

Abstract
The guideline discusses the various milestones in typical neurodevelopment and the various checkpoints where atypical development can be picked up. There is also a remarkable influence of epigenetics and parenting on child development and well – being. It is also essential to establish effective communication to facilitate healthy child development. Well being in children is largely impacted by schooling, curricular design, inclusivity, teacher training and awareness of newer developments, parent teacher interaction. A clinician must also be well acquainted with the National Education Program and its impact. A healthy environment, exercise, adequate nutrition, microplastics on children and adolescents, global warming are key factors in the development of children. It is indispensable for clinicians to approach well- being in a scientific way and get a clear understanding of the laws and policies for child welfare and protection.
Keywords: Children and adolescents, mental health, welll- being
The aim of this study was to bring to the forefront the need for psychiatrists to approach well-being from a neuroscience perspective. In the case of children and adolescents, being in the neurodevelopmental group, this is actually a significant paradigm to determine, as it can affect their developmental trajectory. Hence, instead of studying only illness, it is equally important to study wellness and its scientific correlates. While the authors of this particular document have no independent research in the said field, the attempt is to collate the information available and make it a ready reckoner for the treating psychiatrist.
Hence, we have discussed neurodevelopment and epigenetics, parenting, communication, early schooling, role of the environment, including coronavirus disease 2019 (COVID-19), career choices, and policies involving children and adolescents, which may impact well-being and care overall.
NEURO DEVELOPMENT AND WELL-BEING
Typically, brain development involves a series of changes that facilitate motor, cognitive, social, and academic functioning. Additionally, the typical development and the trajectory for development allow one to understand atypical development.
Typical neurodevelopment: This involves the malleable process of brain development. It is influenced by intrinsic factors, such as genetic makeup and maternal health, and external factors, such as exposure or experience across the lifespan.[1]
Prenatal to early childhood—Neuronal changes, including cell proliferation, cell loss, synaptogenesis, pruning, and synaptic plasticity, as well as myelination, promote brain development. The neuronal changes increase in the first few years of life. The fastest brain growth occurs between 25 and 40 weeks of gestation.[2] By 2 years, the frontal lobe will have 50 percent more synapses. Also, the elimination of synapses occurs throughout childhood, which enables efficiency in functioning and refinement in ability. From the third trimester till the age of 2 years, a growth spurt occurs. Myelination during the gestational period begins from deep inside the brain to the outside and from posterior to anterior. Early on, primary sensory and motor cortices myelinate during the gestational phase. The secondary areas of the basic senses (auditory discrimination, motor planning, visual discrimination, and sensory discrimination) myelinate until 4 months after birth. In the higher cortical areas, such as frontal and parietal lobes, myelination continues until the twenties. The amygdala is responsible for emotional processing, and the hippocampus is responsible for memory increase in volume until the age of 30 years. Male brains develop more slowly than female brains, which adds to the risk of developing neurodevelopmental disorders.
Childhood—The development of connections, brain growth, and myelination continues in childhood. The frontal lobe is responsible for cognition, and the temporal lobe growth is responsible for self-regulation. The development of language and spatial skills occurs during this phase.
Adolescence till young adult—This phase allows higher-order processing. There occur a reduction in gray matter and an increase in white matter. Selective pruning, which is the thinning of the cortex, occurs. This process results in cognitive development—cognitive control and decision-making. Changes in the amygdala and hippocampal growth result in learning and the ability to respond to stress.[1] Myelination at the association cortex enables the achievement of academic skills. With the onset of puberty, concept formation and task switching progressively develop.
The point to note here is that neural development is influenced by various factors, which results in deviance from the usual course of development. Etiological factors, such as genetic factors, perinatal factors, psychosocial factors, and environmental factors, play a role in neurodevelopment. A checklist for typical neuro-development is charted in Table 1.
Table 1.
Checklist for typical neurodevelopment[3]
| Checklist for typical neurodevelopment | |
| √ Social Smile | 2 months |
| √ Follows moving objects with eyes | 2–3 months |
| √ Disappearance of Moro’s and grasp (primitive reflexes) | 5 months |
| √ Squeals/laughs | 5 months |
| √ Sits with support | 6 months |
| √ Peek-a-boo | 8 months |
| √ Walks | 12 months |
| √ Proto-imperative pointing | 12 months |
| √ Vocabulary—15 words | 18 months |
| √ Pretend play/imitation/drawing basic shapes/colors | 3–4 years |
| √ Understands rules and regulations, social and moral norms | 7–8 years |
| √ Peer group influences start dominating | 9 years to adolescence |
Alterations or deviance from the typical course of development may lead to various neurodevelopmental conditions.
Table 2 explains the different conditions in atypical neuro-development.
Table 2.
Conditions with atypical neurodevelopment[1]
|
Conditions with atypical neurodevelopment: Attention deficit hyperactivity disorder:
Autism Spectrum Disorder:
Chronic illness and traumatic brain injury:
Schizophrenia Spectrum disorders:
|
IMPACT OF EPIGENETIC FACTORS ON CHILD DEVELOPMENT AND WELL-BEING
The formation and development of the brain are facilitated by genetic expression and the interplay of the environment with the genes. The environment includes family, social, educational, and experiences of the child. The concept of gene–environment interaction explains, for example, how a certain gene variant may be responsible for predicting a phenotypic outcome in the presence of a stressful environment versus another gene variant, which protects from the phenotypic outcome in a stressful environment. Various environmental factors, which influence brain development in complex ways either by direct or indirect exposure to the placenta, alter maternal physiology, which extends to the postnatal period.[4]
Prenatal period
-
Drug exposures:
Exposure to drugs and toxins during the prenatal period results in epigenetic changes in the placenta, fetus, and infant. Smoking in mothers during pregnancy may result in deoxyribonucleic acid (DNA) methylation changes in the placenta, fetal cord cells, and buccal cell samples in children at 3–6 years of age, resulting in hyperactivity and conduct disorder.[4]
-
Diet and nutrition:
Food deprivation during pregnancy led to DNA methylation changes in imprinted genes, eventually leading to metabolic and neurodevelopmental abnormalities. A reduction in folate alters DNA methylation within the imprinted genes within the placenta and fetal cord cells. With folate supplementation during pregnancy, an alteration in DNA methylation results in a marked reduction in neurodevelopmental abnormality.
Obesity and high-fat diet result in DNA methylation alterations, resulting in the acceleration of aging.
-
Maternal stress:
Exposure to stress, trauma, and anxiety in the mother may result in DNA methylation changes in the HSD11B2 gene in the placenta, which is responsible for exposure to intrauterine stress.
-
Trauma:
Trauma during pregnancy may result in DNA methylation changes in the brain-derived neurotrophic factor (BDNF) gene.
Preterm birth is a risk factor for neurodevelopmental conditions. Epigenetic conditions may result in DNA methylation changes in the NR3C1 gene, resulting in neurodevelopmental conditions.
Infancy: Childhood adversity and parental death illness may result in altered DNA methylation. Depression in mothers results in DNA methylation changes in infants. Preterm infants were associated with increased DNA methylation of NR3C1 and decreased methylation of HSD11B2, resulting in neurobehavioral disorders.
Childhood: Abuse in childhood may result in DNA methylation of the FK506-binding protein, which results in reactivity to stress. Sexual abuse in childhood predicts age acceleration in adults.
Child development: Mother's reciprocity, which is the external regulation of the infant's developing immature emotional system during the selected critical periods, impacts the experience-dependent growth of brain areas relating to mood and behavior. Attachment behaviors promotes infant and parent proximity. Availability of an attachment figure such as mother has a great influence on the child's reduction in fear. Frequent or prolonged separation from maternal figure leads to stress affecting infant and adult personality. Early social interactions facilitate affective regulation, learning through cues such feeding needs, emotional warmth, sensory stimulation by the caregiver and emotional experiences.[5] Tactile experiences such as holding, skin to skin contact and carrying the baby are crucial in the development of the child.[6]
Epigenetic factors, though often implicated, need a lot more research for us to label them as causative. We have some data to show aberrations that occur; however, there are many children and adolescents who face tremendous adversity and yet emerge healthy. The epigenetics of such resilience calls for further research.
IMPACT OF PARENTING ON WELL-BEING
Parenting is another environmental factor that might have an impact on overall child development. Family interaction and experiences impact the genetic variant and influence behavioral and developmental outcomes.[7] Child-rearing practices or parenting practices involve specific behaviors that parents use to interact and socialize with their children. Parenting practices involve disciplining, positive reinforcements, problem-solving, ensuring a child's health and safety, preparing the child to become productive adults, and transmitting cultural value.[8,9] However, parenting alone cannot be implicated as causative. There is always a multimodal impact of various factors that ultimately help the child develop.
Parenting and epigenetics: There is an association between maternal positive caregiving behaviors, such as stroking the child, sensitivity, and responsiveness, and reduced NR3C1 methylation at specific sites.[10]
Transgenerational parenting: Parenting styles are similar from one generation to another. The expression of mothering behavior is associated with prior life experiences. A significant degree of continuity exists between positive and harsh parenting in both males and females across different generations.[11] A positive early experience later predicts maternal behavior. Less authoritarian, positive climate in middle childhood, and positive attachment in adolescence predicted warm, sensitive, and stimulating maternal behavior in adulthood.[12]
Parenting involves nourishing, protecting, and guiding a child through the course of development. Parenting style implies parental attitude and behavior consistently used across different contexts to manage children's behavior and is determined by patterns of control, responsiveness, warmth, and punishment.
Baumrind (1971) first described parenting styles and classified them into three types—authoritarian, authoritative, and permissive parenting styles. This is based on the interaction between parent and child along two dimensions of parental control, expectation, or demandingness and parental warmth.
An authoritarian parent—It is highly demanding with a low level of autonomy and is less responsive.
An authoritative parent—It is highly demanding and grants autonomy. Communication is open and bilateral.
A permissive parent—It grants a high level of autonomy and is less demanding.
Furthermore, Maccoby and Martin (1983) differentiated permissive parenting into permissive indulgent and permissive indifferent. Permissive indulgent parents are those who are highly involved in the child's care, and permissive indifferent parents are those who are uninvolved and neglectful and show responsiveness and demandingness. This is at times termed the fourth type, or simply neglectful parenting.
Parents who demonstrated high levels of control, aggression, anxiety, depression, and problem behaviors in children were seen. Children who displayed autonomy-supported behavior had an intrinsic motivational orientation and a low risk of being bullied over the years than those provided with little support for autonomy. An authoritative parenting style is found to have the best positive outcome. Adolescents with authoritative parents were protected against substance use more than those whose parents were perceived as uninvolved. Authoritative parenting and parental warmth serve as a buffer against suicide and harmful consequences.[7]
Parenting in families with special needs
Families are an essential support for children with disabilities. Children with special needs warrant the families' time and emotional resources and are associated with an increase in the cost of care. Mothers of children with intellectual developmental disorders were found to experience more depression than those of typically developing children. Families with children with behavioral problems experienced an increase in burden and stress. It was also associated with poor parenting efficiency, poorer mental health, and poor marital adjustment. Family burden and stress increased with personal care needs, adaptive behavior deficits, and medical needs. A positive outlook on childhood disability correlates with decreased feelings of stress and burden. Positive appraisals lead to better coping.[13]
Parenting children with neurodevelopmental disorders and externalizing disorders was associated with less positive, less consistent, and ineffective parenting behaviors.[14] The experience of stress in parents limits their abilities to cope, and support for the children diminishes.[15] Hence, while parenting a child with special needs, apart from a limited setting, a certain degree of acceptance and permissiveness is needed.
A common finding in siblings of a child with special needs is the experience of stress, low self-esteem, internalized behavior problems, academic problems, stigma from peers, and sensitivity to typical family stressors.[16] Hence, the clinician must be aware, identify the difficulties faced by the sibling, and appropriately intervene. Siblings need to be involved early on in the family counseling session, so they share a healthy relationship with the special needs child and can help with the environmental stability needed by the said child. This also gives the parents tremendous support in their children's adult years, as they know that the special needs adult will be cared for after them.
EFFECTIVE COMMUNICATION WITH YOUNGER CHILDREN[17]
Communication is often an extension of parenting per se. However, communication occurs in various environments to which the child is exposed, viz., schools and homes, and can impact their overall well-being.
Communication—verbal includes pitch and tone of voice, words, and dialect.
Nonverbal communication—facial expressions, eye contact, personal space, hand gestures, and physical touch such as a hug.
UNICEF lays down nine ways to communicate effectively with children.
Active listening—It helps them feel heard. Using gestures, such as nods and smiles, helps them understand the care and involvement of the caregivers. Getting down to the same level as your child as they speak to you can help them feel safer and more connected to you. Listening intently, asking questions to them, and using stories to communicate help engagement.
Reflective listening—It repeats back in different words, conveying that you have understood.
Speaking clearly.
Avoiding bribes.
Explaining feelings—It enables them to learn how to name feelings and empathic listening while they share their feelings.
Noticing statements—It includes praising the child for good actions. Instead of saying “good job” being specific with a noticing statement, “I noticed that you put all your toys away after playtime. That is very good.”
Having fun together.
Focusing on behavior and not the person. For example, “I don't like that you are messy.” can be reframed to “I don't like it when you leave your clothes all over the floor.”
Leading by example.
IMPACT OF SCHOOLING ON NORMAL DEVELOPMENT AND WELL-BEING
Well-being and life skills as a measure of mental health become imperative to include in school curricula and teacher training curricula as well. The approach needs to be focused, scientific, and cost-effective. The National Education Programme (NEP) aims to achieve some of the above. As psychiatrists, it is important for us to encourage the same, to achieve a generation of healthy and well-developed youth. The various ways in which schooling and education can affect child development and well being are mentioned in Table 3.
Table 3.
Schooling and education in child- development and well- being
Aspects of schooling and education on child development and well-being
|
a. Curricular design
Curricular design in schools plays a crucial role in the normal development and overall well-being of children and adolescents. The curriculum, which includes the subjects, teaching methods, and learning experiences provided by the school, can shape various aspects of a student's life, from their academic achievements to their social and emotional development. A holistic curriculum includes physical activities, interspersed with academics. There should also be exposure to community work, art and craft, visits to, and discussions on various occupations, such as street cleaners, carpenters, and janitors, to inculcate a sense of dignity of labor and respect in the minds of students. If possible, skill-based courses, such as painting, carpentry, and cleaning, can be introduced in the school itself. Here are some ways in which it can help[18] also mentioned in Table 4.
Table 4.
Curricular design
| Curricular design Academic development Social and emotional development Physical development Cognitive development Cultural and Global awareness Career and life skills Individualised learning |
Academic Development: The curriculum determines what knowledge and skills students acquire during their educational journey. A well-designed curriculum can provide a balanced and comprehensive education that fosters intellectual growth and academic success.
Social and Emotional Development: The curriculum can influence the social and emotional development of students by promoting positive interactions, teamwork, and empathy. A supportive and inclusive curriculum can create a safe and nurturing environment, reducing stress and anxiety while promoting a sense of belonging and well-being.
Physical Development: Curricular design can incorporate physical education and sports programs, encouraging regular physical activity and promoting physical well-being. By emphasizing the importance of a healthy lifestyle, the curriculum can instill lifelong habits of exercise and self-care.
Cognitive Development: A well-structured curriculum can stimulate cognitive development by providing age-appropriate content and learning experiences. The curriculum can expand students' cognitive abilities and help them develop a thirst for knowledge.
Cultural and Global Awareness: Curricular design can expose students to diverse cultures, traditions, and global issues. It can also encourage global awareness, preparing students to be responsible global citizens in an increasingly interconnected world.
Career and Life Skills: The curriculum can include practical skills that prepare students for future careers and life beyond school. By developing these skills, the curriculum enhances students' self-confidence and their ability to navigate real-world challenges.
-
Individualized Learning: A flexible and inclusive curriculum design allows for individualized learning experiences tailored to students' needs, interests, and abilities. This also includes learning from external sources, which may have both positive and negavtive consequences.
Life skills training: Life skills training involve the training in adaptive and positive behavior enabling individuals to effectively address daily challenges, stress in daily life and demands. They particularly involve the decision making and problem solving, critical thinking and creative thinking, communication skills and interpersonal relations skills, coping with emotions and stress, self awareness and empathy.[19]
b. Inclusivity
Inclusivity in schools is vital for the overall well-being of children and adolescents. When schools prioritize inclusivity, they create an environment where every student feels valued, respected, and supported, regardless of their background, abilities, or identities. Inclusive schools and colleges cater to students across all strata of society and across intelligence levels and medical diagnoses. In short, no child should not go to school, because the school cannot “cater to” or “manage” such a child. School infrastructure and personnel have to be trained to manage the same. An inclusive environment helps in the following ways:[19,20] as also enlisted in Table 5.
Table 5.
Various ways of bringing inclusivity in schools
| Inclusivity Sense of belonging Emotional well- being Academic achievement Social skills and relationships Reduced stigma and bias Supportive services and resources Empowerment and advocacy |
Sense of Belonging: Inclusive schools foster a sense of belonging among all students. When students feel accepted and included, they are more likely to develop positive self-esteem and a sense of identity.
Emotional Well-being: Inclusive schools provide a safe and supportive space for students to express their emotions, concerns, and challenges.
Academic Achievement: Inclusive schools prioritize individualized learning and support for all students. They recognize and address diverse learning needs and provide appropriate accommodations and resources.
Social Skills and Relationships: Inclusive environments foster positive social interactions and friendships among students from various backgrounds and abilities.
Reduced Stigma and Bias: Inclusive schools challenge stereotypes, prejudices, and biases. They create opportunities for students to learn about different cultures, abilities, and identities, promoting acceptance and understanding.
Supportive Services and Resources: Inclusive schools provide access to a range of support services and resources to address students' diverse needs. These may include counseling, special education, language support, and mental health services.
Empowerment and Advocacy: Inclusive schools empower students to become advocates for themselves and others. They encourage students to voice their opinions, engage in decision-making processes, and take on leadership roles.
c. Teacher Training and the awareness of newer developments
Teacher training and awareness of newer developments in their field are crucial for both the well-being of teachers and the quality of education they provide to children and adolescents in the following ways:[20,21] Table 6 mentions the various ways of training and creating awareness.
Table 6.
Teacher training and awareness of newer developments
| Teacher training and awareness of newer developments Professional growth Increased effectiveness Reduced stress Collaboration and support Adaptation to changing needs Personal and professional reflection Well- being promotion |
Professional Growth: Ongoing teacher training helps educators stay updated with the latest research, pedagogical approaches, and best practices in their field.
Increased Effectiveness: Training and awareness of newer developments enable teachers to implement innovative teaching strategies and instructional methods in their classrooms.
Reduced Stress: When teachers are well-trained and aware of effective teaching techniques, they are better equipped to handle the challenges and demands of their profession.
Collaboration and Support: Teacher training often includes opportunities for collaboration and professional networking. Educators can connect with colleagues, share experiences, and learn from one another.
Adaptation to Changing Needs: The field of education is constantly evolving, with new technologies, research, and educational policies emerging. Teacher training ensures that educators stay abreast of these changes and are prepared to address the evolving needs of students.
Personal and Professional Reflection: Training and awareness programs often provide opportunities for self-reflection and self-improvement. Teachers can assess their teaching practices, identify areas for growth, and set professional goals.
Well-Being Promotion: Teacher training programs are increasingly incorporating well-being initiatives to support the mental, emotional, and physical health of educators.
d. Parent–Teacher Interaction
Parent–teacher interaction plays a crucial role in the well-being and development of students. When parents and teachers collaborate and maintain open lines of communication, it creates a supportive and nurturing environment that positively impacts the overall growth of the child in the following ways:[21,22] Table 7 explains the impact and elements of parent teacher interaction.
Table 7.
Impact and elements of parent teacher interaction
| Parent teacher interaction Academic success Emotional and social development Individualised support Consistency and reinforcement Early identification of issues |
Academic Success: Regular communication between parents and teachers enables the sharing of valuable information about a student's progress, strengths, and areas needing improvement.
Emotional and Social Development: Parents and teachers each bring unique insights and perspectives to a student's life. By sharing information about a child's emotional well-being, behavior, and social interactions, parents and teachers can work collaboratively to create a consistent approach to supporting the student's social and emotional development.
Individualized Support: Effective parent–teacher interaction allows for a comprehensive understanding of a student's strengths, weaknesses, learning styles, and interests.
Consistency and Reinforcement: When parents and teachers align their efforts, it reinforces consistent expectations and values in a student's life. Consistency in discipline, routines, and reinforcement of positive behaviors at home and school promotes stability.
Early Identification of Issues: Parent–teacher interaction facilitates the early identification of any potential challenges or developmental issues a student may be facing. When parents and teachers work hand in hand, students thrive, and their potential is maximized.
National Education Program and its impact
The NEP is a comprehensive framework for transforming the education system in India. It aimed to address various challenges and issues in the existing system while focusing on the holistic development of students. The NEP could have several potential effects on the youth in India[22,23]: The various components of National Education program have mentioned in Table 8.
Table 8.
National Education policy : components
| National Education Policy Holistic development Vocational education Flexibility and Choice Promotion of regional languages Technology integration Higher education reforms Focus on early childhood education Teacher training and professional development Reducing Examination Stress |
Holistic Development: The NEP emphasizes a multidisciplinary approach to education, encouraging students to explore a wide range of subjects and develop a well-rounded skill set.
Vocational Education: The policy stresses the importance of vocational education, providing practical skills and training to students. This can help young people become more employable and reduce the skill gap, enabling them to enter the workforce with relevant expertise.
Flexibility and Choice: The NEP proposes increased flexibility in the education system, allowing students to choose subjects based on their interests and capabilities and allowing youth to pursue fields that align with their passions and aspirations.
Promotion of Regional Languages: The NEP aims to promote regional languages as mediums of instruction up to a certain level, which can help preserve cultural diversity and strengthen students' connection to their roots.
Technology Integration: The policy encourages the integration of technology in education, which can improve access to quality education and equip young learners with digital literacy skills.
Higher Education Reforms: The NEP proposes changes in the higher education system, including multidisciplinary institutions and increased emphasis on research and innovation.
Focus on Early Childhood Education: The NEP recognizes the importance of early childhood education and aims to provide a strong foundation for young learners.
Teacher Training and Professional Development: The policy highlights the need for teacher training and professional development to improve the quality of education.
Reducing Examination Stress: The NEP proposes changes in assessment and evaluation methods to reduce the stress associated with examinations.
A holistic approach to education, along with the welfare and training of educators, can have a profound impact on the well-being of children, and we hope the NEP finds actual implementation in our country and does not remain only as a white paper.
IMPACT OF THE ENVIRONMENT ON WELL-BEING
Environment change is taking a toll on the human race, as we well know. The impact on children is direct (as seen with adults) and indirect (as a consequence of the impact on the mother and therefore transmission through affected genetic material).[23,24]
Table 9 points out the different ways of impact of environment on well- being.
Table 9.
Impact of environment on child well- being
| Impact of environment Impact of a healthy environment Impact of exercise Impact of nutritional awareness Impact of microplastics Impact of global warming Community involvement and awareness |
a. Healthy Environment
A healthy environment can have a profound and positive impact on the well-being of children and adolescents. When children grow up in an environment that supports their physical, emotional, and social needs, they are more likely to experience positive outcomes and develop into resilient and well-adjusted individuals. Here are some key ways in which a healthy environment can benefit child and adolescent well-being:
WHO and UNICEF data on physical well-being and correlation with mental well-being
Physical Health: A clean and safe environment with access to nutritious food, clean water, and adequate sanitation facilities can promote better physical health. Children who grow up in such environments are less likely to suffer from malnutrition, waterborne diseases, or exposure to environmental toxins. Physical activity is beneficial to mental health in children and adolescents.[25]
Mental and Emotional Well-being: A healthy environment can create a supportive and nurturing atmosphere that fosters positive mental health for children and adolescents.
Social Development: A healthy environment that encourages positive social interactions, empathy, and cooperation can promote healthy relationships with family members, peers, and the broader community.
Academic Achievement: A conducive environment for learning, including well-equipped schools, competent teachers, and supportive educational resources, can positively impact academic achievement and cognitive development in children and adolescents.
Physical Activity and Play: A healthy environment with access to safe and stimulating play spaces encourages physical activity and outdoor play. Regular physical activity is essential for physical health, motor skill development, and overall well-being.
Resilience and Coping Skills: Growing up in a healthy environment can contribute to the development of resilience and coping skills in children and adolescents. They learn to adapt to challenges, bounce back from setbacks, and develop problem-solving abilities.
Role Modeling: In a healthy environment, children are more likely to be exposed to positive role models, such as supportive parents, caring teachers, and responsible community members. These role models can have a significant impact on their values, attitudes, and behaviors.
Long-term Outcomes: Children and adolescents who grow up in a healthy environment are more likely to experience positive long-term outcomes, such as higher educational attainment, better employment opportunities, and overall life satisfaction.
b. Impact of Exercise
Exercise has a wide range of positive impacts on children and adolescents, influencing their physical health, mental well-being, cognitive development, and social interactions. Regular physical activity is essential for young individuals' overall growth and development. Here are some of the significant benefits of exercise for children and adolescents[24,26]:
Physical Health: Regular exercise contributes to better cardiovascular health, improved muscular strength and endurance, and increased flexibility and balance.
Bone Health: Weight-bearing exercises, such as running and jumping, promote bone density and strength, reducing the risk of osteoporosis later in life.
Motor Skill Development: Physical activity helps develop gross and fine motor skills in children, enhancing their coordination and control over body movements.
Brain Health and Cognitive Development: Exercise is linked to improved cognitive function, attention, and academic performance. It can enhance memory, information processing, and problem-solving abilities.
Mental Health and Emotional Well-Being: Regular physical activity is associated with reduced stress, anxiety, and symptoms of depression in children and adolescents. Exercise triggers the release of endorphins, the “feel-good” hormones, which can improve mood and overall mental well-being.
Sleep Quality: Engaging in regular physical activity can promote better sleep patterns, leading to improved sleep quality and overall restfulness.
Social Skills and Teamwork: Participating in team sports or group exercise activities fosters social interactions, communication skills, and teamwork abilities.
Self-Confidence and Self-Esteem: Achieving physical milestones and improvements in sports or activities can boost self-confidence and self-esteem in children and adolescents.
Time Management and Discipline: Regular exercise requires commitment and discipline, teaching children to manage their time effectively and follow a routine.
Healthy Habits Formation: Encouraging regular physical activity during childhood lays the foundation for a lifelong commitment to healthy habits and an active lifestyle.
Positive Body Image: Engaging in physical activity can help children and adolescents develop a positive body image and a healthy attitude toward their bodies.
Conflict Resolution and Emotional Regulation: In team sports, children learn conflict resolution skills and emotional regulation through interactions with teammates and opponents.
C. Impact of Nutritional Awareness
Nutritional awareness plays a significant role in the health and well-being of children and adolescents. When young individuals are informed about the importance of healthy eating habits and make conscious choices about their nutrition, several positive impacts can be observed:[25,27]
Improved Physical Health: Nutritional awareness promotes the consumption of balanced and nutritious foods, providing essential nutrients for growth and development.
Healthy Growth and Development: Adequate nutrition supports proper growth and development during childhood and adolescence, ensuring that children reach their full potential in terms of height, weight, and cognitive abilities.
Cognitive Function and Academic Performance: Proper nutrition is essential for optimal brain development and cognitive function. Nutritional awareness can lead to better food choices, positively impacting concentration, memory, and academic performance.
Energy Levels and Physical Performance: A balanced diet provides the necessary energy for physical activities and sports. Nutritional awareness helps young individuals fuel their bodies appropriately, enhancing endurance, strength, and overall athletic performance.
Reduced Risk of Eating Disorders: Nutritional awareness can promote a healthy relationship with food and reduce the likelihood of developing eating disorders, such as anorexia or bulimia.
Positive Body Image: Understanding the role of nutrition in maintaining good health helps young individuals develop a positive body image and self-esteem, focusing on overall well-being rather than appearance alone.
Better Mental Health: Proper nutrition contributes to better mental health, reducing the risk of mood disorders, such as anxiety and depression.
d. Impact of Microplastics on Children and Adolescents[26,28]
Health Concerns: Microplastics are small plastic particles that can be ingested or inhaled. Studies have shown that microplastics can enter the human body through various sources, including contaminated food, water, and even air.
Endocrine Disruption: Some microplastics contain additives, such as phthalates and bisphenols, which can disrupt the endocrine system. These disruptions can lead to hormonal imbalances and may affect growth, development, and reproductive health in children and adolescents. This possibly starts in utero, due to maternal exposure, and is hypothesized to be the cause of many changes in the basic human genome.
Respiratory Issues: Microplastics in the air can be inhaled and may cause or exacerbate respiratory issues in children, such as asthma or other respiratory problems.
Environmental Justice: Children and adolescents from marginalized communities may face a disproportionate burden of microplastic pollution due to living in areas with higher levels of plastic waste and pollution.
e. Impact of Global Warming on Children and Adolescents:[27,29]
Health Risks: Global warming is linked to an increase in extreme weather events, heat waves, and air pollution, all of which can directly impact children's health.
Nutrition and Food Security: Climate change affects agriculture and food production, leading to disruptions in food supply and nutrition. Children in vulnerable regions may face food insecurity and malnutrition as a result.
Migration and Displacement: Climate-induced changes, such as sea-level rise and extreme weather events, can trigger displacement and migration, which can be particularly challenging for children and adolescents, disrupting their education, social networks, and mental well-being.
Mental Health: The uncertainty and fear associated with climate change, including its long-term consequences, can contribute to anxiety, depression, and eco-anxiety in children and adolescents.
Education Disruption: Extreme weather events can disrupt education infrastructure and access to schooling, impacting learning opportunities and educational outcomes for children.
Future livelihoods: The long-term effects of climate change, such as loss of biodiversity and changes in ecosystems, may affect future job prospects and economic opportunities for adolescents.
Inequitable Impact: Children and adolescents in low-income countries and vulnerable communities are often more susceptible to the impacts of global warming due to limited access to resources and adaptive measures.
f. Community involvement and awareness
Children and adolescents play a crucial role in community involvement, and their active participation can have a positive impact on mental health, both for themselves and others in the community. Here are some ways in which children and adolescents can contribute to community involvement and promote mental well-being as also shown in Table 9:[28,30]
Youth-Led Initiatives: Encourage children and adolescents to take the lead in creating and participating in community projects and initiatives that address mental health issues. Youth-led campaigns, support groups, and awareness programs can help reduce stigma, increase understanding, and promote mental health literacy within the community.
Peer Support Networks: Children and adolescents can develop peer support networks to help their peers cope with mental health challenges. These networks can provide a safe space for young individuals to share their experiences, offer empathetic support, and connect with others facing similar issues. These support groups should cover aspects like broken families, break ups, etc.
Mental Health Advocacy: Engage young people in mental health advocacy efforts within the community. They can participate in awareness campaigns, speak up about mental health issues, and advocate for improved access to mental health services and resources.
Community Education Programs: Children and adolescents can actively participate in organizing and conducting educational workshops or events related to mental health. By sharing knowledge and resources, they can help community members better understand mental health and reduce misinformation and stigma.
Artistic Expression: Art, music, and other creative forms of expression can be powerful tools to address mental health issues. Children and adolescents can organize or participate in art exhibitions, performances, or storytelling events that highlight mental health themes and promote emotional well-being.
Youth Mental Health Ambassadors: Designate and empower young individuals as mental health ambassadors in schools and communities. These ambassadors can serve as points of contact for peers who need support or guidance related to mental health.
Volunteering: Engage young people in mental health-related volunteering activities, such as supporting local mental health organizations, participating in helplines, or assisting in community mental health events.
Engagement in physical activity everyday, low screen behavior and with abstinence from substance use was associated with lesser subjective health complaints. A healthy life style was significamtly associated with lesser subjective health complaints. (Marques A, Demetriou Y, Tesler R, Gouveia E, Peralta M, Gaspar Matos, 2019).[31]
Hence, conscious steps toward the protection of the environment and working toward involving children in the awareness and protection of the environment both work toward improved overall quality of life and well-being.
RECENT TRENDS
Maternal stress during pregnancy can have both short-term and long-term effects on the health of both the mother and the child. Stress during pregnancy may increase the risk of complications, such as preterm birth, low birth weight, and developmental issues in the child.
COVID-19 is caused by the novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). When it comes to pregnancy, there are concerns about the potential effects of COVID-19 on maternal and fetal health. Pregnant women were initially considered at higher risk of severe illness if they contracted COVID-19 due to changes in the immune system during pregnancy. However, subsequent studies have indicated that the risk for severe outcomes might not be significantly higher compared with nonpregnant adults of similar age and health status.
Studies were being conducted to examine whether babies born to mothers with COVID-19 during pregnancy, often referred to as “COVID-19 babies,” might have different neonatal outcomes compared with babies born to noninfected mothers. While some studies suggested a potential increase in preterm birth rates among COVID-19-positive pregnant women, the data were not always consistent across different studies.
b. Impact of the Digital Revolution
The digital revolution, characterized by the widespread adoption of digital technologies, Internet connectivity, and the proliferation of smartphones and other digital devices, has had a profound impact on children and adolescents. While digital technologies offer various opportunities and benefits, they also present certain challenges and risks. Here are some of the key impacts of the digital revolution on children and adolescents also mentioned in Table 10:[30,33]
Table 10.
Impact of digital revolution
|
Impact of digital revolution Access to information and education Social connectivity Mental health concern Physical health and sedentary behaviour Cyberbullying and online harassment Privacy and safety concerns Digital addiction Cognitive development Cybersecurity risks Digital literacy and skills |
Access to Information and Education: Digital technologies have made information more accessible than ever before. Children and adolescents can access educational resources, online courses, and academic materials that can enhance their learning experiences and broaden their knowledge.
Social Connectivity: Social media and online platforms have enabled children and adolescents to connect with friends and peers globally, fostering social connections and reducing feelings of isolation.
Mental Health Concerns: Excessive screen time, cyberbullying, and exposure to inappropriate content can negatively impact the mental health of children and adolescents. Social media use has been associated with increased rates of anxiety, depression, and sleep disturbances.
Physical Health and Sedentary Behavior: The digital revolution has led to increased sedentary behavior, as children and adolescents spend more time indoors using digital devices, which can contribute to health issues, such as obesity.
Cyberbullying and Online Harassment: The anonymity provided by digital platforms can facilitate cyberbullying, leading to emotional distress and potential long-term psychological effects on young individuals.
Privacy and Safety Concerns: Children and adolescents may unknowingly share personal information online, leading to privacy and safety risks. Online predators and cybercriminals can exploit this vulnerability.
Digital Addiction: The constant use of digital devices and social media can lead to addictive behaviors, with some children and adolescents finding it challenging to disconnect and engage in other activities.
Cognitive Development: Some studies suggest that excessive screen time, particularly in young children, may impact cognitive development, attention span, and language skills.
Cybersecurity Risks: As children and adolescents engage in online activities, they may become susceptible to cyberattacks, scams, or identity theft.
Digital Literacy and Skills: On the positive side, the digital revolution has emphasized the importance of digital literacy and skills, equipping young individuals with valuable capabilities required for the modern workforce.
c. Dealing with peer pressure
Social media has significantly influenced peer pressure dynamics and can have both positive and negative effects on well-being. Here is an overview of the impact of social media on peer pressure and its effect on well-being:[31,34]
Comparison and Self-Esteem: Social media platforms often present a curated version of people's lives, emphasizing achievements, appearance, and experiences. This can lead to social comparison, where individuals compare themselves to others and feel pressure to meet unrealistic standards.
Fear of Missing Out (FOMO): Social media platforms often showcase people's social activities, events, and experiences. Seeing others' posts about exciting or exclusive events can create FOMO and a sense of social pressure to participate in similar activities. This can lead to anxiety, stress, and a constant need to stay connected and be part of the perceived social “in-crowd.”
Body Image and Beauty Standards: Social media can significantly impact body image perceptions and beauty standards. Influencers and celebrities often promote specific body types, beauty ideals, and beauty products, leading to a desire to conform to these standards.
Risky Behaviors and Peer Influence: Social media can amplify peer pressure to engage in risky behaviors. The online sharing of potentially harmful activities, such as substance abuse, dangerous challenges, or self-destructive behaviors, can normalize and encourage participation.
Supportive Communities and Positive Influences: However, social media can also foster positive peer pressure and support. Online communities and groups centered around shared interests, hobbies, mental health, and well-being can provide a supportive environment and encourage positive behaviors.
Cyberbullying and Social Exclusion: Social media can exacerbate peer pressure by enabling cyberbullying and social exclusion. Negative comments, online harassment, and exclusion from online social groups can severely impact well-being, leading to increased stress, anxiety, and depression.
Encouraging critical thinking, cultivating a positive online environment, and fostering open discussions about the influence of social media can help individuals navigate the pressures effectively. Additionally, fostering offline connections, engaging in activities that promote well-being outside of social media, and setting healthy boundaries with online usage can contribute to maintaining a balanced and positive well-being. Social media conferences or symposia are held in schools and colleges to introduce and reinforce safety and individuality at regular and periodic intervals.
d. Effect of the gender revolution
The gender revolution, characterized by the ongoing progress toward gender equality and the breaking down of traditional gender roles and expectations, has had a significant impact on well-being as also mentioned in Table 11.[32,35]
Table 11.
Effects of gender revolution
| Effect of gender revolution Increased individual agency Improved mental health Enhanced relationship dynamics Halth and reproductive rights Social and community support |
Increased Individual Agency: The gender revolution has granted individuals, irrespective of their gender, greater agency, and the freedom to explore diverse opportunities and life choices. Breaking away from rigid gender stereotypes and expectations allows individuals to pursue their passions, goals, and interests, leading to a sense of fulfillment and personal well-being.
Improved Mental Health: Challenging traditional gender roles and stereotypes has contributed to improved mental health outcomes. By embracing a more inclusive understanding of gender, individuals are less likely to experience the negative psychological effects of gender-based discrimination, stigma, and prejudice.
Enhanced Relationship Dynamics: The gender revolution has had positive implications for relationship dynamics. By challenging traditional gender roles, couples and families have greater flexibility in dividing responsibilities, decision-making, and caregiving.
Health and Reproductive Rights: The gender revolution has also brought attention to women's health issues, reproductive rights, and access to health care. Advocacy for gender equality has contributed to improved healthcare policies, reproductive healthcare services, and increased awareness about gender-specific health concerns.
Social and Community Support: The gender revolution has sparked broader social and community support for gender equality and inclusivity. Advocacy movements, support networks, and awareness campaigns have empowered individuals and fostered a sense of solidarity and belonging.
So, we see that this generation of children and adolescents is faced with many more challenges and situations than those prevalent even a decade ago. It is imperative that we recognize and address these issues early, to foster care and well-being. Table 12 shows scales for quality of life and coping in children and adolescents.
Table 12.
Scales for quality of life and coping in chidren and adolescents
| Scales | Purpose | Age range | Miscellaneous |
|---|---|---|---|
| Youth Quality of Life instrument (YQOL R)[36] | Quality of life | 11 to 18 years | Can also be added in chronic conditions |
| Child Health Questionnaire (CHQ)[37] | Self -scored, Health related quality of life for children and adolescents | 5 to 18 years of age | Parent and child reported |
| Kids coping scale (KCS)[38] | Measures stress and coping | 7 years and above | Subscore reporting – emotion – focused coping, problem – coping coping and seeking social support. |
| The Stirling Children’s Wellbeing Scale (Educational psychology service, Stirling council and Scottish government)[39] | Measure wellbeing (emotional and psychological) – positive emotional state, positive outlook, social desirability subscale | 8-15 years of age | 15 item questionnaire |
| Strengths and Difficulties Questionnaire (SDQ)[40] | Child’s social, emotional and mental health | 2 to 17 years of age | 25 items in 5 domains of well being (emotional problems, conduct, hyperactivity, peer problems, prosocial behavior) |
| Warwick – Edinburgh Mental Wellbeing Scale (WEMWBS) Developed by researchers at the Universities of Warwick and Edinburgh[41] |
14 item , self administered questionnaire to measure wellbeing, positive mental health and well being | Children above 13 years of age |
IMPACT OF CAREER CHOICES ON HEALTH AND WELL-BEING[33,42]
The transition from an educational world (school, college, and university) to work is a linear one. Most professional courses do not really have a period of training or internship integrated into the course.[34,43]
As a result, youth are faced with a reality that is different from expectations, which leads to dissatisfaction and unemployment due to unmatched interests. Career intervention programs are designed to help bridge the gap between the end of the professional course and the choice of a suitable career. Career intervention courses, though not yet widespread globally, are catching on. They lead to more gainful employment, social integration, and social contribution.[35,44]
One of the pioneer works conducted in this area was in Hong Kong using the CLAP@JC project to assess career competency. The project involved the following six steps to ascertain career choices as shown in Figure 1:[33,42]
Figure 1.
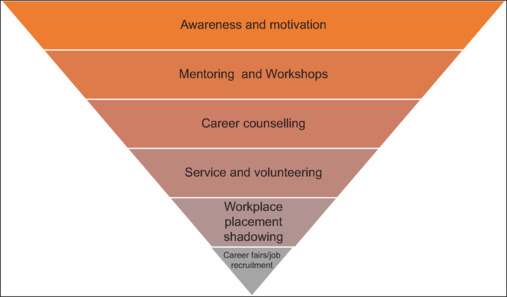
Career interventions for career counseling
Step 1: Creating awareness and motivation regarding various possible options for a profession subsequent to a particular course or competency level achieved in education.
Step 2: Semi-structured learning that involves interaction with mentors and workshops regarding the said profession. This leads to self-assessment and an understanding of the desired profession
Step 3: Career counseling. This takes place at an individual and group level, to foster an explorative process through queries of self and others, to gain further insight. Parents too should be involved in this process.
Step 4: Learning through service and volunteering in the community, usually pro bono or at a nominal stipend, to understand the actual functioning and give an added dimension of impact on society
Step 5: Placement in an actual workplace with hands-on learning and training on the job. This could be as a shadow or apprentice to someone.
Step 6: Stepping out into the market through career fairs or placement drives and connecting with people who have the same philosophy.
In addition to the above, family influence and acceptance also had a significant impact on career choices and well-being. It is at times important, to review the career options with at least one session with the entire family, which may help a more favorable outcome in terms of job satisfaction for the child.[36,45]
It would be worthwhile for Indian colleges and universities to adopt a similar or modified career intervention model to suit the Indian subcontinent. The program should be integrated with the curriculum in the final year of school, college, and professional courses, to help students make appropriate career choices and choose the path ahead accordingly, at each step of the way, and change paths should that not be attractive or suitable enough.
This becomes even more important in careers, such as medicine and paramedical courses, where the bond release to be paid is rather huge, and children feel “trapped” in that branch, despite lacking motivation and interest in the same.
Hence, this is like a funnel effect or an inverted pyramid approach to career competence.
POLICIES TOWARD CHILD WELL-BEING AND DEVELOPMENT
While it is imperative that we approach well-being in a scientific way as medical professionals, the concept itself is largely social. Hence, specific policies (either inclusive or deterrent) help safeguard child interests, thereby indirectly impacting well-being is depicted in Figure 2.
Figure 2.
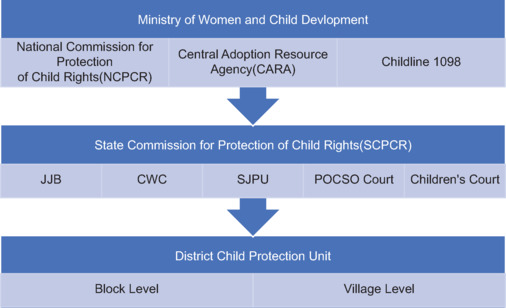
Child Welfare and Protection under the Ministry of Women and Child Development. (JJB—Juvenile Justice Board; CWC—Child Welfare Committee; SJPU—Special Juvenile Police Unit)
A few of the policies prevalent in India are outlined as follows:[37,46]
-
Constitutional Measures:[38,47]
-
Article 21 A: Compulsory education for all from the age of 6–14. This was subsequently extended by the Right to Education Act 2010 (RTE), which endorses compulsory education and freedom from examinations till the age of 14 years. Some states have extended this to 18 years for the girl child.
Education is a fundamental right for all children, and both access to and provision for the same are state mandates. Improved quality of life has been evidenced by better education.[39,40,48,49]
In addition, Article 45 states that the State will endeavor to provide free education till the age of 6 years for all Indian citizens.
Article 24: No child below the age of 14 years shall be employed in for work. This was particularly important in areas where children were employed in dangerous places, such as firework factories. This article led to the Child Labour (Prohibition and Regulation) Act 1986, which clearly outlines offenses, protection, and surveillance through a committee and strict enforcement.
Article 39(f): Safeguards provisions for healthy growth and development through opportunities for children. It also safeguards against exploitation and moral abandonment. This article led to the formation of the Immoral Trafficking (Prevention) Act (ITPA), 1956, which has very stringent measures against child prostitution and trafficking.
-
-
Legislations pertaining to children and adolescents:
Hindu Adoptions and Maintenance Act 1956: It is applicable for Hindu undivided families to ensure that care and maintenance of both girl and boy children are equal. Before this act, girls could not be adopted. Today, all adoptions are mandated to be regulated under the Central Adoption Resource Agency (CARA).
The Pre-Conception and Pre-Natal Diagnostic Techniques Act 1994: It prohibits prenatal gender determination as a measure against female infanticide, making gender determination a cognizable offense.
The Prohibition of Child Marriage Act 2006: It defines the age of marriage as 18 for girls and 21 for boys, and anything below this is punishable under the act. This prevents child marriages and safeguards the welfare of children.
The Juvenile Justice Act 2000 and Amendment Act 2006 (JJ Act): It adopts a child-centric way of dealing with children and adolescents in conflict with the law. Special courts and judges are appointed for the same.
Protection of Children from Sexual Offences Act 2012 (POCSO): It has a special police force, special protocols for medical examinations, and special courts, to penalize offenders with stringent measures and punishments for the same.
Rights of Persons with Disabilities Act (2016): This provides children with concessions at the school and college level, along with reservations for disabled individuals. This is in keeping with the United Nations Charter for Persons with Disabilities. Another unique scheme created by the government is the Unique Disability ID (UDID) for these individuals, which is valid throughout the country.
-
Child Welfare Measures
The Integrated Child Development Scheme (ICDS): This is a scheme that focuses on the overall development of the child below 6 years of age with regard to nutrition, physical health, psychological health, and education. This scheme has achieved great penetration among Anganwadi workers throughout the country. Subsequently, Kishori Shakti Yojana is an adolescent girl's scheme, which focuses on the emotional health and development of adolescent girls.
-
Childline 1098, 1996, is a 24x7, toll-free child helpline started by a nongovernmental organization (NGO) under the Ministry for Women and Child Development, where anonymous help can be sought and attended to by children in distress. It is active in 598 districts in India.
In special conditions, children who are homeless and street orphans, are to be protected and taken care off by the state under the The Homeless Orphan and Street Children (Rehabilitation and Welfare Bill, 2008)[50]
-
Framework for Child Welfare and Protection
The other ministries involved are the Home Ministry, which deals with all legal matters and crime; the Ministry of Labour, which deals with labor laws; and the Ministry of Human Resources and Development, which decides policies related to education.
In special conditions, children who are homeless and street orphans are to be protected and taken care of by the state under the Homeless Orphan and Street Children (Rehabilitation and Welfare Bill, 2008).
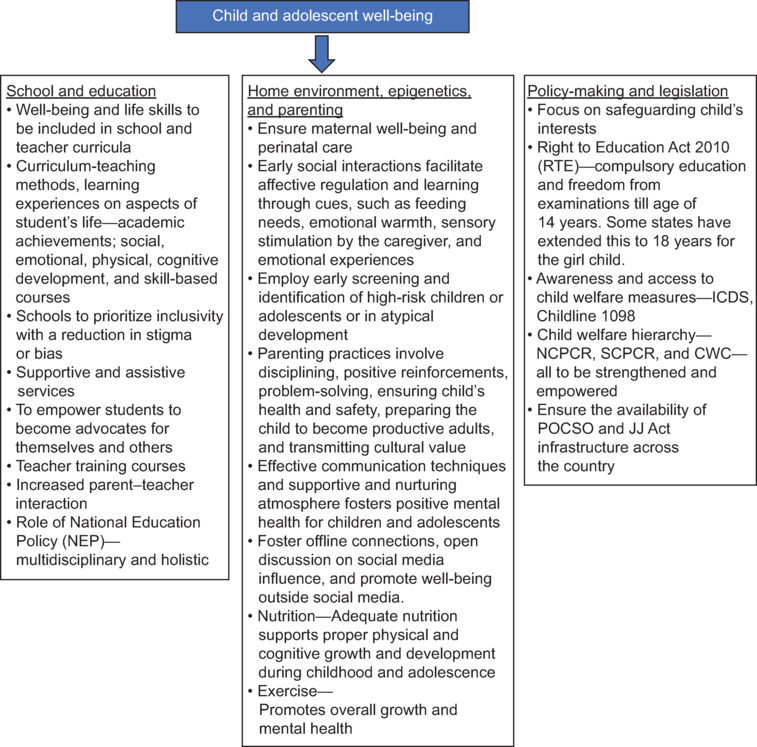
OVERVIEW OF APPROACH TO CHILD WELL-BEING AND MENTAL HEALTH
RECOMMENDATIONS
Do's
Ensure maternal well-being and a safe pregnancy
Have policies in place for environmental control
Adopt a holistic education policy
Early screening and identification of high-risk individuals—checklist for typical development
Make access to and awareness of children in distress easy.
Don'ts
Equate antenatal women with others and give deadlines, additional work stress
Have educational policies and measures that are academically loaded and stressful
Invest only in secondary and tertiary medical care
Have a huge differential between children and adolescents from privileged homes versus those from not-so-privileged homes
Ignore minority populations, such as children in orphanages or residential care, adopted children, and nonbinary-gendered children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Riccio CA, Sun LH, Gonzalez A. Understanding Typical and Atypical Neurodevelopment in Children and Adults. Understanding the Biological Basis of Behavior: Developing Evidence-Based Interventions for Clinical, Counseling and School Psychologists. 2021:71–106. [Google Scholar]
- 2.Semrud-Clikeman M. Understanding the development of the central nervous system and its relationship to clinical practice. Understanding the Biological Basis of Behavior: Developing Evidence-Based Interventions for Clinical, Counseling and School Psychologists. 2021:31–52. [Google Scholar]
- 3.Malik F, Marwaha R. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2023. Developmental Stages of Social Emotional Development in Children. 2022 Sep 18. [PubMed] [Google Scholar]
- 4.Champagne F. The Cambridge handbook of infant development: Brain, Behaviour and Cultural Context 2020 Cambridge University press; 2020. Dynamic Epigenetic Impact of the Environment on the Developing brain. In Lockman JJ, Tamis – LeMonda CS, editors; pp. 70–93. [Google Scholar]
- 5.Murgatroyd C, Spengler D. Epigenetics of early child development. Front Psychiatry. 2011;2:16. doi: 10.3389/fpsyt.2011.00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jensen Peña CL, Champagne FA. Epigenetic and neurodevelopmental perspectives on variation in parenting behavior. Parenting. 2012;12:202–11. doi: 10.1080/15295192.2012.683358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sahithya BR, Manohari SM, Vijaya R. Parenting styles and its impact on children–a cross cultural review with a focus on India. Mental Health, Religion & Culture. 2019;22:357–83. [Google Scholar]
- 8.Encyclopedia of Psychology. Available from: https://www.apa.org/topics/parenting. [Last accessed on 2020 Aug 12] [Google Scholar]
- 9.Kuppens S, Ceulemans E. Parenting styles: A closer look at a well-known concept. J Child Fam Stud. 2019 Jan 15;28:168–81. doi: 10.1007/s10826-018-1242-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Holdsworth EA, Schell LM, Appleton AA. Maternal–infant interaction quality is associated with child NR3C1 CpG site methylation at 7 years of age. American J Human Biol. 2023;35:e23876. doi: 10.1002/ajhb.23876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lomanowska AM, Boivin M, Hertzman C, Fleming AS. Parenting begets parenting: A neurobiological perspective on early adversity and the transmission of parenting styles across generations. Neurosci. 2017;342:120–139. doi: 10.1016/j.neuroscience.2015.09.029. [DOI] [PubMed] [Google Scholar]
- 12.Belsky J, Jaffee SR, Sligo J, Woodward L, Silva PA. Intergenerational transmission of warm-sensitive-stimulating parenting: a prospective study of mothers and fathers of 3-year-olds. Child Dev. 2005;76:384–96. doi: 10.1111/j.1467-8624.2005.00852.x. [DOI] [PubMed] [Google Scholar]
- 13.Neely-Barnes SL. and Dia DA. Families of children with disabilities: A review of literature and recommendations for interventions. 2008:93. [Google Scholar]
- 14.Garner RE, Arim RG, Kohen DE, Lach LM, MacKenzie MJ, Brehaut JC, Rosenbaum PL. Parenting children with neurodevelopmental disorders and/or behaviour problems. Child: care, Health Develop. 2013;39:412–21. doi: 10.1111/j.1365-2214.2011.01347.x. [DOI] [PubMed] [Google Scholar]
- 15.Clauser P, Ding Y, Chen EC, Cho SJ, Wang C, Hwang J. Parenting styles, parenting stress, and behavioral outcomes in children with autism. School Psychol Inte. 2021;42:33–56. [Google Scholar]
- 16.Hannon MD. Supporting Siblings of Children with Disabilities in the School Setting: Implications and Considerations for School Counselors. Journal of School Counseling. 2012;10:n13. [Google Scholar]
- 17. Available from: https://www.unicef.org/parenting/child-care/9-tips-for-better-communication. [Last accessed on 2023 Jul 20] [Google Scholar]
- 18.Henderson N. The Social Ecology of Resilience: A Handbook of Theory and Practice. New York, NY: Springer New York; 2011. Resilience in schools and curriculum design; pp. 297–306. [Google Scholar]
- 19.Bharath S, Kumar KK. Health promotion using life skills education approach for adolescents in schools-development of a model. Journal of Indian Association for Child and Adolescent Mental Health. 2008;4:5–11. [Google Scholar]
- 20.Josefsson J, Wall J. Empowered inclusion: Theorizing global justice for children and youth. Globalizations. 2020;17:1043–60. [Google Scholar]
- 21.Glazzard J, Rose A. The impact of teacher well-being and mental health on pupil progress in primary schools. J Pub Ment Health. 2020;19:349–57. [Google Scholar]
- 22.Đorđević M, Glumbić N, Memisevic H, Brojčin B, Krstov A. Parent-teacher interactions, family stress, well-being, and parental depression as contributing factors to parental involvement mechanisms in education of children with autism. Int J Dev Disabil. 2022;68:838–49. doi: 10.1080/20473869.2021.1896962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yenugu S. The new National Education Policy (NEP) of India: will it be a paradigm shift in Indian higher education? Perspect Policy Pract Higher Educ. 2022;26:121–9. [Google Scholar]
- 24.Amerijckx G, Humblet PC. Child well-being: What does it mean? Children Society. 2014;28:404–15. [Google Scholar]
- 25.Bell SL, Audrey S, Gunnell D, Cooper A, Campbell R. The relationship between physical activity, mental wellbeing and symptoms of mental health disorder in adolescents: a cohort study. International Journal of Behavioral Nutrition and Physical Activity. 2019;16:1–2. doi: 10.1186/s12966-019-0901-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rafferty R, Breslin G, Brennan D, Hassan D. A systematic review of school-based physical activity interventions on children's wellbeing. Int Rev Sport Exercise Psychol. 2016;9:215–30. [Google Scholar]
- 27.Raghavan R, Alexandrova A. Toward a theory of child well-being. Soc Indicators Res. 2015;121:887–902. [Google Scholar]
- 28.Ageel HK, Harrad S, Abdallah MA. Occurrence, human exposure, and risk of microplastics in the indoor environment. Environ Sci Proc Impacts. 2022;24:17–31. doi: 10.1039/d1em00301a. [DOI] [PubMed] [Google Scholar]
- 29.Adams S, Savahl S. Children's discourses of natural spaces: Considerations for children's subjective well-being. Child Indicators Res. 2017;10:423–46. [Google Scholar]
- 30.Frenz P, Videla C. A public-health campaign to raise awareness of children's wellbeing with images drawn by children. The Lancet. 2005;366:1324–9. doi: 10.1016/S0140-6736(05)67532-0. [DOI] [PubMed] [Google Scholar]
- 31.Marques A, Demetriou Y, Tesler R, Gouveia ÉR, Peralta M, Matos MG. Healthy Lifestyle in Children and Adolescents and Its Association with Subjective Health Complaints: Findings from 37 Countries and Regions from the HBSC Study. Int J Environ Res Public Health. 2019;16:3292. doi: 10.3390/ijerph16183292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Prime H, Wade M, Browne DT. Risk and resilience in family well-being during the COVID-19 pandemic. Amer Psychol. 2020;75:631–9. doi: 10.1037/amp0000660. [DOI] [PubMed] [Google Scholar]
- 33.Giedd JN. The digital revolution and adolescent brain evolution. J Adolesc Health. 2012;51:101–5. doi: 10.1016/j.jadohealth.2012.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cruz JM, Torre AP, Castaños OL, Tus J. The Correlation Between Peer Pressure and Mental Well-Being Among Senior High School Students. Psychol Educ. 2022;2:167–75. [Google Scholar]
- 35.Goldscheider F, Bernhardt E, Lappegård T. The gender revolution: A framework for understanding changing family and demographic behavior. Population Dev Rev. 2015;41:207–39. [Google Scholar]
- 36.Ayala N, Edwards T, Patrick D. Michalos A(eds) Encylopedia of Quality of Life and Well- Being Research. Dordecht: Springer; 2014. Youth Quality of Life Instruments. [Google Scholar]
- 37.Landgraf JM. Encyclopedia of quality of life and well-being research. Cham: Springer International Publishing; 2020. Child health questionnaire (CHQ) pp. 1–6. [Google Scholar]
- 38.Maybery D, Steer S, Reupert A, Goodyear M. The kids coping scale. Stress and Health: J Int Soc Investigation of Stress. 2009;25:31–40. [Google Scholar]
- 39.Liddle I, Carter GF. Emotional and psychological well-being in children: the development and validation of the Stirling Children's Well-being Scale. Educational Psychol Practice. 2015;31:174–85. [Google Scholar]
- 40.Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychology and Psychiatry. 1997;38:581–6. doi: 10.1111/j.1469-7610.1997.tb01545.x. [DOI] [PubMed] [Google Scholar]
- 41.Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh mental well-being scale (WEMWBS): a Rasch analysis using data from the Scottish health education population survey. Health and quality of life outcomes. 2009;7:1–8. doi: 10.1186/1477-7525-7-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ngai SS, Cheung CK, Mo J, Wang L, Ng YH, Wang P. Career interventions and social well-being among non-engaged youth: Examining the mediating effects of career competency. Children and Youth Services Review. 2023;148:106903. [Google Scholar]
- 43.Mascherini M, Salvatore L, Meierkord A, Jungblut JM. NEETs-Young people not in employment, education or training: Characteristics, costs and policy responses in Europe. 2012. [Google Scholar]
- 44.Hayden SC, Ledwith KE. Career services in university external relations. New Directions for Student Services. 2014;2014:81–92. [Google Scholar]
- 45.Koçak O, Ak N, Erdem SS, Sinan M, Younis MZ, Erdoğan A. The role of family influence and academic satisfaction on career decision-making self-efficacy and happiness. Int J Environ Res Public Health. 2021;18:5919. doi: 10.3390/ijerph18115919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Satpathy C. Child Welfare Policies and Programmes in India. Yojana. 2012:23. [Google Scholar]
- 47.Constitution of India/India Code. Available from: http://www.indiacode.nic.in/bitstream/123456789/15240/1/constitution_of_india.pdf. [Last accessed on 2023 Jul 20] [Google Scholar]
- 48.Zhan Z, Su ZW, Chang HL. Education and Quality of Life: Does the Internet Matter in China? Frontiers in Public Health. 2022;10:860297. doi: 10.3389/fpubh.2022.860297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Javed S, Javed S, Khan A. Effect of education on quality of life and well being. Int J Indian Psychol. 2016;3:119–28. [Google Scholar]
- 50.The Homeless Orphan and street Children. 2008 Available from: http://164.100.47.4/billstexts/rsbilltexts/AsIntroduced/homless%20LIX%20of%2008.pdf. [Last accessed on 2023 Jul 20] [Google Scholar]