

INTRODUCTION
The fundamental drive behind most feelings, thoughts, and behavior is sexuality. Sexuality influences the way an individual projects himself psychologically and socially, and it is determined by genetic, anatomical, physiological, and other biological characteristics, as well as sociocultural factors. Interpersonal relationships and developmental experiences also shape individual sexuality in a significant way. Sexuality includes the gender identity of a person, internal sexual representations including private thoughts and fantasies as well as manifest behavior with self and others. Our sense of humor, way of dressing, and way of talking are all influenced by sexuality. Neuropsychologist Karl Pribram described four drives that motivate us to accomplish our goals. These drives included feeding, fighting, fleeing, and sex. Physical and psychological health essentially needs these drives. Hence, sex is a crucial aspect of life and sexual health is an important component of overall health. This has been realized by scholars in every field and texts and traditions of ancient origin in almost all cultures attempted to understand, explain, and value sexual knowledge in health and disease. However, sex and sexuality are still relatively less understood and less studied drives.[1]
The history of human sexuality is as ancient as human history. Artifacts from some of the ancient cultures are thought to be fertility totems. A Hindu epic Kama Sutra (400 BC–200 BC) describes love, pleasure, and desire. Torah, Quran, and Bible also have rules, advice, and stories about sex. Scientific studies on sexuality started only 150 years ago. Henry Havelock Ellis, a British physician, used case study methods to study sexuality scientifically.[2] He emphasized sexuality of homosexuals is different from transgenders. He also advocated equal sexual rights for women. Sigmund Freud, the father of Psychiatry, linked sex to healthy development and recognized sexuality throughout life. Alfred Kinsey who is recognized as the father of modern sexuality research believed that most sexual knowledge is guesswork and unbiased scientific literature about sexuality is scarce.[3,4] Although a lot of research studies have been conducted and attention has been given to sexuality in recent years, scientific information is still insufficient in several domains.
SEXUAL HEALTH
The term sex is used in several different ways in different contexts. Sex describes the means of biological reproduction. Sex also describes sexual organs both internal and external defining an individual as male or female. World Health Organisation[5] has defined sexual health as “a state of physical, emotional, mental, and social well-being related to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Human sexuality emerges in the body, but, like other human phenomena, it simultaneously unfolds in mental landscapes, social relations, and cultural spheres. Sexuality is closely linked to personal integrity, identity, body image, bonding, and social curiosity. Physiological and psychosocial determinants contribute significantly to sexual health.”
The mere absence of sexual dysfunction is not considered sexual health. The sexual health is often reflected as normal sexual behavior. The normal sexual behavior is defined as having experiences that are pleasurable for oneself and one's partner and may or may not involve sexual intercourse. The behavior is also free from guilt, compulsion, or distress. The concept of normal sexual behavior is also significantly influenced by social and cultural factors. Sexual health like any other health is multifactorial and contextual.[6] The core concepts related to sexual health are defined in Table 1, and Figure 1 elucidates the component of sexual well-being.
Table 1.
Core concepts related to sexual wellness
| Definition | |
|---|---|
| Sexual health | Sexual health is a state of physical, emotional, mental, and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction, or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination, and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected, and fulfilled.[5] |
| Sexuality | Sexuality is a central aspect of being human throughout life; it encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy, and reproduction. Sexuality is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. While sexuality can include all of these dimensions, not all of them are always experienced or expressed. Sexuality is influenced by the interaction of biological, psychological, social, economic, political, cultural, legal, historical, religious, and spiritual factors (WHO, 2015).[5] |
| Sexual well-being | Sexual well-being is broadly conceptualized as a concept consisting of amalgamation of sexual health, sexual pleasure, sexual quality of life, and sexual justice. |
Figure 1.
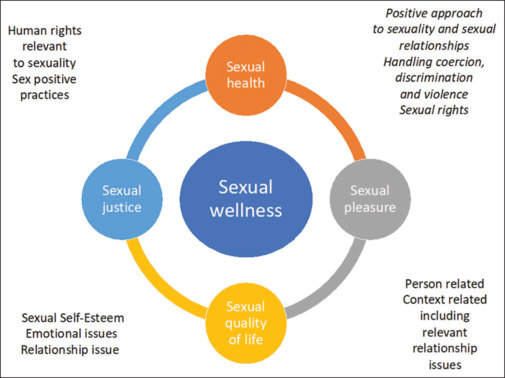
Components of sexual well-being
GENDER AND SEXUAL ORIENTATION
Gender represents the sociological and psychological representation of biological sex, which includes gender roles and gender identity. Although sex and gender are important aspects of a person's identity, it does not convey anything about orientation. Orientation refers to a person's sexual attraction to others. A person's capacity to have a sexual interest in others refers to sexual attraction. An individual must be comfortable with their sex role and chosen gender and accept themselves without guilt, shame, or fear and should be able to maintain good relationships with both sexes, regardless of whether they are intimate or platonic.[7] Gender equality includes concepts related to equal access to resources including material resources, such as money, clothes, books, etc., and non-material resources, such as love, care, and attention, as well as opportunities in education, occupation, economic pursuits, social acceptance, and decision making for their life. Gender sensitization is about providing information and strategy teaching in behavior modification regarding the adoption of gender equality in speech, behavior, and conduct. Provisions of appropriate information, sensitization, training of relevant stakeholders, and creating an enabling environment that is supportive of freedom of expression about one's orientation and gender identity are important aspects in improving sexual health promotion efforts.
ATTITUDE TOWARD SEX
Sexuality and general health are associated in diverse and intricate ways, and they can interact both in positive and negative ways. Culture plays a significant role in determining individuals' attitudes toward sexuality. Beliefs about normal and deviant sexual behavior are majorly influenced by culture. Concepts related to sexuality and gender are changing rapidly across the globe owing to rapid globalization and information technology advances, resulting in enhanced dissemination of information and ideas. Traditionally, cultures has been broadly classified as sex-negative and sex-positive cultures. India and the Asian subcontinent were considered sex-negative culture where sex was considered majorly for procreation. Western countries which were considered sex-positive culture considered sex beyond procreation.[8] The contemporary world is much more globalized and homogeneous, and previous concepts are only partially correct. However, consideration of sex as a taboo subject and the unavailability of sex education are still having much influence on the attitudes of people related to sexuality, especially in India.
MYTHS ABOUT SEXUALITY
A lot of myths and misconceptions prevail about sexuality. In women, myths, like sex is dirty, sex is sweat only during the second decade, having sex during menstruation is harmful, better sex with bigger breasts, women “no” always convey “yes,” orgasm is a must in all encounters, only vaginal and clitoral sex leads to orgasm, women never masturbate, and sexual desire decreases dramatically after menopause, are common and prevalent. Some of the common myths about male sexuality include erectile dysfunction is incurable, if a man does not get an erection by the mere sight of his partner implies that he is unable to perform, masturbation and nocturnal emission leads to impotence, and semen is a special type of cargo.[9] These myths and misconceptions do play an important role in influencing the sexual well-being of a large section of the population. This leads to sexual dissatisfaction, insecurities, and poor sexual interpersonal relationships in couples as well as impacts the presentation, symptomatology, course, and outcome of subjects with sexual dysfunctions. Hence, the provision of age-appropriate sex education addressing common myths and misconceptions can play an important role in handling sexual well-being at public health levels.
Inappropriate depiction of optimal sexuality in popular media and movies, like sex is instant, easy, and leading to amazing gratification, can create unrealistic expectations. Advertisement strategies for several products and services related to sexuality often disseminate wrong and exaggerated expectations of sexuality. Such advertisements are often promoted by individuals or corporations that benefit from the promotion of a sense of sexual inadequacy in public. The unregulated advertisement and inadequate modern medicine health service sector in sexual medicine are responsible for the continuation of several sexual myths and misconceptions in society.
PROMOTION OF SEXUAL WELL-BEING ACROSS AGES
Children and adolescents
Children and adolescents have unique needs for sexual health owing to their physical maturity, cognitive capabilities, and sociocultural factors. To become healthy adults with appropriate sexual functioning, children and adolescents would ideally need comprehensive education related to sexual and reproductive matters, freedom from any sexual coercion, and avoidance of inappropriate and premature exposure to sexual content. Aims of sexual well-being in children and adolescents include enabling them to make developmentally appropriate sexual choices, responsible sexual behavior at individual and community levels, and morally and socioculturally appropriate attitudes and outlook toward sexuality. Hence, policymakers and health professionals have always considered comprehensive sex education (CSE) as an important tool not only to promote sexual health and well-being but also the social, emotional health, and academic output of young individuals.
Studies have reported that implementation of CSE in school settings helps to improve understanding of gender and gender norms, more considerate attitude toward sexual diversity including LGBTQA (lesbian, gay, bisexual, transgender, queer, and asexual) population, improves knowledge and skills to handle healthy relationships, including reduction in interpersonal violence and dating, as well as having awareness and strategies to prevent child sexual abuse.[10]
Older people
Although it is widely believed that sex and sexuality are no longer important for older adults, several research studies reported contrary findings. Sexuality continues to be an important aspect of quality of life even in older adults. However, there is a wide variety of inter-individual diversity in the amount of importance given to sexuality in later life. Clinicians need to be aware of and acknowledge this variability along with offering advice, help, and treatment to those who are seeking help with sexual difficulties. The expression of sexuality in older adults is influenced by age-related limitations imposed by bodily functioning, medical factors, and sociocultural concepts of sexuality norms about older adults. Active sexual life has also been useful in helping with better mental and physical health, improving life span, strengthening relationships, and reducing stress and tension. Several strategies to promote healthy aging are also helpful in the promotion of sexuality in this population.
Following are the important approaches that can be helpful in having better sexual health in older adults.
Accepting and acknowledging age-related changes: Changes in sexual abilities in later life are inevitable. However, it does not necessarily lead to a reduction of enjoyment and pleasure in this activity. Many older adults can continue to enjoy sex in later life at a younger age or even better. Appreciating changes that come with aging is useful. Increasing age is one of the most important predictors of sexual dysfunctions in both genders. However, acknowledging and accepting age-related changes helps in developing skills to navigate around it and do necessary modifications. An enhanced focus on intimacy and physical touch is beneficial. Expanding the repertoire of sexual acts from intercourse to touching, kissing, massage, masturbation, or oral sex can be rewarding, if not already included. Keeping better physical health, having better sleep, regular exercise, and a healthy diet are other generally helpful approaches. It is useful to encourage interested older adults to seek medical help for issues related to sexuality influenced by medical conditions and medications.[11]
SEXUAL WELL-BEING
Gender rights
Sexual health also includes certain aspects of reproductive health, such as fertility control, prevention of sexually transmitted diseases (STDs), prevention and management of sexual violence, and having pleasurable sexual experiences free from violence. The achievement of sexual well-being is closely associated with people's human rights like the right to non-discrimination, the right to privacy and confidentiality, to be free from violence and coercion, and the right to education and information regarding sexual health services. Important bodies have been established to look into gender rights, which include the United Nations human rights treaty, the United Nations Special Rapporteur on the right to the highest attainable standard of health, among others. Harmonizing the laws related to sexuality with human rights standards helps in promoting sexual health. However, many laws have a negative impact on sexuality-related human rights, for example, restricting the access of adolescent girls to sexual health services can lead to unsafe abortion practices. Removal of legal and regulatory barriers to sexual health is an essential part of sexual well-being. As sexual health is related to the private lives of people, confidentiality and informed decision making is very important. For example, adolescents may not seek help in case permission is required from parents or legal guardians to access sexual health services. Access to information and education regarding sexual well-being has been strongly supported by international human rights associations. The ability to express one's gender freely and without any discrimination is an important part of health and sexual well-being. Sexuality-related violence does have a negative impact on health and well-being. An important aspect of laws related to sexual health is the definition of rape. Rape by husbands and issues related to transgender individuals need to be looked into to uphold the human rights of individuals.[5]
Human rights
Sexual health is strongly linked to the weightage given to the human rights of individuals. Sexual rights include human rights, many of which are already a part of national and international human rights associations.[12] The application of human rights to sexuality and sexual health constitutes sexual rights. The application of human rights to sexuality and sexual health constitutes sexual rights, which have been elaborated in Table 2.
Table 2.
Human rights important to uphold sexual health
| Rights | Description |
|---|---|
| The right to equality and non-discrimination | There should not be any distinction based on race, color, sex, language, religion, political opinions, place of residence, birth, property, disability, marital status, sexual orientation or gender identity, and economic or social position of the individual. |
| The right to life, liberty, autonomy, and security | These rights cannot be taken away for reasons related to sexuality, including sexual orientation, consensual sexual practice, or gender identity. |
| The right to bodily integrity | Everyone has the right to control and make decisions regarding their sexuality. This includes choices of sexual behavior and relationships with due regard to the rights of others. Free and informed decision-making by obtaining free and informed consent before an investigation or procedure related to sexual medicine is done. |
| The right to be free from torture and cruel, inhuman, or degrading treatment | Certain harmful traditional practices related to sexuality, gender identity, sexual orientation, forced sterilization, or abortion are to be avoided. |
| The right to privacy | All individuals have the right to withhold information related to their sexual practices, gender identity, sexual relationships, or sexual partners. |
| The right to the highest attainable standard of health and social security | Includes satisfying, safe, and pleasurable sexual health experiences. This requires access to quality health services and conditions that determine sexual health. |
| The right to marry with the free consent of the spouses, the right to equality, and the dissolution of marriage | Everyone has the right to choose whether to marry or not and enter into a marriage or relationship with free consent. All individuals will have equal rights while entering, during, and at dissolution of marriage. Also, there will be equal entitlements to social welfare and other benefits regardless of the type of relationship. |
| The right to decide the number and spacing of children | For exercising this right, access to the conditions that influence sexual health and reproductive health services is required. |
| The right to information and education | Everyone has the right to access correct scientific information related to sexuality, sexual health, law, and sexual rights. Everyone has the right to comprehensive sexuality education. |
| The right to freedom of thought, opinion, and expression | Every individual has the right to express their sexuality in terms of general appearance, communication, and behavior. |
| The right to an effective solution for violation of fundamental rights | Everyone has the right to access justice and redress for violation of their sexual rights. This requires adequate, accessible, and appropriate educative, legislative, and judicial measures. |
| The right to freedom of association and peaceful assembly | |
| The right to participation in public and private life | Free and effective participation in and contribution to civil, economic, social, cultural, and political aspects of human life at local, national, and international levels. |
SEXUAL WELL-BEING: RISK AWARENESS ABOUT STDS
More than one million sexually transmitted infections (STIs) are acquired daily. STIs can have serious consequences apart from the infection which they cause. They have a negative impact on sexual well-being, sexual health, and reproductive health of individuals. More than 500 million people aged 15-49 years suffer from genital herpes infection. HPV (human papilloma virus) is linked with 3,11,000 deaths each year due to cervical cancer. Hepatitis B virus led to approximately 8,20,000 deaths in 2019 mostly as a result of either cirrhosis or hepatocellular cancer.
Despite considerable efforts, change in behavior to prevent STIs is a challenge. Information and counseling can bring a positive change in individuals.
Lack of public awareness, lack of training among healthcare workers, and stigma related to STIs remain a barrier to timely and effective treatment.
People seeking health services for screening and treatment of STIs often face problems due to inadequate resources and poor quality of services.
The subgroup of populations with the highest rate of STIs includes sex workers and LGBTIQ (lesbian, gay, bisexual, transgender, intersex, and queer) individuals, and drug abusers and prisoners do not have access to adequate health services.
STI services are usually underfunded leading to inadequate manpower, resources, and infrastructure.
Within the framework of “Global health sector strategy on HIV, Hepatitis and STIs, 2022-2030” WHO has certain goals as briefed in Table 3.
Table 3.
Global health sector strategy on HIV, hepatitis, and STIs, 2022−2030: WHO
| a) Develop targets, lay down norms and standards for STIs prevention and management. |
| b) Support economic burden due to STIs and improve STIs surveillance. |
| c)) To foster research related to STIs including the development of diagnostic tests, vaccines, and effective treatment options. |
WHO supports all countries to:
Develop strategic plans and guidelines related to STIs;
Create a healthy environment where individuals can discuss STIs and seek treatment;
Primary prevention and integration of STI services with primary healthcare services;
Make STI care people-centred and adopt point-of-care tests;
Upgrade health interventions for STI surveillance in priority populations and management.
GENERAL PUBLIC HEALTH STRATEGIES TO PROMOTE SEXUAL WELL-BEING
Sexual well-being is important as a public health measure. However, there would be some resistance to considering sexual health as a public health measure, more so in traditional and conservative societies.[15] There might be limited resources to cater to the sexual health of individuals. Political resistance to considering sexual well-being as part of public health is likely to make things more difficult. In countries like the United Kingdom (UK), a holistic approach to sexual health is followed, which embraces the idea of sexual well-being.[13]
How sexual well-being is highly relevant to contemporary public health are elaborated in Table 4.
Table 4.
Relevance of sexual well-being to contemporary public health
| Variables | Description |
|---|---|
| (i)) Sexual well-being as a marker of health | Sexual well-being is a marker for population well-being. A positive approach toward population well-being helps in establishing achievable and measurable goals toward health equity. The inequities related to sexual health include racial, ethnic, or immigration-based discrimination, gender or sexual identity-based violence, and STIs, including HIV. A sexual well-being approach recognizes this discrimination across generations, which focuses on the needs of marginalized people. Hence, population-based health strategies need to be developed, which are anti-oppressive, intersectional, and culturally sound.[14,15] |
| (ii)) Sexual well-being as an indicator of well-being in the population | Population well-being is an ambitious goal of public health and sexual well-being is an important part of overall well-being. Sexual well-being gives us an important insight into holistic well-being across the lifespan. Data on sexual well-being will add to community engagement in health issues, address health (structural determinants) at the local level, and link local and larger public health policies related to reproductive and sexual health.[15,16] |
| (iii)) Sexual well-being as a marker of population trends | Sexual well-being incorporates population trends that are distinct from sexual health interventions. Sexual health is linked to well-being in the broader sense. For example, in a national survey done in France between 1970 and 2006, the proportion of people for whom ”sexual intercourse is important to feeling good” increased from 48% to 60% in females and 55% to 69% in males.[17] |
| (iv)) Sexual well-being helps in refocussing the practices of public health | Sexual well-being is an experience felt in the context of the surrounding environment.[18] Hence, it can be used for public health innovation strategies. Monitoring sexual well-being at the community level challenges the notion that sexuality requires privacy. Public health surveillance is there for sexual health and adding sexual well-being to it refocuses such surveillance. We should focus our resources on the population that is in greatest need and track individuals who enter and exit such policy programs. This approach requires that we redefine the relationship between community and public health to build trust and maintain privacy.[19] |
Sexual well-being is a distinct entity from sexual health and integration of both is essential for addressing sexual inequities. The conceptualization of sexual well-being is similar to sexual health and pleasure and socio-cultural and political frameworks of sexual justice. Inclusion of sexual well-being in sexual health is very much possible but would require an additional data-driven approach and certain objectives.
PROMOTING SEXUAL WELL-BEING IN HEALTHY COUPLES
Sexual well-being in a couple's context is one of the key aspects of a romantic relationship. Keeping physical intimacy and sexuality active in the relationship strengthens and enriches the relationship. There are several strategies for committed healthy couples to keep their sexual life robust. The key strategies are enlisted in Table 5.
Table 5.
Components of strategies for enhancements of optimal sexuality in context of partnered sexual activities
|
Important skills are enumerated below.
Communication: Good ongoing communication in couple relationships is an important aspect of maintaining good intimacy. Most couples find it difficult to talk about sex without hesitation. Discussions on sex-related topics may be influenced by shame, embarrassment, guilt, and feelings of hurt or resentment in one or both the members of the couple. Improving communication about sexuality can be very useful in this regard. Increasing spending quality time with one another helps in easing communication about sensitive and intimate issues. Expression of positive feelings, such as appreciation, respect, love, and approval, often and freely helps in developing an appropriate context for discussing other issues. Selecting an appropriate time for discussion related to sexuality is helpful. Avoid blame, mistake finding, and holding someone responsible for perceived or real difficulties. Using humor appropriately and sensitively is valuable.
Improving relationship strength: A strong and close relationship is the backbone of the good sexual well-being of the couple. Investing time, energy, and resources in improving intimacy is rewarding to the couple. Making active efforts to spend quality time together, making attempts to share hobbies and interests, or positively appreciating the hobbies of another partner if it is not shared. Sharing workload, having a fair distribution of responsibilities, and helping each other in daily chores can be another strategy to feel more connected, cared, and emotionally close. Making some extra efforts to keep the romance alive like bringing flowers without an important occasion, planning “date night” with partner alone, visiting places of mutual interest, cooking or bringing food of your partner's choice, making and giving love notes to each other unexpectedly are some of the strategies that can be considered according to taste on oneself and one's partner.
Sexual well-being is closely related to physical health and fitness: Regular physical exercise, especially cardiovascular exercise, is protective of sexual dysfunctions in both men and women.[20,21] Aerobic exercise has been reported to improve erectile dysfunction in a large systemic review report.[22] Similarly, physical exercise has been reported to improve sexual functioning in women, specifically in two groups, that is, women being treated by antidepressants and women who have undergone hysterectomy.[23] Several mindfulness based and cognitive strategies have proven efficacy in the management of sexual dysfunctions in both genders.[24] There are also indications that learning and utilizing the principles of these strategies can have a promotional impact on sexual functioning. Routinely practicing pelvic floor muscle exercise improves sexual fitness in both men and women.
Other general strategies: Smoking, alcohol, and other substances can impair sexual functioning and general health. Hence, it is not prudent to use them. Eating healthy food with lots of fresh fruits, vegetables, and a balanced diet is promotive of sexual health. Avoid high fat, high salt, and unhealthy dietary patterns. The dictum “use it or lose it” also applies to sexual well-being. Hence, maintaining regular sexual activity is useful for couples as a healthy aging strategy.
Improving sexual pleasure and interest: Bringing some novelty and variation in sexual domains by couples can keep sexual pleasure and interest high. Increasing the repertoire of sexual positions, additions of sexual toys if both partners agree and are comfortable with it, places, and timings can bring an element of newness to sexual activity and can be helpful in the enhancement of sexual well-being. Adding some safe, morally, and legally acceptable adventures, like new places, the addition of written or visual erotic material, sexual undergarments if the couple has not used them earlier, etc., can be incorporated if both partners are agreeable to the same.
Prevention of intimate partner violence (IPV): IPV is an important issue pertinent to sexual health. A higher prevalence of physical and sexual IPV is reported in South Asia (35% and 19%, respectively) in comparison to North America (25% and 6%, respectively) (WHO, 2021). In the Indian context, IPV remains an important public health issue. In India, women experiencing domestic violence have reported 41% and 30% lifetime and past 12 months' prevalence, respectively.[25] Physical violence, sexual violence, psychological aggression, controlling/coercive behaviors, stalking, etc., are common forms of IPV experienced by people. IPV is a significant risk factor for health conditions in general and sexual health in particular. Women experiencing IPV have more medical, gynecological, reproductive, and sexual health, as well as stress-related symptoms in comparison to controls. Strategies aimed at the reduction, identification, and handling of clients affected by IPV are important public health strategies for several health indicators, including sexual health.
SEXUAL WELL-BEING IN SPECIAL POPULATION
Mental health conditions
In patients suffering from psychiatric illnesses, such as schizophrenia, bipolar disorder, depression, or anxiety, just to name a few, the occurrence of sexual dysfunction is very high. Psychotropic medications often worsen sexual dysfunction. In severe mental illnesses, such as schizophrenia, sexual dysfunctions can occur as both, a part of the illness and also due to psychotropic medications.[26] In mood disorders, such as depression, the reported prevalence of sexual dysfunction is around 70-80%. Depression has an inverse relation with the sexual response cycle. Various neurotransmitters and pathways contribute to sexual dysfunctions in depression.[27] Anxiety disorders also have higher sexual dysfunctions. Premature ejaculation is more in patients suffering from anxiety disorders. Other anxiety disorders, such as social phobias, are also associated with decreased sexual satisfaction and sexual satisfaction.[28] Sexual dysfunction is more common in bipolar disorders. Factors such as the phase of the illness and medications used affect all the phases of the sexual response cycle.[29]
Substance abuse disorders
The mind-altering drugs in different cultures can be traced back thousands of years and the same holds good for drugs that could increase sexual functioning. The consumption of alcohol usually precedes sexual activity and is commonly believed to be an aphrodisiac. Alcohol consumption can indeed act as a disinhibitor, hence leading some people to be more receptive. This helps in the myth that alcohol can enhance sexuality. Acute effects can interfere with erection, lubrication, and orgasm. The mechanism of alcohol-induced sexual dysfunction is related to the hepatic catabolism of testosterone and its conversion, mediated by the enzyme aromatase. Tobacco, being a potent vasoconstrictor, can cause erectile dysfunction 1.5 times more than non-smokers. Cannabis use has a history of many centuries. Many marijuana users perceive it has a beneficial effect, but its impact on long-term use on sexuality is unclear. In the initial stages of opioid use, some patients experience an improvement in sexual function. Seventy-one percent of men and 60% of women report worsening of their sexual function. Another nervous stimulant drug cocaine appears to have two opposite effects on sexuality according to its acute and chronic abuse. The dopaminergic effect of cocaine can augment desire and arousal, but orgasm will be inhibited. Regular and long-term use of cocaine either through smoking/snorting/injecting has a significant negative impact on sexual functioning. Highly addictive drugs like amphetamine have gained a reputation for increasing sexual desire and orgasm. There have been reports that methamphetamine users participated in sexual activities that they did not when they were sober. There is a strong association between amphetamine use and high-risk sexual behavior. Ecstasy is believed to be a ”love drug,” though many people report an increase in sexual satisfaction, and cases of priapism have also been described. In the case of polydrug use, there is a possibility of unexpected and reciprocal interactions and also an association of illicit drugs with benzodiazepines. Benzodiazepines cause drowsiness, which in turn reduces desire, and also in certain doses, they can be disinhibitors and may increase libido. In the recent past, lay and scientific press has raised awareness of the involvement of licit and illicit drugs in the crime of ”date rape.” It is usually a combination of flunitrazepam, gamma-hydroxybutyrate, and ketamine. When mixed with alcohol (spiked drink), it produces disinhibition and lasting anterograde amnesia, making the victim an unreliable witness.[30] There is ambiguity about the causal association between drug use and high-risk sexual behavior. Some studies found that high-risk sexual behavior was neither entirely specific nor general with drug use, while others found an association between the decreased likelihood of condom use and drug abuse.
Cognitive impairment and sexuality
An older study, which was done on the elderly population without any impairment, showed that 33% of the population was involved in sexual activity, while 40% reported that they still had sexual interest. There are varied findings regarding the association between sexuality and cognitive functioning. A study done among menopausal women did not show any association between sexual functioning and cognitive decline. An Italian study showed subjects who continued sexual interest or activity had better cognitive functioning. Another study that found the prevalence of minimal cognitive impairment in the range of 3-20% found that only one-third of cognitively impaired individuals had sexual activity when compared to 62.3% of the healthy cognitive group. This study revealed minimal cognitive impairment and significantly impaired sexual functioning. The factors that contributed to the sexual decline in these individuals include organic, relational, and comorbid medical conditions. Organic changes include vasculopathy, neuropathy, a decrease in sex hormones, and erectile dysfunction.[31]
Relationship factors include bereavement and role transition from caregivers to the care receiver. Comorbid medical conditions include diabetes, hypertension, and depression. The use of prescribed medications, such as anticholinergics and antipsychotics, can cause impotence and impaired ejaculation. One of the studies reports the importance of abstract thinking in maintaining intact sexual relationships in cognitively impaired individuals. Sexual disinhibition is reported in around 7% of the reviewed literature.[9]
Sexual perspectives in the LGBTQ population
Historically gender identity was viewed as a deeply felt identification of being female or male. In the recent past, gender identity is seen as a spectrum where femaleness or maleness is part of a whole gamut of lesbian, gay, transgender, and queer. Transgender individuals have more body dissatisfaction and negative body image compared to cisgender individuals. Cisgender males have more frequent and intense sexual desire when compared to their female counterparts. Gender-affirming treatment decreases sexual desire predominantly among females, and the main culprit is hormonal therapy. In contrast, transgender males report increased sexual desire after the initiation of hormonal therapy. Low doses of phosphodiesterase inhibitors are required to maintain adequate arousal in transgender females with an intact penis. In transgender females with a neovagina, following erotic stimuli subjective arousal and subsequent vaginal activity and vaginal blood flow comparable to cisgender is observed. Satisfactory arousal is observed 6 months post-surgery. A large number of transgender females with vaginoplasty report satisfactory orgasms, but easier with masturbation than with partner sex. When compared to pre-surgery, orgasm is smoother, more pleasurable, and long-lasting. Interestingly, transgender females do report ejaculation with orgasm though the anatomical correlation is not clear.[32] Orgasm rates are less in transgender males when compared with transgender females. Orgasm rates range from 25% to 100% both in vaginoplasty and metoidioplasty. Fear of damaging the newer organ is common after gender-affirmative surgery, which may lead to muscle tension. Muscle tension may cause pain during coital activity, which in turn may lead to lower sexual satisfaction. Those who were sexually active before gender-affirmative surgery remained the same even after surgery. Gender-affirmative treatment has been shown to improve satisfaction with a partner.[33]
Neurodevelopmental disorders
Various environmental and genetic factors have increased the prevalence of neurodevelopmental disorders. Understanding sexual development and difficulties is an integral part of holistic care. Individuals with neurodevelopmental disorders are more influenced by sociocultural practices, belief systems, ethnic practices, and social stereotypes. Individuals with neurodevelopmental disorders are able to hold positive sexual identities and be aware of their sexual potential. Many studies have a persistent theme where these individuals distance themselves and show ambivalence toward their sexuality. On one hand, they are viewed by caregivers as needing protection from sex and they are “asexual,” while on the other hand, they are viewed as “hypersexual” behaving inappropriately. There is always an internal battle among the intellectually disabled as they are prevented to act on their desires. More are kept away from sexuality as a means of protection, which makes them inexperienced, dependable, and vulnerable. Sexual orientation in this group is seen as heterosexual by default. It is noteworthy that in high-functioning autism, higher rates of homosexual and bisexual orientation are in the range of 15-35% when compared with controls. They have inaccurate knowledge about sexuality, intimacy, and reproductive health.[34] Most of their concepts of sexuality are compromised by myths and need-based understanding. Many believe sex is aggressive and avoid it. Physical and developmental disability impacts sexual development, which in turn leads to lower self-esteem. Lower self-esteem further contributes to confusion about their sexual and reproductive abilities. Autistic individuals had less sexual knowledge and had difficulties in sexual experience. The majority of individuals with intellectual disability had a desire to be in intimate relationships. Being in a relationship made them happy, confident, and independent and also provided a sense of security. Many individuals express intimacy through kissing and hugging but do not engage in intercourse.[35]
People engaged in sex work
The commercial sex work and allied activities are criminal and severely restricted. The stigma, discrimination, and criminalization lead to limitations in the access of the care for sex workers due to fear of being denied for care, prosecution, arrest, and imprisonment. Even sex workers when access to health services do not disclose the complete information and hence receive inadequate treatments and follow-up. The sex workers' sexual health influences sexual health parameters of consumers and other affiliate persons in society. Availability of better access to education, service, and other provisions will help in promoting sexual wellness not only among sex workers but also other persons in the community.
LEGAL DETERMINANTS OF SEXUAL HEALTH
Legal mechanisms are crucial in introducing health intervention, protecting human rights, and guaranteeing the promotion, protection, and provision of sexual health information and services. Laws also help in preventing discrimination, alienation, and marginalization of people based on sexuality and gender. Legal statutes are necessary to combat archaic social positions on sexuality and to protect against bigotry and violence. A complete discussion of each topic is beyond the scope of the current guidelines. An overarching overview has been provided here.
Sexual abuse
Childhood sexual abuse (CSA) is a serious issue and is a significant concern for the promotion of health, in general, and sexual well-being, in particular, of individuals in society. CSA encompasses sexual harassment, commercial exploitation, sexual assault, penetrative sexual acts, non-penetrative sexual acts, and pornography among others. In addition to various adverse medical and social consequences in the immediate aftermath, CSA eventually results in adverse physical and mental long-term consequences if the environment is not conducive to healing. Developing a society that has a safe and healthy developmental environment that is free from sexual exploitation is mandatory for the healthy development of children and adolescents. Hence, the Protection of Children from Sexual Offences (POCSO) Act 2012 was passed in India.
Gender-based sexual violence
Rape, sexual assault, sexual harassment, and stalking are the important gender-based sexual violence reported. Prompt identification, reporting, legal remedies, and prevention of such events are prime factors in promoting the sexual well-being of the people in the country. Several related laws are made in India to safeguard persons vulnerable to gender-based sexual violence. The table further enumerates relevant laws related to this issue.
Homosexuality
Sexual minority people have several challenges in having sexual wellness owing to discrimination, stigma, lack of access to education, and access to health care. The relevant Indian laws are discussed in Table 6.
Table 6.
Important legal provision in relation to promoting sexual well-being in India
| Legal provisions | Brief description |
|---|---|
| The Protection of Children from Sexual Offences (POCSO) Act 2012 | This is an Act to protect children from sexual offenses, harassment, and pornography. It is a strong and empirical legal framework for the protection of children from sexual offenses. |
| The Sexual Harassment of Women at Workplace (Prevention, Prohibition and Redressal) Act, 2013 | An Act to provide protection against sexual harassment of women at the workplace and for the prevention and redressal of complaints of sexual harassment |
| Transgender Persons (Protection of Rights) Act, 2019 | An act of the Parliament of India with the objective of providing for the protection of the rights of transgender people, their welfare, and other related matters. |
| Invalidation of part of Section 377 of the Indian Penal Code | Decriminalization of sexual acts between same-sex persons |
| National Legal Services Authority v. Union of India (2014) | In 2014, the Supreme Court in this landmark case gave legal recognition to the ”third gender.” |
| National Medical Commission ban on conversion therapy | On August 25, 2022, National Medical Commission (NMC) designated conversion therapy as “professional misconduct” and authorized State Medical Councils to take disciplinary action if the guideline is broken |
Provisions of the Indian Penal Code
|
Defines rape and various related terminology Sexual harassment Forcing a woman to undress Watching or capturing images of a woman without her consent (voyeurism) Following a woman and contacting her or trying to contact her despite her saying she does not want contact. Monitoring a woman using the internet or any other form of electronic communication (stalking) |
COMPREHENSIVE SEXUAL EDUCATION
Sex education is defined as a broad program that aims to build a strong foundation for lifelong sexual health by acquiring information and attitudes, beliefs, and values about one's identity, relationships, and intimacy. CSE is essential in the development and promotion of sexual wellness of people. The sexual and reproductive health needs of children and adolescents are traditionally ignored in India. There are several cultural challenges in the wide availability and dissemination of sex education as sex is considered a taboo subject in India. It has been shown that the provision of CSE might result in multiple benefits to the recipients, including delayed initiation of sexual activity, a reduction in unplanned and early pregnancies and their associated complications, fewer unwanted children, reduced risks of sexual abuse, greater completion of education and later marriages, reduced recourse to abortion and the consequences of unsafe abortion, and a curb of the spread of STDs, including HIV.
Health services for people experiencing difficulties in sexual domain
The availability of good quality and accessible health services is an important aspect of maintaining sexual health promotion. The health services related to a sexual domain can be available in different sectors of health like medicine, gynecology, psychiatry, venerology, endocrinology, surgery, and plastic surgery. Services include identification and treatment of sexual disorders and dysfunctions, services for abortion, contraception, STI prevention, testing, and treatment. The provision of services should be easily accessible and practical for a wide range of service seekers, including people from sexual minority groups.
Mass media, information technology, entertainment industry, and sexuality
Sex and sexuality are a significant part of the discourse of mass media, information technology, and the entertainment industry. Sexuality and these industries affect each other in mutual ways. Although people of all ages are affected by information and depiction of sexuality in these media, children, and adolescents are possibly most influenced by it. A lot of information related to sexuality and sex is derived from media owing to the unavailability of reliable information from other trusted resources. Hence, there is a need to study the influences of these effects on persons in relation to sexual well-being. Strategies should be devised to limit inappropriate and excessive exposure to media and pornography in relation to sexuality on people, especially in children and adolescents. Specific therapeutic strategies to deal with adverse consequences due to inappropriate exposure to media should also be explicit and well-planned.
CONCLUSION
Promoting sexual well-being requires strategies aimed at various age groups and vulnerable populations. Human rights related to sexual health and gender-related sensitivities are important aspects of these approaches. Identifying the population who are vulnerable to sexual-related difficulties and exploitation are important prerequisites. A supporting framework consisting of appropriate educational facilities, legal provisions, and sex-positive health sector can help in disseminating and implementing these strategies wherever required. Table 7 summarizes the key recommendations for this paper.
Table 7.
General Recommendations for promotion of sexual well-being in various age groups and relevant population
| Group | Recommendations |
|---|---|
| Children and adolescents |
|
| Adults |
|
| Older adults |
|
| Sexual minority |
|
| Gender-related issues |
|
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Malacane M, Beckmeyer J. A review of parent-based barriers to parent–adolescent communication about sex and sexuality: Implications for sex and family educators. Am J Sex Educ. 2016;11:27–40. [Google Scholar]
- 2.Antón SC, Swisher CC III. Early dispersals of homo from Africa. Annual Rev Anthropol. 2004;33:271–96. [Google Scholar]
- 3.Freud S. New York: WW Norton and Co; 1923. The Ego and the Id. [Google Scholar]
- 4.Freud S. New York: Basic Books; 1905. Three Essays on the Theory of Sexuality. [Google Scholar]
- 5.World Health Organization. Geneva, Switzerland: WHO Press; 2015. Sexual health, human rights and the law. [Google Scholar]
- 6.Marshall DS, Suggs RC. New York: Basic Books; 1971. Human Sexual Behavior: Variations in the Ethnographic Spectrum. [Google Scholar]
- 7.Avasthi A, Rao TSS, Grover S, Biswas P, Kumar S. Clinical practice guidelines for management of sexual dysfuntions. In: Gautham S, , Avasthi A, , editors. Clinical Practice Guidelines for Management of Substance Abuse Disorders, Sexual Dysfunctions and Sleep Disorders. New Delhi: Indian Psychiatric Society; 2006. p. 144. [Google Scholar]
- 8.Bhugra D, DeSilva P. Sexual dysfunction across cultures. Int Rev Psychiatry. 1993;5:243–52. [Google Scholar]
- 9.Sathyanarayana Rao TS, Tandon A, Manohar S, Mathur S. Clinical practice guidelines for management of sexual disorders in elderly. Indian J Psychiatry. 2018;60(Suppl 3):S397–409. doi: 10.4103/0019-5545.224478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Goldfarb ES, Lieberman LD. Three decades of research: The case for comprehensive sex education. J Adolesc Health. 2021;68:13–27. doi: 10.1016/j.jadohealth.2020.07.036. [DOI] [PubMed] [Google Scholar]
- 11.Sinković M, Towler L. Sexual aging: A systematic review of qualitative research on the sexuality and sexual health of older adults. Qual Health Res. 2019;29:1239–54. doi: 10.1177/1049732318819834. [DOI] [PubMed] [Google Scholar]
- 12.The WAS (World Association for sexual health) Declaration of Sexual Rights. 13th World Congress of Sexology in Valencia, Spain. 1997 [Google Scholar]
- 13.Lorimer K, DeAmicis L, Dalrymple J, Frankis J, Jackson L, Lorgelly P, et al. A rapid review of sexual wellbeing definitions and measures: Should we now include sexual wellbeing freedom? J Sex Res. 2019;56:843–53. doi: 10.1080/00224499.2019.1635565. [DOI] [PubMed] [Google Scholar]
- 14.Prather C, Fuller TR, Jeffries WL, 4th, Marshall KJ, Howell AV, Belyue-Umole A, et al. Racism, African American women, and their sexual and reproductive health: A review of historical and contemporary evidence and implications for health equity. Health Equity. 2018;2:249–59.. doi: 10.1089/heq.2017.0045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mitchell KR, Lewis R, O'Sullivan LF, Fortenberry JD. What is sexual wellbeing and why does it matter for public health? Lancet Public Health. 2021;6:e608–13.. doi: 10.1016/S2468-2667(21)00099-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.La Placa V, Knight A. Well-being: Its influence and local impact on public health. Public Health. 2014;128:38–42.. doi: 10.1016/j.puhe.2013.09.017. [DOI] [PubMed] [Google Scholar]
- 17.Bajos N, Bozon M, Beltzer N, Laborde C, Andro A, Ferrand M, et al. Changes in sexual behaviours: From secular trends to public health policies. AIDS. 2010;24:1185–91.. doi: 10.1097/QAD.0b013e328336ad52. [DOI] [PubMed] [Google Scholar]
- 18.Dooris M, Farrier A, Froggett L. Wellbeing: The challenge of ‘operationalising’ an holistic concept within a reductionist public health programme. Perspect Public Health. 2018;138:93–9.. doi: 10.1177/1757913917711204. [DOI] [PubMed] [Google Scholar]
- 19.Haley DF, Matthews SA, Cooper HLF, Haardörfer R, Adimora AA, Wingood GM, et al. Confidentiality considerations for use of social-spatial data on the social determinants of health: Sexual and reproductive health case study. Soc Sci Med. 2016;166:49–56.. doi: 10.1016/j.socscimed.2016.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fergus KB, Gaither TW, Baradaran N, Glidden DV, Cohen AJ, Breyer BN. Exercise improves self-reported sexual function among physically active adults. J Sex Med. 2019;16:1236–45. doi: 10.1016/j.jsxm.2019.04.020. [DOI] [PubMed] [Google Scholar]
- 21.Hossini RN, Norouzi E, Yousefi M, Masrour FF, Ahmadi A. Aerobic exercise and resistance training to improve sexual health and emotional problems of obese women. Trends Psychol. 2022:1–20. [Google Scholar]
- 22.Silva AB, Sousa N, Azevedo LF, Martins C. Physical activity and exercise for erectile dysfunction: Systematic review and meta-analysis. Br J Sports Med. 2017;51:1419–24. doi: 10.1136/bjsports-2016-096418. [DOI] [PubMed] [Google Scholar]
- 23.Stanton AM, Handy AB, Meston CM. The effects of exercise on sexual function in women. Sex Med Rev. 2018;6:548–57. doi: 10.1016/j.sxmr.2018.02.004. [DOI] [PubMed] [Google Scholar]
- 24.Jaderek I, Lew-Starowicz M. A systematic review on mindfulness meditation–based interventions for sexual dysfunctions. J Sex Med. 2019;16:1581–96. doi: 10.1016/j.jsxm.2019.07.019. [DOI] [PubMed] [Google Scholar]
- 25.Kalokhe A, del Rio C, Dunkle K, Stephenson R, Metheny N, Paranjape A, et al. Domestic violence against women in India: A systematic review of a decade of quantitative studies. Glob Public Health. 2017;12:498–513.. doi: 10.1080/17441692.2015.1119293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dossenbach M, Dyachkova Y, Pirildar S, Anders M, Khalil A, Araszkiewicz A, et al. Effects of atypical and typical antipsychotic treatments on sexual function in patients with schizophrenia: 12-month results from the Intercontinental Schizophrenia Outpatient Health Outcomes (IC-SOHO) study. Eur Psychiatry. 2006;21:251–8. doi: 10.1016/j.eurpsy.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 27.Clayton AH, El Haddad S, Iluonakhamhe JP, Ponce Martinez C, Schuck AE. Sexual dysfunction associated with major depressive disorder and antidepressant treatment. Expert Opin Drug Saf. 2014;13:1361–74.. doi: 10.1517/14740338.2014.951324. [DOI] [PubMed] [Google Scholar]
- 28.Figueira I, Possidente E, Marques C, Hayes K. Sexual dysfunction: A neglected complication of panic disorder and social phobia. Arch Sex Behav. 2001;30:369–77.. doi: 10.1023/a:1010257214859. [DOI] [PubMed] [Google Scholar]
- 29.Downey J, Friedman RC, Haase E, Goldenberg D, Bell R, Edsall S. Comparison of sexual experience and behavior between bipolar outpatients and outpatients without mood disorders. Psychiatry J. 2016;2016:5839181. doi: 10.1155/2016/5839181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Palha AP, Esteves M. Drugs of abuse and sexual functioning. Adv Psychosom Med. 2008;29:131–49. doi: 10.1159/000126628. [DOI] [PubMed] [Google Scholar]
- 31.Momtaz YA, Hamid TA, Ibrahim R. The impact of mild cognitive impairment on sexual activity. Am J Alzheimer's Dis Other Demen. 2013;28:759–62. doi: 10.1177/1533317513504612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Holmberg M, Arver S, Dhejne C. Supporting sexuality and improving sexual function in transgender persons. Nat Rev Urol. 2019;16:121–39. doi: 10.1038/s41585-018-0108-8. [DOI] [PubMed] [Google Scholar]
- 33.Lawrence AA. Sexuality before and after male-to-female sex reassignment surgery. Arch Sex Behav. 2005;34:147–66.. doi: 10.1007/s10508-005-1793-y. [DOI] [PubMed] [Google Scholar]
- 34.Löfgren-Mårtenson L. The Invisibility of young homosexual women and men with intellectual disabilities. Sex Disabil. 2009;27:21–6.. [Google Scholar]
- 35.Whittle C, Butler C. Sexuality in the lives of people with intellectual disabilities: A meta-ethnographic synthesis of qualitative studies. Res Dev Disabil. 2018;75:68–81. doi: 10.1016/j.ridd.2018.02.008. [DOI] [PubMed] [Google Scholar]