

INTRODUCTION
Previously, the concept of mental health was seen through the lens of the presence or absence of mental illness. Later, ideas and theories have proven mental health to encompass more aspects. The World Health Organization (WHO) has defined mental health as “a state of well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community.” It is an integral component of health and well-being that underpins our individual and collective abilities to make decisions, build relationships, and shape the world we live in. In recent times, the concept of positive psychology has focused more on aspects of mental health beyond recovery from illness—such as positive experiences and positive aspects of life, such as gratitude, love, social relations, humor, and resilience.
Resilience is “the ability and the capacity of a person to adapt well in the face of adversity, trauma, tragedy, threats, or even significant sources of stress.” It is a dynamic process in which biological, psychological, social, and environmental factors enable an individual to regulate their mental health despite exposure to adversity at any period of life; that is, resilience can be acquired by anyone at any time.[1,2]
Even though resilience can be acquired, many biological and psychosocial factors contribute to it in an individual—either positively or negatively. Among these, the psychosocial factors are shown in Table 1.[3]
Table 1.
Attributing factors for resilience
| Positive attributing factors | Negative attributing factors |
|---|---|
| - Secure attachment and bonding - Intelligence - Social skills - Good physical health - Easily adaptable temperamental traits - Socially approachable - Appearance and self-awareness - Optimism and a sense of humor - Productivity - Purposeful and organized - Compartmentalization - Recreation - Cognitive flexibility - Active coping |
- Poor perinatal care - Adversities in childhood - Dysfunctional family dynamics - Psychopathology in parents - Poor schooling - Absence of role models or mentors - Culture of violence - Wars and natural disasters |
Biological factors that have a role in contributing to the resilience response in a person include polymorphisms seen in genes, such as
Neuropeptide Y (NPY) gene
Corticotropin-releasing hormone (CRH) receptor 1 (CRHR1) gene
Catechol-O-methyltransferase gene (COMT)
Dopamine transporter gene (DAT1), dopamine receptor genes
Promoter region of the serotonin transporter gene (5-HTTLPR)
Serotonin receptor genes
Brain-derived neurotrophic factor gene (BDNF)
This influences resilience via the gene–environment interactions.[4] Apart from NPY, hypothalamic–pituitary–adrenal (HPA) axis, and serotonergic, dopaminergic, and noradrenergic systems, glutamate, gamma-aminobutyric acid (GABA), endocannabinoids have also been implicated in stress response and resilience. Epigenetics, including functional deoxyribonucleic acid (DNA) methylation, have also been implicated in the relationship between trauma and resilience.
It has been found that the dysregulated functioning of certain circuits results in low resilience phenotypes—making them more prone to the development of psychiatric illnesses. The implicated neural circuits include the following:
Mesolimbic dopamine pathway (reward circuit)
Neural circuit for fear (limbic system and prefrontal cortex)
Neural circuit for social behavior (prefrontal cortex, amygdala, nucleus accumbens, and insula).
Thus, there are various factors that influence resilience in an individual and therapies should target these factors during intervention and hence be suggested to be kept as we recommend the guidelines.
Emotional intelligence is “the ability to monitor feelings-both own and others, to understand and discriminate amongst them, and to use this information to guide one's thoughts and behaviour.[5]” It is usually understood and explored through the following domains:
Emotional perception
Emotion facilitation
Understanding of emotions
Emotional regulation
Emotional intelligence is involved in all aspects of life, and psychological disorders with high scores in emotional intelligence correlate with greater psychological well-being and improved social, occupational, and personal functioning.
Biologically, the amygdala, anterior insula, anterior cingulate cortex, and ventromedial prefrontal cortex have been found to play a role in emotional perception and subjective emotional experience. Emotional facilitation helps facilitate thoughts and behavior through empathy and prosocial behavior. The ventrolateral prefrontal cortex, insula, and temporoparietal junction have been found to be involved in this process. Cognitively speaking, the theory of mind gives some explanation about how the development of social and emotional abilities happens through childhood and beyond. Lastly, various interactions between the regions of the ventrolateral prefrontal cortex, ventromedial prefrontal cortex, and amygdala are responsible for successful emotional regulation in any individual.[6]
RELATION BETWEEN RESILIENCE AND EMOTIONAL INTELLIGENCE
Resilience and emotional intelligence have been found to be positively correlated with each other. People who have high levels of emotional intelligence perceive themselves to be more resilient, that is, more capable to cope with adversity and dealing with negative experiences. The specific domains of emotional intelligence also have individual effects on resilience. High levels of emotional perception and facilitation lead to individuals being aware of their emotions in stressful situations and adapting their behavior and thoughts to communicate in a prosocial manner. Understanding emotions will help improve empathy. This will help in strengthening social relations and support. Finally, people with good emotional regulation and control are more likely to respond to personal distress with a more positive affect and helpful coping skills. This improves resilience and helps people respond to life stresses without succumbing to them. Conversely, it has also been found that highly resilient people actively enhance their positive emotionality through altruism, humor, relaxation, and optimism, thus showing that emotional intelligence and resilience have a reciprocal relationship with each other [Figure 1].[7]
Figure 1.
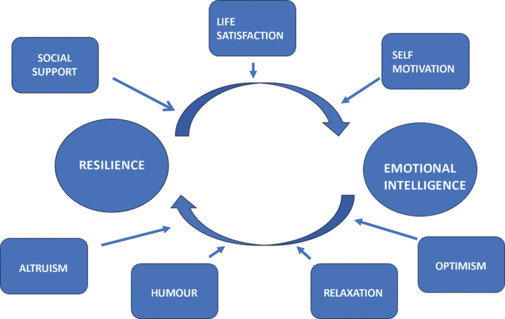
Association between resilience and emotional intelligence
Emotional intelligence helps individuals maintain optimistic feelings and deal with difficulties. Emotionally intelligent people also have high levels of self-motivation and a deeper sense of life satisfaction. Social support, self-motivation, and life satisfaction have been found to have an important mediating influence between emotional intelligence and resilience.[8]
Several studies have been conducted regarding resilience and emotional intelligence in students, war veterans, people in regions of natural and manmade disasters, etc., as they have been exposed to either high levels of stress or severe adversity [Table 2]. Most recently, studies have been performed with coronavirus disease 2019 (COVID-19) as a backdrop in various populations and their resilience and coping skills.
Table 2.
Association of resilience with emotional intelligence and other factors
| Study | Population | Findings |
|---|---|---|
| Sarrionandia et al.[9] | Students | Better resilience and emotional intelligence presented with lower perceived stress |
| Pietrzak et al.[10] | Veterans | Those with lower social support had increased PTSD and depressive symptoms, decreased resilience, and poorer psychosocial functioning |
| Shoshani and Slone[11] | Adolescents in war-torn area | Higher resilience was negatively associated with the development of psychiatric disorders |
| Li et al.[12] | General population during COVID-19 | Higher resilience was positively correlated with better mental health, and social support had the role of a buffer against the negative impact of low resilience on mental health |
Sarrionandia et al.[9] have conducted a study on undergraduate students in two different countries and found that irrespective of region, students with better resilience and emotional intelligence present with lower perceived stress. They highlighted the need for intervention programs that improve both resilience and intelligence and could be helpful to mitigate the high amounts of stress faced by the student populations.
Pietrzak et al.[10] surveyed 272 veterans and found that resilience had a role in mediating the association between unit support and the development of posttraumatic stress disorder (PTSD) and depression; even post-deployment social support played a role. Those with lower unit or social support had increased PTSD and depressive symptoms and decreased resilience and poor psychosocial functioning.
Evidence often supports the dose–response effect between traumatic exposures and mental health; that is, the greater the exposure, the higher the psychological problems. This is seen at all ages. For example, in a study conducted by Shoshani and Slone,[11] on 1078 adolescents aged between 13 and 15 years, they focused on assessing the individual's character strengths and virtues as factors for resilience. They found that higher resilience via interpersonal, temperance, and transcendence strengths was negatively associated with the development of psychiatric symptoms.
COVID-19 presented an unprecedented challenge to the whole of mankind. It presented us with adverse situations and brought many changes to how people live in the face of social isolation and an uncertain future. Li et al.[12] studied the effects of sources of social support and resilience on the mental health of 23192 individuals of different age groups. This study found a positive association of resilience with better mental health, and social support as a buffer against the negative impact of low resilience on mental health.
However, most of the studies have found that many people who have been exposed to traumatic events do not develop psychiatric disorders or psychological problems. For example, lifetime exposure incidence to trauma in the general population ranged from 50% to 80%. However, the development of psychiatric disorders, such as depression, anxiety, and PTSD, ranged from 7 to 15%.[13,14] This shows that even in the case of trauma, not everyone will develop an illness, and this could be due to various factors, among which the most predominant one is resilience.
TRANSCULTURAL ASPECTS OF RESILIENCE
Michael[15] in a multisite study on 1500 youths proposed a culturally and contextually embedded understanding of resilience, which influences the child's life, and suggested appropriate culture-sensitive interventions.[15]
Raghavan and Sandanapitchai[16] assessed 200 trauma-exposed adults from nineteen countries and found greater resilience and spirituality-based coping in the Asian group. Accordingly, they proposed a culturally specific predictors of resilience and the need for further work to explore these variables and culturally tailored interventions for trauma healing.[16]
ASSOCIATION OF RESILIENCE IN PSYCHIATRY
There is some evidence that people with mental illness might have lower resilience and that higher resilience levels may minimize the illness severity or even prevent the development of mental illness.
In bipolar disorder, it has been found that higher resilience levels lead to decreased impulsivity and depressive episodes. In patients with PTSD, it has been found that high levels of resilience are correlated with lower levels of development of PTSD. In these two illnesses, there is a reciprocal inverse relationship between impulsivity and resilience. It shows that to develop and enhance resilience is to improve the stability of mental health, especially in these two population subsets.[17]
Many studies have been conducted to understand the importance of the role of resilience in the development and maintenance of PTSD. Low resilience levels and poor prosocial adaptive abilities are seen in people who are later susceptible to the development of PTSD after being exposed to trauma. They can also hinder recovery in these individuals.[18]
Resilience has been shown to have an attenuating role in suicidal ideation in anxious and depressed people. Positive thinking, social support, and optimism have been shown to be more common in highly resilient people, and thus, this leads to decreased suicidal ideation and attempts in people.[19]
In patients with chronic pain, high resilience has been shown to improve their social, occupational, and personal functioning despite continued adversity. Conversely, those with low resilience often perceive the pain to be debilitating and affecting their quality of life severely.[20]
Studies in children with autism spectrum disorders and attention deficit hyperactivity disorders found that harnessing and enhancing the resilience and emotional intelligence of these individuals might play a role in improving the prognosis of these conditions.[21]
In people with eating disorders, it has been found that highly resilient individuals have a better recovery as compared to those with low resilience levels.[22]
SCHOOL-BASED RESILIENCE BUILDING PROGRAMS: INSIGHT AND EFFECTIVENESS
Child and youth resilience-based initiatives have focused on the identification and inculcation of protective factors and understanding and implementation of individual resilience strengths and adaptation processes.
A thorough understanding of resilience factors, strengths, attitudes, and connections of individuals who engage in bullying is vitally important. To address the risk of bullying and their behavioral issues, strength-based resilience-building approach by parents, educators, peer groups, and society has shown promising results through collaborative strategies.[23]
Pinto et al.[24] in a systematic review and meta-analysis of 13 randomized controlled trials (RCTs) on resilience programs in children and adolescents reported a moderate effect of the programs in promoting resilience among adolescent students (standard mean differences [SMD] = 0.48), and some of these effects were sustained during the 6-month follow-up period (SMD = 0.12, P = 0.02).
Dray et al.[25] in a systematic review of universal resilience-focused interventions in children and adolescents reported a significant effect of these interventions on reducing depressive symptoms, internalizing problems, externalizing problems, and general psychological distress. Intervention trials were effective for anxiety symptoms and general psychological distress among children and for internalizing problems among adolescents. During the follow-up phase, resilience-focused interventions were effective for depressive and anxiety symptoms in the short term and for internalizing problems in the long term.
Fenwick-Smith et al.[26] in a systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs evaluated seven such programs and found a greater impact with teacher-led programs in schools, without having much bearing on the duration of the program. These programs had a positive impact on the primary school students' ability to manage day-to-day stress.
Joyce et al.[27] in a systematic review and meta-analysis of 11 RCTs on resilience training programs reported a moderate positive effect of resilience interventions (SMD = 0.44) with individual therapy being cognitive behavioral therapy (CBT)-based (SMD = 0.27), mindfulness (SMD = 0.46), and mixed (SMD = 0.51) interventions. The combination of CBT and mindfulness techniques was found to be most effective in building resilience.
ASSESSMENT OF RESILIENCE AND EMOTIONAL INTELLIGENCE IN CLINICAL PRACTICE
Scales of resilience in clinical practice
Resilience is a dynamic process with various factors playing a role in it—an attempt has been made to assess it in a cross-sectional manner using various scales. The following scales are suggested in Table 3.
Table 3.
Scales for assessment of resilience and emotional intelligence
| Scales | Item description and tool details |
|---|---|
| Resilience | |
| Connor-Davidson Resilience Scale (CD-RISC)[28] |
One of the most common scales used in studies. Three tools available—2-item, 10-item, and 25-item tools. Adaptation and validation performed in the Indian population |
| Resilience Scale[29] | 25-item tool Abbreviated version—14-, 11-, and 5-item scale Completed in 5–7 min Adaptation and validation performed in the Indian population |
| Resilience Scale for Adults (RSA)[30] | 45- and 33-item scale Subscales: personal competence, social competence, personal structure, family coherence, social support |
| Brief Resilience Scale (BRS)[31] | 6-item scale Commonly used in research |
| Resilience Scale for Adolescents (READ)[32] | 39-item scale for adolescents Developed from the 41-item Resilience Scale for Adults |
| Resiliency Scales for Children and Adolescents (RSCA)[33] | 64-item scale For 9–18 years of age group |
| Emotional Intelligence | |
| Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT)[34] | 141-item scale takes 30–45 minutes Used in corporate, educational, research, and therapeutic settings Measures four aspects: accurately identifying emotions of people and symbolizing by objects in pictures, using emotions and solve problems with these emotions, understanding the causes of emotion, and being open to emotions and fuse emotions with thinking |
| Bar-On Emotional Quotient Inventory (EQ-i)[35] | EQ-i contains 35 items to assess four broad dimensions of Bar-On’s EI model: intrapersonal, interpersonal, adaptability, and stress management. EQ-i: S (short form) contains 10 items |
| Emotional Intelligence Scale (Yadav, 2017)[36] | 32 items of scale represent four dimensions or constructs Adaptation and validation performed in the Indian population |
These scales will help us to understand how resilient an individual is and what are the factors influencing resilience in that individual, across all ages, which will help in planning out interventions. These scales usually have items about how a person can adapt to change, how much can they handle being under pressure, whether they can bounce back after a hardship, etc.
Scales used for measuring emotional intelligence
These scales measure the ability of an individual to perceive, understand, and manage and regulate their emotions and also those of others (also suggested in Table 3).
GENERAL RECOMMENDATIONS TO INCORPORATE STRATEGIES FOR RESILIENCE BUILDING AND EMOTIONAL INTELLIGENCE THROUGHOUT THE LIFESPAN
Resilience, as mentioned, has been implicated in the development and maintenance of an illness. As detailed below, these measures can be used as a resource at any point in the lifespan, with more emphasis on children and adolescents.[37]
Children
Before the development of any illness, resilience training can be used—either as part of primary prevention universally or in selected high-risk populations, such as those children with childhood adversities or in war-torn areas.
Children need to have the following strengths to become resilient:
External resources that provide security and safety—these develop trust in others and the ability to make friends
Personal attitudes, feelings, and beliefs—that will help them bounce back from adversities. These include confidence in self, autonomy, and mastery of self
Social and interpersonal skills
Adolescents
The rates of emotional and behavioral problems in adolescents are increasing when seen longitudinally. We have to understand the biopsychosocial processes in adolescent development and use them to enhance resilience in them.
Adolescents should acquire and master the following strengths to build resilience:
Identity of self
Ability to prepare for adulthood with expectations for the future
Adults
Social support has been shown to be one of the most important factors that improve resilience in adults. Mature defenses have also been shown to be associated with the development of resilience. The following strengths need to be inculcated in adults:
Internal control
Self-esteem
Optimism
Coping strategies
Seeking emotional and social support.
Elderly
Research on aging populations shows us how resilience is a process that is both personal and environmental and how it continues through a person's lifespan.
The following strengths help inculcate resilience in the older individual.
Positive attitude
Counting one's blessings
Spirituality
Keeping oneself busy.
Other intervention strategies for building resilience and emotional intelligence
Intervention programs focusing on improving resilience need not be isolated in their approach.[3] Instead, they should be incorporated as part of any clinical and public health interventions. As resilience can be facilitated at any age, it should be part of
Early childhood intervention programs
School and college-based programs
Unemployment or workplace programs
Neighborhood-centered programs
Certain activity programs in the geriatric population
Resilient facilitation can be reinforced even through the process of a clinician taking a good history and establishing strong rapport. This will help in reinforcing positive attitudes and behaviors and thus improving social support and resilience.
Usual approaches in facilitating resilience include the following three approaches. These have been found to be effective at preventing and mitigating mental illness[15]:
Harm-reduction approach—which explains resilience as having a role in quick recovery after a time of stress, and this includes biological factors and genetic predispositions.
Protection approach—in the way an individual uses certain measures to maintain mental health (i.e. family, school, and friends).
Promotion approach—where the individual promptly uses resources to aid in mental health
Most of the current psychotherapeutic approaches have a basis in resilience facilitation, can also teach us to employ emotional intelligence in daily life, and can be used in resilience training for various psychiatric disorders and various age groups as well.
The following therapies use both resilience and emotional intelligence:
Cognitive behavioral therapy
Mindfulness-based therapy
Problem-solving therapy
Acceptance and commitment therapy.
Hence, it is recommended that as a guideline wherever there is a need to use emotional intelligence and to improve resilience in every distressed individual with psychological distress or psychiatric disorders, we suggest the above psychotherapies as an add-on to other recommended guidelines of the Indian Psychiatric Society (IPS).
Suggested methods
In most programs for resilience training in various psychiatric disorders, the following methods are used in clinical interview and therapy models, and hence, IPS Guidelines suggest to follow these techniques in one-to-one or group therapy settings.
Discussions
Practical exercises and assignments
Role plays
Exposure to mild stresses in a controlled environment
Problem-solving approaches
It is important to remember that the strengths and weaknesses of each individual are different from the others. The resilience training interventions should not have a blanket approach to the patients but instead individualize the therapy according to their resources and needs. Thus, we suggest the necessary caution and monitoring that need to be applied in the related psychiatric disorders where we need to improve resilience.
It has also been shown that treatment with antidepressants, such as sertraline, fluoxetine, and venlafaxine with psychosocial measures, has improved resilience in people suffering from depression and PTSD.[38] So, pharmacological treatment strategies also help improve the cognitive and social abilities of a person suffering from psychiatric illnesses. Hence, the comprehensive management of various psychiatric disorders should be followed as recommended by the IPS's clinical practice guidelines.
Tertiary prevention in psychiatry
Apart from having an attenuating role in the development of psychiatric illnesses, resilience and emotional intelligence have been shown to help improve the prognosis of the illness by aiding in recovery and having a preventive role in relapse.
Patients recovering from any illness have been found to have some amount of distress—whether due to the precipitating or perpetuating factors of the illness or the impact of the illness on their mental and physical health. Resilience is a part of the personal journey of the patients, and it aids in recovery. It consists of creating new personal strengths, making use of the social and emotional environment and support, identifying and expanding positive emotions and beliefs, and inculcating helpful coping skills even in the face of adversity.[2]
CONCLUSIONS
Resilience and emotional intelligence have a strong relationship with each other, often with the same factors playing a role in their development. Incorporating resilience and emotional intelligence in the treatment of psychiatric illnesses will help improve the prognosis of a patient. Resilience interventions are usually individualized and target different competencies and resources of an individual. These interventions help improve personal resilience, performance in all domains of life, and finally mental health. These guidelines are based on available evidence and are suggested to be used in various abovementioned conditions. Likewise, the increasing importance of both emotional intelligence improvement and increasing resilience through IPS guidelines and suggestions can further be considered new emerging evidence in other psychiatric disorders.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.American Psychological Association . Washington, DC: American Psychological Association; 2014. The road to resilience. Available from: http://www.apa.org/helpcenter/road-resilience.aspx. [Last accessed on 2023 Jul 05] [Google Scholar]
- 2.Echezarraga A, Las Hayas C, López de Arroyabe E, Jones SH. Resilience and recovery in the context of psychological disorders. J Humanist Psychol. 2019 doi: 10.1177/0022167819851623. [Google Scholar]
- 3.Levine S. Psychological and social aspects of resilience: A synthesis of risks and resources. Dialogues Clin Neurosci. 2003;5:273–80. doi: 10.31887/DCNS.2003.5.3/slevine. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wu G, Feder A, Cohen H, Kim JJ, Calderon S, Charney DS, et al. Understanding resilience. Front Behav Neurosci. 2013;7:10. doi: 10.3389/fnbeh.2013.00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Smith R, Killgore WDS, Alkozei A, Lane RD. A neuro-cognitive process model of emotional intelligence. Biol Psychol. 2018;139:131–51. doi: 10.1016/j.biopsycho.2018.10.012. [DOI] [PubMed] [Google Scholar]
- 6.Hogeveen J, Salvi C, Grafman J. ‘Emotional Intelligence’: Lessons from Lesions. Trends Neurosci. 2016;39:694–705. doi: 10.1016/j.tins.2016.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Magnano P, Craparo G, Paolillo A. Resilience and emotional intelligence: Which role in achievement motivation. Int J Psychol Res. 2016;9:9–20. [Google Scholar]
- 8.Armstrong AR, Galligan RF, Critchley CR. Emotional intelligence and psychological resilience to negative life events. Pers Indiv Differ. 2011;51:331–6. [Google Scholar]
- 9.Sarrionandia A, Ramos-Díaz E, Fernández-Lasarte O. Resilience as a mediator of emotional intelligence and perceived stress: A cross-country study. Front Psychol. 2018;9:2653. doi: 10.3389/fpsyg.2018.02653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pietrzak RH, Johnson DC, Goldstein MB, Malley JC, Southwick SM. Psychological resilience and postdeployment social support protect against traumatic stress and depressive symptoms in soldiers returning from Operations Enduring Freedom and Iraqi Freedom. Depress Anxiety. 2009;26:745–51. doi: 10.1002/da.20558. [DOI] [PubMed] [Google Scholar]
- 11.Shoshani A, Slone M. The resilience function of character strengths in the face of war and protracted conflict. Front Psychol. 2016;6:2006. doi: 10.3389/fpsyg.2015.02006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Li F, Luo S, Mu W, Li Y, Ye L, Zheng X, et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMC Psychiatry. 2021;21:16. doi: 10.1186/s12888-020-03012-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Do TTH, Correa-Velez I, Dunne MP. Trauma exposure and mental health problems among adults in central Vietnam: A randomized cross-sectional survey. Front Psychiatry. 2019;10:31. doi: 10.3389/fpsyt.2019.00031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.de Vries GJ, Olff M. The lifetime prevalence of traumatic events and posttraumatic stress disorder in the Netherlands. J Trauma Stress. 2009;22:259–67. doi: 10.1002/jts.20429. [DOI] [PubMed] [Google Scholar]
- 15.Michael U. Resilience across Cultures. Br J Soc Work. 2008;38:218–35. [Google Scholar]
- 16.Raghavan SS, Sandanapitchai P. Cultural predictors of resilience in a multinational sample of trauma survivors. Front Psychol. 2019;10:131. doi: 10.3389/fpsyg.2019.00131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shrivastava A, Desousa A. Resilience: A psychobiological construct for psychiatric disorders. Indian J Psychiatry. 2016;58:38–43. doi: 10.4103/0019-5545.174365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Snijders C, Pries LK, Sgammeglia N, Al Jowf G, Youssef NA, de Nijs L, et al. Resilience against traumatic stress: Current developments and future directions. Front Psychiatry. 2018;9:676. doi: 10.3389/fpsyt.2018.00676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sher L. Resilience as a focus of suicide research and prevention. Acta Psychiatr Scand. 2019;140:169–80. doi: 10.1111/acps.13059. [DOI] [PubMed] [Google Scholar]
- 20.Sturgeon JA, Zautra AJ. Resilience: A new paradigm for adaptation to chronic pain. Curr Pain Headache Rep. 2010;14:105–12. doi: 10.1007/s11916-010-0095-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Adaralegbe NJ, Okobi OE, O Omar ZT, Segun E, Evbayekha EO, Abolurin A, et al. Impact of adverse childhood experiences on resilience and school success in individuals with autism spectrum disorder and attention-deficit hyperactivity disorder. Cureus. 2022;14:e31907. doi: 10.7759/cureus.31907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Las Hayas C, Calvete E, Gómez del Barrio A, Beato L, Muñoz P, Padierna JÁ. Resilience Scale-25 Spanish version: Validation and assessment in eating disorders. Eat Behav. 2014;15:460–63. doi: 10.1016/j.eatbeh.2014.06.010. [DOI] [PubMed] [Google Scholar]
- 23.Donnon T, Hammond W. Understanding the relationship between resiliency and bullying in adolescence: An assessment of youth resiliency from five urban junior high schools. Child Adolesc Psychiatr Clin N Am. 2007;16:449–71. doi: 10.1016/j.chc.2006.11.007. xi. [DOI] [PubMed] [Google Scholar]
- 24.Pinto TM, Laurence PG, Macedo CR, Macedo EC. Resilience programs for children and adolescents: A systematic review and meta-analysis. Front Psychol. 2021;12:754115. doi: 10.3389/fpsyg.2021.754115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dray J, Bowman J, Campbell E, Freund M, Wolfenden L, Hodder RK, et al. Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. J Am Acad Child Adolesc Psychiatry. 2017;56:813–24. doi: 10.1016/j.jaac.2017.07.780. [DOI] [PubMed] [Google Scholar]
- 26.Fenwick-Smith A, Dahlberg EE, Thompson SC. Systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs. BMC Psychol. 2018;6:30. doi: 10.1186/s40359-018-0242-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Joyce S, Shand F, Tighe J, Laurent SJ, Bryant RA, Harvey SB. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open. 2018;8:e017858. doi: 10.1136/bmjopen-2017-017858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC) Depress Anxiety. 2003;18:76–82. doi: 10.1002/da.10113. [DOI] [PubMed] [Google Scholar]
- 29.Wagnild GM, Young HM. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas. 1993;1:165–78. [PubMed] [Google Scholar]
- 30.Friborg O, Hjemdal O, Rosenvinge JH, Martinussen M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int J Methods Psychiatr Res. 2003;12:65–76. doi: 10.1002/mpr.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: Assessing the ability to bounce back. Int J Behav Med. 2008;15:194–200. doi: 10.1080/10705500802222972. [DOI] [PubMed] [Google Scholar]
- 32.Hjemdal O, Friborg O, Stiles TC, Martinussen M, Rosenvinge JH. A new scale for adolescent resilience: Grasping the central protective resources behind healthy development. Meas Eval Couns Dev. 2006;39:84–96. [Google Scholar]
- 33.Prince-Embury S. The resiliency scales for children and adolescents, psychological symptoms, and clinical status in adolescents. Can J Sch Psychol. 2008;23:41–56. [Google Scholar]
- 34.Mayer JD, Salovey P, Caruso DR. Toronto, ON: MHS Publishers; 2002. Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) Item Booklet. [Google Scholar]
- 35.Bar-On R. Toronto, ON, Canada: Multi-Health System; 1997. Bar-On Emotional Quotient Inventory (EQ-i): Technical Manual. [Google Scholar]
- 36.Yadav P. Validation of emotional intelligence's scale in Indian context. Int J Eng Res Technol. 2017;5:1–5. [Google Scholar]
- 37.Shastri PC. Resilience: Building immunity in psychiatry. Indian J Psychiatry. 2013;55:224–34. doi: 10.4103/0019-5545.117134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sher L, Stanley BH, Posner K, Arendt M, Grunebaum MF, Neria Y, et al. Decreased suicidal ideation in depressed patients with or without comorbid posttraumatic stress disorder treated with selective serotonin reuptake inhibitors: An open study. Psychiatry Res. 2012;196:261–6. doi: 10.1016/j.psychres.2011.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]