

Summary
This review article explores the potential contribution of Japan's experience in addressing rapid aging in Asia with a specific focus on dementia care. As Japan is a frontrunner in terms of aging society, we consider valuable insights and lessons from Japanese policy history and reflect on its contribution. The World Health Organization, Regional Office for the Western Pacific Regional Action Plan on Healthy Ageing for the Western Pacific was compared with the Japanese "Outline for Promotion of Dementia Policies". The following five issues were discussed: i) improving awareness of dementia and community engagement in Japan from a mutual aid perspective; ii) social activities for prevention of dementia at the local level; iii) human resources for medical and long-term care; iv) local coordinators for old people care at home to evaluate the needs for care and tailor the care-plan on an individual basis; v) research and development of long-term care products. Given these factors, it is important to address the aging society through a combined cross-sectoral approach, including policy, research, development of care products, community, and education of care workers. Aging population measures in Japan do not provide a definitive answer, which prompts the consideration of better solutions derived from Japan's trial and error. The aging rate of 7%, 14%, and 21% are commonly used in international comparisons as indicators of the speed of the aging process, but before this 7% is reached, policies tailored to each country should be considered.
Keywords: long-term care, healthy aging, Japan, policy
Introduction
Population aging is an inevitable global trend. With the improvement of health and survival, as well as the reduction of fertility rates, population aging is expected to increase in many low- and middle-income countries (LMICs), where current populations are relatively young. Population aging is expected to occur considerably faster in LMICs than in high-income countries, which poses a major challenge for LMICs in terms of adopting public policies addressing this social transformation. The Asia- Pacific region is aging faster than any other region, and the number of people aged 60 years or senior will increase from 630 million to 1.3 billion by 2050 (1).
The United Nations (UN) and the World Health Organization (WHO) have discussed aging, which affects all aspects of economies and societies, for decades. The Madrid International Plan of Action on Ageing (2), the UN's landmark international agreement, linked aging to other frameworks for social and economic development and human rights. In 2002, the WHO adopted a policy framework of active aging (3,4). Active aging is a concept that encompasses ongoing involvement in social, economic, cultural, spiritual, and civic affairs beyond physical health and should be addressed by the three pillars of policy: participation, health, and security. Recently, the UN has set 2021-2030 as the Decade of Health Ageing (5) to provide everyone with the opportunity to maintain the functional ability that ensures well-being in old people. In response, the WHO Regional Office for the Western Pacific (WPRO) adopted the "Regional Action Plan on Healthy Ageing for the Western Pacific" in 2021 (6).
Japan has been at the forefront of the global trend of population aging ahead of other countries. When contrasted with other countries, the transition toward a super-aged population in Japan is significant and notably rapid. Compared with Western countries, Japan initially fell behind in reaching a 10% proportion of its population aged 65 years and older adult in the 1980s. However, it has since become one of the earliest countries to achieve a 20% share of this age group in the 2000s (7). As the population continues to age, the prevalence of dementia continues to increase. The prevalence of dementia in Japan is projected to rise from 16.7% in 2020 to 28.7% by 2045, primarily due to further population aging (8). In response to these challenges, a community based integrated care system was introduced in Japan 2017, to provide medical care, nursing care, preventive care and livelihood support integrally in the communities where older people used to live. The increase in dementia is not limited to Japan alone but also elsewhere in the Asia- Pacific region. Nevertheless, studies on the insights garnered from Japan regarding dementia are lacking, as well as the potential for their application in other LMICs, particularly in the Asian context. Decades long endeavours and systematic models enabling sustainable healthy aging and universal access to health and long-term care services in Japan are crucial to share with countries around the world. This study provides recommendations on how to address dementia in the aging society, focusing on the Asia-Pacific region, and compares strategies of Japan and global, consideration from specific Japanese initiatives.
History of Japanese experiences for dementia and areas of possible contributions
The key events in Japanese policy for dementia are summarized in Table 1. In 2000, the Japanese government enacted the Long-Term Care Insurance Act (the Act). The Act contributed to the development of dementia care through the definition of Communal Daily Long-Term Care for a Dementia Patient (Group Homes) as one of the specialized services for dementia, which increased the number of persons certified as in need of long-term care or support (9-13). In 2004, to reduce the prejudice regarding dementia, the Japanese word meaning "dementia" was changed from "Chiho" to "Ninchisho" (14). In 2005, the "Dementia Supporter Program" was started to promote understanding of dementia among citizens; however, this was implemented through only 90 minutes of training for volunteers (15). Following the dementia summit in the UK in 2014 (16), the New Orange Plan, the cross-ministerial strategy for dementia by 12 related ministries and agencies, was launched in 2015 (17). Responding to this new strategy, the Act was revised as follows (18): raising awareness of dementia, comprehensive promotion of proper rehabilitation and support for carers, and prioritizing the viewpoint of persons with dementia and their families. To further promote dementia policies as population aging progressed, the Ministerial Council on the Promotion of Dementia Policies was set up in 2018 (19), and the "National Framework for Promotion of Dementia Policies" (Framework) was adopted at the Council in 2019 (20,21). Recently, as the comprehensive and systematic promotion of policies to enable those with dementia to live in dignity with a sense of purpose, the Basic Act on Dementia to Promote an Inclusive Society was enacted in 2023 (22).
Table 1. Key events of Japanese policy for dementia.
| Year | Events |
|---|---|
| 2000 | Long-term care insurance act was enacted. |
| 2004 | Japanese word to mean "dementia" was changed. |
| 2005 | "Dementia Supporter Program" was started. |
| 2014 | Global Dementia Legacy Event Japan was held. |
| 2015 | "New Orange Plan" was launched. |
| 2017 | Revision of long-term care insurance act was released. |
| 2018 | Ministerial council on the promotion of dementia policies was set up. |
| 2019 | "National Framework for Promotion of Dementia Policies" was adopted at the Ministerial Council. |
| 2023 | "Basic Act on Dementia to Promote an Inclusive Society" was enacted. |
The basic concept of the Framework is to promote policies that focus on "inclusion" and "risk reduction" while underlining the perspectives of people with dementia and their families to delay the onset of dementia and build a society in which everyone can live with hope, even if they develop dementia. "Inclusion" means that persons with dementia can live with the condition with dignity and hope and that people can live together in one society regardless of whether they have dementia. Moreover, "Risk Reduction" means not "to never develop dementia" but "to delay the onset" or "slow the progression" of dementia.
The Framework includes five objectives (20,21): i) raising awareness/supporting persons with dementia to express their views through promoting "Dementia Supporters", especially in the private sector, and publicizing "Declaration to live well with dementia"; ii) reducing the risk of dementia through expanding "Kayoinoba", places for older citizens to meet in the community, gathering and publicizing evidence; iii) strengthening medical and long-term care/support for caregivers through enhancing the quality of the system for early detection/intervention and promotion of training for family caregivers and peer activities among family caregivers; iv) promoting "Dementia Barrier-Free"/ support for people with early onset dementia/support for social participation through establishing living environments accessible for persons with dementia, considering certification and awards for the private sector, and promoting social participation activities; v) research and development (R&D) / industrial promotion/ global expansion through establishing a clinical trial-ready cohort. Furthermore, the policy emphasizes that i)- v) should be promoted, prioritizing the perspectives of persons with dementia and their families.
In 2020, the WHO launched the latest regional strategy (6), the Regional Action Plan on Healthy Ageing for the Western Pacific, which is composed of five objectives: Objective 1: Transforming societies as a whole to promote healthy aging based on understanding the implications of population aging. Objective 2: Transforming health systems to address each individual's lifelong health needs by providing necessary health and non-health services in a coordinated manner. Objective 3: Providing community-based integrated care for older adults tailored to individual needs. Objective 4: Fostering technological and social innovation to promote healthy aging. Objective 5: Strengthening monitoring and surveillance systems and research on older adults to inform programs, services, and policies. A comparison with the Framework in Japan is presented in Table 2. Accordingly, a substantial number of elements are similar to each other, especially regarding emphasis on the importance of interventions not only for individual physical and mental health, but also for social and cultural transformation. Innovation is considered a key component of both policy instruments. However, the WPRO strategy focuses on strengthening the health system to deliver health services in health facilities, whereas the Japanese policy mainly prioritizes risk reduction and promotion of social inclusion. The difference may derive from the long history of awareness and recognition of health problems among the older population in Japan. The Japanese government strongly recognizes that the health system alone cannot solve the complicated issues in the aging society, and more broader stakeholders must collaborate closely.
Table 2. Comparison of dementia policy in Japan with aging policy in WHO Western Pacific Regional Office (WPRO) and possible contribution areas.
| Regional Action Plan on Healthy Aging in the Western Pacific 2020 | Japanese National Framework for the Promotion of Dementia Policy 2019 | Possible Contributable Areas from Japanese Experiences |
|---|---|---|
| Objective 1: Transforming societies as a whole to promote healthy aging based on understanding the implications of population aging |
Pillar 1: Raising awareness/Supporting persons with dementia to express their views ●Promoting dementia supporters in the private sector ●Publicizing the "Declaration to live well with dementia" |
Community awareness activities including dementia supporters and Minsei staff ●Seminar and lectures held by local governments ●Developing local leaders ●Collaborating with other sectors (e.g., education) |
|
i) Understanding the broader implications of population aging ii) Transformating policies across sectors to ensure that they are age-friendly iii) Advocacy to prevent ageism and create a positive culture around aging |
Pillar 4: Promoting "Dementia Barrier-Free"/Support for people with early onset dementia/Support for social participation ●Establishing living environments that are accessible to persons with dementia ●Considerating certification and awards for the private sector ●Promoting social participation activities |
Social activities for prevention of dementia at the local level ●Socialization activities by local communities ●Relevant laws and policies to promote the social participation of older adults ●Collaborating with businesses in the private sector to provide appropriate working environments for older adults |
| Objective 2: Transforming health systems to address each individual's lifelong health needs by providing necessary health and non-health services via a coordinated approach. i) Curative services, including NCDs ii) Preventive services, including NCDs iii) Social and welfare services iv) Innovation |
Pillar 2: Risk Reduction ●Expanding "Kayoinoba" (i.e., places for older citizens to gather in the community) ●Gathering and publicizing evidence Pillar 3: Medical and long-term care/Support for caregivers ●Enhancing the quality of the system for early detection/ intervention and strengthening collaboration ●Promoting training for family caregivers and peer activities among family caregivers |
Human resources for medical and long-term care ●Special education concerning aging for doctors, nurses, and other health professionals ●Collaboration among health professionals (e.g., dental technicians, nutritionists, occupational therapists) to reduce the workload on nurses and strengthen the quality of care |
| Objective 3: Providing community-based integrated care for older adults tailored to individual needs i) Health care ii) Long-term care iii) Social activities and services iv) Individual-level coordination |
Pillars 2, 3, and 4 |
Long-term care insurance system Local coordinators for at-home older adult care to evaluate care needs and tailor care plans on an individual basis (integrated community support center and care managers) ●Maximizing locally available resources for the care of older adults ●Supporting older adults at home to achieve their expectations at end of life and reduce caregivers' workloads, both financially and physically ●Supporting older adults efficiently and inclusively |
| Objective 4: Fostering technological and social innovation to promote healthy aging i) Technological innovation a) Technology to support skill development and maintain the workforce b) Technology to support health and health systems c) Technology to promote social connectedness and aging in place ii) Social innovation |
Pillar 5: Research and development/Industrial Promotion/ Global expansion |
Prioritization of research on aging ●MHLW research funds for aging ●Research centers for aging to be established at the national and prefecture levels |
| Objective 5: Strengthening monitoring and surveillance systems and research on older adults to inform programs, services, and policies i) National survey ii) Research iii) Monitoring and evaluation of healthy aging |
●Establishment of clinical trial cohorts | Innovation of various long-term care products |
As a global front-runner of the super aging society, Japan presents useful lessons for other countries because most will inevitably face age-related issues. To identify the possible area of contributions from Japanese experiences, several specialists of aging in Japan and other countries listed the strengths of Japanese measures for older people care as shown in column 3 of Table 2. The experience of long-term insurance in Japan is an important aspect for establishing financial and service delivery systems for aging in LMIC. Nevertheless, given the extensive literature covering this topic (11), we do not discuss this aspect in this study Other possible contributions are as follows: i) community awareness activities, including dementia supporters; ii) social activities for the prevention of dementia at the local level; iii) human resources for medical and long-term care; iv) local coordinators for older people care at home to evaluate the needs for care and tailor the care-plan on an individual basis; v) R&D of various long-term care products. The details are discussed in the following sections.
Area 1: Dementia supporter: Improving awareness of dementia and community engagement in Japan from a mutual-aid view
In 2005, the Ministry of Health, Labour and Welfare (MHLW) initiated the "Dementia Supporters" program to raise awareness about dementia among local communities. The background to the program was the stigma surrounding dementia owing to the negative name (Chihou). Therefore, the aim was to change the name and promote a correct understanding of dementia. In their annual reports in 2012, the WHO and Alzheimer's Disease International highlighted this program as one of the lessons learned from beating stigma and public understanding of dementia (23,24). The program allows individuals to become supporters after completing training organized by "The National Caravan Mate Liaison Council" (Council). Every municipality in Japan has its council and manages training accessible to people nationwide. Upon completing a 90-minute training course, participants can become certified Dementia Supporters. As of June 2023, approximately 15 million individuals have registered as Dementia Supporters (25).
The Dementia Supporter Program is not exclusive to the Council; it is open to everyone. The council provides standardized training courses, which ensures consistency in the education provided. Further, as courses are held in primary, junior high, and high schools, children can also participate. The primary aim is to ensure Dementia Supporters have correct knowledge and understanding of dementia, without prejudice. Moreover, the program aims to create a dementia-friendly environment so that local people with dementia and their families can live safely in their neighborhoods. To this end, they are expected to take the initiative in the community to create a network of community, interaction, and support. Therefore, the training course covers basic knowledge of dementia, how to treat family members and community members with dementia, and an introduction to various activities.
Most participants are local individuals, and the program also acts to connect local residents with each other. The completion of one course leads to a permanent qualification, but some residents have participated multiple times. Many of the participants are older people. They may be motivated to attend by the need to create a new zest for life after career retirement, join the community, or prepare for their future. In addition, they have a family member or neighbor with dementia.
Numerous supporters are students who attended the course at their school. Other participants include engaged business enterprises and organizations caring for local residents. For instance, most workers include professionals from banking organizations, transportation staff, and stockists, police officers, and the owners of real estate. Nonetheless, despite the substantial number of Dementia Supporters, only a small fraction of the total dementia patient population in Japan is covered.
To address this gap, the Council has established a supporter network called "Team Orange". This network is open to all Dementia Supporters who wish to register. Moreover, supporters have the opportunity to advance to become "Caravan Mates" by meeting specific requirements. These advanced supporters typically collaborate closely with local municipalities to organize various events aimed at improving community awareness about dementia. In 2016, in a joint partnership with the UK, the MHLW appointed celebrities from both countries as "Dementia Supporters Ambassadors" (26,27). The UK has a similar program known as "Dementia Friends". This is intended to go beyond local activities by supporters and the domestic network of Team Orange, with both countries taking the initiative to expand dementia-friendly community development and supporter activities globally. Recently the network is expanding worldwide (28).
Given the substantial number of dementia patients in Japan, fostering greater local awareness about dementia is vital. The "Dementia Supporters" program, alongside the "Team Orange" supporter network, represents a commendable initiative to engage communities, promote understanding, and support those with dementia. With ongoing efforts and collaborations, Japan is continuing to make strides in creating a dementia-friendly society in super-aged society.
Area 2: Social activities for prevention of dementia and healthy aging at the local level (Community Trainers): Dementia prevention activities for people who are not certified as requiring support or nursing care
As Japan's population ages, the opportunities for everyone to receive medical and nursing care are increasing. Japan has universal health insurance - both the patient and the government bear hospital and nursing care costs. However, the country's financial situation is becoming increasingly strained owing to rising medical and nursing care costs. In response, the government is attempting to curb costs by intervening and conducting preventive activities before patients become bedridden or suffer from dementia, which incur high medical and nursing care costs, and working to prevent further deterioration of these conditions.
Under Japan's long-term care insurance system, people can use long-term care services if they become bedridden, suffer from dementia, or need assistance in daily living, such as housework and personal care. However, care prevention activities, in which people can participate before they need assistance, have been developed nationwide. The objectives of these efforts include health maintenance, lifestyle improvement, exercise, nutritional management, dementia prevention, and the promotion of social participation to maintain current physical and mental conditions. Originally, residents and local governments took the initiative in implementing these activities. Nonetheless, the MHLW launched the "Support for Promotion of Care Prevention through Community Development (2016)" as a model project for care prevention policy and further expanded the initiative to a nationwide scale with the "Care Prevention Activity Dissemination and Development Project (2018)" (29). Currently, numerous entities operate the activities and their content.
According to a 2021 survey ("Results of the Survey on the Implementation Status of the Comprehensive Project for Care Prevention and Daily Life Support (Community Support Project)"), the most common main operator of care prevention activities was "residents' groups", followed by "individual residents" and "social welfare councils". The most common main activity was "gymnastics (exercise)", followed by "hobby activities", "tea ceremony", "dementia prevention such as recreation and oral function improvement" and "communal meals" (30). While most residents and local governments offer gymnastics and hobby activities, many private companies offer activities that make the most of the characteristics of their respective companies (31). For example, telecommunications companies hold smartphone classes and encourage older adults to participate in local exercise classes online, which creates opportunities for exercise habits and social participation. In response to frequent traffic accidents caused by older adults, an automobile manufacturer is conducting safe driving courses and providing health education on frailty prevention and cognitive function. All the operating entities involve various professions, ranging from medical professionals to caregivers and welfare workers. As described above, many sectors are undertaking care prevention activities, from residents to private companies, and approaches to prevent bedridden persons and dementia are being taken from various angles through the involvement of multiple professions. However, specific performance indicators for effective projects are in the development stage. A manual for municipalities ("FY2021 Municipal Manual for Strengthening and Promoting Efforts for Long-Term Care Prevention") has been prepared but not from the perspective of private companies, non-profit organizations, or educational institutions. Thus, each organization is currently implementing the program through trial and error (32). To conduct effective care prevention activities in the future, past activities must be evaluated, and manuals and guidelines must be developed for multisectoral efforts.
Care prevention activities now involve many professions and are becoming established as national policies. This is because the aging of the population is expected to increase the number of people requiring nursing care and result in large medical costs. By intervening before people develop dementia or require nursing care, it is possible to keep them healthy. In the future, Asian countries are also expected to witness this phenomenon. To continue to be as healthy as possible, it is important to start exercises and other activities while in good health and work on dementia prevention.
Area 3: Human resources for medical and long-term care
One of Japanese policies for addressing population aging is the training of health-care workers. Japan is faced with the needs of an aging society and has always formulated policies in response to those needs, which has led to several health professionals in Japan (Table 3) (33-53). For example, in 1987, the enactment of the Social Worker and Care Worker Law (54) created the new occupations of "social worker" and "care worker", which became national qualifications. In the 2000s, the Model Core Curriculum (MCC) was developed and revised for several occupations, requiring students to study subjects related to older adults as required courses (credits) (55). This section introduces the status of education on older adults for representative occupations for which the Ministry of Education, Culture, Sports, Science and Technology has begun formulating the MCC as pre-graduate education.
Table 3. Healthcare professionals for the older adults with dementia in Japan.
| Occupation | Qualification | Availability of Model Curriculum | Availability of Older People-Related Contents | Reference |
|---|---|---|---|---|
| Medical Professionals | ||||
| Medical Doctor | National Qualification | Available | Available | (33) |
| Dentist | National Qualification | Available | Available | (34) |
| Pharmacist | National Qualification | Available | Available | (35) |
| Nurse (including Public Health Nurse and Midwife) | National Qualification | Available | Available | (36) |
| Dietician | National Qualification | Available | Available | (37) |
| Physical Therapist | National Qualification | Available | Available | (38) |
| Occupational Therapist | National Qualification | Available | Available | (39) |
| Speech Therapist | National Qualification | Available | Available | (40) |
| Orthoptist | National Qualification | Not available, Guideline only | Available | (41) |
| Radiological Technologist | National Qualification | Not available, Guideline only | Not available | (42) |
| Clinical Laboratory Technician | National Qualification | Not available, Guideline only | Available | (43) |
| Dental Hygienist | National Qualification | Available | Available | (44) |
| Dental Technician | National Qualification | Not available | Available | (45) |
| Biomedical Equipment Technician | National Qualification | Not available, Guideline only | Available | (46) |
| Emergency Life-saving Technician | National Qualification | Not available | Available | (47) |
| Prosthetist and Orthotist | National Qualification | Not available | Available | (48) |
| Care Workers | ||||
| Certified Social Worker | National Qualification | Not available, Guideline only | Available | (49) |
| Mental Health Social Worker | National Qualification | Not available | Available | (50) |
| Certified Care Worker | National Qualification (Qualify for the examination without attending a school. Can take the exam with at least 3 years of work experience and training) | (51) | ||
| Care Manager | Qualification by Prefecture Government Persons with at least five years of work experience in the health and medical welfare field who have passed the practical training examination for Care Manager and completed the practical training course for Care Manager |
(52) | ||
| Caregiver/Home Helper *Occupation, but not qualification |
A system that allows participants to take the training courses for entry-level Care Workers and Caregivers qualificator by the prefectural government while they are working (although it is a job title, it is not the name of the qualification) | (53) | ||
*Not all health care occupations are listed.
Medical Doctor: The introduction of curriculum in geriatrics in medical education has been considerably slow, with only 23.7% of universities offered a course in geriatrics in 2000 (56). In medical education, the 2007 revision of the curriculum made geriatrics-related items mandatory. Notwithstanding, in a panel discussion on geriatrics education at the 51st Annual Meeting of the Japan Geriatrics Society held in 2009, Dr. Hiroyuki Arai highlighted the lack of textbooks for medical students (57). As a result, a textbook edited by the Japan Geriatrics Society was published in 2013.
Dentist: Some dental procedures (dentures, bridges, implants, etc.) were naturally included in lectures related to older patients as they represent most of the target population. Additionally, as a basic policy of the MCC (34), the basic items to be mastered were revised in light of rapid demographic changes, such as the fact that Japan's older population will peak around 2040 and that the aging rate will continue to rise, and the population in the region will have thereafter.
Pharmacist: Pharmacist education comprises a six-year program to strengthen clinical training, contribute to the improvement and enhancement of public health by dispensing and supplying medicines, and play a role in the comprehensive community care system (58). The MCC for 2022 (59) clearly states that pharmacists must have sufficient qualities and abilities to be human resources who proactively contribute to medical care, nursing care, welfare, and community health promotion. Regarding activities of pharmacists in society and the community, they study social security (medical, welfare, and long-term care systems) and comprehensive community care.
Nurse: In the nursing profession, which plays a central role in care, the basic nursing curriculum on gerontic nursing was one of the earliest to be introduced owing to the need to respond to social needs. The 1989 curriculum revision made gerontic nursing a stand-alone subject (60) and began to provide education systematically, specifically focused on older adults (61). In the 2022 revision, the course of home health care nursing was expand to community and home health care nursing to include the community as a place of care for various individuals and groups, and the number of credits (hours) for related courses was increased (62).
Dietician, Physical Therapist, and Occupational Therapist: Along with the MHLW, each professional organization/association is responsible for developing the MCC and guidelines. Dieticians, for example, have studied geriatric nutrition because they work with people in various life stages and health conditions (37), and physical and occupational therapists, who often work with older patients, have studied it before the MCC was developed (38,39).
Radiological Technologist and Clinical Laboratory Technician: There is little content related to older adults in the MCC, which may be because they are expected to provide accurate imaging and test results necessary for diagnosis, regardless of whether the subject is young or older (42,63).
Dental Hygienist: National certification (64) as a specialized profession has existed since 1948. As a profession responsible for preventive dentistry, it also plays an important role in the fight against dementia. The "8020 Movement", a Japanese policy launched in 1989 to raise awareness of the importance of eating well with one's teeth throughout one's life - to eat with one's 20 teeth until the age of 80 - is also considered effective in combating dementia (65,66). Similar to locomotive syndrome; proposed by the Japanese Orthopaedic Association in 2007, refers to "a condition in which motor function is impaired due to disorders of the locomotor system", and many older people suffer from it (67,68), and frailty prevention, based on the concept of preventive dentistry rather than dental treatment, interventions such as dental health checks, tartar removal, and instruction on how to brush are also provided to prevent tooth decay and periodontal disease. The MCC for dental hygienists includes learning and on-the-job training according to the following life stages: fetal (pregnant women), infancy, school age, adolescence, adulthood, old age, and terminal stage. In particular, regarding older adults, students practice at health centers, nursing homes, and dental clinics that provide in-home and home visits, and experience dental-related health education, oral cleaning, home visits, and so on (43).
Care Workers: The shift from a time when family caregiving was the norm in Japan to the nuclear family has resulted in the need for many caregivers who specialize in nursing care (69). In response, a training system has been established to secure caregivers, in which they are trained not through schools or training institutes but by gaining experience in the field while working and the skill-up system (70). Furthermore, from the perspective of guaranteeing the quality of care, it was necessary to provide training to various levels and establish a system to provide care by professionals.
Next, this study discusses the status of post-graduate training, particularly regarding dementia. The Japanese government recommends that each profession conduct Continuing Professional Development to ensure the quality of care in dementia. Such training is linked to Japan's health insurance system, medical insurance, and long-term care insurance, and budgetary measures have been established. Regarding medical personnel, medical doctors, and nurses specializing in dementia provide regular training for all hospital staff. Regarding care workers, the Japanese government distributes budgets to local governments for training and awareness-raising activities related to dementia and provides support for implementation systems. Thus, local governments play a role in training and awareness-raising activities related to dementia countermeasures. Hospitals, long-term care facilities, and home care services employ personnel who have taken these dementia-related training courses, which provides an incentive for hospitals and facilities to provide care based on the training. Hospitals receive an "additional fee for dementia care" through national health insurance (71), and nursing homes and home care service facilities receive an "additional fee for specialized dementia care" through the long-term care insurance system (72).
Area 4: Local coordinators for older people care at home to evaluate the needs for care and tailor the care-plan on an individual basis. (integrated-community support center and care managers)
In many LMICs, family remains the main pillar for giving care for older people. When caregiving becomes necessary, the physical, financial, and emotional burdens on family members and other caregivers increase. In addition, caring for a person with dementia is intensive and continual ensuing opportunity cost incurred by job loss for their family member. For example, they are responsible for household chores such as meal preparation and laundry that the dementia person can no longer do, taking the person to the hospital. After all, they sometimes even quitting their jobs owing to the amount of time they spend caring for the person. In Japan, a number of nursing care service programs exist to reduce the burden on caregivers and to prevent further deterioration of the care recipient's condition. When using long-term care services, a "care plan" (provision of long-term care services, etc.) must be prepared so that the person can lead an independent daily life as much as possible. A care support specialist called care manager consults with the person receiving care and responds to their physical and mental condition, prepares care plans, and liaises and coordinates with municipalities, service providers, and facilities so that the person can receive appropriate services (51). A care manager holds a care support specialist certificate as a person who has professional knowledge and skills in assisting older adults in need of nursing care to lead independent daily lives. In Japan, various professionals such as doctors, nurses, and social workers can become care managers. If they have a certain level of work experience, they can become care managers by passing an examination and undergoing a short training course.
Older people usually have multiple morbidity that demands integrated services delivered to their home. Therefore, one of the main tasks of a care manager is to create a care plan tailored to the individual's level of care, family circumstances, and financial situation, from among 26 different types of care services. A typical care plan modeled for the older person with dementia is presented in Figure 1. The background of the person is that she is able to walk, go to the toilet, and eat meals without assistance, but she has difficulty in bathing, shopping, and cooking meals by herself. She lives with her husband, but he is too old to provide her with all the care she needs. The key points of this care plan are to ensure the patient's social participation and quantity of activities and reduce the burden on her husband, who is her caregiver. She goes to a "Day Service", which is a facility that people can receive nursing care and functional training, three times a week to socialize with helpers and other people, and because she has difficulty bathing at home, she takes her baths at the facility. On days when she does not go to the day service, a nurse visits to check for any deterioration of her physical condition, and a physical therapist provides rehabilitation to prevent muscle weakness. The visiting helper performs shopping and housework that the patient is no longer able to do. On weekends (every other week), a short stay of one night and two days is available to reduce the burden of caregiving on the family. This tailored care plan requires 34 service visits per month at a cost of 207,540 yen (approximately 1,384 USD at exchange rate in 2023) according to long-term care service fees set by the MHLW (73); however, as the patient pays only 10% of the total cost, the actual payment is 20,750 yen (Table 4). The care manager periodically monitors the prepared plan to ensure that it is appropriate and makes revisions when necessary. However, while the number of users of long-term care services is increasing, the number of care managers has remained flat, and the workload assigned to each care manager is growing. The shortage of staff makes it difficult to create care plans and conduct monitoring tailored to everyone, which makes the quality of care a challenge (74).
Figure 1.
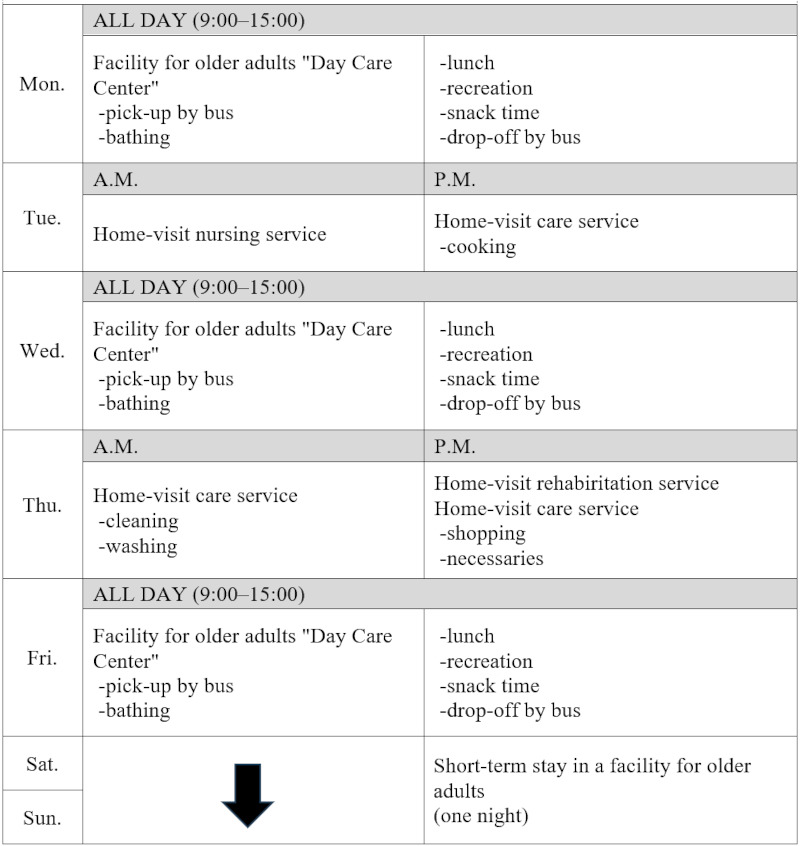
Home-based plan of a model case with dementia for a week. Patient condition: 75 years old, female, with dementia, needs someone's constant support and supervision in daily life.
Table 4. Long-term care service fee of model case*.
| Service | Unit price (JPY) | Frequency | Total (JPY) / month |
|---|---|---|---|
| Facility for older adults "Day Care Center" | 9,610 | 3 times/week | 115,320 |
| Home-care service | 3,230 | 3 times/week | 38,760 |
| Home-visit nursing service | 5,250 | Once a week | 21,000 |
| Home-visit rehabiritation service | 3,360 | Once a week | 13,440 |
| Short-term stay in facility | 9,510 | Twice a month | 19,020 |
| Total | 34 times/month | 207,540 |
*Reference (66)
As Japan's birthrate declines, and the nuclear family becomes more common, fewer family member is taking on the responsibility of caring for older adults, after that the burden on caregivers is increasing, and caregiver fatigue. In Asian countries, it is common for families to provide care for older adults at home, but it is necessary to consider the burden of caregiving when the number of children and nuclear families is declining and increasing, respectively. In recent years in Japan, in addition to the issues of elder abuse and neglect, further social problems have been drawing attention, such as the old family member to provide care for their old people. There are many issues to consider, such as what kind of care is needed, whether it can be provided as a service, and who will coordinate these services. In Japan, care managers are in charge of these tasks, but as the population ages, they must play a role in bridging medical care and welfare services and the community with individuals and families.
Area 5: Research and Development of long-term care products
Research is one of five priority areas in the Framework to provide the knowledge for the promotion of the development of prevention/diagnosis/treatment methods, rehabilitation models and nursing care system (20,21). Multiple ministries have secured substantial research funds for these purposes (75,76). To make effective use of these, various public research centers for dementia at the national level; National Center for Geriatrics and Gerontology, National Center for Neurology and Psychiatry, as well as prefecture level; Tokyo Metropolitan institute for Geriatrics and Gerontology. Furthermore, numerous medical universities, academic societies, and other research institutes exist for diverse areas of research for dementia, and industrial sectors collaborate to translate research results into the improvement of actual practices in nursing care sites. These public-academic-industry collaborations are maintained through a network supported by the Japanese government to share knowledge and information on their relevant activities (77). The lessons learned from such initiatives can contribute to the R&D on dementia in LMICs.
Innovation of products to support older adults is also an important relevant area for Asian countries. In Japan, several initiatives of innovations to support aging society have been organized such as Innovation 25 under the Prime Minister's Office and the Dementia Innovation Alliance Working Group under cross-ministerial initiatives (78,79). These initiatives accelerate R&D of products to support the lives of older adults including robot technology, life-support applications on mobile phones, and social innovations. However, most of these innovative products are not delivered and accessed by older adults in need, especially in LMICs. Therefore, several Japanese public authorities provide a variety of supports for relevant industries to expand their quality products to LMICs, including Medical Excellence of Japan under the Ministry of Economy, Trade and Industry (80), Projects for the Growth for Medical Technologies under MHLW (81), Japan International Cooperation Agency (82) and others.
However, these efforts could not satisfy the high demands from Asian countries. The National Center for Global Health and Medicine (NCGM) organized the knowledge exchange program for aging with Sri Lanka with World Bank support (83). High-level public officials visited older people care facilities expressed interest in Japanese products to reduce the burden of care givers, support the daily living and promote mental care. However, these products were usually only domestically accessible for several backgrounds. First, Japanese companies, especially small and medium-sized companies, have low interests in market expansion overseas in Asia because of their capacity and the risk. Second, if the companies have the interests, complicated processes of access and delivery of health products (84) hinder their efforts to promote their products in Asian countries. These factors include the development of products to match the usability with the local situation, accreditations by local governments, selection of the products in the authorities-approved essential service lists, functioning supply chain, and effective health systems to deliver older people care services to people in need. Public sector aid should be strengthened to promote the interests of Japanese companies and support them to overcome these possible obstacles. However, the government supports related to older people care remain insufficient. To achieve universal health care under the rapid aging of Asian countries in the future, public support should focus more on companies and organizations with the knowledge and skills in older people care to introduce their experiences and products overseas.
Discussion
This review has suggested the areas in which Japan's experience can contribute to dementia measures in LMICs. However, there are several points to consider when incorporating the Japan's approaches into LMICs. Firstly, it is important to acknowledge that Japanese policies for the older person are not universally superior or infallible. In the 1980s, when an aging population rate was around 10%, Japan had been focused on interventions in the medical care, resulting in many older adults seeking hospital care and utilizing a significant amount of healthcare resources. However, Japan acknowledged that many of the older people needed more support in their daily lives and preventive measures to maintain their health, not medical intervention, and furthermore, exercise, diet, and peer involvement were also found to be effective in the treatment of dementia (85). In addition, if the older people are healthy, they have considerable potentials to contribute to society, such as in productive activities, hobbies, and community activities (86,87). Based on these observations, Japanese government has evolved the policies that emphasizes preventive measures. In this way, Japan's policies have developed through a process of trial and error driven by necessity, resulting in their current form. Additionally, there are currently many challenges. For example, there are issues related to the insufficient number and quality of caregivers, and the burden of caregiving by family members has not yet been fully resolved.
Furthermore, it should be believed that in LMICs with diverse regions, religions, and cultures, there is the potential to establish effective mechanisms rooted in the characteristics of the country by leveraging the specificities of the nation ore territories. In LMICs, it is conceivable that there are still many community and regional leaders that Japan has already lost. These leaders taking on leadership roles in such community could assume roles similar to Japan's "Care Managers", coordinating the deployment of caregiving personnel. The development of healthcare professionals is a time-consuming endeavor. Not necessarily, there is no need to certify many occupations or establish complex training and budget systems, as is the case in Japan. Each country and territory should deploy policies tailored to its own circumstances, taking into account its customs, characteristics, and strengths.
In actually implementing the measures, it is necessary to keep the following points in mind. Firstly, based on Japan's experience and current challenges, a crucial aspect in responding to an aging society is the recognition that policy intervention is necessary before the aging rate reaches 7%, that is, before aging becomes prevalent. As it is difficult for the public to perceive the seriousness of the future super-aged society, the government needs to make decisions and initiate measures such as the establishment of legal arrangement. The second point is that stakeholders should share a common understanding that the goal in aging measures is to reduce the number of severely dependent individuals. It is important to provide people with activities such as exercise, nutrition/oral health, and communication from the healthy aging stage, rather than intervening only when care is needed. Hence, there is a need to invest in healthy aging to prevent the escalating demand in health and long-term care. Finally, to meet the needs of individual older persons, it is indispensable to adopt flexible mindsets and collaboration involving various sectors, not confined by the traditional vertical structure. While initially it may appear that measures pertaining to the older person primarily fall within the purview of healthcare, it is imperative to foster collaboration with the Ministry of Finance due to its involvement in government finances, as well as with the Ministry of Economy, Trade, and Industry for the advancement of nursing care equipment. In addition, it should be also important to build partnerships with industry and academia, involving not only government but also local businesses, universities, and volunteer organizations.
Conclusion
Through this review paper, we have proposed areas where Japan's experience in addressing aging issues can contribute to the strategies in low- and middle-income countries. However, directly transferring Japan's policies to other countries is challenging, and it is necessary to understand the uniqueness of Japan's aging policies and the considerations in their implementation. Moving forward, based on the areas discussed in this paper, we would like to examine the effects and issues involved in the transferring Japanese experience to LMICs, for supporting aging strategies.
Acknowledgements
The authors would like to express their sincere gratitude for the invaluable support and encouragement provided by Professor Shigeaki Watanuki, Dr. Chieko Ikeda and Dr. Shunji Takakura.
Funding
This research was supported by NCGM Intramural research Fund for the study design, literature review, analysis, and the necessary publication procedures.
Conflict of Interest
The authors have no conflicts of interest to disclose.
References
- 1. United Nations Economic and Social Commission for Asia and the Pacific. Asia-Pacific intergovernmental meeting on the fourth review and appraisal of the madrid international plan of action on ageing. https://www.unescap.org/events/2022/asia-pacific-intergovernmental-meeting-fourth-review-and-appraisal-madrid-international (accessed October 30, 2023).
- 2. United Nat ions. Madrid plan of act ion andits implementation. https://social.desa.un.org/issues/ageing/madrid-plan-of-action-and-its-implementation-main/madrid-plan-of-action-and-its (accessed October 30, 2023).
- 3. Hijas-Gómez AI, Ayala A, Rodríguez-García MP, Rodríguez-Blázquez C, Rodríguez-Rodríguez V, Rojo- Pérez F, Fernández-Mayoralas G, Rodríguez-Laso A, Calderón-Larrañaga A, Forjaz MJ. The WHO active ageing pillars and its association with survival: Findings from a population-based study in Spain. Arch Gerontol Geriatr. 2020; 90:104114. [DOI] [PubMed] [Google Scholar]
- 4. World Health Organization. Active ageing: A policy framework, 2002. https://iris.who.int/handle/10665/67215 (accessed October 30, 2023).
- 5. United Nations. UN decade of health ageing: Plan of action 2021-2030. N. https://www.who.int/publications/m/item/decade-of-healthy-ageing-plan-of-action (accessed October 30, 2023).
- 6. World Health Organization. Regional action plan on healthy ageing in the Western Pacific. https://www.who.int/publications/i/item/9789290619352 (accessed October 30, 2023).
- 7. Bonnet Carole CE, Fontaine Roméo. Population ageing in high-longevity countries: demographic dynamics and socio-economic challenges. Population. 2021; 2:225-325. [Google Scholar]
- 8. Nakahori N, Sekine M, Yamada M, Tatsuse T, Kido H, Suzuki M. Future projections of the prevalence of dementia in Japan: results from the Toyama dementia survey. BMC Geriatr. 2021; 21:602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Iwagami M, Tamiya N. The long-term care insurance system in Japan: Past, present, and future. JMA J. 2019; 2:67-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ozawa MN, Nakayama S. Long-term care insurance in Japan. J Aging Soc Policy. 2005; 17:61-84. [DOI] [PubMed] [Google Scholar]
- 11. Ikegami N. Financing long-term care: Lessons from Japan. Int J Health Policy Manag. 2019; 8:462-466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tamiya N, Noguchi H, Nishi A, Reich MR, Ikegami N, Hashimoto H, Shibuya K, Kawachi I, Campbell JC. Population ageing and wellbeing: lessons from Japan's long-term care insurance policy. Lancet. 2011; 378:1183-1192. [DOI] [PubMed] [Google Scholar]
- 13. Ministry of Health Labor and Welfare of Japan. Long-term care insurance in Japan. https://www.mhlw.go.jp/english/topics/elderly/care/ (accessed October 30, 2023).
- 14. Takeda A, Tanaka N, Chiba T. Prospects of future measures for persons with dementia in Japan. Psychogeriatrics. 2010; 10:95-101. [DOI] [PubMed] [Google Scholar]
- 15. Aihara Y, Maeda K. National dementia supporter programme in Japan. Dementia. 2021; 20:1723-1728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. National Center for Geriatrics and Gerontology of Japan. About the global dementia legacy event Japan. https://www.ncgg.go.jp/topics/dementia2014e/about.html (accessed October 30, 2023).
- 17. Ministry of Health Labor and Welfare of Japan. A comprehensive strategy to accelerate dementia measures (New Orange Plan), 2015. https://www.mhlw.go.jp/file/06-Seisakujouhou-12300000-Roukenkyoku/0000140379.pdf (accessed October 30, 2023). (in Japanese) .
- 18. National Center for Geriatrics and Gerontology of Japan. Overview of the Revision of the long-term care insurance system. Aichi, 2017. https://www.ilcjapan.org/linksE/doc/Overview_of_the_Revision_of_LTCI.pdf (accessed October 30, 2023).
- 19. Prime Minister's Office of Japan. Ministerial Council on the promotion of dementia care policies, 2018. https://japan.kantei.go.jp/98_abe/actions/201812/_00054.html (accessed October 30, 2023).
- 20. Kurita S. The national framework for promotion of dementia policies. Tokyo, health and global policy institute, 2019. http://japanhpn.org/en/dementia1-3-2/ (accessed October 30, 2023).
- 21. Ministry of Health Labor and Welfare of Japan. The national framework for promotion of dementia policies, 2019. https://www.mhlw.go.jp/content/000522832.pdf (accessed October 30, 2023). (in Japanese) .
- 22. Ministry of Health Labor and Welfare of Japan. The basic act ondementia to promote an inclusive society (Outline), 2023. https://www.japaneselawtranslation.go.jp/outline/92/905R510.pdf (accessed October 30, 2023).
- 23. World Health Organization. Dementia: A public health priority, 2012. https://www.who.int/publications/i/item/dementia-a-public-health-priority (accessed October 30, 2023).
- 24. Alzheimer's Disease International. World Alzheimer report 2012: Overcoming the stigma of dementia. 2012. https://www.alzint.org/u/WorldAlzheimerReport2012.pdf (accessed October 30, 2023).
- 25. Dementia Supporter Caravan. https://www.caravanmate.com (accessed October 30, 2023). (in Japanese) .
- 26. Ministry of Health Labor and Welfare of Japan. Dementia supporters ambassador, 2016. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000177874.html (accessed October 30, 2023).
- 27. Carey Mulligan aims to change global attitudes towards dementia. https://www.gov.uk/government/news/carey-mulligan-aims-to-change-global-attitudes-towards-dementia (accessed October 30, 2023).
- 28. Alzheimer's Society. Creating a global dementia friendly movement. https://www.alzheimers.org.uk/about-us/policy-and-influencing/global-dementia-friends-network (accessed October 30, 2023).
- 29. Ministry of Health Labor and Welfare of Japan. The latest strategies for promoting care prevention. Tokyo, 2023. https://www.mhlw.go.jp/content/000940062.pdf (accessed October 30, 2023). (in Japanese) .
- 30. Ministry of Health Labor and Welfare of Japan. Results of a survey on the implementation of comprehensive projects for care prevention and daily life support, 2019. https://www.mhlw.go.jp/content/12300000/000570876.pdf (accessed October 30, 2023). (in Japanese) .
- 31. Ministry of Health Labor and Welfare of Japan. The 11th extending healthy life expectancy award: List of awarded cases. https://www.mhlw.go.jp/content/10904750/001017667.pdf (accessed October 30, 2023). (in Japanese) .
- 32. Ministry of Health Labor and Welfare of Japan. Municipal manual for strengthening and promoting efforts for long-term care prevention. https://www.mhlw.go.jp/seisakunitsuite/bunya/hukushi_kaigo/kaigo_koureisha/yobou/dl/gaiyo4-1.pdf (accessed October 30, 2023). (in Japanese) .
- 33. Ministry of Education Culture Sports Science and Tehcnology of Japan. Model core curriculum for medical education in Japan. Tokyo, 2022. https://www.mext.go.jp/content/20230207-mxt_igaku-000026049_00001.pdf (accessed October 30, 2023). (in Japanese) .
- 34. Ministry of Education Culture Sports Science and Tehcnology of Japan. Model core curriculum for dental education in Japan, Revision. Tokyo, 2022. https://www.mext.go.jp/content/20230428-mxt_igaku-000029086_2.pdf (accessed October 30, 2023).
- 35. Ministry of Education Culture Sports Science and Tehcnology of Japan. Committee on human resource development in pharmaceutical sciences, Model core curriculum for pharmacist education in Japan, 2022 Revision. https://www.mext.go.jp/content/20230227-mxt_igaku-100000058_01.pdf (accessed October 30, 2023). (in Japanese) .
- 36. Ministry of Education Culture Sports Science and Tehcnology of Japan. Committee on the training of nursing personnel at universities, Model core curriculum for nursing education, 2017. https://www.mext.go.jp/component/a_menu/education/detail/__icsFiles/afieldfile/2017/10/31/1217788_3.pdf (accessed October 30, 2023). (in Japanese) .
- 37. The Japanese Society of Nutrition and Dietetics. The Japanese society of nutrition and dietetics, Report and utilization support guide for "Human resource development in the field of education and training", Human resource development project for registered dietitians by field of expertise in 2019, 2020. https://jsnd.jp/img/H29_houkoku_teisei.pdf (accessed October 30, 2023). (in Japanese) .
- 38. Japanese Society of Physical Therapy Education. Model core curriculum of physical therapy education. https://www.japanpt.or.jp/assets/pdf/activity/books/modelcorecurriculum_2019.pdf (accessed October 30, 2023). (in Japanese) .
- 39. Japanese Association of Occupational Therapists. Occupational therapy education guidelines, Occupational therapist training education model core curriculum 2019. https://www.jaot.or.jp/files/page/wp-content/uploads/2013/12/Education-guidelines2019.pdf (accessed October 30, 2023). (in Japanese) .
- 40. Ministry of Health Labor and Welfare of Japan. Advisory committee for the model core curriculum for speech therapist, Japanese Association of Speech Therapists, Training education, guidelines for speech therapist training education, 2018. https://files.japanslht.or.jp/upload_file/kyoiku_guideline_20181027.pdf (accessed October 30, 2023). (in Japanese) .
- 41. Ministry of Health Labor and Welfare of Japan. Report of the study group on improvement of curriculum of training schools for orthoptists, 2021. https://www.mhlw.go.jp/content/10800000/000878397.pdf (accessed October 30, 2023). (in Japanese) .
- 42. Ministry of Health Labor and Welfare of Japan: Report of the committee for improving the curriculum of radiological technologists school, 2019. https://www.mhlw.go.jp/content/10801000/000570857.pdf (accessed October 30, 2023). (in Japanese) .
- 43. The Japan Association for Dental hygienist education. The Japan Association for Dental Hygienist Education, Core curriculum for dental hygiene education (2022 Revision). 2022. https://www.kokuhoken.or.jp/zen-eiky/publicity/file/core_curriculum_2022.pdf (accessed October 30, 2023). (in Japanese) .
- 44. Curriculum for dental technician education. https://www.kokuhoken.or.jp/zen-eiky/publicity/file/core_curriculum_2022.pdf (accessed October 30, 2023). (in Japanese) .
- 45. Ministry of Health Labor and Welfare of Japan. Report of the committee for improving the curriculum of clinical laboratory technicians training schools, 2020. https://www.mhlw.go.jp/content/10803000/000620490.pdf (accessed October 30, 2023). (in Japanese) .
- 46. Ministry of Health Labor and Welfare of Japan. Report of the study group for improving the curriculum of biomedical equipment technician schools, 2021. https://www.mhlw.go.jp/content/10803000/000776745.pdf (accessed October 30, 2023). (in Japanese) .
- 47. Ministry of Health Labor and Welfare of Japan. Educational content and coursework leading to certification in emergency life-saving technician. https://www.mhlw.go.jp/stf/newpage_26164.html (accessed October 30, 2023). (in Japanese) .
- 48. Ministry of Health Labor and Welfare of Japan. Report of the study group on improvement of curriculum for prosthetist and orthotist school, 2021. https://www.mhlw.go.jp/content/10800000/000863157.pdf (accessed October 30, 2023). (in Japanese) .
- 49. Ministry of Health Labor and Welfare of Japan. Curriculum for social worker training program, 2019. https://www.mhlw.go.jp/content/000606419.pdf (accessed October 30, 2023). (in Japanese) .
- 50. Ministry of Health Labor and Welfare of Japan. Curriculum for the training program for certified care workers, 2018. https://www.mhlw.go.jp/content/12200000/000525760.pdf (accessed October 30, 2023). (in Japanese) .
- 51. Ministry of Health Labor and Welfare of Japan. Care manager. https://www.mhlw.go.jp/file/06-Seisakujouhou-12300000-Roukenkyoku/0000114687.pdf (accessed October 30, 2023). (in Japanese) .
- 52. Ministry of Health Labor and Welfare of Japan. Detailed rules for handling caregiver training related to training for beginning caregivers and daily living assistance workers, 2012. https://www.mhlw.go.jp/file/06-Seisakujouhou-12300000-Roukenkyoku/kaigoinnyouseikennsyuu.pdf (accessed October 30, 2023). (in Japanese) .
- 53. Ministry of Health Labor and Welfare of Japan. Curriculum for training of mental health social workers, 2019. https://www.mhlw.go.jp/content/000719741.pdf (accessed October 30, 2023). (in Japanese) .
- 54. Japanese Law Translation. Certified social worker and certified care worker act. 1987. https://www.japaneselawtranslation.go.jp/en/laws/view/2693 (accessed October 30, 2023). (in Japanese) .
- 55. Ministy of Education Culture Sports Sceience and Technology. Background and schedule of revision of model care curriculum. https://www.mext.go.jp/content/20210818-mxt_igaku-000017471_4.pdf (accessed October 30, 2023). (in Japanese) .
- 56. Science Council of Japan. Committee on Aging, Committee on Cancer and Aging Research, 935th Governing Council Meeting, 17th Period-52, May 29, 2000, Necessity of developing an education, treatment, and research system for gerontology and geriatrics 2000. https://www.scj.go.jp/ja/info/kohyo/17pdf/1752p.pdf (accessed October 30, 2023). (in Japanese) .
- 57. Arai H. Model core curriculum for medical geriatric education in medical school. Japanese Journal of Geriatrics (Nihon Ronen Igakkai Zasshi). 2010, 47:285-287. (in Japanese) [DOI] [PubMed] [Google Scholar]
- 58. Suzuki T. Evaluation of the revised model core curriculum and the future of clinical education in a 6-year pharmacy education. Japanese Journal of Pharmaceutical Education. 2022; 6:1-4. (in Japanese) [Google Scholar]
- 59. Ministry of Health Labor and Welfare of Japan. Report of the committee on pharmacist for human recourses development and qualification improvement, 2021. https://www.mhlw.go.jp/content/11121000/000799524.pdf (accessed October 30, 2023). (in Japanese) .
- 60. Toshiko M, Kanami H, Tsuyako H, Isako U. Professional nursing career development from the viewpoint of historical transitions in basic nursing education and continuing nursing education. Tokushima Bunri University Research Bulletin. 2018; 95:95-114. (in Japanese) [Google Scholar]
- 61. Japanese Nursing Association, 2. Contents of basic nursing education, Nursing in Japan 2023,. https://www.nurse.or.jp/english/assets/nursing/nursing-in-japan-en.pdf (accessed November 24, 2023).
- 62. Ministry of Health Labor and Welfare of Japan. Committee for the preparation of guidance manuals for the new curriculum for education of nurses, Guidance manual for the new nurse training curriculum, 2021. https://www.mext.go.jp/a_menu/shotou/shinkou/kango/20211111-mxt_koukou01-1.pdf (accessed November 24, 2023). (in Japanese) .
- 63. Ministry of Health Labor and Welfare of Japan. Report of the committee for improving the curriculum of medical technologists schools, 2020. https://www.mhlw.go.jp/content/10803000/000620490.pdf (accessed November 24, 2023). (in Japanese) .
- 64. Japan Association for Dental Hygienists. https://www.jdha.or.jp/en/index.html#historyhttps://www.jdha.or.jp/outline/about.html (accessed October 30, 2023). (in Japanese) .
- 65. Kobayashi T, Kubota M, Takahashi T, Nakasato A, Nomura T, Furuya J, Kondo H. Effects of tooth loss on brain structure: A voxel-based morphometry study. J Prosthodont Res. 2018; 62:337-341. [DOI] [PubMed] [Google Scholar]
- 66. Da Silva JD, Ni SC, Lee C, Elani H, Ho K, Thomas C, Kuwajima Y, Ishida Y, Kobayashi T, Ishikawa-Nagai S. Association between cognitive health and masticatory conditions: a descriptive study of the national database of the universal healthcare system in Japan. Aging (Albany NY). 2021; 13:7943-7952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Hideaki Ishibashi. Locomotive syndrome in Japan. Osteoporosis Sarcopenia. 2018; 4:86-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Nakamura K, Ogata T. Locomotive Syndrome: Definition and management. Clinic Rev Bone Miner Metab. 2016; 14:56-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Ministry of Health Labor and Welfare of Japan. Number of care workers needed based on the eighth long-term care insurance business plan. https://www.mhlw.go.jp/stf/newpage_02977.html (accessed October 30, 2023). (in Japanese) .
- 70. Ministry of Health Labor and Welfare of Japan. About introductory training for caregivers, 2018. https://www.mhlw.go.jp/content/12300000/000331389.pdf (accessed November 24, 2023). (in Japanese) .
- 71. Ministry of Health Labor and Welfare of Japan. Explanatory material for FY 2020 revision of medical payment system. 2020. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000196352_00001.html (accessed November 24, 2023) (in Japanese) .
- 72. Ministry of Health Labor and Welfare of Japan. Material for the 232nd subcommittee on long-term care benefits of the council on social seb security. Document 1: Strengthening the capacity to respond to dementia. https://www.mhlw.go.jp/content/12300000/001171209.pdf (accessed November 24, 2023). (in Japanese) .
- 73. Ministry of Health Labor and Welfare of Japan, Estimated fees for nursing care survice. https://www.kaigokensaku.mhlw.go.jp/?action_kouhyou_simulation_index=true (accessed October 30, 2023). (in Japanese) .
- 74. Ministry of Health Labor and Welfare of Japan. Study group on improving the quality of care support specialists (care managers) and their future, 2013. https://www.mhlw.go.jp/stf/shingi/2r9852000002s7f7-att/2r9852000002s7go.pdf (accessed November 24, 2023). (in Japanese) .
- 75. Ministry of Health Labor and Welfare of Japan. Overveiw of research under MHLW research fund 2022. https://www.mhlw.go.jp/english/wp/wp-hw2022/dl/summary.pdf (accessed November 24, 2023).
- 76. Japan Agency for Medical Research and Development. Research and development grants for dementia. https://www.amed.go.jp/en/program/list/14/03/001.html (accessed October 30, 2023).
- 77. Dementia Care Information Network. Overview of center. https://www.dcnet.gr.jp/ (accessed October 30, 2023). (in Japanese) .
- 78. Health and Global Policy Institute. Joining the dementia innovation alliance public and private sector working group. https://hgpi.org/en/lecture/dementiawg-1.html (accessed October 30, 2023).
- 79. Ministry of Economy Trade and Industry. Dementia innovation alliance working group. https://www.meti.go.jp/shingikai/mono_info_service/ninchisho_wg/index.html (accessed October 30, 2023). (in Japanese) .
- 80. Medical Excellence of Japan. What is Medical Excellence JAPAN?. https://medicalexcellencejapan.org/en/about/ (accessed October 30, 2023).
- 81. National Center for Global Health and Medicine. Projects for the growth of medical technologies. https://kyokuhp.ncgm.go.jp/eng/what-we-do/strategy_5/index.html (accessed October 30, 2023).
- 82. Japanese International Cooperation Agency. Public-private partnerships. https://www.jica.go.jp/english/activities/schemes/priv_partner/index.html (accessed October 30, 2023).
- 83. National Center for Global Health and Medicine. Senior officials from Sri Lanka visited BIHC for knowledge exchange program on elderly care. https://kyokuhp.ncgm.go.jp/eng/priority_areas/theme_5.html (accessed October 30, 2023).
- 84. Shimizu E, Yokobori Y, Miyazaki K, Ohara K, Fujii M, Nishioka T, Fujita N. Seven steps in the value chain of health products for equitable access and delivery in low-and middle-income countries. GHM Open. 2023, 3:1-6. [Google Scholar]
- 85. Kanamori S, Inoue S. Group exercise for adults and elderly: Determinants of participation in group exercise and its associations with health outcome. The Japanese Society of Physical Fitness and Sports Medicine. 2015; 4:315-320. [Google Scholar]
- 86. World Health Organization. Health and social care near the end of life: Can policies reduce costs and improve outcomes? https://iris.who.int/handle/10665/349803?show=full (accessed October 30, 2023).
- 87. Cylus J, Figueras J, Normand C. Will population ageing spell the end of the welfare state? A review of evidence and policy options. Copenhagen (Denmark): European Observatory on Health Systems and Policies; 2019. [PubMed] [Google Scholar]