

Summary
Food retail strategies to improve the healthiness of food and beverage options may increase purchasing of healthier options and improve diets. Consumer demand for healthier options is an important determinant of the successful implementation and maintenance of healthy food retail interventions. A systematic review of peer‐reviewed literature was undertaken to explore whether consumers are willing to pay more for healthier foods and to determine the key factors that influence willingness to pay. Fifteen studies reported the results of 26 experiments providing willingness to pay estimates for healthier food products across a range of food retail environments. Twenty three out of the 26 experiments included in this review (88.5%) found consumers would pay a 5.6% to 91.5% (mean 30.7%) price premium for healthier foods. Studies consistently found a positive willingness to pay for foods with reduced fat and wholegrains with additional fruit and vegetables, while willingness to pay for foods with reduced salt or a combination of low fat and sugar, or salt showed mixed results. Adults over 60 years, females, those living with obesity, and consumers who aim to maintain a healthy lifestyle were more likely to pay a price premium for healthier food, whereas younger consumers, consumers with healthy weight, and consumers with higher levels of education were less likely to pay higher prices. The results of this review contribute to our understanding of consumer preferences for healthier products and provide information to retailers on consumer surplus (benefits) associated with the provision of healthier food alternatives.
Keywords: dietary guidelines, healthy food retail, healthy interventions, willingness to pay
Abbreviations
- DCE
discrete choice experiment
- NCD
non‐communicable disease
- WTP
willingness to pay
1. INTRODUCTION
Non communicable diseases (NCDs) are strongly driven by the globalization of unhealthy lifestyles and poorly planned urbanization. 1 In Australia, dietary risks are among the top modifiable risks contributing to NCDs after tobacco use and harmful use of alcohol. 2 Policy interventions to improve food environments may improve diets and assist with NCD prevention and control. 3 , 4 , 5 A key factor that determines what we eat is our community food retail environment and in particular supermarket and grocery stores, which are the main source of food in both developed and developing countries. 6 , 7 Currently, food retail environments predominantly consist of food products that are energy dense and nutrient poor, relatively cheap and heavily promoted. 8
There are promising food retail interventions being implemented by governments, community organizations, and food retailers to promote the purchase and consumption of healthier foods using traditional marketing techniques such as the “4Ps” of marketing (product, promotion, placement, and price). 9 , 10 , 11 Over the last 20 years, the evidence of effectiveness of different healthy food retail strategies has become more robust. Reviews indicate that healthy food retail strategies are effective in increasing the purchasing and availability of healthy food and beverages in both small stores 12 , 13 and large supermarkets. 9 , 14 , 15 , 16 , 17 , 18 , 19 , 20 Interventions were more effective when implemented for longer durations 21 and with multiple components. 12 , 16 , 20
Food retailers are businesses, and therefore, any voluntary changes to retail environments to increase their healthiness also need to meet the business's own commercial needs. 22 In addition to health impacts on the community, business outcomes such as commercial viability, customer perspectives, and retailer perspectives may influence retailer decision‐making related to the adoption and maintenance of healthy food strategies. 23 Consumer perspectives are an important determinant of the successful implementation and maintenance of healthy food retail interventions. 10 , 21 , 23 , 24 , 25
Historically, there have been two general approaches to estimate consumer preferences and willingness to pay (WTP): stated preference and revealed preference approaches. Revealed preference methods determine the value that consumers place on goods and services by observing consumer purchasing in actual markets. On the other hand, stated preference methods such as contingent valuation, conjoint analysis, and discrete choice experiments (DCEs) use hypothetical scenarios to elicit consumer preferences.
There is a vast marketing literature on consumer WTP for various food attributes. Evidence from WTP studies plays a crucial role in pricing and product development decisions by food manufacturers and retailers. 26 WTP studies estimate the maximum price that the consumer would consider paying for a product or service with various attributes. For example, if the market price of a conventional (regular) cheddar cheese product is $10 per kg and a manufacturer would like to introduce a new product such as a reduced fat cheddar cheese into the market, then they may use a WTP study to determine the maximum price consumers are willing to pay for this type of cheese. The amount could be higher or lower than the price of the original product. In addition to pricing decisions, WTP studies may alert retailers of consumer preferences for various attributes of products and may therefore influence stocking and promotional activities. 26
The synthesis of studies investigating the WTP for various food attributes has been limited to systematic reviews that investigated consumer WTP for functional attributes, organic foods, and sustainability features of food production. Dolgopolova and Teuber 27 analyzed the current literature on consumer WTP for health benefits of food products. Their meta‐analysis focused on food with functional attributes which they defined as foods enriched with additional nutritional substances that go beyond basic nutrition, such as resveratrol, omega‐3 fatty acids, vitamin A, fiber, protein, probiotics, antioxidants, lycopene, and iron. The majority of included studies (34/36) focused on consumer WTP for ultra‐processed functional foods, while only two studies examined consumer WTP for low‐fat cheese and low‐fat beef. 28 , 29 The results demonstrated that consumers would pay more for food products that are specifically promoted as having health claims. A systematic review by Li et al. 30 examined consumer WTP for organic foods in China. They found that health consciousness is an important factor that influences consumer WTP for organic food. Further, a meta‐analysis by Li and Kallas 31 found that overall consumer WTP for more sustainably produced food products was on average 29.5% higher than regular products.
To date, no reviews have systematically examined consumer WTP for health aspects of food and beverages as defined by Australian Dietary Guidelines or any other equivalent national healthy eating guidelines. Greater knowledge of consumer WTP for healthier foods could help to determine consumer demand for healthy food and beverages and provide the evidence retailers need to move towards healthier food retail environments. The primary objective of the current review was to assess consumer WTP for healthier food and beverage options. This will help to determine consumer preferences for healthier food choices. The secondary objective was to identify factors that may influence consumer preference for healthier food and beverages.
2. METHODS
This systematic review was undertaken in accordance with the Preferred Reporting Items for Systematic Review and Meta‐Analysis (PRISMA) protocol. The protocol for this systematic review was registered in PROSPERO (CRD42021271974) on September 4, 2021.
2.1. Search strategy
The final search was conducted by the first author (MA) in September 2021 using the following databases: Medline Complete via EBSCOhost, Business Source Complete, Health Policy Reference Center, Global Health, CINAHL, EconLit, Web of Science, Embase, and Google Scholar (first 15 pages). Additional searches were conducted through backward searches (cited studies of included articles) and forward searches using SCOPUS (articles citing included studies) to capture any citations missed by electronic searches. The Cochrane library was searched for any relevant systematic reviews, and the reference list of relevant reviews was examined to identify potentially relevant studies. Search hedges and terms were combined using the following concepts: (i) consumer, (ii) healthy food or beverage, and (iii) WTP. Subject headings, keywords, and acronyms were searched and adapted for each database as appropriate. Details of the search strategy are included in the supporting information (Tables S1 and S2).
2.2. Inclusion and exclusion criteria
This review included original peer‐reviewed papers published in English from 2000 to September 6th, 2021, with full‐text available. Studies using quantitative, qualitative, and mixed methods were included. Conference abstracts, dissertations, protocols, book chapters, reviews, commentaries, letters to editors, editorials, opinion pieces, and newspaper articles were excluded. Consumer WTP‐derived through surveys, focus groups, auctions, choice experiments, conjoint analysis, and revealed preference or any other method were included in this review.
This review aimed to assess consumer WTP for healthy food and beverages as defined by the Australian Dietary Guidelines 32 or any other equivalent national guidelines (such as Canada's Dietary Guidelines for Health Professionals and Policy Makers, 33 Eating and Activity Guidelines for New Zealand Adults, 34 or the Eatwell Guide‐UK). 35 “Healthy” foods and beverages were defined as fruit; vegetables; grains; lean meat and poultry; milk, yoghurt, cheese, and their non‐diary alternatives; and foods and beverages with limited/reduced content of saturated fat, salt, and sugar. The review excluded studies that assessed consumer WTP for organic or specialty diets such as gluten‐free foods. Studies that assessed consumer WTP for functional/fortified food, food safety, alcoholic beverages, environmental, or sustainability aspects of food production (food miles, carbon footprint, etc.), food quality and sensory or flavor attributes of food were also excluded. Table 1 summarizes the review inclusion and exclusion criteria.
TABLE 1.
Final review eligibility criteria
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Language | English | All other languages |
| Publication date | 1st January 2000 to 6th September 2021 | Prior to 1st January 2000 |
| Publication type | Peer reviewed publications where full text was available | Conference abstracts, dissertations, protocols, book chapters, reviews, commentaries, letters to editors, editorials, opinion pieces, and newspaper articles |
| Study design | Real‐world studies, observational studies, natural experiments, case studies, and laboratory experiments | ‐ |
| Healthy food definition | Defined by the Australian Dietary Guidelines or any other equivalent national dietary guidelines | Organic food; functional/fortified food; food safety; alcoholic beverages; environmental aspects of food production; food quality, and sensory or flavor attributes of food |
| Outcome of interest |
Willingness to pay (WTP) results presented in monetary value and/or percentage (increase or decrease) |
No reporting of outcome of interest in monetary value or percentage |
2.3. Study selection
Search results from all databases were imported into an Endnote library in which duplicates were identified and removed. Titles and abstracts of the remaining manuscripts were double screened by the first author (MA) and a second reviewer (MB, TN, or IM) using the Covidence software. The full texts of included articles were double screened by the first author (MA) and a second reviewer (TN or IM), and the reasons for exclusion were noted. Disagreements that arose throughout the screening process were resolved by an additional third reviewer (JA).
2.4. Data extraction
A standardized data extraction template was developed in Microsoft Excel based on the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Good Research Practices for Conjoint Analysis framework. 36 All authors agreed upon the data extraction template in advance. The template was piloted on two studies by the first author (MA), discussed with all authors and then revised. The final data extraction template included the following details: study name, author details, year of publication, objectives, country, target population, context or setting, overall study design, conjoint analysis design, food product categories, attributes (product characteristics), attribute levels, method used to inform attribute levels, number of choice sets, sample size, participant recruitment methods, data collection procedure, statistical methods, and results. The following results were extracted or calculated where able: (i) percentage of consumers who are willing to pay higher prices for healthier food and beverages compared to conventional products, (ii) the price premium consumers are willing to pay in monetary value and/or percentage (increase or decrease), and (iii) factors influencing WTP. The incremental WTP price reported in each study was inflated into 2021 value using the World Bank food price inflation rate 37 and then translated into US dollars using purchasing power parities. 38 Where able, the results were also reported in 2021 US dollars per 100 g of the product. Data extraction was completed by the first author (MA) and checked for accuracy and completeness by a second reviewer (IM or TN). Inconsistencies were resolved by discussion with MB, MM, and JA.
2.5. Assessment of study quality
Most of the included studies were conjoint analyses including choice experiments. Therefore, we used the ISPOR Good Research Practices for Conjoint Analysis checklist to assess the reporting quality and considered this a proxy measure of the methodological quality of included choice experiment studies. The ISPOR checklist assesses 10 criteria, and each criterion has three items (total 30 items). Each item was assessed as “meeting the criteria” (the text sufficiently confirmed the criteria) or “not meeting the criteria” (criteria not met/no evidence or not enough evidence to justify the criteria in the text) and given a score of 1 or 0, respectively. For this study, we assumed that each item was equally weighted. However, the ISPOR checklist has no clear scoring system or cut off values to determine study quality. Quality assessment was completed independently by the first author (MA) and an additional reviewer (IM or TN). Disagreements were discussed and resolved by a third reviewer (JA).
2.6. Data synthesis
For the primary aim, the data were synthesized by food group, that is, (i) fruit and vegetables, (ii) grains, (iii) lean meat, and poultry and their alternatives and by nutrient (i) low in sugar, (ii) low in fat or cholesterol, and (iii) low in salt. In addition, data synthesis explored how WTP varied across products, settings, and consumer groups. Meta‐analysis was not conducted due to the varied methods utilized across studies, heterogeneity of the population and food products, and inconsistency in the reporting of outcomes. For the secondary aim, a qualitative synthesis of the data was undertaken using the following themes determined a priori: “favorable” factors (factors increasing consumer WTP), “unfavorable” factors (factors decreasing consumer WTP), or “neutral” factors (factors having no effect on consumer decisions to pay for healthier food and beverages).
3. RESULTS
Database searching of peer‐reviewed papers identified 9,257 relevant papers. After removal of duplicates, the title and abstract of 7,246 unique papers were screened and resulted in 65 full texts being assessed for eligibility. The inter‐rater reliability (IRR) of the titles and abstracts screening showed strong agreement between the independent reviewers (IRR score = 96%). Three publications were excluded because the full text was not available. Another 47 articles were excluded after full text screening, resulting in 15 articles being included in this review (Figure 1). The main reasons for exclusion were irrelevant outcomes such as consumer appreciation of the sensory quality of food products, impact of carbon food print on consumer choice, and experiments that assessed WTP of promotional strategies, functional food, sensory and flavor attributes of food, environmental or sustainable impacts of food production, or food quality. No additional articles were identified through backwards and forwards searches.
FIGURE 1.
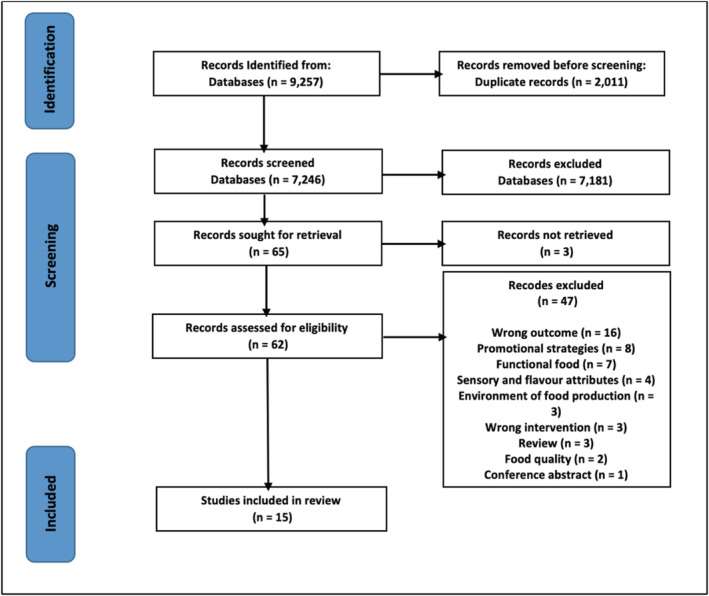
Preferred reporting items for systematic reviews and meta‐analyses (PRISMA) flow diagram of included studies, review of consumer willingness to pay for healthy food, and beverages, 2000–2021
3.1. Features of included studies
A summary of included studies is provided in Tables 2 and 3. The 15 included studies reported the results of 26 experiments. All the included experiments used quantitative approaches to estimate consumer WTP, with the majority using survey methods. Most of the experiments were conducted in Spain (n = 10) 28 , 39 , 43 , 44 , 46 and the USA (n = 5). 42 , 47 , 48 , 50 , 51 Another three experiments took place in the UK, 29 , 39 two in Peru, 41 while the remainder (one each) were from Australia, 40 Italy, 45 South Korea, 49 France, 29 Belgium, 29 and Netherlands. 29 In 10 experiments, the choice tasks were conducted online, 29 , 39 , 40 , 42 while one DCE survey was delivered by mail and completed in the participant's home. 50 The remaining experiments were conducted on‐site (face to face) in the premises of the research agency in metropolitan areas of capital cities or towns (n = 6), 28 , 44 supermarket and grocery stores (n = 3), 45 , 46 , 49 corner stores and food vendor settings in low‐income areas (n = 3), 41 , 47 university campus (n = 1), 48 and in the participant's home (n = 1). 43 One experiment used sales data obtained from grocery and non‐grocery stores to estimate consumer WTP. 51 In the vast majority of experiments (92%), the target population was aged 18 years or older and the primary household shopper or food consumer. 28 , 29 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 48 , 49 , 50 One experiment assessed youth (10–18 years) WTP for whole grain snacks with either fruit or vegetables. 47
TABLE 2.
General characteristics of the studies included in this review
| Author(s) | Country | Participant characteristics | Food product category | Setting | Design | Sample size (n participants) | Statistical analysis approach | Source of funding | |
|---|---|---|---|---|---|---|---|---|---|
| Study setting | Retail setting | ||||||||
| Akaichi et al. 39 | UK and Spain | Primary household shoppers; aged ≥18 years | Beef mince | Online | Not applicable | Stated preference method ‐ discrete choice experiment survey | UK:1211; Spain:1206 | Conditional logit model | The Scottish Government as part of the 2016–2021 Research Program on Food Security |
| Bellhouse et al. 40 | Australia | Australian primary household grocery shopper; aged ≥18 years | Pork product | Australia wide online survey | Not applicable | Stated preference method ‐ discrete choice experiment | 861 | Pearson's chi‐Squared test | The Pork Cooperative Research Centre (Australian Government) |
| Buttorff et al. 41 | Peru | Low‐income populations; aged ≥18 years | Meal with additional fruits or vegetables | Face‐to‐face | Food venders in low‐income urban area | Stated preference method ‐ discrete choice experiment | 432 | Conditional and rank‐ordered logit models | The International Development Research Centre (Canada) |
| Childs and Drake 42 | USA | Women (ages 25–55), primary shoppers of the household | Cheddar and Mozzarella cheeses | Online survey | Not applicable | Stated preference method ‐ conjoint analysis survey | 203 (Cheddar cheese), 198 (Mozzarella cheese); | General linear model | Dairy Management, Inc. (American Diary Association) |
| De‐Magistris and Gracia. 43 | Spain | Primary household shoppers aged ≥18 years | Semi‐cured, pasteurized sheep milk cheese | Face‐to‐face | Participants' homes in regional area (Castilla‐La‐Mancha) | Stated preference method ‐ experimental auction | 129 | Not available | European Commission |
| De‐Magistris, and Lopez‐Galan 28 | Spain | Primary food shoppers in households that consumed cheese products, aged ≥ 18 years | Cheese | Face‐to‐face | Participants recruited by research agency and the experiment was conducted on the premises of the agency | Stated preference method ‐ discrete choice experiment | 219 | Random parameters logit model | European Commission |
| De‐Magistris, Lopez‐alan and Caputo 44 | Spain | Obese and healthy‐weight consumers who are not under any clinical treatment; primary food buyers in households; aged ≥ 18 years | Potato chips | Face‐to‐face | Participants recruited by research agency and the experiment was conducted on the premises of the agency | Stated preference method ‐ discrete choice experiment | 309 | Random parameters logit model | National Institute of Agricultural and Food Research and Technology (Spain) and European Commission |
| Di Vita et al. 45 | Italy | Bread consumers; mean age 40.9 years | Bread | Face‐to‐face | Large retail store (supermarkets) in Sicily | Stated preference method ‐ contingent valuation method through a face‐to‐face questionnaire | 100 | Logistic model | Funded by the Project PO FESR 2007–2013 (supported by Sicily local government, Italian Government and European Union) |
| Jurado and Gracia 46 | Spain | Primary household shoppers who consumed breakfast biscuits | Breakfast cereal | Face‐to‐face | Mock/real‐brick supermarket in medium‐sized town | Stated preference method ‐ discrete Choice Experiment | 121 | Latent class logit model | Gobierno de Aragón (Government of Aragon) |
| Leak et al. 47 | USA | Youth (10–18 years); visitors to corners stores | Whole grain snack in combination with either fruits or vegetables | Face‐to‐face | Corners stores in low‐income communities in New York | Stated preference method ‐ contingent valuation (a one‐and‐one‐half‐bound dichotomous choice approach) | 402 | Multiple linear regression | The United States Department of Agriculture (USDA) |
| Lee et al. 48 | USA | Employees and students at the University of Illinois at Urbana Champaign (82% female); aged ≥18 years | Breakfast cereal | Face‐to‐face | University campus | Stated preference method ‐ conjoint analysis | 367 | Ordinary least squares regression | The Illinois Soybean Association |
| Lee et al. 49 | South Korea | Supermarket consumers | Canned ham | Face‐to‐face survey | Supermarkets | Stated preference method ‐ discrete choice experiment | 300 | Random parameters logit model |
The National Research Foundation of Korea Grant funded by the Korean Government |
| Lusk and Parker 50 | USA | Primary shoppers for home; aged ≥18 years | Ground beef | Delivered through mail survey | Home | Stated preference method ‐ discrete choice experiment | 220 | Multinomial Logit Model Estimates | Source of funding was not reported |
| Nganje et al. 51 | USA | N/A (used sales data) | Breads | Not applicable | Grocery and non‐grocery stores | Revealed preference method‐ data obtained from grocery and non‐grocery stores in regional market in Minnesota and North Dakota | N/A (used sales data)‐ number of observations 681 (include both conventional and low‐ carb bread) | Maximum Likelihood Estimation | Source of funding was not reported |
| Van Wezemael et al. 29 | France, Belgium, Netherland, UK | Beef consumers (i.e., people consuming beef at least once a month) | Beef steak | Online questionnaires | Not applicable |
Stated preference method ‐ discrete choice experiment |
2,400 (600 in each country) | Multinomial logit and error component models | The European Union |
TABLE 3.
Results of primary outcome of included experiments
| Author(s) | Standard food product | Healthier comparison food product | Mean incremental WTP value reported in original article | Mean incremental WTP in USD/100 g (2021 USD values) | Mean percentage change in price consumers willing to pay |
|---|---|---|---|---|---|
| Broad food categories (n = 3) | |||||
| Buttorff et al. 41 | Regular main meal | Regular meal plus additional large salad | 1.12 Nuevo Soles per meal | $0.72 a | 74.7% |
| Regular meal plus additional fruit (2 bananas) | 0.11 Nuevo Soles per meal | $0.07 a | 7.3% | ||
| Leak et al. 47 | Regular whole grain snack | A whole grain snack with either fruit or vegetables and condiments | US$ 2.38 per snack | $2.56 b | 23% |
| Healthier nutrient content of specific food products (reduced fat claims) (n = 16) | |||||
| Akaichi et al. 39 |
Regular beef mince (2 experiments in UK and Spain) |
Low fat beef mince (3 g/100 g serving) (UK) | € 3.41 per 100 g | $5.23 | 41% |
| Moderate fat beef mince (12 g/100 g serving) (UK) | € 2.23 per 100 g | $3.41 | 27% | ||
| Low fat beef mince (3 g/100 g serving) (Spain) | € 1.94 per 100 g | $3.06 | 26% | ||
| Moderate fat beef mince (12 g/100 g serving) (Spain) | € 1.57 per 100 g | $2.48 | 21% | ||
| Bellhouse et al. 40 | Regular pork | Lower cholesterol pork (15% less than regular cholesterol pork) | A$ 1.5/330 g | $0.42 | 21.6% |
| Childs and Drake 42 | Regular full fat Cheddar and Mozzarella cheeses | Lower fat Cheddar and Mozzarella cheeses (75% fat reduction or 3 g of fat or less per reference amount) | Range from US$ 0.25 to 0.5/25 g | Range from 1.24 to 2.48 | NA |
| De‐Magistris and Gracia 43 | Regular full fat cheese | Light cheese (40% reduced fat content) | € 0.060/100 g | $0.1 | 7% |
| De‐Magistris, and Lopez‐Galan 28 | Regular full fat cheese | Cheese with reduced fat content (30% less fat) | € 0.538/100 g | 0.89 | 47.8% |
| De‐Magistris et al. 44 | Regular potato chips | Potato chips with reduced fat claims (30% less fat compared to regular chips) |
People with healthy weight: €0.45/150 g People with obesity: €0.53/150 g |
People with normal weight: $0.49 People with obesity: $ 0.59 |
People with normal weight: 38.5% People with obesity: 45% |
| Jurado and Gracia 46 | Regular breakfast cereal | Reduced saturated fat cereal (amount of fat reduction is not specified) | € 1.83 per box (500 g) | $0.6 | 91.5% |
| Lusk and Parker 50 | Regular ground beef | Ground beef with total fat reduced from 20% to 10% when saturated fat is 30% and 50%, respectively |
30% saturated fat: US$ 2.06/pound 50% saturated fat: US$ 0.58/pound |
30% reduced fat claims: $ 0.57 50% reduced fat claims: $ 0.16 |
30% reduced fat claims: 25% 50% reduced fat claims: 12% |
| Nganje et al. 51 | Regular bread | Reduced fat bread. (36% fat reduction compared to conventional bread) | 0.023 cents per g ($0.14 per loaf) | $3.0 | 5.6% |
| Van Wezemael et al. 29 |
Regular beef steak (4 experiments in Netherlands, Belgium, France, and UK) |
A beef steak with 10% less fat in four European countries (Netherlands) | €5.78/kg | $0.97 | 48% |
| A beef steak with 10% less fat in four European countries (Belgium) | €5.60/kg | $0.96 | 47% | ||
| A beef steak with 10% less fat in four European countries (France) | €6.73/kg | $1.10 | 56% | ||
| A beef steak with 10% less fat in four European countries (UK) | € 1.20/kg | $ 0.2 | 10% | ||
| Healthier nutrient content of specific food products (low salt claims) (n = 4) | |||||
| De‐Magistris, and Lopez‐Galan 28 | Regular cheese | Cheese with low salt content (0.03 g of salt per 150 g) | −€0.38/100 g | −$0.63 | −33% |
| De‐Magistris et al. 44 | Regular potato chips | Potato chips with low salt content (0.03 g of salt per 150 g) |
People with healthy weight: −€0.15/150 g People with obesity: €0.40/15 g |
People with healthy weight: −$0.16 People with obesity: $0.47 |
People with healthy weight: −12.5% People with obesity: 34% |
| Di Vita et al. 45 | Regular bread | Breads with low sodium content (no more than 120 mg of sodium/100 g) |
€ 0.47/100 g |
$0.76 | 20% |
| Lee et al. 49 | Regular canned ham | Reduced salt canned ham (amount of salt reduction is not specified) | 274 KRW to 313 KRW per reduced salt can (340 g) | Range from $0.12 to $0.14 | 7.8 to 8.9% |
| Healthier nutrient content of specific food products (multiple claims) (n = 3) | |||||
| De‐Magistris, and Lopez‐Galan 28 | Regular cheese | Cheese with reduced fat contents (30% less fat compared to traditional cheese) and low salt contents (30 mg of salt per 150 g) | €0.15/100 g | $0.24 | 16% |
| De‐Magistris et al. 44 | Regular potato chips | Potato chips with reduced fat claims (30% less fat compared to traditional chips) and low salt contents (30 mg of salt per 150 g) |
People with healthy weight: €0.48/150 g People with obesity: €0.10/15 g |
People with healthy weight: $0.53 People with obesity: $0.11 |
People with healthy weight: 40.5% People with obesity: 8.5% |
| Lee et al. 48 | Regular breakfast cereal | Healthy breakfast cereal (high fiber, low fat, low sugar, low calorie) (amount not specified) | Participants favorably rated costs of US$1.49 and $2.49 per 14 oz (396.89 g)/ (cost of regular cereal range between US$2.09 and US$3.19) | −$0.50 to −$0.84 | −28% to ‐ 41% |
Abbreviation: KRW, Korean Won.
Per meal.
Per snack.
Most of the experiments (25 of 26) 28 , 29 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 used stated preference methods to elicit consumer WTP for healthier foods, and only one experiment used the revealed preference method of hedonic pricing. 51 Twenty two of the 25 experiments that used stated preference methods were DCEs or conjoint analyses, while the other three used contingent valuation 41 , 47 and experimental auctions. 43 Only 5 of the 15 studies 28 , 29 , 39 , 40 , 44 included in this review reported that their WTP questions were piloted. The sample size of included experiments ranged from 100 45 to 1,211 39 participants. The wide range in the sample size might be related to the mode of administration of the survey and/or the target population of interest. For example, the number of participants in studies that used an online survey 29 , 39 , 40 were higher than studies that used face to face 28 , 41 , 43 , 44 , 46 , 47 , 48 , 49 or mail‐based surveys. 50 Also, studies that were conducted at a national level 29 , 39 , 40 had a larger sample size than studies that were conducted at the city level or in specific settings such as in supermarket, home, or university campus. The experiment by Nganje et al. 51 did not involve participants directly and instead used sales data (681 observations) to estimate consumer WTP.
3.2. Quality appraisal
The methodological quality of included studies varied between 23% (the lowest score achieved) and 97% (highest score achieved). Nine out of 15 (60%) studies reported more than 50% of the recommended items on the ISPOR checklists for conjoint analysis. The ISPOR checklist was specifically designed for conjoint analysis studies; studies that used DCE or conjoint analysis approaches had higher scores in comparison to studies that used different methodology. Some of the ISPOR checklist items such as attribute identification and selection may not be applicable to studies that used experimental auction, contingent valuation, and hedonic pricing methods (four studies). In the remaining two studies that scored with less than 50% on the ISPOR checklist, the studies were published before the ISOPR checklist, and therefore, the low score might indicate inadequate reporting of the ISPOR items rather than poor quality. The items that scored the lowest and were less frequently reported were item 2.2 (Was attribute selection justified and consistent with theory?); item 4.2 (Were the properties of the experimental design evaluated?); item 5.1 (Was there sufficient motivation and explanation of conjoint tasks?); item 7.3 (Were ethical considerations addressed [e.g., recruitment, information and/or consent, compensation]?); and item 8.2 (Was the quality of the responses examined [e.g., rationality, validity, reliability]?). See Table S3 for quality scores of individual studies.
3.3. Consumer willingness to pay for healthier food products
Seven experiments reported the percentage of total participants who would pay more for healthier products. 39 , 40 , 45 , 46 Within these seven experiments, 69.7% to 79% of the participants would pay a price premium (a higher price) for healthier food. All the included experiments reported the incremental monetary value and/or percentage price (increase or decrease) customers would pay for healthier products. Twenty‐three experiments (88.5%) 29 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 49 , 50 , 51 showed that consumers would pay a price premium for healthier products compared to less healthy alternatives (positive WTP), two experiments showed negative WTP results, 28 , 48 and in one experiment, the results were inconclusive. 44 In the 23 (88.5%) experiments that showed positive WTP, consumers were willing to pay a price premium of between 5.6% and 91.5% (mean 30.74%) for healthier products compared to conventional (regular) alternatives.
3.3.1. Willingness to pay for broad food categories
Only three experiments assessed consumer WTP by food category, with the remainder assessing WTP by nutrient content. Buttorff et al. 41 conducted two experiments to assess food vendor consumers' WTP for a meal with additional fresh salad and a meal with additional fruits in low‐income urban areas in Lima, Peru. They found that consumers were willing to pay a mean premium of US$0.72 per meal (a 74.7% price premium) for the addition of a large salad (vegetables), and US$0.07 per meal for the addition of fruit (2 bananas), representing a 7.3% price premium. The third experiment by Leak et al. 47 assessed youth (10–18 years) WTP for whole grain snacks with the addition of either fruits or vegetables in corner stores in low‐income areas in New York city (USA). The results suggested that youth on average would pay US$2.56 (23%) more for the whole grain snack with either fruits or vegetables compared to the whole grain snack alone.
3.3.2. Willingness to pay for healthier nutrient content of specific food products
Sixteen experiments 28 , 29 , 40 , 42 , 43 , 44 , 46 , 48 , 50 assessed consumer WTP for various products such as beef, pork, cheese, potato chips, and breakfast cereals with reduced fat content. All of these experiments showed positive results where consumers were willing to pay a higher price (premium) for lower fat products. Price premiums varied by population and by the percentage reduction in fat content; for example, Akaichi et al. 39 assessed consumer WTP for reduced fat in beef mince in the UK and Spain in 2020. The study reported that participants would pay a premium of US$3.06 (26%) for low fat and US$2.48 (21%) for moderate fat beef mince in Spain, whereas in the UK, participants would pay a mean US$5.23 (41%) more for low fat and US$3.41 (27%) more for moderate fat beef mince.
Four experiments assessed consumer WTP for foods with reduced salt or sodium content. One of these experiments suggested that consumers would pay a 33% lower price for cheese with lower salt content compared to regular products. 28 Two experiments found that consumers would pay a 20% price premium for healthier bread (with reduced salt) 45 and between 7.8% to 8.9% for canned ham 49 with reduced salt content. In one experiment, the results were not conclusive; people with obesity had positive WTP for healthier chips with lower salt and would pay a 34% price premium, while people with healthy weight had negative WTP and would pay 12.5% less for the healthier choice. 44
Three experiments assessed consumer WTP for products with healthier content of multiple nutrients (e.g., low fat and low salt, and low fat and low sugar). De‐Magistris et al. 28 , 44 conducted two experiments to assess consumer WTP for cheese and potato chips with reduced fat and salt content in Spain. They found that consumers on average would pay US$ 0.24/100 g (16%) more for cheese and between US$0.11 and US$0.53/100 g (8.5% to 40.5%) more for potato chips with both lower fat and salt content. A third experiment conducted by Lee et al. 48 found that university employees and students in USA had a mean 28% to 41% lower WTP for healthy breakfast cereals (high in fiber, low fat and sugar and multigrain ingredients) in comparison to regular cereal.
3.4. Factors influencing consumer willingness to pay for healthier food products
Twelve out of the 15 included studies 28 , 29 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 48 , 49 reported at least one factor that influenced consumer WTP for healthier food. These factors can be classified into two groups: consumer‐related factors (gender, age, income, health status, etc.) and product‐related factors (sensory attributes, flavor and texture, price, and labeling). Based on their impact on consumer WTP for healthy food, we categorized them into “favorable” factors (factors increasing consumer WTP for healthier products), “unfavorable” factors (factors decreasing consumer WTP for healthier products), or “neutral” factors (factors having no effect on consumer WTP for healthier products). Table 4 provides an overview of these factors and their empirical support across studies.
TABLE 4.
Overview of factors influencing consumer willingness to pay for healthier food products
| Factor domain | Favorable factors | Unfavorable factors | Neutral factors |
|---|---|---|---|
| Consumer‐related | |||
| Product‐related |
|
‐ |
The results suggest that consumer‐related factors such as age, gender, and BMI status impact WTP estimates. People over 60 years, females, those living with obesity, and consumers who participate in regular physical activity were more willing to pay a premium for healthier food. On the other hand, younger consumers with healthy weight and higher levels of income and education were not willing to pay higher prices for healthier food. Household size and body image dissatisfaction of people with obesity were found to have neutral impacts on consumer WTP for healthier products. Also, the results suggested that some product‐related factors such as higher price and change in food flavor, and texture may act as barriers to purchasing of healthier food. Information provided through health and nutritional labeling was found to have a favorable impact on consumer WTP.
4. DISCUSSION
4.1. Consumer willingness to pay for healthier food products
This is the first systematic review to assess consumer WTP for healthier food according to national dietary guidelines. It reviewed the evidence from 15 articles (26 experiments) and provides a systematic synthesis of the evidence of consumer WTP for healthier products. It advances the existing literature on how consumers value healthier products and contributes to our understanding of consumer preferences for healthier food. Given that customer satisfaction is important to supermarket and grocery store retailers, the findings of this review may be instructive for decision‐making related to implementation and maintenance of interventions to improve the healthiness of the food retail environment.
The overall WTP analysis shows that in most of the experiments (88.5%), consumers showed a preference for healthier food in comparison to conventional food, demonstrated by WTP a price premium ranging from 5.6% to 91% (mean 30.74%) for healthier products. These results were consistent with the results of a meta‐analysis by Dolgopolova and Teuber, 27 who found that 91.4% of included studies showed a positive WTP (range from 50% to 400% price premium) for health benefits associated with food products, and a meta‐analysis by Li and Kallas 31 found that overall consumer WTP for sustainable food products was on average 29.5% higher compared to regular products.
The incremental WTP estimates may be affected by the type of food products, type of elicitation method, setting, and population of study. All experiments that assessed consumer WTP for food with reduced fat showed positive results. This was consistent with the meta‐analysis by Dolgopolova and Teuber, 27 who found that products with a health claim to lower cholesterol levels had a statistically significant positive impact on consumer WTP. Also, our results showed that consumers are willing to pay a premium for snacks with fruits and vegetables. This result was consistent with an analysis that was conducted by Fang and Levy, 52 who found that Chinese and French consumers would pay more for organic fruits. Only two of the four experiments that assessed consumer WTP for food with reduced salt or sodium showed positive results. The reasons behind this could be due to consumers' underestimation of the health risks associated with sodium consumption, 53 attitudes towards impact of salt reduction on the taste of food, 54 and the lack of awareness of dietary sources of salt and the daily recommendations for salt intake. 55 However, when the food product had both reduced salt and fat, our results suggests that consumers would pay a price premium. 28 , 44 , 56 One experiment showed that consumers would pay a lower price for food with both low fat and low sugar. 48 This result was not consistent with the study conducted by Cadena et al., 57 who found that lower fat and sugar ingredients in ice cream did not reduce consumers acceptance of the ice cream. However, there is a paucity of research related to WTP for products with lower sugar content. No experiment assessed consumer WTP for healthier beverage and food with lower sugar levels exclusively. These results suggest that there is strong evidence that consumers are willing to pay a higher price for healthier products and in particular for foods with lower fat content. Future studies need to focus more on consumer WTP for healthier beverage and food with reduced sugar and salt.
Our results also suggest that hypothetical elicitation methods such as DCE, conjoint analysis, and contingent valuation may overestimate the consumer WTP value compared to non‐hypothetical methods (auctions). For example, De‐Magistris et al. 28 , 44 conducted two experiments to assess consumer WTP for cheese with reduced fat content. In the first experiment, they used an experimental auction to assess consumer WTP for light cheese (40% reduced‐fat content) and found that the mean percentage change in price consumers would pay was approximately 7%. 28 , 44 In the second experiment, they used a DCE (30% reduced‐fat content) and found that consumers would pay a mean 47.8% price premium. 28 , 44 These results were consistent with the results of the meta‐analyses by Dolgopolova and Teuber. 27 and Li and Kallas, 31 who found that hypothetical elicitation methods lead to higher WTP compared to non‐hypothetical methods.
Our results suggest that there may be differences in WTP by country. On average, consumers in Europe are willing to pay a mean price premium of 34.8% (range from 7% to 91.5%) for healthier products, 29 , 42 , 45 , 47 , 48 , 50 , 51 which is higher than values elicited in USA (mean: 16.4%; [range from 5.6% to 25%]). 42 , 47 , 48 , 50 , 51 Two experiments conducted in South America (Peru) 41 found WTP ranged from 7.3% to 74.7%. Only one study conducted in Asia (South Korea) 49 and Australia 40 where the mean percentage change in price consumers were willing to pay for healthier products was 8.4% and 21.6%, respectively. However, these differences could reflect the varied products tested in these countries, limiting cross country comparisons.
4.2. Factors influencing consumers' willingness to pay for healthier food products
The results of this review suggest that many factors drive consumer WTP for healthier food. Consumer‐related factors included demographics and consumer attitudes regarding their own health. Product‐related factors including price, food labeling and flavor, and sensory attributes of the food were reported to have the greatest influence on consumer decisions to purchase healthier foods.
Demographic factors such as age, gender, level of education, and income were the most reported demographic factors that may influence consumer WTP. These results are consistent with a previous review by Katt and Meixner, 58 who found that age, gender, income, and education were the main drivers that influence consumer WTP for organic food. Our results indicate that people over 60 years and female consumers were more likely to pay higher prices for healthier products, whereas males and younger populations were less likely to pay a premium for healthier food. A potential explanation is that younger consumers are generally healthier and do not have health problems that are impacted by their diet. People over 60 years and women have been shown to be more likely to make food choices based on health considerations. 59 This review found that a high level of education and income had an unfavorable impact on consumer WTP. 28 , 46 This is contrary to previous evidence that suggests that food shoppers with higher levels of education and income are more likely to purchase food that is lower in risk nutrients such as sugar, salt, and fat. 60 However, it is difficult to make definitive and generalizable conclusions based on the results of two studies.
This review found that consumers who are more concerned with their health 48 , 49 and/or who regularly engage in physical activity 45 would pay a higher price for healthier food. These results are consistent with the results of the study conducted by Nguyen and Truong, 61 who found that psychological factors and, in particular, health concerns had significant favorable impacts on consumer WTP for organic food. A study by Ali and Ali 62 found that health consciousness and awareness about health attributes of food were key factors that influenced consumer WTP for healthier food products.
Sensory attributes, flavor and texture, price and food labeling were the most reported product‐related factors that influenced consumer WTP for healthier food. We found that increase in price of healthier food products compared to regular alternatives, 48 and perceived change in flavor and texture 42 may reduce consumer WTP for healthier products. These results were consistent with the results of a study conducted by Krystallis et al., 63 who found that consumers had lower satisfaction with the sensory characteristics of reduced fat food. Also, our results suggest that increased consumer knowledge through health and nutritional food labelling had a favorable impact on consumer WTP for healthier products. 29 These results were consistent with other studies that found food labeling had a favorable impact on consumer WTP. 27 , 64 , 65
4.3. Strengths and limitations of the review and included studies
This review has several strengths. Only peer‐reviewed studies were included to improve the quality of the results. All study designs that can provide WTP valuations were included to ensure all relevant studies were included in the synthesis. The reporting of results in USD 2021 values per 100 g and calculation of the price premium percentage allowed better comparisons across studies and easier transferability of results. In addition to the assessment of consumer WTP, this review explored factors that may impact on consumers' decisions to purchase healthier products. This may help public health specialists and policy makers to develop and design more effective and targeted health promotion interventions.
However, our review has some limitations. Only studies published in English were included in this review. Also, gray literature and non‐peer‐reviewed studies were not included and therefore some studies that have not been published or are published in other languages may have been missed. It is possible that publication bias impacted these results; however, it is not clear whether publication bias would favor studies reporting increased WTP for healthy or less healthy foods. It is possible that publication bias may have resulted in studies demonstrating lower consumer WTP for healthier foods being less likely to be published. It is likely that studies reporting non‐significant findings may not have been published which would attenuate the findings of this study.
The majority of studies included in this review used elements of best practice reporting as identified by ISPOR. However, the included studies had several limitations. The quality of included studies varied considerably. Forty percent of included studies had a quality rating of less than 50%, 27% had a quality rating between 50% and 74%, and 33% had a quality rating of 75% or above. Since most studies used stated preference methods, the consumer WTP value could potentially be overestimated because stated preference methods present hypothetical purchasing scenarios rather than real purchasing decisions. 66 Using an integrated approach that combines both stated preference methods and revealed preference or auctions may improve the accuracy and reduce bias of the results. 67 However, using integrated methods would entail substantially higher cost and time. Meta‐analysis was not possible due to incomparable methods, heterogeneity of population and food products, and inconsistency in the reporting of outcomes. The results of this review have identified the research gaps in assessing consumers' WTP for healthier food products. Reporting guidelines that cover a range of WTP studies are required to increase comparability of results. This will allow for more consistency in methodology and reporting of the outcomes, and improved generalizability of the results. Most studies were conducted in high‐income countries in Europe, USA, Australia, and South Korea. Only one study that included two experiments was conducted in low‐income neighborhoods in Peru (an upper‐middle income country). 41 Future studies that assess consumer WTP for healthy food in low‐income countries are required to fill this evidence gap. Also, the target group in most studies was primary household shoppers (most commonly women) and persons aged 18 years or over. Therefore, more studies are required to assess consumer WTP for other populations such as youth and other non‐primary household shoppers.
5. CONCLUSION
Consumer perspectives are important to retailers and customers' perception of healthier food retail environments are an important determinant of the successful implementation and maintenance of retail interventions. This review focuses on assessing consumer WTP for healthier products as per Australian Dietary Guidelines. It is clear from the results of this review that, on average, consumers value healthier food products more than conventional alternatives and are willing to pay a premium for healthier options, demonstrating consumer preference and therefore potential demand for healthier products. This could provide food retailers with the evidence required to move towards healthier food retail environments. Future studies need to focus more on assessing consumer WTP for healthier beverages and low sugar food products. Also, further studies are required to focus more on younger populations including youth and school students' preferences for healthier products within retail environments and consumers' WTP for healthier products in middle‐ and low‐income countries.
CONFLICT OF INTEREST
The authors declare that they have no competing interest.
AUTHOR CONTRIBUTIONS
Moosa Alsubhi conceived the study, designed, and conducted the bibliographic search; undertook paper screening, quality assessment, data extraction, and synthesis; interpreted the results; and drafted and edited the paper. Ishani Majmudar and Tan Nguyen undertook paper screening, quality assessment, and data extraction and helped edit the paper. Miranda Blake, Marj Moodie, and Jaithri Ananthapavan contributed to the design of the study, provided methodological input, and assisted in paper screening, quality assessment, and editing the paper. All authors read and approved final version of the paper.
Supporting information
Table S1. Search Strategy
Table S2: List of subject headings terms used for the database searches
Table S3: Quality scores of individual studies.
ACKNOWLEDGMENTS
MA and IM received a Deakin University Postgraduate Research (DUPR) scholarship. MB is funded by an Alfred Deakin Postdoctoral Research Fellowship. TN is funded by the National Health and Medical Research Council Postgraduate Scholarship Scheme (APP1189802) and Dental Health Services Victoria. MA, MB, MM, and JA are researchers within the National Health and Medical Research Council funded Centre of Research Excellence in Food Retail Environments for Health (RE‐FRESH, APP1152968). Funders had no role in the systematic review process. Open access publishing facilitated by Deakin University, as part of the Wiley ‐ Deakin University agreement via the Council of Australian University Librarians.
Alsubhi M, Blake M, Nguyen T, Majmudar I, Moodie M, Ananthapavan J. Consumer willingness to pay for healthier food products: A systematic review. Obesity Reviews. 2023;24(1):e13525. doi: 10.1111/obr.13525
Funding information Deakin University; National Health and Medical Research Council (NHMRC)‐funded Centre of Research Excellence in Food Retail Environments for Health (RE‐FRESH), Grant/Award Number: APP1152968
REFERENCES
- 1. Beaglehole R, Yach D. Globalisation and the prevention and control of non‐communicable disease: the neglected chronic diseases of adults. Lancet. 2003;362(9387):903‐908. doi: 10.1016/s0140-6736(03)14335-8 [DOI] [PubMed] [Google Scholar]
- 2. Crosland P, Ananthapavan J, Davison J, Lambert M, Carter R. The health burden of preventable disease in Australia: a systematic review. Aust N Z J Public Health. 2019;43(2):163‐170. doi: 10.1111/1753-6405.12882 [DOI] [PubMed] [Google Scholar]
- 3. World Health Organisation . Report of the Commission on Ending Childhood Obesity. In: Implementation Plan: Executive Summary; Report No.: WHO/NMH/PND/ECHO/17.1. Geneva: WHO; 2017. [Google Scholar]
- 4. Hawkes C, Jewell J, Allen K. A food policy package for healthy diets and the prevention of obesity and diet‐related non‐communicable diseases: the NOURISHING framework. Obes Rev. 2013;14(Suppl 2):159‐168. doi: 10.1111/obr.12098 [DOI] [PubMed] [Google Scholar]
- 5. Swinburn B, Sacks G, Vandevijvere S, et al. INFORMAS (international network for food and obesity/non‐communicable diseases research, monitoring and action support): overview and key principles. Obes Rev. 2013;14(Suppl 1):1‐12. doi: 10.1111/obr.12087 [DOI] [PubMed] [Google Scholar]
- 6. Carlson AC, Kinsey JD, Nadav C. Consumers' retail source of food: a cluster analysis. Fam Econ Rev. 2002;14(2):11‐20. [Google Scholar]
- 7. Lang THM. Food Wars: The Global Battle for Mouths, Minds and Markets. 2nd ed. Earthscan; 2015. doi: 10.4324/9781315754116 [DOI] [Google Scholar]
- 8. Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804‐814. doi: 10.1016/s0140-6736(11)60813-1 [DOI] [PubMed] [Google Scholar]
- 9. Mah CL, Luongo G, Hasdell R, Taylor NGA, Lo BK. A systematic review of the effect of retail food environment interventions on diet and health with a focus on the enabling role of public policies. Curr Nutr Rep. 2019;8(4):411‐428. doi: 10.1007/s13668-019-00295-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Middel CNH, Schuitmaker‐Warnaar TJ, Mackenbach JD, Broerse JEW. Systematic review: a systems innovation perspective on barriers and facilitators for the implementation of healthy food‐store interventions. Int J Behav Nutr Phys Act. 2019;16(1):108. doi: 10.1186/s12966-019-0867-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Peeters A. Obesity and the future of food policies that promote healthy diets. Nat Rev Endocrinol. 2018;14(7):430‐437. doi: 10.1038/s41574-018-0026-0 [DOI] [PubMed] [Google Scholar]
- 12. Gittelsohn J, Rowan M, Gadhoke P. Interventions in small food stores to change the food environment, improve diet, and reduce risk of chronic disease. Prev Chronic Dis. 2012;9:E59. doi: 10.5888/pcd9.110015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pinard CA, Byker Shanks C, Harden SM, Yaroch AL. An integrative literature review of small food store research across urban and rural communities in the U.S. Prev Med Rep. 2016;3:324‐332. doi: 10.1016/j.pmedr.2016.03.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Adam A, Jensen JD. What is the effectiveness of obesity related interventions at retail grocery stores and supermarkets?—a systematic review. BMC Public Health. 2016;16(1):1247. doi: 10.1186/s12889-016-3985-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Cameron AJCE, Ngan WW, Sacks G. A systematic review of the effectiveness of supermarket‐based interventions involving product, promotion, or place on the healthiness of consumer purchases. Curr Nutr Rep. 2016;5(3):129‐138. doi: 10.1007/s13668-016-0172-8 [DOI] [Google Scholar]
- 16. Escaron AL, Meinen AM, Nitzke SA, Martinez‐Donate AP. Supermarket and grocery store‐based interventions to promote healthful food choices and eating practices: a systematic review. Prev Chronic Dis. 2013;10:E50. doi: 10.5888/pcd10.120156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Glanz K, Bader MDM, Iyer SS. Retail grocery store marketing strategies and obesity: an integrative review. Am J Prev Med. 2012;42(5):503‐512. doi: 10.1016/j.amepre.2012.01.013 [DOI] [PubMed] [Google Scholar]
- 18. Hartmann‐Boyce J, Bianchi F, Piernas C, et al. Grocery store interventions to change food purchasing behaviors: a systematic review of randomized controlled trials. Am J Clin Nutr. 2018;107(6):1004‐1016. doi: 10.1093/ajcn/nqy045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Liberato SC, Bailie R, Brimblecombe J. Nutrition interventions at point‐of‐sale to encourage healthier food purchasing: a systematic review. BMC Public Health. 2014;14(1):919. doi: 10.1186/1471-2458-14-919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Slapø H, Schjøll A, Strømgren B, Sandaker I, Lekhal S. Efficiency of in‐store interventions to impact customers to purchase healthier food and beverage products in real‐life grocery stores: a systematic review and meta‐analysis. Foods. 2021;10(5):922. doi: 10.3390/foods10050922 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ronto R, Rathi N, Worsley A, Sanders T, Lonsdale C, Wolfenden L. Enablers and barriers to implementation of and compliance with school‐based healthy food and beverage policies: a systematic literature review and meta‐synthesis. Public Health Nutr. 2020;23(15):2840‐2855. doi: 10.1017/s1368980019004865 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Gupta A, Alston L, Needham C, et al. Factors influencing implementation, sustainability and scalability of healthy food retail interventions: a systematic review of reviews. Nutrients. 2022;14(2):294. doi: 10.3390/nu14020294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Blake MR, Backholer K, Lancsar E, et al. Investigating business outcomes of healthy food retail strategies: a systematic scoping review. Obes Rev. 2019;20(10):1384‐1399. doi: 10.1111/obr.12912 [DOI] [PubMed] [Google Scholar]
- 24. Houghtaling B, Serrano EL, Kraak VI, Harden SM, Davis GC, Misyak SA. A systematic review of factors that influence food store owner and manager decision making and ability or willingness to use choice architecture and marketing mix strategies to encourage healthy consumer purchases in the United States, 2005‐2017. Int J Behav Nutr Phys Act. 2019;16(1):5. doi: 10.1186/s12966-019-0767-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Thorpe CP, Boelsen‐Robinson T, Cameron AJ, Blake MR. Business outcomes of healthy food service initiatives in schools: a systematic review. Obes Rev. 2021;22(8):e13264. doi: 10.1111/obr.13264 [DOI] [PubMed] [Google Scholar]
- 26. Anderson JC, Jain DC, Chintagunta PK. Customer value assessment in business markets. J Bus‐Bus Mark. 1992;1(1):3‐29. doi: 10.1300/J033v01n01_02 [DOI] [Google Scholar]
- 27. Dolgopolova I, Teuber R. Consumers' willingness to pay for health benefits in food products: a meta‐analysis. Appl Econ Perspect Policy. 2018;40(2):333‐352. doi: 10.1093/aepp/ppx036 [DOI] [Google Scholar]
- 28. de‐Magistris T, Lopéz‐Galán B. Consumers' willingness to pay for nutritional claims fighting the obesity epidemic: the case of reduced‐fat and low salt cheese in Spain. Public Health. 2016;135:83‐90. doi: 10.1016/j.puhe.2016.02.004 [DOI] [PubMed] [Google Scholar]
- 29. van Wezemael L, Caputo V, Nayga R, Chryssochoidis G, Verbeke W. European consumer preferences for beef with nutrition and health claims: a multi‐country investigation using discrete choice experiments. Food Policy. 2014;44(C):167‐176:167‐176. doi: 10.1016/j.foodpol.2013.11.006 [DOI] [Google Scholar]
- 30. Li R, Lee H‐Y, Lin Y‐T, Liu C‐W, Tsai PF. Consumers' willingness to pay for organic foods in China: bibliometric review for an emerging literature. Int J Environ Res Public Health. 2019;16(10):1713. doi: 10.3390/ijerph16101713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Li S, Kallas Z. Meta‐analysis of consumers' willingness to pay for sustainable food products. Appetite. 2021;163:105239. doi: 10.1016/j.appet.2021.105239 [DOI] [PubMed] [Google Scholar]
- 32. National Health and Medical Research Council (NHMRC) . Australian Dietary Guidelines. Canberra: NHMRC; 2013. [Google Scholar]
- 33. Health Canada . Canada's Dietary Guidelines for Health Professionals and Policy Makers. Ottawa: Health Canada; 2019. [Google Scholar]
- 34. Ministry of Health . Eating and Activity Guidelines for New Zealand Adults: Updated 2020. Wellington: Ministry of Health; 2020. [Google Scholar]
- 35. Public Health England . The Eatwell Guide. London: Public Health England; 2016. [Google Scholar]
- 36. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403‐413. doi: 10.1016/j.jval.2010.11.013 [DOI] [PubMed] [Google Scholar]
- 37. The World Bank . A global database of inflation 1970–2022. 2021. Available from: www.worldbank.org/en/research/brief/inflation-database. Accessed 11 May, 2022.
- 38. Organisation for Economic Co‐operation and Development (OECD) . Eurostat‐OECD methodological manual on purchasing power parities. Luxembourg: Eurostat‐ OECD; 2012. [Google Scholar]
- 39. Akaichi F, Revoredo Giha C, Glenk K, Gil JM. How consumers in the UK and Spain value the coexistence of the claims low fat, local, organic and low greenhouse gas emissions. Nutrients. 2020;12(1):120. doi: 10.3390/nu12010120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Bellhouse A, Malcolm B, Griffith GR, Dunshea F. Australian consumers' willingness to pay and willingness to purchase a hypothetical lower cholesterol pork product. Aust Agribus Rev. 2010;18:161‐192. doi: 10.22004/ag.econ.114414 [DOI] [Google Scholar]
- 41. Buttorff C, Trujillo AJ, Diez‐Canseco F, Bernabe‐Ortiz A, Miranda JJ. Evaluating consumer preferences for healthy eating from community kitchens in low‐income urban areas: a discrete choice experiment of Comedores Populares in Peru. Soc Sci Med. 2015;140:1‐8. doi: 10.1016/j.socscimed.2015.06.033 [DOI] [PubMed] [Google Scholar]
- 42. Childs JL, Drake M. Consumer perception of fat reduction in cheese. J Sens Stud. 2009;24(6):902‐921. doi: 10.1111/j.1745-459X.2009.00243.x [DOI] [Google Scholar]
- 43. de‐Magistris T GA. Consumers' willingness to pay for light, organic and PDO cheese. Br Food J. 2016;118(3):560‐571. doi: 10.1108/BFJ-09-2015-0322 [DOI] [Google Scholar]
- 44. de‐Magistris T, López‐Galán B, Caputo V. The impact of body image on the WTP values for reduced‐fat and low‐salt content potato chips among obese and non‐obese consumers. Nutrients. 2016;8(12):830. doi: 10.3390/nu8120830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. di Vita G, DaM LA, Pecorino B. Evaluating trends of low sodium content in food: the willingness to pay for salt‐reduced bread, a case study. Agric Econ Rev. 2016;17(2):82‐99. [Google Scholar]
- 46. Jurado F, Gracia A. Does the valuation of nutritional claims differ among consumers? Insights from Spain. Nutrients. 2017;9(2):132. doi: 10.3390/nu9020132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Leak TM, Setiono F, Gangrade N, Mudrak E. Youth willingness to purchase whole grain snack Packs from new York City corner stores participating in a healthy retail program. Int J Environ Res Public Health. 2019;16(18):3233. doi: 10.3390/ijerph16183233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Lee CM, Moskowitz HR, Lee SY. Expectations, needs and segmentation of healthy breakfast cereal consumers. J Sens Stud. 2007;22(5):587‐607. doi: 10.1111/j.1745-459X.2007.00127.x [DOI] [Google Scholar]
- 49. Lee SH, Han DB, Caputo V, Nayga RM Jr. Consumers' valuation for a reduced salt product: a nonhypothetical choice experiment. Can J of Agric Econ. 2015;63(4):563‐582. doi: 10.1111/cjag.12081 [DOI] [Google Scholar]
- 50. Lusk J, Parker N. Consumer preferences for amount and type of fat in ground beef. J Agric and Appl Econ. 2009;41(1):48763‐48790. doi: 10.1017/S107407080000256X [DOI] [Google Scholar]
- 51. Nganje WE, Kaitibie S, Wachenheim CJ, Acquah ET, Matson J, Johnson G. Estimating price premiums for breads marketed as “low‐carbohydrate breads”. J Food Distrib Res. 2008;39(2):66‐76. doi: 10.22004/ag.econ.55976 [DOI] [Google Scholar]
- 52. Fang Z, Levy E. An analysis of consumption and purchasing toward organic fruits: Cross‐countries study between China and France. 2015.
- 53. Cheung J, Neyle D, Chow PPK. Current knowledge and behavior towards salt reduction among Hong Kong citizens: a cross‐sectional survey. Int J Environ Res Public Health. 2021;18(18):9572. doi: 10.3390/ijerph18189572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Liem DG, Miremadi F, Keast RSJ. Reducing sodium in foods: the effect on flavor. Nutrients. 2011;3(6):694‐711. doi: 10.3390/nu3060694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Grimes CA, Kelley S‐J, Stanley S, et al. Knowledge, attitudes and behaviours related to dietary salt among adults in the state of Victoria, Australia 2015. BMC Public Health. 2017;17(1):532. doi: 10.1186/s12889-017-4451-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Fellendorf S, Kerry JP, O'Sullivan MG. Consumer attitudes on salt and fat reduced foods in the Republic of Ireland. Food Nutr Sci. 2018;9(7):880‐898. doi: 10.4236/fns.2018.97066 [DOI] [Google Scholar]
- 57. Cadena RS, Cruz AG, Faria JAF, Bolini HMA. Reduced fat and sugar vanilla ice creams: sensory profiling and external preference mapping. J Dairy Sci. 2012;95(9):4842‐4850. doi: 10.3168/jds.2012-5526 [DOI] [PubMed] [Google Scholar]
- 58. Katt F, Meixner O. A systematic review of drivers influencing consumer willingness to pay for organic food. Trends Food Sci Technol. 2020;100:374‐388. doi: 10.1016/j.tifs.2020.04.029 [DOI] [Google Scholar]
- 59. Chambers S, Lobb A, Butler LT, Traill WB. The influence of age and gender on food choice: a focus group exploration. Int J Consum Stud. 2008;32(4):356‐365. doi: 10.1111/j.1470-6431.2007.00642.x [DOI] [Google Scholar]
- 60. Turrell G, Kavanagh AM. Socio‐economic pathways to diet: modelling the association between socio‐economic position and food purchasing behaviour. Public Health Nutr. 2006;9(3):375‐383. doi: 10.1079/phn2006850 [DOI] [PubMed] [Google Scholar]
- 61. Nguyen DT, Truong DC. The impact of psychological and environmental factors on consumers' purchase intention toward organic food: evidence from Vietnam. J Asian Finance Econ Bus. 2021;8:915‐925. [Google Scholar]
- 62. Ali T, Ali J. Factors affecting the consumers' willingness to pay for health and wellness food products. J Agric Food Res. 2020;2:100076. doi: 10.1016/j.jafr.2020.100076 [DOI] [Google Scholar]
- 63. Krystallis A, Arvanitoyannis IS, Kapirti A. Investigating Greek consumers' attitudes towards low‐fat food products: a segmentation study. Int J Food Sci Nutr. 2003;54(3):219‐233. doi: 10.1080/09637480120091973 [DOI] [PubMed] [Google Scholar]
- 64. Cooper SL, Butcher LM, Scagnelli SD, et al. Australian consumers are willing to pay for the health star rating front‐of‐pack nutrition label. Nutrients. 2020;12(12):3876. doi: 10.3390/nu12123876 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Ouyang Y, Sharma A. Consumer‐citizen willingness to pay for healthy eating messages. Int Contemp Hosp Manag. 2019;31(2):890‐909. doi: 10.1108/IJCHM-08-2017-0490 [DOI] [Google Scholar]
- 66. Fifer S, Rose J, Greaves S. Hypothetical bias in stated choice experiments: is it a problem? And if so, how do we deal with it? Transportation Research Part a: Policy and Practice. 2014;61(C):164‐177:164‐177. doi: 10.1016/j.tra.2013.12.010 [DOI] [Google Scholar]
- 67. de Corte K, Cairns J, Grieve R. Stated versus revealed preferences: an approach to reduce bias. Health Econ. 2021;30(5):1095‐1123. doi: 10.1002/hec.4246 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Search Strategy
Table S2: List of subject headings terms used for the database searches
Table S3: Quality scores of individual studies.