

Summary
Although Japan's healthcare delivery system is highly regarded internationally, the COVID-19 pandemic has exposed its structural problems. Behind these issues lies a history of medical care provisions supported mainly by an unrestricted, "free labeling" system, and independently financed private hospitals. In addition, patients have a high degree of freedom of choice under the Japanese medical insurance system, making it difficult to provide comprehensive and continuous health management from initial diagnosis and treatment (primary care), specialized treatment, to supporting a return to home, providing nursing care and lifestyle support. As Japan becomes a "super-aged" society with individuals over 65 making up over 30% of the population, the nature of medical care will have to undergo major changes. Medical care's basic function must still be the treatment and cure of patients, but the system will also have to provide support. That means conceiving of care in a way that treats a person's life with dignity and does not sacrifice life for treatment. The implementation of a family doctor function and the clarification of the functions and roles of small and medium-sized community-based hospitals that support this function, as well as the establishment of a community comprehensive care network with multidisciplinary cooperation that goes beyond medical care, should also be set forth in future regional medical care plans.
Keywords: healthcare delivery system, medical insurance system, population ageing, medical care, Japan
Introduction
Hospitals are believed to have originated in the Middle Ages as accommodations for pilgrims. These early hospitals were mainly institutions for the nursing of the poor, sick, and stranded. The Hospice de Beaune in Beaune, France, is the world's oldest sanatorium, established in the mid-15th century.
Later, the Elizabethan Poor Law of the 16th century in England created "Contagious Hospitals" as places to care for patients in isolation. The same laws created poorhouses but these were mainly institutions where workers were treated and then sent to work again. In the 19th century, as modern medicine developed, military medicine and military hospitals developed as separate systems.
Either way, all modern hospitals in Europe for the treatment of the general public developed either as religious hospitals or public hospitals for the poor. In contrast, "clinics" have completely different origins and developed separately.
In Japan, hospitals developed in an altogether different way. As a 2013 government report (1) states:
"The difficulty of Japan's healthcare policy stems from the fact that, unlike in Western and Northern Europe, where national and municipal hospitals and other facilities are publicly owned, physicians have established medical corporations and private capital has been used to manage hospitals and other facilities (private ownership)".
"In the case of a publicly-owned system, governments can mandate reforms, such as how reforms have taken place in response to healthcare needs in some European countries recently".
"No other developed country as Japan has such a deregulated and market-dependent healthcare delivery system. In the case of Japan, publicly-owned healthcare facilities account for only 14% of all healthcare facilities and 22% of all hospital beds. Therefore, it has been difficult for Japan to do what other countries where healthcare institutions are publicly-owned can do systematically".
Characteristics of Japanese healthcare delivery system: Ownership-based medical care structure
Professor Shuhei Ikai of Hitotsubashi University, in his book "A Theory of the Hospital Century" (2), states that the Japanese healthcare delivery system is characterized by an "ownership-based medical care structure", which he defines as having the following characteristics:
i) Free access with a high degree of freedom. This leads to bloated outpatient care. It means "if you wait for three hours, you can see a doctor on the same day. There are very few countries where this type of outpatient consultation is possible.
ii) Ownership of hospital beds by physicians in a system where any licensed physician has the freedom to choose where he or she opens their business and their specialty (free labeling). The functions of large hospitals and clinics are undifferentiated, and large hospitals also have outpatient departments, creating a competitive relationship between them. General practitioners have certain specialties, and both hospitals and clinics provide both primary and secondary care, which means offerings overlap.
iii) Direct employment of physicians by hospitals. It is the physicians attached to (i.e., employed by) the hospital who provide medical care using the hospital's medical resources. So-called open-type hospitals do not function in Japan.
iv) High ratio of private hospitals and hospital bed stock. The historical development of Japanese hospitals is unique in that private clinics became hospitals with their own beds, and then became incorporated as medical corporations.
v) Decentralized distribution of hospital beds and expensive medical equipment. As a consequence of iii) and iv), each medical institution manages its own hospitals based on its own risk and judgment in a competitive relationship. As a result, the distribution of beds among facilities is decentralized, and each institution decides how it will invest capital. making it difficult to systematically allocate beds and equipment.
vi) High specialization of general practitioners. Most general practitioners start their career through the medical office and resident physician system, then open their own practice, and many also have a specialty. This situation is quite different from that of general practitioners in other countries; in reality, Japanese general practitioners are able to provide not only primary care but also a certain level of secondary care.
vii) The lack of a family doctor (GP) system.
viii) Medical office system and egalitarian hiring. Because both resident physicians and doctors in private practice both have the same level of specialization, a system of specialized doctors does not work.
Japan's modern medical care system has taken shape since the Meiji era. This extremely stable and immutable system has come to be a defining factor for medical policy, and, as a result, medical policy has only progressed gradually.
An evaluation of Japan's healthcare system to date
Japan's healthcare system is highly regarded internationally, as the country achieved universal healthcare coverage in the 1960s. There are very few treatments that are not covered by health insurance, and services covered are provided in an extremely fair, equal, and inexpensive manner. Free-access is guaranteed, and Japan was the first in the world to establish a systematic long-term care insurance system (3).
The World Health Organization report in 2000 (4), a Newsweek feature in 2010 (5), and The Lancet in 2011 (6), international media and organizations speak highly of Japan's healthcare delivery system. On the other hand, however, the Lancet points out, for example, that Japan is facing a declining birthrate and an aging population, and there is no guarantee that the current system can be maintained in such an environment. This is a very good system, but if it is to be maintained, it must be reformed.
Issues surrounding Japan's medical care: Challenges of a "super-aged" society
Japan is already one of the world's most aged societies, its population declining by 800,000 to 1,000,000 people every year (7). There are no signs of any reversal to this decline, or to the aging of the population. Japan's population is expected to decline by about 15% by 2040 (7). On the other hand, the number of elderly people, especially those in the later stages of life, will increase, so the growth in the number of people requiring nursing care will outpace that of the overall aging of the population. Japan's elderly population will peak in 2040, and its super-elderly population in the 2060s (8), so numbers of individuals requiring care will not start to ease until after that time.
In addition, the structure of diseases will change. The number of chronic diseases will increase, pushing up treatment rates and length of treatment. The length of time people require nursing care will also increase. In other words, medical care needs per capita will increase.
Furthermore, medical technology is advancing at an ever-increasing pace, so medical care will become more sophisticated, and diseases that could not be cured before will be cured. If diseases can be cured, the average life expectancy will further increase.
An increase in medical care needs is unavoidable. Recently, Japan's fiscal authorities have argued without evidence that an increase in costs can be kept in line with gross domestic product (GDP) growth, but a look at other countries reveals that this is impossible. The Organization for Economic Co-operation and Development has published research showing that the ratio of medical care costs to GDP will increase over the next 20 years in all developed countries (8). This does not mean that nothing can be done about costs, but as long as there is a substantive increase in needs, an increase in medical care costs should be considered inevitable.
Meanwhile, the socioeconomic structure of Japan and the profile of its elderly population continue to evolve. Family and community ties are weakening, and the number of elderly living alone or in pairs will increase. Already today, most of Japan's elderly are already in single- or two-person households. This means that the point at which support is necessary is getting closer and closer to individuals. For example, a helper must be dispatched if an elderly person living alone needs something as small as a lightbulb changed. The proportion of the elderly who depend on public services will continue to increase.
Since the postwar generation will become the core of Japan's elderly population, a majority will be made up by long-time urban residents and Employees' pensioners. On the other hand, however, income disparities within the elderly population will widen.
In addition, the post-bubble generation, who were of working age during Japan's 30 years of economic stagnation, and those over 40 who struggled to find work and became contract employees, will grow old. The number of elderly people who are single, poor, and without relatives will increase. The burden on the social security system will continue to grow.
Issues surrounding Japan's medical care: Challenges of human and material resources
The level of human and material resources supporting medical care in Japan is surprisingly not very high. If we reiterate the characteristics of Japan's medical care delivery system, the reasons for this become clear.
i) Japan has the most private capital-dependent healthcare delivery system of any developed country. Profits and losses of private hospitals ultimately belong to individuals (medical corporations) who manage those corporations at their own risk. Furthermore, even if the hospital is a non-profit corporation, the president of the hospital must act as a personal guarantor for any capital investment, no different from any other small business. Because they are managed by individuals who guarantee their debts, they cannot be easily reorganized and integrated.
ii) Governance of the regional healthcare provision system is not yet established. Until the revision of the Medical Service Act in 1985, it was not even possible to regulate the number of hospital beds. The allocation of human and material resources and capital investment is done by individual medical institutions based on their own judgment. In other words, they are facility-complete, and not "community-complete", in which the entire region coordinates and maintains its own facilities.
Not only private hospitals, but also public hospitals and public medical institutions, which are supposed to be well governed, duplicate functions and investments, wasting resources. In addition, medical institutions have undifferentiated functions and don't sufficiently coordinate between each other. As a result, although the number of hospital beds in Japan is high by international standards, higher functions are weak, medical care functions are inadequate, and there is no coordination with long-term care.
The number of doctors per population in Japan is not so bad, but the number of doctors per hospital bed is only one-fifth of those in the U.S. and the U.K., and less than half of those in Germany and France (Figure 1 and Figure 2). In addition, the number of doctors per hospital bed in other countries is increasing significantly as medical care becomes more sophisticated. The number of doctors per hospital bed in Japan has hardly increased at all, the gap between Japan and other countries is growing wider and wider; and the same is true for nursing staff (Figure 2).
Figure 1.
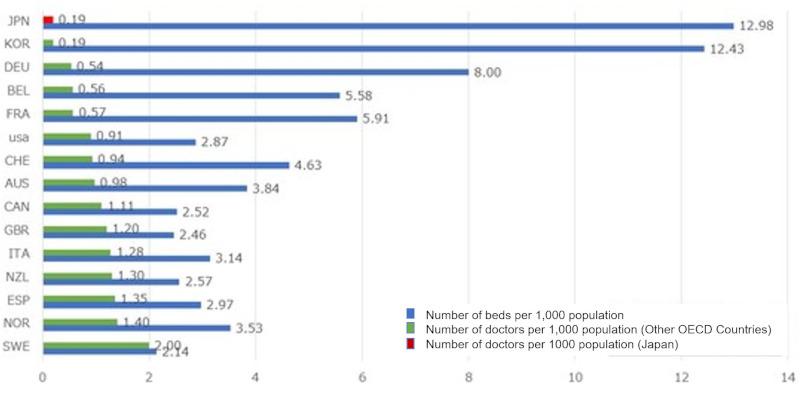
The number of physicians per hospital bed in Japan. Data Source: OECD Health Statistics 2018. https://www.oecd-ilibrary.org/social-issues-migration-health/data/oecd-health-statistics_health-data-en
Figure 2.
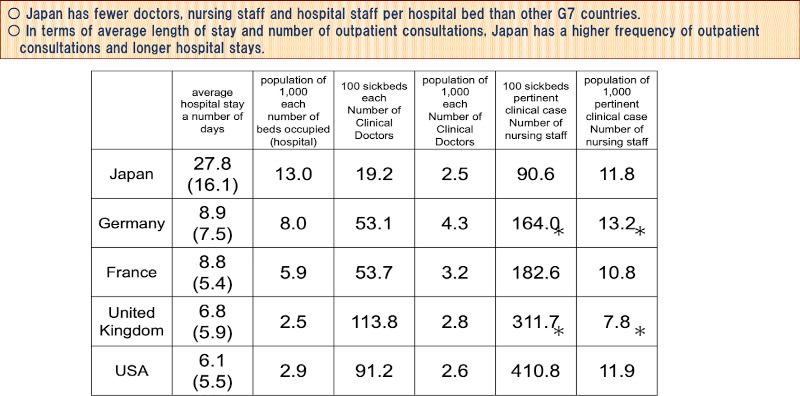
International comparison of the Number of hospital staff per hospital bed, average length of stay and discharge in G7 countries. *includes staff working at research institutes, etc., in addition to staff actually engaged in clinical practice. Data Source: Ministry of Health, Labour and Welfare. Survey of medical facilities (2020). https://www.mhlw.go.jp/bunya/iryouhoken/ database/zenpan/iryoukikan.html
This is reflected in the difference in the average length of hospital stay. Although the hospital stay in Japan has become much shorter, it is still longer than in the West. It is well known that the length of hospital stay is correlated, or rather inversely related, to the number of doctors in a hospital. In short, in Japan, hospital care has become "thin-on-the-ground medical care".
Looking at the percentage of hospitals by type of establishment (Figure 3), 93% of private hospitals have 199 beds or less (9). These hospitals account for 70% of Japan's total (9). The fact that there are many medical facilities and patients can go where they choose, and that there are medical facilities close by, means that it is easy to get medical care, but the question remains as to whether this is the case from the perspective of allocating finite medical resources.
Figure 3.
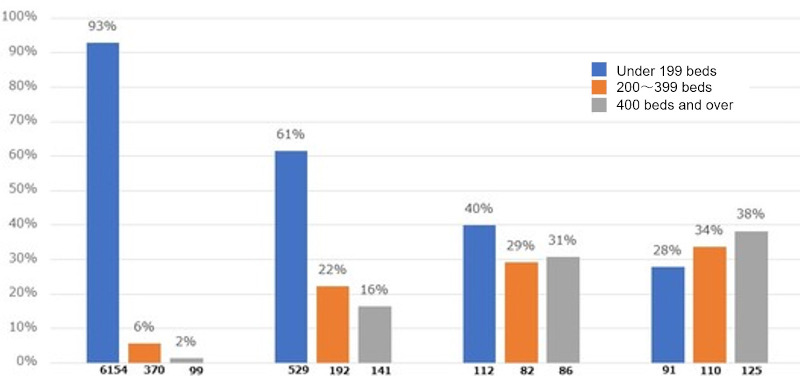
Percentage of hospitals by type of establishment and bed size. Hospitals in Japan are small in size. In particular, more than 90% of private hospitals have less than 200 beds. Data Source: Ministry of Health, Labour and Welfare. Survey of medical facilities (2020). https://www.mhlw.go.jp/bunya/iryouhoken/database/zenpan/iryoukikan.html
A simple calculation shows that each hospital physician is responsible for 5.5 inpatients in Japan, in other words, one doctor is in charge of 5.5 beds. In the U.S., the number is 1.1. This means that Japanese hospital physicians are responsible for five times as many patients as their American counterparts.
In the outpatient setting, the total number of outpatient visits per year by U.S. physicians is 1,538, compared to 5,333 in Japan (10). Under the Japanese healthcare system, which guarantees free access, the working environment for doctors is extremely harsh. It would be strange if reforming physicians' working environment was not on the table.
Why is this happening? Since the achievement of universal health insurance, Japan has not developed enough human and material resources to meet exploding medical needs. The history of medical care demand has been handled mainly by private medical institutions with minimal facilities and manpower. Looked at from a different perspective, the system of fee-for-service payment, may also be said to solve the problem by simply encouraging the creation of more medical institutions.
Hospital doctors and staff are chronically overworked, but unable to provide concentrated inpatient care; diagnosis responsibilities are undifferentiated and hospitals are unable to keep up with changes in the kinds of diseases that patients present. Many medical institutions don't have the facilities or the staff to provide advanced functions.
Nevertheless, since the medical care delivery system is built on the premise that medical institutions are self-financed, the entire system will collapse if reimbursement is not designed so that each medical institution can operate independently. As a consequence, various policy inducements have been made, but the remuneration system (allocation of financial resources) has largely been set up to maintain the status quo.
The problems inherent in this structure were exposed in one fell swoop with COVID-19.
What we learned in the COVID-19 pandemic
Although there are various opinions, mine is that what Japan experienced during the COVID-19 pandemic gives a glimpse of what Japan's medical care will look like 20 years from now.
Even today, 70% of hospitalized patients are already over 65 years old. Half of them are over 75 years old (11). In 20 years, most patients will require nursing care and have underlying diseases. A large percentage of them will have dementia. It will be the norm for such people to come in with infections, acute exacerbations, pneumonia, and broken bones - and there is no one at home to take care of them.
We have to think about the medical and nursing care system with such patients in mind. The plan was to get there by 2040, but this situation is now unfolding before our eyes. Remember what happened in the infectious disease ward when an elderly dementia patient was hospitalized with the coronavirus? In 2040, such situations ― while the majority of patients admitted to acute care hospitals are those in need of care with multiple underlying medical conditions at the same time ― will occur on a large scale on a daily basis.
If this is the case, medical and nursing capabilities must be thought of together. A unilinear regional care delivery system with hospitals at its core, with the hospital upstream and the home care system downstream, will no longer be possible. Acute care hospitals must also consider having medical and long-term care capabilities, and chronic care hospitals must be able to provide at least secondary emergency care in order to support the community.
Nursing homes, as well, cannot skimp on medical care capabilities. The entire home care provision system will literally break down if a comprehensive and coherent care network is not implemented.
These things have been discussed for a long time, but unless they are seriously implemented now, we will not be able to survive in the future society. The pandemic forced this realization upon Japan by exposing structural problems in its healthcare delivery system.
Of course, a pandemic is a one-off, large-scale disaster that does not happen every day. In that sense, it is correct to consider Japan's "contingency response". At the same time, the situation that occurred - the so-called "collapse of medical care" - should be viewed as the manifestation of structural problems that were inherent in the system during normal times, and as an opportunity to solve structural problems in the current healthcare delivery system itself.
The reasons that Japan's system of delivering medical care is functionally undifferentiated, inefficient, "thinly spread", and lacking in spare capacity is precisely because medical care has been delivered mainly by independently-financed private hospitals in an unrestricted medical system where doctors can freely select their own medical specialties and disclose them to the public (free labeling). Cooperation and collaboration among medical institutions is not the default, and any cooperation among doctors and medical institutions is basically left to the resourcefulness and actions of individual doctors and medical institutions on the frontline.
Furthermore, under a free-access medical insurance system with a high degree of freedom of choice on the part of patients, there is no institutional control of patient flow. In Japan's free access system, patients are entirely responsible for deciding whether or not to go to a doctor, which doctor to go to, and which department to go to, without any advice or assistance from professional medical personnel. In other words, the system is not designed to objectively provide timely and appropriate medical care or to provide necessary medical care when needed. If this is the case, it is difficult to create a system for comprehensive and continuous health management, a flow of prevention and health management, initial diagnosis and treatment (primary care), specialized treatment, return home, and nursing care and lifestyle support. In other words, neither the supply, nor the demand side can be controlled.
Despite this situation, the system has managed to function to date. However, the frontline healthcare workers who support medical care shoulder a heavy burden. As mentioned above, the number of inpatients per physician in Japan is five times that of the U.S., and the total number of outpatients per year is 3.5 times that of the U.S. As the recent pandemic has made clear, Japan's healthcare system is fragile and can easily collapse if there is two much pressure put on one specific point.
Will medicine really be able to sustain itself for the next 15 to 20 years in Japan? Even now, there are cases of emergency patients being shunted around from hospital to hospital and individuals who are unable to access medical care and nursing care. The lack of coordination and networking on the provider side has led to blockages here and there, and there have been many cases of families running around looking for a facility to stay in.
Now that the pandemic has brought the problem to the fore, perhaps now is the time for reform.
What is required of medical care in a super-aged society
In the long-term care world, it's already common understanding that the goal of elderly care should be to enable people to live with dignity at home, in their community, for as long as possible (12). The role of long-term care service is to support lives and lifestyles. In a super-aged society, regular medical practitioners need to also start thinking this way.
The basic function of medicine - providing treatment to cure - will not change, but in addition to that, it will be important to heal and support. In other words, what will be required is medical care that supports the dignity of people's lives, and does not sacrifice life for the sake of treatment. Medical care will exist as a part of life.
"Healing and support" cannot be achieved by medical care alone, unless a comprehensive regional care network, provided by medical care and long-term care together, with the cooperation of many different professions that support patients, is created.
As is already the case in the world of social service and, outreach to patients/users in close proximity will also be required of medical care. House calls will become more important, and asynchronous, remote medical care, such as telemedicine, will become an important weapon in the future, especially when considering the limited human and material resources available to support local medical care. There have been remarkable advances in medical digital transformation and other home healthcare support technologies, and it is already technically possible to perform a considerable amount of diagnostic procedures remotely (13). These technological innovations will contribute to reducing the burden on both patients and medical personnel, and should be actively implemented.
In order for this system to work, IT infrastructure to centralize patient health information and share information, is an indispensable prerequisite. "Tooling" such as medical IT, IoT, and digital transformation must be standard, and should be prioritized as essential to support home medical care and community comprehensive and coherent care networks.
Medical care challenges faced by a super-aged society
The functions of hospitals in a super-aged society will be divided into two major approaches. On one hand will be highly-specialized, acute care hospitals that provide intensive acute care, on the other, community-based hospitals that provide medical care for healing and support (3).
While there has been a lot of discussion about rethinking regional medical care, we should further promote functional differentiation of hospital beds, selection and concentration, strengthening of acute care functions, and concentrated investment of resources (efficient use of hospital beds by reducing the number of hospital beds). At the same time, we should also clearly set a direction for strengthening regional medical care and home medical care. As I have emphasized in this paper, if home medical care is not strengthened, the burden on hospitals and emergency medical services will increase, and the entire medical care delivery system will break down.
In this sense, the implementation of primary care physician function and the clarification of the functions and roles of small and medium-sized community-based hospitals that support this function, as well as the establishment of a regional comprehensive and coherent care network with multidisciplinary cooperation that transcends medical care, should also be pillars of regional medical care.
Regional medical care impacts the overall medical care delivery system. Although debate tends to focus on reducing the number of hospital beds, the original purpose of regional medical care is to reallocate and reorganize human and physical resources to "efficiently meet the future medical (and nursing care) needs of the region with the existing human and physical resources".
The realization of better regional medical care will lead to better resource allocation and the optimization of overall medical care costs. Reforming how care is delivered is the most realistic and effective way to optimize costs.
Long-term care becomes more important in a super-aging society
Finally, I would like to share some interesting data. As you may recall, all elderly people aged 65 and over are enrolled in Medicare in the US. In other words, all medical costs for the US population after the age of 65 are reflected in the Medicare database.
One study (14) compares the cumulative amount of medical and long-term care expenses spent by those aged 65 or older who are enrolled in Medicare up to the time of their death, segmented by age at death. The data shows that the longer a person lives, the more his/her lifetime medical expenses increase until they peak out at around age 90-95. In other words, the lifetime medical costs of someone who lives to be 100 or and someone who lives to be 110 years old are not very different. It follows, then, that if average life expectancy were to increase to 90 or 100 years, medical costs would gradually start to peak out as people lived longer healthy lives.
The data for long-term care costs shows a different picture. The lifetime cost of long-term care increases with the age at death, and exceeds the lifetime cost of medical care for those over age 95. This means that as more people age in a super-aged society, the relationship between cumulative medical costs and cumulative long-term care costs by the time of death is reversed.
In other words, aging (increase in life expectancy) will be a factor in increasing lifetime medical costs until about the age of the 90s, but long-term care (long-term care) will continue to grow without peaking out.
In conclusion, The COVID-19 disaster revealed structural weaknesses in Japan's healthcare delivery system. We should take this as an important warning: this is only the beginning. Looking ahead to the year 2040, it is inevitable that Japan will need to streamline and optimize its healthcare delivery system given its limited resources. This will depend on a reform of the entire regional medical care delivery system, and a move towards a more community approach to medical care. Only this shift will allow Japan to more efficiently use resources and give patients better care - and a shot at a better quality of life - overall.
Funding
None.
Conflict of Interest
The author has no conflicts of interest to disclose.
References
- 1. Cabinet Secretariat (Japan). Report of National Council for Social Security Reform, 2013. https://www5.cao.go.jp/keizai-shimon/kaigi/minutes/2013/0808/sankou_02.pdf (accessed November 21, 2023). (in Japanese) .
- 2. Shuhei Ikai. A Theory of the Hospital Century. Yuhikaku Publishing, Tokyo, Japan. 2010. [Google Scholar]
- 3. Ministry of Health, Labour and Welfare. White Paper on Health, Labour and Welfare (2000). https://www.mhlw.go.jp/toukei_hakusho/hakusho/kousei/2000/ (accessed January 16, 2024). (in Japanese) .
- 4. World Health Organization. The world health report 2000. Health Systems: Improving Performance. https://www.who.int/publications/i/item/924156198X (accessed November 21, 2023).
- 5. Newsweek. The best countries in the world (August 16, 2010). https://www.newsweek.com/best-countries-world-71817 (accessed November 21, 2023).
- 6. The Lancet. Japan: Universal health care at 50 Years. https://www.thelancet.com/series/japan (accessed November 21, 2023). [DOI] [PubMed]
- 7. National Institute of Population and Social Security Research. Population projections for Japan: 2021-2070 (2023). https://www.ipss.go.jp/site-ad/index_english/population-e.html (accessed January 16, 2024).
- 8. OECD iLibrary. Health at a grance 2019: OECD indicators. https://www.oecd-ilibrary.org/sites/4dd50c09-en/index.html?itemId=/content/publication/4dd50c09-en (accessed January 16, 2024).
- 9. Ministry of Health, Labour and Welfare. Medical facilities survey (2020). https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/20/dl/09gaikyo02.pdf (accessed January 16, 2024). (in Japanese) .
- 10. OECD iLibrary. OECD health working Paper 2020. https://www.oecd-ilibrary.org/social-issues-migration-health/oecd-health-working-papers_18152015
- 11. Ministry of Health, Labour and Welfare. Patient survey (2020). https://www.mhlw.go.jp/toukei/saikin/hw/kanja/20/index.html (accessed January 16, 2024). (in Japanese) .
- 12. Ministry of Health, Labour and Welfare. Elderly care in 2015. https://www.mhlw.go.jp/topics/kaigo/kentou/15kourei/3.html (accessed January 16, 2024). (in Japanese) .
- 13. Takao H. Digital Medicine - Current ability and future. Nikkei BP, Tokyo, Japan, 2022. (in Japanese). [Google Scholar]
- 14. Spillman BC, Lubitz J. The effect of longevity on spending for acute and long-term care. N Engl J Med. 2000; 342:1409-1415. [DOI] [PubMed] [Google Scholar]