

Abstract
Objective: This study aimed to analyze the efficacy of acupuncture alone or combined with physical therapy compared to other treatment interventions for relieving pain and improving function in rotator cuff diseases. Methods: Our study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. After PROSPERO (CRD42023396740) registration, all randomized controlled trials (RCTs) published from the inception of the databases to October 10, 2023, evaluating the efficacy of acupuncture either alone or in combination with physical therapy for treating rotator cuff diseases, were extracted from seven databases, including PubMed, Embase, the Web of Science, the Cochrane Library, the China National Knowledge Infrastructure (CNKI), the VIP Database for Chinese Technical Periodicals (VIP), and the Wanfang Date. Two independent researchers assessed the quality of the included studies and extracted relevant data. Furthermore, a meta-analysis was conducted using Stata 14 software. Results: We included 13 RCTs - 12 published in English and 1 in Chinese - that enrolled 1,371 patients. The meta-analysis results demonstrated that acupuncture alone or in combination with physical therapy was superior to other interventions for short-term shoulder joint function improvement (standardized mean difference [SMD] = -0.82, 95% confidence interval [95% CI]: -1.28 to -0.35, P = 0.001), medium-term shoulder joint function improvement (SMD = -1.00, 95% CI: -1.62 to -0.38, P = 0.002), short-term pain relief (weighted mean difference [WMD] = -1.37, 95% CI: -2.39 to -0.38, P = 0.006), medium-term pain relief (WMD = -1.66, 95% CI: -2.70 to -0.63, P = 0.002), and post-treatment shoulder joint abduction improvements (SMD = 0.68, 95% CI: 0.20 to 1.16, P = 0.005), external rotation (SMD = 0.62, 95% CI: 0.13 to 1.11, P = 0.012), and forward flexion (SMD = 0.71, 95% CI: 0.44 to 0.97, P < 0.001), with significant differences (P < 0.05). Conclusion: Based on the current clinical data, meta-analysis showed that acupuncture alone or combined with physical therapy is efficacious for short- and medium-term (< 3 months) pain relief and functional improvements. However, compared to other interventions, the efficacy of the long-term (3 to 12 months) period did not significantly differ. After treatment, these modalities displayed advantages such as improved shoulder joint abduction, external rotation, and forward flexion movements. However, no significant difference was noted in internal rotation movement. Thus, future studies might further investigate whether different acupuncture methods affect the efficacy of treating rotator cuff diseases and improving long-term outcome.
Keywords: Acupuncture, meta-analysis, physical therapy, rotator cuff diseases, rotator cuff injury, subacromial pain syndrome
Introduction
Rotator cuff diseases, accounting for approximately 70% of shoulder joint pain cases [1], primarily include rotator cuff tendinitis, subacromial impingement syndromes, and others. However, rotator cuff injuries are more common than other conditions. It has been reported that more than 4.5 million people worldwide seek treatment for rotator cuff injuries annually [2]. The prevalence of rotator cuff injuries was 20% and 25% in individuals aged ≥ 20 years and ≥ 50 years, respectively [3]. Most patients complain of shoulder pain at night and reduced range of motion, significantly impacting their work and daily lives [4].
Although the exact causes of rotator cuff diseases are unclear, potential associations have been observed with rotator cuff muscle dysfunction [5], alterations in shoulder joint kinematics and joint capsule constriction [6], and scapular motion disorders [7]. Myofascial trigger points (MTrPs) are sensitive nodules in skeletal muscles that are tender to palpation, thereby causing referred pain [8]. Several studies have also corroborated the association between MTrPs and shoulder pain [9-12]. MTrP-associated pain and mobility restrictions can alter scapular movement rhythm and lead to subacromial pain syndrome [13]. While the trigger point theory is still under discussion, a few studies have suggested various factors, such as higher concentrations of inflammatory mediators in the subacromial bursa and rotator cuff tendons [14,15] as well as increased acetylcholine receptor activity [16], as reasons for sustained pain and contraction.
Modalities such as anti-inflammatory drugs, exercise rehabilitation, and physical therapy are widely used as primary intervention for rotator cuff diseases [17,18]. When the primary therapeutic effects are unsatisfactory, corticosteroid (CS) injections or platelet-rich plasma (PRP) injections into the subacromial space are commonly employed to improve symptoms [19,20]. For patients with rotator cuff diseases who have not responded to conservative treatment for 4-6 months, arthroscopic surgery, subacromial decompression, and acromioplasty are classical surgical treatment options [21]. Extracorporeal shock wave therapy is a widely used physical therapy for these conditions; however, research by Surace et al. [22] suggests that its advantages over other non-surgical treatments are not clear, and its safety is uncertain. Despite the frequent use of subacromial CS injections in the treatment of rotator cuff diseases, there is limited repeatable evidence demonstrating the ability of these injections to improve long-term outcomes independently [23,24]. Recent studies indicate that subacromial CS injections are effective only within 3-8 weeks and may have adverse effects, including humeral head cartilage degeneration, supraspinatus tendon degeneration, tears, or even spontaneous rupture, leading to increased risks of subsequent surgical complications [25-27]. A meta-analysis by Peng et al. [28] suggested no significant difference in mid-term efficacy between subacromial injections of PRP and CS. The long-term outcomes of surgical treatment for rotator cuff diseases are mixed [29]; a meta-analysis by Ryosa et al. [30] indicated that surgical intervention is not more effective than conservative treatment alone. Therefore, conservative treatment is still advocated as the initial approach for rotator cuff diseases.
Currently, invasive therapies, such as acupuncture alone or in combination with physical therapy, are a growing trend for managing rotator cuff diseases. Acupuncture and physical therapy are given together as vital components of conservative interventions. Acupuncture is often administered for musculoskeletal disorders and has been recommended as an effective non-surgical intervention for treating shoulder pain and mobility restrictions [31]. Current research suggests that the efficacy of acupuncture primarily stems from its ability to (1) modulate peripheral and central nervous systems related to pain [32-34], alter biochemical [35,36] and neuroinflammatory [37] mediators, and induce connective tissue mechanical disruption to improve microcirculation, thereby reducing peripheral nerve sensitivity [38,39]; (2) reduce neuromuscular endplate activity, activate central pathways for pain relief [40,41], improve sympathetic nerve activity, and reduce local as well as distal mechanical sensitivity [42]; and (3) acupuncture for tendons, which leads to vasodilation, accelerated collagen proliferation, and enhanced blood flow [43].
Navarro-Santana et al. [11] reported the efficacy of acupuncture in alleviating nonspecific shoulder pain in MTrPs. A meta-analysis conducted by Sanchez-Infante et al. [44] demonstrated that acupuncture relieves pain in patients with various musculoskeletal disorders, including nonspecific shoulder pain. A systemic review by Blanco-Diaz et al. [45] assessed the effectiveness of acupuncture in combination with physical therapy for the treatment of subacromial pain syndrome patients but did not perform a quantitative analysis. The clinical significance of this study lies in the quantitative evaluation of the efficacy of acupuncture in treating conditions such as subacromial pain syndrome and rotator cuff injuries. Using a meta-analysis approach, this study aimed to provide evidence-based medicine to assess the differences in the efficacy of acupuncture alone or combined with physical therapy and other intervention measures for treating rotator cuff diseases.
Materials and methods
Study design
We followed the PRISMA statement and Cochrane Collaboration’s Handbook for Systematic Reviews of Interventions guidelines [46]. The study was registered in PROSPERO with registration number CRD42023396740.
Inclusion and exclusion criteria
The inclusion criteria for patients were as follows: (1) aged ≥ 18 years with untreated rotator cuff diseases; (2) diagnosed with rotator cuff impingement syndrome, subacromial impingement syndrome, subacromial bursitis, rotator cuff injuries, or rotator cuff tendonitis; (3) received acupuncture or acupuncture combined with physical therapy; (4) the control group were collected; (5) had primary outcome measures related to pain or mobility restrictions; and (6) were RCTs.
The exclusion criteria were as follows: (1) patients with incomplete information or data extraction; (2) had RCTs published as conference abstracts; (3) applied acupuncture interventions simultaneously in two groups; and (4) failed to measure shoulder pain or mobility restrictions.
Data search
After the PROSPERO registration, seven databases were searched electronically (PubMed, Embase, Web of Science, Cochrane Library, CNKI, VIP, and Wanfang Date). We included articles published from database inception until October 10, 2023. Our search strategy used Medical Subject Heading (MeSH) and free terms for both English- and Chinese-language RCTs on acupuncture and rotator cuff diseases. Our search terms used were “Rotator cuff injuries”, “Rotator cuff tears”, “Shoulder impingement syndromes”, “Acupuncture”, and “Acupuncture Therapy”. As an example of the English search terms, the PubMed search strategy was as follows: #1 Rotator Cuff Injuries [Mesh Terms] OR Rotator Cuff Injury [Title/Abstract] OR Rotator Cuff Tears [Title/Abstract] OR Rotator Cuff Tendinosis [Title/Abstract] OR Glenoid Labral Tears [Title/Abstract] OR Shoulder Impingement Syndromes [Title/Abstract] OR Rotator Cuff Impingement [Title/Abstract] OR Subacromial Impingement Syndrome [Title/Abstract]; #2 Acupuncture [Mesh Terms] OR Acupuncture Therapy [Title/Abstract] OR Auricular points [Title/Abstract] OR needling [Title/Abstract] OR needle [Title/Abstract] OR Acupuncture Points [Title/Abstract] OR Moxibustion [Title/Abstract] OR Acupoint catgut embedding [Title/Abstract]; #3 randomized controlled trial [Mesh Terms]; #4 #1 AND #2 AND #3.
Literature screening and data extraction
After removing duplicates, two researchers (Hai-Ning Zhang and Jian-Ge Chen) independently screened the literature. After excluding unsuitable articles based on title and abstract, the researchers examined the full text of those studies that could be included. Strict screening was conducted as per the inclusion and exclusion criteria. Disagreements about the inclusion of a particular study were resolved through discussion with a third researcher (Hua-Nan Li).
The data extracted from the included studies included various features, such as the first author’s name, publication year, country where the study was conducted, sample size, age and sex of the subjects, type of rotator cuff disease, treatment interventions, control measures for each group, follow-up time, and outcome measures. Two researchers (Shun Fan and An Bao) independently extracted the data, which were cross-checked and adjudicated by a third researcher (Jin-Gui Wang) in case of any discrepancy.
Risk of bias (RoB) and methodological quality assessment
The risk of bias in the included studies was assessed using the Cochrane Handbook for Systematic Reviews of Interventions [46]. Moreover, the following RoB domains were evaluated: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Subsequently, each domain was rated as “low risk of bias”, “unclear risk of bias”, or “high risk of bias”.
The studies’ methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale [47]. This scale included several items: random allocation, allocation concealment, baseline similarity between groups, blinding of subjects, therapists, and assessors, follow-up, intention-to-treat analysis, intragroup statistical comparisons, point measures, and variability measures. A PEDro score of ≥ 5 points was considered high-quality research.
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to evaluate the quality of evidence for acupuncture therapy, and the results were rated as high, moderate, low, or very low quality [48]. The assessment criteria included several parameters, such as RoB, the indirectness of evidence, inconsistency of results or unexplained heterogeneity, imprecision in results, and a high probability of publication bias. High-quality evidence comprises all negative criteria. A sample was downgraded to moderate quality if one criterion indicated a serious risk. However, when two criteria indicate a serious risk or one criterion indicates an extremely serious risk, the evidence is considered low quality. If ≥ 3 criteria indicate a serious risk or ≥ 2 criteria indicate a very serious risk, the evidence is deemed very low quality [49].
Although two researchers (Jian-Ge Chen and Xiao-Yu Wang) conducted these assessments independently, a third researcher (Jin-Gui Wang) was consulted if any discrepancies existed.
Statistical analysis
Stata 14 (StataCorp, College Station, TX, USA) software was used for the data analysis. Binary and continuous outcome variables are expressed as risk ratios and standardized mean differences or weighted mean differences. With 95% confidence intervals, the analysis used a significance level of α = 0.05.
The chi-square test and I2 statistic assessed qualitative (significance level: α = 0.1) and quantitative heterogeneities, respectively. When the included studies were homogeneous (P ≥ 0.1, I2 ≤ 50%), a fixed-effects model was used for analysis. If the test results indicated heterogeneity (P < 0.1, I2 > 50%), a random effects model was used after excluding the source of heterogeneity. Moreover, sensitivity analyses were performed for heterogeneous results (P < 0.1, I2 > 50%), switching between the fixed-effect and random-effect models.
Publication bias was analyzed using Stata 14 software, and it was assessed qualitatively by funnel plots and quantitatively by Egger’s test.
Results
Literature search and selection
Two researchers conducted electronic searches of seven databases, PubMed, Embase, the Cochrane Library, Web of Science, CNKI, Wanfang Date, and VIP, and obtained 382 articles. After removing 56 duplicates, we excluded the remaining 272 articles based on title and abstract reviews. Two researchers read the full texts of the remaining 54 articles and eliminated 41 based on the exclusion criteria. Finally, we included 13 RCT articles involving a total of 1,371 patients. Detailed information on the literature search and screening process is presented in Figure 1. Table 1 provides the detailed characteristics of all the included studies.
Figure 1.
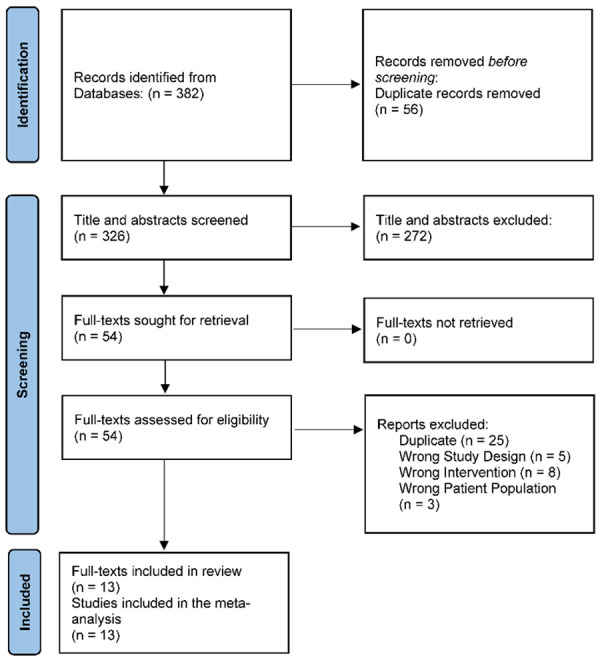
Literature search and screening process.
Table 1.
Basic characteristics of the included studies
| Author | Year | Country | Intervention | Control | Sample Size, n | Age, Mean SD, yr | Sex: M/F, n | Symptom Duration, Mean SD, m | Follow-up, w/m | Diagnosis | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||||||||
| Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | |||||||
| Arias-Buria et al. [50] | 2017 | Spain | DN+PT | PT | 25 | 25 | 49±5 | 48±6 | 18/7 | 19/6 | NA | NA | 4 w, 3 m, 6 m, 12 m | SPS |
| Imani et al. [51] | 2020 | Iran | DN | PT | 22 | 22 | 43.45±10.08 | 41.91±10.11 | 8/14 | 9/13 | NA | NA | 1 m | SAIS |
| Jalilipanah et al. [13] | 2021 | Iran | DN | PT | 13 | 13 | 35.62±8.72 | 36.62±7.92 | 3/10 | 6/7 | NA | NA | 1 w | SIS |
| Johansson et al. [52] | 2011 | Sweden | Acupuncture | Corticosteroid | 42 | 49 | 51±9 | 50±9 | 16/26 | 22/27 | NA | NA | 6 w, 3 m, 6 m, 12 m | SIS |
| Johansson et al. [53] | 2005 | Sweden | Acupuncture | Ultrasound | 44 | 41 | 49±7 | 49±8 | 12/32 | 14/27 | NA | NA | 4 w, 3 m, 6 m, 12 m | SIS |
| Kibar et al. [54] | 2017 | Turkey | Acupuncture | SA | 30 | 32 | 64.5±11.0 | 63.0±9.5 | 9/21 | 10/22 | NA | NA | 4 w | SAIS |
| Kleinhenz et al. [55] | 1999 | Germany | Acupuncture | SA | 25 | 27 | 32.72±7.91 | 37.37±10.08 | 13/12 | 18/9 | 29.04±34.86 | 26.52±35.13 | 4 w | RCT |
| Rha et al. [56] | 2013 | Korea | DN | PRP | 19 | 20 | 53.9±11.6 | 52.2±9.5 | 8/11 | 9/11 | 9.2±3.2 | 9.6±3.6 | 2 w, 4 w, 6 w, 3 m, 6 m | RCD |
| Rueda et al. [57] | 2016 | Spain | Acupuncture | SA | 35 | 33 | 36.86±13.94 | 29.73±9.76 | 20/15 | 18/5 | NA | NA | 4 w, 3 m | SIS |
| Song et al. [58] | 2021 | China | Acupuncture+PT | PT | 30 | 30 | 49.77±10.96 | 53.33±12.98 | 12/18 | 16/14 | NA | NA | 3 w | RCI |
| Vas et al. [59] | 2008 | Spain | Acupuncture | SA | 205 | 220 | 54.9±10.8 | 56.4±11.8 | 53/152 | 65/155 | 8.5±4.7 | 8.4±4.4 | 1 m, 3 m, 6 m, 12 m | RCD |
| Wang et al. [60] | 2018 | China | Acupuncture+PT | PT | 40 | 40 | 56±5 | 53±4 | 20/20 | 22/18 | 10±2 | 9±2 | 6 w | RCI |
| Molsberger et al. [61] | 2010 | Germany | Acupuncture | SA | 154 | 135 | 50.3±9.6 | 51.3±9.4 | 66/88 | 45/89 | 10.7±9.7 | 11.6±11.4 | 6 w, 3 m | RCD |
PRP: Platelet-rich plasma; PT: Physiotherapy; RCD: Rotator cuff disease; RCI: Rotator cuff injury; RCT: Rotator cuff tendinitis; SA: Sham acupuncture; SAIS: Subacromial impingement syndrome; SIS: Shoulder impingement syndrome; SPS: Subacromial pain syndrome.
Risk assessment and methodological quality evaluation
Two researchers independently assessed the risk of bias and methodological quality of all included articles. Among the 13 included articles, eight described their randomization methods and were assessed as having a low risk of bias. However, the remaining five studies described incomplete randomization methods, thus resulting in an unclear risk of bias. Seven articles mentioned allocation concealment, indicating a low risk of bias, while the remaining six did not mention allocation concealment, leading to an unclear risk of bias grading. Although seven articles implemented participant blinding, none of the 13 articles managed to blind the researchers due to the nature of the interventions, resulting in a high risk of bias. The risk assessment details for the included articles can be found in Figures 2 and 3. Moreover, the methodological quality scores ranged from 6 to 8 (out of a maximum of 10), with an average of 7.3 (standard deviation [SD] = 0.74). All the articles were rated as having high methodological quality (≥ 5 points). Table 2 provides detailed information on the PEDro scale for all the studies.
Figure 2.
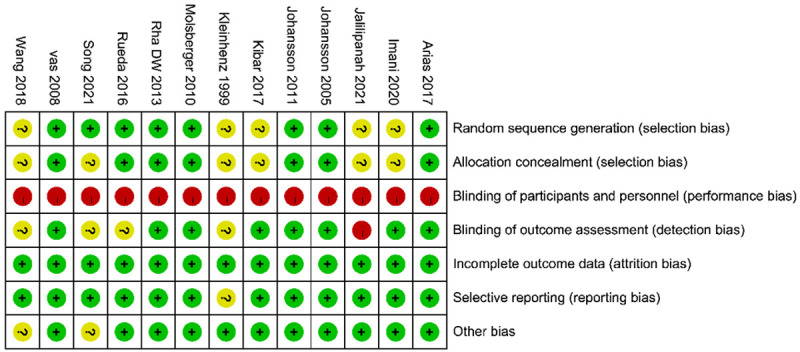
Summary of bias risk assessment: a review of the judgment for each bias risk in all included studies. Red (-): high risk of bias, Yellow (?): Bias risk unclear, Green (+): Low bias risk.
Figure 3.

Bias risk chart: a retrospective review of the judgment for each bias risk in all included studies, represented as percentages.
Table 2.
Scores of RCTs evaluated using the PEDro scale
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arias-Buria et al. 2017 [50] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Imani et al. 2020 [51] | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 |
| Jalilipanah et al. 2021 [13] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Johansson et al. 2011 [52] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Johansson et al. 2005 [53] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Kibar et al. 2017 [54] | Y | N | Y | Y | N | Y | Y | Y | Y | Y | 8 |
| Kleinhenz et al. 1999 [55] | Y | N | Y | Y | N | N | Y | Y | Y | Y | 7 |
| Rha et al. 2013 [56] | Y | Y | Y | Y | N | Y | Y | N | Y | Y | 8 |
| Rueda et al. 2016 [57] | Y | Y | Y | Y | N | N | Y | N | Y | Y | 7 |
| Song et al. 2021 [58] | Y | N | Y | Y | N | N | Y | Y | Y | Y | 7 |
| Vas et al. 2008 [59] | Y | Y | Y | Y | N | Y | Y | N | Y | Y | 8 |
| Wang et al. 2018 [60] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Molsberger et al. 2010 [61] | Y | Y | Y | Y | N | Y | Y | N | Y | Y | 8 |
Y: Yes; N: No.
Results of functional score changes after acupuncture or combined physical therapy
Among the 13 included articles, ten [50-59] provided complete functional score data before and after treatment. The primary scoring methods included the Constant-Murley Shoulder Assessment (CM), the Shoulder Pain and Disability Index (SPADI), and the University of California at Los Angeles End-Result Score (UCLA). Due to differences in the scoring criteria, all outcomes were represented using standardized mean differences, as detailed in Supplementary Tables 1, 2, 3. Ten of those articles [50-59] reported short-term (0 to 1 month) functional score changes, with high heterogeneity (P < 0.001, I2 = 89.8%); eight [50-53,56,57,59,60] reported medium-term (1 to 3 months) enhanced heterogeneous functional score changes (P < 0.001, I2 = 93.0%); and four [50,52,53,56] reported long-term (P < 0.001, I2 = 89.2%) functional score changes. Therefore, random effects models were used for data synthesis. Our results showed that the acupuncture group had significantly greater functional score changes than the control group in terms of short-term scores (SMD = -0.82, 95% CI (-1.28, -0.35), P = 0.001), while the acupuncture group had significantly greater medium-term functional score changes than did the control group (SMD = -1.00, 95% CI (-1.62, -0.38), P = 0.002). Nonetheless, no significant difference was observed in long-term functional score changes between the acupuncture and control groups (SMD = -0.48, 95% CI (-1.30, 0.34), P = 0.251). The forest plot is shown in Figure 4.
Figure 4.

Forest plot for observing the improvement in functional score associated with acupuncture, exercise rehabilitation, or their combination compared to other interventions for treating rotator cuff diseases in the short, medium, and long-term periods.
Results of pain changes after acupuncture or combined with physical therapy
Among the 13 articles, nine [13,50,51,54,57-61] provided complete pain score data before and after treatment. The two scoring methods used were the visual analogue scale (VAS) or numerical rating scale (NRS), internationally recognized single-dimensional pain intensity assessment methods; the outcomes were represented using weighted mean differences. Of these, eight articles [13,50,51,54,57-59,61] reported short-term (0 to 1 month) pain score changes, with high heterogeneity (P < 0.001, I2 = 91.2%); six [50,51,57,59-61] reported medium-term (> 1 to 3 months) pain score changes, with high heterogeneity (P < 0.001, I2 = 94.7%); and two articles [50,59] reported long-term (> 3 to 12 months) pain score changes, with enhanced heterogeneity (P < 0.001, I2 = 94.4%). Therefore, random effects models were used. We found that the acupuncture group displayed significantly greater pain score changes than the control group (WMD = -1.37, 95% CI (-2.36, -0.38) in the short-term period, P = 0.006), while the acupuncture group reported significantly greater pain score changes than did the control group in terms of medium-term scores (WMD = -1.66, 95% CI (-2.70, -0.63), P = 0.002). Moreover, during the long-term period, there was no significant difference in pain score changes between the acupuncture and control groups (WMD = -1.78, 95% CI (-3.83, 0.28), P = 0.09). The forest plot is shown in Figure 5.
Figure 5.

Forest plot for pain reduction in the short-, medium-, and long-term periods with acupuncture, exercise rehabilitation, or their combination when compared to other interventions for rotator cuff diseases.
Results of shoulder joint range of motion improvement after acupuncture or combined with physical therapy
Among the 13 included articles, six [13,54,56,58,60,61] provided shoulder joint range of motion data before and after treatment. However, most of these articles reported only immediate or short-term improvement in shoulder joint range of motion post-treatment; therefore, we could analyze these data only. Five articles [54,56,58,60,61] reported shoulder joint abduction improvements before and after the intervention, with high heterogeneity (P < 0.001, I2 = 82.3%); five articles [13,54,56,58,60] reported shoulder joint external rotation improvements before and after treatment, with enhanced heterogeneous results (P = 0.006, I2 = 72.4%). After using random effects models for data synthesis, our results showed that the acupuncture group displayed significantly better shoulder joint abduction improvements after treatment than did the control group (SMD = 0.68, 95% CI (0.20, 1.16), P = 0.005). In contrast, the acupuncture group reported significantly better improvement in shoulder joint external rotation post-treatment than did the control group (SMD = 0.62, 95% CI (0.13, 1.11), P = 0.012). Four articles [54,56,58,60] reported shoulder joint flexion improvement before and after the intervention, with low heterogeneity (P = 0.414, I2 = 0%), whereas three [13,56,58] of them reported shoulder joint internal rotation improvement before and after treatment, with low heterogeneity (P = 0.189, I2 = 40.0%). After utilizing fixed effects models for data synthesis, we reported that the acupuncture group showed significantly better improvement in shoulder joint flexion post-treatment than did the control group (SMD = 0.71, 95% CI (0.44, 0.97), P < 0.001). However, no significant difference was observed in shoulder joint internal rotation improvements after treatment between the acupuncture and control groups (SMD = 0, 95% CI (-0.35, 0.35), P = 0.998). As shown in Figures 6, 7, 8 and 9.
Figure 6.
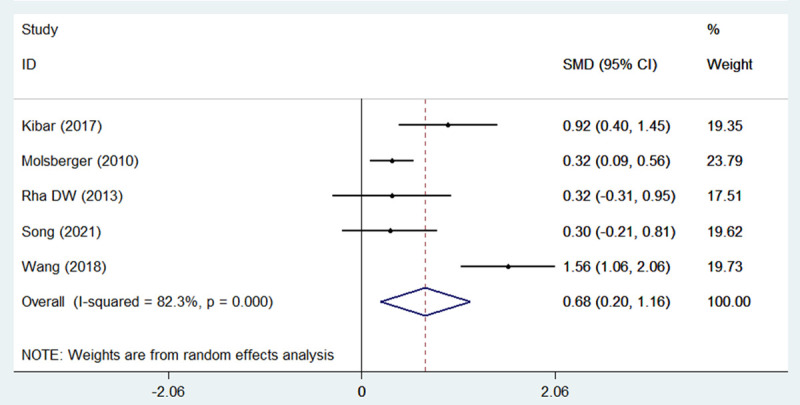
Forest plot for shoulder joint abduction improvement after treatment with acupuncture, exercise rehabilitation, or their combination when compared to other interventions for managing rotator cuff diseases.
Figure 7.
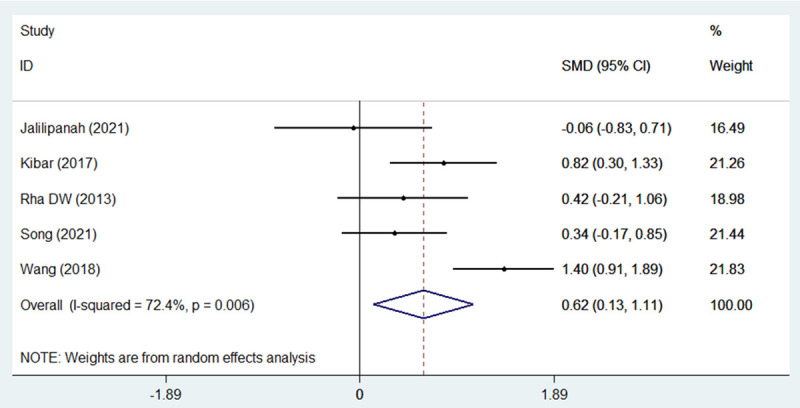
Forest plot for shoulder joint external rotation improvement after treatment with acupuncture, exercise rehabilitation, or their combination in comparison to other interventions for managing rotator cuff diseases.
Figure 8.
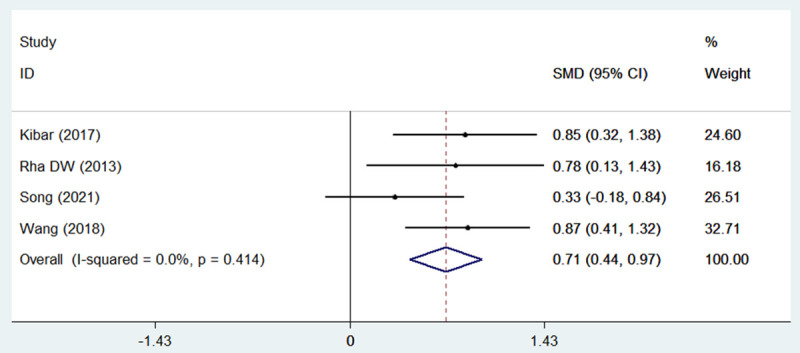
Forest plot for shoulder joint flexion improvement after treatment with acupuncture, exercise rehabilitation, or their combination compared to other interventions for rotator cuff diseases.
Figure 9.
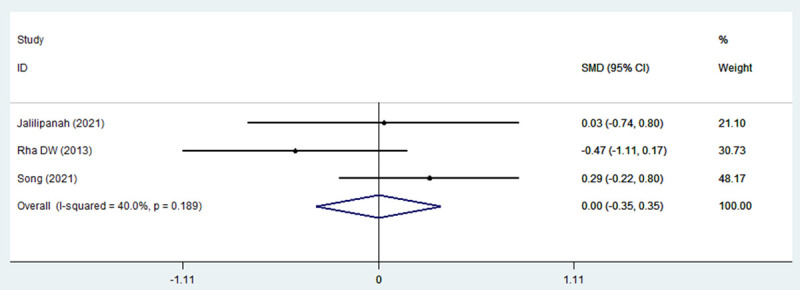
Forest plot for shoulder joint internal rotation improvement after treatment with acupuncture, exercise rehabilitation, or their combination when compared to other interventions for treating rotator cuff diseases.
Sensitivity analysis and publication bias
For significant heterogeneous outcomes (short-, medium-, and long-term pain reduction; short-, medium-, and long-term functional improvement; shoulder joint abduction; and external rotation improvement), as indicated by I2 > 50% and P < 0.10 in the heterogeneity test, sensitivity analysis was conducted by switching between fixed-effect and random-effect models. Our results showed that, except for long-term pain reduction and functional improvement, the other outcome results were consistent between the fixed effects and random effects models (Table 3).
Table 3.
Sensitivity analysis results
| Outcome Measure | I2 (%) | Random Effects Model WMD or SMD (95% CI) | P | Fixed Effects Model WMD or SMD (95% CI) | P |
|---|---|---|---|---|---|
| Short-term Function Improvement | 89.8 | -0.816 (-1.283, -0.348) | 0.001 | -0.549 (-0.681, -0.416) | < 0.001 |
| Medium-term Function Improvement | 93.0 | -1.000 (-1.624, -0.376) | 0.002 | -0.781 (-0.924, -0.638) | < 0.001 |
| Long-term Function Improvement | 89.2 | -0.482 (-1.304, 0.340) | 0.251 | -0.441 (-0.703, -0.179) | 0.001 |
| Short-term Pain Reduction | 91.2 | -1.373 (-2.362, -0.385) | 0.006 | -1.692 (-1.964, -1.421) | < 0.001 |
| Medium-term Pain Reduction | 94.7 | -1.663 (-2.699, -0.627) | 0.002 | -2.636 (-2.816, -2.456) | < 0.001 |
| Long-term Pain Reduction | 94.4 | -1.551 (-2.171, -0.930) | 0.090 | -2.228 (-2.664, -1.793) | < 0.001 |
| Shoulder Joint Abduction Improvement | 82.3 | 0.679 (0.200, 1.158) | 0.005 | 0.540 (0.364, 0.715) | < 0.001 |
| Shoulder Joint External Rotation Improvement | 72.4 | 0.622 (0.135, 1.108) | 0.012 | 0.689 (0.447, 0.949) | < 0.001 |
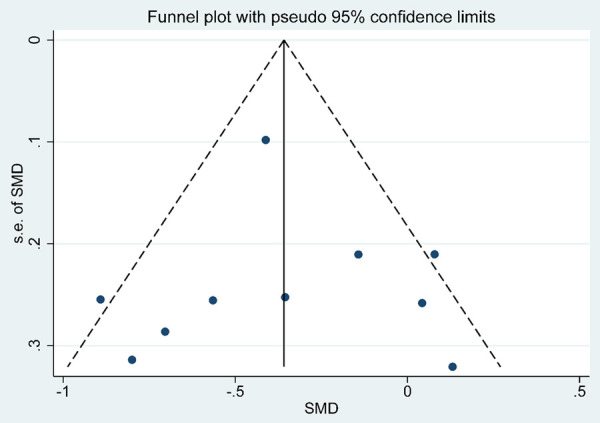
The Egger’s test results for short- and medium-term pain reduction; short-, medium-, and long-term functional improvement; shoulder joint abduction, external rotation, flexion, and internal rotation improvement were p values > 0.05, with 95% CI containing 0, as shown in Table 4. We plotted funnel plots for pain reduction and function improvement, and its distribution was symmetric as shown in Figures 10, 11. Both qualitative and quantitative analyses showed that there was no significant publication bias in the included original studies.
Table 4.
Publication bias of the included studies
| Outcome Measure | Parameter or Group (No. of Studies) | SE | t | P > |t| | 95% CI |
|---|---|---|---|---|---|
| Function Improvement | Short-term subgroup (10) | 2.09 | -1.45 | 0.19 | -7.83, 1.79 |
| Medium-term subgroup (8) | 3.00 | -0.7 | 0.51 | -9.42, 5.24 | |
| Long-term subgroup (4) | 9.74 | -0.26 | 0.82 | -44.45, 39.39 | |
| Pain Reduction | Short-term subgroup (8) | 2.69 | -0.46 | 0.66 | -7.45, 4.95 |
| Medium-term subgroup (6) | 3.53 | -1.37 | 0.24 | -14.62, 4.96 | |
| Shoulder Joint Range of Motion Improvement | Abduction (5) | 2.76 | 0.97 | 0.40 | -6.11, 11.47 |
| External Rotation (5) | 4.52 | -1.66 | 0.20 | -21.89, 6.91 | |
| Flexion (4) | 4.89 | -0.03 | 0.98 | -21.20, 20.91 | |
| Internal Rotation (3) | 5.45 | -0.58 | 0.66 | -72.43, 66.07 |
Figure 10.

Funnel plot of publication bias for pain reduction.
Figure 11.
Funnel plot of publication bias for function improvement.
Quality of evidence
Due to the highly heterogeneous results, the quality of evidence for functional score and pain reduction improvement following acupuncture or combined physical therapy was rated low. The detailed GRADE assessment information is displayed in Table 5.
Table 5.
Summary of GRADE evidence for functional score improvement and pain reduction improvement associated with acupuncture alone or in combination with physical therapy
| Outcome Measure | Parameter or Group (No. of Studies) | Risk of Bias | Inconsistencya | Indirectness of Evidence | Imprecision | Publication Bias | Quality of Evidence |
|---|---|---|---|---|---|---|---|
| Function Improvement | Overall effect (10) | NO | Very serious (I2 = 90.6%) | NO | NO | NO | Low |
| Short-term subgroup (10) | NO | Very serious (I2 = 89.8%) | NO | NO | NO | Low | |
| Medium-term subgroup (8) | NO | Very serious (I2 = 93.0%) | NO | NO | NO | Low | |
| Long-term subgroup (4) | NO | Very serious (I2 = 89.2%) | NO | Seriousb | NO | Low | |
| Pain Reduction | Overall effect (9) | NO | Very serious (I2 = 93.3%) | NO | NO | NO | Low |
| Short-term subgroup (8) | NO | Very serious (I2 = 91.2%) | NO | NO | NO | Low | |
| Medium-term subgroup (6) | NO | Very serious (I2 = 94.7%) | NO | NO | NO | Low | |
| Long-term subgroup (2) | NO | Very serious (I2 = 94.4%) | NO | NO | NO | Low |
Serious: I2 = 40%-80%, very serious: I2 > 80.
Patients, n < 250.
Discussion
We aimed to analyze the impact of acupuncture alone or in combination with physical rehabilitation therapy on pain and functional impairment in patients with rotator cuff disease. Based on the results of this meta-analysis, we suggest that acupuncture alone or in combination with physical rehabilitation therapy is more beneficial for pain relief and functional improvement than other forms of treatment, such as CS injections, PRP injections, exercise therapy, or sham acupuncture, in short- and medium-term periods. However, no significant advantage of acupuncture alone or in combination with physical therapy was observed in terms of long-term pain or functional scores. In terms of shoulder joint range of motion before and after treatment, acupuncture alone or combined with physical therapy significantly improved abduction, flexion, and external rotation, but not internal rotation.
Currently, invasive treatments such as CS injections, PRP injections, and acupuncture are widely used for rotator cuff diseases. The American Academy of Orthopedic Surgeons’ 2020 guidelines [62] stated that a single CS injection under local anesthesia can provide short-term pain relief and improved function, but multiple CS injections might harm the rotator cuff structure. Several studies have suggested that PRP injections have slower but more stable effects than CS injections [63]. In another study, meta-analyses have shown that PRP injections are similar to CS injections in terms of pain relief and functional recovery at any time during follow-up [64]. PRP injections reduce the subsequent surgery rate and provide better pain and functional improvements in the medium- to long-term, suggesting that they are a potential alternative to CS injections. However, these guidelines do not support the routine use of PRP for partial rotator cuff injuries due to insufficient high-quality RCT evidence.
While some meta-analyses have reported the advantages of acupuncture for treating rotator cuff diseases, these guidelines do not mention the application of acupuncture for this condition. A meta-analysis by Griswold et al. [65] suggested that dry needling might reduce pain and functional impairment in rotator cuff disease patients more effectively than other conservative treatments. However, additional high-quality RCTs are needed to validate these findings. Another meta-analysis by Para-Garcia et al. [31] revealed that dry needling, alone or when combined with exercise therapy, might slightly alleviate pain in the short- and medium-term. However, the evidence regarding functional improvement during these durations is inconclusive. Navarro-Santana et al. [11] reported moderate to low-quality evidence indicating a short-term positive impact of dry needling on non-traumatic shoulder pain and functional impairment; however, the identification of long-term effects still requires long-term clinical trial follow-up.
The main difference in our results compared to those of other meta-analyses is that the durations of short- and medium-term (< 3 months) pain reduction and functional improvement after acupuncture intervention were greater than those after other treatments. The analysis of shoulder joint range of motion improvement after acupuncture showed better results in abduction, external rotation, and flexion movements than in the other treatments, but no significant difference was noted in internal rotation. This might be due to the inclusion of various acupuncture methods for treating rotator cuff diseases in the original literature, not just dry needling. Under the guidance of traditional Chinese medicine theory, several acupuncture methods are available, and different choices of acupuncture points and needling techniques can affect individual efficacy. Currently, several scholars believe that the mechanism through which acupuncture relieves pain involves the stimulation of endogenous opioid peptides through needle insertion, which leads to analgesic effects and improved pain tolerance [66]. Many scholars have proposed that acupuncture improves the local total blood volume and oxygen saturation in patients with tendon diseases. Kubo et al. [67] reported a significant increase in local total blood volume and blood oxygen saturation in the midportion of the Achilles tendon after acupuncture compared to baseline. Sandberg et al., studying acupuncture in the tibialis anterior muscle, discovered that needle stimulation releases calcitonin gene-related peptide (CGRP), causing vasodilation, which may be responsible for the accelerated local blood flow, and that this effect remains constant within the first 60 minutes after treatment [68,69]. However, these proposed mechanisms cannot fully explain the differences in treatment outcome following acupuncture intervention. This discrepancy is mainly attributed to variations in acupuncture technique. There is a lack of high-quality RCTs comparing different acupuncture methods for rotator cuff diseases.
The safety of acupuncture should be evaluated. Apart from 25% of patients experiencing post-needling pain [11], most studies did not report any adverse events. Moreover, post-needling pain is primarily caused by the stimulation of soft tissues during needle insertion and manipulation, which subsides without any treatment within 48-72 h. A few mild adverse events, including subcutaneous bleeding and bruising, have been reported in those studies that reported acupuncture-related adverse events. However, several rare serious adverse events, such as pneumothorax, have also been noted, with a rate of < 0.1% [70]. Therefore, acupuncture is a safe intervention when used correctly, but therapists should be aware of its risks in certain areas.
Some of the original articles included in this study combined acupuncture with other treatment interventions, including general exercise therapy, physical therapy, and local massage. A recent meta-analysis on conservative treatments for subacromial pain syndrome suggested that exercise therapy is one of the best interventions for treating subacromial pain syndrome [71]. The 2020 American Academy of Orthopedic Surgeons’ guidelines for rotator cuff disease recommend the application of physical therapy for full-thickness rotator cuff tears [62]. While most of the studies in our research focused on acupuncture, the lack of data on the frequency, intensity, timing, and type (FITT) of other interventions when combined with acupuncture (following the FITT principle) limits our understanding of the treatment effects of acupuncture alone. Due to the nature of acupuncture interventions, it is challenging to blind participants adequately, and at least half of the studies were assessed as having a high risk of bias in blinding. However, blinding is crucial in clinical studies using self-reported outcome measures such as pain and functional scores, as it helps prevent overestimation of the intervention’s effect. Otherwise, pain and functional scores might be overestimated by up to 25% [72]. A study by Braithwaite et al. [73] emphasized the impact of blinding on acupuncture results in comparison to sham acupuncture. In the case of insufficient blinding, the results favored acupuncture, whereas when the participants were adequately blinded, no significant difference was observed between the two groups. Although acupuncture may have advantages in short- and medium-term durations in terms of pain relief and functional scores, these results should be cautiously interpreted, as the true effects may vary significantly from the reported effects [74].
In summary, we confirmed the efficacy of acupuncture alone or in combination with conservative interventions in terms of pain relief and functional improvement within three months. However, during the long term (3-12 months), no significant difference in efficacy was noted compared to that of other interventions, such as CS and PRP injections. Additionally, acupuncture has shown an advantage in improving shoulder joint range of motion in abduction, external rotation, and flexion, but not in internal rotation.
Strengths and limitations
This is the first meta-analysis that included several acupuncture methods, including traditional Chinese medicine-based acupuncture and western medicine-based dry needling. The meta-analysis also included non-English literature, which made the sources of the original studies more extensive; all included studies were rated as high quality. These were our strengths. This study has several limitations. Our results were heterogeneous, and the evidence level according to the GRADE system was low. This may be due to the inclusion of various acupuncture techniques and the findings of some studies that combined other interventions, thus hampering our understanding of the effects of acupuncture alone. Due to the specificity of the acupuncture interventions, the participants were not sufficiently blinded, and at least half of the studies were assessed as having a high risk of bias in blinding. This was a crucial component for highly subjective outcome measures such as pain and functional scores and a source of heterogeneity. Although there was heterogeneity in the results of some studies and we rigorously downgraded the level of evidence, it can be still affirmed that this meta-analysis will be valuable as all of the original articles were high quality studies. Due to limitations in the available original data, our analysis considered only shoulder joint range of motion improvements after treatment. We did not analyze shoulder joint motion during follow-up, which reduced the completeness of our findings.
Conclusion
Based on the results of this meta-analysis, we suggest that acupuncture alone or combined with other conservative interventions is efficacious at reducing pain and improving function within 3 months, with statistically significant results. However, no significant difference was observed in long-term (3-12 months) efficacy compared to that of other modalities, such as CS or PRP injections. Although this therapy was more effective at improving shoulder joint abduction, flexion, and external rotation movements after treatment, no significant difference was observed in internal rotation movement compared to other interventions. Thus, future research could investigate whether different acupuncture techniques might have varying efficacy in treating rotator cuff diseases and improving long-term outcome.
Acknowledgements
This study was supported by the Second Batch of High-Level Talent Selection and Training Engineering Project in the Health and Health Industry of Tianjin (TJSQNYXXZ-D2-002); and the National Key Discipline Construction Project in Traditional Chinese Medicine for 2023 - Massage (2023ZDXK002).
Disclosure of conflict of interest
None.
Supporting Information
References
- 1.Greenberg DL. Evaluation and treatment of shoulder pain. Med Clin North Am. 2014;98:487–504. doi: 10.1016/j.mcna.2014.01.016. [DOI] [PubMed] [Google Scholar]
- 2.Kesikburun S, Tan AK, Yilmaz B, Yasar E, Yazicioglu K. Platelet-rich plasma injections in the treatment of chronic rotator cuff tendinopathy: a randomized controlled trial with 1-year follow-up. Am J Sports Med. 2013;41:2609–2616. doi: 10.1177/0363546513496542. [DOI] [PubMed] [Google Scholar]
- 3.Nourissat G, Ornetti P, Berenbaum F, Sellam J, Richette P, Chevalier X. Does platelet-rich plasma deserve a role in the treatment of tendinopathy? Joint Bone Spine. 2015;82:230–234. doi: 10.1016/j.jbspin.2015.02.004. [DOI] [PubMed] [Google Scholar]
- 4.Jo CH, Shin WH, Park JW, Shin JS, Kim JE. Degree of tendon degeneration and stage of rotator cuff disease. Knee Surg Sports Traumatol Arthrosc. 2017;25:2100–2108. doi: 10.1007/s00167-016-4376-7. [DOI] [PubMed] [Google Scholar]
- 5.Escamilla RF, Hooks TR, Wilk KE. Optimal management of shoulder impingement syndrome. Open Access J Sports Med. 2014;5:13–24. doi: 10.2147/OAJSM.S36646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tyler TF, Nicholas SJ, Roy T, Gleim GW. Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med. 2000;28:668–673. doi: 10.1177/03635465000280050801. [DOI] [PubMed] [Google Scholar]
- 7.Cools AM, Witvrouw EE, Mahieu NN, Danneels LA. Isokinetic scapular muscle performance in overhead athletes with and without impingement symptoms. J Athl Train. 2005;40:104–110. [PMC free article] [PubMed] [Google Scholar]
- 8.Alvarez DJ, Rockwell PG. Trigger points: diagnosis and management. Am Fam Physician. 2002;65:653–660. [PubMed] [Google Scholar]
- 9.Sergienko S, Kalichman L. Myofascial origin of shoulder pain: a literature review. J Bodyw Mov Ther. 2015;19:91–101. doi: 10.1016/j.jbmt.2014.05.004. [DOI] [PubMed] [Google Scholar]
- 10.Ribeiro DC, Belgrave A, Naden A, Fang H, Matthews P, Parshottam S. The prevalence of myofascial trigger points in neck and shoulder-related disorders: a systematic review of the literature. BMC Musculoskelet Disord. 2018;19:252. doi: 10.1186/s12891-018-2157-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Navarro-Santana MJ, Gomez-Chiguano GF, Cleland JA, Arias-Buria JL, Fernandez-de-Las-Penas C, Plaza-Manzano G. Effects of trigger point dry needling for nontraumatic shoulder pain of musculoskeletal origin: a systematic review and meta-analysis. Phys Ther. 2021;101:pzaa216. doi: 10.1093/ptj/pzaa216. [DOI] [PubMed] [Google Scholar]
- 12.Liu L, Huang QM, Liu QG, Ye G, Bo CZ, Chen MJ, Li P. Effectiveness of dry needling for myofascial trigger points associated with neck and shoulder pain: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2015;96:944–955. doi: 10.1016/j.apmr.2014.12.015. [DOI] [PubMed] [Google Scholar]
- 13.Jalilipanah P, Okhovatian F, Serri RA, Bagban AA, Zamani S. The effect of dry needling & muscle energy technique separately and in combination in patients suffering shoulder impingement syndrome and active trigger points of infraspinatus. J Bodyw Mov Ther. 2021;26:94–100. doi: 10.1016/j.jbmt.2020.12.030. [DOI] [PubMed] [Google Scholar]
- 14.Farfaras S, Roshani L, Mulder J, Mitsios N, Hallstrom EK, Kartus JT. Increased levels of inflammatory markers in the subscapularis tendon and joint capsule in patients with subacromial impingement. Knee Surg Sports Traumatol Arthrosc. 2021;29:2228–2236. doi: 10.1007/s00167-020-05992-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shah JP, Danoff JV, Desai MJ, Parikh S, Nakamura LY, Phillips TM, Gerber LH. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89:16–23. doi: 10.1016/j.apmr.2007.10.018. [DOI] [PubMed] [Google Scholar]
- 16.Gerwin RD, Dommerholt J, Shah JP. An expansion of Simons’ integrated hypothesis of trigger point formation. Curr Pain Headache Rep. 2004;8:468–475. doi: 10.1007/s11916-004-0069-x. [DOI] [PubMed] [Google Scholar]
- 17.Ramme AJ, Robbins CB, Patel KA, Carpenter JE, Bedi A, Gagnier JJ, Miller BS. Surgical versus nonsurgical management of rotator cuff tears: a matched-pair analysis. J Bone Joint Surg Am. 2019;101:1775–1782. doi: 10.2106/JBJS.18.01473. [DOI] [PubMed] [Google Scholar]
- 18.Dickinson RN, Ayers GD, Archer KR, Fan R, Page C, Higgins LD, Kuhn JE, Baumgarten KM, Matzkin E, Jain NB. Physical therapy versus natural history in outcomes of rotator cuff tears: the Rotator Cuff Outcomes Workgroup (ROW) cohort study. J Shoulder Elbow Surg. 2019;28:833–838. doi: 10.1016/j.jse.2018.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Doiron-Cadrin P, Lafrance S, Saulnier M, Cournoyer E, Roy JS, Dyer JO, Fremont P, Dionne C, MacDermid JC, Tousignant M, Rochette A, Lowry V, Bureau NJ, Lamontagne M, Coutu MF, Lavigne P, Desmeules F. Shoulder rotator cuff disorders: a systematic review of clinical practice guidelines and semantic analyses of recommendations. Arch Phys Med Rehabil. 2020;101:1233–1242. doi: 10.1016/j.apmr.2019.12.017. [DOI] [PubMed] [Google Scholar]
- 20.Neal BS, Longbottom J. Is there a role for acupuncture in the treatment of tendinopathy? Acupunct Med. 2012;30:346–349. doi: 10.1136/acupmed-2012-010208. [DOI] [PubMed] [Google Scholar]
- 21.Jaeger M, Berndt T, Ruhmann O, Lerch S. Patients with impingement syndrome with and without rotator cuff tears do well 20 years after arthroscopic subacromial decompression. Arthroscopy. 2016;32:409–415. doi: 10.1016/j.arthro.2015.08.026. [DOI] [PubMed] [Google Scholar]
- 22.Surace SJ, Deitch J, Johnston RV, Buchbinder R. Shock wave therapy for rotator cuff disease with or without calcification. Cochrane Database Syst Rev. 2020;3:CD008962. doi: 10.1002/14651858.CD008962.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Koester MC, Dunn WR, Kuhn JE, Spindler KP. The efficacy of subacromial corticosteroid injection in the treatment of rotator cuff disease: a systematic review. J Am Acad Orthop Surg. 2007;15:3–11. doi: 10.5435/00124635-200701000-00002. [DOI] [PubMed] [Google Scholar]
- 24.Penning LI, de Bie RA, Walenkamp GH. The effectiveness of injections of hyaluronic acid or corticosteroid in patients with subacromial impingement: a three-arm randomised controlled trial. J Bone Joint Surg Br. 2012;94:1246–1252. doi: 10.1302/0301-620X.94B9.28750. [DOI] [PubMed] [Google Scholar]
- 25.Kew ME, Cancienne JM, Christensen JE, Werner BC. The timing of corticosteroid injections after arthroscopic shoulder procedures affects postoperative infection risk. Am J Sports Med. 2019;47:915–921. doi: 10.1177/0363546518825348. [DOI] [PubMed] [Google Scholar]
- 26.Forsythe B, Agarwalla A, Puzzitiello RN, Sumner S, Romeo AA, Mascarenhas R. The timing of injections prior to arthroscopic rotator cuff repair impacts the risk of surgical site infection. J Bone Joint Surg Am. 2019;101:682–687. doi: 10.2106/JBJS.18.00631. [DOI] [PubMed] [Google Scholar]
- 27.Cook T, Minns Lowe C, Maybury M, Lewis JS. Are corticosteroid injections more beneficial than anaesthetic injections alone in the management of rotator cuff-related shoulder pain? A systematic review. Br J Sports Med. 2018;52:497–504. doi: 10.1136/bjsports-2016-097444. [DOI] [PubMed] [Google Scholar]
- 28.Peng Y, Li F, Ding Y, Sun X, Wang G, Jia S, Zheng C. Comparison of the effects of platelet-rich plasma and corticosteroid injection in rotator cuff disease treatment: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2023;32:1303–1313. doi: 10.1016/j.jse.2023.01.037. [DOI] [PubMed] [Google Scholar]
- 29.Ketola S, Lehtinen J, Elo P, Kortelainen S, Huhtala H, Arnala I. No difference in long-term development of rotator cuff rupture and muscle volumes in impingement patients with or without decompression. Acta Orthop. 2016;87:351–355. doi: 10.1080/17453674.2016.1177780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ryosa A, Laimi K, Aarimaa V, Lehtimaki K, Kukkonen J, Saltychev M. Surgery or conservative treatment for rotator cuff tear: a meta-analysis. Disabil Rehabil. 2017;39:1357–1363. doi: 10.1080/09638288.2016.1198431. [DOI] [PubMed] [Google Scholar]
- 31.Para-Garcia G, Garcia-Munoz AM, Lopez-Gil JF, Ruiz-Cardenas JD, Garcia-Guillen AI, Lopez-Roman FJ, Perez-Pinero S, Abellan-Ruiz MS, Canovas F, Victoria-Montesinos D. Dry needling alone or in combination with exercise therapy versus other interventions for reducing pain and disability in subacromial pain syndrome: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19:10961. doi: 10.3390/ijerph191710961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cagnie B, Dewitte V, Barbe T, Timmermans F, Delrue N, Meeus M. Physiologic effects of dry needling. Curr Pain Headache Rep. 2013;17:348. doi: 10.1007/s11916-013-0348-5. [DOI] [PubMed] [Google Scholar]
- 33.Fernandez-de-Las-Penas C, Nijs J. Trigger point dry needling for the treatment of myofascial pain syndrome: current perspectives within a pain neuroscience paradigm. J Pain Res. 2019;12:1899–1911. doi: 10.2147/JPR.S154728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dommerholt J. Dry needling - peripheral and central considerations. J Man Manip Ther. 2011;19:223–227. doi: 10.1179/106698111X13129729552065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Shah JP, Phillips TM, Danoff JV, Gerber LH. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J Appl Physiol (1985) 2005;99:1977–1984. doi: 10.1152/japplphysiol.00419.2005. [DOI] [PubMed] [Google Scholar]
- 36.Shah JP, Gilliams EA. Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. J Bodyw Mov Ther. 2008;12:371–384. doi: 10.1016/j.jbmt.2008.06.006. [DOI] [PubMed] [Google Scholar]
- 37.Kavoussi B, Ross BE. The neuroimmune basis of anti-inflammatory acupuncture. Integr Cancer Ther. 2007;6:251–257. doi: 10.1177/1534735407305892. [DOI] [PubMed] [Google Scholar]
- 38.Langevin HM, Bouffard NA, Churchill DL, Badger GJ. Connective tissue fibroblast response to acupuncture: dose-dependent effect of bidirectional needle rotation. J Altern Complement Med. 2007;13:355–360. doi: 10.1089/acm.2007.6351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Min S, Lee H, Kim SY, Park JY, Chae Y, Lee H, Park HJ. Local changes in microcirculation and the analgesic effects of acupuncture: a laser Doppler perfusion imaging study. J Altern Complement Med. 2015;21:46–52. doi: 10.1089/acm.2013.0442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Liu QG, Liu L, Huang QM, Nguyen TT, Ma YT, Zhao JM. Decreased spontaneous electrical activity and acetylcholine at myofascial trigger spots after dry needling treatment: a pilot study. Evid Based Complement Alternat Med. 2017;2017:3938191. doi: 10.1155/2017/3938191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Abbaszadeh-Amirdehi M, Ansari NN, Naghdi S, Olyaei G, Nourbakhsh MR. Neurophysiological and clinical effects of dry needling in patients with upper trapezius myofascial trigger points. J Bodyw Mov Ther. 2017;21:48–52. doi: 10.1016/j.jbmt.2016.04.014. [DOI] [PubMed] [Google Scholar]
- 42.Lazaro-Navas I, Lorenzo-Sanchez-Aguilera C, Pecos-Martin D, Jimenez-Rejano JJ, Navarro-Santana MJ, Fernandez-Carnero J, Gallego-Izquierdo T. Immediate effects of dry needling on the autonomic nervous system and mechanical hyperalgesia: a randomized controlled trial. Int J Environ Res Public Health. 2021;18:6018. doi: 10.3390/ijerph18116018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kubo K, Iizuka Y, Yajima H, Takayama M, Takakura N. Changes in blood circulation of the tendons and heart rate variability during and after acupuncture. Med Acupunct. 2020;32:99–107. doi: 10.1089/acu.2019.1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sanchez-Infante J, Navarro-Santana MJ, Bravo-Sanchez A, Jimenez-Diaz F, Abian-Vicen J. Is dry needling applied by physical therapists effective for pain in musculoskeletal conditions? A systematic review and meta-analysis. Phys Ther. 2021;101:pzab070. doi: 10.1093/ptj/pzab070. [DOI] [PubMed] [Google Scholar]
- 45.Blanco-Diaz M, Ruiz-Redondo R, Escobio-Prieto I, De la Fuente-Costa M, Albornoz-Cabello M, Casana J. A systematic review of the effectiveness of dry needling in subacromial syndrome. Biology (Basel) 2022;11:243. doi: 10.3390/biology11020243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, Thomas J. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:ED000142. doi: 10.1002/14651858.ED000142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–721. [PubMed] [Google Scholar]
- 48.Schunemann HJ, Oxman AD, Brozek J, Glasziou P, Bossuyt P, Chang S, Muti P, Jaeschke R, Guyatt GH. GRADE: assessing the quality of evidence for diagnostic recommendations. Evid Based Med. 2008;13:162–163. doi: 10.1136/ebm.13.6.162-a. [DOI] [PubMed] [Google Scholar]
- 49.Austin TM, Richter RR, Sebelski CA. Introduction to the GRADE approach for guideline development: considerations for physical therapist practice. Phys Ther. 2014;94:1652–1659. doi: 10.2522/ptj.20130627. [DOI] [PubMed] [Google Scholar]
- 50.Arias-Buria JL, Fernandez-de-Las-Penas C, Palacios-Cena M, Koppenhaver SL, Salom-Moreno J. Exercises and dry needling for subacromial pain syndrome: a randomized parallel-group trial. J Pain. 2017;18:11–18. doi: 10.1016/j.jpain.2016.08.013. [DOI] [PubMed] [Google Scholar]
- 51.Imani M, Abbasi L, Taghizadeh S, Amiri M. Comparison of the effect of two different types of dry-needling techniques on subacromial impingement syndrome. J Bodyw Mov Ther. 2021;25:35–40. doi: 10.1016/j.jbmt.2020.10.018. [DOI] [PubMed] [Google Scholar]
- 52.Johansson K, Bergstrom A, Schroder K, Foldevi M. Subacromial corticosteroid injection or acupuncture with home exercises when treating patients with subacromial impingement in primary care--a randomized clinical trial. Fam Pract. 2011;28:355–365. doi: 10.1093/fampra/cmq119. [DOI] [PubMed] [Google Scholar]
- 53.Johansson KM, Adolfsson LE, Foldevi MO. Effects of acupuncture versus ultrasound in patients with impingement syndrome: randomized clinical trial. Phys Ther. 2005;85:490–501. [PubMed] [Google Scholar]
- 54.Kibar S, Konak HE, Evcik D, Ay S. Laser acupuncture treatment improves pain and functional status in patients with subacromial impingement syndrome: a randomized, double-blind, sham-controlled study. Pain Med. 2017;18:980–987. doi: 10.1093/pm/pnw197. [DOI] [PubMed] [Google Scholar]
- 55.Kleinhenz J, Streitberger K, Windeler J, Gussbacher A, Mavridis G, Martin E. Randomised clinical trial comparing the effects of acupuncture and a newly designed placebo needle in rotator cuff tendinitis. Pain. 1999;83:235–241. doi: 10.1016/s0304-3959(99)00107-4. [DOI] [PubMed] [Google Scholar]
- 56.Rha DW, Park GY, Kim YK, Kim MT, Lee SC. Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial. Clin Rehabil. 2013;27:113–122. doi: 10.1177/0269215512448388. [DOI] [PubMed] [Google Scholar]
- 57.Rueda Garrido JC, Vas J, Lopez DR. Acupuncture treatment of shoulder impingement syndrome: a randomized controlled trial. Complement Ther Med. 2016;25:92–97. doi: 10.1016/j.ctim.2016.01.003. [DOI] [PubMed] [Google Scholar]
- 58.Song W, Wang X, Zhou J, Shi P, Gu W, Fang F. Rehabilitation of an analgesic bracelet based on wrist-ankle acupuncture in patients with rotator cuff injury: a randomized trial. Pain Res Manag. 2021;2021:9946548. doi: 10.1155/2021/9946548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Vas J, Ortega C, Olmo V, Perez-Fernandez F, Hernandez L, Medina I, Seminario JM, Herrera A, Luna F, Perea-Milla E, Mendez C, Madrazo F, Jimenez C, Ruiz MA, Aguilar I. Single-point acupuncture and physiotherapy for the treatment of painful shoulder: a multicentre randomized controlled trial. Rheumatology (Oxford) 2008;47:887–893. doi: 10.1093/rheumatology/ken040. [DOI] [PubMed] [Google Scholar]
- 60.Wang Y, Wang C, Chen H, Ye X. Shoulder joint pain of rotator cuff injury treated with electroacupuncture and Mulligan’s mobilization: a randomized controlled trial. Zhongguo Zhen Jiu. 2018;38:17–21. doi: 10.13703/j.0255-2930.2018.01.004. [DOI] [PubMed] [Google Scholar]
- 61.Molsberger AF, Schneider T, Gotthardt H, Drabik A. German Randomized Acupuncture Trial for chronic shoulder pain (GRASP) - a pragmatic, controlled, patient-blinded, multi-centre trial in an outpatient care environment. Pain. 2010;151:146–154. doi: 10.1016/j.pain.2010.06.036. [DOI] [PubMed] [Google Scholar]
- 62.Weber S, Chahal J. Management of rotator cuff injuries. J Am Acad Orthop Surg. 2020;28:e193–e201. doi: 10.5435/JAAOS-D-19-00463. [DOI] [PubMed] [Google Scholar]
- 63.Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-rich plasma: new performance understandings and therapeutic considerations in 2020. Int J Mol Sci. 2020;21:7794. doi: 10.3390/ijms21207794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Pang L, Xu Y, Li T, Li Y, Zhu J, Tang X. Platelet-rich plasma injection can be a viable alternative to corticosteroid injection for conservative treatment of rotator cuff disease: a meta-analysis of randomized controlled trials. Arthroscopy. 2023;39:402–421. e401. doi: 10.1016/j.arthro.2022.06.022. [DOI] [PubMed] [Google Scholar]
- 65.Griswold D, Learman K, Ickert E, Tapp A, Ross O. Dry needling for subacromial pain syndrome: a systematic review with meta-analysis. Pain Med. 2023;24:285–299. doi: 10.1093/pm/pnac131. [DOI] [PubMed] [Google Scholar]
- 66.Srbely JZ, Dickey JP, Lee D, Lowerison M. Dry needle stimulation of myofascial trigger points evokes segmental anti-nociceptive effects. J Rehabil Med. 2010;42:463–468. doi: 10.2340/16501977-0535. [DOI] [PubMed] [Google Scholar]
- 67.Kubo K, Yajima H, Takayama M, Ikebukuro T, Mizoguchi H, Takakura N. Effects of acupuncture and heating on blood volume and oxygen saturation of human Achilles tendon in vivo. Eur J Appl Physiol. 2010;109:545–550. doi: 10.1007/s00421-010-1368-z. [DOI] [PubMed] [Google Scholar]
- 68.Sandberg M, Lundeberg T, Lindberg LG, Gerdle B. Effects of acupuncture on skin and muscle blood flow in healthy subjects. Eur J Appl Physiol. 2003;90:114–119. doi: 10.1007/s00421-003-0825-3. [DOI] [PubMed] [Google Scholar]
- 69.Shinbara H, Okubo M, Sumiya E, Fukuda F, Yano T, Kitade T. Effects of manual acupuncture with sparrow pecking on muscle blood flow of normal and denervated hindlimb in rats. Acupunct Med. 2008;26:149–159. doi: 10.1136/aim.26.3.149. [DOI] [PubMed] [Google Scholar]
- 70.Boyce D, Wempe H, Campbell C, Fuehne S, Zylstra E, Smith G, Wingard C, Jones R. Adverse events associated with therapeutic dry needling. Int J Sports Phys Ther. 2020;15:103–113. [PMC free article] [PubMed] [Google Scholar]
- 71.Pieters L, Lewis J, Kuppens K, Jochems J, Bruijstens T, Joossens L, Struyf F. An update of systematic reviews examining the effectiveness of conservative physical therapy interventions for subacromial shoulder pain. J Orthop Sports Phys Ther. 2020;50:131–141. doi: 10.2519/jospt.2020.8498. [DOI] [PubMed] [Google Scholar]
- 72.Savovic J, Jones HE, Altman DG, Harris RJ, Juni P, Pildal J, Als-Nielsen B, Balk EM, Gluud C, Gluud LL, Ioannidis JP, Schulz KF, Beynon R, Welton NJ, Wood L, Moher D, Deeks JJ, Sterne JA. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann Intern Med. 2012;157:429–438. doi: 10.7326/0003-4819-157-6-201209180-00537. [DOI] [PubMed] [Google Scholar]
- 73.Braithwaite FA, Walters JL, Li LSK, Moseley GL, Williams MT, McEvoy MP. Effectiveness and adequacy of blinding in the moderation of pain outcomes: systematic review and meta-analyses of dry needling trials. PeerJ. 2018;6:e5318. doi: 10.7717/peerj.5318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, Vist GE, Falck-Ytter Y, Meerpohl J, Norris S, Guyatt GH. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–406. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.