

Abstract
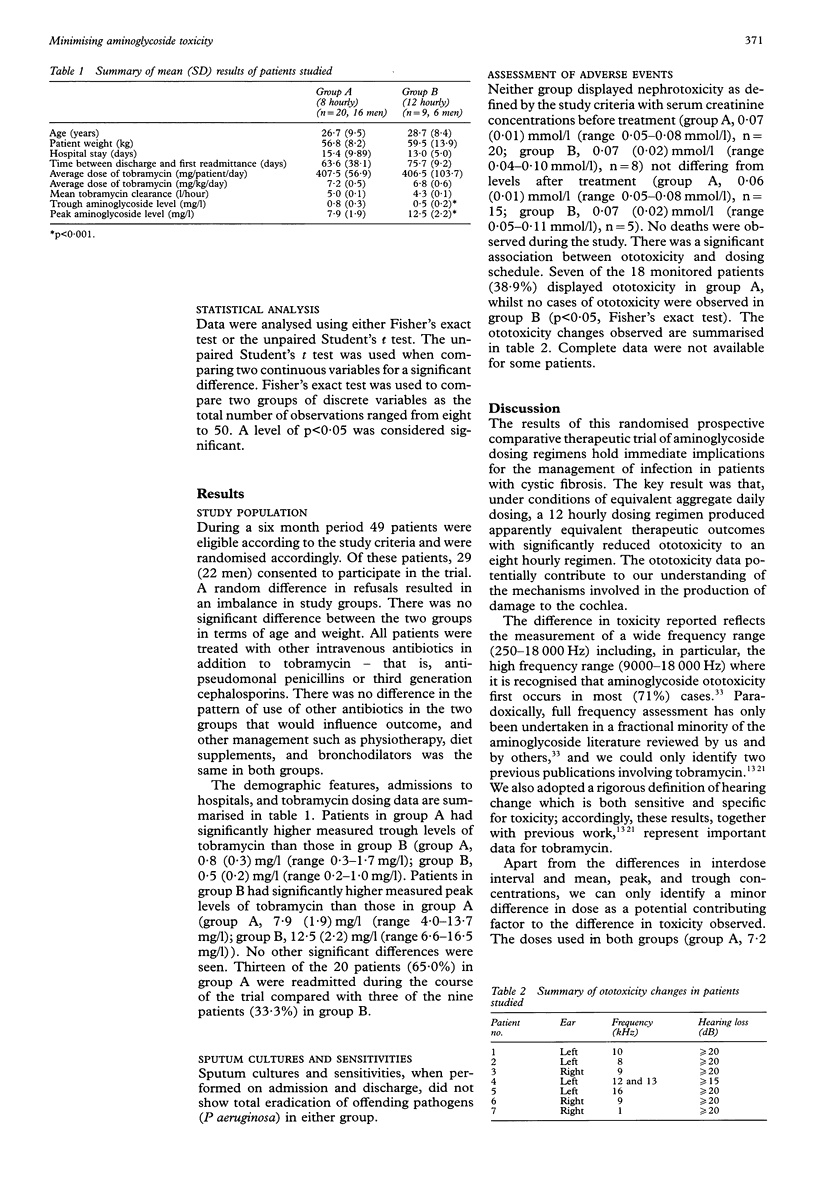
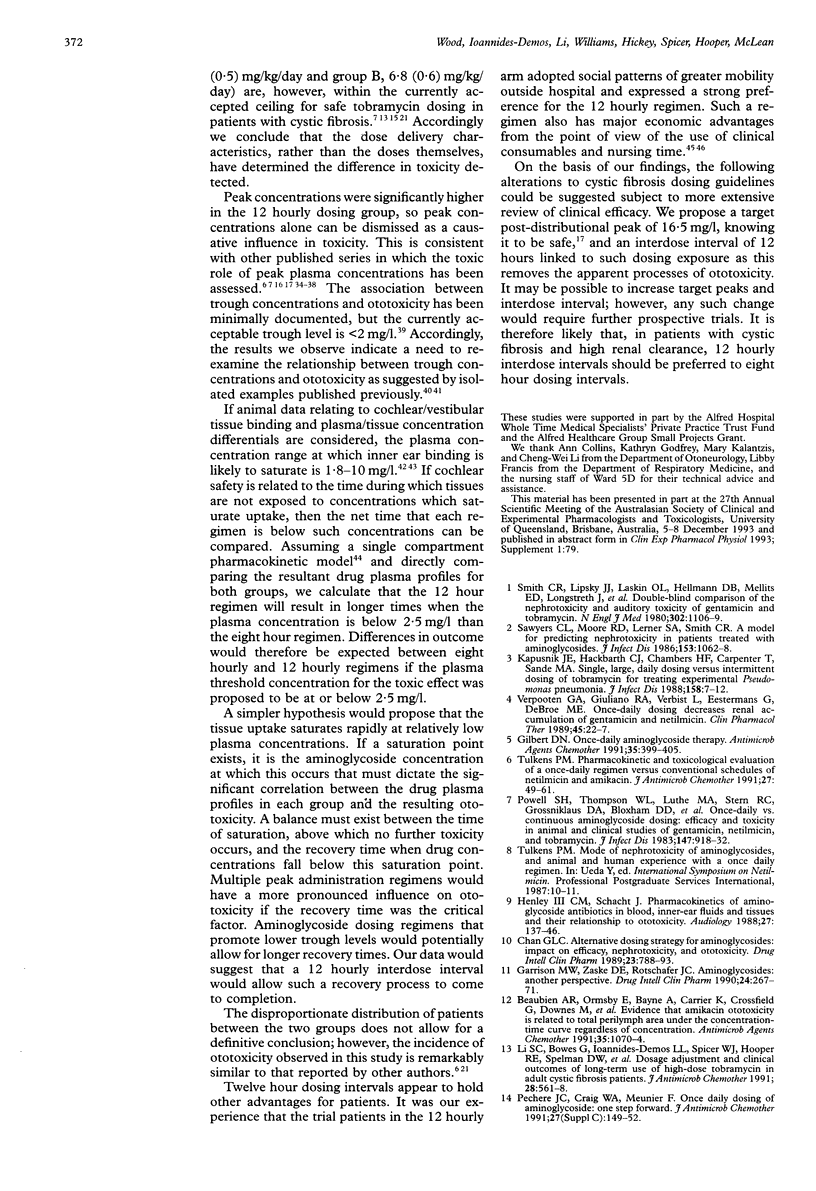
BACKGROUND: There is evidence that administration of higher doses of aminoglycosides given less frequently improves the bactericidal effect and reduces the potential to cause side effects. To investigate this, a prospectively randomised open label therapeutic trial was undertaken in stratified groups of patients with cystic fibrosis to examine the efficacy and toxic potential of an aminoglycoside dosing regimen designed to generate high peak drug concentrations at 12 hourly intervals compared with conventional dosing at eight hourly intervals. METHODS: Patients in group A received tobramycin eight hourly using a dose aimed at generating a peak concentration of 10 mg/l with trough concentrations below 2 mg/l, and those in group B received the total daily dose required to achieve eight hourly target concentrations administered as two equal 12 hourly doses. Clinical outcomes measured and assessed included vestibular symptoms, hearing and renal function, length of hospital stay, readmission rate, and mortality. RESULTS: Twenty nine patients were recruited during a six month period, 20 to group A and nine to group B. The average peak tobramycin level was higher in group B (12.5 (2.2) mg/l) than in group A (7.9 (1.9) mg/l), whilst the average trough level was higher in group A (0.8 (0.3) mg/l) than in group B (0.5 (0.2) mg/l). There was a difference in the number of ototoxic events between patients in group A (seven of 18, 38.9%) and group B (none of eight), but no difference was found in other outcome measures assessed. CONCLUSIONS: These results suggest that 12 hourly high peak aminoglycoside dosing may be less toxic than equivalent eight hourly dosing, without any apparent difference in efficacy.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Attitudes, knowledge and behaviour of general practitioners in relation to HIV infection and AIDS. Commonwealth AIDS Research Grant Committee Working Party. Med J Aust. 1990 Jul 2;153(1):5–12. [PubMed] [Google Scholar]
- Beaubien A. R., Ormsby E., Bayne A., Carrier K., Crossfield G., Downes M., Henri R., Hodgen M. Evidence that amikacin ototoxicity is related to total perilymph area under the concentration-time curve regardless of concentration. Antimicrob Agents Chemother. 1991 Jun;35(6):1070–1074. doi: 10.1128/aac.35.6.1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brushwood D. B. Government liable for failure to monitor a patient's serum gentamicin concentration in an Army hospital. Am J Hosp Pharm. 1992 Jul;49(7):1748–1750. [PubMed] [Google Scholar]
- Fausti S. A., Henry J. A., Schaffer H. I., Olson D. J., Frey R. H., McDonald W. J. High-frequency audiometric monitoring for early detection of aminoglycoside ototoxicity. J Infect Dis. 1992 Jun;165(6):1026–1032. doi: 10.1093/infdis/165.6.1026. [DOI] [PubMed] [Google Scholar]
- Freeman C. D., Quintiliani R., Nightingale C. H. Vancomycin therapeutic drug monitoring: is it necessary? Ann Pharmacother. 1993 May;27(5):594–598. doi: 10.1177/106002809302700514. [DOI] [PubMed] [Google Scholar]
- Garrison M. W., Zaske D. E., Rotschafer J. C. Aminoglycosides: another perspective. DICP. 1990 Mar;24(3):267–272. doi: 10.1177/106002809002400312. [DOI] [PubMed] [Google Scholar]
- Gibson J., Johnson L., Snowdon L., Joshua D., Young G., MacLeod C., Sader C., Iland H., Vincent P., Kronenberg H. Single daily ceftriaxone and tobramycin in the empirical management of febrile neutropenic patients: a randomised trial. Int J Hematol. 1993 Aug;58(1-2):63–72. [PubMed] [Google Scholar]
- Gilbert D. N. Once-daily aminoglycoside therapy. Antimicrob Agents Chemother. 1991 Mar;35(3):399–405. doi: 10.1128/aac.35.3.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Govan J. R., Nelson J. W. Microbiology of lung infection in cystic fibrosis. Br Med Bull. 1992 Oct;48(4):912–930. doi: 10.1093/oxfordjournals.bmb.a072585. [DOI] [PubMed] [Google Scholar]
- Halmagyi G. M., Fattore C. M., Curthoys I. S., Wade S. Gentamicin vestibulotoxicity. Otolaryngol Head Neck Surg. 1994 Nov;111(5):571–574. doi: 10.1177/019459989411100506. [DOI] [PubMed] [Google Scholar]
- Henley C. M., 3rd, Schacht J. Pharmacokinetics of aminoglycoside antibiotics in blood, inner-ear fluids and tissues and their relationship to ototoxicity. Audiology. 1988;27(3):137–146. doi: 10.3109/00206098809081584. [DOI] [PubMed] [Google Scholar]
- Hodson M. E., Warner J. O. Cystic fibrosis: respiratory problems and their treatment. Br Med Bull. 1992 Oct;48(4):931–948. doi: 10.1093/oxfordjournals.bmb.a072586. [DOI] [PubMed] [Google Scholar]
- Hsu M. C., Aguila H. A., Schmidt V. L., Munzenberger P. J., Kauffman R. E., Polgar G. Individualization of tobramycin dosage in patients with cystic fibrosis. Pediatr Infect Dis. 1984 Nov-Dec;3(6):526–529. doi: 10.1097/00006454-198411000-00009. [DOI] [PubMed] [Google Scholar]
- Ioannides-Demos L. L., Li S. C., Bastone E. B., Spelman D. W., Hooper R. E., Cousins V. C., McLean A. J. Absence of toxicity in patients with malignant otitis externa following long-term treatment with high dosage tobramycin. J Antimicrob Chemother. 1994 Aug;34(2):267–274. doi: 10.1093/jac/34.2.267. [DOI] [PubMed] [Google Scholar]
- Kapusnik J. E., Hackbarth C. J., Chambers H. F., Carpenter T., Sande M. A. Single, large, daily dosing versus intermittent dosing of tobramycin for treating experimental pseudomonas pneumonia. J Infect Dis. 1988 Jul;158(1):7–12. doi: 10.1093/infdis/158.1.7. [DOI] [PubMed] [Google Scholar]
- Kelly H. B., Menendez R., Fan L., Murphy S. Pharmacokinetics of tobramycin in cystic fibrosis. J Pediatr. 1982 Feb;100(2):318–321. doi: 10.1016/s0022-3476(82)80664-1. [DOI] [PubMed] [Google Scholar]
- Li S. C., Bowes G., Ioannides-Demos L. L., Spicer W. J., Hooper R. E., Spelman D. W., Tong N., McLean A. J. Dosage adjustment and clinical outcomes of long-term use of high-dose tobramycin in adult cystic fibrosis patients. J Antimicrob Chemother. 1991 Oct;28(4):561–568. doi: 10.1093/jac/28.4.561. [DOI] [PubMed] [Google Scholar]
- Li S. C., Ioannides-Demos L. L., Spicer W. J., Spelman D. W., Tong N., McLean A. J. Prospective audit of an aminoglycoside consultative service in a general hospital. Med J Aust. 1992 Sep 7;157(5):308–311. [PubMed] [Google Scholar]
- Lindsay C. A., Bosso J. A. Optimisation of antibiotic therapy in cystic fibrosis patients. Pharmacokinetic considerations. Clin Pharmacokinet. 1993 Jun;24(6):496–506. doi: 10.2165/00003088-199324060-00005. [DOI] [PubMed] [Google Scholar]
- McCormack J. P., Jewesson P. J. A critical reevaluation of the "therapeutic range" of aminoglycosides. Clin Infect Dis. 1992 Jan;14(1):320–339. doi: 10.1093/clinids/14.1.320. [DOI] [PubMed] [Google Scholar]
- Parker S. E., Davey P. G. Once-daily aminoglycoside administration in gram-negative sepsis. Economic and practical aspects. Pharmacoeconomics. 1995 May;7(5):393–402. doi: 10.2165/00019053-199507050-00004. [DOI] [PubMed] [Google Scholar]
- Pedersen S. S., Jensen T., Osterhammel D., Osterhammel P. Cumulative and acute toxicity of repeated high-dose tobramycin treatment in cystic fibrosis. Antimicrob Agents Chemother. 1987 Apr;31(4):594–599. doi: 10.1128/aac.31.4.594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pleasants R. A., Williams D. M., Waltner W. E., Knowles M. R. Influence of infusion method on serum tobramycin concentrations in adults with cystic fibrosis. Clin Pharm. 1990 Jul;9(7):541–545. [PubMed] [Google Scholar]
- Powell S. H., Thompson W. L., Luthe M. A., Stern R. C., Grossniklaus D. A., Bloxham D. D., Groden D. L., Jacobs M. R., DiScenna A. O., Cash H. A. Once-daily vs. continuous aminoglycoside dosing: efficacy and toxicity in animal and clinical studies of gentamicin, netilmicin, and tobramycin. J Infect Dis. 1983 May;147(5):918–932. doi: 10.1093/infdis/147.5.918. [DOI] [PubMed] [Google Scholar]
- Prandota J. Clinical pharmacology of antibiotics and other drugs in cystic fibrosis. Drugs. 1988 May;35(5):542–578. doi: 10.2165/00003495-198835050-00004. [DOI] [PubMed] [Google Scholar]
- Prins J. M., Büller H. R., Kuijper E. J., Tange R. A., Speelman P. Once versus thrice daily gentamicin in patients with serious infections. Lancet. 1993 Feb 6;341(8841):335–339. doi: 10.1016/0140-6736(93)90137-6. [DOI] [PubMed] [Google Scholar]
- Ramsey B. W., Dorkin H. L., Eisenberg J. D., Gibson R. L., Harwood I. R., Kravitz R. M., Schidlow D. V., Wilmott R. W., Astley S. J., McBurnie M. A. Efficacy of aerosolized tobramycin in patients with cystic fibrosis. N Engl J Med. 1993 Jun 17;328(24):1740–1746. doi: 10.1056/NEJM199306173282403. [DOI] [PubMed] [Google Scholar]
- Rybak M. J., Boike S. C., Levine D. P., Erickson S. R. Clinical use and toxicity of high-dose tobramycin in patients with pseudomonal endocarditis. J Antimicrob Chemother. 1986 Jan;17(1):115–120. doi: 10.1093/jac/17.1.115. [DOI] [PubMed] [Google Scholar]
- Sawyers C. L., Moore R. D., Lerner S. A., Smith C. R. A model for predicting nephrotoxicity in patients treated with aminoglycosides. J Infect Dis. 1986 Jun;153(6):1062–1068. doi: 10.1093/infdis/153.6.1062. [DOI] [PubMed] [Google Scholar]
- Smith C. R., Lipsky J. J., Laskin O. L., Hellmann D. B., Mellits E. D., Longstreth J., Lietman P. S. Double-blind comparison of the nephrotoxicity and auditory toxicity of gentamicin and tobramycin. N Engl J Med. 1980 May 15;302(20):1106–1109. doi: 10.1056/NEJM198005153022002. [DOI] [PubMed] [Google Scholar]
- Sturm A. W. Netilmicin in the treatment of gram-negative bacteremia: single daily versus multiple daily dosage. J Infect Dis. 1989 May;159(5):931–937. doi: 10.1093/infdis/159.5.931. [DOI] [PubMed] [Google Scholar]
- Touw D. J., Vinks A. A., Heijerman H. G., Bakker W. Validation of tobramycin monitoring in adolescent and adult patients with cystic fibrosis. Ther Drug Monit. 1993 Feb;15(1):52–59. doi: 10.1097/00007691-199302000-00010. [DOI] [PubMed] [Google Scholar]
- Tran Ba Huy P., Bernard P., Schacht J. Kinetics of gentamicin uptake and release in the rat. Comparison of inner ear tissues and fluids with other organs. J Clin Invest. 1986 May;77(5):1492–1500. doi: 10.1172/JCI112463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran Ba Huy P., Deffrennes D. Aminoglycoside binding sites in the inner ears of guinea pigs. Antimicrob Agents Chemother. 1988 Apr;32(4):467–472. doi: 10.1128/aac.32.4.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tulkens P. M. Pharmacokinetic and toxicological evaluation of a once-daily regimen versus conventional schedules of netilmicin and amikacin. J Antimicrob Chemother. 1991 May;27 (Suppl 100):49–61. doi: 10.1093/jac/27.suppl_c.49. [DOI] [PubMed] [Google Scholar]
- Verpooten G. A., Giuliano R. A., Verbist L., Eestermans G., De Broe M. E. Once-daily dosing decreases renal accumulation of gentamicin and netilmicin. Clin Pharmacol Ther. 1989 Jan;45(1):22–27. doi: 10.1038/clpt.1989.4. [DOI] [PubMed] [Google Scholar]
- ter Braak E. W., de Vries P. J., Bouter K. P., van der Vegt S. G., Dorrestein G. C., Nortier J. W., van Dijk A., Verkooyen R. P., Verbrugh H. A. Once-daily dosing regimen for aminoglycoside plus beta-lactam combination therapy of serious bacterial infections: comparative trial with netilmicin plus ceftriaxone. Am J Med. 1990 Jul;89(1):58–66. doi: 10.1016/0002-9343(90)90099-y. [DOI] [PubMed] [Google Scholar]