

Abstract
Background:
The success of anterior cruciate ligament (ACL) reconstruction relies on the accurate replication of the native ACL anatomy, including attachment shapes. The tibial attachment of the ACL exhibits significant shape variations with elliptical, C, and triangular shapes, highlighting the need for objective classification methods and additional information to identify individual anatomic variations.
Hypothesis:
The location of the attachment of the anterior horn of the lateral meniscus (AHLM) may determine the shape of the ACL attachment.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The study used 25 knees from 17 Japanese cadavers for macroscopic anatomic examination and quantitative analysis. The shape of the ACL attachment was quantified using principal component analysis with elliptical Fourier descriptors, whereas the AHLM location was quantified by measuring its mediolateral and anteroposterior positions on the superior surface of the tibia. Reliability was assessed statistically.
Results:
The shape of the tibial attachment of the ACL varied among individuals and was classified as elliptical, C-shaped, or triangular. Scatterplots of the principal components of the ACL attachment shape showed overlapping regions of elliptical, C-shaped, and triangular ACL attachments, indicating that a C-shaped attachment is intermediate between elliptical and triangular attachments. The location of the AHLM attachment also varied, with areas in the anterolateral, anteromedial, or posteromedial region. The ACL shape and AHLM location were related, with elliptical, C-shaped, and triangular ACL attachments corresponding to anterolateral, anteromedial, and posteromedial AHLM attachments, respectively.
Conclusion:
The AHLM attachment location influences the shape of the ACL attachment. Information on the location of the AHLM attachment can aid in predicting the shape of the ACL attachment during ACL reconstruction, potentially improving footprint coverage.
Keywords: anterior cruciate ligament, lateral meniscus, anatomy
The success of anterior cruciate ligament (ACL) reconstruction requires accurate replication of the native ACL anatomy, including insertion sites and dimensions.12,28,30,32,33 To improve surgical outcomes, the procedure must be individualized based on each patient's distinct anatomic characteristics. 16 Interindividual variation in the shape of the ACL attachment must be recognized, particularly on the tibial insertion, because the shape of the tibial attachment of the ACL is more variable than the femoral attachment. 1
Previously, the tibial attachment site of the ACL was described to be on the anterior intercondylar region, with an oval or elliptical attachment site.21,25 More recent studies have indicated that the shape of the attachment site can vary, and triangular2,3,20,26 and C-shaped 24 attachments were also observed. Currently, the shape of the tibial attachment is commonly classified into 3 types—oval or elliptical, C-shaped, and triangular attachments—and their frequencies have been reported.6,8,15,27 However, this classification is subjective, and information on frequency is not sufficient to identify anatomic variations of each patient. Some information related to the shape of the ACL attachment would be useful in recognizing individual variations.
Previously, an anatomic study reported that the ACL and anterior horn of the lateral meniscus (AHLM) were in contention for the attachment range in the anterior intercondylar region. 17 Thus, we hypothesized that the location of the AHLM attachment may determine the shape of the ACL attachment. Identifying consistent patterns in the shape of the ACL attachment and location of the AHLM attachment would help predict the individual shape of the ACL attachment. This study aimed to objectively evaluate anatomic variations in the shape of the ACL tibial attachment, clarify its relationship with the location of the AHLM attachment, and provide an anatomic foundation for ACL reconstruction.
Methods
Preparation of Cadaveric Specimens
In total, 25 knees from 17 Japanese cadavers (12 men and 13 women; mean age at death, 77.8 years; range, 52-99 years) were donated to our department. The donation document format was congruent with the Japanese law titled “The Act on Body Donation for Medical and Dental Education” (act No. 56 of 1983). Before their deaths, all donors voluntarily declared that their remains would be donated as education and study materials. At that time, the purpose and methods of using body donor corpses were explained, and informed consent was obtained. After their deaths, this informed consent was also explained to the bereaved families, and there was no opposition.
All cadavers were fixed by arterial perfusion of 8% formalin and preserved in 30% alcohol. Cadavers with a history of knee abnormalities were not included in the study. The study was approved by the board of ethics at our institution (approval No. M2018-243). All methods were carried out in accordance with the relevant guidelines and regulations.
Macroscopic Anatomy
On the knee specimens, the skin, subcutaneous adipose tissue, and muscles were excised, the ligamentous structures surrounding the knee joint were removed, and the articular capsule was incised. The proximal tibial surface where the ACL and menisci were preserved was used. A transverse midsection of the ACL was made, and all other supporting tissues, including the posterior cruciate ligament, capsule, and collateral ligament, were separated at their respective attachments to the tibia. Specimens with marked ACL or lateral meniscus (LM) degeneration, trauma, or disease involving the proximal tibia were excluded. By using the knee specimens of the superior aspect of the tibia, including the tibial half of the ACL, the surrounding fat, connective tissue, and synovium were removed to expose the ACL and meniscal fibers. ACL fascicles were gradually excised, and the periphery of the ACL attachment was delineated using a black marker. After the complete excision of all ACL fascicles, the shape of the ACL attachment, AHLM location, and relationship between the 2 were meticulously observed. The shape of the ACL attachment was classified into 3 types—elliptical, C-shaped, and triangular—by 2 observers (S.M. and J.K.), according to the general classification method (Figure 1A). The menisci were subsequently removed to identify the boundaries of the articular cartilage for use as a reference during measurements. At each stage of the dissection, the superior aspect of the specimen was captured using a high-resolution camera, and the shape of the ACL attachment and the AHLM location were quantitatively analyzed.
Figure 1.

Assessment methods of anatomic structures. (A) Type classification and principal component analysis were performed to evaluate the shape of the anterior cruciate ligament (ACL) attachment. (B) To evaluate the location of the anterior horn of the lateral meniscus (AHLM) attachment, coordinates (horizontal axis [Lat] and vertical axis [Ant] values) of the AHLM tip were measured on the superior surface of the tibia. LM, lateral meniscus. See text for details.
The ACL has 3 distinct modes of attachment on the tibial side: (1) attachment to bone, (2) attachment to cartilage, and (3) continuity to the LM. 17 This study focused on the shape of the combined area of the (1) attachment to bone and (2) attachment to cartilage. This is because attachments to bone and cartilage have clear boundaries both macroscopically and histologically, whereas the continuity to the LM lacks a defined boundary because of the intermingled collagen fibers, rendering it inappropriate for the analysis of the attachment shape. In addition, the extent of the continuity to the LM is relatively diminutive, representing 4% to 5% of the total ACL attachment area on the tibial side; therefore, the exclusion of this region from the analysis would exert a negligible effect on the results.
Quantification of the Shape of the ACL Attachment
The outline of the ACL attachment recorded with a black marker was captured as a digital image, and the principle component (PC) analysis using elliptical Fourier descriptors (EFDs) was performed on the shape of the ACL attachment of the 25 samples (Figure 1A). The software package SHAPE (Version 1.3; Hiroyoshi Iwata; http://lbm.ab.a.u-tokyo.ac.jp/~iwata/) was used for this analysis. This software automatically performs the following procedures: (1) extraction of the contour of objects from an image file, (2) EFD calculation, (3) standardization of the size and orientation of the contour, (4) PC analysis of the EFDs, and (5) visualization of the shape of each PC by reconstructing of the contours. 9 The operational procedures and software results were double-checked by 2 investigators (S.M. and J.K.). The PC analysis conducted by this software is based on the variance-covariance matrix of the coefficients and can efficiently summarize the information contained in normalized EFD coefficients. The PC scores were automatically output by the software and can be used as observed values of morphological features. A scatterplot was created by taking PC1 and PC2 on the horizontal and vertical axes, respectively.
Quantification of the AHLM Location
On a photograph of the superior aspect of the tibia, a rectangle tangent to the border of the articular cartilage was delineated as the foundational reference for measurement (Figure 1B). The horizontal axis (Lat) is established along the posterior side of the rectangular shape, whereas the vertical axis (Ant) runs along its medial side. The origin is positioned at the posteromedial corner, establishing a coordinate system. Subsequently, the lateral margin of the rectangular reference frame was assigned a value of 100 on the horizontal axis (Lat), whereas the anterior margin was attributed a value of 100 on the vertical axis (Ant). Thereby, the Lat and Ant values for the points on the coordinate axes represent the relative position on the superior tibial surface. This measurement method is similar to the tibial quadrant method described by Tsuda et al. 29 Nonetheless, the measurement method used in this study differs from the tibial quadrant method in that it is based on articular cartilage margins, which can be readily identified through macroscopic dissection. The same holds true for the relative positioning with respect to the rectangular reference frame.
The AHLM edge, at which the tips of the fibers terminate, is defined as the leading edge (arrow curves in Figure 1B). Using the “Measure tool” function of Adobe Illustrator, we identified the midpoint on the curve of the leading edge and defined that point as the AHLM tip (arrowhead in Figure 1B). The Lat and Ant values of the AHLM tip on the coordinate axis were obtained.
Statistical Analysis
R software for Windows Version 4.1.0 (The R Foundation for Statistical Computing) was used in the statistical analyses, with the level of significance set at P < .05.
Type classification of the shape of the ACL attachment was performed by 2 observers (S.M. and J.K.), and the Kendall coefficient of concordance was calculated to test the reliability of the classification. The types of classification were compared, and the Kendall coefficient of concordance scores in our study was 0.8607 (P = .000002368).
Measurements of the AHLM location were performed by 2 investigators (S.M. and J.K.), and an intraclass correlation coefficient (ICC) was calculated to test the reliability of the measurements. Measurement values were the Lat and Ant values representing the horizontal (lateromedial) and vertical (anteroposterior) positions, respectively, and these values as measured by the 2 investigators were compared. The qualitative cutoffs of the ICCs were as follows: poor, <0.5; moderate, 0.50 to 0.75; good, 0.75 to 0.9; and excellent, >0.9. In this study, for the measurement of the horizontal and vertical positions of the AHLM, the ICC scores were 0.999 (95% CI, 0.997-0.999) and 0.998 (95% CI, 0.996-0.999), respectively.
Results
The shape of the tibial attachment of the ACL exhibited interindividual variability (Figures 2 and 3). In some individuals, the tibial side of the ACL occupied a large area of the anterior intercondylar region, and this attachment type was classified as elliptical (Figure 2A). In some individuals, the contour of the ACL attachment featured a concave depression at the lateral margin and hence was classified as C-shaped (Figure 2B). In other individuals, the posterior portion of the ACL attachment area was narrower than the anterior portion and thus classified as triangular (Figure 2C). Hence, the shapes of the ACL attachment were classified into these 3 types. Table 1 shows the type classification by the 2 observers. In addition, a certain relationship between the shape of the ACL attachment and the AHLM location was observed. In individuals with elliptical, C-shaped, and triangular ACL attachments, the AHLM attachment was located anterolaterally, medially, and posteromedially in the intercondylar region, respectively (Figure 2). The transverse ligament (intermeniscal ligament) was observed in 4 of the 25 cases, some in which the transverse ligament contacted the anterior margin of the ACL attachment and others in which it was approximately 5 mm away from it (see Appendix Figure A1, available in the online version of this article). Figure 3 displays a graphical illustration of the shape of the ACL attachment and location of the AHLM attachment for all 25 specimens (for specimens of the left knee, mirrored images are presented to adjust its orientation to that of the specimen of the right knee: No. 2, 3, 5, 8, 10, 12, 14, 16, 19, 25).
Figure 2.

Anatomic variation of the tibial side of anterior cruciate ligament (ACL) and anterior horn of the lateral meniscus (AHLM) attachments. The superior side of the tibia is observed from the superior aspect. (A) Elliptical ACL attachment area with anterolaterally located AHLM attachment. (B) C-shaped ACL attachment area with medially located AHLM attachment. (C) Triangular ACL attachment area with posteromedially located AHLM attachment. The transverse ligament (intermeniscal ligament) was observed in this sample (see Appendix Figure A1, available online). LM, lateral meniscus.
Figure 3.

Shape of the anterior cruciate ligament (ACL) attachment and location of the anterior horn of the lateral meniscus (AHLM) attachment of all 25 specimens. The ACL attachment area is shown in yellow, the leading edge of the AHLM is shown with both arrow curves, and the AHLM tip is shown with arrowheads. For the left knee specimens, mirrored images are presented (No. 2, 3, 5, 8, 10, 12, 14, 16, 19, 25). Sample numbers correspond to those in Table 1.
Table 1.
Attributes and Quantitative Data for All 25 Samples a
| Shape of ACL Attachment | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type Classification | Location of AHLM | |||||||||
| No. | Age | Sex | Side | Observer 1 | Observer 2 | PC1 (41.4%) | PC2 (27.9%) | PC3 (13.4%) | Lat | Ant |
| 1 | 62 | Female | Right | C-shaped | C-shaped | 0.06650 | −0.13255 | −0.03393 | 48.7 | 54.5 |
| 2 | Left | Triangular | Triangular | 0.23988 | −0.11685 | −0.04757 | 53.2 | 54.6 | ||
| 3 | 65 | Male | Left | Elliptical | Elliptical | 0.00642 | 0.01768 | −0.02846 | 51.6 | 64.7 |
| 4 | Right | Elliptical | Elliptical | 0.07429 | 0.08728 | −0.07296 | 59.2 | 56.9 | ||
| 5 | 69 | Female | Left | C-shaped | Triangular | 0.04565 | −0.08637 | −0.11412 | 45.7 | 51.3 |
| 6 | Right | Elliptical | Elliptical | 0.15722 | 0.11089 | 0.09428 | 51.8 | 55.1 | ||
| 7 | 70 | Female | Right | Triangular | Triangular | 0.14344 | −0.12298 | 0.06123 | 47.8 | 51.4 |
| 8 | Left | Triangular | Triangular | −0.05380 | 0.03423 | 0.08968 | 49.8 | 53.6 | ||
| 9 | 70 | Male | Right | C-shaped | C-shaped | −0.12522 | −0.05215 | 0.04348 | 50.2 | 53.1 |
| 10 | Left | C-shaped | C-shaped | −0.13135 | −0.07581 | 0.13039 | 48.2 | 47.9 | ||
| 11 | 87 | Male | Right | Triangular | Triangular | −0.08676 | −0.07355 | −0.10914 | 45.3 | 41.8 |
| 12 | Left | C-shaped | C-shaped | 0.01302 | −0.13850 | 0.05952 | 48.3 | 50.5 | ||
| 13 | 94 | Male | Right | C-shaped | Elliptical | −0.21276 | 0.08268 | −0.07502 | 48.7 | 54.3 |
| 14 | Left | C-shaped | Elliptical | 0.00698 | 0.14676 | 0.11048 | 48.9 | 55.1 | ||
| 15 | 99 | Female | Right | Triangular | Triangular | −0.02701 | −0.02216 | −0.01678 | 49.2 | 44.0 |
| 16 | Left | C-shaped | C-shaped | −0.16878 | −0.03617 | −0.01941 | 50.7 | 46.0 | ||
| 17 | 52 | Female | Right | Triangular | Triangular | 0.01633 | −0.04766 | 0.08748 | 43.2 | 54.7 |
| 18 | 71 | Female | Right | C-shaped | Elliptical | −0.07709 | 0.01644 | −0.09219 | 44.6 | 58.7 |
| 19 | 74 | Male | Left | C-shaped | C-shaped | −0.10255 | −0.13746 | 0.05849 | 47.6 | 57.1 |
| 20 | 78 | Female | Right | Elliptical | Elliptical | 0.20914 | 0.17415 | 0.04902 | 50.5 | 53.4 |
| 21 | 80 | Male | Right | C-shaped | C-shaped | −0.13129 | 0.01974 | 0.02336 | 49.7 | 57.5 |
| 22 | 82 | Male | Right | Elliptical | Elliptical | −0.05846 | 0.23558 | −0.04146 | 50.4 | 60.1 |
| 23 | 91 | Female | Right | Triangular | Triangular | −0.10378 | 0.01382 | −0.05009 | 47.7 | 49.8 |
| 24 | 92 | Female | Right | Elliptical | Elliptical | 0.03201 | 0.14084 | −0.03687 | 45.3 | 59.3 |
| 25 | 94 | Male | Left | Triangular | Triangular | 0.26798 | −0.03786 | −0.06940 | 46.9 | 58.0 |
Sample numbers correspond to Figure 3. ACL, anterior cruciate ligament; AHLM, anterior horn of the lateral meniscus; Ant, vertical axis; Lat, horizontal axis; PC, principal component.
Table 1 shows the results of the PC analysis of the shape of the ACL attachment, and Figure 4 presents the reconstructed contours of each PC. The mean shape of the ACL attachments in the 25 samples was slightly wider at the anterior portion than at the posterior portion, with a concave lateral border and convex medial border (Figure 4). The contributions of PC1, PC2, and PC3 to the shape of the ACL attachment were 41.4%, 27.9%, and 13.4%, respectively. The scatterplots of PC1 and PC2, which are overlaid with the results of the type classification by observer 1, are shown in Figure 5. Elliptical types were mainly distributed in the first quadrant (high PC1 and PC2 values), the C shape in the second and third quadrants (low PC1 values), and the triangular in the fourth quadrant (high PC1 and low PC2 values). Each type did not form a distinct cluster in the coordinate plane, and the regions of each type overlapped. The overlap between the elliptical and C shapes and between the C and triangular shapes was particularly pronounced.
Figure 4.
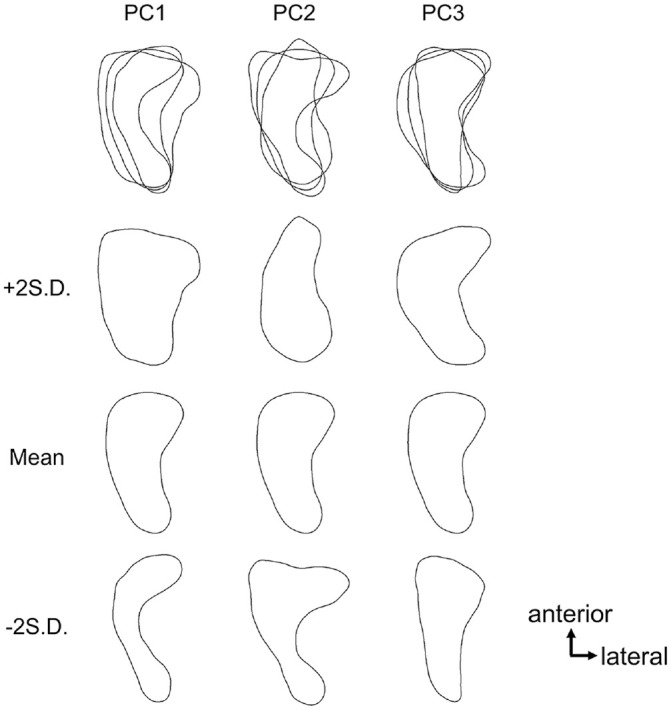
Reconstructed contours of the principal components (PCs) of the anterior cruciate ligament (ACL) attachment shape. The mean shape of the ACL attachments in 25 samples was slightly wider at the anterior portion than at the posterior portion, with a concave lateral border and convex medial border. PC1 is considered to reflect the intensity of the expansion/contraction of the overall width of the attachment area and the concave shape of the lateral edge, such that higher PC1 values are closer to an elliptical or triangular shape and lower values to the C shape. PC2 is thought to reflect the intensity of the reduction and expansion of the width of the anterior portion and the concavity of the lateral edge, such that higher PC2 values are closer to an elliptical shape and lower values are closer to a triangular or C shape. The contributions of PC1, PC2, and PC3 to the shape of the ACL attachment were 41.4%, 27.9%, and 13.4%, respectively.
Figure 5.
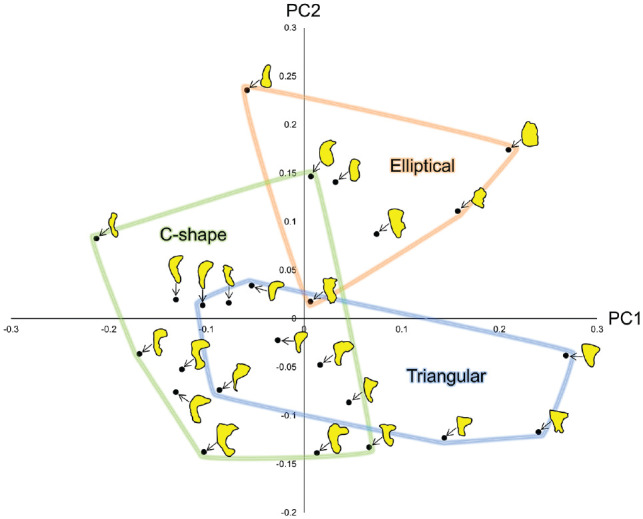
Scatterplots of PC1 and PC2 of the anterior cruciate ligament attachment shape. The results of the type classification by observer 1 are overlaid. Each type did not form a distinct cluster in the coordinate plane, and the regions of each type overlapped. The overlap between the elliptical and C shapes, and between the C and triangular shapes was particularly pronounced, indicating that the C shape is intermediate between the elliptical and triangular shapes. PC, principal component.
Table 1 shows the measurement results for the location of AHLM attachments, and Figure 6A presents the scatterplots. The location of the AHLM attachment exhibited interindividual variability, and its possible range was the anterolateral, anteromedial, or posteromedial area of the anterior intercondylar region. Figure 6B shows the expansion of the scatterplots of the location of the AHLM attachment, overlaid with the shapes of the ACL attachments for each individual. Individuals with anterior, medial, and posteromedial AHLM attachments tended to have elliptical, C, and triangular shapes in their ACL attachments, respectively (Figure 6B).
Figure 6.

Scatterplots of the location of anterior horn of the lateral meniscus (AHLM) attachments. (A) The location of the AHLM attachment exhibited interindividual variability, and its possible range was the anterolateral, anteromedial, or posteromedial area of the anterior intercondylar region. (B) Expansion of the rectangular area in panel A, overlaid with the shape classification of anterior cruciate ligament (ACL) attachments. Individuals with anterior, medial, and posteromedial AHLM attachments tended to have elliptical, C, and triangular shapes in their ACL attachments, respectively. Ant, vertical axis; Lat, horizontal axis.
Discussion
The shape of the ACL attachments varied continuously, ranging from elliptical to triangular, with the C shape being the intermediate between the elliptical and triangular shapes. Furthermore, this variation of the ACL attachment shape showed a consistent trend with the location of the AHLM attachment: the shape of the ACL attachment showed an elliptical, C-shaped, or triangular morphology, as the location of the AHLM attachment was continuously distributed from the anterolateral to the posteromedial direction. This suggests that the shape of the ACL attachment depends on the AHLM location. The AHLM location would be key information for the prediction of the shape of the ACL attachment during ACL reconstruction.
To achieve optimal outcomes in ACL reconstruction, the anatomic structure of the ligament must be restored.30,32 Anatomic reconstruction is defined as “the functional restoration of the ACL to its native dimensions, collagen orientation, and insertion sites,” 30 which has been shown to result in better clinical outcomes than nonanatomic ACL reconstruction.7,13 The anatomy of the ACL attachment site differs between the femoral and tibial sides, with the tibial side being more variable than the femoral side 1 and exhibiting various attachment patterns, including nonbony attachment. 17 In the highly variable tibial attachment, the shape of the attachment critically affects the coverage of the footprint when creating a bone tunnel during ACL reconstruction.22,23 Several researchers have developed techniques to modify the shape of the bone tunnel into oval, rectangular, rounded-rectangular, or C shapes, with some favorable early clinical outcomes, to better restore the architecture of the native ACL attachment.4,14,18,22
The attachment shape on the tibial ACL has been generally considered oval or elliptical.21,25 Triangular2,3,20,26 and C-shaped attachments 24 have been reported in recent studies, indicating the variability in the morphology of the attachment site. Nowadays, they are often described as elliptical, C-shaped, and triangular.6,8,15,27 Some have rated it as an L shape, which appears to be close to the C shape. 10 This study analyzed the variations in the shape of the tibial attachment of the ACL as a continuous phenomenon rather than the conventional method of classifying types. The results of the PC analysis using EFDs showed that PC1, which has the highest contribution ratio, is considered to reflect the intensity of the expansion or contraction of the overall width of the attachment area and the concave shape of the lateral edge, such that higher PC1 values are closer to an elliptical or triangular shape and lower values are closer to the C shape. PC2, the next highest contributing component, is thought to reflect the intensity of the reduction and expansion of the width of the anterior portion and concavity of the lateral edge, such that higher PC2 values are closer to an elliptical shape and lower values to a triangular or C shape (Figure 4). In addition, the inclusion of the relationship between the AHLM locations in the analysis is also a new and unique perspective in this study. The quantitative analysis revealed a continuous spectrum of the variations in the shape of the ACL attachments (Figure 5), with a consistent trend in the AHLM location (Figure 6).
This study reveals that the variation in the shape of the ACL attachment is not an independent phenomenon but is continuous (Figure 7). In other words, the fundamental principle of the ACL attachment shape is that it ranges from elliptical to triangular, with a multitude of intermediate shapes recognized as C-shaped between them. The results of no disagreement between the 2 observers in classifying the type between elliptical and triangular (Table 1) and that the PC of the C shape overlaps with both elliptical and triangular shapes in the scatterplots (Figure 5) suggests that the C shape is an intermediate type between the elliptical and triangular shapes. The tibial attachments of the C and L shapes that have been previously reported are probably individuals with shapes that are intermediate between elliptical and triangular.6,8,10,15,24 In previous studies that have examined frequency based on typology, elliptical and triangular shapes were reported with high frequency, whereas for C shapes the reported frequency ranged from 0% to 48.4%.6,15,27 Because C shapes are intermediate between elliptical and triangular shapes, the frequency of the C shapes varies significantly, depending on how the observer classifies the C shapes that are more elliptical or more triangular. Thus, the previous type classification system would have only captured a portion of the continuous variation. By acknowledging the continuous variations of the ACL attachment shape, any variation can be explained from this fundamental principle.
Figure 7.
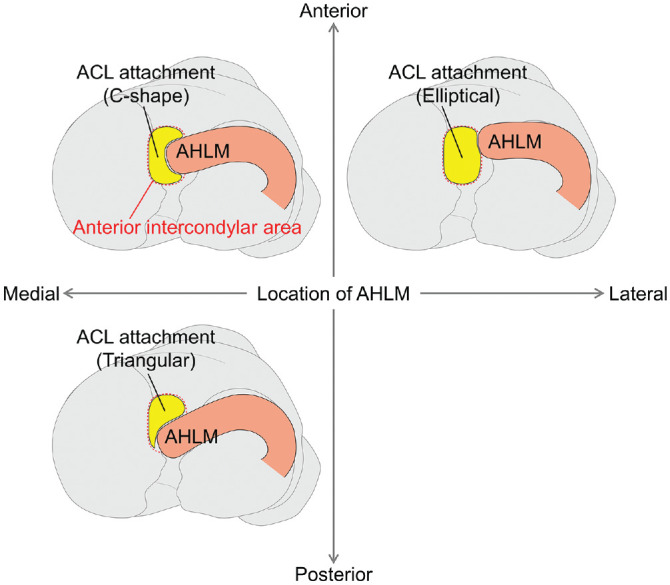
Morphological relationship between the shape of the anterior cruciate ligament (ACL) attachment and anterior horn of the lateral meniscus (AHLM) attachment location. The tibial sides of the ACL and AHLM both occupy the anterior intercondylar region, and the location of the AHLM attachment would determine the shape of the ACL attachment. Consequently, the AHLM attachment anterolateral, anteromedial, and posteromedial locations correspond to the ACL attachment elliptical, C, and triangular shapes, respectively. Information on the AHLM attachment location may be useful in predicting the ACL attachment shape during ACL reconstruction.
Regarding the determinants of the shape of the tibial attachment of the ACL, Morales-Avalos et al 15 reported an association between age and variation in the tibial attachment shape. Morphological variation would be influenced by multiple factors, and the AHLM location, as disclosed by this study, may be one of the contributing factors. On the basis of histological findings, Muro et al 17 reported that the ACL tibial side and AHLM compete for the attachment area in the intercondylar region. In many individuals, the AHLM attaches intrusively to the intercondylar region, and the leading edge of this intrusiveness is designed to fit into the depression of the C- or L-shaped attachment.5,10,17,24 The proximity between the ACL and AHLM could be associated with the high incidence of iatrogenic AHLM injury (range, 21.7%-100%) in ACL reconstruction.11,19,31 Thus, the AHLM and ACL tibial attachment area are complementary, occupying the anterior intercondylar region and competing with or complementing each other's attachment area. Consequently, the AHLM location may affect the shape of the ACL attachment area (Figure 7). Based on these principles, the shape of the ACL tibial attachment may be deduced by assessing the AHLM location. Intraoperative arthroscopy is limited in its visualization of the entire ACL attachment site and thus precludes the exact determination of the true shape of the ACL attachment site. 26 On the contrary, the AHLM location can be observed under arthroscopy during surgery. Our anatomic findings indicate that the AHLM location provides useful information to determine the bone tunnel position during ACL reconstruction. This information enables surgeons to predict the shape of the ACL attachment. Previously, the shape of the ACL attachment could only be inferred from the ACL tear tissue; however, at present, other anatomic information can be used. Therefore, we propose intraoperative arthroscopic observation of the AHLM location to predict the shape of the ACL attachment and provide additional information to determine the bone tunnel position. Such an approach may contribute to the rationale for anatomic reconstruction procedures, individualizing ACL reconstruction, 16 and achieve better footprint coverage and better clinical outcomes. The development of new diagnostic methods and surgical approaches is necessary based on these new anatomic findings.
This study has a few limitations. First, the ages of the cadavers were skewed because they were older adults with a mean age of >70 years. The effect of aging on morphological changes cannot be excluded. However, in comparison with previous studies including analysis of younger individuals, no notable discrepancy was found in the findings of ACL tibial attachment variations.6,15,27 The C shape is reportedly more common in elderly individuals, while the elliptical shape is reportedly more common in young individuals; therefore, it would not be possible to directly extrapolate the frequency of shape variations seen in this study to young patients. 15 However, a previous study of 100 young patients (mean age, 26 ± 11 years) reported that the 3 shape types shown in this study were also seen in young patients (elliptical, 51%; C-shaped, 16%; and triangular, 33%), so the relationship between the ACL attachment shape and AHLM location shown in this study may also be seen in young individuals. 6 Future morphological studies of young individuals are required to generalize the results of this study to young patients, the typical patient population subjected to ACL reconstruction. Second, this study was purely anatomic; therefore, whether the anatomic findings presented in this study will result in better footprint coverage in ACL reconstruction, prevention of iatrogenic AHLM injury, and enhanced clinical outcomes remains to be elucidated. Future clinical studies may provide additional information regarding the clinical application of these findings.
Conclusion
This study provides an anatomic basis for highly accurate and individualized ACL reconstruction. The tibial attachment of the ACL exhibits a gradual transition from an elliptical to a triangular shape, with the C shape being intermediate in its anatomic variation. The tibial sides of the ACL and AHLM both occupy the anterior intercondylar region, and the AHLM attachment location appears to play a role in determining the shape of the ACL attachment. Thus, information on AHLM attachment location may be useful in predicting the shape of the ACL attachment during ACL reconstruction. Such a predictive approach may contribute to better footprint coverage and prevention of iatrogenic AHLM injury in ACL reconstruction.
Supplemental Material
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231219978 for Morphometric Analysis of the Tibial Attachment Shape of the Anterior Cruciate Ligament and Its Relationship With the Location of the Anterior Horn of the Lateral Meniscus by Satoru Muro, Jiyoon Kim, Akimoto Nimura, Sachiyuki Tsukada and Keiichi Akita in The American Journal of Sports Medicine
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomic research could be performed. Results from such research can potentially increase humankind's overall knowledge, which can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Footnotes
Submitted June 23, 2023; accepted October 16, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
ORCID iDs: Satoru Muro  https://orcid.org/0000-0002-4709-6359
https://orcid.org/0000-0002-4709-6359
Akimoto Nimura
https://orcid.org/0000-0002-3054-0273
References
- 1. Colombet P, Robinson J, Christel P, et al. Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy. 2006;22(9):984-992. [DOI] [PubMed] [Google Scholar]
- 2. de Abreu-e-Silva GM, de Oliveira MH, Maranhao GS, et al. Three-dimensional computed tomography evaluation of anterior cruciate ligament footprint for anatomic single-bundle reconstruction. Knee Surg Sports Traumatol Arthrosc. 2015;23(3):770-776. [DOI] [PubMed] [Google Scholar]
- 3. Ferretti M, Doca D, Ingham SM, Cohen M, Fu FH. Bony and soft tissue landmarks of the ACL tibial insertion site: an anatomical study. Knee Surg Sports Traumatol Arthrosc. 2012;20(1):62-68. [DOI] [PubMed] [Google Scholar]
- 4. Fink C, Smigielski R, Siebold R, Abermann E, Herbort M. Anterior cruciate ligament reconstruction using a ribbon-like graft with a C-shaped tibial bone tunnel. Arthrosc Tech. 2020;9(2):e247-e262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Fujishiro H, Tsukada S, Nakamura T, et al. Attachment area of fibres from the horns of lateral meniscus: anatomic study with special reference to the positional relationship of anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):368-373. [DOI] [PubMed] [Google Scholar]
- 6. Guenther D, Irarrázaval S, Nishizawa Y, et al. Variation in the shape of the tibial insertion site of the anterior cruciate ligament: classification is required. Knee Surg Sports Traumatol Arthrosc. 2017;25(8):2428-2432. [DOI] [PubMed] [Google Scholar]
- 7. Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH. Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am J Sports Med. 2012;40(3):512-520. [DOI] [PubMed] [Google Scholar]
- 8. Irarrázaval S, Albers M, Chao T, Fu FH. Gross, arthroscopic, and radiographic anatomies of the anterior cruciate ligament: foundations for anterior cruciate ligament surgery. Clin Sports Med. 2017;36(1):9-23. [DOI] [PubMed] [Google Scholar]
- 9. Iwata H, Ukai Y. SHAPE: a computer program package for quantitative evaluation of biological shapes based on elliptic Fourier descriptors. J Hered. 2002;93(5):384-385. [DOI] [PubMed] [Google Scholar]
- 10. Kusano M, Yonetani Y, Mae T, et al. Tibial insertions of the anterior cruciate ligament and the anterior horn of the lateral meniscus: a histological and computed tomographic study. Knee. 2017;24(4):782-791. [DOI] [PubMed] [Google Scholar]
- 11. LaPrade CM, Smith SD, Rasmussen MT, et al. Consequences of tibial tunnel reaming on the meniscal roots during cruciate ligament reconstruction in a cadaveric model, part 1: the anterior cruciate ligament. Am J Sports Med. 2015;43(1):200-206. [DOI] [PubMed] [Google Scholar]
- 12. Lee JS, Kim TH, Kang SY, et al. How isometric are the anatomic femoral tunnel and the anterior tibial tunnel for anterior cruciate ligament reconstruction? Arthroscopy. 2012;28(10):1504-1512. [DOI] [PubMed] [Google Scholar]
- 13. Marchant BG, Noyes FR, Barber-Westin SD, Fleckenstein C. Prevalence of nonanatomical graft placement in a series of failed anterior cruciate ligament reconstructions. Am J Sports Med. 2010;38(10):1987-1996. [DOI] [PubMed] [Google Scholar]
- 14. Matsuo T, Kusano M, Uchida R, Tsuda T, Toritsuka Y. Anatomical rectangular tunnel anterior cruciate ligament reconstruction provides excellent clinical outcomes. Knee Surg Sports Traumatol Arthrosc. 2022;30(4):1396-1403. [DOI] [PubMed] [Google Scholar]
- 15. Morales-Avalos R, Castillo-Escobedo TA, Elizondo-Omaña RE, et al. The morphology of the tibial footprint of the anterior cruciate ligament changes with ageing from oval/elliptical to C-shaped. Knee Surg Sports Traumatol Arthrosc. 2021;29(3):922-930. [DOI] [PubMed] [Google Scholar]
- 16. Murawski CD, Wolf MR, Araki D, et al. Anatomic anterior cruciate ligament reconstruction: current concepts and future perspective. Cartilage. 2013;4(3)(suppl):27S-37S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Muro S, Kim J, Tsukada S, Akita K. Significance of the broad non-bony attachments of the anterior cruciate ligament on the tibial side. Sci Rep. 2022;12(1):6844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Nakase J, Toratani T, Kosaka M, et al. Technique of anatomical single bundle ACL reconstruction with rounded rectangle femoral dilator. Knee. 2016;23(1):91-96. [DOI] [PubMed] [Google Scholar]
- 19. Oishi K, Sasaki E, Naraoka T, et al. Anatomical relationship between insertion sites, tunnel placement, and lateral meniscus anterior horn injury during single and double bundle anterior cruciate ligament reconstructions: a comparative macroscopic and histopathological evaluation in cadavers. J Orthop Sci. 2019;24(3):494-500. [DOI] [PubMed] [Google Scholar]
- 20. Petersen W, Zantop T. Anatomy of the anterior cruciate ligament with regard to its two bundles. Clin Orthop Relat Res. 2007;454:35-47. [DOI] [PubMed] [Google Scholar]
- 21. Scott WN, Insall JN, Diduch DR, Iorio R, Long WJ. Insall and Scott Surgery of the Knee. 6th ed. Elsevier; 2018. [Google Scholar]
- 22. Shao J, Zhang J, Ren S, et al. Better coverage of the ACL tibial footprint and less injury to the anterior root of the lateral meniscus using a rounded-rectangular tibial tunnel in ACL reconstruction: a cadaveric study. Orthop J Sports Med. 2022;10(3):23259671221083581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Siebold R. The concept of complete footprint restoration with guidelines for single- and double-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19(5):699-706. [DOI] [PubMed] [Google Scholar]
- 24. Siebold R, Schuhmacher P, Fernandez F, et al. Flat midsubstance of the anterior cruciate ligament with tibial “C”-shaped insertion site. Knee Surg Sports Traumatol Arthrosc. 2015;23(11):3136-3142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. Elsevier Health Sciences;2015. [Google Scholar]
- 26. Tállay A, Lim MH, Bartlett J. Anatomical study of the human anterior cruciate ligament stump's tibial insertion footprint. Knee Surg Sports Traumatol Arthrosc. 2008;16(8):741-746. [DOI] [PubMed] [Google Scholar]
- 27. Tashiro Y, Lucidi GA, Gale T, et al. Anterior cruciate ligament tibial insertion site is elliptical or triangular shaped in healthy young adults: high-resolution 3-T MRI analysis. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):485-490. [DOI] [PubMed] [Google Scholar]
- 28. Triantafyllidi E, Paschos NK, Goussia A, et al. The shape and the thickness of the anterior cruciate ligament along its length in relation to the posterior cruciate ligament: a cadaveric study. Arthroscopy. 2013;29(12):1963-1973. [DOI] [PubMed] [Google Scholar]
- 29. Tsuda E, Ishibashi Y, Fukuda A, et al. Tunnel position and relationship to postoperative knee laxity after double-bundle anterior cruciate ligament reconstruction with a transtibial technique. Am J Sports Med. 2010;38(4):698-706. [DOI] [PubMed] [Google Scholar]
- 30. van Eck CF, Lesniak BP, Schreiber VM, Fu FH. Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy. 2010;26(2):258-268. [DOI] [PubMed] [Google Scholar]
- 31. Watson JN, Wilson KJ, LaPrade CM, et al. Iatrogenic injury of the anterior meniscal root attachments following anterior cruciate ligament reconstruction tunnel reaming. Knee Surg Sports Traumatol Arthrosc. 2015;23(8):2360-2366. [DOI] [PubMed] [Google Scholar]
- 32. Yasuda K, van Eck CF, Hoshino Y, Fu FH, Tashman S. Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 1: basic science. Am J Sports Med. 2011;39(8):1789-1799. [DOI] [PubMed] [Google Scholar]
- 33. Zheng L, Harner CD, Zhang X. The morphometry of soft tissue insertions on the tibial plateau: data acquisition and statistical shape analysis. PLoS One. 2014;9(5):e96515. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231219978 for Morphometric Analysis of the Tibial Attachment Shape of the Anterior Cruciate Ligament and Its Relationship With the Location of the Anterior Horn of the Lateral Meniscus by Satoru Muro, Jiyoon Kim, Akimoto Nimura, Sachiyuki Tsukada and Keiichi Akita in The American Journal of Sports Medicine