 0.50 (−0.68‐1.267) | .398 | 1.20 (0.80‐1.80) | .38 |
| Model 2 | 0.28 (−0.86‐1.42) | .62 | 1.10 (0.71‐1.70) | .658 |
| Model 3 | 0.12 (−1.13‐1.37) | .848 | 1.08 (0.67‐1.74) | .755 |
| Trouble with sleeping | ||||
| Crude modela | 1.55 (0.77‐2.33) | <.001 | 1.24 (1.08‐1.42) | .003 |
| Multivariable model | ||||
| Model 1 | −0.55 (−1.30‐0.20) | .15 | 1.06 (0.088‐1.27) | .549 |
| Model 2 | −0.37 (−1.06‐0.31) | .278 | 1.15 (0.95‐1.39) | .152 |
| Model 3 | −0.69 (−1.37‐0.00) | .049 | 1.09 (0.90‐1.33) | .348 |
| Obstructive sleep apnea symptoms | ||||
| Crude modela | 0.97 (−0.41‐2.35) | .164 | 1.06 (0.80‐1.42) | .68 |
| Multivariable model | ||||
| Model 1 | 0.34 (−0.90‐1.58) | .585 | 1.32 (0.88‐1.98) | .177 |
| Model 2 | 0.18 (−0.89‐1.25) | .733 | 1.26 (0.87‐1.83) | .216 |
| Model 3 | −0.18 (−1.30‐0.93) | .741 | 1.17 (0.79‐1.74) | .429 |
Model 1: adjusted for age. Model 2: adjusted for age and other demographic factors (sex, race, education, income, health insurance). Model 3: adjusted for age, demographic factors, medical history, and noise exposure. Bold‐face values indicate models with P < .05.
Crude model: unadjusted crude model.
Figure 2 summarizes the conceptual model for the mediation analysis for the association between poor sleep characteristics and tinnitus with audiometry‐measured hearing as a potential mediator. We found no significant association between poor sleep characteristics and audiometry‐measured hearing mediating the association between poor sleep characteristics and tinnitus. Multivariable models with or without hearing levels as a covariate (Table 2, Model 3 vs Model 4) found no significant shifts in the degree of the associations between sleep‐related variables and bothersome tinnitus suggestive of the mediation effect.
Figure 2.
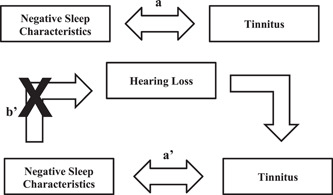
Path diagrams for the association among sleep characteristics, hearing loss, and tinnitus. a/a′: Models in Table 2. b′: Models in Table 3.
Discussion
In this nationally representative sample of US adults, negative sleep characteristics were significantly associated with bothersome tinnitus. Report of bothersome tinnitus was associated with less hours of sleep per night, being diagnosed with sleep disorders, report of trouble with sleeping, and OSA symptoms. Contrarily, there was no significant association between negative sleep characteristics and audiometry‐measured hearing loss. Our findings suggest no significant role of hearing loss as a mediator contributing to the association between negative sleep characteristics and bothersome tinnitus on a population‐level.
Our findings linking negative sleep characteristics to tinnitus are consistent with previous studies and this association has been described extensively. 14 , 35 , 36 , 37 , 38 Contrarily, few epidemiological studies have investigated the association between audiometry‐measured hearing loss and sleep characteristics. 39 , 40 To our knowledge, this is the first population‐based study exploring the role of hearing loss as a potential mediator in the association between tinnitus and negative sleep characteristics. Prior studies have found that the reported severity of tinnitus is highly correlated to the severity of sleep disturbance. 41 One proposed hypothesis underlying this association is that severe tinnitus can cause inappropriate activation of the limbic and sympathetic nervous systems. 42 To support this theory, one study investigating four patients who could alter the loudness of their tinnitus showed links between the limbic system and auditory system when measured by Positron Emission Tomography, although an exact mechanism for this has not been revealed. 43 This activation can be associated with the sleep disorder characteristics described in this study and others such as anxiety, depression, and panic disorders which also have a higher prevalence in tinnitus patients. 44 , 45 , 46 Hyperarousal and enhanced activation of the limbic and sympathetic nervous system are likewise implicated in sleep disturbances, as has been shown in various animal models. 17 , 47 , 48 The similarities in neural activation in tinnitus and sleep disturbances may reveal implications on clinical treatment options that can target these pathways.
In this cohort, there was no clinically meaningful association between sleep‐related variables and audiometry‐measured hearing. Several prior cohort studies interestingly have found significant associations between increased sleep duration and subclinical hearing loss. The inconsistent findings may have been contributed by variability in the cohort characteristics. A study based on a cohort of older adults in the US aged 70 years and older found that each additional hour of sleep after 8 hours was associated with a 2.89 dB HL high‐frequency PTA. 39 Another study based on a large population‐based cohort of adults aged 20 to 79 from Japan demonstrated an association between longer sleep duration and subclinical hearing loss at 1k and 4k Hz. 40 Although an underlying mechanism explaining the association between longer sleep duration and hearing loss has not been identified, some have hypothesized that this may be linked to the cardiovascular effects of increased sleep, particularly diabetes, obesity, and stroke. 49 , 50 These diseases have also been shown to be associated with HL. 51 , 52 , 53 In our cohort, we did not find any significant association of sleep duration with speech‐frequency or high‐frequency hearing loss with or without adjusting for cardiovascular diseases. There was no significant role of audiometry‐measured hearing as a mediator for the association between sleep‐related variables and tinnitus.
A few prior studies have investigated the potential role of treatment for sleep disorders such as OSA on hearing and tinnitus. A meta‐analyses of 20 cohort, case‐control, and cross‐sectional studies that diagnosed OSA by polysomnography or sleep tests and hearing threshold level totaling 33,391 adult patients found that continuous positive airway pressure (CPAP) treatment for OSA did not show improvement in audiometry‐measured hearing loss. 54 In contrast, a prior non‐randomized, noncontrolled study assessing the impact of CPAP treatment on tinnitus found that the Tinnitus Handicap Inventory scores significantly decreased with CPAP use after 3 months for 14 patients with sleep‐disorder breathing and tinnitus symptoms. 55 Multiple studies have shown improvements in depression and anxiety symptoms following CPAP use, which have been heavily linked to tinnitus. 56 , 57 CPAP treatment for OSA may have positive impact on mitigating bothersome tinnitus. Whether this is due to CPAP's improvement of tinnitus or the noise‐masking of a CPAP machine, a known treatment for tinnitus, is unknown. Further studies investigating this and the impact of medical and surgical treatments of OSA on hearing loss and tinnitus are needed to understand their effectiveness.
There are several limitations to this study. First, this is a cross‐sectional study, and temporal and causal relationships between the associations are unable to be established in this data. Furthermore, there may be additional confounders and mediators that were not available in this dataset. Examples of these include anxiety, diet, and alcohol consumption. Presence of OSA symptoms were defined by the questionnaire, and data on formal diagnosis of OSA via polysomnography were unavailable. Tinnitus and sleep variables were defined based on self‐report without objective measures (eg, tracked sleep hours, polysomnography, or clinical diagnosis from physicians) and are subject to misreporting and recall bias. In a population‐based study of middle‐aged adults, participants tended to overestimate their sleep duration, especially among those with shorter sleep durations. 58 Furthermore, tinnitus was defined based on a single question in this study, which restricted our ability to assess the associations stratified by the varying degrees of tinnitus severity. Additionally, participants were asked if they had ever been told by a doctor that they had a sleeping disorder so mild or undiagnosed cases may have been missed. Lastly, the sleep‐related variables were defined based on categorization from prior studies. The results may have been different based on the questions asked and their response choices. This study utilized various questionnaires on sleep characteristics, and we found generally similar associations of variables across the poor sleep indicators with tinnitus and hearing loss.
Conclusion
The current study used a nationally representative sample of US adults to investigate the association between sleep characteristics, tinnitus, and hearing loss. The objective was to explore whether hearing levels mediate the association between sleep disorders and tinnitus. Negative sleep characteristics were significantly associated with tinnitus, while no significant role of audiometry‐measured hearing as a mediator for the association between sleep variables and tinnitus was discovered. Despite limitations, these findings have future implications in understanding the potential mechanism underlying the association between sleep disorders and tinnitus, along with exploring conjunctive management options for both conditions that are difficult to treat.
Author Contributions
Matthew Awad, study conception and design, acquisition of data and analysis, drafting the manuscript, critical revisions, final approval for submission; Ibrahim Abdalla, drafting the manuscript, critical revisions, final approval for submission; Sebastian Jara, interpretation of study data, critical revisions, final approval for submission; Tina C. Huang, study conception, critical revisions, final approval for submission; Meredith E. Adams, study conception, critical revisions, final approval for submission; Janet S. Choi, study conception, study design, acquisition of data and analysis, drafting the manuscript, critical revisions, final approval for submission.
Disclosures
Competing interests
None.
Funding source
None.
This article was presented as a poster at the AAO‐HNSF 2023 Annual Meeting & OTO Experience (Poster 053); October 1‐3, 2023; Nashville, Tennessee.
References
- 1. Han BI, Lee HW, Kim TY, Lim JS, Shin KS. Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neurol. 2009;5(1):11‐19. 10.3988/jcn.2009.5.1.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Erlandsson SI, Hallberg LRM. Prediction of quality of life in patients with tinnitus. Br J Audiol. 2000;34(1):11‐19. [DOI] [PubMed] [Google Scholar]
- 3. Krog NH, Engdahl B, Tambs K. The association between tinnitus and mental health in a general population sample: results from the HUNT Study. J Psychosom Res. 2010;69(3):289‐298. [DOI] [PubMed] [Google Scholar]
- 4. Zeman F, Koller M, Langguth B, Landgrebe M, Tinnitus Research Initiative Database Study Group . Which tinnitus‐related aspects are relevant for quality of life and depression: results from a large international multicentre sample. Health Qual Life Outcomes. 2014;12:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Nondahl DM, Cruickshanks KJ, Dalton DS, et al. The impact of tinnitus on quality of life in older adults. J Am Acad Audiol. 2007;18(03):257‐266. [DOI] [PubMed] [Google Scholar]
- 6. Goldstein E, Ho CX, Hanna R, et al. Cost of care for subjective tinnitus in relation to patient satisfaction. Otolaryngol Head Neck Surg. 2015;152(3):518‐523. [DOI] [PubMed] [Google Scholar]
- 7. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. 2014;151(suppl 2):S1‐S40. [DOI] [PubMed] [Google Scholar]
- 8. Department of Veterans Affairs, V. B. A . Va.gov: Veterans Affairs. Annual Benefits Report. 2024. https://www.benefits.va.gov/REPORTS/abr/
- 9. Asnis GM, Majeed K, Henderson MA, Sylvester C, Thomas M, La Garza RD. An examination of the relationship between insomnia and tinnitus: a review and recommendations. Clin Med Insights: Psychiatry. 2018;9:1179557318781078. [Google Scholar]
- 10. Crönlein T, Langguth B, Pregler M, Kreuzer PM, Wetter TC, Schecklmann M. Insomnia in patients with chronic tinnitus: cognitive and emotional distress as moderator variables. J Psychosom Res. 2016;83:65‐68. 10.1016/j.jpsychores.2016.03.001 [DOI] [PubMed] [Google Scholar]
- 11. Richter K, Zimni M, Tomova I, et al. Insomnia associated with tinnitus and gender differences. Int J Environ Res Public Health. 2021;18(6):3209. 10.3390/ijerph18063209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hébert S, Carrier J. Sleep complaints in elderly tinnitus patients: a controlled study. Ear Hear. 2007;28(5):649‐655. [DOI] [PubMed] [Google Scholar]
- 13. Trevis KJ, McLachlan NM, Wilson SJ. A systematic review and meta‐analysis of psychological functioning in chronic tinnitus. Clin Psychol Rev. 2018;60:62‐86. [DOI] [PubMed] [Google Scholar]
- 14. Alster J, Shemesh Z, Ornan M, Attias J. Sleep disturbance associated with chronic tinnitus. Biol Psychiatry. 1993;34(1‐2):84‐90. [DOI] [PubMed] [Google Scholar]
- 15. Lai JT, Lin CY, Yan YH, Shen PH. High prevalence of obstructive sleep apnea syndrome in patients with tinnitus. J Hear Sci. 2017;43(2):722‐725. [Google Scholar]
- 16. Marks E, Hallsworth C, McKenna L. Cognitive behavioural therapy for insomnia (CBTi) as a treatment for tinnitus‐related insomnia: protocol for a randomised controlled trial. Trials. 2019;20:667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Wallhäusser‐Franke E, Schredl M, Delb W. Tinnitus and insomnia: is hyperarousal the common denominator? Sleep Med Rev. 2013;17(1):65‐74. 10.1016/j.smrv.2012.04.003 [DOI] [PubMed] [Google Scholar]
- 18. Wang C, Xu F, Chen M, et al. Association of obstructive sleep apnea‐hypopnea syndrome with hearing loss: a systematic review and meta‐analysis. Front Neurol. 2022;13:1017982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Chopra A, Jung M, Kaplan RC, et al. Sleep apnea is associated with hearing impairment: the hispanic community health study/study of Latinos. J Clin Sleep Med. 2016;12(5):719‐726. 10.5664/jcsm.5804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. İriz A, Düzlü M, Köktürk O, et al. The effect of obstructive sleep apnea syndrome on the central auditory system. Turk J Med Sci. 2018;48(1):5‐9. 10.3906/sag-1705-66 [DOI] [PubMed] [Google Scholar]
- 21. Kayabasi S, Hizli O, Yildirim G. The association between obstructive sleep apnea and hearing loss: a cross‐sectional analysis. Eur Arch Otrhinolaryngol. 2019;276:2215‐2221. [DOI] [PubMed] [Google Scholar]
- 22. Ekin S, Turan M, Arısoy A, et al. Is there a relationship between obstructive sleep apnea (OSA) and hearing loss? Med Sci Monit. 2016;22:3124‐3128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Deniz M, Çiftçi Z, Ersözlü T, Gültekin E, Alp R. The evaluation of auditory system in obstructive sleep apnea syndrome (OSAS) patients. Am J Otolaryngol. 2016;37(4):299‐303. 10.1016/j.amjoto.2016.03.004 [DOI] [PubMed] [Google Scholar]
- 24. Sheu JJ, Wu CS, Lin HC. Association between obstructive sleep apnea and sudden sensorineural hearing loss: a population‐based case‐control study. Arch Otolaryngol Head Neck Surg. 2012;138(1):55‐59. [DOI] [PubMed] [Google Scholar]
- 25. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation's updated sleep duration recommendations: final report. Sleep health. 2015;1(4):233‐243. 10.1016/j.sleh.2015.10.004 [DOI] [PubMed] [Google Scholar]
- 26. Gu X, Tang D, Xuan Y, Shen Y, Lu LQ. Association between obstructive sleep apnea symptoms and gout in US population, a cross‐sectional study. Sci Rep. 2023;13(1):10192. 10.1038/s41598-023-36755-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Centers for Disease Control . Audiometry/Tympanometry Procedures Manual; 2001. Accessed March 21, 2023. http://www.cdc.gov/nchs/data/nhanes/au.pdf
- 28. World Health Organization . Report of the informal working group on prevention of deafness and hearing impairment prevention of deafness and hearing impairment Programme planning, Geneva, 18‐21 June 1991. No. WHO/PDH/91.1. World Health Organization. 1991. [Google Scholar]
- 29. Shargorodsky J, Curhan GC, Farwell WR. Prevalence and characteristics of tinnitus among US adults. Am J Med. 2010;123(8):711‐718. 10.1016/j.amjmed.2010.02.015 [DOI] [PubMed] [Google Scholar]
- 30. Narayanan SS, Murali M, Lucas JC, Sykes KJ. Micronutrients in tinnitus: a National Health and Nutrition Examination Survey analysis. Am J Otolaryngol. 2022;43(3):103460. 10.1016/j.amjoto.2022.103460 [DOI] [PubMed] [Google Scholar]
- 31. Goshtasbi K, Abouzari M, Risbud A, et al. Tinnitus and subjective hearing loss are more common in migraine: a cross‐sectional NHANES analysis. Otol Neurotol. 2021;42(9):1329‐1333. 10.1097/MAO.0000000000003247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Shargorodsky J. Change in prevalence of hearing loss in US adolescents. JAMA. 2010;304(7):772‐778. 10.1001/jama.2010.1124 [DOI] [PubMed] [Google Scholar]
- 33. Wang Y, Lopez JMS, Bolge SC, Zhu VJ, Stang PE. Depression among people with type 2 diabetes mellitus, US National Health and Nutrition Examination Survey (NHANES), 2005‐2012. BMC Psychiatry. 2016;16(88):88. 10.1186/s12888-016-0800-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Centers for Disease Control . NHANES Analytic and Reporting Guidelines. Accessed March 21, 2023. www.cdc.gov/nchs/data/nhanes/nhanes_03_04/nhanes_analytic_guidelines_dec_2005.pdf
- 35. Li YL, Hsu YC, Lin CY, Wu JL. Sleep disturbance and psychological distress in adult patients with tinnitus. J Formos Med Assoc. 2022;121(5):995‐1002. 10.1016/j.jfma.2021.07.022 [DOI] [PubMed] [Google Scholar]
- 36. Gallo KEB, Corrêa CC, Gonçalves CGO, et al. Effect of tinnitus on sleep quality and insomnia. Int Arch Otorhinolaryngol. 2023;27(2):e197‐e202. 10.1055/s-0041-1735455 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Wakabayashi S, Saito H, Oishi N, Shinden S, Ogawa K. Effects of tinnitus treatments on sleep disorders in patients with tinnitus. Int J Audiol. 2018;57(2):110‐114. 10.1080/14992027.2017.1374565 [DOI] [PubMed] [Google Scholar]
- 38. Koo M, Hwang JH. Risk of tinnitus in patients with sleep apnea: a nationwide, population‐based, case‐control study. Laryngoscope. 2017;127(9):2171‐2175. 10.1002/lary.26323 [DOI] [PubMed] [Google Scholar]
- 39. Jiang K, Spira AP, Reed NS, Lin FR, Deal JA. Sleep characteristics and hearing loss in older adults: the national health and nutrition examination survey 2005–2006. J Gerontol Series A. 2022;77(3):632‐639. 10.1093/erona/glab214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Nakajima K, Kanda E, Hosobuchi A, Suwa K. Subclinical hearing loss, longer sleep duration, and cardiometabolic risk factors in Japanese general population. Int J Otolaryngol. 2014;2014(2014):1‐11. 10.1155/2014/218218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Asplund R. Sleepiness and sleep in elderly persons with tinnitus. Arch Gerontol Geriat. 2003;37(2):139‐145. 10.1016/S0167-4943(03)00028-1 [DOI] [PubMed] [Google Scholar]
- 42. Bhatt JM, Bhattacharyya N, Lin HW. Relationships between tinnitus and the prevalence of anxiety and depression. Laryngoscope. 2017;127(2):466‐469. 10.1002/lary.26107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Lockwood AH, Salvi RJ, Coad ML, Towsley ML, Wack DS, Murphy BW. The functional neuroanatomy of tinnitus: evidence for limbic system links and neural plasticity. Neurology. 1998;50(1):114‐120. 10.1212/WNL.50.1.114 [DOI] [PubMed] [Google Scholar]
- 44. Belli S, Belli H, Bahcebasi T, Ozcetin A, Alpay E, Ertem U. Assessment of psychopathological aspects and psychiatric comorbidities in patients affected by tinnitus. Eur Arch Otrhinolaryngol. 2008;265(3):279‐285. 10.1007/s00405-007-0440-8 [DOI] [PubMed] [Google Scholar]
- 45. Conrad I, Kleinstäuber M, Jasper K, Hiller W, Andersson G, Weise C. The role of dysfunctional cognitions in patients with chronic tinnitus. Ear Hear. 2015;36(5):e279‐e289. 10.1097/AUD.0000000000000168 [DOI] [PubMed] [Google Scholar]
- 46. Andersson G. Psychological aspects of tinnitus and the application of cognitive–behavioral therapy. Clin Psychol Rev. 2002;22(7):977‐990. [DOI] [PubMed] [Google Scholar]
- 47. Cano G, Mochizuki T, Saper CB. Neural circuitry of stress‐induced insomnia in rats. J Neurosci. 2008;28(40):10167‐10184. 10.1523/JNEUROSCI.1809-08.2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Nofzinger EA. Functional neuroimaging evidence for hyperarousal in insomnia. Am J Psychiatry. 2004;161(11):2126‐2128. 10.1176/appi.ajp.161.11.2126 [DOI] [PubMed] [Google Scholar]
- 49. Jike M, Itani O, Watanabe N, Buysse DJ, Kaneita Y. Long sleep duration and health outcomes: a systematic review, meta‐analysis and meta‐regression. Sleep Med Rev. 2018;39:25‐36. 10.1016/j.smrv.2017.06.011 [DOI] [PubMed] [Google Scholar]
- 50. Cappuccio FP, Cooper D, D'Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta‐analysis of prospective studies. Eur Heart J. 2011;32(12):1484‐1492. 10.1093/eurheartj/ehr007 [DOI] [PubMed] [Google Scholar]
- 51. Cruickshanks KJ, Nondahl DM, Dalton DS, et al. Smoking, central adiposity, and poor glycemic control increase risk of hearing impairment. J Am Geriatr Soc. 2015;63(5):918‐924. 10.1111/jgs.13401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Mitchell P, Gopinath B, McMahon CM, et al. Relationship of Type 2 diabetes to the prevalence, incidence and progression of age‐related hearing loss. Diabetic Med. 2009;26(5):483‐488. 10.1111/j.1464-5491.2009.02710.x [DOI] [PubMed] [Google Scholar]
- 53. Gates GA, Cobb JL, D'agostino RB, Wolf PA. The relation of hearing in the elderly to the presence of cardiovascular disease and cardiovascular risk factors. Arch Otolaryngol Head Neck Surg. 1993;119(2):156‐161. 10.1001/archotol.1993.01880140038006 [DOI] [PubMed] [Google Scholar]
- 54. Kasemsuk N, Chayopasakul V, Banhiran W, et al. Obstructive sleep apnea and sensorineural hearing loss: a systematic review and meta‐analysis. Otolaryngol Head Neck Surg. 2022;169:201‐209. 10.1177/01945998221120777 [DOI] [PubMed] [Google Scholar]
- 55. Lai JT, Shen PH, Lin CY, Liu CL, Liu TC. Higher prevalence and increased severity of sleep‐disordered breathing in male patients with chronic tinnitus: our experience with 173 cases. Clin Otolaryngol. 2018;43(2):722‐725. 10.1111/coa.13024 [DOI] [PubMed] [Google Scholar]
- 56. Velescu DR, Marc M, Manolescu D, Trăilă D, Oancea C. CPAP therapy on depressive and anxiety symptoms in patients with moderate to severe obstructive sleep apnea syndrome. Medicina. 2022;58(10):1402. 10.3390/medicina58101402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Povitz M, Bolo CE, Heitman SJ, Tsai WH, Wang J, James MT. Effect of treatment of obstructive sleep apnea on depressive symptoms: systematic review and meta‐analysis. PLoS Med. 2014;11(11):e1001762. 10.1371/journal.pmed.1001762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ. Self‐reported and measured sleep duration: how similar are they? Epidemiology. 2008;19(6):838‐845. 10.1097/EDE.0b013e318187a7b0 [DOI] [PMC free article] [PubMed] [Google Scholar]