

Abstract
Background:
Neighborhood disadvantage (ND) is a risk factor for child behavior problems (CBPs), but is understudied outside the United States and Europe. Our mixed methods study aims to (1) create a culturally meaningful measure of ND, (2) test cross-sectional associations between ND and CBPs and (3) qualitatively explore life in the neighborhoods of families participating in the Salud Ambiental Montevideo (SAM) study.
Methods:
The quantitative study (Study 1) comprised 272, ~7-year-old children with geolocation and complete data on twelve behavioral outcomes (Conner’s Teachers Rating Scale – Revised Short Form: CTRS-R:S and Behavioral Rating Inventory of Executive Functioning: BRIEF). A ND factor was created at the census segment level (1,055 segments) with 19 potential indicators of ND downloaded from the Municipality of Montevideo Geographic Services. Children were assigned ND scores based on the location of their household within a census segment. Multilevel models tested associations between ND and all CBP scales, controlling for confounders at the individual level. The qualitative study (Study 2) comprised 10 SAM caregivers. Photovoice alongside semi-structured interviews in Spanish were used to foster conversations about neighborhood quality, activities, and raising children. Thematic analysis with inductive coding was used to summarize qualitative study findings.
Results:
The ND factor consisted of 12 census-based indicators related to education, employment, ethnicity, housing quality, and age characteristics, but unrelated to home ownership and some ethnicity variables. In multivariable models, ND was associated with greater conduct problems (β=1.37, p<.05), poor shifting (β=1.56, p<.01) and emotional control problems (β=2.36, p<.001). Photovoice and semi-structured interviews yielded four themes: physical disorder, recreation, safety and crime, and community resources. Residents discussed improving waste management and transportation, updating playgrounds, and ensuring neighborhood safety.
Conclusions:
ND in Montevideo comprised a unique set of census indicators. ND was primarily related to behavioral regulation problems. Hypothesized pathways whereby ND affects CBPs are discussed.
Background
Childhood behavior problems (CBPs) are an important familial, educational and societal issue with multiple levels of determinants, from exposure to environmental toxicants such as lead (1–3) to neighborhood disadvantage (ND) (4). CBPs have a bi-directional relationship with parental stress over time (5) and contribute to poor academic achievement in childhood (6), as well as unsafe sex (7) and higher consumption of alcohol (8, 9) later in adolescence. ND is an important contributor to CBPs. Studies conducted in North America and Europe demonstrate that behavior problems are more common among children living in disadvantaged neighborhoods (10–15). In these contexts, ND is specifically related to: proactive aggression (16), social-emotional problems (17), conduct problems (18, 19) and problems with self-regulation (20).
Research on ND and CBPs outside North America and Europe is lacking. This is a problem as an estimated 26% of children have poor socioemotional development in low and middle income countries (LMICs) (21). Nevertheless, inappropriate definitions or application of ND concepts in settings outside of their original development can result in misclassification of disadvantage, underestimation of effects and erroneous inferences. Mitlin and Satterthwaite (2013) argue that western definitions of poverty do not capture the extent and nature of urban poverty in other settings; revealing inconsistencies between official estimates and other indicators of urban poverty (22). For example, while 18% of Dar es Salaam’s Tanzanian population officially live in poverty, 30% of households live in one room and 70% of the population live in informal settlements (22, 23). In Pune India, 40% of residents live in poor quality housing while the official poverty estimate is 2% (24). It is important to carefully consider the conceptualization of ND in the Global South to better understand its effects on CBPs.
Sociocultural and economic differences among high and lower-income countries make the translation of North American or European indices of ND to other settings problematic, necessitating the development of context-specific metrics. In North American or European studies census-based demographic variables (e.g. ethnic composition, number of children, single parent households), poverty level, housing (e.g. ownership, monetary value, crowding), employment, and education level (25–29) are commonly included. Many studies replicate the ND factor developed by Sampson and colleagues from U.S. census variables using percentage of the population: on welfare, below poverty line, unemployed, with female headed households, African American and younger than 18 years of age (25, 26). There is little guidance on how to develop indices of ND outside of the U.S., Canada and Europe. One study based in Brazil constructed a ND index using only income level and racial composition (30) while a study in Nigeria defined ND on the basis of housing quality, employment, education, and poverty level (31). As suggested above, failure to appropriately measure ND may underestimate its impact on CPBs. Exemplar studies are needed that rigorously develop context-specific measures of ND.
Even if ND is measured adequately, there is evidence that ND operates differently depending on cultural and societal context. For example, the presence of affluent neighbors is unrelated to delinquency (school absence and teenage pregnancy) among low-income adolescents, however, the presence of low income neighbors relates to higher delinquent behaviors among affluent adolescents (32). While white children have lower negative behavior scores when residing in higher income neighborhoods, this is not the case for African American children (33). ND is related to higher substance use among African American, but not white adolescents (34). The effects of ND on academic achievement also appear stronger among adolescent immigrants compared to U.S.-born children (35). Conversely, in Germany, ND is associated with violent behavior among native-born girls compared to immigrant girls (36). Thus, cultural factors play an important role in the relationship between ND and CBPs, necessitating the evaluation of ND in different cultures and contexts.
Montevideo, Uruguay is a unique city to study the conceptualization of ND and its association with CBPs. Cities in Latin America have grown rapidly, with punctuated expansion from 1960–1970 (37–39). While population growth has slowed in recent years, urban areas continue to expand (40). For example, 95% of the Uruguayan population lives in urban centers (Montevideo primarily), up 15% since 1960 (41). This growth has resulted in formation of irregular settlements, incomplete infrastructure, and poor access to services throughout Latin America (39). In Montevideo (42) and other Latin American cities (43, 44), several studies have also linked lead exposure and behavior problems in school-age children. Yet, few studies in any setting (especially outside of North America), account for specific environmental factors, like lead exposure, in the relationship between neighborhood disadvantage and child behavior (45).
The objectives of this study were to (i) assess the construct validity of a ND factor for a South American city (Montevideo, Uruguay), (ii) test associations between ND and behavior problems in children within the first year of schooling (~ 7 years) accounting for lead exposure, and (iii) describe neighborhood characteristics and childrearing in select neighborhoods of Montevideo. Two approaches were used to address these questions. First, a quantitative analysis conducted in 2009–2011 leveraged data on the location, family characteristics, and behavior of Montevideo first-graders to inform the creation of a ND factor and test its association with CBPs. Second, a subsequent (2019) qualitative study based on semi-structured interviews and photovoice revealed caregivers’ views of Montevideo neighborhoods.
Methods
Study 1 – Quantitative
Study Sample
The current study utilizes a cross sectional sample of first-grade children from Montevideo (n=357). Families were recruited between July 2009 and August 2013 from neighborhoods with known or suspected exposure to heavy metals. Eleven primary schools located in these areas and serving low-middle income populations agreed to participate in the study, as described in detail elsewhere (46). Primary caregivers, mostly mothers, provided written consent before enrolling into the study. Protocols were approved by the participating universities. Of the children enrolled into the study, 342 had complete geo-located addresses (96%). Of those, 272 (80%) had complete data on all child behavior rating scales, comprising our final analysis sample. We also assessed selection bias by testing mean differences in ND factor(s) between children with and without behavior rating scales.
Measures
Child Behavior Rating Scales
Our primary outcomes were the subscales from the Spanish versions of the Conners’ Teachers Rating Scale – Revised, Short Form (CTRS-R:S-28 items) (47, 48) and the Behavior Rating Inventory of Executive Function (BRIEF–86 items) (49). Teachers rated children’s behavior in the previous month with the CTRS-R:S and in the previous 6 months with the BRIEF. The CTRS-R:S yields four scales: conduct problems, hyperactivity, cognitive problems and an attention deficit hyperactivity disorder (ADHD) index, which have excellent internal consistency, 0.87–0.95 (50). The BRIEF yields eight scales under two domains: behavioral regulation – (inhibit, shift, emotional control) and metacognition – (initiate, working memory, planning and organizing, organization of materials, and monitoring). The internal consistency for these scales is also excellent, 0.80 to 0.98 (51). For all scales, age and sex-specific T-scores were derived. For both CTRS-R:S and BRIEF, higher T-scores indicate greater behavior problems.
Neighborhood Disadvantage
Aggregated variables and shapefiles from the 2011 census were downloaded from the Municipality of Montevideo Geographic Services (IMSG) website (52). Census data was collected by Uruguayan government officials who visited homes to administer questionnaires and perform inspections (53). The polygons in the shapefile are census sections, 1055 of which are inhabited and delimited by roads or natural boundaries. The average population size for these census sections is 1,241 persons (5th – 95th percentile: 174–2,324). The average area is 497 square meters (range 145–18,822). For this study, all population and housing based variables were divided by the total population or total homes in the census section to account for variability in population density.
Biomarkers: Blood Lead Levels (BLL), Hemoglobin and Serum Ferritin
Children underwent a blood draw, performed by a phlebotomist after an overnight fast during the morning hours, between 8 and 11am. Blood samples were collected in lithium heparin coated tubes, stored, transported, and analyzed for lead as described previously using Atomic Absorption Spectrometry (AAS, VARIAN SpectrAA-55B) with graphite furnace or flame ionization (depending on sample volume) (54). Approximately 28% of samples were analyzed using flame ionization and 72% were analyzed with graphite furnace. The limit of detection was 1.8 μg/dL for flame ionization and 0.7 μg/dL for graphite furnace. BLL was included as a model covariate given the strong body of literature linking lead exposure to CBPs, with laboratory analytic method added to statistical models to account for differences in LOD. During blood draw, a drop of blood was taken to measure hemoglobin concentration using a portable hemoglobinometer (HemoCue, Lake Forest, CA). Blood drawn into a separate tube yielded serum that was shipped to the Department of Nutritional Sciences, Pennsylvania State University where serum ferritin (a circulating iron storage protein and an indicator of iron status) was measured. Greater detail on laboratory methodology has been published elsewhere (55).
Other Covariates and Confounders
Children’s IQ was measured using the Woodcock-Muñoz Battery, which yields a general intellectual ability (W-M GIA) score (56). A HOME score was derived from the Home Observation for Measurement of the Environment Inventory (57) and was collected by a social worker who visited the homes of the participants, or, in the case of 32 families in the study sample, from a questionnaire-based assessment administered to the caregivers. HOME score is a measure of household enrichment, with higher scores indicating greater environmental enrichment. Details concerning the administration of the W-M GIA and the derivation of the HOME scores were provided previously (54, 58). Number of household possessions of wealth was derived via principal component analysis of reported household items (i.e. TV, car, dishwasher, cellphone) (59). Demographic information including parental occupational exposure to heavy metals, variable income status, mother’s age, education, employment status, number of children less than 5 years of age in the household, proportion of persons per bedroom in the household (household crowding), child’s age, and child’s sex were obtained via parental questionnaire. Children’s height and weight were recorded. Body mass index (BMI) and height for age z-scores (HAZ) were derived from these data points.
Statistical Analysis
Exploratory factor analysis (EFA) was performed using variables collected from the 2011 Uruguayan census at the census segment level (1,055 segments). Measures of sampling adequacy (MSA) were generated for each census variable to determine significant covariation with other census variables. Census variables with MSA values below 0.50 were excluded, as this level indicates non-meaningful covariation with other variables (60). Kaiser-Meyer-Olkin (KMO) sampling adequacy criterion was used to test for a significant number of factors in the census dataset. A KMO value above 0.60 is considered adequate (61). Bartlett’s test of sphericity was also used to test if the correlations between census variables are not due to chance alone (62). For the EFA, parallel analysis was utilized to determine the number of factors to be extracted (63).
Next, confirmatory factor analysis (CFA) was implemented to determine how well the resulting factor(s) fit the data. Comparative fit index (CFI), Tucker Lewis index (TLI) and standardized root mean squared residual (SRMR) were used to determine how well the factor(s) model fit the data. CFI and TLI greater than 0.95 and SRMR less than 0.08 indicated good model fit (64). Factor values were subsequently assigned to participants based on the census section wherein their home address is located. This is a common factor assignment technique (28, 29).
Construct validity was tested using spearman correlations and t-tests. First, we hypothesized moderate negative correlations between ND and: mother’s education, mother’s age, HOME score, and number of household possessions of wealth. We hypothesized moderately positive correlations between the ND factor and: child BLL, number of children less than five in the household and household crowding. We further hypothesized greater ND among parents who smoke, parents with variable income and parents with occupational exposure to heavy metals.
Finally, we tested the association of our ND factor(s) with each of the behavior problem scales separately. A directed acylic graph (DAG) was used to select confounders from the following variables: BLL, lead analytic method, hemoglobin, serum ferritin, W-M GIA, BMI, HAZ, parental smoking status, mother’s unemployment status, mother’s education in years, mother’s age, number of children less than five years of age in the household, whether the family has a variable income, parents’ occupational exposure to heavy metals (Yes/No), HOME score, household crowding (proportion of persons per bedroom in household), family variable income (Yes/No), number of household possessions of wealth, child’s age (in months), sex, and year of study consent. The DAG retained the following covariates to be included in Model 1: household crowding, HOME score, mother’s age, mother’s education, mother’s unemployment status, parent occupational exposure to heavy metals and number of household possessions of wealth. Child age, sex and year of study consent were also retained as covariates to account for variation in behavior problems across these variables. In Model 2, biomarkers (BLL, lead analytic method, serum ferritin and hemoglobin) were further added as covariates.
Because our sampling scheme involved participants clustered within neighborhoods, we used multilevel analyses. Variation in behavior problem scales across census segments was reported using intraclass correlation coefficients (ICCs) in intercept only models. All variables were centered at the grand mean. Full information maximum likelihood accounted for missing level 1 covariate data. All multilevel analyses were conducted in Mplus (65).
Study 2 – Qualitative
A qualitative study was conducted among a convenience sample of 10 caregivers selected from the Salud Ambiental Montevideo (SAM) longitudinal cohort study. Approximately 30% of children in Study 1 continue to be followed-up long term as part of the longitudinal cohort. The qualitative method used was photovoice with semi-structured interviews. Photovoice is a method whereby participants take pictures of their environment and describe the meaning of these photos to researchers. The study was conducted during July and August 2019.
Study Recruitment and Overview
Participants already enrolled in the SAM study were recruited via a phone call, during which they were informed about the nature of the qualitative study. If the participant indicated interest, a brief home visit was scheduled to provide a study flyer, consent forms, photovoice guide and, a more complete explanation of the study. Once consent was granted, participants received a basic digital camera (which they kept after study completion as a token of appreciation for their participation), an explanation of the kinds of photos that should be taken, and a short demonstration of how to use the camera if needed. The photovoice guide provided prompts like: “Think about what you want to tell us about your neighborhood. What matters to you? Is there an object or place that represents what you are trying to convey?” along with instructions on how to take the photo like: “Keep the sun to your back”, and “Make sure the main subject of the photo is clear and easy to see!”. Participants were instructed not to take photos of persons to maintain privacy. Participants were asked to take at least 4 photos during a 1-week period. Finally, a follow-up meeting was scheduled for the photovoice and semi-structured interview. Recruitment, informational materials and semi-structured interviews were conducted in Spanish.
Procedures and Instruments
The photovoice and semi-structured interviews were completed at the Catholic University of Uruguay in a research room that provided privacy. Interviews were conducted by a native-Spanish speaker with university training in anthropology and a deep familiarity with Montevideo. The recorded interviews lasted between 60 and 90 minutes. Participants were provided with refreshments to make the interview more comfortable. The semi-structured interview was conducted first, using facilitating, open-ended questions such as: “Tell me about your neighborhood”, “Tell me what you and your family do in your neighborhood”, “Tell me what you would change about your neighborhood”, and “In what ways is your neighborhood good for raising children?”.
Participants were also provided with a black and white map of the area surrounding their house. The map included the unmarked location of their home along with street names, railroads and bodies of water. All maps were set to approximately the same scale (~1:10,000–15,000cm – 1 centimeter of the map corresponds to 100–150-meter distance). Participants were asked to draw the boundaries of their neighborhood, and the map facilitated discussion about neighborhood features.
After the semi-structured interview, participants selected and described at least four photos. In this process, they were given prompts: “What is happening in your photo?”, “Why did you take a picture of this?” and “What is the story behind this photo?”. All photos were saved to a password-protected study folder; interviews were transcribed in Spanish from the recordings and transcriptions were saved for later analysis.
Photovoice and semi-structured interviews underwent thematic analysis (66) by a single coder. Themes were generated from an inductive coding approach. Transcripts were coded until a point of saturation was reached where no new themes emerged. Subsequently, to assess the rigor of the themes generated, a keyword search for each theme was performed on the remaining transcripts. Keywords were generated using derivatives and synonyms of the codes comprising each theme. As an additional test of rigor, all themes were required to be discussed by at least half of the research participants and be the subject of at least two corresponding photographs by separate participants.
Results
Study 1
Sample characteristics
Descriptive statistics for the sample can be found in Table 1. The sample was 56% male and approximately 7 years of age (81 months). Children came from families generally considered to have low-medium SES. The median number of household possessions of wealth (i.e. TV, car, cellphone) was 4 (range: 0–5) and median maternal education was 8 (range: 4–17) years. Mean ± SD BLL was 4.1±2.2 μg/dL.
Table 1.
Characteristics of the Sample (n=272) with Number of Missing Values
| Variables | Statistic | Number Missing |
|---|---|---|
| Child Sex, % Male | 56% | 0 |
| Child Age in Months, Mean (SD1) | 81.32 (6.36) | 0 |
| Child BMI2, Mean (SD) | 16.87 (2.60) | 11 |
| Child HAZ3, Mean (SD) | 0.47 (1.04) | 13 |
| Child W-M GIA4 Score, Mean (SD) | 472.75 (11.97) | 7 |
| Child Blood Lead Level (BLL) μg/dL5, Mean (SD) | 4.12 (2.17) | 20 |
| BLL Method, % Graphite Furnace | 75% | 21 |
| Child Hemoglobin, Mean (SD) | 13.22 (1.06) | 15 |
| Child Serum Ferritin, Mean (SD) | 37.93 (37.02) | 26 |
| % Parental Smoking Status | 53% | 29 |
| Mother’s Education Years, Mean (SD) | 8.88 (2.66) | 7 |
| Mother’s Age Years, Mean (SD) | 33.26 (6.14) | 25 |
| % Mother Unemployed | 66% | 16 |
| Proportion of Household Crowded, Mean (SD) | 1.95 (0.74) | 29 |
| Number of Possessions of Wealth, Mean (SD) | 3.47 (1.16) | 27 |
| HOME Score, Mean (SD) | 43.99 (8.30) | 10 |
| Number of Children < 5 Years in Household, Mean (SD) | 0.34 (0.47) | 43 |
| % Variable Income | 53% | 32 |
| % Parental Occupational Exposure to Heavy Metals | 25% | 0 |
| Year of Study Recruitment | 0 | |
| % 2009 | 15% | |
| % 2010 | 32% | |
| % 2011 | 10% | |
| % 2012 | 26% | |
| % 2013 | 17% | |
| CTRS-R:S Conduct Problems T-Score, Mean (SD) | 53.63 (13.47) | 0 |
| CTRS-R:S Hyperactive Behaviors T-Score, Mean (SD) | 54.03 (11.62) | 0 |
| CTRS-R:S Cognitive Problems T-Score, Mean (SD) | 54.09 (12.65) | 0 |
| CTRS-R:S ADHD Index T-Score, Mean (SD) | 54.47 (11.39) | 0 |
| BRIEF Inhibit T-Score, Mean (SD) | 53.35 (11.80) | 0 |
| BRIEF Shift T-Score, Mean (SD) | 54.19 (11.50) | 0 |
| BRIEF Emotional Control T-Score, Mean (SD) | 54.92 (13.94) | 0 |
| BRIEF Initiate T-Score, Mean (SD) | 58.17 (14.74) | 0 |
| BRIEF Working Memory T-Score, Mean (SD) | 57.88 (14.25) | 0 |
| BRIEF Planning and Organizing T-Score, Mean (SD) | 57.17 (15.07) | 0 |
| BRIEF Organization of Materials T-Score, Mean (SD) | 53.66 (11.47) | 0 |
| BRIEF Monitoring T-Score, Mean (SD) | 55.94 (13.04) | 0 |
SD – standard deviation,
BMI – Body Mass Index,
HAZ – Height for age z-score,
W-M GIA - Woodcock Munoz general intellectual ability IQ score,
μg/dL – micrograms per deciliter
Neighborhood Disadvantage Factor
Supplemental Table 1 lists the census variables obtained from Montevideo municipality website, their correlations and descriptive statistics. Access to this table is available through Open Science Framework (https://osf.io/72kaj/). Census variables with an MSA value below the 0.50 cut-off (indicating no significant covariation with other variables) were removed from the EFA. The KMO value generated from the final set of census variables was 0.89, indicating a significant number of factor(s) in the dataset. Bartlett’s test of sphericity (χ2=7,486.8, df=66, p<.001) indicated that covariances between census variables were not due to chance alone. In sum, both KMO and Bartlett’s test of sphericity suggested that EFA was warranted.
Parallel analysis indicated two factors could be extracted. However, the two factor solution was difficult to interpret and the eigenvalue for the second factor (1.36) was only marginally larger than the random eigenvalues generated from parallel analysis for the second factor (1.13). Therefore, one factor was estimated and termed the “ND factor”. The final variable list and factor loadings can be found in Table 2. Higher factor scores indicate greater ND.
Table 2.
Exploratory Factor Analysis – Factor Loadings for the ND Factor, Based on 2011 National Census Variables Using a One Factor Solution
| ND1 Factor | |
|---|---|
| Education | |
| Average Years of Education ≥ 21 Year-Olds | −0.78 |
| % 3–4 Year-Olds Not Attending Preschool | 0.78 |
| % 6–11 Year-Olds Not Attending School | 0.33 |
| % 12–17 Year-Olds Not Attending School | 0.86 |
| % 21–65 Year-Olds Never Attended School | 0.41 |
| % Households With Average Education <9 Years | 0.96 |
| Employment | |
| % Unemployed (≥14 Yrs. of Age) | 0.34 |
| Ethnic Composition | |
| % with Indigenous Ancestry | 0.38 |
| % with African Ancestry | 0.76 |
| Housing Quality | |
| % Households with 3 or more UBNs2 | 0.41 |
| Demographic Characteristics | |
| % of Population 0–14 Yrs. of Age | 0.83 |
| % of Population ≥65 Yrs. of Age | −0.71 |
Neighborhood Disadvantage;
Unsatisfied Basic Needs
We used confirmatory factor analysis to evaluate the model fit of a single factor on the data and generate the ND factor. The original model had less than adequate model fit (CFI=0.86, TLI=0.83, SRMR=0.06). Based on modification indices, 21 residual covariances between census variables were added to improve model fit. The final model fit the data well (CFI=1.0, TLI=0.99, SRMR=0.02). A map of the ND factor, including sampled participants is provided in Figure 1.
Figure 1.
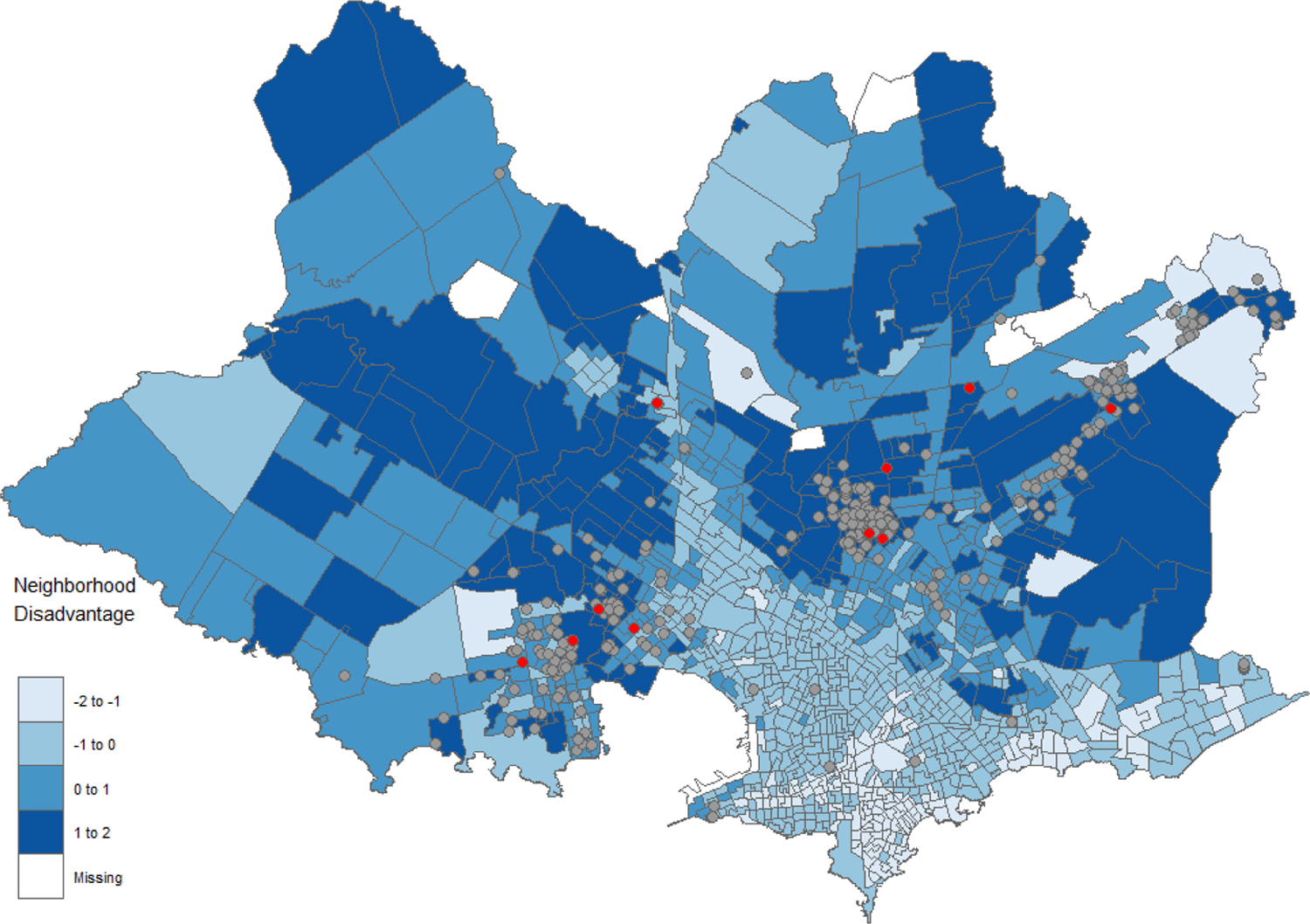
ND Factor Scores1 and Distribution of study Participants2 Across 1,055 Census Segments in Montevideo, Uruguay
1Darker census segments indicate more disadvantage; 2Study 1 participants plotted in grey and Study 2 participants in red.
As hypothesized, ND was negatively correlated with maternal education (rho=−0.24, p<.001, n=265), maternal age (rho=−0.13, p<.05, n=247), HOME score (rho=−0.23, p<.001, n=262), and number of household possessions of wealth (rho=−0.22, p<.001, n=245). ND was positively correlated with number of children below five years of age in the household (rho=0.22, p<.001, n=229) and marginally associated with the proportion of persons per bedroom (rho=0.12, p=0.05, n=243). Contrary to hypothesis, ND was not associated with child BLLs (rho=−0.04, p=0.56, n=252). Furthermore, ND was not greater among children with parents who smoke (t241 = −1.22, p=0.89, n=243), among parents with variable income (t238=−1.88, p=0.97, n=240), or parents with occupational exposure to heavy metals (t270=0.29, p=0.39, n=272).
Association of Neighborhood Disadvantage and Child Behavior Problems
Children with behavior data lived in slightly more disadvantaged neighborhoods compared to those who were excluded from analysis due to missing data (t340=−2.41, p=0.02, n=342). We included unadjusted regression coefficients between all covariates and each child behavior rating scale in the Supplemental Table 2 (https://osf.io/72kaj/). ND was tested for associations with behavior scores on the CTRS-R:S and BRIEF in multilevel models (Table 3) among children with behavior data (n=272). Skewness of behavior outcomes ranged from 0.39–1.7 and kurtosis ranged from 1.9–5.9. Our sample drew from 131 of the original 1,055 census segments within the city of Montevideo. On average there were 2.6 (range: 1–19) observations per census segment. The intraclass correlation coefficient (ICC) ranged 0.01–0.06 indicating that variation between neighborhoods on behavior scores was very low. Because ICCs as low as 0.01 and average cluster sizes as low as 2 can increase Type I error rate (67, 68), we decided to use multilevel models Robust maximum likelihood was used to obtain robust standard errors.
Table 3.
Multilevel Models: Association of ND on CBPs (n=272)
| Model 1 | Model 2 | |
|---|---|---|
| Behavior Rating Scale (T-Score) | (Beta) (CI)1 | (Beta) (CI)1 |
| CTRS-R:S Conduct Problems | 1.37 (0.23, 2.50)* | 1.19 (0.03, 2.35)# |
| CTRS-R:S Hyperactive Behaviors | 0.40 (−0.78, 1.57) | 0.39 (−0.81, 1.58) |
| CTRS-R:S Cognitive Problems | 0.19 (−0.80, 1.18) | 0.01 (−1.01, 1.02) |
| CTRS-R:S ADHD Index | 0.46 (−0.74, 1.67) | 0.39 (−0.93, 1.70) |
| BRIEF Inhibit | 0.52 (−0.52, 1.56) | 0.53 (−0.61, 1.66) |
| BRIEF Shift | 1.56 (0.67, 2.44)** | 1.35 (0.44, 2.27)* |
| BRIEF Emotional Control | 2.36 (1.28, 3.43)*** | 2.24 (1.08, 3.40)*** |
| BRIEF Initiate | 0.98 (−0.23, 2.19) | 0.82 (−0.46, 2.10) |
| BRIEF Working Memory | 0.39 (−0.87, 1.66) | 0.27 (−1.01, 1.64) |
| BRIEF Planning and Organizing | 0.83 (−0.37, 2.04) | 0.63 (−0.82, 2.08) |
| BRIEF Organization of Materials | 0.21 (−0.86, 1.28) | 0.20 (−0.86, 1.25) |
| BRIEF Monitoring | 0.58 (−0.61, 1.76) | 0.49 (−0.84, 1.82) |
CI – 95% confidence interval
p<.10,
p<.05,
p<.01,
p<.001
Model 1 covariates: household crowding, HOME score, mother’s age, mother’s education, mother’s unemployment status, parent occupational exposure to heavy metals, number of possessions of wealth, child age, child sex and year of study recruitment
Model 2 additional covariates: child BLL, lead analytic method, child serum ferritin and child hemoglobin
In model 1 (biomarkers not included as covariates), one standard deviation difference in ND factor was statistically associated with 1.37 (0.23–2.50) points higher conduct problems on the CTRS-R:S. One standard deviation difference in ND was also associated with 1.56 (0.67–2.44) and 2.36-point (1.28–3.43) higher behavior problems scores on the BRIEF shift and emotional control scores, respectively. ND was not associated with hyperactivity, cognitive problems or ADHD Index on the CTRS-R:S nor the inhibit, initiate, working memory, planning and organizing, organization of materials and monitoring scales of the BRIEF. After adjustment for biomarkers (BLL, serum ferritin and hemoglobin) in model 2, the associations of ND with conduct problems (1.19, 0.03–2.35), shift (1.35, 0.44–2.27) and emotional control (2.24, 1.08–3.40) scores remained, but were somewhat attenuated.
Study 2
Ten participants were sampled from eight different neighborhoods across Montevideo. One father, eight mothers, and one grandmother participated. The average age of the participants was 38 years. Five participants reported living in their current neighborhood for their entire life. The average area of the perceived neighborhood was approximately 1,100 square meters (range: 100–3,500 m2). One participant did not provide their perceived neighborhood boundary. Eight participants were from census segments at least one standard deviation above the mean ND value, indicating that the majority of our sample came from disadvantaged neighborhoods.
When discussing the meaning of the word ‘neighborhood’, participants often mentioned people, social connections and values shared by the community. “The neighborhood is a group of people…how you live, how you get along with the neighbors…that’s a neighborhood” (ID 2). ‘Neighborhood’ also reflected a sense of permanence: “[Neighborhood is] where you grew up, the area you know.” (ID 9). Many participants reported that they liked living in their neighborhood: “I wouldn’t live anywhere else. I’m used to it. I wouldn’t see myself in another neighborhood.” (ID 7). There was a sense of connection to neighbors and a quietude or peacefulness referenced. Participants perceived lack of safety as something separate from the community: “[I live there because] it is close to everything: my family, the neighborhood where I grew up, everything…While it is an unsafe neighborhood, nothing ever happened to me personally.” (ID 9).
Four broad themes emerged: physical disorder, recreation, safety and crime, and community resources. All themes, along with explanations and keywords, can be found in Table 4.
Table 4.
Qualitative themes from photovoice and semi-structured interviews.
| Themes: Keyword Examples | Theme Description | Referenced the Theme with Photovoice n (%) |
|---|---|---|
| Physical Disorder: trash, garbage, garbage bin, waste, smell, broken | Primarily relates to deterioration of physical aspects of the neighborhood including: buildings, streets, plumbing and waste disposal. | 8 (80%) |
| Recreation: play, sport(s), soccer, basketball, bike(s), playground, field, court | Any aspect where the neighborhood facilitates recreation including the location and types of leisure activities. Examples could be playgrounds, but also references to children playing in the street. | 7 (70%) |
| Safety and Crime: gang(s), gunshot, shooting, theft, stealing, safety, drugs police | References to violent or other criminal behavior in the neighborhood. Also pertaining to responses by the police. | 3 (30%) |
| Community Resources: hospital, clinic, community center, food outlet, shopping, transportation, bus stop, supermarket, church | Interaction, prevalence, utilization and condition of community resources. Community resources include but are not limited to: roads, hospitals, bus-stops, supermarkets and churches. | 6 (60%) |
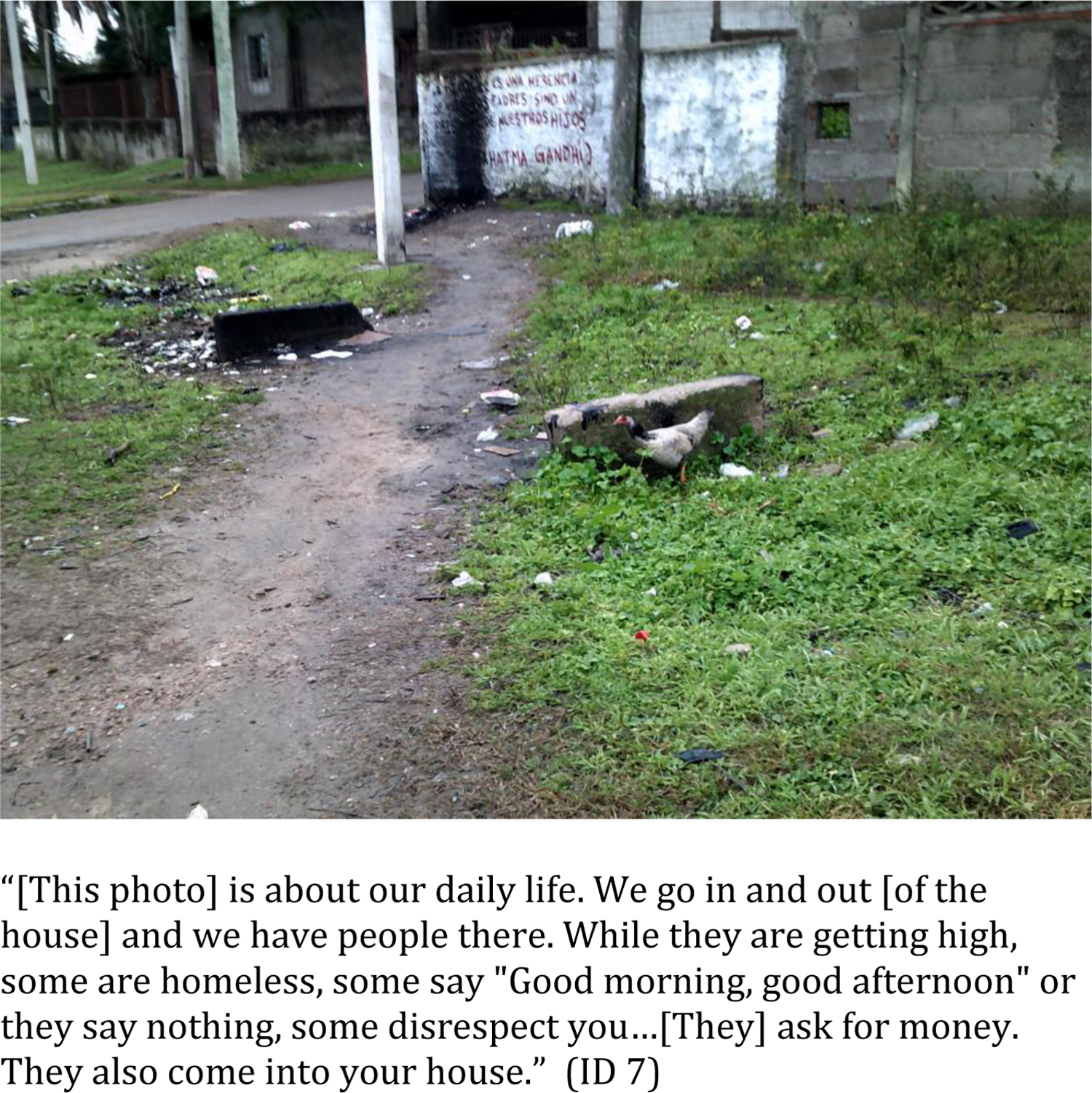
Theme 1: Physical Disorder
Interviewees mentioned problems with waste disposal, littered streets, flooding or broken pipes. Many photographed garbage in the streets and streams. Participants saw trash as a safety concern. They mentioned children playing in gutters with polluted water. Burning trash was also a concern: “Another thing they do is burn trash…My husband and I put it [the fire] out and then we go home to bathe because the smell that remains is horrible.” (ID 10).
Some caregivers proposed that the local community did not have collective will to clean the garbage: “Nobody cares…if it is like this or not because nobody works together” (ID 6). Suggested ways to improve the problem included more garbage containers and careful waste disposal by garbage collectors: “Containers or something to improve the environment there.” (ID 8). Photos related to physical disorder or infrastructure improvements are found in Figure 2.
Figure 2.
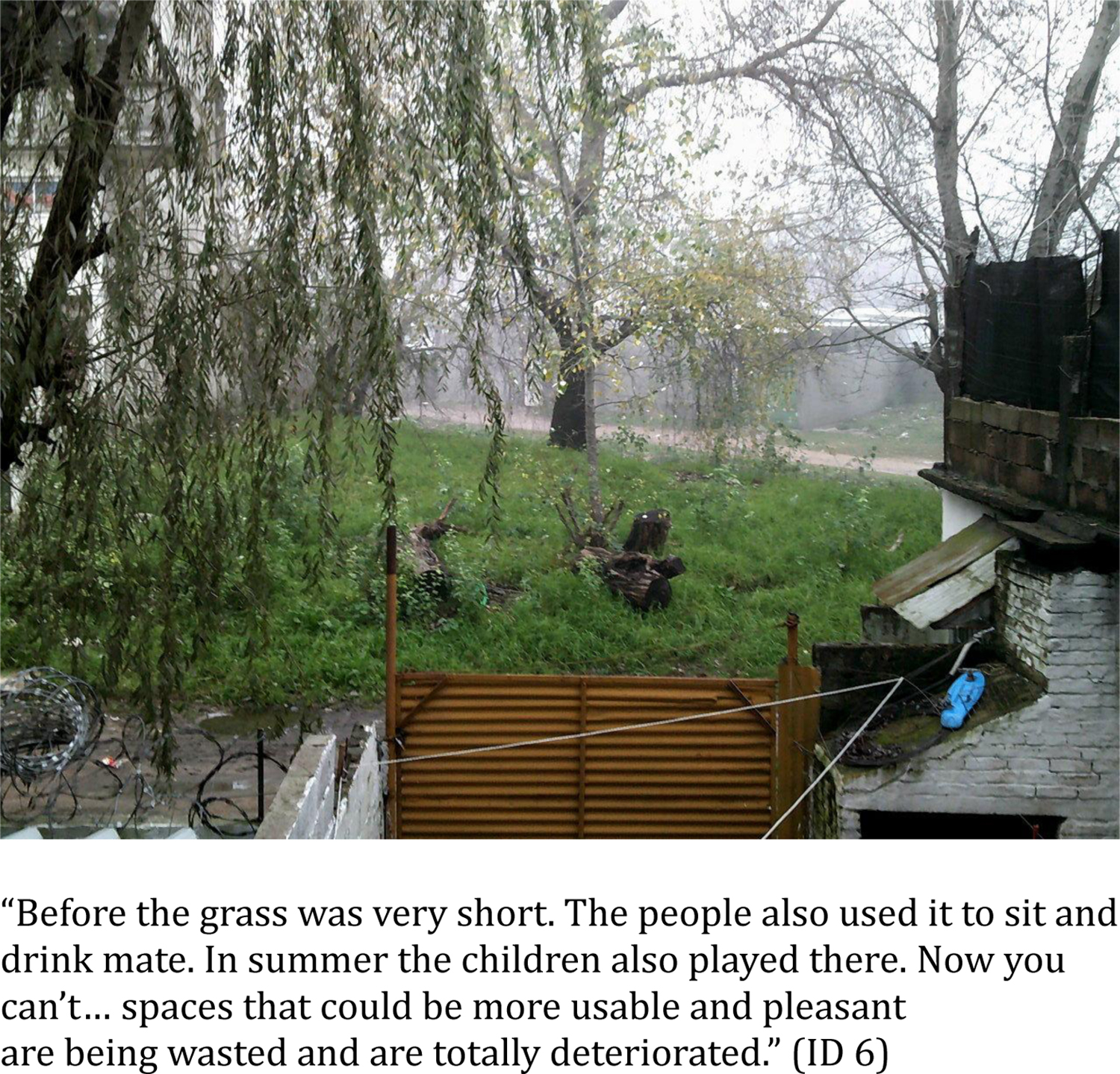
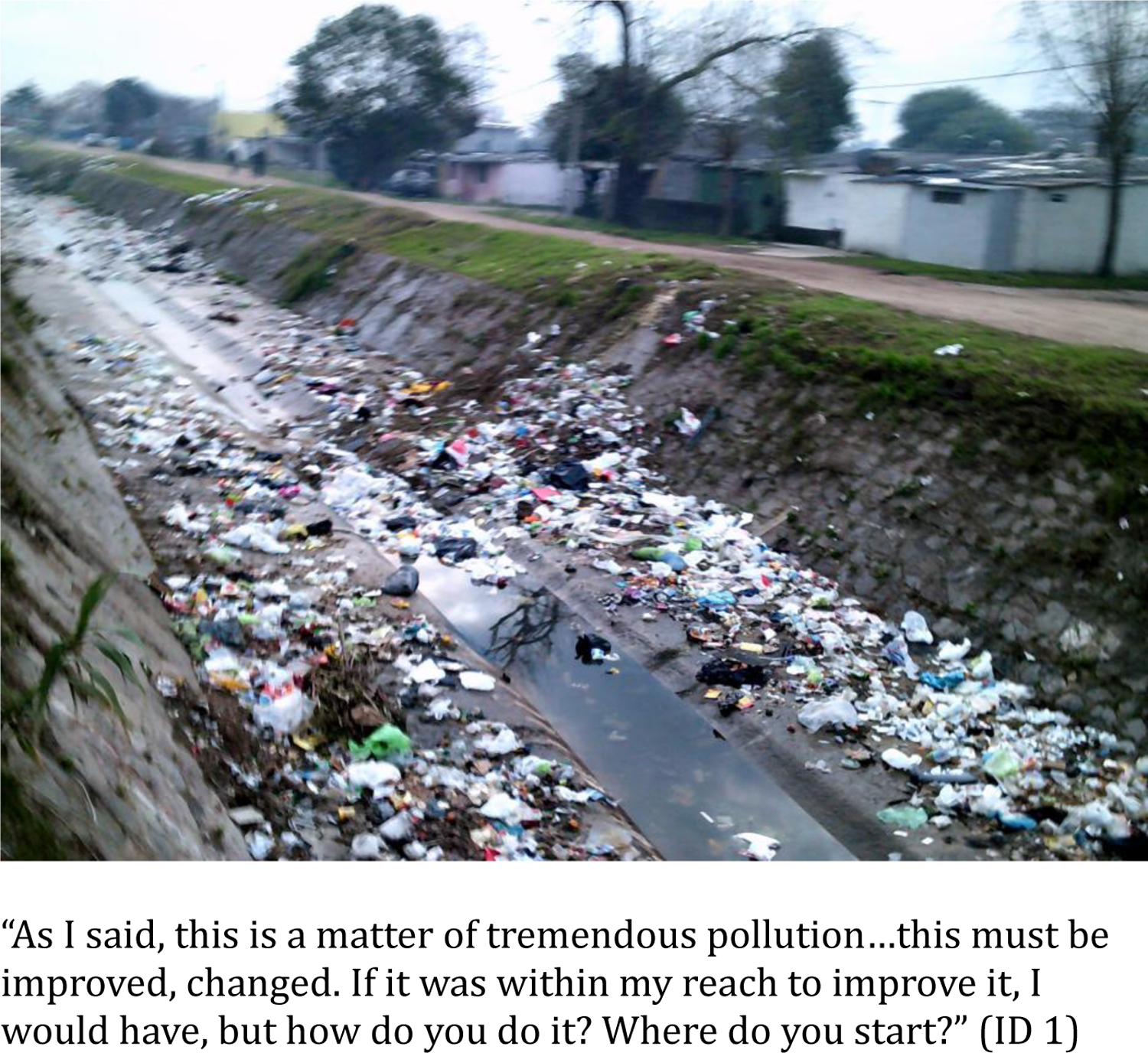
Photographs and Corresponding Quotes for Theme - ‘Physical Disorder’
Theme 2: Recreation
Many participants referenced parks as important places for play and relaxation. While most of the discussion around parks was positive, many caregivers wished for better playground equipment: “My son does not go because there aren’t swings anymore. People break things. They steal…before the grass was cut. Now it is neglected.” (ID 4), and “There is a swing set but no swings. There is a slide, but it is split in half so you cannot use it.” (ID 6). Another caregiver complained that there weren’t spaces for children to play: “There are also no places nearby, there are no places to play.” (ID 9). Recreation themed photographs are found in Figure 3.
Figure 3.
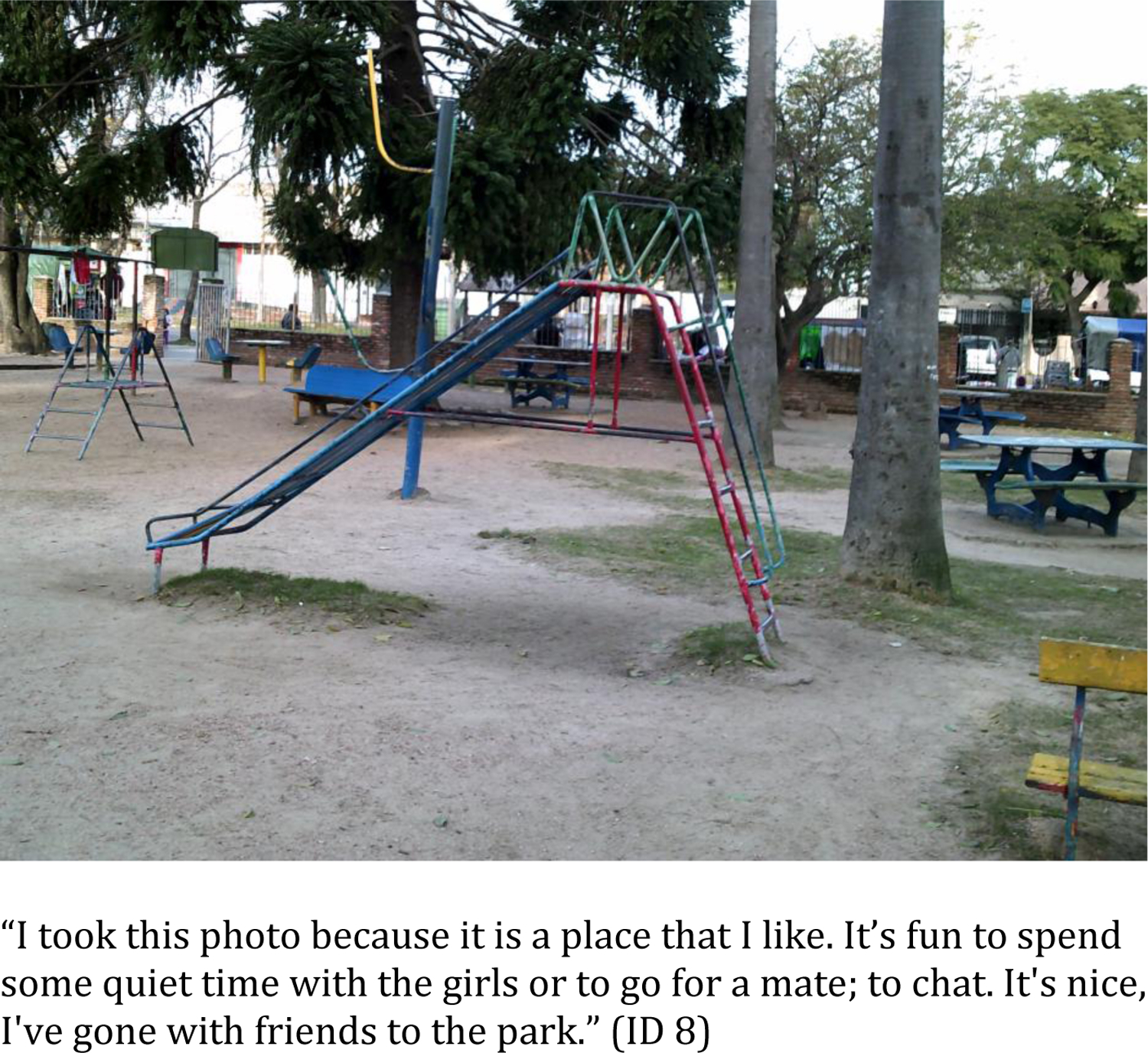
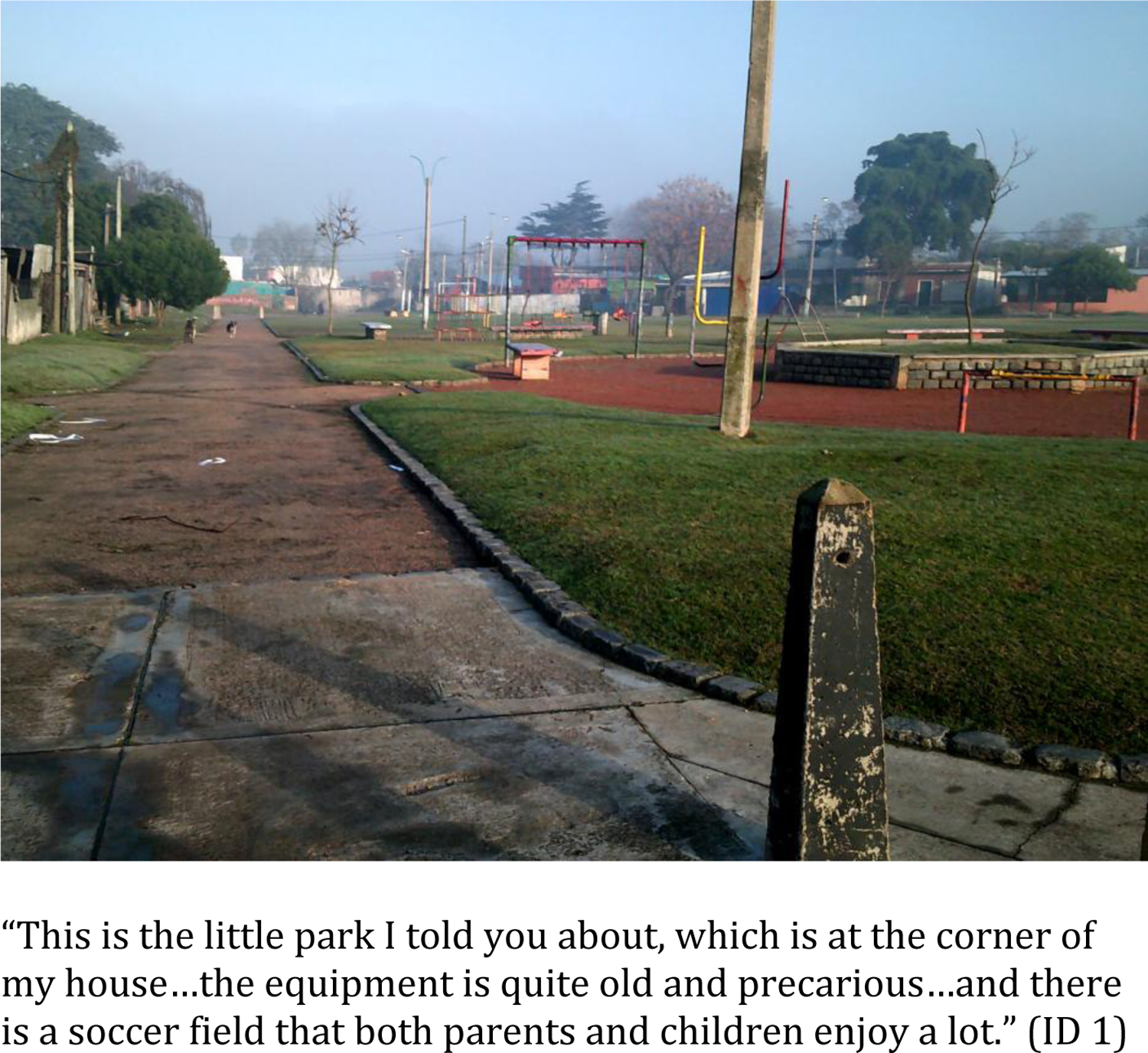
Photographs and Corresponding Quotes for Theme - ‘Recreation’
Theme 3: Safety and Crime
All participants referenced some aspect of safety and crime during the semi-structured interview. Interviewees mentioned robberies of health clinics and private houses. Specific areas were known to be unsafe including playgrounds and parks during certain times of day. Often motorcycles were used for robberies: “If you had a backpack they take it. If you had a wallet too. If you had a cell phone in your hand…They drive by on a motorcycle and steal it from you” (ID 2). Children were taught that motorcycles were a sign of danger: “[My daughter] knows that if she sees a motorcycle, she has to come and leave her bike lying down” (ID 5). Explaining violence in the community to children was a particularly difficult aspect of parenting: “These are very difficult things. How do you explain to a 7-year-old girl all these things?” (ID 5).
Gun violence was another important aspect of neighborhood safety to many (n=5) interviewees. In some neighborhoods, shootings happen regularly: “Where the health center is, there are shootings every night.” (ID 3). Participants expressed particular concern for neighborhood children, citing stories of gun violence: “My mother-in-law has a little store…they came in and pointed a gun at my 8-year-old niece’s head.” (ID 1), and “Very recently, a girl…was in bed, and was shot…a tiny baby girl of 7 years.” (ID 3). Shootings were perceived as a new development in Montevideo, necessitating greater surveillance of children while playing. A photo relevant to safety and crime is presented in Figure 4.
Figure 4.
Photograph and Corresponding Quote for Theme - ‘Safety and Crime’
Theme 4: Community Resources
Large variation existed in caregivers’ perceptions of access and availability of community resources. Some believed they did not lack anything: “I have everything at hand. I have the clinic where [the children] go…The only thing we don’t have is a pharmacy nearby, but there is a bakery, there is a supermarket” (ID 2). However, interviewees living in other neighborhoods mentioned: “You have to leave the neighborhood to go to a butcher shop, to go to a pharmacy, those things are not there” (ID 5). Another participant mentioned they were unsatisfied with the variety and quality of foods at her local store: “There is no variety…I go to [another neighborhood] to the supermarket because it is much cleaner than those of [my neighborhood]” (ID 10).
Transportation was another important concern. In some neighborhoods, public transportation was seen as adequate, while participants from other neighborhoods wished there were more bus lines: “Horrible. There is only one bus. If you do not get there on time you have to go to [another bus stop] … I have to walk 15 blocks or so” (ID 7). A few interviewees mentioned ‘red zones’, areas where transportation services, including ambulances, do not enter at night due to safety concerns. Only one participant mentioned improvements to infrastructure by photographing a newly paved street: “This is a street that they paved very recently. [This picture] represents progress. Progress not only for me, but also for my neighbors who are no longer going to lose anything because their house will no longer be flooded” (ID 3). Community resource photos are found in Figure 5.
Figure 5.

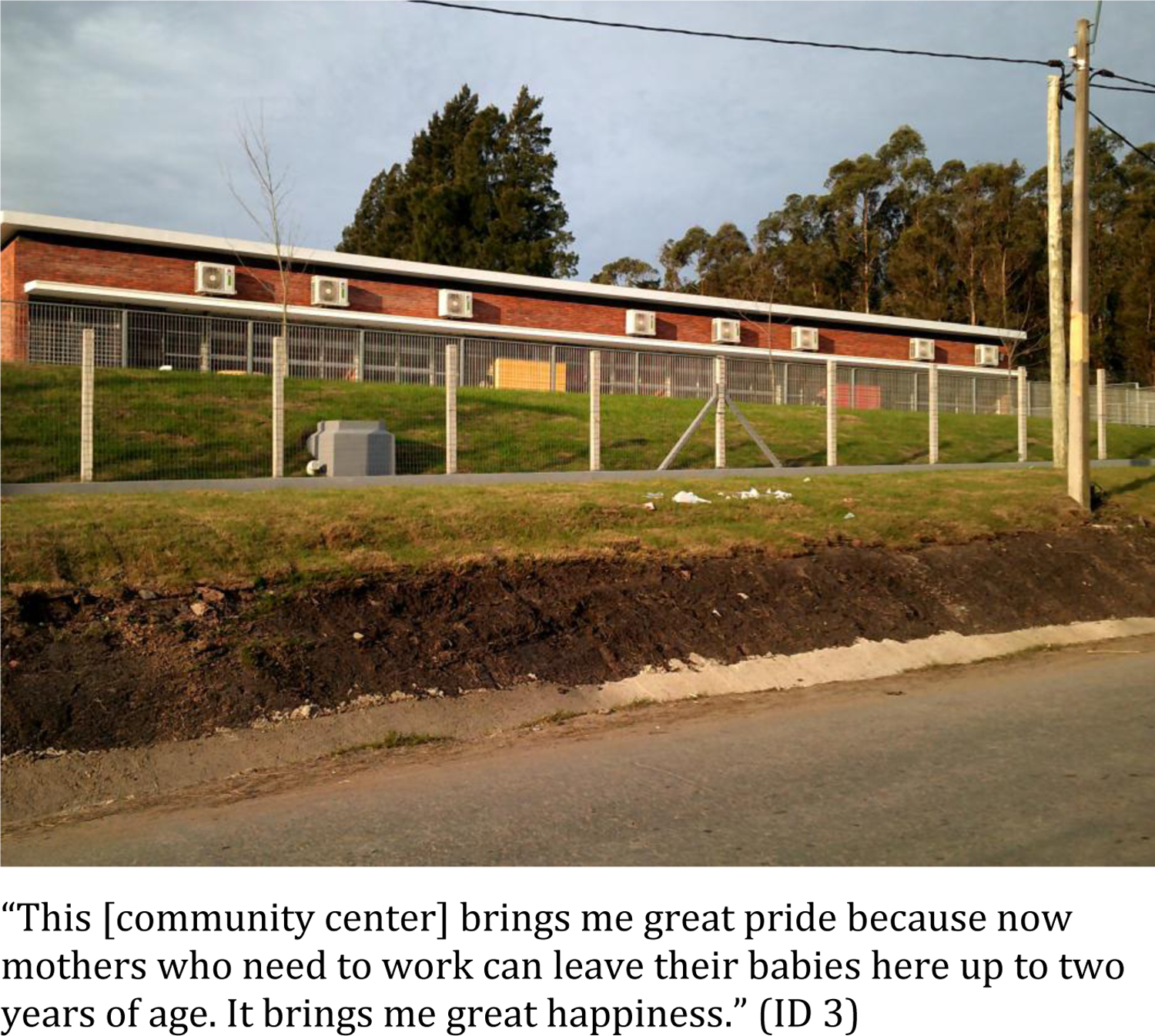
Photographs and Corresponding Quotes for Theme - ‘Community Resources’
Discussion and Conclusion
As CPBs are more common in poor, disadvantaged neighborhoods, studying ND in a variety of contexts and cultures, particularly in cities outside of North America and Europe, is important. In a mixed methods study of ND in Montevideo, Uruguay, we found that: 1) our ND factor was context specific, retaining moderate construct validity, 2) greater ND was associated with certain CBPs (conduct problems, shift and emotional control), and 3) themes generated from participant interviews included: physical disorder, recreation, safety and crime, and community resources.
Defining Neighborhood Disadvantage
The variables included in the ND factor were related to: education, employment, ethnic composition, housing quality and demographic characteristics (see Table 2). Certain variables related to racial composition of the neighborhood and home ownership were removed due to a lack of covariation with other neighborhood variables.
While Montevideo is home to populations of Asian and African descent, the population is mostly of European (Spanish and Italian) ancestry, possibly contributing to low covariation of some racial composition variables (ex., Asian descent) with other neighborhood indicators. Nevertheless, our ND factor included the proportion of individuals with African and indigenous ancestry. Between 1996 and 2006, the proportion of persons of African descent grew from 1.7% to 9.1% and indigenous descent from 0.8% to 3.8%. It has been suggested that this change in merely 10 years is not solely related to differences in minority population growth or immigration. Instead, these differences are related to changes in race-based questions used during census collections. Specifically, being allowed to choose more than one race category, the wording of ‘ancestry’ rather than ‘race’, and a renewal of identification with ethnic heritage among the Uruguayan population (69). Additionally, recent immigrants from Central America to Uruguay (70) are significantly more vulnerable to unemployment and underemployment (71). Thus, inclusion of racial and ethnic demographic information in our ND factor reflects current aspects of Uruguayan society.
While home ownership is often included as an important indicator of ND in US studies, home ownership variables were not associated with other neighborhood variables in Montevideo. Home ownership is similar across high and low socioeconomic neighborhoods (72). More important to ND is the percentage of houses with UBNs (unsatisfied basic needs). Lack of basic housing necessities including inadequate insulation, water supply, lighting, waste removal and overcrowding were a more important indicator of ND than home ownership. Future research should examine the mechanisms linking unsatisfied basic housing needs with CBPs.
When examining construct validity for ND, we found modest correlations with individual-level socioeconomic indicators. We did not see an association with ND and child BLLs, current parental smoking, variable income or occupational exposure to heavy metals. While lead exposure is often geographically stratified by neighborhood (73), we did not find an association between ND and child BLLs in our sample. While some sources of lead in Montevideo are place-specific (for example, battery and materials recycling), this is not a complete picture of childhood lead exposure. Other sources include leaded gasoline (phased out in 2004), proximity to industry, parents’ occupational exposure and dietary sources (59, 74, 75). Further research is needed to examine the extent to which specific neighborhood factors predict child BLLs in Montevideo. For smoking, a lack of correlation might be unsurprising, given the high prevalence of smoking in Uruguay. For example, one or both parents smoked in ~53% of SAM households (in 2009–13). Nationally, 20% of males and 16% of females smoke regularly; on average, males smoke 18 cigarettes/day and women 14 cigarettes/day (76), although prevalence has decreased in recent years (77).
Not many studies assess the validity of their ND construct by comparing it to individual measures of SES. In one study of Canadian youth gang affiliation, their ND factor correlated with individual and family level indicators of SES: family SES (−0.35), non-intact family status (0.17) and family residential instability (0.02) (78). Another study of ND and child behavior problems in the U.S. also found similar correlations between individual SES and ND: family SES (−0.30), family income/needs (−0.44) and maternal depression (0.24). Because the level of correlation between ND and individual level indicators in our study is similar to other studies, we conclude that our ND factor has construct validity. We urge future studies to report correlations with individual-level indicators of SES and other related, neighborhood-level variables to assess and compare construct validity.
Our qualitative findings suggest that ND may be related to other important neighborhood factors, not captured by the census statistics, such as physical disorder, crime, access to greenspace and playgrounds, grocers and other services.
Neighborhoods drawn by our respondents were relatively smaller (range: 100 – 3,500 m2) than the census segments (range: 14.5 – 18,822 m2). Perceived neighborhood boundaries in our sample were comparable to a study of U.S. adolescents’ perceptions of neighborhood size (79). These findings suggest that for whatever reason—culture, access to vehicles, geographically concentrated extended families or sample age—caregivers in Montevideo reported relatively small neighborhood areas.
Neighborhood disadvantage and child behavior problems
Controlling for a variety of individual-level socioeconomic predictors as well as biomarkers related to CBPs, we detected small, positive associations between ND and some CBPs. Higher ND factor was related to higher scores on conduct problem scales (aggressive and rule-breaking behavior), poor shift (inability to adapt to new situations or tasks) and emotional control (inappropriate responses to situations or an inability to control an emotional response). Given the relative size difference of census segments and neighborhood boundaries reported by caregivers in this study, it is remarkable that associations were observed. Resizing the area considered to constitute the child’s neighborhood may result in more precise estimates of the influence of ND on CBPs. Furthermore, it is important to understand which specific neighborhood factors play a role in conduct and behavioral regulation in children, and the extent to which these influences may persist into adolescence.
We found no association of ND with children’s ability to inhibit behaviors, hyperactive behaviors, ADHD index, or BRIEF sub-scales comprising the measure of metacognition. While some studies demonstrated associations between ND and child ADHD symptoms (80, 81), others reported null findings (82–84), suggesting more research is need on ND and ADHD. To our knowledge, we are the first study to examine the effect of ND on childhood metacognition, defined as the “monitoring and control of thought” (85); consisting of school-success related skills or abilities like working memory, planning and organizing, organization of materials, and self-monitoring. In past studies, greater metacognition was associated with high SES, more parent involvement in schoolwork, greater metacognitive language in the home and traumatic brain injury (86–89). While we did not find an association between ADHD, metacognition and ND, it would be important to examine different aspects of the neighborhood context, which were unmeasured in this study, but might influence the development of these behaviors in children.
Contribution of interview themes to understanding neighborhoods and their effects on child behavior problems
Reports concerning life in Montevideo neighborhoods can help generate theories to explain the relationship between ND and CBPs. First, caregivers mentioned physical disorder as a serious concern in their neighborhoods. Physical disorder is associated with CBPs. In a study of Canadian children 6–16 years of age, neighborhood disorder (measured through housing conditions, abandoned buildings, garbage and vandalism) was associated with children’s externalizing behaviors (90). The same study also found that physical disorder was related to externalizing behavior through a mediational pathway connecting parental psychological distress and poor parenting practices to behavior problems. Physical improvements to disadvantaged neighborhoods may help decrease disorder, leading to lower stress among parents and better behavior outcomes in children.
Second, caregivers reported recreation as important for childrearing. Socialization is linked to the development of self-regulation in children. A study of fourth-graders from the U.S., found that structured leisure activities were associated with psychosocial maturity and social competence (91). Playgrounds may facilitate socialization and interactions with peers. There is limited research on neighborhood access to playgrounds and behavior problems in children; some evidence suggests that access to greenspace is associated with lower CBPs. In a study of greenspace and neighborhood poverty, children between 3–5 years of age were most likely to have emotional problems when living in poor neighborhoods with low level of greenspace compared to children living in poor neighborhoods with high level of greenspace (92). Neighborhoods with access to playgrounds may mitigate the detrimental effects of ND on CBPs.
Third, caregivers were concerned about safety and violence in their neighborhood. Violent crimes have increased in Montevideo between 2006 and 2015 (93). Exposure to violence and crime affects CBPs through numerous pathways including: increased childhood stress (94), maternal distress (95), and changes in social norms (96). As crime increases in Montevideo, its connection to CBPs could be investigated in future studies.
Lastly, some caregivers mentioned limited community resources. There is some evidence that community services influence child behavior. In Chicago, the presence of youth-based community services was related to lower levels of aggression in children aged 9–15 years (97). Furthermore, if parental stress is related to CBPs, then efforts to reduce parental stress may mitigate CBPs. Neighborhood structural components related to adult stress include poor transportation, long commutes (98), food insecurity and hazardous waste sites (99). Important areas of research could address associations between household distance to community services (such as grocery stores, community centers and hospitals) and child behavior outcomes.
Study strengths and limitations
This is a cross-sectional study and therefore, causal relationships cannot be inferred. We are also unable to determine how ND may influence CBPs at different ages. For example, while metacognition was not associated with ND in our sample (7 years of age) it is possible that stronger effects could emerge at later ages. Future studies could include a wide range of ages or a longitudinal approach to address these questions. Second, our sampling scheme focused on recruiting children from areas where environmental exposure to toxic metals like lead was known or suspected. Additionally, children without data on CBPs that were excluded from analysis lived in less disadvantaged neighborhoods. These aspects of study design and analysis resulted in a sample characterized by lower socioeconomic status, which may have influenced the relationship between ND and CBPs. It is possible that excluding children from more advantaged neighborhoods might have actually attenuated the association between ND and CBPs. Fewer children from high socioeconomic status backgrounds may have reduced the difference in behavior scores between high and low ND, thus limiting our ability to detect the association of ND and CBPs scale scores. We also relied on teacher reports (CTRS-R:S and BRIEF) because they are valid measures of child cognitive and behavior problems (100, 101). We acknowledge, however, that having reports from multiple informants, including parents, would enrich our understanding of CBPs and the link between neighborhood factors and CBPs. Lastly, similarly to other census-based studies, we made the assumption that the 2011 census provides an accurate representation of neighborhoods for households enrolled in our study (from 2009–2013).
There are numerous strengths to our study. First, using a mixed methodology has allowed us to investigate the relationship between ND and CBPs and to place it within the daily life of families in Montevideo neighborhoods. We were also able to hypothesize explanatory pathways through which ND may impact CBPs in this setting. Second, we created a ND factor that relied on objectively collected data for the entire city of Montevideo, was data-driven, and specific to the context of this South American city. We utilized teacher reports of child behavior, finding relationships between ND and conduct problems and behavioral regulation scales. Third, our collection of child and family-related variables allowed us to estimate the associations between ND and CPBs above and beyond the influence individual SES, as well as child nutritional status or lead exposure. Fourth, our qualitative study utilized photovoice and semi-structured interviews to assess perceptions of neighborhood living and childrearing in disadvantaged Montevideo neighborhoods. This qualitative strategy allowed participants to actively engage with the research process and suggest changes in their neighborhood. Finally, our study makes a distinctive contribution to understanding of ND by focusing on a South American city.
In conclusion, we created a ND factor that was context-specific to Montevideo, Uruguay. This factor was positively associated with conduct, shifting and behavioral regulation problems in ~7-year-old children. Themes in our qualitative sample included: physical disorder, recreation, safety and crime and community resources. We combined our qualitative and quantitative findings to hypothesize potential pathways by which ND may influence CBPs. These pathways were specifically related to parental and child stress (e.g. crime, physical disorder, lack of resources) and child enrichment (e.g. access to greenspace). Creating neighborhood environments that reduce stress and increase child enrichment are important areas of future research into CBPs.
Supplementary Material
Highlights.
Created a neighborhood disadvantage (ND) factor in Montevideo, Uruguay.
Assessed construct validity and associations with child behavior problems.
Valid ND factor associated with conduct, shifting and emotional control problems.
Qualitative study addressed neighborhood characteristics, resources and problems.
Qualitative data led to hypotheses linking ND and child behavior in Montevideo.
Acknowledgements:
Dr. Craig Colder for his expertise in exploratory and confirmatory factor analysis.
This work was supported by the U.S. National Institute of Environmental Health Sciences (NIEHS) under grant R21ES019949, NIHES & Fogarty International (FI) Institute under grant R21ES16523, and by the Community of Excellence in Global Health Equity (CGHE) at the University at Buffalo –State University of New York.
Footnotes
No competing interests to declare.
References
- 1.Boucher O, Jacobson SW, Plusquellec P, Dewailly É, Ayotte P, Forget-Dubois N, et al. Prenatal methylmercury, postnatal lead exposure, and evidence of attention deficit/hyperactivity disorder among Inuit children in Arctic Quebec. Environmental health perspectives. 2012;120(10):1456–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kim S, Arora M, Fernandez C, Landero J, Caruso J, Chen A. Lead, mercury, and cadmium exposure and attention deficit hyperactivity disorder in children. Environmental research. 2013;126:105–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Reyes JW. Lead exposure and behavior: effects on antisocial and risky behavior among children and adolescents. Economic Inquiry. 2015;53(3):1580–605. [Google Scholar]
- 4.Butler AM, Kowalkowski M, Jones HA, Raphael JL. The relationship of reported neighborhood conditions with child mental health. Academic pediatrics. 2012;12(6):523–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Neece CL, Green SA, Baker BL. Parenting stress and child behavior problems: A transactional relationship across time. American Journal on Intellectual and Developmental Disabilities. 2012;117(1):48–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sektnan M, McClelland MM, Acock A, Morrison FJ. Relations between early family risk, children’s behavioral regulation, and academic achievement. Early Childhood Research Quarterly. 2010;25(4):464–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schofield H-LT, Bierman KL, Heinrichs B, Nix RL, Group CPPR. Predicting early sexual activity with behavior problems exhibited at school entry and in early adolescence. Journal of Abnormal Child Psychology. 2008;36(8):1175–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Colder CR, Shyhalla K, Frndak S, Read JP, Lengua LJ, Hawk LW Jr, et al. The prospective association between internalizing symptoms and adolescent alcohol involvement and the moderating role of age and externalizing symptoms. Alcoholism: Clinical and Experimental Research. 2017;41(12):2185–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Colder CR, Frndak S, Lengua LJ, Read JP, Hawk LW, Wieczorek WF. Internalizing and externalizing problem behavior: a test of a latent variable interaction predicting a two-part growth model of adolescent substance use. Journal of Abnormal Child Psychology. 2018;46(2):319–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ingoldsby EM, Shaw DS. Neighborhood contextual factors and early-starting antisocial pathways. Clinical Child and Family Psychology Review. 2002;5(1):21–55. [DOI] [PubMed] [Google Scholar]
- 11.Roosa MW, Deng S, Ryu E, Lockhart Burrell G, Tein JY, Jones S, et al. Family and child characteristics linking neighborhood context and child externalizing behavior. Journal of Marriage and Family. 2005;67(2):515–29. [Google Scholar]
- 12.Plybon LE, Kliewer W. Neighborhood types and externalizing behavior in urban school-age children: Tests of direct, mediated, and moderated effects. Journal of Child and Family Studies. 2001;10(4):419–37. [Google Scholar]
- 13.Winslow EB, Shaw DS. Impact of neighborhood disadvantage on overt behavior problems during early childhood. Aggressive Behavior: Official Journal of the International Society for Research on Aggression. 2007;33(3):207–19. [DOI] [PubMed] [Google Scholar]
- 14.Caughy MOB, Nettles SM, O’Campo PJ. The effect of residential neighborhood on child behavior problems in first grade. American Journal of Community Psychology. 2008;42(1–2):39. [DOI] [PubMed] [Google Scholar]
- 15.Kalff A, Kroes M, Vles J, Hendriksen J, Feron FJ, Steyaert J, et al. Neighbourhood level and individual level SES effects on child problem behaviour: a multilevel analysis. Journal of Epidemiology & Community Health. 2001;55(4):246–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fite PJ, Wynn P, Lochman JE, Wells KC. The effect of neighborhood disadvantage on proactive and reactive aggression. Journal of Community Psychology. 2009;37(4):542–6. [Google Scholar]
- 17.Jeon L, Buettner CK, Hur E. Family and neighborhood disadvantage, home environment, and children’s school readiness. Journal of Family Psychology. 2014;28(5):718. [DOI] [PubMed] [Google Scholar]
- 18.Zalot A, Jones DJ, Kincaid C, Smith T. Hyperactivity, Impulsivity, Inattention (HIA) and Conduct Problems among African American Youth: The Roles of Neighborhood and Gender. Journal of Abnormal Child Psychology. 2009;37(4):535–49. [DOI] [PubMed] [Google Scholar]
- 19.Boyle MH, Lipman EL. Do places matter? Socioeconomic disadvantage and behavioral problems of children in Canada. Journal of Consulting and Clinical Psychology. 2002;70(2):378–89. [DOI] [PubMed] [Google Scholar]
- 20.Roy AL, McCoy DC, Raver CC. Instability versus quality: Residential mobility, neighborhood poverty, and children’s self-regulation. Developmental Psychology. 2014;50(7):1891–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.McCoy DC, Peet ED, Ezzati M, Danaei G, Black MM, Sudfeld CR, et al. Early childhood developmental status in low-and middle-income countries: national, regional, and global prevalence estimates using predictive modeling. PLoS Medicine. 2016;13(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mitlin D, Satterthwaite D. Urban poverty in the global south: scale and nature: Routledge; 2013. [Google Scholar]
- 23.Ndezi T. The limit of community initiatives in addressing resettlement in Kurasini ward, Tanzania. Environment and Urbanization. 2009;21(1):77–88. [Google Scholar]
- 24.Bapat M. Poverty lines and lives of the poor: Underestimation of urban poverty-the case of India: IIED; 2009. [Google Scholar]
- 25.Sampson RJ, Sharkey P, Raudenbush SW. Durable effects of concentrated disadvantage on verbal ability among African-American children. Proceedings of the National Academy of Sciences. 2008;105(3):845–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science. 1997;277(5328):918–24. [DOI] [PubMed] [Google Scholar]
- 27.Knighton AJ, Savitz L, Belnap T, Stephenson B, VanDerslice J. Introduction of an area deprivation index measuring patient socioeconomic status in an integrated health system: implications for population health. eGEMs. 2016;4(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kind AJ, Jencks S, Brock J, Yu M, Bartels C, Ehlenbach W, et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Annals of Internal Medicine. 2014;161(11):765–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Roux AD, Kiefe CI, Jacobs DR Jr, Haan M, Jackson SA, Nieto FJ, et al. Area characteristics and individual-level socioeconomic position indicators in three population-based epidemiologic studies. Annals of Epidemiology. 2001;11(6):395–405. [DOI] [PubMed] [Google Scholar]
- 30.Villarreal A, Silva BF. Social cohesion, criminal victimization and perceived risk of crime in Brazilian neighborhoods. Social Forces. 2006;84(3):1725–53. [Google Scholar]
- 31.Antai D, Moradi T. Urban area disadvantage and under-5 mortality in Nigeria: the effect of rapid urbanization. Environmental Health Perspectives. 2010;118(6):877–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Brooks-Gunn J, Duncan GJ, Klebanov PK, Sealand N. Do neighborhoods influence child and adolescent development? American Journal of Sociology. 1993;99(2):353–95. [Google Scholar]
- 33.Turley RNL. When do neighborhoods matter? The role of race and neighborhood peers. Social Science Research. 2003;32(1):61–79. [Google Scholar]
- 34.Fagan AA, Wright EM, Pinchevsky GM. Racial/ethnic differences in the relationship between neighborhood disadvantage and adolescent substance use. Journal of Drug Issues. 2013;43(1):69–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Pong S-l, Hao L. Neighborhood and school factors in the school performance of immigrants’ children. International Migration Review. 2007;41(1):206–41. [Google Scholar]
- 36.Oberwittler D. The effects of neighbourhood poverty on adolescent problem behaviours: A multi-level analysis differentiated by gender and ethnicity. Housing Studies. 2007;22(5):781–803. [Google Scholar]
- 37.Barros J. Exploring urban dynamics in Latin American cities using an agent-based simulation approach. Agent-based models of geographical systems: Springer; 2012. p. 571–89. [Google Scholar]
- 38.Lawson V, Klak T. An argument for critical and comparative research on the urban economic geography of the Americas. Environment and Planning A. 1993;25(8):1071–84. [Google Scholar]
- 39.Duque JC, Lozano-Gracia N, Patino JE, Restrepo P, Velasquez WA. Spatiotemporal dynamics of urban growth in Latin American cities: An analysis using nighttime light imagery. Landscape and Urban Planning. 2019;191:103640. [Google Scholar]
- 40.Habitat U. State of Latin American and Caribbean cities: Towards a new urban transition. Nairobi: UN Habitat. 2012. [Google Scholar]
- 41.Bank TW. Urban population (% of total population) - Uruguay United Nations Population Division. World Urbanization Prospects: 2018 Revision. 2018. [Available from: https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS?locations=UY. [Google Scholar]
- 42.Barg G, Daleiro M, Queirolo EI, Ravenscroft J, Mañay N, Peregalli F, et al. Association of low lead levels with behavioral problems and executive function deficits in schoolers from Montevideo, Uruguay. International journal of environmental research and public health. 2018;15(12):2735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kordas K, Stoltzfus RJ, López P, Rico JA, Rosado JL. Iron and zinc supplementation does not improve parent or teacher ratings of behavior in first grade Mexican children exposed to lead. The Journal of pediatrics. 2005;147(5):632–9. [DOI] [PubMed] [Google Scholar]
- 44.Horton MK, Hsu L, Henn BC, Margolis A, Austin C, Svensson K, et al. Dentine biomarkers of prenatal and early childhood exposure to manganese, zinc and lead and childhood behavior. Environment international. 2018;121:148–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Winter AS, Sampson RJ. From Lead Exposure in Early Childhood to Adolescent Health: A Chicago Birth Cohort. American Journal of Public Health. 2017;107(9):1496–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Roy A, Queirolo E, Peregalli F, Mañay N, Martínez G, Kordas K. Association of blood lead levels with urinary F2–8α isoprostane and 8-hydroxy-2-deoxy-guanosine concentrations in first-grade Uruguayan children. Environmental Research. 2015;140:127–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Conners CK. Conners’ Teacher Rating Scale--Revised (L): Multi-Health Systems; North Tonawanda, NY; 1997. [Google Scholar]
- 48.Gurley JR. Conners’ Teacher Rating Scales: Revised. In: Goldstein S, Naglieri JA, editors. Encyclopedia of Child Behavior and Development. Boston, MA: Springer US; 2011. p. 405–6. [Google Scholar]
- 49.Gioia GA, Isquith PK. Behavior rating inventory for executive functions: Springer; 2011. [Google Scholar]
- 50.Conners CK, Sitarenios G, Parker JD, Epstein JN. Revision and restandardization of the Conners Teacher Rating Scale (CTRS-R): factor structure, reliability, and criterion validity. Journal of abnormal child psychology. 1998;26(4):279–91. [DOI] [PubMed] [Google Scholar]
- 51.Sullivan JR, Riccio CA. Diagnostic Group Differences in Parent and Teacher Ratings on the BRIEF and Conners’ Scales. Journal of Attention Disorders. 2007;11(3):398–406. [DOI] [PubMed] [Google Scholar]
- 52.Municipality of Montevideo Geographic Services. Sistema de Información Geográfica 2020. [Available from: http://sig.montevideo.gub.uy/.
- 53.Instituto National de Estadistica. Census 2011 2020. [Available from: http://www.ine.gub.uy/censos-2011.
- 54.Frndak S, Barg G, Canfield RL, Quierolo EI, Manay N, Kordas K. Latent subgroups of cognitive performance in lead- and manganese-exposed Uruguayan children: Examining behavioral signatures. Neurotoxicology. 2019;73:188–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Ravenscroft J, Roy A, Queirolo EI, Mañay N, Martínez G, Peregalli F, et al. Drinking water lead, iron and zinc concentrations as predictors of blood lead levels and urinary lead excretion in school children from Montevideo, Uruguay. Chemosphere. 2018;212:694–704. [DOI] [PubMed] [Google Scholar]
- 56.Woodcock RW. Woodcock-Muñoz Language Survey–Revised. Itasca, IL: Riverside Publishing. 2005. [Google Scholar]
- 57.Bradley RH, Caldwell BM, Corwyn RF. The Child Care HOME Inventories: Assessing the quality of family child care homes. Early Childhood Research Quarterly. 2003;18(3):294–309. [Google Scholar]
- 58.Desai G, Barg G, Queirolo EI, Vahter M, Peregalli F, Manay N, et al. A cross-sectional study of general cognitive abilities among Uruguayan school children with low-level arsenic exposure, potential effect modification by methylation capacity and dietary folate. Environmental Research. 2018;164:124–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kordas K, Burganowski R, Roy A, Peregalli F, Baccino V, Barcia E, et al. Nutritional status and diet as predictors of children’s lead concentrations in blood and urine. Environment International. 2018;111:43–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Prasetya A, Ridlo S, editors. Factor analysis for instruments of science learning motivation and its implementation for the chemistry and biology teacher candidates. Journal of Physics: Conference Series; 2018: IOP Publishing. [Google Scholar]
- 61.Howard MC. A review of exploratory factor analysis decisions and overview of current practices: What we are doing and how can we improve? International Journal of Human-Computer Interaction. 2016;32(1):51–62. [Google Scholar]
- 62.Tobias S, Carlson JE. Brief report: Bartlett’s test of sphericity and chance findings in factor analysis. Multivariate Behavioral Research. 1969;4(3):375–7. [DOI] [PubMed] [Google Scholar]
- 63.Horn JL. A rationale and test for the number of factors in factor analysis. Psychometrika. 1965;30(2):179–85. [DOI] [PubMed] [Google Scholar]
- 64.Lt Hu, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: a Multidisciplinary Journal. 1999;6(1):1–55. [Google Scholar]
- 65.Muthén L, Muthén B. Mplus. The comprehensive modelling program for applied researchers: user’s guide. 2018;5. [Google Scholar]
- 66.Braun V, Clarke V. Using thematic analysis in psychology. Qualitative research in psychology. 2006;3(2):77–101. [Google Scholar]
- 67.Huang FL. Multilevel modeling myths. School Psychology Quarterly. 2018;33(3):492. [DOI] [PubMed] [Google Scholar]
- 68.Clarke P. When can group level clustering be ignored? Multilevel models versus single-level models with sparse data. Journal of Epidemiology & Community Health. 2008;62(8):752–8. [DOI] [PubMed] [Google Scholar]
- 69.Cabella W, Porzecanski R. The growth of ethnic minorities in Uruguay: Ethnic Renewal or Measurement Problems? Social Statistics and Ethnic Diversity: Springer, Cham; 2015. p. 175–89. [Google Scholar]
- 70.Prieto Rosas V, Márquez Scotti C. Inclusión social de inmigrantes recientes que residen en viviendas particulares de Uruguay. Documento de Trabajo/FCS-PP; 04. 2019.
- 71.Prieto V, Robaina S, Koolhaas M. Acceso y calidad del empleo de la inmigración reciente en Uruguay. REMHU: Revista Interdisciplinar da Mobilidade Humana. 2016;24(48):121–44. [Google Scholar]
- 72.Ferre Z, Gandelman N, Piani G. Housing and neighborhood satisfaction in Montevideo, Uruguay. The quality of life in Latin American cities: Markets and perception. 2010:223–53. [Google Scholar]
- 73.Leech TG, Adams EA, Weathers TD, Staten LK, Filippelli GM. Inequitable chronic lead exposure. Family & community health. 2016;39(3):151–9. [DOI] [PubMed] [Google Scholar]
- 74.Queirolo EI, Ettinger AS, Stoltzfus RJ, Kordas K. Association of anemia, child and family characteristics with elevated blood lead concentrations in preschool children from Montevideo, Uruguay. Archives of environmental & occupational health. 2010;65(2):94–100. [DOI] [PubMed] [Google Scholar]
- 75.Cousillas A, Mañay N, Pereira L, Alvarez C, Coppes Z. Evaluation of lead exposure in Uruguayan children. Bulletin of environmental contamination and toxicology. 2005;75(4):629–36. [DOI] [PubMed] [Google Scholar]
- 76.Asma S, Mackay J, Song SY, Zhao L, Morton J, Palipudi KM, et al. The GATS Atlas. Atlanta, GA: CDC Foundation; 2015. [Google Scholar]
- 77.Ministerio de Salud Pública. Consumo de tabaco en Uruguay sigue tendencia a la baja y pasó de 21,6 % de prevalencia a 20,4 % el último año 2018. [Available from: https://www.gub.uy/ministerio-salud-publica/comunicacion/noticias/consumo-de-tabaco-en-uruguay-sigue-tendencia-la-baja-y-paso-de-216-de.
- 78.Dupéré V, Lacourse É, Willms JD, Vitaro F, Tremblay RE. Affiliation to Youth Gangs During Adolescence: The Interaction Between Childhood Psychopathic Tendencies and Neighborhood Disadvantage. Journal of Abnormal Child Psychology. 2007;35(6):1035–45. [DOI] [PubMed] [Google Scholar]
- 79.Basta LA, Richmond TS, Wiebe DJ. Neighborhoods, daily activities, and measuring health risks experienced in urban environments. Social science & medicine. 2010;71(11):1943–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Edwards B, Bromfield LM. Neighbourhood influences on young children’s emotional and behavioural problems. Family Matters. 2010(84):7. [Google Scholar]
- 81.Sharp W, Mangalmurti A, Hall C, Choudhury S, Shaw P. Associations between neighborhood, family factors and symptom change in childhood attention deficit hyperactivity disorder. Social Science & Medicine. 2019:112203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Nfonoyim B, Griffis H, Guevara J. Disparities in Childhood Attention Deficit Hyperactivity Disorder Symptom Severity by Neighborhood Poverty. Academic Pediatrics. 2020. [DOI] [PubMed] [Google Scholar]
- 83.Ford T, Goodman R, Meltzer H. The relative importance of child, family, school and neighbourhood correlates of childhood psychiatric disorder. Social psychiatry and psychiatric epidemiology. 2004;39(6):487–96. [DOI] [PubMed] [Google Scholar]
- 84.Razani N, Hilton JF, Halpern-Felsher BL, Okumura MJ, Morrell HE, Yen IH. Neighborhood characteristics and ADHD: results of a national study. Journal of attention disorders. 2015;19(9):731–40. [DOI] [PubMed] [Google Scholar]
- 85.Martinez ME. What is metacognition? Phi delta kappan. 2006;87(9):696–9. [Google Scholar]
- 86.Wang AY. Cultural-Familial Predictors of Children’s Metacognitive and Academic Performance. Journal of Research in Childhood Education. 1993;7(2):83–90. [Google Scholar]
- 87.Thompson RB, Williams D. Diversity Among Low SES Families: An Exploration of Predictive Variables for Mothers’ Metacognitive Questions to Their Children. Research in Human Development. 2006;3(4):191–209. [Google Scholar]
- 88.Pappas S, Ginsburg HP, Jiang M. SES differences in young children’s metacognition in the context of mathematical problem solving. Cognitive Development. 2003;18(3):431–50. [Google Scholar]
- 89.Hanten G, Bartha M, Levin HS. Metacognition following pediatric traumatic brain injury: A preliminary study. Developmental Neuropsychology. 2000;18(3):383–98. [DOI] [PubMed] [Google Scholar]
- 90.Jocson RM, McLoyd VC. Neighborhood and housing disorder, parenting, and youth adjustment in low-income urban families. American journal of community psychology. 2015;55(3–4):304–13. [DOI] [PubMed] [Google Scholar]
- 91.Fletcher AC, Nickerson P, Wright KL. Structured leisure activities in middle childhood: Links to well‐being. Journal of community psychology. 2003;31(6):641–59. [Google Scholar]
- 92.Flouri E, Midouhas E, Joshi H. The role of urban neighbourhood green space in children’s emotional and behavioural resilience. Journal of environmental psychology. 2014;40:179–86. [Google Scholar]
- 93.Ministry of the Interior. Statistics 2019. [Available from: https://www.minterior.gub.uy/observatorio/index.php/estadisticas.
- 94.Theall KP, Shirtcliff EA, Dismukes AR, Wallace M, Drury SS. Association between neighborhood violence and biological stress in children. JAMA pediatrics. 2017;171(1):53–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Linares LO, Heeren T, Bronfman E, Zuckerman B, Augustyn M, Tronick E. A mediational model for the impact of exposure to community violence on early child behavior problems. Child development. 2001;72(2):639–52. [DOI] [PubMed] [Google Scholar]
- 96.Stewart EA, Simons RL. Race, code of the street, and violent delinquency: A multilevel investigation of neighborhood street culture and individual norms of violence. Criminology. 2010;48(2):569–605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Molnar BE, Cerda M, Roberts AL, Buka SL. Effects of neighborhood resources on aggressive and delinquent behaviors among urban youths. American Journal of Public Health. 2008;98(6):1086–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Wener RE, Evans GW, Phillips D, Nadler N. Running for the 7: 45: The effects of public transit improvements on commuter stress. Transportation. 2003;30(2):203–20. [Google Scholar]
- 99.Yang T-C, Matthews SA. The role of social and built environments in predicting self-rated stress: A multilevel analysis in Philadelphia. Health & place. 2010;16(5):803–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Luk S, Leungt P. Conners’ teacher’s rating scale—a validity study in Hong Kong. Journal of Child Psychology and Psychiatry. 1989;30(5):785–93. [DOI] [PubMed] [Google Scholar]
- 101.McCandless S, O’Laughlin L. The clinical utility of the Behavior Rating Inventory of Executive Function (BRIEF) in the diagnosis of ADHD. Journal of attention disorders. 2007;10(4):381–9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.