

Abstract
Background:
Regional Centers for Occupational and Environmental Pathologies (CRPPE) are responsible for identifying possible occupational etiologies of pathologies. When an occupational origin is determined, an Initial Medical Certificate (IMC) is given to the patient to allow him to initiate a procedure for recognition as an occupational disease (OD) by his health insurance organization.
Objectives:
The main aim of this study was to investigate the outcome of occupational disease claims in patients who received an IMC delivered by the CRPPE of Lyon.
Methods:
A telephone interview was systematically conducted with patients who consulted the CRPPE for a claim for occupational disease recognition between 07/2020 and 06/2021, about six months after the consultation. It was conducted by a physician using a standardized questionnaire.
Results:
Out of 128 patients eligible for this study, 98 were included. Diseases of the respiratory system (34.7%) and cancers (28.6%) were the most common pathologies in our population. A process of OD compensation was initiated by 86 patients (87.8%). At the time of the study, the outcome was favorable for 63 patients (73.3%). Moreover, 18 patients (18.4%) wished for additional help from the CRPPE to carry out the procedures. Nine patients requested a new consultation, including five who still needed to complete the process.
Conclusion:
This study shows the benefit of a consultation by occupational disease consultants. However, difficulties still need to be solved in these procedures. Thus, the systematic follow-up of patients shows its advantages. The provision of support to carry out the process seems necessary.
Keywords: Occupational Disease, Compensation, Cancer, Interstitial Lung Disease, Medical and Social Support
1. Introduction
A disease is considered of occupational origin if it is the direct consequence of a worker’s exposure to a hazard (physical, chemical, biological, or psychological risk) or results from the conditions under which they work [1]. This definition is internationally approved. Thus, the International Labor Office (ILO) publishes and periodically updates a list of pathologies and nuisances for which a causal relationship has been established. Each country can then adapt this list to its regulations [2, 3].
In France, to be recognized as occupational and to be compensated, a disease must correspond to one of the following two systems [4]:
- The system of occupational disease tables (OD): The disease must be designated in an OD table and meet the medical, administrative, and job-related criteria detailed in the table. The disease is then considered occupational by the presumption of origin.
- The additional system for compensation: either the disease is listed in a table but it does not meet all the criteria, or the disease is not listed in a table but leads to a significant disability. The occupational origin of the disease may be recognized after the assessment of a Regional Committee for the Recognition of Occupational Diseases (CRRMP), which has to establish a direct causal link if there is a table or an immediate and essential link between the victim’s pathology and his usual working activity for pathologies not listed in any table.
This definition concerns all employees, whether the French general health insurance system or the French agricultural health insurance system covers them. For employees of the public sector, there is a specific system based on the tables of the general health insurance system.
Several scientific, administrative and parliamentary publications report a limited access to recognition and compensation of pathologies as occupational diseases in France and other European countries. This system is marked mainly by the under-reporting and under-recognition of several ODs. A literature review published in 2021 regarding these two phenomena noted, first of all, a lack of involvement of the victims in the process of recognition as an OD [5]. The reasons mentioned were a lack of information on the work-related risks they had been exposed to, lack of knowledge of their social rights, a poor health status (especially for victims suffering from pathologies requiring heavy treatment), [6] and fears of the impact on their relationship with their company or their employability. Secondly, in the event of a declaration, the victims experience medico-administrative difficulties due to a lack of understanding of the procedures of the National Health Service or difficulties in compiling the documents requested under the procedure.
Moreover, the physician who issues the medical certificate plays a central role in the recognition process. However, the question of the lack of training on the links between health and occupational exposure in most medical specialties and the overall lack of interest in occupational diseases has been raised by several studies [7-10]. Also, the frequent representation of cancers as related to lifestyle, hygiene, and smoking is an essential factor of under-recognition in OD. The authors Counil and Henry [11] have pointed out that an epidemiology focusing on lifestyle habits could more easily be used to manage a preventive action than an approach that would focus on the social determinants of health, taking into account the working conditions.
To evaluate and address these issues, several occupational risk surveillance systems contribute to assessing occupational exposures that may contribute to diseases and the visibility of these pathologies. For example, in France, the National Mesothelioma Surveillance Program (PNSM), which contributes to the estimation of mesothelioma cases and the assessment of unreported mesotheliomas, has noted a significant under-reporting of 42% of cases that did not apply for occupational disease compensation over the period 1998-2017 [12].
To better take into account occupational pathologies, Regional Centers for Occupational and Environmental Pathologies (CRPPE/Centres Régionaux de Pathologies Professionnelles et Environnementales) are expert structures that offer specialized medical and socio-professional advice. Their mission is to provide technical advice and assistance in searching for the observed pathologies’ origin and occupational etiology [13-15].
Indeed, when a patient consults CRPPE for an illness suspected of being of occupational origin, the specialist carries out an exhaustive occupational interview. If the practitioner identifies a possible link between the pathology and occupational exposure, an Initial Medical Certificate (IMC) is completed to enable the patient to initiate a procedure for recognition as an occupational disease (OD) with their health insurance organization. Then, the declaration as an occupational disease remains the patient’s initiative. Therefore, after the consultation, the practitioner who has issued the IMC has no information regarding the actual declaration of occupational disease by the patient nor its outcome if the patient does not inform him about the decision of his Primary Health Insurance.
The main objective of our study was to analyze the outcome of the procedures for recognizing occupational disease in patients who received an Initial Medical Certificate at the CRPPE of the Lyon University Teaching Hospital. The secondary objective was to identify ways to improve the care and support of patients referred to the CRPPE.
2. Methods
The study population consisted of patients who attended a consultation at the Regional Center for Occupational and Environmental Pathologies of the Lyon University Teaching Hospital (second largest university teaching hospital in France) between July 2020 and June 2021 for an assessment of the occupational origin of their disease and to determine whether to apply for recognition as an occupational disease. The inclusion criterion was the delivery of an IMC to the patient by a CRPPE physician. The requirements for non-inclusion were the absence of an IMC during consultation and a lack or refusal to respond to the telephone interview.
Following a consultation for OD at the CRPPE with delivery of an IMC, an occupational physician systematically conducted a telephone interview with all patients or their relatives. A single practitioner (Scherer Mathilde) led all the interviews in a systematic way using a standardized questionnaire in December 2021. First, the practitioner questioned the patients on whether or not they had applied for recognition as an OD by their health insurance organization. Patients were also asked if they had received the certificate in person during the consultation or by postal mail afterward. Then, if the patient had applied, the practitioner would ask about the outcome of the process and the entitlement to a possible compensation. If the health insurance organization refused, the practitioner would ask the patient why and then propose a new consultation. If the patient encountered difficulties, a further consultation was also offered to support the patient in this process. If the patient had yet to make the request, the practitioner asked them to explain why and suggested a new consultation to enable them to initiate the process. Finally, all patients were asked about their professional situation during the telephone interview and their opinion regarding the assistance provided by the CRPPE and any improvement that could be made to assist them better. As a follow-up to the first telephone interview, the practitioner conducted a second interview in June 2022 and then a third interview in November 2022 with patients still waiting for a decision from their health insurance organization to update the outcomes.
Medical-administrative data were collected in the patient’s medical file to build an anonymized database with the following variables: age, gender, level of education, socio-professional category coded in ISCO-2008 (International Standard Classification of Occupations) and NAF-2008 (Nomenclature d’Activités Française), pathology, table of declared OD, primary occupational exposure.
Descriptive analyses were performed with the statistical software R by applying a chi-square test or Fisher’s exact test when the conditions did not allow for a chi-square test, with α risk set at 5%.
This study was approved by the Scientific and Ethical Committee of the Hospices Civils de Lyon (N°22_704 on April 22, 2022). It conforms to the research methodology MR-004 and is registered in the CNIL register of the HCL (under the number 22_5704). During the telephone interview, the interviewer systematically informed patients of the study being conducted. Participants received a detailed written information note describing the study’s objectives, the nature of the data collected, and their rights, and they could oppose their participation in the study.
3. Results
During the period covered by the study, 562 patients underwent consultation at the CRPPE to assess the occupational origin of one or more pathologies and recommend a compensation procedure if it appeared to be relevant. Among them, 128 patients were eligible for our study, and we finally included 98 patients (76.6%): 26 did not respond to the phone call, 1 refused, and 3 responded to the interview but did not consent for their data to be used. The complete flowchart of this study is available in Figure 1. Table 1 shows the main sociodemographic characteristics. The mean age of the study population was 61.9 years. Most of the patients were retired (51%), while 41.8% were of working age. Most patients (84.7%) had less than a secondary education degree. It should be noted that five patients received several IMCs during the exact consultation, either for multiple associated pathologies of the same anatomic system or for a bilateral pathology. Since these IMCs were issued under the same OD table, these patients were counted only once in our data collection.
Figure 1.
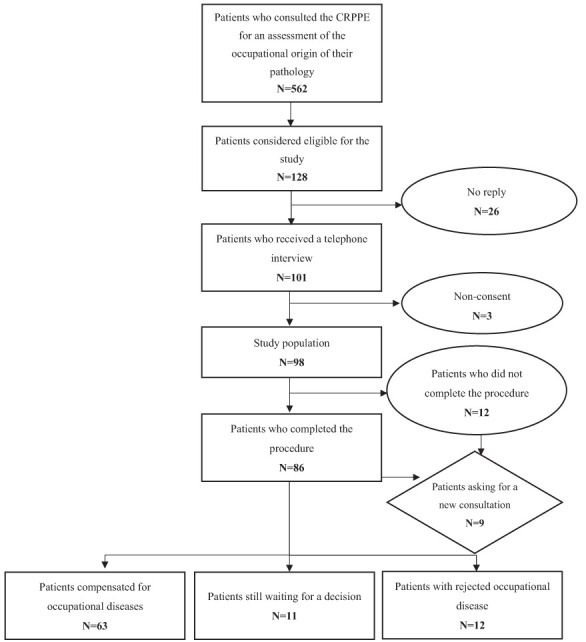
Flowchart.
Table 1.
Sociodemographic characteristics of patients.
| Caracteristics | Number (n=98) | Percentage (%) | |
|---|---|---|---|
| Age (years) | ≤49 | 12 | 12.2 |
| 50-59 | 26 | 26.5 | |
| 60-69 | 24 | 24.5 | |
| 70-79 | 27 | 27.6 | |
| ≥80 | 9 | 9.2 | |
| Sex | Male | 85 | 86.7 |
| Female | 13 | 13.3 | |
| Education | No qualification | 26 | 26.5 |
| Level 3 (GCSE) | 57 | 58.2 | |
| Level 4 (A-level) | 12 | 12.2 | |
| Level 5 (Higher national diploma) | 1 | 1.0 | |
| Level 6 (BSc/BA) | 1 | 1.0 | |
| Level 7 (MSc/MA/MBA) | 1 | 1.0 | |
| Level 8 (PhD) | 0 | 0 | |
| Employment status | Active | 36 | 36.7 |
| Looking for a job | 3 | 3.1 | |
| Disabled | 2 | 2.0 | |
| Retired | 50 | 51.0 | |
| Deceased (next of kin) | 7 | 7.1 | |
The outcomes of the occupational disease recognition procedures and their possible causes are summarized in Table 2. Of 98 patients interviewed by telephone, 86 (87.8%) had initiated the recognition process as an occupational disease with their health insurance organization. Of these, 56 patients (65.1%) had received help from a third party to complete the procedure. On the other hand, 12 patients (12.2%) had not undertaken the procedure for recognition as an occupational disease. The main reasons were administrative difficulties (33.3%) and the patient’s unwillingness to make a declaration (25%). Another reason mentioned was the death of the patient and the lack of motivation to initiate new administrative procedures by the family members.
Table 2.
The outcome of the occupational disease compensation procedure.
| Number | Percentage (%) | |
|---|---|---|
| Process completed | 86 | 87.8 |
| Positive decision | 63 | 73.3 |
| Compensated patients | 35 | 55.6 |
| Non compensated patients (ongoing) | 28 | 44.4 |
| Negative decision | 12 | 14.0 |
| Non-compliance with one or more criteria of the occupational disease table | 3 | 25.0 |
| Direct and essential association not accepted for a disease not listed in a table | 4 | 33.3 |
| Disability rate <25% for disease not listed in a table | 1 | 8.3 |
| Other situation (self-employed, unknown) | 4 | 33.3 |
| Ongoing process | 11 | 12.8 |
| Process not completed | 12 | 12.2 |
| Difficulties in applying for compensation | 4 | 33.3 |
| Patient refusal | 3 | 25.0 |
| Initial medical certificate lost | 2 | 16.7 |
| Death of the patient | 2 | 16.7 |
| Other situation / unknown | 1 | 8.3 |
In our study population, we investigated the way the IMC was delivered. 53 IMCs (54.1%) were hand-delivered at the end of the consultation and 45 (45.9%) were sent to patients by postal mail. Of the patients who completed the process, 47 had received their IMC by hand and 39 had received it by postal mail. Thus, the circumstances of delivery of the IMC did not seem to have any impact on the actual completion of the procedure (p=0.76).
Among the 86 patients who completed the procedure, 63 patients (73.3%) had their occupational disease accepted, 42 of them were assisted by a third party. However, assistance by a third party in the procedures was not significantly linked with a favorable notification (p value=0.33). In addition, 12 patients (14%) had received a negative decision regarding their occupational disease and 11 patients (12.8%) were still waiting for a decision from their health insurance organization at the time of the last telephone interview (in November 2022). It should be emphasized that 4 patients (2 having received a refusal and 2 still awaiting a decision by their health insurance office) who had at the same time filed a claim with the FIVA (Fonds d’Indemnisation des Victimes de l’Amiante / French Asbestos Victim Compensation Fund) for compensation for occupational exposure to asbestos indicated that they had received a favorable response from this organization. As a consequence, they reported that they had abandoned the procedure with their health insurance fund. As they did not receive any compensation from their health insurance organization, these 4 patients were not considered in the percentage of compensated patients.
Table 3 details the distribution of the patients according to their pathologies based on the ICD-10, grouped by OD table of the General Regime (RG) of the National Health Insurance. Asbestos diseases were the most declared diseases; it concerned 44 patients (44.9%), followed by hearing loss caused by [noise exposure (12 patients (12.2%)), silica diseases, and musculoskeletal disorders (for both 7 patients (7.1%)).
Table 3.
Classification of patients by disease according to ICD-10 and grouped by occupational disease tables defined by the National Health Insurance.
| OD Table number and declared diseases | Total Population | Patients who completed the process | Compensated patients | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| N°4 Benzene | 1 | 1.0 | 0 | 0 | 0 | 0 |
| Acute myeloblastic leukemia | 1 | 0 | 0 | 0 | 0 | |
| N°6 Ionizing radiation | 1 | 1.0 | 1 | 100 | 0 | 0 |
| Bronchial and lung cancer | 1 | 1 | 100 | 0 | 0 | |
| N°10 TER Chromium and derivate | 3 | 3.1 | 3 | 100 | 1 | 33.3 |
| Bronchial and lung cancer | 2 | 2 | 100 | 1 | 50.0 | |
| Sinus cancer | 1 | 1 | 100 | 0 | 0 | |
| N°25 Silica Diseases | 7 | 7.1 | 5 | 71.4 | 4 | 80.0 |
| Silicosis | 3 | 3 | 100 | 3 | 100 | |
| Systemic sclerosis | 2 | 1 | 50.0 | 1 | 100 | |
| Rheumatoid lung disease | 1 | 1 | 100 | 0 | 0 | |
| Pneumoconiosis of coal miners | 1 | 0 | 0 | 0 | 0 | |
| N°30 Asbestos diseases* | 30 | 30.6 | 27 | 90.0 | 21 | 77.8 |
| Pleural mesothelioma* | 6 | 6 | 100 | 3 | 50.0 | |
| Asbestos pneumoconiosis | 14 | 12 | 85.7 | 12 | 100 | |
| Pleural effusion | 2 | 2 | 100 | 2 | 100 | |
| Pleural plaque* | 6 | 5 | 83.3 | 3 | 60.0 | |
| Other specified pleural diseases | 2 | 2 | 100 | 1 | 50.0 | |
| N°30 BIS Asbestos diseases* | 14 | 14.3 | 12 | 85.7 | 10 | 83.3 |
| Bronchial and lung cancer* | 14 | 12 | 85.7 | 10 | 83.3 | |
| N°33 Beryllium | 1 | 1.0 | 1 | 100 | 0 | 0 |
| Beryllium disease | 1 | 1 | 100 | 0 | 0 | |
| N°36 Mineral or synthetic oils | 2 | 2.0 | 2 | 100 | 2 | 100 |
| Allergic contact dermatitis | 1 | 1 | 100 | 1 | 100 | |
| Irritative contact dermatitis | 1 | 1 | 100 | 1 | 100 | |
| N°42 Noise | 12 | 12.2 | 12 | 100 | 10 | 83.3 |
| Bilateral sensorineural hearing loss | 12 | 12 | 100 | 10 | 83.3 | |
| N°57 Musculoskeletal disorders | 7 | 7.1 | 5 | 71.4 | 3 | 60.0 |
| Rotator cuff syndrome | 3 | 3 | 100 | 2 | 66.7 | |
| Epicondylitis | 1 | 1 | 100 | 1 | 100 | |
| Ulnar nerve compression | 1 | 0 | 0 | 0 | 0 | |
| Carpal tunnel syndrome | 2 | 1 | 50.0 | 0 | 0 | |
| N°63 Enzymes | 1 | 1.0 | 1 | 100 | 1 | 100 |
| Allergic rhinitis | 1 | 1 | 100 | 1 | 100 | |
| N°65 Contact dermatitis | 4 | 4.1 | 4 | 100 | 4 | 100 |
| Allergic contact dermatitis | 4 | 4 | 100 | 4 | 100 | |
| N°66 Rhinitis and Asthma | 1 | 1.0 | 0 | 0 | 0 | 0 |
| Allergic rhinitis | 1 | 0 | 0 | 0 | 0 | |
| N°69 Vibrations | 1 | 1.0 | 1 | 100 | 0 | 0 |
| Hypothenar hammer syndrome | 1 | 1 | 100 | 0 | 0 | |
| N°84 Organic solvents | 3 | 3.1 | 3 | 100 | 2 | 66.7 |
| Allergic contact dermatitis | 1 | 1 | 100 | 1 | 100 | |
| Acute conjunctivitis | 1 | 1 | 100 | 1 | 100 | |
| Accidental intoxication by organic solvents and halogenated hydrocarbons | 1 | 1 | 100 | 0 | 0 | |
| Not listed diseases | 10 | 10.2 | 9 | 90.0 | 5 | 55.6 |
| Malignant tumor of the sigmoid colon | 1 | 0 | 0 | 0 | 0 | |
| Kidney cancer | 1 | 1 | 100 | 0 | 0 | |
| Bladder cancer | 1 | 1 | 100 | 0 | 0 | |
| Post-traumatic stress disorder | 1 | 1 | 100 | 1 | 100 | |
| Sleep disorders | 1 | 1 | 100 | 1 | 100 | |
| Chronic bronchitis | 1 | 1 | 100 | 1 | 100 | |
| Centro-lobular emphysema | 1 | 1 | 100 | 0 | 0 | |
| Other interstitial lung diseases with fibrosis | 1 | 1 | 100 | 1 | 100 | |
| Rheumatoid arthritis | 1 | 1 | 100 | 1 | 100 | |
| Cervical disc disease with radiculopathy | 1 | 1 | 100 | 0 | 0 | |
*4 patients (2 having received a refusal and 2 still awaiting a decision by their health insurance office) who had at the same time filed a claim with the FIVA (Fonds d’Indemnisation des Victimes de l’Amiante / French Asbestos Victim Compensation Fund) for compensation for occupational exposure to asbestos indicated that they had received a favorable response from this organization.
In addition, we analyzed the outcome of the recognition procedures for occupational disease according to the disease categories most represented in our population. The results are globally comparable to those of the total population of our study, both for the proportion of patients who have completed the procedure and for the proportion who received a positive decision. However, for the tumor subgroup (28 patients), the proportion of patients who received a favorable notification is slightly lower. Of the 24 patients (85.7%) who completed the process, 14 patients (58.3%) received a positive decision, 4 (16.7%) received a negative decision, and 6 (25%) were still waiting for a decision at the time of the last telephone interview. In comparison, patients from the diseases of the respiratory tract and noise-induces hearing loss subgroups were respectively 29 (85.3%) and 12 (100%) to complete the process among which 24 (82.8%) and 10 (83.3%) received a positive decision.
During our telephone interview, we asked all the patients included in the study population about the quality of their management at the CRPPE of Lyon. The results of this evaluation are summarized in Table 4. A great part of patients (79.6%) was satisfied with the service provided and did not suggest any improvement, while 18 patients (18.4%) declared they would have liked to benefit from additional help. The main suggestions for improvement were access to a social worker to help them with administrative procedures, but also access to a telephone help line to ask questions to a qualified person in occupational pathologies, or links with associations helping victims of occupational diseases. In addition, among the 47 patients initially identified as having difficulties to whom we proposed a new consultation, 9 patients (19.1%) agreed to this offer, in order to be accompanied in initiating or continuing their process of recognition for occupational disease.
Table 4.
Patients’ evaluation of their management at the CRPPE of Lyon.
| N (98) | % | |
|---|---|---|
| Satisfied by their care management at the CRPPE | 78 | 79.6 |
| Would have appreciated additional assistance | 18 | 18.4 |
| Appointment with a social worker | 14 | 77.8 |
| Telephonic assistance | 3 | 16.7 |
| Connection with associations | 1 | 5.6 |
| Other / do not rate | 2 | 2.0 |
4. Discussion
In this survey, 87.8% of the patients had initiated the process towards occupational disease compensation. This high rate can be explained by the fact that the CRRPE practitioner made an exhaustive occupational interview, giving the patients detailed explanations of their past occupational exposure. This enabled them to establish a link between the work performed and their pathology. In addition, the delivery of information regarding their right to claim compensation for the damage suffered and the explanations provided by health specialists in occupational diseases concerning the occupational disease claim process may also explain this high rate of patient involvement. Indeed, Gisquet et al. [16] insisted on the fact that educational and personalized information, transmitted by the doctor to the patient, on the past occupational exposure and on the existing procedures is decisive to initiate an occupational disease declaration. In their study, 83.1% of the patients for whom an occupational exposure had been identified had made the occupational disease claim. In addition, the GISCOP 93 study, carried out on patients suffering from respiratory cancers that may be work-related, found a far lower claim rate of 53%. Of these patients, 67% received compensation for occupational disease. The authors partly explain this low rate of claim by a gap between the seriousness of the disease experienced by the patients and claiming financial compensation [17, 18]. In the current study, 63 (73.3%) of the patients who completed the procedure obtained compensation for occupational disease from their health insurance company. This result is close to that of the GISCOP 93 study in which the IMCs were delivered by an experienced physician with regard to medico-administrative issues. Indeed, the wording of the IMC must be precise and include some crucial information such as the date of the first medical diagnosis of the disease [19]. However, several studies have shown that the practitioners experience difficulties in completing the IMC, as it is a medico-administrative exercise outside the purely medical field [9, 10]. In the present study, the high rate of occupational disease compensation may be linked to the fact that the initial medical certificate was properly completed by occupational pathology specialists who were fully aware of the medico-administrative subtleties.
Moreover, the CRPPE’s medical team provides a copy of the medical records that support the diagnosis of the disease, as requested by the health insurance organization. It is also suggested that the patient enclose the report of the CRPPE consultation, detailing the medical and occupational information, which provides clinical and scientific support for the compensation of the disease as an occupational disease. And yet, as noted by Anne Marchand [6], the difficulties in collecting and assembling medical documents within the framework of the procedures constitute an obstacle to obtaining compensation. Compared with the statistics of the French Health Insurance (FHI) for 2020, the rate of OD compensation in our study is higher than the average national rate of positive decisions of 65.4% among claims with complete files. However, consider the number of positive decisions on all the occupational disease declarations (including incomplete files) received by the FHI, which is much more representative of reality. In that case, the average rate drops to 55.5% [20]. However, it should be pointed out that our study population, composed mainly of diseases of the respiratory system (34.7%) and tumors (28.6%), differs from the general population claiming for occupational diseases, more than 87% of which consists of musculoskeletal disorders. The characteristics of our population can be explained by the fact that the patients referred to the CRPPE have more complex pathologies in terms of their origin than other pathologies with etiologies that are more easily identifiable by general practitioners, such as musculoskeletal disorders.
Our work follows the implementation of a collaboration between the Reference Center for Rare Pulmonary Diseases and the CRPPE, two departments of the Lyon University Hospital Center, with the objective of assessing the proportion of work-related Interstitial Lung Disease (“ILD”). This work highlighted the relevance of a dedicated occupational interview, allowing 15.6% of patients not previously identified to be eligible for a claim for occupational disease [21].
Furthermore, we find similar results to a previous study (PROPOUMON) conducted by the Léon Bérard Regional Cancer Center (CLCC) and the CRPPE of Lyon as part of a program to improve the identification and compensation of occupational lung cancers. In this series of cases, 66.7% had received a positive decision for compensation, with an initial application rate of 77.1% [22, 23]. Among patients with a tumor in our study, there is a better rate of application (85.7%) but a lower rate of acceptance as a work-related disease at 58.3%. In comparison, European statistics concerning compensation for occupational cancers in 2016 reveal that in Denmark, only 28.2% of reported cancer cases were compensated as OD. In contrast, we find a rate of 79.1% in France and a rate as high as 87.2% in Austria. However, it should be noted that comparing national statistics remains difficult. Indeed, on the one hand, there are differences in the levels and conditions of exposure between countries, affecting the number of workers exposed to occupational risks and potentially suffering from OD. On the other hand, the conditions for compensation differ from one country to another due to the diversity of insurance systems for the compensation of occupational diseases, and this has an impact on the number of cases compensated as work-related [24]. The PROPOUMON program also performed a psychosocial study highlighting the essential role played by healthcare workers in informing victims of their rights and emphasizing the need to provide more support to patients who may be victims of occupational disease in order to complete the required declaration forms and provide additional medical information [25]. This need for help is indeed found in our study, showing that most patients who had carried out the occupational disease process (76.8%) had been supported by a third party. A Spanish study also raised this need for support, in particular for cases of occupational cancers that often occur after retirement and in elderly patients, but also for patients suffering from MSDs and still in professional activity with potential consequences of the compensation process on their employment preservation [26]. Several other studies have been conducted in France by CRPPEs in collaboration with health care services [27-30]. A study conducted at the CRPPE in Grenoble, aiming to identify all occupational lung cancers followed up at the Grenoble University Hospital [27], found 20% of patients eligible for a claim for occupational disease out of a population of 305 identified. Of the 39 occupational disease claims finally filed, 77% were certified as occupational diseases. A study at the CRPPE in Rouen [28], aiming to identify occupational bladder cancers in Upper Normandy, found a 55% rate of claims. The compensation rate for these patients was about 42%.
In summary, these programs aiming at improving the identification and compensation of occupational diseases by the health insurance system show a real medico-social relevance in order to allow patients to benefit from their right to compensation and to detect and count occupational diseases. In this context, Barlet and Prete [5] call for the implementation of systems dealing with the identification and support of patients and for the implementation of sustainable cooperation between hospital services treating diseases that may have occupational etiologies and occupational disease specialists. Moreover, 12.8% of patients who had filed a claim were still waiting for a decision more than one year after their consultation at the CRPPE. The long time taken for the investigation has been described by some authors as the main reason for discouraging patients, in addition to a procedure that is unclear and even stressful for patients who are weakened by their illness [31].
Most patients (79.6%) in our study population expressed satisfaction with their care at the CRPPE of Lyon. However, a significant proportion (18.4%) of patients would have appreciated additional help. As mentioned by Benavides et al., a follow-up during the whole process of occupational disease claim and assistance by frequent contact with the patient during his interactions with the Health Insurance would be useful [26]. In our work, several suggestions have been made to improve patient care and support. Implementing telephone assistance or an appointment with a social worker is useful in helping the patients initiate and make their process of OD compensation successful.
In addition, we observed significant changes in patients’ professional activities in our study population in relation to their occupational disease. Among the 36 employed patients, only one third were working in the same position as before they claimed for their occupational disease. Hence, an appointment with a social worker at the CRPPE would allow patients suffering from occupational diseases to ensure that their medico-social rights are preserved as much as possible, but also to facilitate and sustain return to work.
5. Conclusion
This study has confirmed the value of a specific occupational disease consultation providing assessment and information on the link between occupational exposure and the pathology observed, and explaining the procedure for occupational disease claim and its challenges. However, our work has highlighted a real need for patient support after the delivery of the initial medical certificate, in order to help patients initiate and complete the claim process. The systematic follow-up of patients after the consultation for occupational diseases at the CRPPE of Lyon has demonstrated its usefulness and its continuation seems appropriate. The implementation of an appointment with a social worker would be an improvement to consider for efficient medico-social management of CRPPE patients. To our knowledge, this is the first study in France to evaluate the outcome of occupational disease compensation procedures initiated by a CRPPE. It would be interesting to scale up this project at the national level to collect more data on the outcome of OD recognition procedures undertaken within the CRPPEs and to investigate possible inequalities that might be reduced.
Author Contribution Statement:
MS contributed to the design of the study, the collection of data, the analysis of the results, and the drafting of the manuscript; CL to the analysis of the results and manuscript submission; AMP, LG, JBF, AF to data collection; BC contributed to the study design, data collection analysis of results. All authors have seen and approved the final version of the manuscript.
Institutional Review Board Statement:
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Scientific and Ethics Committee of the Hospices Civils de Lyon (N°22_704 on April 22, 2022).
Declaration of Interest:
The authors declare no conflict of interest.
References
- INRS. Social insurance for occupational risks in France. 2021 Available on: https://en.inrs.fr/prevention-in-france/social-insurance-for-occupational-risks-in-France.html. [Last Accessed 10-03-2023] [Google Scholar]
- International Labour Office (ILO) List of occupational diseases. Occupational Safety and Health Series. 2010;74:82. Available on: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_150323.pdf . [Last Accessed March 20, 2023] [Google Scholar]
- Kim EA, Kang SK. Historical review of the List of Occupational Diseases recommended by the International Labour organization (ILO) Ann Occup Environ Med. 2013;25:14. doi: 10.1186/2052-4374-25-14. Doi: https://doi.org/10.1186/2052-4374-25-14 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Article L461-1 – Code de la sécurité sociale - Légifrance [Internet] Available on: https://www.legifrance.gouv.fr/codes/article_lc/LEGIARTI000036393217. [Last Accessed 22-01-2023] [Google Scholar]
- Barlet B, Prete G. The under-recognition of occupational diseases in France. Bibliographical review of social science and public health works (1990-2020) Research report, CRD Anses/Inserm (IRIS) (in French) 2021 Available on: https://www.anses.fr/fr/system/files/Rapport-IRIS_INSERM2021.pdf . [Last Accessed 20-03-2023] [Google Scholar]
- Marchand A. Recognition and concealment of occupational cancers: the right to compensation challenged by practice (Seine-Saint-Denis) Doctoral Thesis, University of Paris-Saclay (in French) 2018 Available on: https://www.theses.fr/2018SACLE005. [Last Accessed 31-08-2022] [Google Scholar]
- Viau A, Arnaud S, Ferrer S, et al. Factors associated with physicians’ under-reporting of asbestos-related bronchopulmonary cancers. Telephone survey conducted among general practitioners and pulmonologists randomly selected in the French region of Provence-Alpes-Côte-d’Azur. Rev Prat. 2008;58:9, 16. [PubMed] [Google Scholar]
- Gehanno JF, Bulat P, Martinez-Jarreta B, et al. Undergraduate teaching of occupational medicine in European schools of medicine. Int Arch Occup Environ Health. 2014;87(4):397–401. doi: 10.1007/s00420-013-0878-5. Doi: 10.1007/s00420-013-0878-5. [DOI] [PubMed] [Google Scholar]
- Arnaud S, Cabut S, Viau A, et al. Different reporting patterns for occupational diseases among physicians: a study of French general practitioners, pulmonologists and rheumatologists. Int Arch Occup Environ Health. 2010;83:251–8. doi: 10.1007/s00420-009-0457-y. Doi: https://doi.org/10.1007/s00420-009-0457-y . [DOI] [PubMed] [Google Scholar]
- Saliba ML, Iarmarcovai G, Souville M, et al. Physicians and occupational health: a qualitative study in south-eastern France. Rev Epidemiol Sante Publique. 2007;55:376–81. doi: 10.1016/j.respe.2007.07.002. Doi: https://doi.org/10.1016/j.respe.2007.07.002 . [DOI] [PubMed] [Google Scholar]
- Counil É, Henry E. Producing ignorance rather than knowledge. Expertise in occupational health. Travail et emploi. 2016;148:5–29. Doi: https://doi.org/10.4000/travailemploi.7347 . [Google Scholar]
- Gilg Soit Ilg A, Ducamp S, Grange D, Audignon S, et al. National Pleural Mesothelioma Surveillance Programme (PNSM): twenty years of monitoring cases, their exposures and their medico-social compensation (France, 1998-2017) Bull Epidémio Hebd. 2020;12:234–43. Available on: http://beh.santepubliquefrance.fr/beh/2020/12/2020_12_1.html . [Google Scholar]
- Direction générale de l’offre de soins (2019) F10: Regional Centers for Occupational and Environmental Pathologies (CRPPE) (in French) Available on: https://solidarites-sante.gouv.fr/IMG/pdf/fiche_mig_f10_crppe.pdf. [Last Accessed 31-08-2022] [Google Scholar]
- Chapitre IX: Centres régionaux de pathologies professionnelles et environnementales (Articles R1339-1 à R1339-4) (2019) Légifrance [Internet] Available on: https://www.legifrance.gouv.fr/codes/section_lc/LEGITEXT000006072665/LEGISCTA000039426527/#LEGISCTA000039426527. [Last Accessed 31-08-2022] [Google Scholar]
- Arrêté du 16 février 2021 relatif aux centres régionaux de pathologies professionnelles et environnementales. Available on: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043173393. [Last Accessed 13-04-2023] [Google Scholar]
- Gisquet E, Chamming’s S, Pairon JC, et al. The determinants of under-reporting occupational diseases. The case of mesothelioma. Rev Epidemiol Sante Publique. 2011;59:393–400. doi: 10.1016/j.respe.2011.06.006. Doi: https://doi.org/10.1016/j.respe.2011.06.006 . [DOI] [PubMed] [Google Scholar]
- Thébaud-Mony A. Building the visibility of occupational cancers. An ongoing survey in Seine-Saint-Denis. Revue française des affaires sociales. 2008:237–54. https://doi.org/10.3917/rfas.082.0237. [Google Scholar]
- Brisacier AC, Thébaud-Mony A, Lazarus A. Physicians’ contribution to the reporting and recognition of work-related cancers in France. Doctoral Thesis, University of Paris 6 (in French) 2008 [Google Scholar]
- Bensefa-Colas L, Choudat D. Reconnaissance et réparation des maladies professionnelles en France. EMC - Pathologie professionnelle et de l’environnement. 2019;14:1–12. https://dx.doi.org/10.1016/S1877-7856(18)88532-4. [Google Scholar]
- Assurance Maladie - Risques professionnels (2021) Annual report 2020 of the Assurance Maladie. Occupational risks. Caisse nationale de l’Assurance Maladie, Paris. Available on line at: https://assurance-maladie.ameli.fr/sites/default/files/rapport_annuel_2020_de_lassurance_maladie_-_risques_professionnels_decembre_2021_0.pdf. [Last Accessed 10-03-2023] [Google Scholar]
- Carlier S, Nasser M, Fort E, et al. Role of the occupational disease consultant in the multidisciplinary discussion of interstitial lung diseases. Respir Res. 2022;23:332. doi: 10.1186/s12931-022-02257-6. Doi: https://doi.org/10.1186/s12931-022-02257-6 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varin M, Charbotel B, Perol O, et al. Propoumon project: implementation and evaluation of a systematic search for the occupational origin of bronchopulmonary cancers: validation of a self-questionnaire for identifying occupational exposure. Arch Mal Prof Environ. 2016;77:505. Doi: https://doi.org/10.1016/j.admp.2016.03.348 . [Google Scholar]
- Pérol O, Charbotel B, Perrier L, et al. Systematic Screening for Occupational Exposures in Lung Cancer Patients: A Prospective French Cohort. Int J Environ Res Public Health. 2018;15:65. doi: 10.3390/ijerph15010065. Doi: https://doi.org/10.3390/ijerph15010065 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eurogip (2018) Occupational cancer incidence and detection of occupational cancers in nine European countries. Available on line at: https://www.eurogip.fr/images/documents/5125/Eurogip-141F-Sinistralite-Reperage_cancers_professionnels_Europe.pdf . [Last Accessed on 06-09-2022] [Google Scholar]
- Britel M, Pérol O, Blois Da Conceiçao S, et al. Motivations and obstacles to occupational disease claims in lung cancer patients: an exploratory psychosocial study. Sante Publique. 2017;29:569–78. doi: 10.3917/spub.174.0569. Doi: https://doi.org/10.3917/spub.174.0569 . [DOI] [PubMed] [Google Scholar]
- Benavides FG, Ramada JM, Ubalde-López M, et al. A hospital occupational diseases unit: an experience to increase the recognition of occupational disease. Med Lav. 2019;110:278–84. doi: 10.23749/mdl.v110i4.8138. Doi: https://doi.org/10.23749/mdl.v110i4.8138 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Lamberterie G, Maître A, Goux S, et al. How do we reduce the under-reporting of occupational primary lung cancer. Rev Mal Respir. 2002;19:190–5. [PubMed] [Google Scholar]
- Audureau E, Karmaly M, Daigurande C, et al. Bladder cancer and occupation: a descriptive analysis in Haute Normandie in 2003. Prog Urol. 2007;17:213–8. doi: 10.1016/s1166-7087(07)92266-6. Doi: https://doi.org/10.1016/s1166-7087(07)92266-6 . [DOI] [PubMed] [Google Scholar]
- Legrand Cattan K, Chouaïd C, Monnet I, et al. Evaluation of occupational exposures in lung cancer. Rev Mal Respir. 2020;17:957–62. [PubMed] [Google Scholar]
- Grignoux J, Lodde B, Dewitte JD, et al. Better screening for work-related cancers: The experience of Brest University Hospital Occupational Disease Center inpatient service. Arch Mal Prof Environ. 2020;81:726. doi: 10.1016/j.bulcan.2020.01.013. Doi: https://doi.org/10.1016/j.admp.2020.03.770 . [DOI] [PubMed] [Google Scholar]
- Blum le Coat JY, Pascual M. The difficult recognition of the occupational character of mental health damages. Perspectives interdisciplinaires sur le travail et la santé. 2017 19-1: https://doi.org/10.4000/pistes.4922 . Available on line at: http://journals.openedition.org/pistes/4922. [Last Accessed 10-03-2023] [Google Scholar]