

Abstract
Background:
There are few studies on the health effects of long-term exposure to neighborhood greenness in a longitudinal setting, especially in Asian countries with high population densities.
Objectives:
This study investigates the association between long-term exposure to neighborhood greenness and hypertension among adults in Taiwan.
Methods:
We selected 125,537 participants ( of age) without hypertension from Taiwan who had joined the standard medical examination program between 2001 and 2016. Neighborhood greenness was estimated using the normalized difference vegetation index (NDVI), derived from satellite images at a resolution of . The 2-y average NDVI value within a circular buffer around participants’ residences was calculated. A time-varying Cox regression model was used to investigate the association between neighborhood greenness and incident hypertension. Mediation analyses were performed to examine whether the association was explained by air pollution, leisure-time physical exercise, or body mass index (BMI).
Results:
Compared with living in areas within the first quartile of neighborhood greenness, living in areas within the second, third, and fourth quartiles of neighborhood greenness was found to be associated with a lower risk of hypertension, with hazard ratios (HRs) and 95% confidence intervals (CIs) of 0.95 (95% CI: 0.91, 1.00), 0.95 (95% CI: 0.90, 0.99), and 0.93 (95% CI: 0.88, 0.97), respectively. Each 0.1-unit increase in the NDVI was associated with a 24% lower risk of developing hypertension (0.76; 95% CI: 0.66, 0.87), with this associations being stronger among males and those with higher education levels. This association was slightly mediated by BMI but not by air pollution or leisure-time physical exercise.
Discussion:
Our findings suggest the protective effects of neighborhood greenness on hypertension development, especially in males and well-educated individuals. Our results reinforced the importance of neighborhood greenness for supporting health. https://doi.org/10.1289/EHP13071
Introduction
Hypertension is one of the leading risk factors for cardiovascular diseases and premature deaths worldwide. It is estimated that high systolic blood pressure (SBP) contributed to 10.4 million deaths (30.4% of total deaths) in the world in 2017.1 Moreover, in 2019, the number of people 30–79 years of age living with hypertension was 1.28 billion, twice the number in 1990.2 One of the World Health Organization’s global targets for noncommunicable diseases is to reduce the prevalence of hypertension by 33% by 2030.3
Neighborhood greenness is increasingly recognized as a modifiable environmental factor, and as an important element of the urban environment.4 Previous studies found that exposure to greenness may lower the prevalence of hypertension.5–10 However, most studies have relied on cross-sectional data, which cannot capture changes in exposure to greenness and covariates over time. In addition, few cohort studies have investigated the associations of exposure to greenness with hypertension, especially in Asian countries. Two cohort studies conducted in European countries failed to detect a significant negative association between exposure to greenness and hypertension.11,12 By contrast, a cohort study in Australia reported a negative association between tree canopy and hypertension.13 Similarly, a cohort study conducted in China found an inverse association between greenness exposure and hypertension, but it focused on people of age.14
It has been hypothesized that exposure to greenness may benefit population health by reducing exposure to air pollution and noise, by promoting engagement in physical exercise (PE) and increasing social interaction, and by decreasing psychological stress and depression.4 However, a limited number of studies have investigated the underlying pathways linking exposure to greenness with hypertension, and their results are inconsistent. Specifically, a few studies, conducted mainly among adults, have explored the mediating effects of exposure to air pollution,9,10,14,15 engagement in PE,9,14,16 and body mass index (BMI)6,9,14,15,17 on the association between exposure to greenness and hypertension. However, although some of these studies have found that one or two of these variables partially mediated the association between exposure to greenness and hypertension,6,9,10,14,16 the other studies did not find evidence that any of these variables mediate this association.15,17 Furthermore, although some studies found the beneficial effects of greenness on hypertension, the directions of mediating effects of air pollution on the association between greenness and hypertension were inconsistent. Zhou found the indirect effects of greenness exposure mediated through air pollution were associated with an increased risk of hypertension,14 whereas Yang reported decreasing SBP associated with greenness exposure mediated through air pollution.9
The primary aim of the present study was to investigate the association between long-term exposure to neighborhood greenness and hypertension based on a Taiwanese cohort. The second aim was to assess whether the association was mediated by exposure to air pollution, leisure-time PE, or BMI.
Methods
Study Design and Population
The participants were selected from an ongoing cohort in Taiwan. The cohort profile has been documented in our previous publications.18,19 As previously described, the Mei Jau (MJ) Health Management Institution, a private fee-for-service company, established the cohort.20 In brief, this institution offers a comprehensive standard health screening program. Participants, from various parts of Taiwan, paid a membership fee and an additional charge for health examinations since 1994.20 These participants generally had a higher level of education compared with the average Taiwanese population. In addition, the MJ Health Management Institution also provided services to individuals whose screenings were financed by various companies. Participants were encouraged to visit the clinical center periodically for a series of medical examinations and to complete a standard self-administered questionnaire. By 2016, Taiwan residents had been recruited into the program and 44% had visited the clinical center at least twice. Each participant signed an informed consent form prior to each medical visit, authorizing the MJ Health Management Institution to release the data for research purposes. In addition, ethical approval for this study was obtained from the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee.
Figure 1 shows the procedure for participant selection. We targeted 442,782 participants of age who had joined the program from 2001 to 2016, given that satellite data were available for greenness and air pollution assessments during this period. We excluded 106,654 participants because of incomplete information (33,313 lacked information on greenness exposure owing to having no listed address or living near water [i.e., people living within the radius buffer, including some pixels of NDVI value were excluded), 3,736 lacked blood pressure measurements, and 69,605 lacked information on covariates, including demographics, socioeconomic status, lifestyle factors, anthropometric measurements, blood tests, medical history, and particulate matter with an aerodynamic diameter of () exposure]. We further excluded 10 participants who exhibited outlier blood pressure values [i.e., or diastolic blood pressure , or ]; 190,169 participants who had undergone only one medical examination; and 20,412 participants who had hypertension at baseline (i.e., , , or self-reported physician-diagnosed hypertension). Finally, a total of 125,537 participants with 442,435 medical measurements were selected for the data analysis.
Figure 1.

Flow chart of participant selection for a study on neighborhood greenness and incident hypertension in Taiwanese adults.
Compared with the 125,537 participants included in the data analysis, the 317,245 excluded participants exhibited similar distributions for most characteristics, except that they were slightly older (40.60 vs. 37.33) and slightly less educated (college or above: 60.32% vs. 70.58%) (Table 1).
Table 1.
Comparison of baseline characteristics of the included and excluded participants from Taiwan (included, ; excluded, ).
| Characteristic | Included participants ()a |
Excluded participants ()b |
|---|---|---|
| Age [y ()] | ||
| Sex [ (%)] | ||
| Male | 61,076 (48.65) | 152,278 (48.00) |
| Female | 64,461 (51.35) | 164,967 (52.00) |
| Education [ (%)] | ||
| Lower than high school | 11,992 (9.55) | 57,471 (19.30) |
| High school | 24,939 (19.87) | 60,651 (20.37) |
| College or university | 71,882 (57.26) | 146,628 (49.25) |
| Postgraduate | 16,724 (13.32) | 32,971 (11.07) |
| Marital status [ (%)] | ||
| Unmarried | 40,172 (32.00) | 79,813 (32.14) |
| Married or remarried or cohabiting | 79,916 (63.66) | 150,214 (60.49) |
| Divorced | 2,978 (2.37) | 7,742 (3.12) |
| Widowed | 2,471 (1.97) | 10,554 (4.25) |
| Smoking status [ (%)] | ||
| Never | 94,743 (75.47) | 212,539 (73.08) |
| Former | 6,418 (5.11) | 17,581 (6.05) |
| Current | 24,376 (19.42) | 60,695 (20.87) |
| Alcohol consumption [ (%)] | ||
| Seldom | 109,103 (86.91) | 239,776 (85.06) |
| Occasional | 11,588 (9.23) | 27,094 (9.61) |
| Regular | 4,846 (3.86) | 15,019 (5.33) |
| Physical labor at work [ (%)] | ||
| Sedentary jobs | 81,911 (65.25) | 174,169 (61.11) |
| Jobs that are approximately half sedentary and half standing/walking | 32,217 (25.66) | 75,972 (26.66) |
| Jobs that mostly involve walking and standing | 9,348 (7.45) | 27,875 (9.78) |
| Jobs that involve vigorous physical activity | 2,061 (1.62) | 6,977 (2.45) |
| Vegetable intake [ (%)] | ||
| Seldom | 16,954 (13.51) | 43,731 (14.88) |
| Moderate | 75,191 (59.90) | 171,304 (58.30) |
| Frequent | 33,392 (26.60) | 78,813 (26.82) |
| Fruit intake [ (%)] | ||
| Seldom | 41,038 (32.69) | 105,034 (35.75) |
| Moderate | 68,882 (54.87) | 155,632 (52.98) |
| Frequent | 15,617 (12.44) | 33,108 (11.27) |
| Occupational exposure [ (%)]c | ||
| Yes | 10,447 (8.32) | 23,922 (7.64) |
| No | 115,090 (91.68) | 293,323 (92.46) |
| BMI [ ()] | ||
| d | 0.28 (0.15) | 0.28 (0.15) |
| [ ()] | ||
| Season [ (%)] | ||
| Spring | 31,443 (25.05) | 80,127 (25.26) |
| Summer | 35,065 (27.93) | 89,209 (28.12) |
| Fall | 33,570 (26.74) | 82,879 (26.12) |
| Winter | 25,459 (20.28) | 65,030 (20.50) |
Note: Values are presented as for continuous variables with normal distributions and as counts (%) for categorical variables. BMI, body mass index; IQR, interquartile range; NDVI, normalized difference vegetation index; , particulate matter with an aerodynamic diameter of ; SD, standard deviation.
Baseline characteristics of the 125,537 participants included in the study. Data are complete for all variables for the included participants.
Baseline characteristics of the 317,245 participants excluded in the study. Statistics are based on valid observations for the excluded participants (missing cases are not counted).
Classified as exposure to dust or organic solvents in the workplace; this was established by asking, “Are there any occupational hazards in your workplace?”
Refers to the average NDVI values within a buffer in the year of the visit and in the year before the visit. Each value is presented as a median (IQR) owing to the skewed distribution.
Neighborhood Greenness Assessment
Neighborhood greenness was estimated using a satellite image-based vegetation index—the normalized difference vegetation index (NDVI). The NDVI is calculated based on the difference in spectral reflectance and absorption of leaves in two light bands (i.e., leaves strongly reflect near infrared light, and they strongly absorb visible red light for use in photosynthesis). In theory, the valid range of the NDVI is from to ; negative values indicate the presence of freestanding water, clouds, or snow; values around 0 indicate barren areas (i.e., rocks, sand, or buildings); and positive values indicate grassland or bushland, with higher positive values indicating densely vegetated areas. We restricted our data to values to differentiate the effects of greenness from the potential effects of living near water.
Satellite images containing layers of NDVI were obtained from the Moderate Resolution Imaging Spectroradiometer Vegetation Index products (version 6; MODIS VI), which were available across Taiwan at 16-d intervals at a spatial resolution of .21 The current MODIS VI product was validated and the accuracy of the NDVI is within units.22 The valid range for the NDVI from the products is to units with a scale factor of 0.0001, and an NDVI value of indicates a missing value.21 Each satellite image also contains a summary quality layer with a valid range from 0 to 3 to indicate the pixel reliability. A pixel with a reliability index of 2 or 3 was regarded as a missing value because such values indicate that the target in the pixel is covered by snow, ice, or cloud, which may affect the NDVI value.21 We therefore used pixels with a reliability index of 0 or 1 to fill the missing values through the spatiotemporal prediction method in the R package gapfill.23
The address of each participant was geocoded into latitude and longitude data, which were transferred as spatial points into the satellite images. The 16-d interval NDVI estimates were aggregated as annual average values. The annual mean NDVI value within a circular buffer with a radius around each spatial point was calculated and regarded as the indicator of neighborhood greenness.9,24 Participants reported their address during each medical visit, thus any change of address was recorded. If the participant’s address was updated in a follow-up medical visit, the NDVI value at the new address since the follow-up time point was applied in the data analysis. A 2-y average NDVI value (i.e., the average annual NDVI value for the year of the medical examination and the previous year) was assigned to each address and served as the indicator of long-term exposure to neighborhood greenness. Both continuous and categorical NDVI values (i.e., those in the , 25th to 50th, 50th to 75th, and percentile of the NDVI distribution) were used for data analysis.
Potential Mediators
Previous studies have reported the association of air pollution,25,26 PE,27,28 and obesity29–31 with greenness and hypertension. Further, it has been hypothesized that the benefits of exposure to greenness may be mediated by reducing exposure to air pollution, as well as reducing obesity levels and improving PE.4 Therefore, the mediating effects of exposure to , leisure-time PE, and BMI were examined in the analysis.6,9,14
The details of the assessment have been described in our previous studies.32,33 In brief, we estimated ambient exposure at each participant’s residence using a spatiotemporal model. This model integrates satellite-based atmospheric optical depth (AOD) data, collected at a fine spatial resolution of , with meteorological information such as visibility and relative humidity.32,33 The AOD data, essential for our model, was sourced from the MODIS on board satellites of the US National Aeronautics and Space Administration.32,33 The data sample size for AOD, , aligns with the global average level.34 To mitigate the challenges of missing data and temporal constraints, we applied a correction factor derived from terrestrial observations.35 This model was previously validated by comparing estimated exposures with monitoring data from ground-level air-pollution monitoring stations across Taiwan,18 revealing that the correlation coefficients between two measurements ranged from 0.72 to 0.83.18 A 2-y average concentration was assigned to each participant’s address as their exposure to ambient . This was calculated by taking the average of the annual concentrations for the medical examination year and the previous year.
Details regarding the assessment of PE have been described elsewhere.26,36,37 PE was estimated using a standard self-administrated questionnaire. The participants reported the intensity level of weekly leisure-time PE they had performed in the previous month, with the following intensity levels: light (e.g., walking), moderate (e.g., brisk walking), moderately vigorous (e.g., jogging), and highly vigorous (e.g., rope skipping). These intensity levels were assigned a specific metabolic equivalent of task (MET; 1 per hour per kilogram of body weight) value: 2.5 (light), 4.5 (moderate), 6.5 (moderately vigorous), or 8.5 (highly vigorous).36,37 Participants also reported the duration of weekly exercise. If they had engaged in more than one intensity level of exercise, they were assigned a weighted MET that was based on the duration of each intensity level of exercise they had engaged in. The weekly exercise volume (MET-h) of each participant was calculated as the product of intensity level (MET) and duration (hours) of exercise. The participants were classified into two groups for data analysis based on the median weekly exercise volume: inactive () and moderate/high ( MET-h).
The weight and height of each participant were measured by trained staff using an auto-anthropometer (KN-5000A, Nakamura). BMI was calculated as the weight (in kilograms) divided by the square of the height (in meters).
Outcome Ascertainment
A total of 125,537 participants without hypertension at baseline were followed up, and the incident hypertension was identified in accompanying medical examinations when the participants visited the clinical center. Incident hypertension was defined as an , , or self-reported physician-diagnosed hypertension.38 The participants’ SBP and DBP were measured using a computerized auto-mercury sphygmomanometer (Citizen CH-5000) in the morning and after they had been seated at rest for 10 min. The right-arm blood pressure was measured (or the left-arm blood pressure was measured if the right arm was unavailable). If participants exhibited an or , a second measurement was taken 10 min later and the information from the second measurement was used for the data analysis. In addition, participants were required to answer the question: “Have you ever been diagnosed with hypertension?” on the standard self-administered questionnaire survey when they visited the clinical center. If a participant reported having been diagnosed with hypertension but their measured blood pressure was not consistent with the self-reported hypertension status, the self-reported physician-diagnosed hypertension was used. The end point was defined as the first identification of hypertension during subsequent medical examination visits or the final visit if hypertension did not occur over the study period.
Covariates
The details on data collection and quality-control measures have been described in the Technical Reports of the MJ Health Research Foundation20,39 and previous studies.18,19 An overnight fasting blood sample was taken in the morning for a series of laboratory tests. The plasma glucose and lipid profiles were enzymatically determined using a Hitachi 7150 Automated Biochemical Analyzer (before 2005) or Toshiba C8000 Automated Biochemical Analyzer (after 2005). In addition, data regarding the participants’ demographic characteristics, behavioral and lifestyle factors, and medical history were collected through a standard self-administered questionnaire.9,13,14
We included the following covariates in our data analyses: age (years); sex (male or female); education status [lower than high school (), high school (10–12 y), college or university (13–16 y) or postgraduate ()]; marital status [unmarried, married (including remarried or cohabiting), divorced, or widowed]; smoking status [never, ever (smoked at least once but quit later), or current (more than once a week)]; alcohol consumption [seldom (), occasional (1–3 times/wk), or regular ()]; vegetable intake [seldom (), moderate (1–2 servings/d), or frequent ()]; fruit intake [seldom (), moderate (1–2 servings/d), or frequent ()]; occupational exposure to dust or solvent in the workplace (yes or no); physical labor at work [sedentary jobs (e.g., clerk), jobs that are approximately half sedentary and half standing/walking (e.g., nurse), jobs that mostly involve walking and standing (e.g., retail salesperson), or jobs that involve vigorous physical activity (e.g., porter)], diabetes (defined as fasting blood glucose concentration or self-reported physician-diagnosed diabetes); dyslipidemia (a total cholesterol concentration , a triglyceride concentration , or a high-density lipoprotein–cholesterol concentration ); self-reported cardiovascular disease, including stroke (yes or no); any self-reported form of cancer (yes or no); season of medical examination [spring (March–May), summer (June–August), fall (September–November), winter (December–February)]; and calendar year of baseline visit.
Data Analysis
A time-varying Cox regression model was fitted to investigate the association between neighborhood greenness (i.e., NDVI) and incident hypertension. The follow-up time was used as the timescale in the model. All of the variables (except for sex and baseline year) were treated as time-varying variables in the model to account for the changes in these variables during the study period. In addition to a crude model (without any adjustment), three models were developed by gradually adding the aforementioned covariates to investigate the main effects of neighborhood greenness: a) model 1, which was adjusted for age, sex, marital status, and education level; b) model 2, which was adjusted for the covariates in model 1 and for smoking status, alcohol consumption, vegetable intake, fruit intake, occupational exposure, physical labor at work, season, and calendar year at baseline visit; and c) model 3 (the main model), which was adjusted for the covariates in model 2 and for diabetes, dyslipidemia, self-reported cardiovascular disease, and self-reported cancer. Three potential mediators (i.e., , leisure-time PE, and BMI) were also included in the main model to explore whether the association was affected by the potential mediators. A trend test was performed across NDVI categories, with the corresponding category treated as a numeric variable (coded as 1 to 4). Hazard ratios (HRs) and 95% confidence intervals (CIs) for the NDVI were estimated for every 0.1-unit increase in NDVI value or using the first quartile of the NDVI values as the reference. The natural cubic spline function was used to evaluate the shape of the concentration–response relationship between continuous NDVI values and incident hypertension. We used the likelihood ratio test to detect the linearity by comparing the model with the linear term to the model with the linear and the cubic spline terms. We also checked collinearity by calculating correlations among the NDVI and covariates using Spearman correlation coefficients.
Subgroup analyses were further conducted to investigate whether the association was modified by age ( vs. ), sex (male vs. female), education level ( vs. high school or above), smoking status (never vs. ever/current), alcohol consumption (seldom vs. occasional/regular), BMI ( vs. ), leisure-time PE [inactive () vs. moderate/high ( MET-h)], and [ (median) vs. ]. Each potential modifier was examined in a separate model by adding a multiplicative interaction term (i.e., ).
A causal mediation analysis was performed to examine whether the potential mediators (, leisure-time PE, or BMI) mediate the effect of neighborhood greenness on hypertension, whereas the exposure, covariates and the mediator at baseline were selected for data analysis. To start the casual mediation analysis, first, for each potential mediator, we fitted the following two models40: a) outcome regression: a Cox model was fitted for the association of exposure to greenness with hypertension adjusted for the potential mediator; and b) mediator regression: a linear regression model was fitted for the association of exposure to greenness with a continuous mediator ( or BMI) or a logistic regression model for the association of exposure to greenness with a binary mediator (leisure-time PE). Both models were adjusted for the covariates included in the main model. Second, we obtained the estimates of total effect (TE), natural direct effect (NDE), natural indirect effect (NIE), and the proportion mediated (i.e., the extent of the association mediated by that specific mediator) by direct counterfactual imputation estimation41 using the above models, and 95% CIs were estimated by Bootstrap with 5,000 repetitions.42 The causal mediation analysis was conducted using R package CMAverse.40
A series of sensitivity analyses were performed to test the robustness and stability of the association between neighborhood greenness and hypertension. This involved a) using the 2-y average of NDVI values within a circular buffer of and a radius around each spatial point as the indicators of neighborhood greenness9,24; b) using the seasonal average of NDVI values rather than the annual mean of NDVI values as the indicator of exposure to neighborhood greenness to reflect the short-term exposure to greenness; c) excluding participants who had changed their address during follow-up; d) using the annual NDVI value of the year prior to the year of medical examination to investigate whether variation in time windows may affect our main results; e) excluding participants with a follow-up of , given that the development of hypertension is a chronic process; f) using the new definition of hypertension provided by the American College of Cardiology and American Heart Association (i.e., or )43; g) excluding participants with baseline diabetes, dyslipidemia, cardiovascular diseases, and/or cancer, to eliminate potential comorbidity effects; h) further including a city-level random intercept in model 3 to adjust for the cluster effect; i) further adjusting for area-level family income in model 3 to account for the effect of socioeconomic status, where the area-level family income was obtained from National Statistics of Taiwan44; j) using inverse probability weight to account for the selection bias; and k) truncating negative NDVI values to 0 rather than restricting our data to NDVI values .
Statistical analyses were performed using R (version 4.2.0; R Development Core Team). A two-tailed was used to define statistical significance.
Results
A total of 125,537 participants with 442,435 medical records were included in the data analysis. The median follow-up duration was 4.08 y, with an interquartile range (IQR) of 5.17 y. Approximately 55% of participants underwent at least 3 medical examinations, with a median number of 3 (IQR: 2). The median interval of examinations was 3.75 y (IQR: 4.33 y). During the study period, 14,103 incident cases of hypertension were identified over 628,966.58 person-years of follow-up, leading to an incidence rate of 2.24/100 person-years. In addition, 14% of participants moved after a median of 5 y (IQR: 3.75 y) during follow-up. The general characteristics of the participants at baseline and observations during follow-up are shown in Tables 1 and 2. The mean age of the participants at baseline was 37.33 y, and 48.65% were male. The majority had higher levels of education and were nonsmokers and light drinkers. In addition, more than half of the participants were married, remarried, or cohabiting and had a sedentary job. The temporal distribution of the 2-y average NDVI values by year is presented in Figure S1. Overall, the NDVI values remained stable over the years; the values declined slightly from 2001 to 2005, fluctuated somewhat from 2005 to 2011, and increased after 2011.
Table 2.
Characteristics of 316,898 observations during follow-up for 125,537 participants from Taiwan.
| Characteristic | Observations at follow-up visits ()a |
|---|---|
| Age [y ()] | |
| Sex [ (%)] | |
| Male | 155,477 (49.06) |
| Female | 161,421 (50.94) |
| Education [ (%)] | |
| Lower than high school | 26,218 (8.27) |
| High school | 58,983 (18.61) |
| College or university | 182,836 (57.70) |
| Postgraduate | 48,861 (15.42) |
| Marital status [ (%)] | |
| Unmarried | 64,538 (20.37) |
| Married or remarried or cohabiting | 235,932 (74.45) |
| Divorced | 9,583 (3.02) |
| Widowed | 6,845 (2.16) |
| Smoking status [ (%)] | |
| Never | 244,584 (77.18) |
| Former | 18,234 (5.75) |
| Current | 54,080 (17.07) |
| Alcohol consumption [ (%)] | |
| Seldom | 272,431 (85.97) |
| Occasional | 30,984 (9.78) |
| Regular | 13,483 (4.25) |
| Physical labor at work [ (%)] | |
| Sedentary jobs | 219,331 (69.21) |
| Jobs that are approximately half sedentary and half standing/walking | 73,755 (23.27) |
| Jobs that mostly involve walking and standing | 19,978 (6.30) |
| Jobs that involve vigorous physical activity | 3,834 (1.21) |
| Vegetable intake [ (%)] | |
| Seldom | 31,506 (9.94) |
| Moderate | 185,242 (58.45) |
| Frequent | 100,150 (31.60) |
| Fruit intake [ (%)] | |
| Seldom | 82,059 (25.89) |
| Moderate | 186,657 (58.90) |
| Frequent | 48,182 (15.20) |
| Occupational exposure [ (%)]b | |
| Yes | 24,259 (7.66) |
| No | 292,639 (92.34) |
| BMI [ ()] | |
| Systolic blood pressure [mmHg ()] | |
| Diastolic blood pressure [mmHg ()] | |
| Dyslipidemia [ (%)] | 67,398 (21.27) |
| Cardiovascular disease [ (%)] | 12,422 (3.92) |
| Diabetes mellitus [ (%)] | 10,011 (3.16) |
| Cancer [ (%)] | 6,891 (2.17) |
| c | 0.28 (0.15) |
| [ ()] | |
| Season [ (%)] | |
| Spring | 75,965 (23.97) |
| Summer | 92,404 (29.16) |
| Fall | 88,490 (27.92) |
| Winter | 60,039 (18.95) |
Note: Values are presented as for continuous variables with normal distributions and as counts (%) for categorical variables. Data are complete for all variables. BMI, body mass index; IQR, interquartile range; NDVI, normalized difference vegetation index; , particulate matter with an aerodynamic diameter of ; SD, standard deviation.
Characteristics of 316,898 observations during follow-up for 125,537 participants with complete information and without hypertension at baseline.
Classified as exposure to dust or organic solvents in the workplace, established by asking, “Are there any occupational hazards in your workplace?”
Refers the average NDVI values within a buffer in the year of the visit and in the year before the visit. Each value is presented as a median (IQR) owing to the skewed distribution.
Table 3 shows the results of the association of neighborhood greenness with incident hypertension. Compared with the first quartile of NDVI value, the HRs for incident hypertension for the second, third, and fourth quartiles of NDVI were 0.95 (95% CI: 0.91, 1.00), 0.95 (95% CI: 0.90, 0.99), and 0.93 (95% CI: 0.88, 0.97), respectively (model 3). In addition, there was a significant trend in the association of incident hypertension across the categories of NDVI. When NDVI was treated as a continuous variable, each 0.1-unit increase in NDVI was associated with a 24% lower risk of hypertension (0.76; 95% CI: 0.66, 0.87). The association remained stable after including one or more potential mediators in model 3 (Table S1). The concentration–response curve for the association between NDVI values and incident hypertension is approximately linear overall (likelihood ratio test: , ; Figure S2). Figure S3 illustrates the correlation matrix among the greenness and covariates, including age, sex, marital status, education status, smoking status, alcohol drinking, fruit intake, vegetable intake, occupational exposure, physical labor during work, season, year of enrollment, diabetes, dyslipidemia, self-reported cardiovascular disease, self-reported cancer, BMI, , and PE. The corresponding Spearman correlation coefficients were .
Table 3.
Overall association between long-term exposure to neighborhood greenness and incident hypertension in Taiwanese adults ().
| Crude model | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | -Value | HR (95% CI) | -Value | HR (95% CI) | -Value | HR (95% CI) | -Value | |
| 2nd quartile | 0.99 (0.95, 1.04) | 0.78 | 0.97 (0.93, 1.02) | 0.23 | 0.96 (0.91, 1.00) | 0.06 | 0.95 (0.91, 1.00) | 0.04 |
| 3rd quartile | 0.99 (0.95, 1.04) | 0.77 | 0.96 (0.91, 1.00) | 0.08 | 0.95 (0.91, 1.00) | 0.03 | 0.95 (0.90, 0.99) | 0.02 |
| 4th quartile | 1.02 (0.97, 1.07) | 0.46 | 0.93 (0.89, 0.97) | 0.002 | 0.93 (0.88, 0.97) | 0.001 | 0.93 (0.88, 0.97) | 0.001 |
| Trend test | 1.01 (0.99, 1.02) | 0.47 | 0.98 (0.96, 0.99) | 0.002 | 0.98 (0.96, 0.99) | 0.002 | 0.98 (0.96, 0.99) | 0.002 |
| Per 0.1-unit increase in | 1.00 (0.87, 1.15) | 0.96 | 0.74 (0.65, 0.85) | 0.75 (0.65, 0.86) | 0.76 (0.66, 0.87) | |||
Note: was the 2-y average value of the NDVI within a buffer and the quartile cutoffs were 0.23, 0.28, and 0.38. Time-varying Cox regression model was used. Crude model: without adjustment. Model 1 was adjusted for age, sex, marital status, and education status. Model 2 was adjusted for model 1’s covariates plus smoking status, alcohol consumption, fruit intake, vegetable intake, occupational exposure, physical labor during work, season, and year of enrollment. Model 3 was adjusted for model 2’s covariates plus diabetes, dyslipidemia, self-reported cardiovascular disease, and self-reported cancer. Data are complete for all variables. CI, confidence interval; HR, hazard ratio; NDVI, normalized difference vegetation index. was considered statistically significant.
The results of the stratified analysis for the potential modifiers are shown in Table 4. No statistically significant interactions were observed when data analyses were stratified by baseline age, smoking status, alcohol consumption, BMI, leisure-time PE, and . However, the inverse association between neighborhood greenness and hypertension was more pronounced among males and participants with an education level of above high school (both ).
Table 4.
Stratified analysis on associations between long-term exposure to neighborhood greenness and incident hypertension in Taiwanese adults ().
| Subgroup | Cases/participants | HR (95% CI) | |
|---|---|---|---|
| Age (y) | |||
| 13,240/123,209 | 0.76 (0.65, 0.88) | 0.48 | |
| 863/2,328 | 0.84 (0.50, 1.41) | ||
| Sex | |||
| Male | 9,108/61,076 | 0.72 (0.60, 0.86) | |
| Female | 4,995/64,461 | 0.89 (0.71, 1.12) | |
| Education | |||
| 2,960/11,992 | 1.09 (0.82, 1.44) | 0.02 | |
| 11,143/113,545 | 0.69 (0.59, 0.82) | ||
| Smoking status | |||
| Never | 9,809/94,743 | 0.80 (0.67, 0.94) | 0.08 |
| Ever/current | 4,294/30,794 | 0.69 (0.54, 0.89) | |
| Alcohol consumption | |||
| Seldom | 11,337/109,103 | 0.79 (0.68, 0.92) | 0.09 |
| Occasional/regular | 2,766/16,434 | 0.68 (0.50, 0.93) | |
| BMI () | |||
| 8,282/98,593 | 0.80 (0.67, 0.96) | 0.06 | |
| 5,821/26,944 | 0.74 (0.60, 0.93) | ||
| PE () | |||
| 6,192/62,933 | 0.69 (0.56, 0.85) | 0.41 | |
| 7,911/62,604 | 0.81 (0.67, 0.98) | ||
| () | |||
| 6,923/61,099 | 0.76 (0.64, 0.90) | 0.81 | |
| 7,180/64,438 | 0.72 (0.56, 0.92) | ||
Note: Neighborhood greenness was estimated as the 2-y average value of the NDVI within a (continuous). Time-varying Cox regression model was used. All models were adjusted for age (except for in age-stratified analyses), sex (except for in sex-stratified analyses), marital status, education status (except for in education level-stratified analyses), smoking status (except for in smoking-stratified analyses), alcohol consumption (except for in drinking-stratified analyses), fruit intake, vegetable intake, occupational exposure, physical labor during work, season, year of enrollment, diabetes, dyslipidemia, self-reported cardiovascular disease, and self-reported cancer. Data are complete for all variables. BMI, body mass index; CI, confidence interval; HR, hazard ratio; MET, metabolic equivalent of task; NDVI, normalized difference vegetation index; PE, physical exercise (leisure-time); , particulate matter with an aerodynamic diameter of . was considered statistically significant.
Figure 2 shows the potential mediating effects of air pollution, leisure-time PE, and BMI on the association between neighborhood greenness and hypertension. The estimate of the NIE of BMI was 0.998 (95% CI: 0.996, 1.000) (), which accounts for 8.90% of the association between NDVI and incident hypertension, whereas the natural indirect effects for and leisure-time PE on hypertension were not statistically significant.
Figure 2.
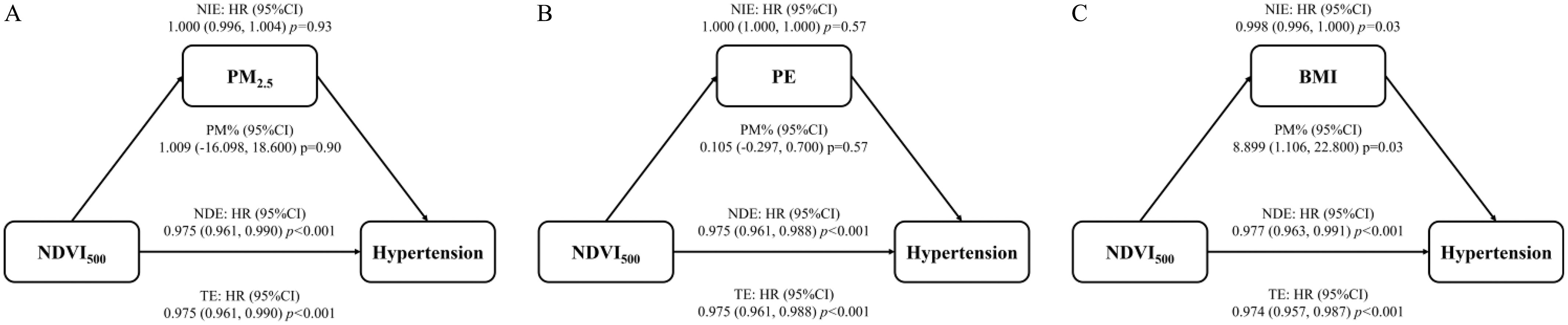
Mediation analyses of whether the associations between neighborhood greenness and incident hypertension in Taiwanese adults are explained by (A) air pollution exposure, (B) leisure-time PE, and (C) BMI (). was the 2-y average value of the NDVI within a buffer (continuous). and BMI were treated as continuous variables, whereas PE was treated as a dichotomous variable ( vs. MET-h/week). Two models were fitted to calculate the estimates (NIE, NDE, TE, and PM%). Outcome regression: a Cox model for the association of exposure to greenness with hypertension adjusted for the potential mediator; Mediator regression: a linear regression model for the association of exposure to greenness with a continuous mediator ( or BMI), or a logistic regression model for the association of exposure to greenness with a binary mediator (leisure-time PE). All models were adjusted for age, sex, marital status, education status, smoking status, alcohol consumption, fruit intake, vegetable intake, occupational exposure, physical labor during work, season, year of enrollment, diabetes, dyslipidemia, self-reported cardiovascular disease, and self-reported cancer. Data are complete for all variables. Note: BMI, body mass index; CI, confidence interval; HR, hazard ratio; MET, metabolic equivalent of task; NDE, natural direct effect; NDVI, normalized difference vegetation index; NIE, natural indirect effect; PE, physical exercise (leisure-time); PM%, proportion mediated percentage; , particulate matter with an aerodynamic diameter of ; TE, total effect. was considered statistically significant.
Tables S2 and S3 show that the associations remained robust after using average NDVI values within different buffers (Table S2, Sensitivity analyses 1 and 2) and time windows (Table S2, Sensitivity analyses 3 and 5), excluding participants with a follow-up of (Table S2, Sensitivity analysis 6), further adjusting for a city-level random intercept or area-level family income (Table S3, Sensitivity analyses 9 and 10), using inverse probability weight (Table S3, Sensitivity analysis 11), and truncating negative NDVI values to 0 (Table S3, Sensitivity analysis 12). However, the associations were weakened after excluding participants who changed address during follow-up (Table S2, Sensitivity analysis 4), using the new definition of hypertension (Table S3, Sensitivity analysis 7), and excluding participants who had comorbidities at baseline (Table S3, Sensitivity analysis 8).
Discussion
The findings from this large Taiwanese cohort show that long-term exposure to neighborhood greenness, as measured by the NDVI, is associated with a lower risk of incident hypertension. This association is significantly stronger among males and participants with an education level of above high school. The finding also suggests that BMI may mediate the effects of exposure to greenness on hypertension.
Our findings are consistent with most cross-sectional studies that have reported the beneficial effects of exposure to greenness on hypertension.5,6,9,16 Our study found a 24% lower risk of hypertension for each 0.1-unit increase in NDVI within a buffer. This result is comparable to previous cross-sectional studies that identified 17%–36% lower odds of hypertension associated with NDVI among adults and children.8,10,15,45 On the other hand, the effects observed in other studies among older adults were generally stronger, showing 49%–85% lower odds.6,16,46 However, few studies have adopted a longitudinal cohort design, which typically can provide stronger evidence than cross-sectional studies. The results from several cohort studies are inconsistent with each other. The Sax Institute’s 45 and Up Study found that lower odds of incident hypertension ( 0.993; 95% CI: 0.989, 0.997) was associated with a 1% increase in exposure to tree canopy but not with exposure to total green space.13 A study in Kaunas, the second largest city in Lithuania, reported no significant association between incident hypertension and distance to green space.12 Another study based on the Stockholm Diabetes Prevention Program cohort failed to detect any association between NDVI and incident hypertension.11 A recent cohort study conducted among older Chinese adults ( of age) found the protective effects of greenness on incident hypertension, but these effects were only observed in the third tertile of NDVI when compared with the first tertile of NDVI (0.51; 95% CI: 0.40, 0.64). In the present study, our stratified analysis shows that the negative association was not statistically significant among participants of age. This is possibly due to the small sample size of this subgroup in our study. Overall, it may be difficult to directly compare our results with other studies owing to heterogeneities in study populations, study regions, and exposure assessments. Furthermore, most previous studies did not account for lifestyle behavioral factors, which are also potential confounders.
We did not observe that age modified the association of exposure to greenness with hypertension (Table 4), similar to what was found in a previous study.47 However, our stratified analyses observed that the inverse association between exposure to greenness and hypertension was significantly stronger in males than in females. Previous findings concerning the effect modifier of sex on the association between greenness and hypertension are inconclusive. Yang et al. found a stronger negative association between exposure to community greenness and hypertension in Chinese females than in males,9 whereas three other studies conducted in China found that the beneficial effects of exposure to greenness on hypertension are more pronounced in males than in females.16,47,48 However, other studies have found no clear evidence for effect modification by sex.6,8,14 Possible explanations for these mixed results of analyses stratified by sex include variations in lifestyles and exposure patterns (i.e., participants may be exposed to greenness during their daily activities), which may be partly influenced by travel mode, occupation, child-rearing activities, and perceptions of nature.49,50 In addition, education, a proxy for socioeconomic status, was detected as a significant effect modifier in the present study, with exposure to greenness having more protective effects of greenness against hypertension in participants with higher education levels than in those with lower education levels. The evidence for the effect modification of socioeconomic status on greenness–hypertension association is limited. A few studies have found no effect modification by education or household income levels,6,8,9 whereas another study found that compared with participants living in high-income neighborhoods, there were more substantial protective effects of exposure to greenness on hypertension in participants living in low- and medium-income neighborhoods.5 Similar to our findings, a Canadian cohort study found that exposure to greenness had stronger effects on participants with a higher income and education level, although the outcome was nonaccidental death.51 As suggested by the study by Pinault et al.,52 this may be because people with higher socioeconomic status tend to spend more time in contact with nature and participate in more leisure-time activities, thus increasing their chance of exposure to greenness. This might be the reason for the more beneficial effects of greenness observed among affluent individuals.
Although the mechanism underlying the association between greenness exposure and hypertension remains unclear, several pathways have been proposed and explored. Reduced air pollution is a potential mediator of this association, given that vegetation can decrease concentrations of air pollutants through deposition, dispersion, and modification,25 thus alleviating the adverse effects of air pollution on human health. Exposure to air pollution [e.g., , (particulate matter with an aerodynamic diameter of less than ) , and nitrogen dioxide ()] has been found to explain of the association between greenness and hypertension.9,10 It was also found that exposure to completely mediated the association of exposure to greenness with hypertension in urban areas but only partially mediated the association in rural areas.46 However, we did not observe the mediating effect of in our study. Similarly, a study found no indirect effects of on the association between NDVI and SPB.45 Another study conducted among children and adolescents in China found no evidence that exposure to air pollution (i.e., and ) mediated the association between greenness with hypertension.15 Further studies are warranted for the correlation between the specific pollutants and neighborhood greenness. Exposure to greenness was found to be associated with increasing leisure-time PE,27 which is known to be beneficial to human health.28 However, we did not find mediating effects of PE in the present study, which was in line with other studies.9,10 In contrast, one study focusing on middle-aged and older adults found that approximately half of the association between NDVI with hypertension was mediated by PE.16 Previous studies suggested that residing in greener areas was associated with lower adiposity,29,30 which is a well-documented risk factor for hypertension. Our findings and previous studies support the suggestion that the greenness–hypertension association is partially explained by reducing adiposity.6,9 However, other studies have failed to find evidence of mediation for BMI.8,15 Further studies are needed to investigate the mediating effects on the association between greenness and hypertension.
Our study adds value to the emerging evidence on the effects of exposure to greenness on hypertension and the mediating effects in the pathways linking greenness and hypertension, using data from a large-scale prospective cohort. The large sample size allowed us to obtain stable and precise estimates. In addition, the longitudinal design of this study allowed us to develop time-varying metrics for greenness exposure and various covariates. We observed a median yearly change in the NDVI of 1.93% among our participants. This change was more pronounced, at 2.94%, for participants who relocated during the follow-up period. Furthermore, certain covariates, such as age and physical activity, can change significantly over time and substantially influence blood pressure. Therefore, a longitudinal approach is crucial for accurately assessing the relationship between greenness and hypertension, as it enables us to prospectively consider both greenness exposure and a comprehensive range of covariates.
On the other hand, this study has certain limitations. First, the participants’ blood pressures were measured only once at each visit if their blood pressures fell within the normal range. This was not strictly in accordance with clinical guidelines, which require repeated measurements. However, if the participants had an or at the first measurement, a second measurement was taken to minimize the “white coat” effect. In addition, the census date for a hypertension participant was the medical examination date in the MJ Health Management Institution. We are not sure how long the participant had hypertension before the examination. Second, it was suggested that greater exposure to greenness was associated with reduced exposure to noise and heat, decreased psychological stress, and increased social interaction, which are thought to be the potential mechanisms underlying the association between greenness and hypertension. Heat waves have also been reported to have an interactive influence on the health effects of greenness.53 However, such information is not available or cannot be considered in the present study. Further studies are warranted to investigate the underlying mechanisms. Third, NDVI is sensitive to season, but our sensitivity analysis indicated that using seasonal NDVI as greenness exposure yields similar results to annual NDVI as greenness exposure. Fourth, although NDVI has been used in most studies and was more accessible for comparison, it does not tell the difference in vegetations’ structure, type, usability, and quality. There are studies that show inconsistent correlations between NDVI-based greenness and perceptions of greenness. For instance, one study found a relatively high correlation () between environmental psychologists’ ratings of greenness around residents’ areas using the Likert scale and the NDVI,54 whereas another study found a lack of agreement between a dichotomized greenness score based on 17 perceived items and a dichotomized NDVI (Cohen’s , ).55 Fifth, exposure patterns may reflect participants’ actual use of greenness but cannot be tracked in our study owing to the large sample size. In particular, although we used and exposure buffers around residences to cover participants’ leisure-time activities in areas within a 5–15 min walk from their homes, further studies using advanced technology are needed to track participants’ exposure patterns and thereby obtain more precise measurements of their exposure to greenness. Sixth, the resolution of NDVI data (i.e., ) used in our study is not relatively high. Further studies using data with higher resolution like data from Landsat 7 and 8 were warranted to validate our findings. Higher resolution data help to reduce the exposure misclassification and improve accuracy of greenness exposure, although processing higher resolution data is computationally intensive, particularly when dealing with time-varying exposure data. However, one study compared NDVI from MODIS (), Landsat 8 (), Sentinel-2 (), and the National Agricultural Imagery Program (NAIP, ) around the address of 31,328 children in the Greater Boston Area in 2016.56 The study found that the distribution of NDVI from MODIS was comparable to that from Landsat 8. When the buffer sizes are expanded from a 50- to a radius, the agreement in the quantiles of NDVI from Sentinel 2, Landsat 8, and MODIS with respect to NAIP NDVI increases. At the same time, the differences in the extent of misclassification between NDVI at coarser resolution reduced. Given that we chose a buffer size of a radius in our main analysis, using coarser NDVI (i.e., MODIS NDVI) should not be a critical issue, and it is also cost effective and less time consuming. Seventh, we acknowledge that income is a potential confounder that is associated with greenness and health outcomes in previous studies,51,57 but we were unable to adjust for this in our analyses owing to the significant amount of missing data on individual income. Instead, we included personal education, an important indicator of socioeconomic status, in our main analysis. Our sensitivity analysis adjusting for area-level household income indicated results similar to those of our main analysis (Table S3, Sensitivity analysis 10). Finally, the participants were generally well educated (70.58% of participants in our study and of Taiwanese adults in 201058 had an education of college or above). Therefore, we should be cautious when generalizing our findings to other populations. However, the main characteristics of the participants such as sex and marital status were generally comparable with those of the general population in Taiwan (48.65% vs. 49.47% for males, and 32.00% vs. 32.97% for the unmarried).
In summary, living in an area with a higher level of greenness was associated with a lower risk of developing hypertension. The protective effect of exposure to greenness was more pronounced in males and people with higher education levels. The association between greenness and hypertension was mediated by a decrease in BMI, although the proportion mediated was small. Given the potential benefits of exposure to greenness on health, the findings from this study will be valuable for urban planning and development, especially in areas with high population densities.
Supplementary Material
Acknowledgments
We thank the MJ Health Research Foundation for the authorization of using MJ health data (authorization code MJHR2019006A). Any interpretation or conclusion related to this manuscript does not represent the views of the MJ Health Research Foundation.
This work was supported by the Research Grants Council General Research Fund of University Grant Committee of Hong Kong (14600522) and the City University of Hong Kong startup project (9610613), both to Xiang Qian. Ms. Yi Qian Zeng and Ms. Xue Liang are supported by the Ph.D. Studentship of the Chinese University of Hong Kong. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conclusions and opinions are those of the individual authors and do not necessarily reflect the policies or views of EHP Publishing or the National Institute of Environmental Health Sciences.
References
- 1.GBD 2017 Risk Factor Collaborators. 2018. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159):1923–1994, PMID: , 10.1016/S0140-6736(18)32225-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.NCD-RisC (NCD Risk Factor Collaboration). 2021. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 398(10304):957–980, PMID: , 10.1016/S0140-6736(21)01330-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO (World Health Organization). 2021. Hypertension. [Fact sheet.] https://www.who.int/news-room/fact-sheets/detail/hypertension [accessed 10 November 2022].
- 4.WHO. 2016. Urban Green Spaces and Health. https://apps.who.int/iris/handle/10665/345751 [accessed 15 November 2022].
- 5.Brown SC, Lombard J, Wang K, Byrne MM, Toro M, Plater-Zyberk E, et al. 2016. Neighborhood greenness and chronic health conditions in Medicare beneficiaries. Am J Prev Med 51(1):78–89, PMID: , 10.1016/j.amepre.2016.02.008. [DOI] [PubMed] [Google Scholar]
- 6.Bauwelinck M, Zijlema WL, Bartoll X, Vandenheede H, Cirach M, Lefebvre W, et al. 2020. Residential urban greenspace and hypertension: a comparative study in two European cities. Environ Res 191:110032, PMID: , 10.1016/j.envres.2020.110032. [DOI] [PubMed] [Google Scholar]
- 7.Bijnens EM, Nawrot TS, Loos RJ, Gielen M, Vlietinck R, Derom C, et al. 2017. Blood pressure in young adulthood and residential greenness in the early-life environment of twins. Environ Health 16(1):53, PMID: , 10.1186/s12940-017-0266-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dzhambov AM, Markevych I, Lercher P. 2018. Greenspace seems protective of both high and low blood pressure among residents of an Alpine valley. Environ Int 121(pt 1):443–452, PMID: , 10.1016/j.envint.2018.09.044. [DOI] [PubMed] [Google Scholar]
- 9.Yang BY, Markevych I, Bloom MS, Heinrich J, Guo Y, Morawska L, et al. 2019. Community greenness, blood pressure, and hypertension in urban dwellers: the 33 Communities Chinese Health Study. Environ Int 126:727–734, PMID: , 10.1016/j.envint.2019.02.068. [DOI] [PubMed] [Google Scholar]
- 10.Xiao X, Yang BY, Hu LW, Markevych I, Bloom MS, Dharmage SC, et al. 2020. Greenness around schools associated with lower risk of hypertension among children: findings from the Seven Northeastern Cities Study in China. Environ Pollut 256:113422, PMID: , 10.1016/j.envpol.2019.113422. [DOI] [PubMed] [Google Scholar]
- 11.Persson Å, Pyko A, Lind T, Bellander T, Pershagen G, Eriksson C, et al. 2019. Long-term exposure to residential greenness and development of hypertension in Stockholm County. Environ Epidemiol 3:310, 10.1097/01.EE9.0000609380.20557.1f. [DOI] [Google Scholar]
- 12.Braziene A, Tamsiunas A, Luksiene D, Radisauskas R, Andrusaityte S, Dedele A, et al. 2020. Association between the living environment and the risk of arterial hypertension and other components of metabolic syndrome. J Public Health (Oxf) 42(2):e142–e149, PMID: , 10.1093/pubmed/fdz046. [DOI] [PubMed] [Google Scholar]
- 13.Astell-Burt T, Feng X. 2020. Urban green space, tree canopy and prevention of cardiometabolic diseases: a multilevel longitudinal study of 46 786 Australians. Int J Epidemiol 49(3):926–933, PMID: , 10.1093/ije/dyz239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhou W, Wang W, Zhou F, Chen W, Ling L. 2022. The effects of greenness exposure on hypertension incidence among Chinese oldest-old: a prospective cohort study. Environ Health 21(1):66, PMID: , 10.1186/s12940-022-00876-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Luo YN, Yang BY, Zou Z, Markevych I, Browning MHEM, Heinrich J, et al. 2022. Associations of greenness surrounding schools with blood pressure and hypertension: a nationwide cross-sectional study of 61,229 children and adolescents in China. Environ Res 204(pt A):112004, PMID: , 10.1016/j.envres.2021.112004. [DOI] [PubMed] [Google Scholar]
- 16.Jia X, Yu Y, Xia W, Masri S, Sami M, Hu Z, et al. 2018. Cardiovascular diseases in middle aged and older adults in China: the joint effects and mediation of different types of physical exercise and neighborhood greenness and walkability. Environ Res 167:175–183, PMID: , 10.1016/j.envres.2018.07.003. [DOI] [PubMed] [Google Scholar]
- 17.Iyer HS, James P, Valeri L, Bajunirwe F, Nankya-Mutyoba J, Njelekela M, et al. 2021. Neighborhood greenness and burden of non-communicable diseases in sub-Saharan Africa: A: a multi-country cross-sectional study. Environ Res 196:110397, PMID: , 10.1016/j.envres.2020.110397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang Z, Chang LY, Lau AKH, Chan TC, Chieh Chuang Y, Chan J, et al. 2017. Satellite-based estimates of long-term exposure to fine particulate matter are associated with C-reactive protein in 30 034 Taiwanese adults. Int J Epidemiol 46(4):1126–1136, PMID: , 10.1093/ije/dyx069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zeng Y, Lin C, Guo C, Bo Y, Chang LY, Lau AKH, et al. 2021. Combined effects of chronic PM2.5 exposure and habitual exercise on renal function and chronic kidney disease: a longitudinal cohort study. Int J Hyg Environ Health 236:113791, PMID: , 10.1016/j.ijheh.2021.113791. [DOI] [PubMed] [Google Scholar]
- 20.MJ Health Foundation. 2016. The Introduction of MJ Health Database. MJ Health Research Foundation Technical Report, MJHRF-TR-01. http://www.mjhrf.org/file/file/report/MJHRF-TR-01%20MJ%20Health%20Database.pdf [accessed 20 July 2020].
- 21.Didan K, Munoz AB, Solano R, Huete A. 2015. MODIS Vegetation Index User’s Guide (MOD13 Series). Tucson, AZ: University of Arizona, Vegetation Index and Phenology Lab. https://lpdaac.usgs.gov/documents/103/MOD13_User_Guide_V6.pdf [accessed 30 November 2021]. [Google Scholar]
- 22.NASA (National Aeronautics and Space Administration). 2019. Goddard Space Flight Center. Validation at stage 3 has been achieved for the MODIS Vegetation Index (VI) product suite. https://modis-land.gsfc.nasa.gov/ValStatus.php?ProductID=MOD13 [accessed 27 December 2022].
- 23.Gerber F, de Jong R, Schaepman ME, Schaepman-Strub G, Furrer R. 2018. Predicting missing values in spatio-temporal remote sensing data. IEEE Trans Geosci Remote Sens 56(5):2841–2853, 10.1109/TGRS.2017.2785240. [DOI] [Google Scholar]
- 24.Chen H, Burnett RT, Bai L, Kwong JC, Crouse DL, Lavigne E, et al. 2020. Residential greenness and cardiovascular disease incidence, readmission, and mortality. Environ Health Perspect 128(8):087005, PMID: , 10.1289/EHP6161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Diener A, Mudu P. 2021. How can vegetation protect us from air pollution? A critical review on green spaces’ mitigation abilities for air-borne particles from a public health perspective - with implications for urban planning. Sci Total Environ 796:148605, PMID: , 10.1016/j.scitotenv.2021.148605. [DOI] [PubMed] [Google Scholar]
- 26.Guo C, Zeng Y, Chang LY, Yu Z, Bo Y, Lin C, et al. 2020. Independent and opposing associations of habitual exercise and chronic PM2.5 exposures on hypertension incidence. Circulation 142(7):645–656, PMID: , 10.1161/CIRCULATIONAHA.120.045915. [DOI] [PubMed] [Google Scholar]
- 27.Mytton OT, Townsend N, Rutter H, Foster C. 2012. Green space and physical activity: an observational study using Health Survey for England data. Health Place 18(5):1034–1041, PMID: , 10.1016/j.healthplace.2012.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.DHHS (U.S. Department of Health and Human Services). 2018. Physical Activity Guidelines for Americans, 2nd ed. https://health.gov/our-work/physical-activity/current-guidelines [accessed 10 December 2022].
- 29.Sarkar C. 2017. Residential greenness and adiposity: findings from the UK Biobank. Environ Int 106:1–10, PMID: , 10.1016/j.envint.2017.05.016. [DOI] [PubMed] [Google Scholar]
- 30.Jiang J, Xiang Z, Liu F, Li N, Mao S, Xie B, et al. 2022. Associations of residential greenness with obesity and BMI level among Chinese rural population: findings from the Henan Rural Cohort Study. Environ Sci Pollut Res Int 29(49):74294–74305, PMID: , 10.1007/s11356-022-20268-0. [DOI] [PubMed] [Google Scholar]
- 31.WHO. 1997. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation on Obesity. https://apps.who.int/iris/handle/10665/63854 [accessed 16 August 2023].
- 32.Lin C, Li Y, Yuan Z, Lau AKH, Li C, Fung JCH, et al. 2015. Using satellite remote sensing data to estimate the high-resolution distribution of ground-level PM2.5. Remote Sens Environ 156:117–128, 10.1016/j.rse.2014.09.015. [DOI] [Google Scholar]
- 33.Lin CQ, Liu G, Lau AKH, Li Y, Li CC, Fung JCH, et al. 2018. High-resolution satellite remote sensing of provincial PM2.5 trends in China from 2001 to 2015. Atmos Environ 180:110–116, 10.1016/j.atmosenv.2018.02.045. [DOI] [Google Scholar]
- 34.Liu Y. 2014. Monitoring PM2.5 from space for health: past, present, and future directions. EM (Pittsburgh Pa) 6:6–10. [Google Scholar]
- 35.Lin C, Li Y, Lau AKH, Deng X, Tse TKT, Fung JCH, et al. 2016. Estimation of long-term population exposure to PM2.5 for dense urban areas using 1-km MODIS data. Remote Sens Environ 179:13–22, 10.1016/j.rse.2016.03.023. [DOI] [Google Scholar]
- 36.Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. 2000. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 32(suppl 9):S498–S504, PMID: , 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- 37.Wen CP, Wai JPM, Tsai MK, Yang YC, Cheng TYD, Lee MC, et al. 2011. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 378(9798):1244–1253, PMID: , 10.1016/S0140-6736(11)60749-6. [DOI] [PubMed] [Google Scholar]
- 38.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. 2003. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 42(6):1206–1252, PMID: , 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 39.Wang ML. 2016. MJ Health Screening Equipment Use and Replacement Records, MJ Health Research Foundation Technical Report, MJHRF-TR-06. http://www.mjhrf.org/file/file/report/MJHRF-TR-06%20Screening%20Equipment.pdf [accessed 20 July 2020].
- 40.Shi B, Choirat C, Coull BA, VanderWeele TJ, Valeri L. 2021. CMAverse: a suite of functions for reproducible causal mediation analyses. Epidemiology 32(5):e20–e22, PMID: , 10.1097/EDE.0000000000001378. [DOI] [PubMed] [Google Scholar]
- 41.Vansteelandt S, Bekaert M, Lange T. 2012. Imputation strategies for the estimation of natural direct and indirect effects. Epidemiol Methods 1(1):131–158, 10.1515/2161-962X.1014. [DOI] [PubMed] [Google Scholar]
- 42.Schomaker M, Heumann C. 2018. Bootstrap inference when using multiple imputation. Stat Med 37(14):2252–2266, PMID: , 10.1002/sim.7654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2018. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 71(6):1269–1324, PMID: , 10.1161/HYP.0000000000000066. [DOI] [PubMed] [Google Scholar]
- 44.National Statistics, R.O.C. (Taiwan). 2023. The survey of family income and expenditure. [In Chinese.] https://www.stat.gov.tw/ [accessed 4 August 2023].
- 45.Chien JW, Wu C, Chan CC. 2022. The association of hypertension and prehypertension with greenness and PM2.5 in urban environment. Sci Total Environ 821:153526, PMID: , 10.1016/j.scitotenv.2022.153526. [DOI] [PubMed] [Google Scholar]
- 46.Huang B, Xiao T, Grekousis G, Zhao H, He J, Dong G, et al. 2021. Greenness-air pollution-physical activity-hypertension association among middle-aged and older adults: evidence from urban and rural China. Environ Res 195:110836, PMID: , 10.1016/j.envres.2021.110836. [DOI] [PubMed] [Google Scholar]
- 47.Jiang J, Chen G, Li B, Lu Y, Guo Y, Li S, et al. 2020. Does long-term green space exposure improve hypertension and blood pressure? The Henan Rural Cohort Study. SSRN. 10.2139/ssrn.3667846. [DOI]
- 48.Li G, Zhang H, Hu M, He J, Yang W, Zhao H, et al. 2022. Associations of combined exposures to ambient temperature, air pollution, and green space with hypertension in rural areas of Anhui Province, China: a cross-sectional study. Environ Res 204(pt D):112370, PMID: , 10.1016/j.envres.2021.112370. [DOI] [PubMed] [Google Scholar]
- 49.Wu J, Xu Z, Jin Y, Chai Y, Newell J, Ta N, et al. 2022. Gender disparities in exposure to green space: an empirical study of suburban Beijing. Landsc Urban Plan 222:104381, 10.1016/j.landurbplan.2022.104381. [DOI] [Google Scholar]
- 50.Fernández Núñez MB, Campos Suzman L, Maneja R, Bach A, Marquet O, Anguelovski I, et al. 2022. Gender and sex differences in urban greenness’ mental health benefits: a systematic review. Health Place 76:102864, PMID: , 10.1016/j.healthplace.2022.102864. [DOI] [PubMed] [Google Scholar]
- 51.Crouse DL, Pinault L, Balram A, Hystad P, Peters PA, Chen H, et al. 2017. Urban greenness and mortality in Canada’s largest cities: a national cohort study. Lancet Planet Health 1(7):e289–e297, PMID: , 10.1016/S2542-5196(17)30118-3. [DOI] [PubMed] [Google Scholar]
- 52.Pinault L, Fioletov V. 2017. Sun exposure, sun protection and sunburn among Canadian adults. Health Rep 28(5):12–19, PMID: . [PubMed] [Google Scholar]
- 53.Zhou W, Wang Q, Li R, Kadier A, Wang W, Zhou F, et al. 2023. Combined effects of heatwaves and air pollution, green space and blue space on the incidence of hypertension: a national cohort study. Sci Total Environ 867:161560, PMID: , 10.1016/j.scitotenv.2023.161560. [DOI] [PubMed] [Google Scholar]
- 54.Rhew IC, Vander Stoep A, Kearney A, Smith NL, Dunbar MD. 2011. Validation of the normalized difference vegetation index as a measure of neighborhood greenness. Ann Epidemiol 21(12):946–952, PMID: , 10.1016/j.annepidem.2011.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Leslie E, Sugiyama T, Ierodiaconou D, Kremer P. 2010. Perceived and objectively measured greenness of neighbourhoods: are they measuring the same thing? Landsc Urban Plan 95(1–2):28–33, 10.1016/j.landurbplan.2009.11.002. [DOI] [Google Scholar]
- 56.Jimenez RB, Lane KJ, Hutyra LR, Fabian MP. 2022. Spatial resolution of normalized difference vegetation index and greenness exposure misclassification in an urban cohort. J Expo Sci Environ Epidemiol 32(2):213–222, PMID: , 10.1038/s41370-022-00409-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Mitchell R, Popham F. 2008. Effect of exposure to natural environment on health inequalities: an observational population study. Lancet 372(9650):1655–1660, PMID: , 10.1016/S0140-6736(08)61689-X. [DOI] [PubMed] [Google Scholar]
- 58.National Statistics Republic of China (Taiwan). 2010. Population and housing census. [In Chinese.] https://www.stat.gov.tw/News_Content.aspx?n=2752&s=88005 [accessed 22 July 2023].
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.