

Abstract
Cochlear Implantation (CI) is a well-accepted treatment for severe-to-profound sensorineural hearing loss, refractory to conventional hearing amplification. Pre-operative Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) play pivotal roles in patient selection to rule out findings that preclude surgery or identify conditions that may impact the surgical procedure. A prospective study was carried out in a tertiary care center over three years, from January 2020 to January 2023. One hundred and ninety (380 ears) patients’ High-Resolution Computed Tomography (HRCT) studies of the temporal bone and MRI scans of the auditory pathways were analyzed. A reporting format was followed which was devised by a team of senior implant surgeons and senior neuro-radiologists. Our study aims to provide a comprehensive radiologic protocol for CI candidacy including normative data for the essential morphometrics in the Indian setting.
Keywords: Cochlear implant, Radiologic protocol, Morphometrics
Introduction
Cochlear implantation (CI) is a well-accepted treatment for severe-to-profound sensorineural hearing loss patients who are refractory to conventional hearing amplification [1, 2]. Pre-operative CT and MRI play a pivotal role in patient selection to rule out findings that preclude surgery or identify conditions that may impact the surgical procedure [3]. With the advent of HRCTand CBCT (Cone Beam Computed Tomography) systems and currently, with excellent multiplanar reconstructions, it is possible to localize anatomical structures in great detail. High-end CBCT systems allow images with a resolution of 75–85 μm. Structures such as crura and the footplate of the stapes, chorda tympani, Jacobson’s nerve, tympanic nerve branches, etc., can now be reliably visualized [4]. The radiologist and surgeon must be familiar with these imaging findings [5]. Temporal bone has a complex anatomy and comprises numerous vital structures in a small area. Also, each cochlea itself is unique and can have various anatomical variations. Knowledge of such variations beforehand can prepare the surgeons for the difficulties ahead during surgery. Patients who have specific anatomical variations/associated abnormalities are likely to have more difficult surgeries with increased intraoperative times as compared to patients with normal anatomy [6]. This study was conducted to obtain a comprehensive morphometric analysis of temporal bone radiology for cochlear implant candidacy in an Indian setting.
Methods
A prospective study was carried out in a tertiary care center over three years, from January 2020 to January 2023. One hundred and ninety (190) patients were radiologically investigated for cochlear implant candidacy in this period. A total of 380 ears were included in the study. HRCTof the temporal bone (160 slices) and 3 Tesla MRI of the auditory pathways were performed and analysed by two senior neuro-radiologists and a team of cochlear implant surgeons. In three years, 11 patients (n = 11) with cochleovestibular anomalies and/or cochlear nerve hypoplasia were identified and excluded from the study (not in the 190 cohort). A reporting format was followed which was devised by a team of senior implant surgeons and senior neuro-radiologists (Table 1). Data management and analyses were carried out using the Statistical Package for Social Sciences (SPSS) software version 20.
Table 1.
Radiological reporting fomat
| Region | Right | Left |
|---|---|---|
| Infratentorial region | ||
| Cerebellar hemisphere | ||
| Fourth ventricle | ||
| Brain stem | ||
| External auditory canal | ||
| Mastoid air cells | ||
| Tegmen plates | ||
| Sigmoid plates | ||
| Sinodural angle | ||
| Mastoid emissary vein | ||
| Middle ear | ||
| Ossicular chain | ||
| Facial recess & sinus tympani | ||
| Oval window & round window | ||
| Fallopian canal | ||
| Jugular bulb | ||
| Carotid canal | ||
| Vestibules | ||
| Semicircular canals | ||
| Vestibular aqueduct | ||
| Cochlear aqueduct | ||
| Turns of cochlea | ||
| Cochlear size | ||
| Modiolus | ||
| Interscalar partition | ||
| Cochlear aperture | ||
| Lines along posterior wall of external auditory canal and sigmoid sinus anterior wall (Axial cut) | ||
| Lines along posterior wall of external auditory canal and long axis of basal turn | ||
| Relative position of the basal turn of cochlea to the malleoincudal joint in axial plane | ||
| Lines along the anterior margin of the IAC’s (rotated cochlea) | ||
| Alpha angle | ||
| Beta angle | ||
| Internal auditory canal (IAC) | ||
| Lamina cribosa | ||
| Interscalar septum | ||
| Cerebellopontine angle cisterns | ||
| 7th & 8th nerve complexes | ||
| Superior & inferior vestibular nerve | ||
| Cochlear nerve | ||
| Cochlear aperture (mm) | ||
| Cochlear height (mm) | ||
| Cochlear base width (mm) | ||
| Hardy’s A | ||
| Cochlear duct length (mm) | ||
| IAC diameter (mm) | ||
| Basal turn diameter (mm) | ||
| Middle turn diameter (mm) | ||
| Apical turn diameter (mm) | ||
| Calibre of the cochlear nerve (diameter at the Fundus)(mm) | ||
| Calibre of the facial nerve (diameter at the Fundus)(mm) | ||
| Distance from vertical facial to annulus (mm) | ||
| Distance from mastoid cortex to vertical facial (cm) | ||
| Supratentorial region | ||
| Basal cisterns | ||
| Third & lateral ventricle | ||
| Cortical sulci & sylvian fissure | ||
| Focal mass lesion | ||
| Midline shift | ||
| Evidence of intracerebral/subdural bleed/infarct | ||
| Brain parenchyma shows normal gray/white matter differentiation | ||
| Sella, pituitary, and parasellar regions | ||
| Basal ganglia and thalami | ||
| Myelination |
Radiological protocol: Axial, coronal, and sagittal oblique DRIVE sequences. Axial T2 Wt sequence through the brain. 3D reconstruction through the cochlea and semicircular canals. 1 mm axial and coronal reconstructions through petrous temporal bones
3D Multiplanar reconstruction (3D MPR) of the HRCT temporal bone and High-resolution heavily T2-weighted MRI (3D) Driven Equilibrium (DRIVE) of the Internal Auditory Canal (IAC) of the subjects were used. The sequence of reporting was as follows:
First, the right temporal region is focused and the coronal projection is aligned along the basal turn of the right cochlea on the axial and sagittal images bringing the entire cochlea into focus on the oblique coronal plane (Fig. 1).
In the above oblique coronal image, the distance measured from the midpoint of the round window through the centre of the cochlea to the other end gives the Cochlear Base Width (CBW and Hardy’s A) (Fig. 2).
Cochlear Duct Length (CDL) is calculated by Jolly’s Formula given as , where A (Hardy’s A) is the cochlear base width obtained in the previous step.
Cochlear height is measured in the oblique sagittal image as the distance from the apical turn to the cochlear aperture (at the midpoint of the basal turn) (Fig. 3).
Diameters (width) of basal, middle, and apical turns of the cochlea are taken separately from the inner-to-inner margin in the above oblique coronal image (Fig. 4).
On the axial images at the level of the round window niche, the distance of the vertical facial nerve from the posterior annulus of the tympanic membrane is obtained. At the same level, in the coronal projection, the distance of the facial nerve from the mastoid cortex is measured (Fig. 5a, b).
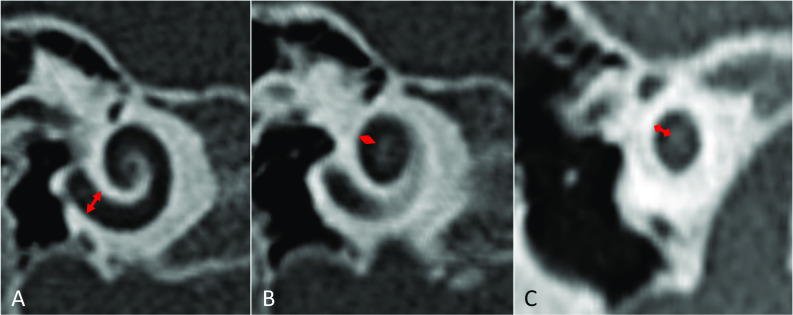
In the axial projection, cochlear aperture width is measured and recorded (Fig. 6).
The coronal projection is aligned in line with the Internal Auditory Canal (IAC), and the diameter of the IAC is taken closer to the fundus (Fig. 7).
The ear ossicles are focused and inspected to look for any morphological abnormalities. The facial canal is traced throughout to look for any dehiscence. Jugular bulb, semicircular canals, vestibular aqueduct, and cochlear aqueduct are also visualized for anomalies.
Facial nerve and cochlear nerve calibres are measured in the oblique para-sagittal view of the 3D DRIVE of the IAC at the level of the fundus of the IAC (Fig. 8).
The cochlear rotation is assessed on the axial images at the level of the round window niche using alpha and beta angles. The alpha angle is an angle between the cochlear basal turn plane at the level of the round window niche i.e. the line along the basal turn of the cochlea and head midsagittal plane (Fig. 9).
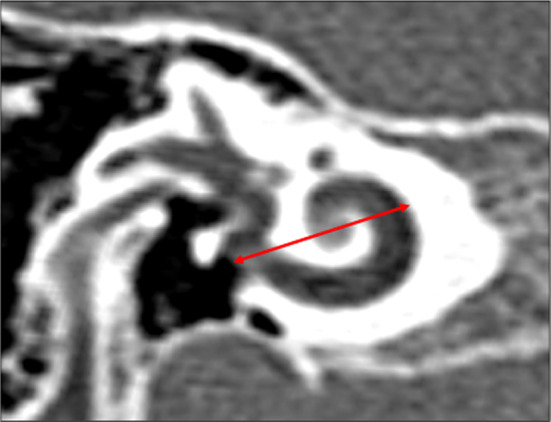
The beta angle is the angle between the cochlear basal turn plane and a line drawn along the proposed intra-operative axis of surgery, through the mastoid, facial recess and round window, running as near as possible to the posterior wall of the external auditory canal (Fig. 10).
On axial HRCT images of the temporal bone at the level of the round window niche the round window orientation is determined based on the orientation of the axes of the basal turn of the cochlea and posterior wall of the external auditory canal. The parallel orientation of these axes are associated with easier round window accessibility and intersecting axes of these structures are usually associated with difficult access (Fig. 11).
On axial HRCT images of the temporal bone types of the sigmoid sinus (lateralization of the sigmoid sinus) are determined based on the extension of the sigmoid plate beyond the axis of the posterior SCC, the tympanic segment of the facial nerve and the malleal-incudal axis type 1: located medial to the long axis of the posterior SCC; type 2: located between the long axis of the posterior SCC and the tympanic segment of the facial nerve; type 3: located between the long axis of the tympanic segment of the facial nerve and the malleal-incudal axis and type 4: located beyond the malleal-incudal axis (Fig. 12).
Steps 1 to 14 are repeated on the left side.
The entire CT and MR images including brain parenchyma for any other lesions/abnormalities are carefully examined.
Fig. 1.

A Axial section of the temporal bone. B Sagittal section of the temporal bone. The coronal projection (Pink line in A and B) is aligned along the basal turn of right cochlea on the axial A and sagittal B images bringing the entire cochlea into focus on oblique coronal plane C. Pink line – Coronal projection; Blue line – Sagittal projection; Yellow line: Axial Projection
Fig. 2.
Cochlear Base Width. In the coronal image of cochlea the distance from the midpoint of round window through the center of the cochlea to the other end gives the Cochlear Base Width
Fig. 3.

Cochlear height is measured in the oblique sagittal image as distance from the apical turn to the cochlear aperture (at the midpoint of basal turn)
Fig. 4.
Width of basal, middle and apical turns of cochlea are taken separately from inner-to-inner margin in the oblique coronal projection
Fig. 5.

a On the axial images at the level of round window niche the distance of mastoid segment of the facial nerve from the posterior annulus of tympanic membrane is obtained. b The coronal image is aligned based on the axial images at the level of the round window niche A. On the coronal projection the distance of facial nerve from the mastoid cortex is measured B. Pink line – Coronal projection; Blue line – Sagittal projection
Fig. 6.

In axial projection, cochlear aperture width is measured
Fig. 7.
The coronal projection is aligned in line with the internal auditory canal and the diameter of internal auditory canal is taken closer to the fundus
Fig. 8.

The oblique sagittal C image showing the contents of the IAC obtained by aligning the sagittal plane on the axial image A and axial plane on the coronal image B. Pink line – Coronal projection; Blue line – Sagittal projection; Yellow line: Axial Projection
Fig. 9.

The angle between cochlear basal turn plane (blue line) and head midsagittal plane (red arrow)
Fig. 10.

The angle between cochlear basal turn plane (blue line) and a line drawn along the proposed intra-operative axis of surgery, through the mastoid, facial recess and round window, running as near as possible to the posterior wall of the external auditory canal. (Yellow arrow)
Fig. 11.

Round window orientation. On axial HRCT images of the temporal bone at the level of the round window niche the orientation of the axes of the basal turn of the cochlea (dashed red line) and posterior wall of the external auditory canal (dashed yellow line) is determined. Parallel orientation of these axes are associated with easier round window accessibility and intersecting axes of these structures are usually associated with difficult access
Fig. 12.

Lateralization of the sigmoid sinus. On axial HRCT images of the temporal bone types of sigmoid sinus is determined based on the extension of the sigmoid plate beyond the axis of the posterior SCC (red line), the tympanic segment of the facial nerve (yellow line) and the malleal-incudal axis (blue line). Type 1: located medial to the long axis of the posterior SCC; type 2: located between the long axis of the posterior SCC and the tympanic segment of the facial nerve; type 3: located between the long axis of the tympanic segment of the facial nerve and the malleal-incudal axis and type 4: located beyond the malleal-incudal axis
Results
One hundred and ninety patients (380 ears) underwent HRCT of the temporal bones and MRI of the cochlea and auditory pathways. All were in the pediatric age group between 1.2 years and 12 years (Mean 3.8 years) with 112 males and 78 females. The results of both sides were combined, and data was interpreted.
Hardy’s A was calculated; the mean was 7.95 mm with a range of 6.4 mm to 8.7 mm.
Incorporating Hardy’s A, Cochlear Duct Length (CDL) was calculated using the Jolly formula. Mean CDL was 30.37 mm with a range of 23.92 mm to 33.49 mm.
Mean Cochlear Aperture (Bony Cochlear Nerve Canal, BCNC or Cochlear Fossette) was 1.79 mm, ranging from 1.5 mm to 2 mm.
Each Cochlear turn was measured individually. The mean Apical turn diameter was 1.09 mm with a range of 0.9 mm to 1 mm.
The mean Middle turn diameter was 1.51 mm with a range of 1.21 mm to 1.73 mm.
The mean Basal turn diameter was 1.91 mm with a range of 1.4 mm to 2.2 mm.
The mean Cochlear Base Width (CBW) was 7.95 mm with a range of 6.4 mm to 8.7 mm (same as Hardy’s A measurement).
The mean diameter of the Internal auditory canal (IAC) measured was 5.06 mm, values ranged from 2.96 mm to 7.08 mm.
The mean diameter (caliber) of the cochlear nerve (at the fundus or lateral end of the IAC) measured in MRI was 0.97 mm, and values ranged from 0.8 mm to 1.2 mm.
The mean diameter (caliber) of the facial nerve (at the fundus or lateral end of the IAC) measured in MRI was 0.64 mm, values ranged from 0.5 mm to 0.8 mm.
The mean distance from the vertical segment of the facial nerve to the annulus was measured (maximum; at the superior base of the Facial Recess triangle) and was 3.07 mm, with values ranging from 2.8 mm to 3.3 mm.
The mean distance from the vertical segment of the facial nerve to the mastoid cortex was measured and was 1.17 cm, values ranged from 1 cm to 1.3 cm.
All the key values, i.e., morphometrics, obtained are summarised in Table 2.
Table 2.
Morphometrics data
| Parameter | Mean | Standard deviation | Range |
|---|---|---|---|
| Hardy’s A | 7.95 mm | 0.44 | 2.3 |
| Cochlear duct length | 30.37 mm | 1.86 | 9.56 |
| Cochlear aperture | 1.79 mm | 0.125 | 0.5 |
| Apical turn diameter | 1.09 mm | 0.09 | 0.7 |
| Middle turn diameter | 1.51 mm | 0.13 | 0.52 |
| Basal turn diameter | 1.91 mm | 0.13 | 0.8 |
| Cochlear base width | 7.95 mm | 0.44 | 2.3 |
| Internal auditory canal (IAC) diameter | 5.06 mm | 1.17 | 4.12 |
| Cochlear nerve calibre (at Fundus) | 0.97 mm | 0.13 | 0.4 |
| Facial nerve calibre (at Fundus) | 0.64 mm | 0.074 | 0.3 |
| Distance from vertical facial to Annulus (maximum) | 3.07 mm | 0.12 | 0.49 |
| Distance from mastoid cortex to vertical facial | 1.17 cm | 0.06 | 0.29 |
| Alpha angle | 58.7 degree | 4.3 | 17.7 |
| Beta angle | 17.3 degree | 2.1 | 9.3 |
Discussion
For the decision of candidacy for cochlear implantation, imaging evaluation plays a vital role. Imaging evaluation of the ear and temporal bone is primarily done by CT and MRI. Surgeons need to be aware of the anomalies and pathologies that may represent a potential surgical hazard or that may require modification of the surgical approach. Numerous vital structures are present in close proximity and morphometric knowledge of the anatomy beforehand can smoothen the overall surgical process, help in choosing the right electrode for the patient, and thus give the best surgical outcome.
Cochlear Duct Length (CDL): Cochlear duct length (CDL) is defined as the length of the scala media as measured from the middle of the round window to the helicotrema. To calculate CDL 4.16A-2.7, the formula (popularly known as Jolly formula) given by Alexiades et al. was used [5], the value of A is defined as the linear measurement from the round window to the farthest point on the opposite wall of the cochlea on a reformatted CT scan slice [5]. In this study, the mean Hardy’s A was 7.95 mm with a range of 6.4 mm–8.7 mm.
A study published by Grover et al. had a mean cochlear duct length of 29.8 mm with a range from 28 to 34.3 mm [7]. In our study, Mean CDL was 30.37 with a range from 23.92 to 33.49 mm. Cochlear duct length holds significance in choosing the right length of the electrode. In temporal bone studies, deep electrode insertions beyond 360° significantly increased the risk of cochlear trauma [8–12]. Shallower insertions may, however, result in poorer implant hearing performance [13, 14].
Cochlear Aperture (CA): The cochlear aperture (CA) is the bony opening at the base of the modiolus that transmits blood vessels and nerve fibres from the spiral ganglion to the cochlear nerve. This is also known as the Bony Cochlear Nerve Canal (BCNC) or the Cochlear Fosette. Hypoplasia of the cochlear aperture is defined by a width less than 1.4 mm and aplasia is characterized by the replacement of the cochlear aperture with bone [15]. The cochlear aperture was measured in its mid-portion at a mid-modiolar level. In the current study mean CA was 1.79 ranging from 1.5 to 2 mm, which is slightly less than the 1.91 mm found by Sachiko et al. [16]. The detection of IAC stenosis alone may be insufficient to indicate a Cochlear nerve deficiency: therefore, the measurement of CA is also required to predict cochlear nerve status [17].
Cochlear Diameters (Apical, Middle, and Basal turn): The development of the cochlea is complete by the middle of gestation and reaches adult size; no further change in size and shape takes place after birth [18, 19]. There is great variability in the size of different turns of the cochlea in human beings. Apical, middle, and basal turns diameter in this study were 1.09 mm,1.51 mm, and 1.91 mm respectively which were similar to results obtained by Kumar et al. [20]; apical turn diameter—1.13 mm, middle turn diameter—1.38 mm, basal turn diameter was 1.81 mm. This metric is of importance when choosing longer electrodes that need to get beyond one and a half turns of the cochlea.
Cochlear Base Width (CBW): To come up with atraumatic cochlear implant (CI) electrodes and atraumatic insertions, knowledge of the variability of human anatomy is required. Cochlear base measurements can be used to determine the required lengths for both lateral and midscalar locations of the implant [21]. The mean cochlear base width in this study was 7.95 mm ranging from 6.4 mm to 8.7 mm. Results are slightly more than those obtained by Zahara et al. where the mean base width was 6.53 and values ranged from 5.73 to 7.5 mm [22].
Internal Auditory Canal (IAC): The IAC is a narrow canal that extends for roughly 1 cm within the petrous part of the temporal bone. Several published reports indicate variations in the anteroposterior (AP) diameter and length of the canal. In order to avoid damage to the labyrinth, a preview of the measurements of the IAC is important for interpreting radiographs [23]. The canal is considered stenotic if its diameter is smaller than 2 mm. The normal diameter varies from 4 to 8 mm [24, 25]. The mean diameter of the IAC measured in our study was 5.06 mm, and values ranging from 2.96 mm to 7.08 mm; results are comparable to those by Erkoc et al. in which the mean IAC diameter was 5.93 mm [26].
Cochlear Nerve (CN) and Facial Nerve (FN) Calibre: The cochlear nerve size is associated with the population of spiral ganglion cells. Therefore, determining the caliber of the nerve may be helpful in predicting the outcome of CI [27]. CN is larger in diameter than FN and Superior and Inferior vestibular nerves. CN hypoplasia is when the diameter is less than 0.8 mm. The mean CN and FN diameters were 0.97 mm and 0.64 mm respectively in our study.
Distance from Vertical Facial Canal to Annulus: The facial nerve follows a complex course in the temporal bone. Complications usually arise when there is a limited understanding of its anatomy. The tympanic annulus is a consistent bony landmark that can be easily identified preoperatively on a CT scan. The widest distance from the posterior edge of the annulus to the vertical segment of FN was calculated which roughly corresponds to the maximum base width of the facial recess triangle (bounded by Incus buttress/bridge and vertical Fallopian canal and chorda tympani). In our study the mean distance from the vertical segment of the facial nerve to the annulus was measured and was 3.07 mm, values ranged from 2.8 mm to 3.3 mm. Results are comparable to those by Adad et al. where the mean distance was 3.8 mm [28].
Distance from Mastoid Cortex to Vertical Facial Canal: In a study by Jatale et al. the distance of the second genu from the outer cortex varied from 1.78 cm to 2.36 cm with a mean of 1.96 cm [29], which is slightly more than what we observed in our study where the mean distance from a vertical segment of the facial nerve to the mastoid cortex was measured and was 1.17 cm, values ranged from 1 cm to 1.3 cm. This perhaps was because we had a number of children under 2 years of age in our study cohort.
Alpha(α) and Beta(β) Angle: In our study mean α angle was 58.7 degrees with a range from 48 to 65.7 degrees which is very similar to the results obtained by Lloyd et al. [30] where the mean basal turn angle was 54.6 degrees with a range, of 46.8–63.8 degrees and the standard deviation of 3.5. Calculation of cochlear orientation and its angle with the surgical axis α and β angle can aid surgical planning and cochleostomy site decisions [30]. In patients whom an α angle of less than 50 degrees and β angle of more than 20 degrees, surgeons can face difficulty in electrode insertion. The mean β angle in this study was 17.3 with a range from 13 to 22.3 degrees. The β angle indicates the extent of angulation between the surgical axis and the axis of the basal turn of the cochlea [31].
Conclusion
One of the most essential components in the decision-making for cochlear implant candidacy is radiology. A standardized protocol including morphometric analysis of important radiological parameters is desirable. Our study thus provides a comprehensive radiologic protocol for CI candidacy including normative data for the essential morphometrics in the Indian setting.
Funding
The authors did not receive support from any organization for the submitted work.
Conflict of interest
The authors report no conflict of interest.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Joshi VM, Navlekar SK, Kishore GR, Reddy KJ, Kumar EC. CT and MR imaging of the inner ear and brain in children with congenital sensorineural hearing loss. Radiographics. 2012;32:683–698. doi: 10.1148/rg.323115073. [DOI] [PubMed] [Google Scholar]
- 2.Witte RJ, Lane JI, Driscoll CL, Lundy LB, Bernstein MA, Kotsenas AL, et al. Pediatric and adult cochlear implantation. Radiographics. 2003;23:1185–1200. doi: 10.1148/rg.235025046. [DOI] [PubMed] [Google Scholar]
- 3.Widmann G, Dejaco D, Luger A, et al. Pre- and post-operative imaging of cochlear implants: a pictorial review. Insights Imaging. 2020;11:93. doi: 10.1186/s13244-020-00902-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Casselman JW, Veillon F. Temporal bone and auditory pathways. In: Hodler J, von Schulthess GK, Zollikofer CL, editors. Diseases of the brain, head & neck, Spine 2012–2015. Milano: Springer; 2012. [Google Scholar]
- 5.Alexiades G, Dhanasingh A, Jolly C. Method to estimate the complete and two-turn cochlear duct length. Otol Neurotol. 2014;36:904–907. doi: 10.1097/MAO.0000000000000620. [DOI] [PubMed] [Google Scholar]
- 6.Vaid S, Vaid N, Manikoth M, Zope A. Role of HRCT and MRI of the temporal bone in predicting and grading the degree of difficulty of cochlear implant surgery. Indian J Otolaryngol Head Neck Surg. 2015;67(02):150–158. doi: 10.1007/s12070-015-0858-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grover M, Sharma S, Singh SN, Kataria T, Lakhawat RS, Sharma MP. Measuring cochlear Duct length in an Asian population: worth giving a thought! Eur Arch Otorhinolaryngol. 2018;275(3):725–728. doi: 10.1007/s00405-018-4868-9. [DOI] [PubMed] [Google Scholar]
- 8.Gstoettner W, Franz P, Hamzavi J, et al. Intracochlear position of cochlear implant electrodes. Acta Otolaryngol. 1999;119:229–233. doi: 10.1080/00016489950181729. [DOI] [PubMed] [Google Scholar]
- 9.Gstoettner W, Plenk HJ, Franz P, et al. Cochlear implant deep electrode insertion: extent of insertional trauma. Acta Otolaryngol. 1997;117(2):274–277. doi: 10.3109/00016489709117786. [DOI] [PubMed] [Google Scholar]
- 10.Kennedy DW. Multichannel intracochlear electrodes: mechanism of insertion trauma. Laryngoscope. 1987;97:42–49. doi: 10.1288/00005537-198701000-00011. [DOI] [PubMed] [Google Scholar]
- 11.Welling DB, Hinojosa R, Gantz BJ, et al. Insertional trauma of multichannel cochlear implants. Laryngoscope. 1993;103:995–1001. doi: 10.1288/00005537-199309000-00010. [DOI] [PubMed] [Google Scholar]
- 12.Hochmair I, Arnold W, Nopp P, et al. Deep electrode insertion in cochlear implants: apical morphology, electrodes and speech perception results. Acta Otolaryngol. 2003;123:612–617. [PubMed] [Google Scholar]
- 13.Friesen LM, Shannon RV, Slattery WH. Effects of electrode location on speech recognition with the nucleus-22 cochlear implant. J Am Acad Audiol. 2000;11:418–428. doi: 10.1055/s-0042-1748129. [DOI] [PubMed] [Google Scholar]
- 14.Karaca CT, Toros SZ, Noseri HK. Analysis of anatomic variations in temporal bone by radiology. Int Adv Otol. 2012;8:239–243. [Google Scholar]
- 15.Sennaroglu L, Bajin MD. Classification and current management of inner ear malformations. Balkan Med J. 2017;34:397–411. doi: 10.4274/balkanmedj.2017.0367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Komatsubara S, Haruta A, Nagano Y, Kodama T. Evaluation of cochlear nerve imaging in severe congenital sensorineural hearing loss. ORL J Otorhinolaryngol Relat Spec. 2007;69:198–202. doi: 10.1159/000099231. [DOI] [PubMed] [Google Scholar]
- 17.Tahir E, Bajin MD, Atay G, Mocan BÖ, Sennaroğlu L. Bony cochlear nerve canal and internal auditory canal measures predict cochlear nerve status. J Laryngol Otol. 2017;131:676–683. doi: 10.1017/S0022215117001141. [DOI] [PubMed] [Google Scholar]
- 18.Jackler RK, Luxford WM, House WF. Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope. 1987;97:2–14. doi: 10.1002/lary.5540971301. [DOI] [PubMed] [Google Scholar]
- 19.Pappas DG, Simpson LC, McKenzie RA, et al. High-resolution computed tomography: determination of the cause of pediatric sensorineural hearing loss. Laryngoscope. 1990;100:564–569. doi: 10.1288/00005537-199006000-00002. [DOI] [PubMed] [Google Scholar]
- 20.Kumar JU, Kavitha Y. Application of curved MPR algorithm to high resolution 3 dimensional T2 weighted CISS images for virtual uncoiling of membranous cochlea as an aid for cochlear morphometry. J Clin Diagn Res. 2017;11(2):12–14. doi: 10.7860/JCDR/2017/23206.9456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Avci E, Nauwelaers T, Lenarz T, Hamacher V, Kral A. Variations in microanatomy of the human cochlea. J Comp Neurol. 2014;522:3245–3261. doi: 10.1002/cne.23594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zahara D, Dewi RD, Aboet A, Putranto FM, Lubis ND, Ashar T. Variations in cochlear size of cochlear implant candidates. Int Arch Otorhinolaryngol. 2019;23(2):184–190. doi: 10.1055/s-0038-1661360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fujita S, Sando I. Postnatal development of the vestibular aqueduct in relation to the internal auditory canal. Computer-aided three-dimensional reconstruction and measurement study. Ann Otol Rhinol Laryngol. 1994;103(9):719–22. doi: 10.1177/000348949410300910. [DOI] [PubMed] [Google Scholar]
- 24.Guirado RC. Malformations du conduit auditif interne. Bordx Fr Rev Laryngol Otol Rhinol. 1992;113(5):419–421. [PubMed] [Google Scholar]
- 25.Valvassori GE, Pierce RH. The normal internal auditory canal. Am J Roentgenol Radium Ther Nucl Med. 1964;92:1232–1241. [PubMed] [Google Scholar]
- 26.Erkoç MF, Imamoglu H, Okur A, Gümüş C, Dogan M. Normative size evaluation of internal auditory canal with magnetic resonance imaging: review of 3786 patients. Folia Morphol (Warsz) 2012;71(4):217–220. [PubMed] [Google Scholar]
- 27.Nadol JB, Jr, Xu W-Z. Diameter of the cochlear nerve in deaf humans: implications for cochlear implantation. Ann Otol Rhinol Laryngol. 1992;101(12):988–993. doi: 10.1177/000348949210101205. [DOI] [PubMed] [Google Scholar]
- 28.Adad B, Rasgon BM, Ackerson L. Relationship of the facial nerve to the tympanic annulus: a direct anatomic examination. Laryngoscope. 1999;109(8):1189–1192. doi: 10.1097/00005537-199908000-00002. [DOI] [PubMed] [Google Scholar]
- 29.Jatale SP, Chintale SG, Kirdak VR, Shaikh KA. Our experience of anatomical variations of facial nerve in cadaveric temporal bone dissection. Indian J Otolaryngol Head Neck Surg. 2021;73(3):271–275. doi: 10.1007/s12070-020-01969-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lloyd SK, Kasbekar AV, Kenway B, Prevost T, Hockman M, Beale T, et al. Developmental changes in cochlear orientation–implications for cochlear implantation. Otol Neurotol. 2010;31:902–907. doi: 10.1097/MAO.0b013e3181db7146. [DOI] [PubMed] [Google Scholar]
- 31.Sharma S, Grover M, Singh SN, Kataria T, Lakhawat RS. Cochlear orientation: pre-operative evaluation and intra-operative significance. J Laryngol Otol. 2018;132:540–543. doi: 10.1017/S002221511800066X. [DOI] [PubMed] [Google Scholar]