

Abstract
Objective:
Parental leave and breastfeeding breaks influence the ability to initiate and continue breastfeeding. We investigated how eligibility criteria in the Family and Medical Leave Act (FMLA) and Affordable Care Act (ACA) affect access to unpaid parental leave and breastfeeding breaks and assessed affordability and alternative policy models.
Methods:
We used family income data to assess the affordability of unpaid leave by race and ethnicity. We used 2017-2018 US Current Population Survey data to determine the percentage of private sector workers aged 18-44 years who met the minimum hour (1250 hours of work during a 12-month period), tenure (12 months), and firm size (≥50 employees) requirements of FMLA and ACA. We analyzed eligibility by gender, race and ethnicity, and age. We also examined parental leave and breastfeeding break policies in 193 countries.
Results:
Most Latinx (66.9%), Black (60.2%), and White (55.3%) workers were ineligible and/or unlikely to be able to afford to take unpaid FMLA leave. Of 69 534 workers, more women (16.9%) than men (10.3%) did not meet the minimum hour requirement. Minimum tenure excluded 23.7% of all workers and 42.2% of women aged 18-24 years. Minimum firm size excluded 30.3% of all workers and 37.7% of Latinx workers. Of 27 520 women, 28.8% (including 32.9% of Latina women) were excluded from ACA breastfeeding breaks because of firm size. Nearly all other countries guaranteed mothers paid leave regardless of firm size or minimum hours and guaranteed ≥6 months of paid leave or breastfeeding breaks.
Conclusions:
Adopting a comprehensive, inclusive paid parental leave policy and closing gaps in breastfeeding break legislation would remove work-related barriers to breastfeeding; reduce racial, ethnic, and gender inequities; and align US national policies with global norms.
Keywords: breastfeeding, paid leave, infant health, racial and ethnic inequalities, gender inequalities
Breastfeeding has long been identified as one of the most effective infant health interventions. Both the World Health Organization and the American Academy of Pediatrics recommend 6 months of exclusive breastfeeding and continued breastfeeding for longer.1,2 In the short term, breastfeeding significantly reduces infants’ risks of respiratory infections, diarrhea, and postneonatal mortality.3-6 In the long term, evidence suggests that breastfed children have lower rates of overweight and diabetes than children who were not breastfed or were breastfed for a short duration. 3 Breastfeeding also reduces mothers’ long-term risks of breast cancer and potentially lowers risks of ovarian cancer, heart disease, and osteoporosis.4,7
Nevertheless, among babies born in the United States in 2018, just 25.8% were exclusively breastfed for at least 6 months. 8 Although many women would like to breastfeed longer, the need to return to work, coupled with unsupportive work environments, often impedes breastfeeding.9-11 One survey of low-income employed women found that their odds of discontinuing breastfeeding were 32% greater during their first month back at work than a mother without paid employment. 11 Although employment is only 1 factor affecting breastfeeding practices, the effect of employment is significant.11-13
Two policies can meaningfully support women’s ability to breastfeed while maintaining employment: parental leave and breastfeeding breaks. Longer paid leave after childbirth increases breastfeeding rates.12-15 For example, California’s introduction of a state-level paid parental leave policy increased rates of exclusive breastfeeding by 3 to 5 percentage points. 16 Fathers’ use of parental leave is also associated with increased breastfeeding. 17 Breastfeeding breaks—the provision of adequate time and a private location to express breastmilk at work—represent a critical complementary policy, with demonstrated effects on breastfeeding duration. 18
In the United States, 2 national policies govern the availability of parental leave and breastfeeding breaks for private sector workers: the Family and Medical Leave Act (FMLA), 19 which guarantees 12 weeks of unpaid parental leave, and the Affordable Care Act (ACA), 20 which amended the Fair Labor Standards Act (FLSA) 21 to guarantee women “reasonable break time” to express milk for 1 year after birth. Eligibility criteria in both policies have shaped their coverage. The FMLA limits eligibility based on the employer’s number of workers, the worker’s length of employment, and the worker’s annual hours of work. The ACA/FLSA, alongside coverage restrictions based on income and occupation, exempts businesses with <50 employees if providing breaks would create an “undue hardship.”20,21
We investigated whether these policy features contributed to disparities in access to parental leave and breastfeeding breaks among racial and ethnic, gender, and age groups and determined the overall coverage gaps. We also analyzed comparative policy data from 193 countries to understand whether more comprehensive approaches are feasible.
Methods
Data and Sample
To quantify who was excluded by each policy eligibility criterion in the FMLA and ACA/FLSA, we used data from the US Current Population Survey (CPS) Annual Social and Economic Supplement, a nationally representative survey of the noninstitutionalized US population. 22 We pooled data from 2017 and 2018, which was the most recent period in which the CPS captured firm size data in a way that made it possible to identify workers employed by firms with ≥50 employees; this time frame also allowed us to analyze 2 years of typical employment patterns before the effects of COVID-19.
To assess likely affordability of unpaid leave, we used annual family income and family size to calculate income relative to 100%, 150%, and 200% of the federal poverty level. To determine exclusion based on FMLA unpaid parental leave eligibility criteria, we limited our analysis to adults aged 18-44 years, because women in this age group account for 98.6% of the annual births in the United States, 23 and adults who reported working at least 15 hours per week for a private employer (N = 69 534).
To determine exclusion from breastfeeding breaks based on ACA policies, we analyzed women aged 18-44 years who were otherwise covered by the FLSA. We considered a woman to perform executive, administrative, and professional duties and, thus, be excluded if she reported working in a “management” occupation (2010 US Census occupation codes 0010-0043). 24 We considered a woman to earn above the minimum threshold for FLSA coverage if her reported earnings exceeded $455 per week or $23 660 per year in 2017 and 2018. We limited the sample to women working at least 15 hours per week (N = 27 520).
For both the FMLA and FLSA/ACA analyses, we excluded public sector workers, who are often covered by separate legislation. We also excluded the self-employed, whom neither law was designed to cover.
This study meets both university and federal human subjects guidelines. Consistent with federal guidelines, UCLA has determined that studies “that only include interactions involving . . . survey procedures” and that record information in “such a manner that the identity of the human subjects cannot readily be ascertained, directly or through identifiers linked to the subjects” are exempt from institutional review board review. 25
Demographic Characteristics
For gender, survey data reported only a binary measure indicating male or female. Survey respondents self-identified race and ethnicity. We coded respondents who indicated “Spanish, Hispanic, or Latino” as Latinx regardless of the race(s) they self-identified. Among those who did not self-identify as Latinx, we coded respondents as Black if they indicated “Black” and as Asian if they indicated “Asian.” Because of small sample sizes, we grouped Indigenous respondents who indicated either “American Indian/Aleut/Eskimo” or “Native Hawaiian/Pacific Islander.” We coded respondents as multiracial if they identified as multiple races. We constructed 3 age groups: 18-24, 25-34, and 35-44 years of age.
Employment Characteristics
For our analysis of access to unpaid parental leave, we examined the 3 employee eligibility requirements in the FMLA: (1) 1250 hours of work for a single employer during the 12 months preceding leave, (2) 12 months of tenure with the same employer, and (3) working at a location where the employer has ≥50 employees within 75 miles. 26
To estimate whether someone worked at least 1250 hours in the past 12 months, we multiplied total weeks worked at any job during the calendar year prior to the survey by usual weekly hours on the main job. This measure provides an upper-bound estimate of coverage because some individuals coded as eligible may have had multiple jobs but insufficient hours at their main job.
To estimate whether someone worked at least 12 months, we used the total weeks worked at any job in the preceding year and coded as eligible those with ≥50 weeks who reported having only 1 employer during that survey year.
To estimate employee eligibility based on firm size, we used the number of employees working for the respondent’s employer across all locations. This measure also provides an upper-bound estimate of coverage because the FMLA excludes individuals working for large businesses if their worksite has <50 employees within a 75-mile radius.
For our analysis of access to breastfeeding breaks, we examined the potential effects of the ACA/FLSA “undue hardship” exemption of employers with <50 employees. 27 We estimated firm size following the same methodology used for FMLA.
Parental Leave and Breastfeeding Breaks in Other Countries
To understand the approaches to parental leave and breastfeeding breaks at work in other countries, we assessed the national paid leave policies as of January 2022 in all 193 United Nations member countries. We captured data on paid leave reserved specifically for mothers, gender-neutral paid leave, and breastfeeding breaks available to parents in the private sector. Many countries, including the United States, treat public and private sector workers differently in labor legislation.
A multilingual research team reviewed and systematically assessed original labor-, social security–, and sector-specific legislation and global information on social security systems for each country by using a common coding framework. We coded countries with federal systems as having paid leave for mothers if they had a national policy covering the private sector.
Statistical Analysis
Using a pooled sample of 2017 and 2018 data from the CPS Annual Social and Economic Supplement, we calculated the percentage of workers in each racial and ethnic, gender, and age group meeting each eligibility requirement described previously, as well as intersectional disparities across race and ethnicity and gender. 28 To calculate the significance level of differences in percentages across race and ethnicity, gender, and age groups, we used logistic regressions. We considered P < .05 to be significant. We used survey sampling weights in all analyses. We used Stata version 14.2 (StataCorp LLC) for our analyses.
Results
Overall Coverage Gaps in FMLA Parental Leave
When we accounted for all 3 FMLA eligibility requirements for parental leave (minimum hour, minimum tenure, and minimum firm size), 51.1% of women aged 18-44 years and 48.3% of men aged 18-44 years were excluded. The rates of exclusion were significantly higher among women and men aged 18-24 years (67.9% and 64.2%, respectively) than among women and men aged 25-34 years (48.6% and 46.6%, respectively; P < .001 for both) and women and men aged 35-44 years (43.9% and 41.8%, respectively; P < .001 for both). Although we found little difference in exclusion rates by race and ethnicity when all eligibility criteria were considered, Black and Latinx families were the least likely to be able to afford unpaid parental leave compared with other racial and ethnic groups. Black and Latinx families were twice as likely as White families to have an annual family income <200% of the federal poverty level (P < .001). When we accounted for all 3 FMLA eligibility requirements, 60.2% of Black workers, 66.9% of Latinx workers, and 55.3% of White workers were either ineligible for unpaid leave and/or unlikely to be able to afford to take it based on annual family income levels before leave (P < .001) (Figure 1).
Figure 1.

Estimated percentage of women without access to parental leave because of Family Medical Leave Act 19 eligibility requirements and/or annual family income <200% of the federal poverty level, according to US Current Population Survey 2017 and 2018 data. Data source: Flood et al. 22
FMLA Parental Leave Eligibility and Minimum Hour Requirements
The FMLA’s 1250-hour requirement excluded nearly 1 in 7 workers, with a higher share of women than men (16.9% vs 10.3%; P < .001). Women aged 25-34 years were nearly twice as likely as men aged 25-34 years to be ineligible for FMLA parental leave because of work hours (12.9% vs 7.4%; P < .001), with women aged 18-24 years experiencing higher rates of exclusion (34.9%) than women aged 25-34 years (12.9%) and 35-44 years (11.1%) (P < .001) (Figure 2).
Figure 2.
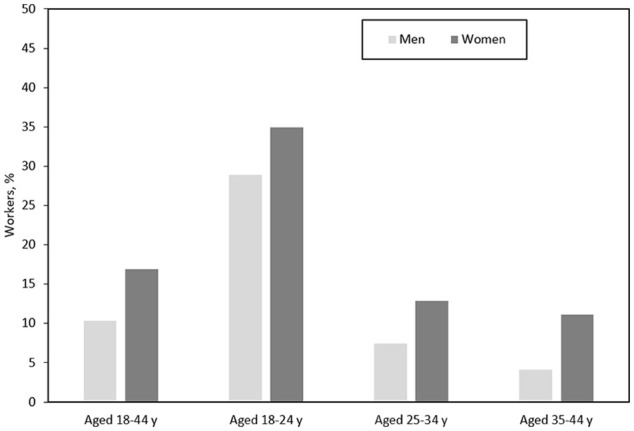
Estimated percentage of workers excluded by the Family Medical Leave Act 19 1250-hour requirement, by sex and age, according to US Current Population Survey 2017 and 2018 data. Data source: Flood et al. 22
Exclusions also varied across race and ethnicity among age groups. Among women aged 25-34 years, Latina women had the highest rate of exclusion (14.5%; P = .04 compared with White women) because of part-time employment. By race and ethnicity among women aged 18-24 years, Asian women were the most likely to be excluded by part-time employment (P = .004) (Figure 3).
Figure 3.

Estimated percentage of women excluded by Family Medical Leave Act 19 1250-hour requirement, by race and ethnicity and age, according to US Current Population Survey 2017 and 2018 data. Data source: Flood et al. 22
FMLA Parental Leave Eligibility and Minimum Tenure Requirements
The FMLA’s 12-month tenure requirement excluded nearly one-fourth (23.7%) of all workers aged 18-44 years. Women were more likely than men to be excluded (25.6% vs 22.1%; P < .001); women aged 18-24 years had a higher level of exclusion (42.2%) than women aged 25-34 (23.5%) and 35-44 (18.2%; P < .001) years (Figure 4). Among women aged 18-24 years, White women (44.6%) were significantly more likely than Black (38.3%; P < .001) or Latina (37.8%; P < .001) women to be excluded from eligibility.
Figure 4.
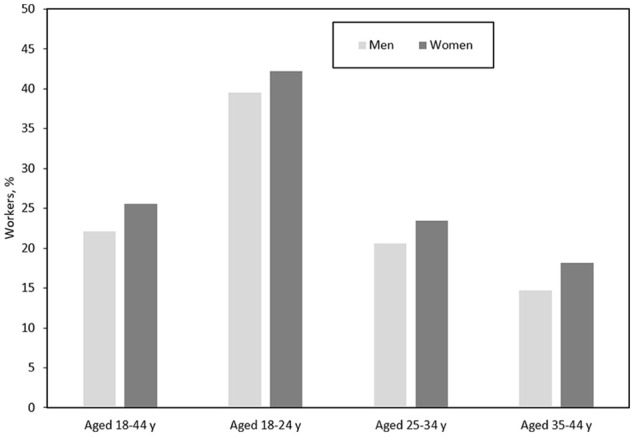
Estimated percentage of workers excluded by Family Medical Leave Act 19 12-month tenure requirement, by sex and age, according to US Current Population Survey 2017 and 2018 data. Data source: Flood et al. 22
FMLA Parental Leave Eligibility and Minimum Firm Size Requirements
The FMLA’s minimum firm size requirement excluded 30.3% of workers aged 18-44 years; rates were similar across age and gender groups. However, compared with White workers, Latinx workers were more likely to be excluded from parental leave because of firm size (37.7%; P < .001) and Black workers were the least likely to be excluded (21.2%; P < .001). Similarly, among women aged 25-34 years, Black women had significantly lower rates of exclusion than White, Latina, and Asian women (P < .001) and multiracial women (P = .03) (Figure 5).
Figure 5.

Estimated percentage of women excluded by Family Medical Leave Act 19 employer size requirement, by race and ethnicity and age, according to US Current Population Survey 2017 and 2018 data. Data source: Flood et al. 22
ACA Breastfeeding Breaks Eligibility and Minimum Firm Size Requirements
The ACA minimum firm size exemption excluded 28.8% of women who were covered by FLSA provisions. We found that differences were small across age groups but marked across racial and ethnic groups. Overall, Latina women had the highest rates of exclusion compared with White women (32.9% vs 30.3%; P = .005). Across all age groups, Black women were less likely than White, Latina, or Asian women to be excluded (P < .001 for all comparisons). Differences between Black women and multiracial or Indigenous women were significant for some comparisons.
Paid Leave and Breastfeeding Breaks in Other Countries
Of 193 countries analyzed, 179 countries guaranteed paid options to support breastfeeding for at least 12 weeks either by guaranteeing paid leave to mothers of infants or by providing paid breastfeeding breaks at work. The United States is the only country worldwide to solely guarantee unpaid parental leave and 1 of only 4 countries—joining Cote d’Ivoire, New Zealand, and Japan—to make breastfeeding breaks unpaid. Of 193 countries, 146 had policies that guaranteed paid options to support breastfeeding for at least 6 months. Among those countries that guaranteed any duration of paid leave (n = 186), only 1 had a broad firm size exclusion higher than 5 employees (India excluded workers at businesses with <10 employees; Bangladesh more narrowly excluded agricultural workers at farms with <10 employees). Furthermore, 90% of countries (172 of 191 for which data were available) guaranteed paid leave for mothers without requiring mothers to meet an explicit minimum hour requirement.
Discussion
Supporting mothers to initiate and continue breastfeeding for the duration recommended by public health experts requires policies that enable parents to take leave from work after a child is born and provide mothers with time and space to express milk after they return to their jobs. However, our analysis found that the unpaid leave provided to US workers through the FMLA is inaccessible to an estimated 51.1% of women as a result of eligibility requirements; even more lack access when factoring in affordability.
Each eligibility requirement excluded a sizeable proportion of workers. Nearly one-fourth of workers aged 18-44 years were ineligible for FMLA parental leave because they had not worked for the same employer for at least 12 months. The minimum employer size rules had an even larger effect, excluding nearly one-third of workers aged 18-44 years. Similarly, nearly 29% of women in this age group, who otherwise met FLSA requirements, did not qualify for breastfeeding breaks because of their employer’s size. Among workers aged 18-44 years, 14% were ineligible for FMLA parental leave due to inadequate work hours.
Specific criteria had disproportionate effects across race and ethnicity, gender, and age groups. The FMLA’s minimum hour requirements resulted in pronounced gender disparities in coverage; 17% of women aged 18-44 years and 10% of men did not qualify for parental leave because of insufficient work hours, reflecting the broader effects of restrictive gender norms on women’s overrepresentation in part-time work. Minimum firm size requirements disproportionately affected Latinx workers; across age groups, 38% of Latinx workers were ineligible for FMLA leave because of their employer’s size. Minimum tenure and hour requirements also disproportionately affected young mothers across race and ethnicity groups, excluding 34.9% and 42.2% of women aged 18-24 years, respectively.
These gaps and inequalities are particularly troubling given that the United States falls well below established breastfeeding targets, especially with regard to duration. 8 Moreover, workplace policies on breastfeeding may further exacerbate disparities related to race, ethnicity, and age. At 3 months, about 50% of White and Asian infants but only 42.6% of Latinx infants and only 39.3% of Black infants are breastfeeding. Breastfeeding rates decline further at 6 months, with just 33.3% of Asian infants, 28.8% of White infants, 23.3% of Latinx infants, and 19.8% of Black infants exclusively breastfeeding. 29 Younger mothers (aged 20-29 years) overall are less likely to breastfeed than those aged ≥30 years. 28
A range of factors can shape breastfeeding intention, initiation, and duration, as well as disparities in breastfeeding by race and ethnicity, including a family history of breastfeeding and the availability of family and community support. 30 Other health and socioeconomic factors driven by structural racism—including racial and ethnic disparities in income, food security, marital status, age at birth, and the incidence of premature birth—also contribute to differences in breastfeeding rates.31,32
Nonetheless, substantial evidence suggests that working conditions influence breastfeeding rates overall12-18; thus, racial and ethnic disparities in working conditions are likely to contribute to racial and ethnic disparities in breastfeeding practices. Studies of breastfeeding among Latina mothers highlighted this potential relationship; despite high breastfeeding intentions, Latina mothers reported low average duration, partly due to work environments that made pumping challenging. 33 Although White and Latina mothers initiate breastfeeding at similar rates, Latina mothers have far less employer-provided leave 34 and are significantly less likely to breastfeed for 3 and 6 months in practice than White mothers. 29 Our findings demonstrated that Latina mothers are also disproportionately excluded from unpaid FMLA leave and the ACA’s breastfeeding breaks, which likely further contributes to early cessation of breastfeeding.
Economic necessity compels many women to return to work shortly after childbirth, creating a substantial barrier to establishing breastfeeding. Indeed, while breastfeeding is one critical determinant of child health, so too is income. However, despite ample evidence that the birth of a child increases a household’s risk of poverty and income loss,35,36 the United States stands alone in guaranteeing private sector workers no paid leave that can be used after childbirth. This policy gap broadly undermines infant health and significantly worsens inequalities; unpaid leave is only a benefit for those who can afford to take it and requires having adequate income and savings before leave. Black and Latinx families are twice as likely as White families to be living near the federal poverty level, and our findings underscored the consequences of these underlying inequalities: 2 in 3 Latinx workers and 3 in 5 Black workers, compared with slightly more than half of White workers, are either ineligible for FMLA leave or cannot afford to take it. This finding is consistent with previous data showing that only 36% of Black parents and 26% of Latinx parents both qualify for and can afford to take FMLA leave. 37 Moreover, these percentages are likely underestimates of the racial inequalities in affordability, because disparities in wealth by race and ethnicity are even larger than income disparities: the median net worth of White families is nearly 8 times that of Black families and 5 times that of Latinx families, and net worth is lowest for families headed by workers aged <35 years. 38 Furthermore, racial and ethnic and socioeconomic disparities also persist in access to employer-provided leave. Just 12% of private sector workers in the bottom quarter of the income distribution, compared with 37% in the top quarter, have paid family leave. 38
Our analysis of globally comparative policy data demonstrated that stronger, more inclusive policies are feasible. Among the 193 countries analyzed, only 13 countries did not provide paid options to facilitate breastfeeding for at least 12 weeks, and the vast majority guaranteed at least 6 months of paid leave or 6 months of paid breastfeeding breaks at work. Among countries that provided paid parental leave, nearly all covered workers without linking eligibility to a minimum number of work hours and only 1 broadly limited eligibility based on firm size. Moreover, previous research of paid medical leave found that other countries typically applied less stringent tenure requirements than the FMLA, for example, by conditioning eligibility on shorter tenure periods or on social security contributions rather than tenure in a single job, thereby allowing time employed across multiple jobs to satisfy any minimum threshold.39,40
Limitations
This study had several limitations. First, because we focused on policies with national coverage, we did not analyze paid leave and breastfeeding break policies enacted by states and localities. Although these policies are not substitutes for strong national legislation, future research examining the extent to which they fill gaps and/or reproduce inequalities would be valuable. Second, although the examination of FMLA and ACA/FLSA leave coverage among individual racial and ethnic groups is critical, existing data sources include only a small sample of certain populations. Having a larger pool of survey respondents from racial and ethnic minority groups whose overall population is smaller, such as American Indian and Alaska Native people, would enable more precise analysis of coverage disparities and additional analyses of intersectional inequalities. Third, because different groups of self-identified multiracial individuals have different experiences of discrimination, a disaggregated analysis of the “multiracial” respondent category would have been preferable, although this analysis was infeasible because of small sample sizes. Finally, because the FMLA and ACA/FLSA exclude self-employed adults from coverage, our estimates may represent a lower bound of the true portion of the workforce lacking breastfeeding breaks and/or paid family leave.
Conclusions
Improving child health requires supporting more mothers to initiate and continue breastfeeding. Yet current gaps and inequalities in US policies exacerbate the documented barriers to breastfeeding that women face upon return to work. In particular, the United States’ failure to adopt a paid parental leave policy covering all parents in all jobs, alongside its needless exemption of a large proportion of employers from breastfeeding break legislation, undermines families’ efforts to provide optimal nutrition for their infants, while more broadly threatening a wide range of public health goals. To better support all families to meet their children’s nutritional needs and to reduce racial, ethnic, and socioeconomic health disparities, the United States must address these gaps.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are deeply grateful to the Blue Shield of California Foundation for its support to examine paid leave in the United States and the relationship between policy choices and racial and ethnic disparities in access, and to the William and Flora Hewlett Foundation for its support in examining global approaches to expanding social protection for caregiving to accelerate women’s economic empowerment.
ORCID iD: Aleta Sprague, JD  https://orcid.org/0000-0002-5794-1851
https://orcid.org/0000-0002-5794-1851
References
- 1. Meek JY, Noble L. Policy statement: breastfeeding and the use of human milk. Pediatrics. 2022;150(1):e2022057988. doi: 10.1542/peds.2022-057988 [DOI] [PubMed] [Google Scholar]
- 2. World Health Organization. Breastfeeding. Accessed May 5, 2022. https://www.who.int/health-topics/breastfeeding#tab=tab_2
- 3. Victora CG, Bahl R, Barros AJ, et al. ; Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475-490. doi: 10.1016/S0140-6736(15)01024-7 [DOI] [PubMed] [Google Scholar]
- 4. Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep). 2007;153:1-186. [PMC free article] [PubMed] [Google Scholar]
- 5. Chen A, Rogan WJ. Breastfeeding and the risk of postneonatal death in the United States. Pediatrics. 2004;113(5):e435-e439. doi: 10.1542/peds.113.5.e435 [DOI] [PubMed] [Google Scholar]
- 6. Bartick MC, Schwarz EB, Green BD, et al. Suboptimal breastfeeding in the United States: maternal and pediatric health outcomes and costs. Matern Child Nutr. 2017;13(1):e12366. doi: 10.1111/mcn.12366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Schwarz EB, Ray RM, Stuebe AM, et al. Duration of lactation and risk factors for maternal cardiovascular disease. Obstet Gynecol. 2009;113(5):974-982. doi: 10.1097/01.AOG.0000346884.67796.ca [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2030: infants. Accessed July 15, 2022. https://health.gov/healthypeople/objectives-and-data/browse-objectives/infants
- 9. Ahluwalia IB, Morrow B, Hsia J. Why do women stop breastfeeding? Findings from the Pregnancy Risk Assessment and Monitoring System. Pediatrics. 2005;116(6):1408-1412. doi: 10.1542/peds.2005-001 [DOI] [PubMed] [Google Scholar]
- 10. Murtagh L, Moulton AD. Working mothers, breastfeeding, and the law. Am J Public Health. 2011;101(2):217-223. doi: 10.2105/AJPH.2009.185280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kimbro RT. On-the-job moms: work and breastfeeding initiation and duration for a sample of low-income women. Matern Child Health J. 2006;10(1):19-26. doi: 10.1007/s10995-005-0058-7 [DOI] [PubMed] [Google Scholar]
- 12. Baker M, Milligan K. Maternal employment, breastfeeding, and health: evidence from maternity leave mandates. J Health Econ. 2008;27(4):871-887. doi: 10.1016/j.jhealeco.2008.02.006 [DOI] [PubMed] [Google Scholar]
- 13. Chuang CH, Chang PJ, Chen YC, et al. Maternal return to work and breastfeeding: a population-based cohort study. Int J Nurs Stud. 2010;47(4):461-474. doi: 10.1016/j.ijnurstu.2009.09.003 [DOI] [PubMed] [Google Scholar]
- 14. Kottwitz A, Oppermann A, Spiess CK. Parental leave benefits and breastfeeding in Germany: effects of the 2007 reform. Rev Econ Household. 2016;14:859-890. doi: 10.1007/s11150-015-9299-4 [DOI] [Google Scholar]
- 15. Ogbuanu C, Glover S, Probst J, Liu J, Hussey J. The effect of maternity leave length and time of return to work on breastfeeding. Pediatrics. 2011;127(6):e1414-1427. doi: 10.1542/peds.2010-0459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Huang R, Yang M. Paid maternity leave and breastfeeding practice before and after California’s implementation of the nation’s first paid family leave program. Econ Hum Biol. 2015;16:45-59. doi: 10.1016/j.ehb.2013.12.009 [DOI] [PubMed] [Google Scholar]
- 17. Flacking R, Dykes F, Ewald U. The influence of fathers’ socioeconomic status and paternity leave on breastfeeding duration: a population-based cohort study. Scand J Public Health. 2010;38(4):337-343. doi: 10.1177/1403494810362002 [DOI] [PubMed] [Google Scholar]
- 18. Dinour LM, Szaro JM. Employer-based programs to support breastfeeding among working mothers: a systematic review. Breastfeed Med. 2017;12:131-141. doi: 10.1089/bfm.2016.0182 [DOI] [PubMed] [Google Scholar]
- 19. Family and Medical Leave Act of 1993, Pub L No 103-3 (1993). [Google Scholar]
- 20. Patient Protection and Affordable Care Act of 2010, Pub L No 111-148 (2010). [Google Scholar]
- 21. Fair Labor Standards Act of 1938, Pub L No 75-718 (1938). [Google Scholar]
- 22. Flood S, King M, Rodgers R, Ruggles S, Warren JR. Integrated public use microdata series (IPUMS), Current Population Survey (CPS). Version 8.0. 2020. Accessed January 11, 2021. https://www.ipums.org/projects/ipums-cps/d030.v8.0
- 23. Osterman M, Hamilton B, Martin JA, Driscoll AK, Valenzuela CP. Births: final data for 2020. Natl Vital Stat Rep. 2021;70(17):1-50. [PubMed] [Google Scholar]
- 24. US Department of Labor, Bureau of Labor Statistics. 2010 Census Occupational Classification. Revised 2016. Accessed November 14, 2022. https://www.bls.gov/cps/cenocc2010.htm
- 25. University of California Los Angeles Research Administration, Human Research Protection Program. Guidance and procedure: level of review—certification of exemption from IRB review (August 19, 2022). Accessed November 19, 2022. https://ora.research.ucla.edu/OHRPP/Documents/Policy/4/Exemption.pdf
- 26. US Department of Labor, Wage and Hour Division. Fact sheet #28: the Family and Medical Leave Act. Revised 2012. Accessed May 5, 2022. https://www.dol.gov/sites/dolgov/files/WHD/legacy/files/whdfs28.pdf
- 27. US Department of Labor, Wage and Hours Division. Fact sheet #73: break time for nursing mothers under the FLSA. Revised April 2018. Accessed May 5, 2022. https://www.dol.gov/agencies/whd/fact-sheets/73-flsa-break-time-nursing-mothers
- 28. Crenshaw KW. Demarginalizing the intersection of race and sex: a Black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ Chicago Legal Forum. 1989;140:139-167. [Google Scholar]
- 29. Centers for Disease Control and Prevention. Rates of any and exclusive breastfeeding by sociodemographics among children born in 2018 (percentage ± half 95% confidence interval). Accessed May 5, 2022. https://www.cdc.gov/breastfeeding/data/nis_data/rates-any-exclusive-bf-socio-dem-2018.html
- 30. McKinney CO, Hahn-Holbrook J, Chase-Lansdale PL, et al. Racial and ethnic differences in breastfeeding. Pediatrics. 2016;138(2):e20152388. doi: 10.1542/peds.2015-2388 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Gallo S, Kogan K, Kitsantas P. Racial and ethnic differences in reasons for breastfeeding cessation among women participating in the Special Supplemental Nutrition Program for Women, Infants, and Children. J Midwifery Womens Health. 2019;64(6):725-733. doi: 10.1111/jmwh.13031 [DOI] [PubMed] [Google Scholar]
- 32. Segura-Pérez S, Hromi-Fiedler A, Adnew M, Nyhan K, Pérez-Escamilla R. Impact of breastfeeding interventions among United States minority women on breastfeeding outcomes: a systematic review. Int J Equity Health. 2021;20(1):72. doi: 10.1186/s12939-021-01388-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Hohl S, Thompson B, Escareño M, Duggan C. Cultural norms in conflict: breastfeeding among Hispanic immigrants in rural Washington State. Matern Child Health J. 2016;20(7):1549-1557. doi: 10.1007/s10995-016-1954-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bartel AP, Kim S, Nam J, Rossin-Slater M, Ruhm C, Waldfogel J. Racial and ethnic disparities in access to and use of paid family and medical leave: evidence from four nationally representative datasets. Monthly Lab Rev. 2019;142:1. [Google Scholar]
- 35. Sandler D, Szembrot N. Maternal Labor Dynamics: Participation, Earnings, and Employer Changes. Discussion paper no. 19-33. US Census Bureau, Center for Economic Studies; 2019. [Google Scholar]
- 36. Waldfogel J. International policies toward parental leave and child care. Future Child. 2001;11(1):99-111. doi: 10.2307/1602812 [DOI] [PubMed] [Google Scholar]
- 37. Joshi P, Baldiga M, Huber R, Acevedo-Garcia D. The Family and Medical Leave Act: Policy Equity Assessment. Institute for Child, Youth & Family Policy, Heller School for Social Policy & Management at Brandeis University; 2020. [Google Scholar]
- 38. Board of Governors of the Federal Reserve System. Survey of Consumer Finances, 1989-2019. Accessed July 15, 2022. https://www.federalreserve.gov/econres/scf/dataviz/scf/table/#series:Net_Worth;demographic:racecl4;population:all;units:median;range:1989,2019
- 39. US Bureau of Labor Statistics. Employee benefits in the United States: summary. September 23, 2001. Accessed May 5, 2022. https://www.bls.gov/news.release/ebs2.nr0.htm
- 40. Heymann J, Sprague A, Earle A, McCormack M, Waisath W, Raub A. US sick leave in global context: US eligibility rules widen inequalities despite readily available solutions. Health Aff (Millwood). 2021;40(9):1501-1509. doi: 10.1377/hlthaff.2021.00731 [DOI] [PubMed] [Google Scholar]