

Abstract
Introduction
A newly developed surgical robot system, hinotori, with various unique advantages has been in clinical use in Japan; however, there have not been any studies of robot‐assisted radical nephrectomy and inferior vena cava tumor thrombectomy using hinotori.
Case presentation
We describe two male patients aged 67 and 76 years old with right renal cell carcinoma and a level II and I inferior vena cava tumor thrombus, respectively, undergoing robot‐assisted radical nephrectomy and inferior vena cava tumor thrombectomy using hinotori. Both operations were successfully completed with a purely robotic procedure without any major perioperative complications, resulting in the following findings: time using robotic system, 158 and 156 min; total operative time, 228 and 214 min; estimated blood loss, 535 and 200 mL, respectively.
Conclusion
Based on our first experience, robot‐assisted radical nephrectomy and inferior vena cava tumor thrombectomy using hinotori may be an effective treatment for renal cell carcinoma with inferior vena cava tumor thrombus ≤level II.
Keywords: hinotori, inferior vena cava tumor thrombectomy, renal cell carcinoma, robot‐assisted radical nephrectomy
Abbreviations & Acronyms
- IVC
inferior vena cava
- RARN/IVCTT
robot‐assisted radical nephrectomy and inferior vena cava tumor thrombectomy
- RCC
renal cell carcinoma
- RN
radical nephrectomy
- WHO/ISUP
World Health Organization/International Society of Urological Pathology
Keynote message.
This is the first case report presenting two patients receiving RARN/IVCTT using newly developed hinotori surgical system, and our experience suggests that purely robotic surgery using hinotori may be a useful treatment for RCC with IVC tumor thrombus ≤level II.
Introduction
Although open RN and IVCTT remain the standard approach for patients with RCC with IVC tumor thrombus, 1 recent progress in robotic technologies has led to the application of robotic surgery to these patients. 2 Since the first study in 2011, 3 promising outcomes of RARN/IVCTT have been reported in several studies at high‐volume centers. 2 , 3 , 4 , 5 , 6 , 7
The da Vinci surgical system (Intuitive Surgical Inc., Sunnyvale, CA, USA) has monopolized the surgical robot market for the past 2 decades. On the other hand, numerous alternative robotic systems are being actively developed, and some are in clinical use. 8 , 9 , 10 , 11 , 12 , 13 , 14 Among them, hinotori, launched in 2019 by the Medicaloid Corporation (Kobe, Japan), has unique advantages that are different from existing platforms. 12
To our knowledge, there have been no studies of RARN/IVCTT using hinotori. The objective of the present report was to summarize the initial experience of RARN/IVCTT using hinotori for two patients with right RCC and IVC tumor thrombus corresponding to levels I and II, based on the Mayo clinic classification. 1
Case presentation
Case 1
A 67‐year‐old male patient presented with a right renal mass and was referred to our institution. An enhanced right renal tumor with a level II IVC tumor thrombus (22 mm high from the right renal vein) without evidence of distant metastasis was observed on computed tomography (Table 1; Fig. 1). We administered 20 mg of cabozantinib daily as presurgical medication. After 4 weeks, the size of the right renal tumor decreased from 78 to 71 mm in diameter, while the height of the IVC tumor thrombus was not changed. Considering the slight reduction of the tumor and favorable condition of the patient, RARN/IVCTT using hinotori was planned.
Table 1.
Perioperative characteristics of two patients who underwent robot‐assisted RN and IVC thrombectomy using hinotori surgical robot system
| Variables | Case 1 | Case 2 |
|---|---|---|
| Age (years) | 67 | 79 |
| Sex | Male | Male |
| Body mass index (kg/m2) | 27.1 | 22.1 |
| ECOG‐PS | 0 | 0 |
| ASA score | II | I |
| History of abdominal surgery | No | No |
| Tumor side | Right | Right |
| Tumor size (mm) | 78 | 106 |
| TNM classification | cT3bN0M0 | cT3bN0M0 |
| Distance of thrombus above the renal vein (mm) | 22 | 4 |
| Level of IVC thrombus | Level II | Level I |
| Presurgical medication | Cabozantinib 20 mg x4weeks | No |
| Surgical approach | Transperitoneal | Transperitoneal |
| Operative time (min) | 228 | 214 |
| Time using robotic system (min) | 158 | 156 |
| Estimated blood loss (mL) | 535 | 200 |
| Blood translation | No | No |
| Open conversion | No | No |
| Postoperative major complication (Clavien‐Dindo ≥3) | No | No |
| Length of postoperative hospital stay (days) | 8 | 10 |
| Resected weight (g) | 595 | 635 |
| Histological subtype | Clear cell RCC | Clear cell RCC |
| pT stage | pT3b | pT3b |
| WHO/ISUP grading | Grade 3 | Grade 4 |
ASA, American Society of Anesthesiologists; ECOG‐PS, Eastern Cooperative Oncology Group Performance Status.
Fig. 1.
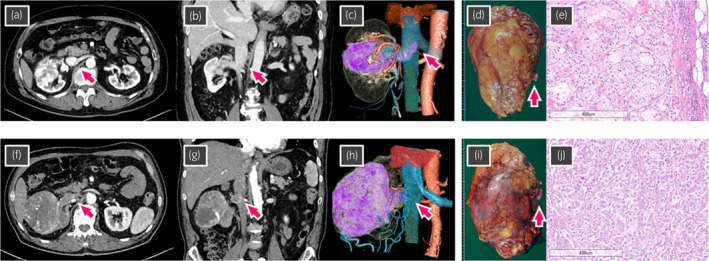
(a–e) Case 1 showing right RCC with a level II IVC tumor thrombus (arrow). (a) Axial section of computed tomography (CT). (b) Coronal section of CT. (c) Three‐dimensional reconstructed image from CT. (d), Macroscopic findings of the excised right kidney and IVC tumor thrombus (arrow). Excised weight was 595 g. (e) Microscopic findings of hematoxylin and eosin staining showing clear cell RCC, pT3b, WHO/ISUP grade 3. (f–j) Case 2 showing right RCC with level I IVC tumor thrombus (arrow). (f) Axial section of CT. (g) Coronal section of CT. (h) Three‐dimensional reconstructed image from CT. (i), Macroscopic findings of the excised right kidney and IVC tumor thrombus (arrow). Excised weight was 635 g. (j), Microscopic findings of hematoxylin and eosin staining showing clear cell RCC, pT3b, WHO/ISUP grade 4.
Surgical procedure including the operative position and trocar placement were the same as those in our previous report using da Vinci Xi. 15 , 16 Time using the robotic system, total operating time, and estimated blood loss were 158, 228 min, and 535 mL, respectively. No major complications occurred, and blood transfusion during and after RARN/IVCTT was not required. On the eighth day after surgery, the patient was discharged from the hospital. The following findings were revealed by pathological assessment: clear cell RCC, pT3b, and WHO/ISUP grade 3 (Table 1).
Case 2
A 67‐year‐old male patient with right renal tumor (106 mm in diameter) and a level I IVC tumor thrombus (4 mm high from the right renal vein) was referred to our institution. Clinical stage was diagnosed as cT3bN0M0 (Table 1, Fig. 1). RARN/IVCTT using hinotori was performed without presurgical therapy using surgical procedures similar to those in case 1 (Fig. 2).
Fig. 2.
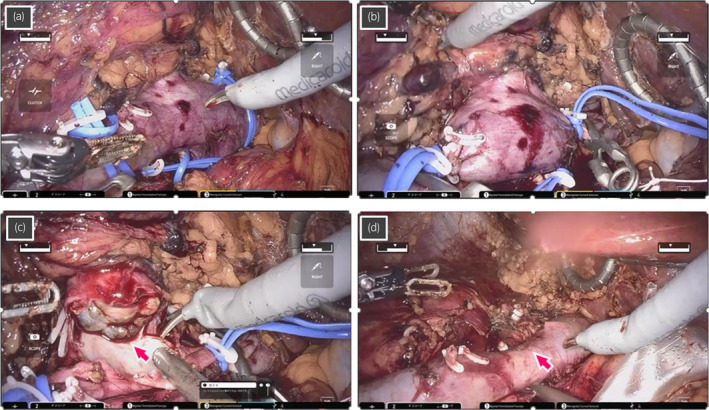
Intraoperative images during robot‐assisted RN and IVC tumor thrombectomy for case 2 who had level I IVC tumor thrombus. (a) The left renal vein, caudal IVC, and cephalic IVC are secured by twice‐wrapped vessel loops, and (b) sequentially clamped with the vessel loops by clipping in addition to the use of bulldogs. (c) Tumor thrombus (arrow) is removed from the IVC, and the wall of IVC is cut. (d) The IVC is reconstructed by continuous suture with a 4‐0 polypropylene (arrow), following removal of the tumor thrombus.
Time using the robotic system, total operating time, and estimated blood loss were 156, 214 min, and 200 mL, respectively. The surgery was conducted with a purely robotic approach without open conversion, major complications, or blood transfusion, and duration of hospital stay after surgery was 10 days. The following findings were revealed by pathological assessment: clear cell RCC, pT3b, and WHO/ISUP grade 4.
Discussion
Since the initial study, 3 robot‐assisted surgery for RCC with IVC tumor thrombus have increased as a minimally invasive procedure alternative to the conventional open approach, since the outcomes of RARN/IVCTT have been reported to be significantly less intraoperative blood loss and complications compared to open approaches. 2 , 3 , 4 , 5 , 6 , 7 Thus, the robotic surgery has been extended to RCC patients with a higher level of IVC tumor thrombus by a small number of limited institutions. 17 , 18 However, it remains unclear whether novel robotic platforms, including hinotori, can be safely used for RARN/IVCTT. To the best of our knowledge, this may be the first report of purely robotic RARN/IVCTT procedures being successfully completed using hinotori.
Hinotori has several unique features that make it different from the existing da Vinci system, such as a flexibly positionable three‐dimensional viewer in the surgeon cockpit, calibration of the position of trocars by software without docking of an arm with a port, and flexible movement of compactly designed robotic arms with 8 axes of motion. 12 In Japan, several fields of surgery, including urology, gynecology, and gastroenterology, have introduced the hinotori in daily clinical practice. In the present report, considering the promising features of its equipment and clinical performance, we performed RARN/IVCTT using hinotori for two surgeries.
The RARN/IVCTT surgeries using hinotori were completed without any major perioperative complications according to the procedures same as those in cases using da Vinci since these two surgical robot systems are characterized by the fundamentally common structural design, consisting of an operation unit, surgeon cockpit, and monitor cart. The time using the robotic system was approximately 150 min for both surgeries, which is shorter than previous studies that used da Vinci. 2 , 3 , 4 , 5 , 6 , 7 These findings are similar to the console times reported in our previous study of two cases with IVC tumor thrombus receiving RARN/IVCTT with da Vinci (167 and 233 min, respectively). 16 In addition, other perioperative outcomes with hinotori, including estimated blood loss and length of postoperative hospital stay, were comparable to those with da Vinci in our experienced cases. Collectively, these findings suggest that for cases with IVC tumor thrombus ≤infrahepatic level II, RARN/IVCTT using hinotori can achieve similar perioperative outcomes to da Vinci.
This study had several limitations. Firstly, it was required to consider whether procedures omitted in these cases, such as covering of the removed thrombus by using a specimen bag and irrigation of the caval lumen, should be performed. Secondly, length of hospital stay in Japan tends to be longer compared to Western countries regardless of surgical procedure. Thirdly, cabozantinib was used as a presurgical medication in case 1; however, since the efficacy of presurgical medication remains controversial in the field of RCC, this indication should be carefully determined. Finally, further studies are needed for the application of the hinotori for patients with an IVC tumor thrombus ≥level III or all levels of IVC tumor thrombus with left‐sided renal tumor.
In conclusion, this is the initial report presenting successful completion of RARN/IVCTT for two cases with level I and II IVC tumor thrombus using hinotori. Purely robotic surgery using hinotori may be an effective treatment for such patients.
Author contributions
Daisuke Motoyama: Data curation; formal analysis; investigation; methodology; project administration; resources; validation; visualization; writing – original draft. Yuto Matsushita: Investigation. Hiromitsu Watanabe: Investigation. Keita Tamura: Investigation. Atsushi Otsuka: Investigation. Masato Fujisawa: Supervision. Hideaki Miyake: Conceptualization; investigation; writing – review and editing.
Conflict of interest
The authors have no conflict of interest.
Approval of the research protocol by an Institutional Reviewer Board
21‐091.
Informed consent
Not applicable.
Registry and the Registration No. of the study/trial
Not applicable.
Acknowledgments
None.
References
- 1. Blute ML, Leibovich BC, Lohse CM, Cheville JC, Zincke H. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int. 2004; 94: 33–41. [DOI] [PubMed] [Google Scholar]
- 2. Murphy C, Abaza R. Complex robotic nephrectomy and inferior vena cava tumor thrombectomy: an evolving landscape. Curr. Opin. Urol. 2020; 30: 83–89. [DOI] [PubMed] [Google Scholar]
- 3. Abaza R. Initial series of robotic radical nephrectomy with vena caval tumor thrombectomy. Eur. Urol. 2011; 59: 652–656. [DOI] [PubMed] [Google Scholar]
- 4. Abaza R, Eun DD, Gallucci M et al. Robotic surgery for renal cell carcinoma with vena caval tumor thrombus. Eur. Urol. Focus 2016; 2: 601–607. [DOI] [PubMed] [Google Scholar]
- 5. Ghoreifi A, Djaladat H. Surgical tips for inferior vena cava thrombectomy. Curr. Urol. Rep. 2020; 21: 51. [DOI] [PubMed] [Google Scholar]
- 6. Rose KM, Navaratnam AK, Abdul‐Muhsin HM et al. Robot assisted surgery of the vena cava: perioperative outcomes, technique, and lessons learned at the Mayo Clinic. J. Endourol. 2019; 33: 1009–1016. [DOI] [PubMed] [Google Scholar]
- 7. Chopra S, Simone G, Metcalfe C et al. Robot‐assisted level II‐III inferior vena cava tumor thrombectomy: step‐by‐step technique and 1‐year outcomes. Eur. Urol. 2017; 72: 267–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Almujalhem A, Rha KH. Surgical robotic systems: what we have now? A urological perspective. BJUI Compass 2020; 1: 152–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Farinha R, Puliatti S, Mazzone E et al. Potential contenders for the leadership in robotic surgery. J. Endourol. 2022; 36: 317–326. [DOI] [PubMed] [Google Scholar]
- 10. Rao PP et al. Robotic surgery: new robots and finally some real competition! World J. Urol. 2018; 36: 537–541. [DOI] [PubMed] [Google Scholar]
- 11. Bravi CA, Paciotti M, Sarchi L et al. Robot‐assisted radical prostatectomy with the novel Hugo robotic system: initial experience and optimal surgical set‐up at a tertiary referral robotic center. Eur. Urol. 2022; 82: 233–237. [DOI] [PubMed] [Google Scholar]
- 12. Hinata N, Yamaguchi R, Kusuhara Y et al. Hinotori surgical robot system, a novel robot‐assisted surgical platform: preclinical and clinical evaluation. Int. J. Urol. 2022; 29: 1213–1220. [DOI] [PubMed] [Google Scholar]
- 13. Miyake H, Motoyama D, Matsushita Y et al. Initial experience of robot‐assisted partial nephrectomy using Hinotori surgical robot system: single institutional prospective assessment of perioperative outcomes in 30 cases. J. Endourol. 2023; 37: 531–534. [DOI] [PubMed] [Google Scholar]
- 14. Motoyama D, Matsushita Y, Watanabe H et al. Robot‐assisted adrenalectomy using a hinotori surgical robot system: report of first series of six cases. Asian J. Endosc. Surg. 2023; 16: 489–495. [DOI] [PubMed] [Google Scholar]
- 15. Miyake H, Motoyama D, Kawakami A et al. Initial experience of robot‐assisted radical nephrectomy in Japan: single institutional study of 12 cases. Asian J. Endosc. Surg. 2022; 15: 162–167. [DOI] [PubMed] [Google Scholar]
- 16. Motoyama D, Ito T, Sugiyama T, Otsuka A, Miyake H. Robot‐assisted radical nephrectomy and inferior vena cava tumor thrombectomy: initial experience in Japan. IJU Case Rep. 2022; 5: 145–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Gill IS, Metcalfe C, Abreu A et al. Robotic level III inferior vena cava tumor thrombectomy: initial series. J. Urol. 2015; 194: 929–938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Shen D, Du S, Huang Q et al. A modified sequential vascular control strategy in robot‐assisted level III–IV inferior vena cava thrombectomy: initial series mimicking the open ‘milking’ technique principle. BJU Int. 2020; 126: 447–456. [DOI] [PubMed] [Google Scholar]