

Abstract
Revaccination after receipt of a hematopoietic cell transplant (HCT) or cellular therapies is a pillar of patient supportive care, with the potential to reduce morbidity and mortality linked to vaccine‐preventable infections. This review synthesizes national, international, and expert consensus vaccination schedules post‐HCT and presents evidence regarding the efficacy of newer vaccine formulations for pneumococcus, recombinant zoster vaccine, and coronavirus disease 2019 in patients with hematological malignancy. Revaccination post‐cellular therapies are less well defined. This review highlights important considerations around poor vaccine response, seroprevalence preservation after cellular therapies, and the optimal timing of revaccination. Future research should assess the immunogenicity and real‐world effectiveness of new vaccine formulations and/or vaccine schedules in patients post‐HCT and cellular therapy, including analysis of vaccine response that relates to the target of cellular therapies.
Keywords: bispecific, CAR‐T cell, cellular therapy, hematologic malignancy, stem cell transplant, vaccination
Abbreviations
- aRZV
adjuvanted recombinant zoster vaccine
- BCMA
B‐cell maturation antigen
- CAR‐T
chimeric antigen receptor T cell
- CD19
cluster of differentiation 19
- CD20
cluster of differentiation 20
- COVID‐19
coronavirus disease 2019
- GvHD
graft‐versus‐host disease
- HCT
hematopoietic cell transplant
- HM
hematologic malignancy
- IgG
immunoglobulin G
- IVIg
intravenous immunoglobulin
- MMR
measles, mumps, and rubella
- PCV
pneumococcal conjugate vaccine
- PPSV23
pneumococcal 23‐valent polysaccharide vaccine
- SARS‐CoV‐2
severe acute respiratory syndrome coronavirus 2
- VZV
varicella zoster virus
1. INTRODUCTION
Between 50 000 and 100 000 hematopoietic cell transplants (HCT) are performed annually worldwide. 1 , 2 Over 20 000 people globally have received Food and Drug Administration‐approved cellular therapy, particularly chimeric antigen receptor T‐cell (CAR‐T) product for treatment of lymphoma, myeloma, or leukemia. 3 Infection remains a significant cause of morbidity and mortality among patients with hematological malignancies (HM), including those experiencing enduring remission after transplant or cellular therapies. Vaccination strategy represents a pillar of supportive care that can help augment protection against infection (Figure 1).
FIGURE 1.
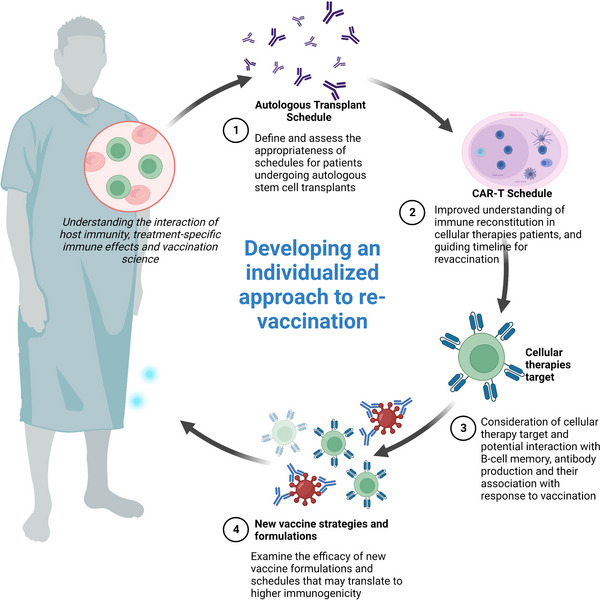
Future approaches to vaccine research for hematopoietic cell transplant (HCT) and cellular therapies patients.
Together with antimicrobial prophylaxis, intravenous immunoglobulin (IVIg), and early antimicrobial therapy, vaccination aims to reduce the burden of infection in patients post‐transplant and cellular therapies. Regarding vaccine‐preventable infections, late viral reactivations, such as varicella zoster, are common among both HCT recipients and cellular therapy patients, with reports of severe disseminated disease. 4 , 5 , 6 , 7 , 8 Similarly, instances of overwhelming sepsis secondary to encapsulated organisms, such as Streptococcus pneumoniae or Haemophilus influenzae, have been reported. 9 , 10 , 11 The coronavirus disease 2019 (COVID‐19) pandemic demonstrated how hematology patients, especially those treated with cellular therapies and HCT, are disproportionately affected by infectious diseases that lack adequate prevention strategies, leading to more severe disease, more frequent re‐infections and poorer vaccine response. 12 , 13 , 14 , 15
However, marrying vaccine studies with clinical outcomes remains challenging. The clinical relevance of reduced antibody titers post‐HCT or cellular therapies is poorly understood, given that only a limited number of vaccine‐preventable diseases have been reported. For the general population, with exception of the influenza vaccine, there is a lack of immune correlates of absolute or relative protection for other vaccine‐preventable diseases, including COVID‐19. 16 , 17 , 18 , 19 When interpreting results from published studies of vaccine response in HCT recipients, it is important to recognize the dominant focus of humoral (serologic) endpoints, the lack of measurement of cell‐mediated responses and the lack of correlation between immunogenicity and clinical endpoints. 20 , 21 An ongoing challenge that remains, including recent examples of vaccination against Respiratory syncytial virus (RSV) 22 and influenza, 23 is that the inclusion of HCT recipients in initial clinical trials is often delayed despite being one of the highest risk groups for disease and related complications.
This review aims to comprehensively discuss the evidence for vaccination strategies in HCT patients, focusing on newer vaccine formulations, evidence for optimized dosing regimens, and vaccine adjuncts. It also aims to review the emerging evidence informing vaccination strategies following cellular therapies, highlighting questions around retained seroprevalence, vaccine response, and the interplay between immune reconstitution and vaccine timing. Potential future directions for translational vaccinology, including the individualization of revaccination approach in hematology patients, are discussed.
2. VACCINATION IN HCT RECIPIENTS
Infection after HCT is a major cause of morbidity and mortality, with vaccine‐preventable infections being a potential contributor. Underpinning this are complex deficiencies in humoral and cell‐mediated immune responses, including opsonization, related to the transplant conditioning regimen, hypogammaglobulinemia, prophylaxis or management of graft‐versus‐host disease (GvHD) for allogeneic HCT or maintenance therapies for autoHCT. 24 , 25 , 26 , 27 , 28 , 29 , 30 Regardless of pre‐transplant donor or recipient vaccinations, HCT recipients may lose their immunity to various pathogens if the recipient is not revaccinated. 25 , 26 , 27 , 28 , 29 Therefore, it is recommended to consider HCT patients as “never vaccinated” and requiring a full revaccination schedule, considering age, country, and epidemiology.
International guidelines with recommended schedules have been published, with commencement of vaccination usually occurring 3–6 months after HCT. 24 , 31 , 32 , 33 , 34 , 35 , 36 This may differ between centers and be deferred (other than inactivated influenza vaccine) to commence at 12 months if there is potential for delayed immune reconstitution or negative impact of therapy, indicated by therapies received including anti‐cluster of differentiation 20 (CD20) mAb <6 months ago or blood parameters including CD4+ T‐cell count <200/μL and cluster of differentiation 19 (CD19)+ B‐cell count <20/μL. 24 , 31 , 32 , 33 , 34 , 35 There are no data to support any specific lymphocyte level for starting vaccines, however, and delaying vaccination increases the at‐risk period for the patient. 32 After HCT, it may be reasonable to delay vaccination for at least 6 months after the last dose of anti‐CD20 mAb therapy and/or other B‐cell‐depleting therapies. 24 , 32
Inactivated vaccines are safe after transplant, although immunogenicity may be reduced post‐transplant compared with healthy individuals, with improvement over time and close to expected response at 2–3 years post‐transplant. 31 , 37 Inactivated vaccines are not inhibited by IVIg replacement. 24 Patients with GvHD are at higher risk of infection and therefore benefit from vaccination; however, vaccine response may be impaired due to immunosuppression used to treat GvHD. Live‐attenuated vaccines are only recommended in specific circumstances and at least 24 months post‐transplantation due to the risk of vaccine‐transmitted disease. 31 , 32 , 33 , 34 Optimal vaccination of household contacts is encouraged, including live‐attenuated measles, mumps, and rubella (MMR) and varicella zoster virus (VZV) vaccine if indicated, but not intranasal live‐attenuated influenza vaccine or live‐attenuated oral polio vaccine due to prolonged viral shedding and risk of transmission. 33 , 38
Where available, updates are discussed in the sections below with existing recommendations by various international bodies summarized in Table 1. 31 , 32 , 33 , 34 , 35 , 36
TABLE 1.
Recommended vaccines and timing post‐hematopoietic cell transplant (HCT) from established international guidelines.
| Vaccine‐preventable infection and vaccine(s) | Recommendations | ||||||
|---|---|---|---|---|---|---|---|
| ECIL‐7 (2017) 32 | DGHO (2018) 141 | IDSA (2013) 33 | International (2009) 35 | UK (2023) 36 | ACIP (2023) 142 | AIH (2023) 143 | |
|
Pneumococcal: PCV13, PCV15, PCV20 PPSV23 |
Three doses of PCV 1 month apart from 3–6 months after HCT, followed by a fourth dose of PCV if GvHD or PPSV23 6 months later 32 |
Three doses of PCV 1 month apart, from 3 to 6 months after HCT Booster dose given at 18 months post‐HCT with PCV if GvHD or PPSV23 if no GvHD |
Three doses of PCV 1–2 months apart, from 3 to 6 months after HCT, with PPSV23 8 weeks after last dose of PCV or at 12 months post‐HCT. PCV as fourth dose if GvHD. New proposal to substitute fourth dose of PPSV23 with PCV20 144 |
Three doses of PCV from 6 months after HCT at 6, 8, and 12 months post‐HCT PPSV23 starting at 24 months post‐HCT then >5 years later |
|||
|
Hemophilus type B: Hib conjugate vaccine |
Three doses of Hib vaccine at 1‐month intervals, from 3 months after HCT OR Three doses of combined diphtheria–tetanus–pertussis–Hib vaccine from 6 months after HCT |
Three doses of Hib vaccine, from 6 to 12 months post‐HCT | Three doses of HiB at 2‐month intervals, from 6 to 12 months post‐HCT | Similar to DGHO/IDSA | Three doses of Hib vaccine, at least 1‐month interval, at 6 months post‐HCT | Three doses of Hib vaccine at 6, 8, and 12 months after HCT | |
|
Neisseria meningitidis: Quadrivalent (ACYW135) Conjugate (MCV‐4) Monovalent C conjugate (MCV‐C) Anti‐B vaccines MenB‐MC MenB‐fHBP |
Recommended in accordance with local guidelines Two doses of vaccine against serotypes B and C, 6 months post‐HCT |
1–2 doses of conjugate tetravalent vaccine, 6–12 months post‐HCT | Two doses of MCV‐4 6–12 months post‐HCT for 11– 18 years | Follow country guidelines, one dose, 6–12 months post‐HCT |
Two doses of MCV‐4, 8 and 10 months post‐HCT Two doses of a MenB vaccine at a 2‐month interval, at 6 months post‐HCT |
MCV‐4 for individuals 11–18 years or at high risk from 6 months post‐HCT Serogroup B meningococcal vaccine for individuals 16–23 years of age or at high risk, at 6 months post‐HCT |
Two doses of any MCV‐4 vaccine at 2‐month intervals, from 6 months post‐HCT MenB: Two doses of Bexsero, at 2 month intervals, from 6 months post‐HCT OR Three doses of Trumenba at 1 and 5‐month intervals, from 6 months post‐HCT |
|
Diphtheria and tetanus a : DT (full dose diphtheria) Td (reduced dose diphtheria) DTaP (higher dose of tetanus, diphtheria, pertussis toxoid) Tdap (lower dose formulation) Bordetella pertussis a : Acellular pertussis vaccine—ap (pertussis toxoid) |
Three doses of diphtheria–tetanus vaccine at 1–2‐month interval, from 6 months after HCT for all ages 145 Full dose diphtheria (DT) vaccine preferred over reduced dose antigen formulation diphtheria toxoid (Td) to achieve adequate seroprotection Three doses (for pertussis) given in combination with each dose of the diphtheria–tetanus vaccine from 6 months after HCT |
Three doses of DTaP for patients <7 years, 1–2‐month intervals, at 6 months post‐HCT For patients ≥7 years, options include: three doses of DTaP OR one dose of Tdap and two doses of DT OR one dose of Tdap and two doses of Td at 1–2‐month intervals, from 6 months post‐HCT |
Three doses of diphtheria‐tetanus vaccine at 1–2 months interval, from 6 months after HCT DTPa for children <10 years dTpa for ≥10 years of age for first dose then two doses of dT. If unavailable, then complete with dTpa |
||||
|
Polio virus a : IPV DTPa‐IPV dTpa‐IPV |
Three doses of IPV administered at 1–2‐month intervals, 6–12 months after HCT |
Three doses of IPV administered at 1–2‐month intervals 6–12 months after HCT Can be given in combination with diphtheria, tetanus, pertussis vaccines |
|||||
|
HPV: 4vHPV or 9vHPV |
Follow local guidelines for general population and start 6–12 months post‐HCT |
Three‐dose schedule is recommended for all HCT recipients aged 12 and over ACIP currently advises vaccination with either 4vHPV or 9vHPV in immunocompromised persons age 9–26 years |
Three doses of 9vHPV at 0, 2, 6 months, starting at 8 months post‐HCT If >25 years of age, conduct risk assessment to determine their need for HPV vaccination |
||||
|
HBV: HBV vaccine Engerix |
Three doses at 0, 1, and 6 months apart, 6–12 months post‐HCT in those non‐immune to HBV | Three doses at 0, 1, and 6 months apart at 6–12 months post‐HCT | Follow general population recommendations in their country of residence | Three doses at 0, 1, and 6 months, from 6 months post‐HCT | Three doses at 0, 1, and 6 months apart, from 6 months post‐HCT | Three doses (high‐dose formulation is preferred) at 6, 8, and 12 months post‐HCT | |
|
Influenza virus: IIV Live intranasal influenza vaccine is contraindicated |
One dose of IIV, annually, at the beginning of influenza season Second dose at 3–4 weeks later could be considered in patients expected to have impaired immune response, or during outbreaks in patients vaccinated <6 months post‐HCT |
One dose of IIV, annually, at 3–6 months post‐HCT Second dose should be considered in patients who have had early vaccination |
One dose of IIV annually, starting 6 months post‐HCT or 4 months post‐HCT if there is a community outbreak |
One dose of IIV annually Consider second dose if the vaccine is given <6 months post‐HCT |
One dose of IIV annually, from 6 months post‐HCT Consider commencing at 3 months post‐HCT if a peak influenza transmission period |
One dose of IIV, annually from 6 months post‐HCT Second dose if first dose is given <4 months after HCT |
Two doses of IIV in the first year post‐HCT and then one dose annually thereafter. Adjuvant IIV recommended for those ≥65 years of age 143 |
| SARS‐CoV‐2 | Predated SARS‐CoV‐2 |
Three doses of COVID‐19 (preferably mRNA) vaccine starting 3–6 months post‐HCT as primary course Further booster vaccine doses recommended as per local guidelines, and at least 3–6 months after the last dose of vaccine 36 , 75 , 79 , 146 |
|||||
|
Varicella zoster virus: LAVV |
LAVV can be administered at ≥24 months post‐HCT in varicella‐seronegative HCT recipients who do not have active GvHD, are not receiving any immunosuppression (some recommend for >12 months) and are 8–11 months after the last dose of IVIg (UK guidelines suggest 3 months post‐IVIg) 24 , 33 , 48 , 49 , 50 A second dose could be administered 4 weeks after the first |
LAVV at 24 months post‐HCT and no GvHD and the patient is considered immunocompetent | Two doses of LAVV, 4 weeks apart at 24 months post‐HCT if there is evidence of immune reconstitution | ||||
|
Herpes zoster virus: aRZV, adjuvanted recombinant zoster virus vaccine (inactivated), Shingrix |
Predated aRZV vaccine | Two doses aRZV at least 2 months apart, commencing at 6 months following HCT | Two doses of aRZV 6–12 months post‐allogeneic SCT and 3–12 months post‐autologous SCT | Two doses of aRZV at 6 and 8 months post‐HCT | |||
|
MMR: MMR live virus vaccine |
One dose of MMR vaccine to seronegative HCT recipients >24 months post‐transplantation; no GvHD, no immunosuppression, no relapse of the underlying disease, no recent IVIg (at least 3 months) |
Two doses of MMR vaccine to seronegative patients with same criteria applied | Two doses of MMR vaccine, 6 months apart in adult recipients of autologous and allogeneic HCT who are 24 months post procedure, no GvHD, no systemic immunosuppression for >12 months, and are seronegative | MMR vaccine at 24 months post‐HCT if the patient does not have GvHD and is considered immunocompetent | One dose of MMR vaccine at 24 months post‐HCT if they have met criteria. Check serology at 4–6 weeks after 1st vaccine dose—if no seroconversion, repeat the dose | ||
Abbreviations: 4vHPV, 4‐valent human papillomavirus vaccine; 9vHPV, 9‐valent human papillomavirus vaccine; ACIP, Advisory Committee on Immunization Practices; ACYW‐135, meningococcal quadrivalent conjugate vaccine; AIH, Australian Immunization Handbook; ap, acellular pertussis vaccine; aRZV, adjuvanted recombinant zoster virus vaccine; COVID‐19, coronavirus disease 2019; DGHO, German Society of Hematology and Oncology; DT, full dose diphtheria vaccine; DTaP, higher dose diphtheria, tetanus, and acellular pertussis vaccine; DTPa‐IPV, higher dose diphtheria, tetanus, acellular pertussis, and inactivated poliovirus combination vaccine; dTpa‐IPV, reduced antigen formulation diphtheria–tetanus–pertussis–inactivated poliovirus combination vaccine; ECIL‐7, European Conference on Infections in Leukaemia; GvHD, graft‐versus‐host disease; HBV vaccine, hepatitis B virus; Hib, Haemophilus influenzae type B conjugate vaccine; HiB, Haemophilus influenzae B; HPV, human papillomavirus vaccine; IDSA, Infectious Diseases Society of America; IIV, inactivated influenza vaccine; IPV, inactivated polio virus vaccine; IVIg, intravenous immunoglobulin; LAVV, live‐attenuated varicella vaccine; MCV‐4, meningococcal conjugate vaccine; MCV‐C, monovalent meningococcal serogroup C conjugate vaccine; MenB‐fHBP—Trumenba, recombinant lipidated factor H binding protein meningococcal serogroup B vaccine; MenB‐MC, recombinant multicomponent meningococcal serogroup B vaccine; MMR, measles, mumps, and rubella live virus vaccine; PCV, pneumococcal conjugate vaccine; PPSV23, pneumococcal 23‐valent polysaccharide vaccine; SARS‐CoV‐2, severe acute respiratory syndrome coronavirus 2; Td, reduced dose diphtheria–tetanus combination vaccine; Tdap, reduced dose tetanus, diphtheria, acellular pertussis combination vaccine.
Combination vaccine available diphtheria–tetanus–pertussis plus polio (dTpa‐IPV).
2.1. Updated or new formulation vaccines for HCT
2.1.1. Streptococcus pneumoniae
There is a recognized high risk of invasive pneumococcal disease after autologous and allogeneic HCT, related to low specific antibody titers, with approximately 85% of patients unprotected 6 months after transplantation. 10 , 39 , 40 Of note, most patients are infected by vaccine serotypes. 9 , 41 The current guideline recommendation is to provide three doses of pneumococcal conjugate vaccine (PCV) 1 month apart starting 3–6 months post‐HCT. The increased immunogenicity and clinical effectiveness of PCV compared to pneumococcal 23‐valent polysaccharide vaccine (PPSV23) has been demonstrated. 30 , 32 , 33 , 42 , 43 , 44 , 45 This is then followed by a fourth dose of PCV if the patient has GvHD or one dose of PPSV23 6 months later to increase the spectrum of serotype coverage. 30 , 32 , 33 Some centers may start pneumococcal vaccination at 12 months post‐HCT and check serology 1 month after the third or fourth dose of vaccine.
Newer vaccine formulations are now available in some countries, including 20‐valent PCV (PCV20) and 15‐valent PCV (PCV15), offering additional serotype coverage. There are no current studies of PCV20 in HCT recipients. An alternate strategy proposed by the Advisory Committee on Immunization Practices is to provide a fourth dose of PCV20 (in place of PPSV23) at least 6 months after the third PCV20 dose or 12 months after HCT, whichever is later. This specific recommendation has not been studied; however, it is based on two studies that assessed the use of four PCV13 doses and found improved humoral immunity from after the third dose to after the fourth dose. 45 , 46 Local and systemic reactions however occurred more frequently after the fourth PCV13 dose than after the first to third dose of PCV13, although most were mild–moderate. 45
2.1.2. Varicella zoster virus vaccines
The prevention of primary VZV infection in seronegative patients and reactivation in seropositive patients (zoster and postherpetic neuralgia) is of prime importance in patients post‐HCT. 7 , 8 Antiviral prophylaxis (acyclovir or valacyclovir) is usually administered for at least 24 months post‐allogeneic HCT and 12 months after autologous HCT; however, may be longer if there is ongoing immunosuppression or GvHD. 7 , 8 , 47 However, there are limitations to prophylaxis, including uncertainty around optimal duration, ongoing compliance, and lack of reconstitution of cellular immunity. Based on evidence from several observational studies, the live‐attenuated varicella vaccine can be administered at ≥24 months post‐HCT in varicella‐seronegative HCT recipients who do not have active GvHD, are not receiving any immunosuppression (some recommend for >12 months) and are not receiving immunoglobulin (Ig) replacement. 24 , 33 , 48 , 49 , 50 There is an expected response rate of ∼65% with some clinical protection. A second dose could be administered 4 weeks after the first, although evidence of clear benefit is lacking. 24 , 33 , 48 , 49 , 50 The risks and benefit of this decision should be carefully considered, given reports of fatal cases of vaccine‐related disseminated VZV. 6 , 51 Patients should be aware of this risk within 3 weeks of vaccination and to seek antiviral treatment if required. 32 The live‐attenuated zoster vaccine (Zostavax) is not recommended by some published guidelines due to higher antigen levels in this formulation and has been associated with case reports of fatal disseminated vaccine‐strain infection. 32 , 33 , 35 , 52 , 53 , 54 However, Zostavax has been assessed in patients >24 months post‐HCT with adequate immunogenicity and no adverse effects on safety profiling in carefully selected patient cohorts. 55 , 56 , 57 , 58 , 59 Zostavax is no longer marketed in the United States. An inactivated version of Zostavax was also studied in autologous HCT recipients and found to be efficacious against the prevention of herpes zoster; however, it has not been made commercially available. 60
Shingrix, an inactivated, adjuvanted recombinant zoster vaccine (aRZV) is now available and recommended to prevent reactivation in seropositive immunocompromised patients. 61 , 62 It is a subunit vaccine containing VZV glycoprotein E and the AS01b adjuvant system. 5 , 62 In a large, international, multicenter phase III clinical trial, 1846 adult autologous HCT recipients were randomized to receive two doses of aRZV or placebo 50–70 days following HCT and then 1–2 months later. 5 After a median of 21 months of follow‐up, the vaccinated group had a lower incidence of herpes zoster compared with the placebo group, with reported efficacy of 68.2%. 5 Humoral immune response rates were in the range of 70%–80%, with similar rates reported in other immunocompromised patients, including those with HM, solid tumors, human immunodeficiency virus, and solid organ transplant. 5 There was also reduction in postherpetic neuralgia, herpes zoster virus‐associated complications and hospitalization. 5
For allogeneic seropositive HCT recipients, only observational data exists for the assessment of adjuvanted vaccines including the aRZV vaccine. 63 , 64 In these studies, patients have been vaccinated between 9 months to greater than 2 years post‐allogeneic HCT. 63 , 64 , 65 There have been mixed results in regard to immunogenicity but no increase in GvHD. 63 , 64 , 65 In one study, cell‐mediated immunity was significantly enhanced in patients with prior shingles compared to those without prior shingles and male sex. 65 The recommended aRZV vaccine schedule is with two doses 2–6 months apart and to continue antiviral prophylaxis 1 month after the first vaccination. The use of aRZV in allogeneic HCT recipients and optimal timing need to be defined through future studies.
For all zoster vaccines, it is important to acknowledge that efficacy is difficult to assess, given that most of the data are based on company‐developed assays and are specific to these vaccine studies. Currently, there are no commercially available methods for addressing the protection of herpes zoster.
2.1.3. COVID‐19 vaccines
Observational studies have demonstrated impaired humoral immune response post two doses of vaccine in patients post‐HCT, with estimated seroresponse rates of 61%–81%. 66 , 67 , 68 , 69 B‐cell‐depleting therapy within 12 months has been found to be a major determinant of impaired humoral immunity. 67 , 70 , 71 Despite this, there does appear to be a preserved cellular immune response, even in patients treated with B‐cell‐depleting therapy, which has demonstrated prior importance in the severity of COVID‐19 infection. 66 , 72 , 73 , 74 In this context, the recommended primary course of vaccination is with three doses of COVID‐19 vaccine. 67 , 75 , 76 , 77 , 78 , 79 , 80 Seroresponse rates post three doses of vaccine are improved compared to two doses and have been estimated to be in the range of 63%–90% in autologous HCT recipients and 58%–90% in allogeneic HCT recipients. 66 , 81 , 82 , 83 , 84 This may be dependent on timing of vaccination relative to the transplant and use of any concurrent immunosuppressive therapies. 69 , 77 In allogeneic HCT recipients, lower seroresponse to three doses of vaccine has been found in HCT recipients of haploidentical donors, those with chronic kidney disease and lower lymphocyte count. 69 , 73 Starting from 3 to 6 months after transplantation, it is recommended to revaccinate HCT recipients with a full primary series of three doses, following the recommended schedule for each specific vaccine. 75 , 79 Immunogenicity analysis (humoral and cell‐mediated immunity) from a recent observational cohort study of allogeneic HCT recipients supports the commencement of mRNA severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) revaccination at 3 months post‐transplantation, immune responses were not influenced by concurrent GvHD or immunosuppressive regimen. 85 The third dose should be given at least 28 days after the second dose. The mRNA vaccine alternatives (Pfizer Bio‐N‐Tech or Moderna mRNA‐1273) are the preferred option where available due to greater efficacy and safety evidence in immunocompromised patients for an expanded primary course and further booster doses. 67 , 75 , 76 , 77 , 78 , 79 , 86 Booster dose(s) are recommended after the three‐dose primary course to optimize immunogenicity, and 86 the timing is suggested as per local guidelines but at least 3 months after the third dose. 76 At the time of writing, updated variant‐specific mRNA COVID‐19 vaccines are now preferred as the booster dose. 79
Clinical effectiveness studies have found reduced severity of COVID‐19 in vaccinated patients with HM; however, there is still significant morbidity and mortality from breakthrough infection. 13 , 75 , 87 In a study of four‐dose vaccinated patients with HM, rates of hospitalization, oxygen requirement, and mortality of 38.2%, 21.6%, and 3.9%, respectively, were found with breakthrough COVID‐19. 87 Waning immunity and reduced vaccine effectiveness against SARS‐CoV‐2 variants of concern have also been observed in patients with HM. 88 Alternate vaccination strategies, including delayed intervals between vaccine doses, heterologous dosing, and bivalent Omicron‐specific mRNA vaccines, have shown improved immunogenicity in the general population and require ongoing assessment in HCT recipients. 89 , 90 , 91 , 92 , 93 , 94
Non‐mRNA COVID‐19 vaccines are also available, including non‐replicating competent adenovirus vector vaccines (AstraZeneca/ChAdOx1‐S and Johnson&Johnson/Jansen/Ad26.COV2‐S), as well as the recombinant nanoparticle protein‐based vaccine Novavax/NVX‐CoV2373, although published safety and efficacy data are limited in HCT recipients. 75 , 95 , 96 , 97 In a small study of hemato‐oncological patients, Ad26.COV2‐S appeared safe as a heterologous vaccine booster after two doses of BNT162b2 vaccine. 98 In hematology malignancy patients with diseases and treatments impacting B‐cell immunity, in those who received two doses of ChAdOx1 vaccination followed by an mRNA vaccine, even in the absence of seroconversion robust SARS‐CoV‐2‐specific T‐cell immunity was documented. 74
3. VACCINATION FOLLOWING CELLULAR THERAPIES
Less is known about the burden of vaccine‐preventable infections and the role of revaccination in patients treated with cellular therapies. 11 , 99 , 100 Late‐infection data are still emerging, and the long‐term effects of sustained B‐cell depletion on infection are unclear. 101 , 102 , 103 Prolonged B‐cell aplasia, loss of memory B cells, and subsequent hypogammaglobulinemia may impair humoral protection against various infections, including vaccine‐preventable diseases. 101 , 104 , 105 , 106 , 107 The field is currently aiming to determine the extent to which antibody immunity is preserved following cellular therapies, optimize timing of revaccination following treatment, and identify key predictors of vaccine response from hematological markers of immune reconstitution.
3.1. Preservation of immunity: the retention of pathogen‐specific antibodies following cellular therapies
Few studies have systematically explored the persistence of pathogen‐specific IgGs after CAR‐T therapy. Available seroprevalence data is often adjunctive and exploratory; for example, comparing the prevalence of existing antibodies to vaccine‐preventable infections between CAR‐T treated patients and healthy controls to explore reasons for poor humoral response following SARS‐CoV‐2 vaccination. 108 , 109 Studies specifically aiming to characterize the effect of CAR‐T therapy on circulating pathogen‐specific IgGs are summarized in Table 2. 110 , 111 , 112 , 113 , 114 , 115 Studies differ in the timing of antibody measurement post‐CAR‐T, the exclusion or inclusion of patients receiving Ig replacement, and data are aggregated across mixed populations of leukemia, lymphoma, and myeloma patients. 110 , 111 , 112 , 113 , 114 , 115 , 116 Data regarding seroprevalence in patients treated with bispecific or non‐CD19+ directed CAR‐T (e.g., B‐cell maturation antigen [BCMA]) therapies are lacking. 117
TABLE 2.
Summary of studies examining seroprevalence of circulating immunoglobulin G against vaccine‐preventable infections.
| Author (year) | Angelidakis et al. (2022) 110 | Bansal et al. (2021) 111 | Rahman et al. (2019) 116 | Hill et al. (2019) 113 | Shah et al. (2021) 114 | Walti et al. (2021) 115 |
|---|---|---|---|---|---|---|
| Design | Prospective | Retrospective | Prospective | Retrospective | Retrospective | Retrospective |
| Population | 38 | 40 | 8 | 40 | 21 | 85 |
| Malignancy | Mixed | Lymphoma | DLBCL | Mixed | DLBCL | Mixed |
| CAR‐T target | CD19+ | CD19+ | CD19+ | CD19+ | CD19+ | CD19+ BCMA |
| Prior HCT | 5 (13) | 25 (63) | Not reported | Not reported | 5 (24) | 32 (49) |
| IVIg | 3/31 (10) | 23 (58) | Not reported | Excluded | 9 (43) | Excluded |
| Study baseline | Pre‐CAR‐T | Pre‐CAR‐T | Pre‐CAR‐T | Pre‐CAR‐T | 12 months from CAR‐T | Median 20 months from CAR‐T |
| VZV | – | 31/38 (82) | – | – | 18 (87) | 23/26 (90) |
| Hepatitis A | – | 16/34 (47) | – | – | – | 12/28 (41) |
| Hepatitis B | – | 8/35 (23) | – | – | 11 (52) | 11/28 (40) |
| Measles | – | 32/38 (84) | 6/8 (75) | 22/40 (55) | 16 (77) | 24/30 (80) |
| Mumps | – | 10/12 (83) | 5/8 (63) | – | 18 (86) | 15/30 (50) |
| Rubella | – | 33/38 (87) | 3/8 (38) | – | 17 (81) | 27/30 (90) |
| Pneumococcal | 8/37 (22) | – | – | – | 0 (0) | 0/25 |
| Tetanus | 37/37 (100) | 36/37 (97) | 8/8 (100) | – | 20 (95) | 25/28 (90) |
| Diphtheria | 35/37 (95) | – | 7/8 (88) | – | – | 25/28 (90) |
| Pertussis | – | – | 0/8 (0) | – | 11 (50) | 0/14 |
| Study endpoint | 6 months post‐CAR‐T | 3 months post‐CAR‐T | N/A | 12 months post‐CAR‐T | N/A | N/A |
| VZV | – | 26/27 (96) | – | – | – | – |
| Hepatitis A | – | 22/31 (71) | – | – | – | – |
| Hepatitis B | – | 22/31 (71) | – | – | – | – |
| Measles | – | 22/27 (81) | 6/8 (75) | 21/40 (53) | – | – |
| Mumps | – | 26/27 (96) | 3/8 (63) | – | – | – |
| Rubella | – | 26/27 (96 | 5/8 (38) | – | – | – |
| Pneumococcal | 2/3 (67) | 5/35 (14) | – | – | – | – |
| Tetanus | 13/13 (100) | 27/27 (100) | 8/8 (100) | – | – | – |
| Diphtheria | 11/13 (85) | – | 7/8 (88) | – | – | – |
| Pertussis | – | – | 0/8 (0) | – | – | – |
Abbreviations: BCMA, B‐cell maturation antigen; CAR‐T, chimeric antigen receptor T cell; CD19, cluster of differentiation 19; DLBCL, diffuse large B‐cell lymphoma; HCT, hematopoietic cell transplant; IVIg, intravenous immunoglobulin; VZV, varicella zoster virus.
3.1.1. The effects of CAR‐T target
Significant discussion surrounds how CAR‐T patients retain antibodies after B‐cell aplasia. One theory is that although CD19 directed CAR‐T cells deplete memory‐B and CD19+ plasma cells, they spare a CD19– plasma cell population, which replenish antibody production against previously encountered pathogens. 118 BCMA CAR‐T, used in the treatment of multiple myeloma, depletes all BCMA‐expressing plasma cells and could therefore be associated with lower antibody positivity after treatment compared to the CD19+ product. 103 At present, seroprevalence studies in BCMA treated patients are very limited, but a small study demonstrates (BCMA = 4) a lower rate of aggregated seropositivity (48%) compared to CD19+ treated patients (67%). 115
3.1.2. Streptococcus pneumoniae
Fewer than 14% of patients, not receiving IVIg replacement after CAR‐T, demonstrated antibodies against tested serovars of S. pneumoniae at 3–20 months post‐infusion. 114 , 115 These estimates reflect predominantly patients with lymphoma receiving CD19+ depletion. There is a lack of baseline data on S. pneumoniae seroprevalence prior to CAR‐T infusion. 110 Similarly, reference data for healthy population seroprevalence for S. pneumoniae were not available. 115 Small subgroups (N = 13) with S. pneumoniae IgG detected prior to CAR‐T infusion have demonstrated reduction in mean titers of IgG 3–6 months post‐infusion, although a proportion remained seroprotection throughout. 109 , 110
3.1.3. Diphtheria, tetanus, and pertussis
Studies demonstrate a high rate of circulating IgG specific to tetanus (100% of patients) prior to CAR‐T infusion that was maintained, or comparable to healthy controls, at 3–20 months post‐infusion in 90%–100% of sampled patients. 108 , 110 , 111 , 116 , 119 , 120 Similarly, diphtheria antibodies were detected in 88%–95% of patients pre‐infusion, with similar seroprevalence maintained at post‐infusion follow‐up (median 3–20 months). 110 , 112 Pertussis data were sparse, with low seroprevalence rates identified at pre‐infusion in small samples, and equally low rates of detection at 12‐ and 20‐month follow‐up. 112 , 114 , 115
3.1.4. Measles, mumps, and rubella
Moderate seropositivity to measles (55%–84%), mumps (63%–83%), and rubella (38%–87%) was appreciated in CAR‐T patients prior to cellular therapy. 111 , 112 , 113 If enduring response was achieved, patients maintained expression of MMR IgG. 111 , 112 , 114 , 115
3.1.5. Varicella zoster virus
Within the limitations of a single study with pre‐infusion results, a high proportion of CAR‐T treated patients had demonstrable antibodies against VZV (82%). 111 Post‐infusion serosurveys have demonstrated similar seroprevalence (87%–96%). 114 , 115 Seropositive patients are currently prophylaxed against VZV reactivation for between 6 and 12 months depending on center. 121 , 122 , 123
3.2. Vaccine response
Most research examining vaccine response following CAR‐T therapies have focused on response to SARS‐CoV‐2 vaccines and are synthesized in existing systematic reviews. 81 , 84 , 124 , 125 Prospective observational studies have demonstrated that one or two vaccines are insufficient to elicit a robust humoral response in patients receiving cellular therapies, although the T‐cell response remains comparable to healthy controls. 108 , 126 , 127 , 128 Higher rates of antibody seroconversion are observed with subsequent booster doses (3–5 vaccines), and this is currently recommended HM patients, including those on cellular therapies. 36 , 129 , 130 , 131 Furthermore, mRNA vaccines elicited improved vaccine responses in this population compared to non‐mRNA vaccines. 125 Predictors of vaccine response were heterogeneously modeled between studies. Steroid use and underlying non‐Hodgkin lymphoma predicted poor vaccine response. 84 , 126 , 132 Higher numbers of circulating B cells were predictive of improved vaccine response in two studies. 129 , 133 Across studies, absolute lymphocyte count, Ig replacement, time since CAR‐T, and age of the patient were not predictive. 84 , 132 , 134
Most vaccine studies have examined CD19+ directed CAR‐T therapies. Mechanistically, it is plausible that CD19+ and BCMA CAR‐T might differ in vaccine response. 135 BCMA COVID‐19 vaccine data are again scarce and driven predominantly by a single study (N = 19) in which 79% of patients demonstrated seroconversion to SARS‐CoV‐2 after two doses. 136 , 137 The prior treatment history, time between CAR‐T therapy and vaccination, presence or absence of IVIg replacement, and levels of circulating B lymphocytes in this cohort are not known.
To date, only two studies have examined vaccine responses outside of COVID‐19 in CAR‐T treated patients. Lee et al. 109 retrospectively examined paired pre‐ and post‐vaccine IgG titers in response to PCV13 vaccination in a cohort of CAR‐T treated lymphoma patients. Patients vaccinated at either day 90 (N = 13) or day 180 (N = 8) post‐CAR‐T demonstrated a reduction in titers between pre‐vaccination baseline and 90 days post‐vaccine. 109 Of the eight patients in enduring remission at day 540 who demonstrated seroprotection against pneumococcus, three had confirmed baseline immunity prior to CAR‐T infusion, a further three patients were vaccinated, one patient received IVIg, and one patient received neither IVIg nor vaccination but had an unknown baseline antibody response. 109
Additionally, Walti et al. 117 prospectively examined response to the quadrivalent influenza vaccine in a mixed lymphoma/myeloma population treated with CD19+ and BCMA directed CAR‐T. Partial response to inactivated influenza vaccine was appreciated in 60%–70% of the cohort, defined as a twofold increase in antibody response to a vaccine strain, while 31%–40% of the cohort had robust antibody response (fourfold increase). 117 There was no association between vaccine response and age, time from CAR‐T, IgG level, or underlying malignancy. 117
3.3. Vaccination guidelines
Vaccine studies in patients undergoing treatment with cellular therapies remain limited. Thus, vaccination schedules are derived largely from expert opinion and mirror the advice surrounding autoHCT.
3.3.1. Vaccinations prior to CAR‐T
As demonstrated by the seroprevalence surveys, most patients who demonstrated humoral antibody response to vaccine‐specific pathogens prior to CAR‐T, maintained seropositivity at follow‐up. 110 , 111 , 116 Optimizing timely revaccination following autoHCT or HCT might potentially improve seroprotection in the event of relapse and subsequent need for CAR‐T therapies.
Considering the epidemic nature of both influenza and SARS‐CoV‐2, the EBMT/JACIE/EHA and ASH‐ASTCT consensus guidelines advocate for vaccination against SARS‐CoV‐2 and influenza at least 2 weeks prior to lymphodepletion, citing the likely lack of vaccine response after CAR‐T infusion due to B‐cell aplasia. 75 , 138 Expert commentary has extended this recommendation to include pre‐CAR‐T vaccination against S. pneumoniae and hepatitis B in high endemicity areas and consideration of vaccination of household contacts. 100
3.3.2. Vaccinations following CAR‐T
Vaccine selection and dosing intervals for CAR‐T patients mimic guidelines for HCT summarized in Table 1. Revaccination post‐CAR‐T is derived from expert consensus, center and physician opinion, with general recommendations summarized in Table 3 and an example vaccination schedule in Table 4. 99
TABLE 3.
Recommendations on revaccination timing post cellular therapy from expert international guidelines, expert center protocols, and expert opinion.
| Consensus guidelines (EBMT/JACIE/EHA, ASH‐ASTCT) | Expert center protocols | Expert opinions | |
|---|---|---|---|
|
Killed and inactivated vaccines: PCV13 (3 doses) PPSV23 (1 doses) DTaP (3 doses) HBV (3 doses) HAV (2 doses) SARS‐CoV‐2 (3+ doses) IIV (2 doses) VZV (aRZV) (2 doses) ACYW‐135 (2 doses) a Hib (3 doses) a |
≥3 months after CAR‐T therapy AND Demonstrated immune reconstitution* AND No ongoing immunosuppression (see text). |
No IVIg in prior 2 months No anti‐CD19 or anti‐CD20 antibody therapy in prior 6 months Demonstrate vaccine response on one killed vaccine prior to revaccination with remaining schedule |
Demonstrate detectable serum IgA (evidence of class switching) If no vaccine response demonstrated, re‐check immune reconstitution in 6 months and continue IVIg |
|
Live vaccines MMR (2 doses) VZV (LAVV) (2 doses) Many travel vaccines (e.g., typhoid, yellow fever, and polio oral vaccine) |
≥12 months after CAR‐T therapy AND Demonstrated immune reconstitution* AND No ongoing immunosuppression AND No IVIg in prior 8 months |
No IVIg in prior 5 months No anti‐CD19 or anti‐CD20 antibody therapy in prior 6 months No HCT ≤2 years prior No systemic immunosuppression in prior 12 months Demonstrated response to killed/inactive vaccine |
Demonstrate detectable serum IgA (evidence of class switching) |
Abbreviations: ACYW‐135, meningococcal quadrivalent conjugate vaccine; aRZV, adjuvanted recombinant zoster virus vaccine; CAR‐T, chimeric antigen receptor T cell; CD19, cluster of differentiation 19; CD20, cluster of differentiation 20; DTaP, higher dose diphtheria, tetanus, and acellular pertussis vaccine; HAV vaccine, hepatitis A virus; HBV vaccine, hepatitis B virus; HCT, hematopoietic cell transplant; Hib, Haemophilus influenzae type B conjugate vaccine; IgA, immunoglobulin A; IIV, inactivated influenza vaccine; IVIg, intravenous immunoglobulin; LAVV, live‐attenuated varicella vaccine; MMR, measles, mumps, and rubella live virus vaccine; PCV, pneumococcal conjugate vaccine; PPSV23, pneumococcal 23‐valent polysaccharide vaccine; SARS‐CoV‐2, severe acute respiratory syndrome coronavirus 2; VZV, varicella zoster virus.
Revaccination against meningococcal and hemophilus to be considered in patients with CAR‐T patients and additional risk factors, such as splenectomy.
TABLE 4.
Vaccination schedule a for adult patients treated with chimeric antigen receptor T‐cell (CAR‐T) therapy. 99
| Vaccines | Pre‐CAR‐T | ≥6 months | ≥8 months | ≥10 months | ≥12 months | ≥18 months |
|---|---|---|---|---|---|---|
| IIV | Influenza | Influenza | ||||
| PCV | PCV13 | PCV13 | PCV13 | |||
| PPSV23 | PPSV23 | |||||
| DTaP | DTaP | Td | Td | |||
| HAV | HAV | HAV | ||||
| HBV | HBV | HBV | HBV | |||
| Varicella zoster b | aRZV | aRZV |
Abbreviations: aRZV, adjuvant recombinant zoster vaccine; DTaP, higher dose diphtheria, tetanus, and acellular pertussis vaccine; HAV vaccine, hepatitis A virus; HBV vaccine, hepatitis B virus; IIV, inactivated influenza vaccine; PCV, pneumococcal conjugate vaccine; PPSV23, pneumococcal 23‐valent polysaccharide vaccine; Td, tetanus–diphtheria.
This schedule was published prior to the availability of coronavirus disease 2019 (COVID‐19) vaccines. Revaccination with a primary course of three mRNA COVID‐19 vaccines is now recommended for patients following CAR‐T therapy. 75
Seropositive patients.
Consensus guidelines advise that killed or inactivated vaccines be administered ≥3 months after CAR‐T administration. Patients should demonstrate immune reconstitution prior to vaccination, defined as CD4+ >0.2 × 109/L, CD19 or CD20+ B cells >0.2 × 109/L. 99 , 138 , 139 Patients should not be receiving concomitant immunosuppressive treatment including cytotoxic chemotherapy, systemic corticosteroids, T‐cell‐depleting or anti‐lymphocyte agents, or IVIg within the previous 2 months. 99 , 138 , 139 Certain immunotherapies may not be considered additionally immunosuppressive in the context of inactivated vaccines, such as checkpoint inhibitors, or immunomodulatory agents. 139 In patients with multi‐modal immunomodulatory therapy, expert infectious disease consultation is advised. 11 , 99 , 140 The exception is the influenza vaccine, which should be given annually prior to the expected influenza season, and ideally 2 weeks prior to lymphodepleting chemotherapy. 93
Live vaccines should be different until at least 1 year following CAR‐T and require demonstration of immune reconstitution. Several expert groups suggest that live vaccines are contraindicated within 8 months of receiving IVIg replacement. 138 Expert centers, for example, the Fred Hutchinson Cancer Center, recommend delaying live and non‐live adjuvant vaccines until ≥5 months from last IVIg replacement. 139 Further expert commentary has suggested that before live and non‐live adjuvant vaccines, vaccine responses to killed/attenuated vaccines should be demonstrated. 99 , 139
3.3.3. Future directions
For HCT recipients, owing to differences in conditioning regimen, stem cell source, and underlying disease, there is an opportunity to refine and personalize revaccination schedules for autologous HCT recipients rather than extrapolating from allogeneic HCT recipients. Ongoing assessment by clinical studies is important for newer vaccine formulations, including PCV20, aRZV, and the bivalent COVID‐19 vaccines. Alternate vaccination strategies to improve immunogenicity, such as examining new dosing schedules of vaccination, are required. Candidate RSV vaccines 22 are in development, going forward, it will be important to advocate for the inclusion of HCT recipients in clinical trials to understand their safety and efficacy.
Significantly more research is required to optimize the vaccine schedule for cellular therapy (CAR‐T) treated patients. Longitudinal, prospective observational studies are required to properly assess retention of antibody‐specific IgG from baseline, through treatment, and following immune reconstitution to determine which vaccines, if any, are most required. Vaccine response in BCMA CAR‐T treated patients also warrants investigation. Clinical trials are required to determine the best way to time vaccine initiation post‐CAR‐T, directly comparing standard timepoints to timepoints driven by markers of immune reconstitution, or following demonstrable vaccine response. Methods to heighten immunogenicity, including booster regimens, should also be explored.
4. CONCLUSION
In summary, there are well‐recognized vaccine schedules for the HCT population, with new vaccine formulations including PCV20, aRZV, and bivalent booster COVID‐19 vaccines that require ongoing assessment. Revaccination post‐cellular therapies at present mostly follow the HCT schedule, but further research is required to optimize the timing of vaccine delivery and clarify which vaccines would be of most benefit to the cellular therapy patients.
CONFLICT OF INTEREST STATEMENT
Victoria G. Hall and Gemma Reynolds have no conflicts of interest. Benjamin W. Teh has been on the advisory board for Moderna, CSL‐Behring, and Takeda. He has also received research funding from Merck Sharp and Dohme, Sanofi, and Seqirus.
ACKNOWLEDGMENTS
Victoria G. Hall is supported by NHMRC post‐graduate PhD scholarship (#2014210). Gemma Reynolds is supported by NHMRC post‐graduate PhD scholarship (#2013970). Benjamin W. Teh is supported by MRFF investigator (Emerging leader Level 2) fellowship (#1195894).
Open access publishing facilitated by The University of Melbourne, as part of the Wiley ‐ The University of Melbourne agreement via the Council of Australian University Librarians.
Reynolds G, Hall VG, Teh BW. Vaccine schedule recommendations and updates for patients with hematologic malignancy post‐hematopoietic cell transplant or CAR T‐cell therapy. Transpl Infect Dis. 2023;25(Suppl. 1):e14109. 10.1111/tid.14109
Gemma Reynolds and Victoria G. Hall have equal contribution as first authors.
DATA AVAILABILITY STATEMENT
This is a review article with no new original data provided.
REFERENCES
- 1. Niederwieser D, Baldomero H, Atsuta Y, et al. One and half million hematopoietic stem cell transplants (HSCT). Dissemination, trends and potential to improve activity by telemedicine from the worldwide network for blood and marrow transplantation (WBMT). Blood. 2019;134(suppl_1):2035. doi: 10.1182/blood-2019-125232 [DOI] [Google Scholar]
- 2. Aljurf M, Weisdorf D, Alfraih F, et al. Worldwide network for blood & marrow transplantation (WBMT) special article, challenges facing emerging alternate donor registries. Bone Marrow Transplant. 2019;54(8):1179‐1188. doi: 10.1038/s41409-019-0476-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mackall C. How CAR‐T cells became the hot rods of cancer therapy. Nature. 2023;613. Accessed April 6th, 2023. https://www.nature.com/articles/d41586-023-00177-z [Google Scholar]
- 4. Baird JH, Epstein DJ, Tamaresis JS, et al. Immune reconstitution and infectious complications following axicabtagene ciloleucel therapy for large B‐cell lymphoma. Blood Adv. 2021;5(1):143‐155. doi: 10.1182/bloodadvances.2020002732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bastidas A, de la Serna J, El Idrissi M, et al. Effect of recombinant zoster vaccine on incidence of herpes zoster after autologous stem cell transplantation: a randomized clinical trial. JAMA. 2019;322(2):123‐133. doi: 10.1001/jama.2019.9053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bhalla P, Forrest GN, Gershon M, et al. Disseminated, persistent, and fatal infection due to the vaccine strain of varicella‐zoster virus in an adult following stem cell transplantation. Clin Infect Dis. 2014;60(7):1068‐1074. doi: 10.1093/cid/ciu970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Boeckh M, Kim HW, Flowers ME, Meyers JD, Bowden RA. Long‐term acyclovir for prevention of varicella zoster virus disease after allogeneic hematopoietic cell transplantation–a randomized double‐blind placebo‐controlled study. Blood. 2006;107(5):1800‐1805. doi: 10.1182/blood-2005-09-3624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Xue E, Xie H, Leisenring WM, et al. High incidence of herpes zoster after cord blood hematopoietic cell transplant despite longer duration of antiviral prophylaxis. Clin Infect Dis. 2020;72(8):1350‐1357. doi: 10.1093/cid/ciaa222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Debbache K, Varon E, Hicheri Y, et al. The epidemiology of invasive Streptococcus pneumoniae infections in onco‐haematology and haematopoietic stem cell transplant patients in France. Are the serotypes covered by the available anti‐pneumococcal vaccines? Clin Microbiol Infect. 2009;15(9):865‐868. doi: 10.1111/j.1469-0691.2009.02810.x [DOI] [PubMed] [Google Scholar]
- 10. Youssef S, Rodriguez G, Rolston KV, Champlin RE, Raad II, Safdar A. Streptococcus pneumoniae infections in 47 hematopoietic stem cell transplantation recipients: clinical characteristics of infections and vaccine‐breakthrough infections, 1989–2005. Medicine (Baltimore). 2007;86(2):69‐77. doi: 10.1097/md.0b013e31803eb176 [DOI] [PubMed] [Google Scholar]
- 11. Stewart AG, Henden AS. Infectious complications of CAR T‐cell therapy: a clinical update. Ther Adv Infect Dis. 2021;8:20499361211036773‐20499361211036773. doi: 10.1177/20499361211036773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Čerňan M, Szotkowski T, Minařík J, et al. Breakthrough COVID‐19 in vaccinated patients with haematologic malignancies—the first single‐centre experience from the Czech Republic. Life (Basel). 2022;12(8):1184. doi: 10.3390/life12081184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pagano L, Salmanton‐García J, Marchesi F, et al. COVID‐19 in vaccinated adult patients with hematological malignancies: preliminary results from EPICOVIDEHA. Blood. 2022;139(10):1588‐1592. doi: 10.1182/blood.2021014124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Spanjaart AM, Ljungman P, de La Camara R, et al. Poor outcome of patients with COVID‐19 after CAR T‐cell therapy for B‐cell malignancies: results of a multicenter study on behalf of the European Society for Blood and Marrow Transplantation (EBMT) Infectious Diseases Working Party and the European Hematology Association (EHA) Lymphoma Group. Leukemia. 2021;35(12):3585‐3588. doi: 10.1038/s41375-021-01466-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Busca A, Salmanton‐García J, Corradini P, et al. COVID‐19 and CAR T cells: a report on current challenges and future directions from the EPICOVIDEHA survey by EHA‐IDWP. Blood Adv. 2022;6(7):2427‐2433. doi: 10.1182/bloodadvances.2021005616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hobson D, Curry RL, Beare AS, Ward‐Gardner A. The role of serum haemagglutination‐inhibiting antibody in protection against challenge infection with influenza A2 and B viruses. J Hyg (Lond). 1972;70(4):767‐777. doi: 10.1017/s0022172400022610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Coudeville L, Bailleux F, Riche B, Megas F, Andre P, Ecochard R. Relationship between haemagglutination‐inhibiting antibody titres and clinical protection against influenza: development and application of a Bayesian random‐effects model. BMC Med Res Methodol. 2010;10:18. doi: 10.1186/1471-2288-10-18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Fox JP, Cooney MK, Hall CE, Foy HM. Influenzavirus infections in Seattle families, 1975–1979. II. Pattern of infection in invaded households and relation of age and prior antibody to occurrence of infection and related illness. Am J Epidemiol. 1982;116(2):228‐242. doi: 10.1093/oxfordjournals.aje.a113408 [DOI] [PubMed] [Google Scholar]
- 19. Ng S, Fang VJ, Ip DK, et al. Estimation of the association between antibody titers and protection against confirmed influenza virus infection in children. J Infect Dis. 2013;208(8):1320‐1324. doi: 10.1093/infdis/jit372 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Trombetta CM, Perini D, Mather S, Temperton N, Montomoli E. Overview of serological techniques for influenza vaccine evaluation: past, present and future. Vaccines (Basel). 2014;2(4):707‐34. doi: 10.3390/vaccines2040707 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gilbert PB, Donis RO, Koup RA, Fong Y, Plotkin SA, Follmann D. A Covid‐19 milestone attained—a correlate of protection for vaccines. N Engl J Med. 2022;387(24):2203‐2206. doi: 10.1056/NEJMp2211314 [DOI] [PubMed] [Google Scholar]
- 22. Papi A, Ison MG, Langley JM, et al. Respiratory syncytial virus prefusion F protein vaccine in older adults. N Engl J Med. 2023;388(7):595‐608. doi: 10.1056/NEJMoa2209604 [DOI] [PubMed] [Google Scholar]
- 23. Schuster JE, Hamdan L, Dulek DE, et al. Influenza vaccine in pediatric recipients of hematopoietic‐cell transplants. N Engl J Med. 2023;388(4):374‐376. doi: 10.1056/NEJMc2210825 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Carpenter PA, Englund JA. How I vaccinate blood and marrow transplant recipients. Blood. 2016;127(23):2824‐2832. doi: 10.1182/blood-2015-12-550475 [DOI] [PubMed] [Google Scholar]
- 25. Giebink GS, Warkentin PI, Ramsay NKC, Kersey JH. Titers of antibody to pneumococci in allogeneic bone marrow transplant recipients before and after vaccination with pneumococcal vaccine. J Infect Dis. 1986;154(4):590‐596. doi: 10.1093/infdis/154.4.590 [DOI] [PubMed] [Google Scholar]
- 26. Sheridan JF, Tutschka PJ, Sedmak DD, Copelan EA. Immunoglobulin G subclass deficiency and pneumococcal infection after allogeneic bone marrow transplantation. Blood. 1990;75(7):1583‐1586. doi: 10.1182/blood.V75.7.1583.1583 [DOI] [PubMed] [Google Scholar]
- 27. Pao M, Papadopoulos EB, Chou J, et al. Response to pneumococcal (PNCRM7) and Haemophilus influenzae conjugate vaccines (HIB) in pediatric and adult recipients of an allogeneic hematopoietic cell transplantation (alloHCT). Biol Blood Marrow Transplant. 2008;14(9):1022‐1030. doi: 10.1016/j.bbmt.2008.06.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Meerveld‐Eggink A, van der Velden AMT, Ossenkoppele GJ, van de Loosdrecht AA, Biesma DH, Rijkers GT. Antibody response to polysaccharide conjugate vaccines after nonmyeloablative allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15(12):1523‐1530. doi: 10.1016/j.bbmt.2009.07.020 [DOI] [PubMed] [Google Scholar]
- 29. Hilgendorf I, Freund M, Jilg W, et al. Vaccination of allogeneic haematopoietic stem cell transplant recipients: report from the international consensus conference on clinical practice in chronic GVHD. Vaccine. 2011;29(16):2825‐2833. doi: 10.1016/j.vaccine.2011.02.018 [DOI] [PubMed] [Google Scholar]
- 30. Cordonnier C, Labopin M, Jansen KU, et al. Relationship between IgG titers and opsonocytophagocytic activity of anti‐pneumococcal antibodies after immunization with the 7‐valent conjugate vaccine in allogeneic stem cell transplant. Bone Marrow Transplant. 2010;45(9):1423‐1426. doi: 10.1038/bmt.2009.364 [DOI] [PubMed] [Google Scholar]
- 31. Ljungman P, Cordonnier C, Einsele H, et al. Vaccination of hematopoietic cell transplant recipients. Bone Marrow Transplant. 2009;44(8):521‐526. doi: 10.1038/bmt.2009.263 [DOI] [PubMed] [Google Scholar]
- 32. Cordonnier C, Einarsdottir S, Cesaro S, et al. Vaccination of haemopoietic stem cell transplant recipients: guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019;19(6):e200‐e212. doi: 10.1016/S1473-3099(18)30600-5 [DOI] [PubMed] [Google Scholar]
- 33. Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2013;58(3):e44‐e100. doi: 10.1093/cid/cit684 [DOI] [PubMed] [Google Scholar]
- 34. Ljungman P, Engelhard D, de La Cámara R, et al. Vaccination of stem cell transplant recipients: recommendations of the Infectious Diseases Working Party of the EBMT. Bone Marrow Transplant. 2005;35(8):737‐746. doi: 10.1038/sj.bmt.1704870 [DOI] [PubMed] [Google Scholar]
- 35. Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009;15(10):1143‐1238. doi: 10.1016/j.bbmt.2009.06.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Miller PDE, Patel SR, Skinner R, et al. Joint consensus statement on the vaccination of adult and paediatric haematopoietic stem cell transplant recipients: prepared on behalf of the British society of blood and marrow transplantation and cellular therapy (BSBMTCT), the Children's Cancer and Leukaemia Group (CCLG), and British Infection Association (BIA). J Infect. 2023;86(1):1‐8. doi: 10.1016/j.jinf.2022.11.005 [DOI] [PubMed] [Google Scholar]
- 37. Ljungman P. Vaccination of immunocompromised patients. Clin Microbiol Infect. 2012;18:93‐99. doi: 10.1111/j.1469-0691.2012.03971.x [DOI] [PubMed] [Google Scholar]
- 38. Kamboj M, Sepkowitz KA. Risk of transmission associated with live attenuated vaccines given to healthy persons caring for or residing with an immunocompromised patient. Infect Control Hosp Epidemiol. 2007;28(6):702‐707. doi: 10.1086/517952 [DOI] [PubMed] [Google Scholar]
- 39. Meisel R, Kuypers L, Dirksen U, et al. Pneumococcal conjugate vaccine provides early protective antibody responses in children after related and unrelated allogeneic hematopoietic stem cell transplantation. Blood. 2007;109(6):2322‐2326. doi: 10.1182/blood-2006-06-032284 [DOI] [PubMed] [Google Scholar]
- 40. Cordonnier C, Labopin M, Chesnel V, et al. Randomized study of early versus late immunization with pneumococcal conjugate vaccine after allogeneic stem cell transplantation. Clin Infect Dis. 2009;48(10):1392‐1401. doi: 10.1086/598324 [DOI] [PubMed] [Google Scholar]
- 41. Olarte L, Lin PL, Barson WJ, et al. Invasive pneumococcal infections in children following transplantation in the pneumococcal conjugate vaccine era. Transplant Infect Disease. 2017;19(1):e12630. doi: 10.1111/tid.12630 [DOI] [PubMed] [Google Scholar]
- 42. Parkkali T, Käyhty H, Ruutu T, Volin L, Eskola J, Ruutu P. A comparison of early and late vaccination with Haemophilus influenzae type b conjugate and pneumococcal polysaccharide vaccines after allogeneic BMT. Bone Marrow Transplant. 1996;18(5):961‐967. [PubMed] [Google Scholar]
- 43. Cordonnier C, Labopin M, Chesnel V, et al. Immune response to the 23‐valent polysaccharide pneumococcal vaccine after the 7‐valent conjugate vaccine in allogeneic stem cell transplant recipients: results from the EBMT IDWP01 trial. Vaccine. 2010;28(15):2730‐2734. doi: 10.1016/j.vaccine.2010.01.025 [DOI] [PubMed] [Google Scholar]
- 44. Roberts MB, Bak N, Wee LYA, et al. Clinical effectiveness of conjugate pneumococcal vaccination in hematopoietic stem cell transplantation recipients. Biol Blood Marrow Transplant. 2020;26(2):421‐427. doi: 10.1016/j.bbmt.2019.10.006 [DOI] [PubMed] [Google Scholar]
- 45. Cordonnier C, Ljungman P, Juergens C, et al. Immunogenicity, safety, and tolerability of 13‐valent pneumococcal conjugate vaccine followed by 23‐valent pneumococcal polysaccharide vaccine in recipients of allogeneic hematopoietic stem cell transplant aged ≥2 years: an open‐label study. Clin Infect Dis. 2015;61(3):313‐323. doi: 10.1093/cid/civ287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Garcia Garrido HM, Haggenburg S, Schoordijk MCE, et al. Immunogenicity of a 5‐dose pneumococcal vaccination schedule following allogeneic hematopoietic stem cell transplantation. Am J Hematol. 2022;97(5):592‐602. doi: 10.1002/ajh.26493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Styczynski J, Reusser P, Einsele H, et al. Management of HSV, VZV and EBV infections in patients with hematological malignancies and after SCT: guidelines from the Second European Conference on Infections in Leukemia. Bone Marrow Transplant. 2009;43(10):757‐770. doi: 10.1038/bmt.2008.386 [DOI] [PubMed] [Google Scholar]
- 48. Ljungman P, Wang FZ, Nilsson C, Solheim V, Linde A. Vaccination of autologous stem cell transplant recipients with live varicella vaccine: a pilot study. Support Care Cancer. 2003;11(11):739‐741. doi: 10.1007/s00520-003-0527-8 [DOI] [PubMed] [Google Scholar]
- 49. Sasadeusz J, Prince HM, Schwarer A, et al. Immunogenicity and safety of a two‐dose live attenuated varicella vaccine given to adults following autologous hematopoietic stem cell transplantation. Transplant Infect Disease. 2014;16(6):1024‐1031. doi: 10.1111/tid.12295 [DOI] [PubMed] [Google Scholar]
- 50. Kussmaul SC, Horn BN, Dvorak CC, Abramovitz L, Cowan MJ, Weintrub PS. Safety of the live, attenuated varicella vaccine in pediatric recipients of hematopoietic SCTs. Bone Marrow Transplant. 2010;45(11):1602‐1606. doi: 10.1038/bmt.2010.31 [DOI] [PubMed] [Google Scholar]
- 51. Schrauder A, Henke‐Gendo C, Seidemann K, et al. Varicella vaccination in a child with acute lymphoblastic leukaemia. Lancet North Am Ed. 2007;369(9568):1232. doi: 10.1016/S0140-6736(07)60567-4 [DOI] [PubMed] [Google Scholar]
- 52. Ullmann AJ, Schmidt‐Hieber M, Bertz H, et al. Infectious diseases in allogeneic haematopoietic stem cell transplantation: prevention and prophylaxis strategy guidelines 2016. Ann Hematol. 2016;95(9):1435‐1455. doi: 10.1007/s00277-016-2711-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Costa E, Buxton J, Brown J, Templeton KE, Breuer J, Johannessen I. Fatal disseminated varicella zoster infection following zoster vaccination in an immunocompromised patient. BMJ Case Rep. 2016;2016:bcr2015212688. doi: 10.1136/bcr-2015-212688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Dubey V, MacFadden D. Disseminated varicella zoster virus infection after vaccination with a live attenuated vaccine. CMAJ. 2019;191(37):E1025‐E1027. doi: 10.1503/cmaj.190270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Chun JY, Kim K, Lee MK, et al. Immunogenicity and safety of a live herpes zoster vaccine in hematopoietic stem cell transplant recipients. BMC Infect Dis. 2021;21(1):117. doi: 10.1186/s12879-021-05806-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Naidus E, Damon L, Schwartz BS, Breed C, Liu C. Experience with use of Zostavax® in patients with hematologic malignancy and hematopoietic cell transplant recipients. Am J Hematol. 2012;87(1):123‐125. doi: 10.1002/ajh.22196 [DOI] [PubMed] [Google Scholar]
- 57. Pandit A, Leblebjian H, Hammond SP, et al. Safety of live‐attenuated measles–mumps–rubella and herpes zoster vaccination in multiple myeloma patients on maintenance lenalidomide or bortezomib after autologous hematopoietic cell transplantation. Bone Marrow Transplant. 2018;53(7):942‐945. doi: 10.1038/s41409-018-0112-x [DOI] [PubMed] [Google Scholar]
- 58. Issa NC, Marty FM, Leblebjian H, et al. Live attenuated varicella‐zoster vaccine in hematopoietic stem cell transplantation recipients. Biol Blood Marrow Transplant. 2014;20(2):285‐287. doi: 10.1016/j.bbmt.2013.11.013 [DOI] [PubMed] [Google Scholar]
- 59. Aoki T, Koh K, Kawano Y, et al. Safety of live attenuated high‐titer varicella‐zoster virus vaccine in pediatric allogeneic hematopoietic stem cell transplantation recipients. Biol Blood Marrow Transplant. 2016;22(4):771‐775. doi: 10.1016/j.bbmt.2015.12.025 [DOI] [PubMed] [Google Scholar]
- 60. Winston DJ, Mullane KM, Cornely OA, et al. Inactivated varicella zoster vaccine in autologous haemopoietic stem‐cell transplant recipients: an international, multicentre, randomised, double‐blind, placebo‐controlled trial. Lancet. 2018;391(10135):2116‐2127. doi:10.1016/s0140‐6736(18)30631‐7 [DOI] [PubMed] [Google Scholar]
- 61. Anderson TC, Masters NB, Guo A, et al. Use of recombinant zoster vaccine in immunocompromised adults aged ≥19 years: recommendations of the Advisory Committee on Immunization Practices, United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(3):80‐84. doi: 10.15585/mmwr.mm7103a2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Dooling KL, Guo A, Patel M, et al. Recommendations of the advisory committee on immunization practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep. 2018;67(3):103‐108. doi: 10.15585/mmwr.mm6703a5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Camargo JF, Lin RY, Natori Y, et al. Reduced immunogenicity of the adjuvanted recombinant zoster vaccine after hematopoietic cell transplant: a pilot study. Blood Advances. 2020;4(19):4618‐4622. doi: 10.1182/bloodadvances.2020002269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Baumrin E, Izaguirre NE, Bausk B, et al. Safety and reactogenicity of the recombinant zoster vaccine after allogeneic hematopoietic cell transplantation. Blood Advances. 2021;5(6):1585‐1593. doi: 10.1182/bloodadvances.2020003749 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Koldehoff M, Horn PA, Lindemann M. Cellular immune response after vaccination with an adjuvanted, recombinant zoster vaccine in allogeneic hematopoietic stem cell transplant recipients. Vaccines (Basel). 2022;10(5):809. doi: 10.3390/vaccines10050809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Einarsdottir S, Martner A, Waldenström J, et al. Deficiency of SARS‐CoV‐2 T‐cell responses after vaccination in long‐term allo‐HSCT survivors translates into abated humoral immunity. Blood Adv. 2022;6(9):2723‐2730. doi: 10.1182/bloodadvances.2021006937 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Teh JSK, Coussement J, Neoh ZCF, et al. Immunogenicity of COVID‐19 vaccines in patients with hematologic malignancies: a systematic review and meta‐analysis. Blood Adv. 2022;6(7):2014‐2034. doi: 10.1182/bloodadvances.2021006333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Shem‐Tov N, Yerushalmi R, Danylesko I, et al. Immunogenicity and safety of the BNT162b2 mRNA COVID‐19 vaccine in haematopoietic stem cell transplantation recipients. Br J Haematol. 2022;196(4):884‐891. doi: 10.1111/bjh.17918 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Chevallier P, Coste‐Burel M, Le Bourgeois A, et al. Safety and immunogenicity of a first dose of SARS‐CoV‐2 mRNA vaccine in allogeneic hematopoietic stem‐cells recipients. EJHaem. 2021;2(3):520‐524. doi: 10.1002/jha2.242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Greenberger LM, Saltzman LA, Senefeld JW, Johnson PW, DeGennaro LJ, Nichols GL. Antibody response to SARS‐CoV‐2 vaccines in patients with hematologic malignancies. Cancer Cell. 2021;39(8):1031‐1033. doi: 10.1016/j.ccell.2021.07.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Thakkar A, Gonzalez‐Lugo JD, Goradia N, et al. Seroconversion rates following COVID‐19 vaccination among patients with cancer. Cancer Cell. 2021;39(8):1081‐1090.e2. doi: 10.1016/j.ccell.2021.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Bange EM, Han NA, Wileyto P, et al. CD8+ T cells contribute to survival in patients with COVID‐19 and hematologic cancer. Nat Med. 2021;27(7):1280‐1289. doi: 10.1038/s41591-021-01386-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Kimura M, Ferreira VH, Kothari S, et al. Safety and immunogenicity after a three‐dose SARS‐CoV‐2 vaccine schedule in allogeneic stem cell transplant recipients. Transplant Cell Ther. 2022;28(10):706.e1‐706.e10. doi: 10.1016/j.jtct.2022.07.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Nguyen THO, Rowntree LC, Allen LF, et al. Robust SARS‐CoV‐2 T cell responses with common TCR motifs towards COVID‐19 vaccines in haematological malignancy patients impacting B cell immunity. Cell Rep Med. 2023;4(4):101017. doi: 10.1016/j.xcrm.2023.101017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. American Society of Hematology . ASH‐ASTCT COVID‐19 Vaccination for HCT and CAR T Cell Recipients: Frequently Asked Questions . 2022. Accessed April 2023. https://www.hematology.org/covid‐19/ash‐astct‐covid‐19‐vaccination‐for‐hct‐and‐car‐t‐cell‐recipients
- 76. Fendler A, Shepherd STC, Au L, et al. Immune responses following third COVID‐19 vaccination are reduced in patients with hematological malignancies compared to patients with solid cancer. Cancer Cell. 2022;40(2):114‐116. doi: 10.1016/j.ccell.2021.12.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Haggenburg S, Hofsink Q, Lissenberg‐Witte BI, et al. Antibody response in immunocompromised patients with hematologic cancers who received a 3‐dose mRNA‐1273 vaccination schedule for COVID‐19. JAMA Oncol. 2022;8(10):1477‐1483. doi: 10.1001/jamaoncol.2022.3227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Bellusci L, Grubbs G, Srivastava P, et al. Neutralization of SARS‐CoV‐2 Omicron after vaccination of patients with myelodysplastic syndromes or acute myeloid leukemia. Blood. 2022;139(18):2842‐2846. doi: 10.1182/blood.2022016087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Center for Disease Control and Prevention . Use of COVID‐19 Vaccines in the United States. Accessed April 2023. https://www.cdc.gov/vaccines/covid‐19/clinical‐considerations/covid‐19‐vaccines‐us.html
- 80. Naranbhai V, Pernat CA, Gavralidis A, et al. Immunogenicity and reactogenicity of SARS‐CoV‐2 vaccines in patients with cancer: the CANVAX cohort study. J Clin Oncol. 2022;40(1):12‐23. doi: 10.1200/jco.21.01891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Ge C, Du K, Luo M, et al. Serologic response and safety of COVID‐19 vaccination in HSCT or CAR T‐cell recipients: a systematic review and meta‐analysis. Exp Hematol Oncol. 2022;11(1):46. doi: 10.1186/s40164-022-00299-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Wu X, Wang L, Shen L, He L, Tang K. Immune response to vaccination against SARS‐CoV‐2 in hematopoietic stem cell transplantation and CAR T‐cell therapy recipients. J Hematol Oncol. 2022;15(1):81. doi: 10.1186/s13045-022-01300-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Debie Y, Vandamme T, Goossens ME, van Dam PA, Peeters M. Antibody titres before and after a third dose of the SARS‐CoV‐2 BNT162b2 vaccine in patients with cancer. Eur J Cancer. 2022;163:177‐179. doi: 10.1016/j.ejca.2021.12.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Abid MB, Rubin M, Ledeboer N, et al. Efficacy of a third SARS‐CoV‐2 mRNA vaccine dose among hematopoietic cell transplantation, CAR T cell, and BiTE recipients. Cancer Cell. 2022;40(4):340‐342. doi: 10.1016/j.ccell.2022.02.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Hill JA, Martens MJ, Young JH, et al. SARS‐CoV‐2 vaccination in the first year after allogeneic hematopoietic cell transplant: a prospective, multicentre, observational study. EClinicalMedicine. 2023;59:101983. doi: 10.1016/j.eclinm.2023.101983 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Re D, Seitz‐Polski B, Brglez V, et al. Humoral and cellular responses after a third dose of SARS‐CoV‐2 BNT162b2 vaccine in patients with lymphoid malignancies. Nat Commun. 2022;13(1):864. doi: 10.1038/s41467-022-28578-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Salmanton‐García J, Marchesi F, Glenthøj A, et al. Improved clinical outcome of COVID‐19 in hematologic malignancy patients receiving a fourth dose of anti‐SARS‐CoV‐2 vaccine: an EPICOVIDEHA report. Hemasphere. 2022;6(11):e789. doi: 10.1097/hs9.0000000000000789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Fendler A, de Vries EGE, GeurtsvanKessel CH, et al. COVID‐19 vaccines in patients with cancer: immunogenicity, efficacy and safety. Nat Rev Clin Oncol. 2022;19(6):385‐401. doi: 10.1038/s41571-022-00610-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Hall VG, Ferreira VH, Wood H, et al. Delayed‐interval BNT162b2 mRNA COVID‐19 vaccination enhances humoral immunity and induces robust T cell responses. Nat Immunol. 2022;23(3):380‐385. doi: 10.1038/s41590-021-01126-6 [DOI] [PubMed] [Google Scholar]
- 90. Voysey M, Costa Clemens SA, Madhi SA, et al. Single‐dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV‐19 (AZD1222) vaccine: a pooled analysis of four randomised trials. Lancet. 2021;397(10277):881‐891. doi: 10.1016/s0140-6736(21)00432-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Wang Q, Bowen A, Valdez R, et al. Antibody response to Omicron BA.4–BA.5 bivalent booster. N Engl J Med. 2023;388(6):567‐569. doi: 10.1056/NEJMc2213907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Chalkias S, Harper C, Vrbicky K, et al. A bivalent Omicron‐containing booster vaccine against Covid‐19. N Engl J Med. 2022;387(14):1279‐1291. doi: 10.1056/NEJMoa2208343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Altarawneh HN, Chemaitelly H, Ayoub HH, et al. Protective effect of previous SARS‐CoV‐2 infection against Omicron BA.4 and BA.5 subvariants. N Engl J Med. 2022;387:1620‐1622. doi: 10.1056/NEJMc2209306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Lin D‐Y, Xu Y, Gu Y, et al. Effectiveness of bivalent boosters against severe Omicron infection. N Engl J Med. 2023;388(8):764‐766. doi: 10.1056/NEJMc2215471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Chaekal OK, Gomez‐Arteaga A, Chen Z, et al. Predictors of Covid‐19 vaccination response after in‐vivo T‐cell‐depleted stem cell transplantation. Transplant Cell Ther. 2022;28(9):618.e1‐618.e10. doi: 10.1016/j.jtct.2022.06.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Hütter‐Krönke ML, Neagoie A, Blau IW, et al. Risk factors and characteristics influencing humoral response to COVID‐19 vaccination in patients after allogeneic stem cell transplantation. Original research. Front Immunol. 2023;14:1174289. doi: 10.3389/fimmu.2023.1174289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Piñana JL, López‐Corral L, Martino R, et al. SARS‐CoV‐2‐reactive antibody detection after SARS‐CoV‐2 vaccination in hematopoietic stem cell transplant recipients: prospective survey from the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group. Am J Hematol. 2022;97(1):30‐42. doi: 10.1002/ajh.26385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Reimann P, Ulmer H, Mutschlechner B, et al. Efficacy and safety of heterologous booster vaccination with Ad26.COV2.S after BNT162b2 mRNA COVID‐19 vaccine in haemato‐oncological patients with no antibody response. Br J Haematol. 2022;196(3):577‐584. doi: 10.1111/bjh.17982 [DOI] [PubMed] [Google Scholar]
- 99. Hill JA, Seo SK. How I prevent infections in patients receiving CD19‐targeted chimeric antigen receptor T cells for B‐cell malignancies. Blood. 2020;136(8):925‐935. doi: 10.1182/blood.2019004000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Los‐Arcos I, Iacoboni G, Aguilar‐Guisado M, et al. Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T‐cell therapy: a position paper. Infection. 2021;49(2):215‐231. doi: 10.1007/s15010-020-01521-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Cordeiro A, Bezerra ED, Hirayama AV, et al. Late events after treatment with CD19‐targeted chimeric antigen receptor modified T cells. Biol Blood Marrow Transplant. 2020;26(1):26‐33. doi: 10.1016/j.bbmt.2019.08.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Jimenez‐Galan R, Ciudad‐Gutierrez P, Prado‐Mel E. Real world toxicity and management of chimeric antigen receptor T cell therapies targeting CD19 in patients with haematological malignancies. Eur J Hospital Pharm. 2021;28(suppl 1):A70. doi: 10.1136/ejhpharm-2021-eahpconf.143 [DOI] [Google Scholar]
- 103. Wang Y, Li C, Xia J, et al. Humoral immune reconstitution after anti‐BCMA CAR T‐cell therapy in relapsed/refractory multiple myeloma. Blood Adv. 2021;5(23):5290‐5299. doi: 10.1182/bloodadvances.2021004603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Bupha‐Intr O, Haeusler G, Chee L, Thursky K, Slavin M, Teh B. CAR‐T cell therapy and infection: a review. Expert Rev Anti Infect Ther. 2021;19(6):749‐758. doi: 10.1080/14787210.2021.1855143 [DOI] [PubMed] [Google Scholar]
- 105. Cappell KM, Sherry RM, Yang JC, et al. Long‐term follow‐up of anti‐CD19 chimeric antigen receptor T‐cell therapy. J Clin Oncol. 2020;38(32):3805‐3815. doi: 10.1200/JCO.20.01467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Kampouri E, Walti CS, Gauthier J, Hill JA. Managing hypogammaglobulinemia in patients treated with CAR‐T‐cell therapy: key points for clinicians. Expert Rev Hematol. 2022;15(4):305‐320. doi: 10.1080/17474086.2022.2063833 [DOI] [PubMed] [Google Scholar]
- 107. Kochenderfer JN, Somerville RPT, Lu T, et al. Long‐duration complete remissions of diffuse large B cell lymphoma after anti‐CD19 chimeric antigen receptor T cell therapy. Mol Ther. 2017;25(10):2245‐2253. doi: 10.1016/j.ymthe.2017.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108. Atanackovic D, Luetkens T, Omili D, et al. Vaccine‐induced T‐cell responses against SARS‐CoV‐2 and its Omicron variant in patients with B cell‐depleted lymphoma after CART therapy. Blood. 2022;140(2):152‐156. doi: 10.1182/blood.2022016175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Lee D, Jordan AI, Menges MA, et al. Pneumococcal conjugate vaccine does not induce humoral response when administrated within the six months after CD19 CAR T‐cell therapy. Transplant Cell Therapy. 2023;29(4):277.e1‐277.e9. doi: 10.1016/j.jtct.2022.08.011 [DOI] [PubMed] [Google Scholar]
- 110. Angelidakis G, Chemaly RF, Kebriaei P, et al. Evaluation of retained immunity for tetanus‐diphtheria and pneumococcal vaccines in recipients of cellular therapies. Open Forum Infect Dis. 2021;8(suppl1):S131‐S132. Infectious Diseases Week, IDWeek 2021. Virtual. doi: 10.1093/ofid/ofab466.217 [DOI] [Google Scholar]
- 111. Bansal R, Vergidis P, Tosh P, et al. Vaccine titers in lymphoma patients receiving chimeric antigen receptor T‐cell therapy. J Clin Oncol. 2021;39( suppl15):7555‐7555. Annual Meeting of the American Society of Clinical Oncology, ASCO 2021. Online. doi: 10.1200/JCO.2021.39.15_suppl.7555 [DOI] [Google Scholar]
- 112. Rahman ZA, Gannon N, Melody M, et al. Impact of anti‐CD19 CAR‐T axicabtagene ciloleucel on vaccine titers of DTaP and MMR. Blood. 2019;134(suppl1):5610. 61st Annual Meeting of the American Society of Hematology, ASH 2019. Orlando, FL, USA. doi: 10.1182/blood-2019-122067 [DOI] [Google Scholar]
- 113. Hill JA, Krantz EM, Hay KA, et al. Durable preservation of antiviral antibodies after CD19‐directed chimeric antigen receptor T‐cell immunotherapy. Blood Adv. 2019;3(22):3590‐3601. doi: 10.1182/bloodadvances.2019000717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Shah N, Alarcon A, Palazzo M, et al. High rates of residual vaccine titers at 1‐year post CD19 chimeric antigen receptor T cell therapy. Transplant Cell Therapy. 2021;27( suppl3):S355. The 2021 TCT Meetings Digital Experience. Virtual, Online. doi: 10.1016/S2666-6367(21)00456-5 [DOI] [Google Scholar]
- 115. Walti CS, Krantz EM, Maalouf J, et al. Antibodies against vaccine‐preventable infections after CAR‐T cell therapy for B cell malignancies. JCI Insight. 2021;6(11):e146743. doi: 10.1172/jci.insight.146743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Rahman ZA, Gannon N, Melody M, et al. Impact of anti‐CD19 CAR‐T axicabtagene ciloleucel on vaccine titers of DTaP and MMR. Blood. 2019;134(suppl1):5610. 61st ASH Annual Meeting. Orlando, FL, USA. doi: 10.1182/blood-2019-122067 [DOI] [Google Scholar]
- 117. Walti CS, Loes AN, Shuey K, et al. Humoral immunogenicity of the seasonal influenza vaccine before and after CAR‐T‐cell therapy: a prospective observational study. J Immunother Cancer. 2021;9(10):e003428. doi: 10.1136/jitc-2021-003428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Bhoj VG, Arhontoulis D, Wertheim G, et al. Persistence of long‐lived plasma cells and humoral immunity in individuals responding to CD19‐directed CAR T‐cell therapy. Blood. 2016;128(3):360‐370. doi: 10.1182/blood-2016-01-694356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119. Dahiya S, Luetkens T, Avila S, et al. Impaired mRNA based COVID‐19 vaccine response in patients with B‐cell malignancies after CD19 directed CAR‐T cell therapy. Blood. 2021;138(suppl1):1738. 63rd American Society of Hematology Annual Meeting and Exposition, ASH 2021. Atlanta, GA, USA. doi: 10.1182/blood-2021-153949 [DOI] [Google Scholar]
- 120. Iraguha T, Dahiya S, Avila S, Rapoport A, Luetkens T, Atanackovic D. Immune response to COVID‐19 vaccination in patients with B‐cell malignancies after CD19 CART cell therapy. Cancer Res. 2022;82( suppl12):3586. American Association for Cancer Research Annual Meeting, ACCR 2020. New Orleans, LA, USA. doi: 10.1158/1538-7445.AM2022-3586 [DOI] [Google Scholar]
- 121. Hill JA, Li D, Hay KA, et al. Infectious complications of CD19‐targeted chimeric antigen receptor‐modified T‐cell immunotherapy. Blood. 2018;131(1):121‐130. doi: 10.1182/blood-2017-07-793760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Logue JM, Zucchetti E, Bachmeier CA, et al. Immune reconstitution and associated infections following axicabtagene ciloleucel in relapsed or refractory large B‐cell lymphoma. Haematologica. 2021;106(4):978‐986. doi: 10.3324/haematol.2019.238634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Park JH, Romero FA, Taur Y, et al. Cytokine release syndrome grade as a predictive marker for infections in patients with relapsed or refractory B‐cell acute lymphoblastic leukemia treated with chimeric antigen receptor T cells. Clin Infect Dis. 2018;67(4):533‐540. doi: 10.1093/cid/ciy152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Rotshild V, Hirsh‐Raccah B, Miskin I, Muszkat M, Matok I. Comparing the clinical efficacy of COVID‐19 vaccines: a systematic review and network meta‐analysis. Sci Rep. 2021;11(1):22777. doi: 10.1038/s41598-021-02321-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Abid MA, Abid MB. SARS‐CoV‐2 vaccine response in CAR T‐cell therapy recipients: a systematic review and preliminary observations. Hematol Oncol. 2022;40(2):287‐291. [DOI] [PubMed] [Google Scholar]
- 126. Dong N, Jain AG, Tan ES, et al. Immunogenicity of Sars‐Cov‐2 mRNA 1273 vaccine in patients with lymphoid malignancies. Blood. 2021;138(suppl1):2504. 63rd ASH Annual Meeting. Atlanta, GA, USA. doi: 10.1182/blood-2021-150465 [DOI] [Google Scholar]
- 127. Fox TA, Kirkwood AA, Enfield L, et al. Low seropositivity and suboptimal neutralisation rates in patients fully vaccinated against COVID‐19 with B‐cell malignancies. Br J Haematol. 2021;195(5):706‐709. doi: 10.1111/bjh.17836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Gastinne T, Le Bourgeois A, Coste‐Burel M, et al. Antibody response after one and/or two doses of BNT162B2 anti‐SARS‐CoV‐2 mRNA vaccine in patients treated by CAR T‐cells therapy. Blood. 2021;138(suppl1):254. 63rd American Society of Hematology Annual Meeting and Exposition, ASH 2021. Atlanta, GA, USA. doi: 10.1182/blood-2021-149476 [DOI] [Google Scholar]
- 129. Goessi S, Bacher U, Haslebacher C, et al. Poor humoral responses to mRNA vaccines against SARS‐CoV‐2 in patients after CAR‐T‐cell therapy. Swiss Medical Weekly. 2021;151(suppl 255):6S. Swiss Oncology and Hematology Congress, SOHC 2021. Zurich, Switzerland. [Google Scholar]
- 130. Sharma A, Bhatt NS, Hijano DR. Clinical experience of coronavirus disease 2019 in hematopoietic cell transplant and chimeric antigen receptor T‐cell recipients. Curr Opin Hematol. 2021;28(6):394‐400. [DOI] [PubMed] [Google Scholar]
- 131. Wudhikarn K, Palomba ML, Pennisi M, et al. Infection during the first year in patients treated with CD19 CAR T cells for diffuse large B cell lymphoma. Blood Cancer J. 2020;10(8):1‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Shapiro LC, Gali R, Thakkar A, et al. Seroconversion rates after COVID‐19 vaccination amongst patients with hematologic malignancies: results of a rapid vaccination and evaluation program in a minority rich, ethnically diverse inner city cohort. Blood. 2021;138(suppl1):2537. 63rd American Society of Hematology Annual Meeting and Exposition, ASH 2021. Atlanta, GA, USA. doi: 10.1182/blood-2021-151309 [DOI] [Google Scholar]
- 133. Gossi S, Bacher U, Haslebacher C, et al. Humoral responses to repetitive doses of COVID‐19 mRNA vaccines in patients with CAR‐T‐cell therapy. Cancers. 2022;14(14):3527. doi: 10.3390/cancers14143527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Parvathaneni K, Toress‐Rodriguez K, Meng W, et al. Adoptive immune responses to SARS‐CoV2 vaccination in CART19 treated patients. Blood. 2021;138(suppl1):1757. 63rd American Society of Hematology Annual Meeting and Exposition, ASH 2021. Atlanta, GA, USA. doi: 10.1182/blood-2021-153730 34041523 [DOI] [Google Scholar]
- 135. Pollard AJ, Bijker EM. A guide to vaccinology: from basic principles to new developments. Nat Rev Immunol. 2021;21(2):83‐100. doi: 10.1038/s41577-020-00479-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Van Oekelen O, Agte S, Aleman A, et al. Suboptimal humoral and cellular immune response to Sars‐Cov‐2 RNA vaccination in myeloma patients is associated with anti‐cd38 and bcma‐targeted treatment. Blood. 2021;138(suppl1):822. 63rd American Society of Hematology Annual Meeting and Exposition, ASH 2021. Atlanta, GA, USA. doi: 10.1182/blood-2021-152365 34499154 [DOI] [Google Scholar]
- 137. Van Oekelen O, Gleason CR, Agte S, et al. Highly variable SARS‐CoV‐2 spike antibody responses to two doses of COVID‐19 RNA vaccination in patients with multiple myeloma. Cancer Cell. 2021;39(8):1028‐1030. doi: 10.1016/j.ccell.2021.06.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138. Hayden PJ, Roddie C, Bader P, et al. Management of adults and children receiving CAR T‐cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol. 2022;33(3):259‐275. doi: 10.1016/j.annonc.2021.12.003 [DOI] [PubMed] [Google Scholar]
- 139. Fred Hutchinson Cancer Centre . Immunotherapy (IMTX): Vaccination after B Cell‐Targeted CAR‐T Cell Therapy for Adult and Pediatric Immune Effector Cell (IEC) Patients. Accessed April 2023. https://www.fredhutch.org/content/dam/www/research/patient‐treatment‐and‐support/ltfu/imtx_immunotherapy_vaccination_b_cell_targeted.pdf
- 140. Styczynski J. Infections following car‐t cells therapy: current state‐of‐the‐art review and recommendations. Acta Haematol Pol. 2020;51(1):11‐16. doi: 10.2478/ahp-2020-0004 [DOI] [Google Scholar]
- 141. Rieger CT, Liss B, Mellinghoff S, et al. Anti‐infective vaccination strategies in patients with hematologic malignancies or solid tumors—guideline of the Infectious Diseases Working Party (AGIHO) of the German Society for Hematology and Medical Oncology (DGHO). Ann Oncol. 2018;29(6):1354‐1365. doi: 10.1093/annonc/mdy117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Advisory Committee on Immunization Practices . Vaccine Recommendations and Guidelines from ACIP: Altered Immunocompetence. Accessed April 2023. https://www.cdc.gov/vaccines/hcp/acip‐recs/general‐recs/immunocompetence.html
- 143. Australian Government Department of Health and Aged Care . Australian Immunisation Handbook: Vaccination for People who are immunocompromised. Accessed April 2023. https://immunisationhandbook.health.gov.au/contents/vaccination‐for‐special‐risk‐groups/vaccination‐for‐people‐who‐are‐immunocompromised#haematopoietic‐stem‐cell‐transplant‐recipients
- 144. Advisory Committee on Immunization Practices . Proposed Updates to Clinical Guidance on Pneumococcal Vaccine Use among Adults. Accessed April 2023. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides‐2022‐10‐19‐20/04‐pneumococcal‐kobayashi‐508.pdf
- 145. Parkkali T, Ölander RM, Ruutu T, et al. A randomized comparison between early and late vaccination with tetanus toxoid vaccine after allogeneic BMT. Bone Marrow Transplant. 1997;19(9):933‐938. doi: 10.1038/sj.bmt.1700768 [DOI] [PubMed] [Google Scholar]
- 146. Australian Government Department of Health and Aged Care . ATAGI 2023 Booster Advice. Accessed April 2023. https://www.health.gov.au/news/atagi‐2023‐booster‐advice
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This is a review article with no new original data provided.