

Abstract
Background:
Reduction and stabilisation of fractures at the earliest is valuable in the paediatric age groups. This novel technique focuses on stabilisation of the fracture fragments using vicryl, which has an added advantage to conventional plating and wiring. This study aimed on a novel cost-effective technique of stabilising the paediatric mandibular fracture using 2-0 resorbable polyglactin 910 suture with minimal trauma to tooth buds and bone and adequate stability.
Technique:
After raising a full-thickness mucoperiosteal flap, the fracture segments are identified and reduced. 1.6mm drill bit is used to make holes through the buccal cortex on either side of the fractured segment in an anteroposterior direction. The patency of holes is checked by passing a long 26-gauge wire. The proximal end of the wire is bent into a loop, a 2-0 resorbable polyglactin suture (vicryl) is passed through this loop and the loop is pressed in place to lock the suture. The wire with the attached suture is pulled through the distal end. Once the suture is secure in place, the 26G wire is cut, and the two ends of sutures are knotted and stabilised. The mucoperiosteal flap is then closed.
Conclusion:
A novel method of stabilisation of paediatric fracture without hampering the tooth and jaw growth, especially in the financially unstable population. 2–0 polyglactin 910 suture is cost-effective, $2 US, compared to resorbable plates costing about $150 US, and easily available. Polyglactin 910 takes 40–60 days for resorption, and half-life tensile strength is 2 weeks; thus, it gives adequate stability and time for callus formation and does not damage the tooth buds or bone by cutting through them.
Keywords: Growth phase, paediatric mandibular fracture, polyglactin 910 suture, tooth bud
BACKGROUND
Paediatric trauma is a challenging sector pertaining to their diminutive morphology andimmature dental and skeletal components, which make them extremely difficult to treat.[1] Reduction and stabilisation of fractures at the earliest is valuable in the paediatric age groups. In a developing country like India, people defer from treatment mainly due to financial instability. We propose a novel technique of reducing and stabilising the paediatric mandibular fractures using 2-0 polyglactin 910 suture. The technique is an effective method in children as it is resorbable with minimal trauma to tooth buds and bone, achieves adequate stability and is cost-effective.
The Ethical Committee approval and informed consent were taken before the surgery.
CLINICAL TECHNIQUE
After aseptic preparation of the operation site, local anaesthetic solution (2% lignocaine with 1:80,000 adrenaline) is administered at the fracture site. After raising a full-thickness mucoperiosteal flap, the fracture segments are identified and reduced. 1.6mm drill bit is used to make holes through the buccal cortex on either side of the fractured segment in an anteroposterior direction. The patency of holes is checked by passing a long 26-gauge wire [Figure 1]. The proximal end of the wire is bent into a loop, a 2–0 resorbable polyglactin suture (vicryl) is passed through this loop and the loop is pressed in place to lock the suture. The wire with the attached suture is pulled through the distal end [Figure 2]. Once the suture is secure in place, the 26-gauge wire is cut, and the two ends of sutures are knotted and stabilised [Figure 3]. The mucoperiosteal flap is then closed.
Figure 1.

Twenty six gauge stainless steel wire passed through the drill holes
Figure 2.
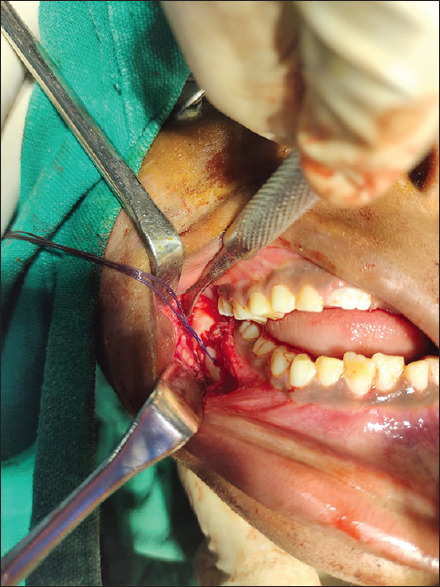
Polyglactin 910 suture passed through the drill holes
Figure 3.

Reduced fracture fragments and knotted suture in situ
DISCUSSION
The use of circum-mandibular wiring, miniplates and bioresorbable plates has their own cons of cutting through the immature bone, damage to the tooth bud and migration of the plate during the growth of the child and expensiveness, respectively.[2] 2-0 polyglactin 910 suture is cost-effective, $2 US, compared to resorbable plates costing about $150 US and easily available. Polyglactin 910 takes 40–60 days for resorption, and half-life tensile strength is 2 weeks; thus, it gives adequate stability and time for callus formation and does not damage the tooth buds or bone by cutting through them.[3] There is no material migration in the growth phase; thus, an unhampered jaw growth is made possible, and giving it an advantage over other techniques with the larger affordability to the population. This technique does have a limitation of being time-consuming in the posterior mandible due to less accessibility.
CLINICAL SIGNIFICANCE
This novel method is useful for the financially unstable population who refrain from treatment due to lack of money. Due to its low cost, it will benefit a larger sector of society. It is minimally invasive and resorbable, thus making it biocompatible without any damage to the tooth or bone and unhampered jaw growth.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Bhutia DP, Singh G, Mohammed S, Ram H, Gamit J, Howlader D. Prevalence and etiology of pediatric maxillofacial injuries: A unicenter-based retrospective study. Int J Clin Pediatr Dent. 2019;12:528–31. doi: 10.5005/jp-journals-10005-1687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lim HY, Jung CH, Kim SY, Cho JY, Ryu JY, Kim HM. Comparison of resorbable plates and titanium plates for fixation stability of combined mandibular symphysis and angle fractures. J Korean Assoc Oral Maxillofac Surg. 2014;40:285–90. doi: 10.5125/jkaoms.2014.40.6.285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Müller DA, Snedeker JG, Meyer DC. Two-month longitudinal study of mechanical properties of absorbable sutures used in orthopedic surgery. J Orthop Surg Res. 2016;11:111. doi: 10.1186/s13018-016-0451-5. [DOI] [PMC free article] [PubMed] [Google Scholar]