

Abstract
Background
eHealth interventions have been postulated as a feasible, acceptable, and possibly effective tool to promote physical activity (PA) among children and adolescents; however, a comprehensive quantitative analysis of the effects of eHealth interventions promoting PA is lacking.
Objective
This study aims to conduct a systematic review and meta-analysis on experimental studies reporting the effects of eHealth interventions aimed at promoting PA on PA parameters and sedentary behavior parameters in children and adolescents.
Methods
The CENTRAL, MEDLINE, Embase, and Web of Science databases were searched from inception to February 2022 for randomized controlled trials that analyzed the effects of eHealth interventions aimed at promoting PA on PA and sedentary parameters in children and adolescents. The Hartung-Knapp-Sidik-Jonkman random effects method was used to determine the mean differences (MDs) with their respective 95% CIs. The risk of bias was assessed using the Risk of Bias 2 (RoB2; Cochrane) tool and its extension for cluster randomized controlled trials. The certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool.
Results
A total of 20 trials reporting the effects of different eHealth interventions aimed at promoting PA were included. Results for each parameter were as follows: counts per minute (MD −16.11 counts, 95% CI −122.76 to 90.53; k=3; n=402; I2=69%; favoring control), steps per day (MD 593.46 steps, 95% CI −2102.27 to 3289.19; k=2; n=152; I2=0%; favoring intervention [FI]), moderate to vigorous PA (MD −1.99 min/d, 95% CI −8.95 to 4.96; k=14; n=2336; I2=86%; favoring control), light PA (MD 3.28 min/d, 95% CI −15.48 to 22.04; k=5; n=355; I2=67%; FI), screen time (MD −31.48 min/d, 95% CI −68.62 to 5.65; k=5; n=904; I2=0%; FI), and sedentary time (MD −33.12 min/d, 95% CI −57.27 to −8.97; k=8; n=819; I2=75%; FI). Our results should be interpreted cautiously because of important limitations such as the scarcity of evidence, overall risk of bias, and low to very low certainty of evidence.
Conclusions
We did not find conclusive evidence regarding the impact of PA-targeted eHealth interventions on PA parameters, but the very low certainty of evidence suggests that eHealth interventions may reduce sedentary time in children and adolescents. Our results may have important scientific implications as they highlight that the rapid development of eHealth interventions to promote PA lacks robust supporting evidence.
Trial Registration
PROSPERO CRD42020211020; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=211020
Keywords: eHealth technologies, physical activity, sedentary behaviors, children, mobile phone
Introduction
Physical inactivity is considered one of the most important modifiable risk factors for noncommunicable diseases, as 1.6 million deaths per year can be attributed to insufficient physical activity (PA) [1]. Moreover, physical inactivity is associated with an increased risk of cardiovascular disease, hypertension, type 2 diabetes, multiple types of cancer, dementia, depression, as well as cardiovascular disease–related mortality and all-cause mortality in adults [2,3]. As childhood PA-related behaviors are associated with cardiometabolic risk and tend to endure from childhood through adolescence into adulthood [4,5], the promotion of PA at early ages is not only a cardiometabolic prevention strategy but can also be considered an adult prevention intervention [6-8].
According to the World Health Organization guidelines, children and adolescents (aged 5 to 17 years) should engage in an average of 60 minutes of moderate to vigorous PA (MVPA) per day and limit their sedentary time. In addition, these guidelines recommend that vigorous PA and muscle- and bone-strengthening activities should each be incorporated at least 3 days per week [9,10]. However, approximately 70% of this age group do not meet these recommendations [11]. Consequently, the intervention strategies for PA promotion in children and adolescents remain an important public health topic. Understanding waking activities as a continuum, where sedentary behaviors are waking activities characterized by low energy expenditure and performed in a sitting or reclining posture [12], interventions aimed at increasing energy expenditure during waking time may be able to increase PA while diminishing sedentary time.
Despite evidence supporting the substantial health benefits of engaging in adequate levels of PA and decreasing sedentary behaviors during childhood [13-15], interventions promoting PA targeting children and adolescents have shown serious shortcomings, including a lack of scalability, high costs, or difficulties in sustaining or implementing them [16]. Therefore, finding feasible, scalable, and effective interventions to encourage children and adolescents to adopt active lifestyles is a public health priority [17].
eHealth is defined as a cost-effective and safe use of information and communication technologies in support of health and health-related domains, enabling better communication between practitioners and patient practitioners, better monitoring and data management, and acting as a vehicle to deliver health information and interventions for prevention and care [18]. eHealth has been postulated as a feasible, acceptable, and possibly effective tool for promoting PA among children and adolescents [19]. The potential of eHealth interventions to engage young population not only resides in the fact that they are digital natives but also on the characteristics and diverse possibilities of eHealth delivery; these include features such as allowance for tailored feedback, monitoring, direct interaction, report on goals and track of progress, or access to a community [19,20].
Previous systematic reviews and meta-analyses studying the effects of mobile health (mHealth) technologies [21-28], SMS text message interventions [29], and digital interventions [30] in children and adolescents on PA and sedentary behavior parameters are inconclusive. However, when the horizon is broadened to analyze eHealth interventions aimed at promoting PA as a whole, they are postulated as a successful approach to increase PA; however, there is a lack of quantitative synthesis to support such conclusions [19,20]. This makes it difficult to make a pronouncement on the pillars of solid evidence as to whether the eHealth interventions that promote PA can be more effective than traditional PA promotion interventions.
Furthermore, owing to the scarcity and heterogeneity of available data, previous evidence [19-30] supports the necessity for more comparable studies to accumulate meaningful evidence.
The most recent study [22] showed the most promising results by only analyzing smartphone-based interventions, but the effect size pooled estimates show a mix of very different PA-related outcome measures (steps, counts, distance, and intensity of PA) that, in most cases, are not interchangeable with each other. In accordance with these inconsistencies, a comprehensive quantitative analysis of the effects of different eHealth interventions aimed at promoting PA on PA and sedentary behaviors is lacking.
Consequently, this systematic review and meta-analysis aims to comprehensively analyze the available scientific literature on the effect of eHealth interventions promoting PA on PA parameters (count/min, steps/d, light PA [LPA], and MVPA) and sedentary behavior parameters (screen time and sedentary time) in children and adolescents and to clarify the potential reasons for the conflicting results. For this purpose, we will analyze the effect of eHealth interventions promoting PA compared with a control (waitlist, nontreatment, or minimal alternative intervention), hence analyzing the combination of intervention content (PA promotion) and intervention delivery mechanism (eHealth).
Methods
Systematic Review
This systematic review and meta-analysis has been reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [31] and the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [32] and was registered in PROSPERO (CRD42020211020), which has been modified to broaden the scope, changing the intervention scope (mHealth to eHealth) and the population (children to children and adolescents).
Search Strategy
A systematic search of the literature was conducted in the CENTRAL, Embase (via Scopus), MEDLINE (via PubMed), and Web of Science databases from inception of the database to February 2022. The search strategy was designed using the PICO (patient, intervention, comparison, and outcomes) strategy, as shown in Textbox 1. The search strategy was designed combining the following relevant terms: (1) “m-health,” “ehealth,” “ICT,” “technology assisted,” “mobile technology,” “health technology,” “internet based,” “mobile health” and “mobile phone-based”; (2) “physical activity,” “exercise,” “fitness,” “cardiorespiratory fitness,” “aerobic fitness,” “physical fitness,” “step-count,” “daily steps,” “daily activity counts,” “sedentar*” and “screen-time”; (3) “effect,” “effecti*” and “evaluation”; and (4) “child*,” “infant,” “kids,” “young,” “adolescents.” Moreover, a reverse search was performed by checking the reference lists of previous systematic reviews and meta-analyses for other relevant studies. Moreover, previous systematic reviews [19-30] were reviewed to perform a reverse search. Detailed search strategies for each database are included in Table S1 of Multimedia Appendix 1 [33-57].
Summary of the eligibility criteria following the PICO (patient, intervention, comparison, and outcomes) strategy.
Population
Inclusion: children and adolescents with mean age between 5 and 17 years without physical or psychological morbidities that would prevent the realization of the respective interventions
Exclusion: studies including adult populations where disaggregation of data for children, adolescents, and adults was not possible
Intervention
Inclusion: active monitoring or active interventions including eHealth technologies aimed to promote physical activity (PA) or reduce sedentary behaviors delivered to children and adolescents; multicomponent interventions including eHealth as the main component
Exclusion: passive interventions (eg, nonfeedback monitoring), and multicomponent interventions not including eHealth as the main component or interventions aimed at physical exercise coaching
Comparator
Inclusion: studies with waitlist, nonintervention, or usual care control groups
Exclusion: studies without a control group or with a technology-delivered comparator
Outcome
Inclusion: PA parameters (count/min, steps/d, light PA, and moderate to vigorous PA [MVPA]) and sedentary behavior parameters (screen time and sedentary time)
Exclusion: eHealth intervention studies not involving PA or sedentary behavior parameters as a primary or secondary outcome
Study design
Inclusion: experimental studies including randomized controlled trial (RCT) and feasibility studies with an RCT design
Exclusion: nonexperimental study designs and non–peer-reviewed studies (eg, letters, comments, conference proceedings, reviews, and narrative articles)
Selection of Studies
The eligibility criteria according to the PICO strategy are summarized in Textbox 1. For inclusion in this systematic review and meta-analysis, studies had to meet the following criteria: (1) designed as experimental studies (randomized controlled trials [RCTs] or feasibility studies with an RCT design); (2) interventions delivered to children and adolescents with a mean age between 5 and 17 years without physical or psychological morbidity that would prevent the respective interventions; (3) include active monitoring or active interventions with eHealth technologies as a main component aimed at promoting PA or reducing sedentary behaviors; (4) compared with a waitlist, no to minimal intervention, or usual care control group; and (5) report its effects on PA parameters (count/min, steps/d, LPA, and MVPA) and sedentary behavior parameters (screen time and sedentary time). The study population was limited to ages between 5 and 17 years to use homogeneous samples in physical and psychological development consistent with those used in different PA recommendations [9,10,58].
Studies were included when PA and sedentary behavior parameters were reported according to objective or subjective measures using established thresholds or cut points, not necessarily in the same units. When data were reported using both objective and subjective measures, the objective measures were prioritized. When trials reported multiple follow-up points, the longest available follow-up period was prioritized.
Studies were excluded if they were not written in English or Spanish or if they included adult populations where disaggregation of data for children, adolescents, and adults was not possible. Crossover studies were also excluded because of potential carryover effects resulting from a PA intervention that is not unreasonable to expect to continue for a prolonged period, which limited generalizability. Screening and trial selection were conducted independently by 2 reviewers (ISD and ICR), and disagreements were resolved by consensus.
Data Extraction and Quality Assessment
The following information was extracted from the included studies: (1) study reference, (2) country, (3) study design, (4) population characteristics (sample size, percentage of female participants, mean age, and type of population), (5) outcome variables included, and (6) type of eHealth intervention.
The Cochrane Collaboration tool for assessing the Risk of Bias 2 (RoB2; version 2) [59] was used to assess the potential bias of the included RCTs. Five bias domains were reviewed: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Studies could be rated as “low risk of bias” if all domains are classified as “low risk,” “some concerns” if there is at least 1 domain rated as “some concern,” and “high risk of bias” if there is at least 1 domain rated as “high risk” or ≥3 domains rated as “some concerns.” For cluster RCT, a specific version of the RoB2 tool with additional considerations was used [60], which includes a modification in the first domain to assess the identification or recruitment bias. A risk of bias (RoB) analysis was performed by analyzing the allocation to the intervention in both cases.
Data extraction and quality assessment were independently performed by 2 reviewers (ISD and ICR). Inconsistencies were resolved by consensus or by involving a third researcher (CPM).
Grading the Quality of Evidence
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework was used to evaluate the certainty of evidence provided by this meta-analysis on the different outcomes [61]. Each outcome (counts/min, steps/d, LPA, MVPA, sedentary time, and screen time) could be scored as high, moderate, low, and very low evidence value, depending on the design of the studies, RoB, inconsistency, indirect evidence, imprecision, and publication bias. In this sense, some factors could increase or decrease the quality of the evidence score as follows: (1) RoB (−1 when <75% of the analyzed studies were at low RoB); (2) inconsistency (−1 when I2>50%); (3) indirect evidence related to indirect population, intervention, control, or outcomes; (4) imprecision related to wide CIs; and (5) publication bias (−1 when it exists).
Statistical Analyses
When extracting data from the same trial, priority was given to the most recent and complete objectively measured data. For the statistical analysis, means before and after for both intervention and control groups (longest time after the intervention reported) with their respective SDs were preferably extracted. Data that did not meet these criteria as means before and after and SEs or mean differences (MDs) were extracted and converted. When data were reported as median (IQR), they were converted to mean (SD) following the most correct method according to the sample size devised by Hozo et al [62]. Furthermore, when primary data were reported in different units, unit conversions were performed.
To minimize unit-of-analysis errors when analyzing multiarm trials, similar intervention arms were combined into 1 arm. When interventions were not sufficiently similar, multiple entries were maintained in the splitting control group according to the number of intervention arms. Split samples were also combined.
To check for the normality of each outcome, we evaluated whether the authors tested the normality of the outcome through specific tests, and we calculated the mean/SD ratio for each intervention group (IG) to evaluate skewness.
When cluster RCTs were included, considering that the unit of allocation is the cluster, we checked for proper cluster analysis to avoid unit-of-analysis error [63]. When cluster RCTs were not appropriately analyzed, approximately correct analyses were performed using the inflated SEs method [64].
As opposed to final scores, change scores were analyzed, and when change was not available, final scores were converted to change scores using the following formula: ([pre-T mean – post-T mean] – [pre-C mean – post-C mean]). When studies did not report change scores SDs and the exact correlation coefficients were not available, we assumed a correlation coefficient of 0.5 and calculated change scores SDs using Comprehensive Meta-Analysis software (version 2.2.064; Biostat, Inc.). The Hartung-Knapp-Sidik-Jonkman random effects method was used to compute the pooled MD estimates with their respective 95% CIs in PA parameters (counts/min, steps/d, LPA, and MVPA) and sedentary behavior parameters (sedentary time and screen time) [65]. Only the most recent analyses were included for quantitative synthesis when performed on the same population to avoid sample duplication. Moreover, when studies presented results stratified by sex, age, or weight status, they were analyzed as pooled.
The heterogeneity of results across studies was evaluated using the I2 statistic [30] considering the following values: might not be important (0%-30%), may represent moderate heterogeneity (30%-50%), substantial heterogeneity (50%-75%), or considerable heterogeneity (75%-100%). The corresponding P values were also taken into account [66]. Raw data and all data conversions are provided in the Multimedia Appendix 1.
Exploratory sensitivity analyses were performed to analyze the results when skewed data, high RoB data, and nonobjectively assessed data were removed. To assess the robustness of the pooled estimates and to detect whether any particular study accounted for a large proportion of heterogeneity, sensitivity analyses using the leave-one-out method were conducted. Furthermore, to analyze whether children with comorbidities could have influenced the results, an exploratory sensitivity analysis was performed.
Exploratory random effects meta-regression models were used to evaluate whether summary estimates were influenced by the percentage of female participants and the mean age of the participants. Exploratory multigroup analyses were performed based on the type of eHealth intervention (mobile phone app, multicomponent intervention, telephone-delivered intervention, text messages, or web-based intervention).
Finally, to evaluate publication bias, visual examination of funnel plots and the regression asymmetry test proposed by Egger [67] were used, and a P value <.10 was considered statistically significant.
Statistical analyses were performed using STATA SE software (version 15; StataCorp) and the metagen package from R statistical software (version 4.1.2; R Foundation for Statistical Computing).
Results
Systematic Review
The systematic search, which included an inverse search, retrieved a total of 4087 articles. One study that had not been retrieved through the systematic search was included by contact with experts [33]. After removing duplicates, 146 articles were selected based on the title and abstract screening for a full content review. Finally, 25 reports of 20 studies [33-57] met the inclusion criteria and were included in the systematic review (Figure 1). One study [68] was classified as “awaiting assessment” because more information was needed to clarify whether it was a duplicate report of 1 of the included studies [49]. Excluded studies and their respective reason for exclusion are displayed in Table S2 of Multimedia Appendix 1.
Figure 1.
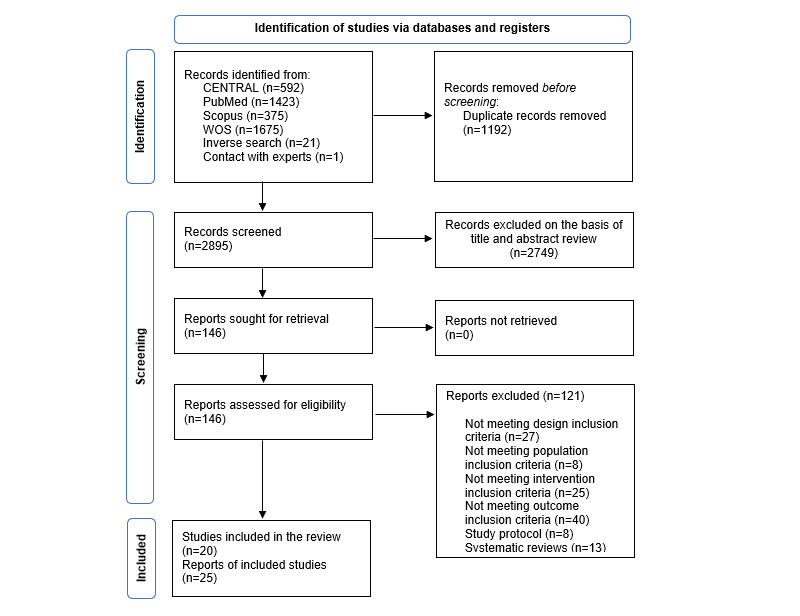
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of the systematic literature search strategy. WOS: Web of Science.
Table 1 summarizes the characteristics of the included studies. All studies meeting the inclusion criteria had an RCT design; 3 studies were pilot randomized trials [43,48,53], and 6 studies [36,37,41,50,52,54] had cluster RCT designs. Studies were published between 2006 and 2020 and were conducted in 7 different countries: Australia (3/20, 15%), Belgium (1/20, 5%), Finland (1/20, 5%), New Zealand (2/20, 10%), the Netherlands (3/20, 15%), the United Kingdom (1/20, 5%), and the United States (7/20, 35%), and 1 study [50] was conducted in 6 different European countries (Austria, Belgium, Crete, Germany, Greece, and Sweden).
Table 1.
Characteristics of the included studies.
| Study type and study name | Reference | Design | Country | Population characteristics | Outcome | |||||||||||||
|
|
|
|
|
Type of population | Participants, n (female) | Age (y), mean (SD) | PAa parameters | Sedentary parameters | ||||||||||
| App intervention | ||||||||||||||||||
|
|
AIMFITb | Direito et al [34], 2015 | RCTc | New Zealand | Healthy adolescents | IGd1: 17 (9); IG2: 16 (10); CGe: 18 (10) | IG1: 15.78 (1.11); IG2: 15.69 (1.04); CG: 15.55 (1.32) | Counts per minute, PAQ-Af, PACESg, light PA, moderate PA, vigorous PA, and MVPAh (min/d) | Sedentary time (min/d) | |||||||||
| Exergame intervention | ||||||||||||||||||
|
|
—i | Staiano et al [35], 2017 | RCT | United States | Adolescents with overweight and obesity | IG: 19 (19); CG: 18 (18) | IG: 15.30 (1.3); CG: 16.10 (1.3) | Light PA, moderate PA, and vigorous PA (min/d) | Sedentary time (min/d) | |||||||||
|
|
GameSquad | Staiano et al [57], 2018 | RCT | United States | Children with overweight and obesity | 46 (21); IG: 23; CG: 23 | 11.2 (0.8) | MVPA (min/d) | — | |||||||||
| Multicomponent intervention | ||||||||||||||||||
|
|
Switch-off 4 Healthy Minds | Babic et al [36], 2016 | Clustered RCT | Australia | Healthy adolescents | IG: 167 (107); CG: 155 (104) | IG: 14.47 (0.6); CG: 14.33 (0.5) | MVPA (min/d) | Screen time (min/d) | |||||||||
|
|
Nutrition and Enjoyable Activity for Teen Girls | Dewar et al [37], 2013 Dewar et al [38], 2014; Lubans et al [39], 2012 | Clustered RCT | Australia | Healthy adolescents | IG: 178 (178) CG: 179 (179) | IG: 13.2 (0.5) CG: 13.2 (0.4) | Counts per minute and MVPA (min/d, %) | Screen time (min/d) and sedentary time (min/d) | |||||||||
|
|
Fit4Life | Huang et al [40], 2014 | RCT | United States | Children surviving acute lymphoblastic leukemia | IG: 19 (7); CG: 19 (8) | IG: 13 (1.74); CG: 13 (1.74) | MVPA (min/d) | — | |||||||||
|
|
Avoiding Screen-time ATLASj | Lubans et al [41], 2016; Smith et al [42], 2014 | Clustered RCT | Australia | Healthy adolescents | IG: 181 (0); CG: 180 (0) | IG: 12.7 (0.5); CG: 12.7 (0.5) | Counts per minute and MVPA (%) | Screen time (min/d) | |||||||||
|
|
— | Mendoza et al [43], 2017 | Pilot RCT | United States | Childhood cancer survivors | IG: 29 (17); CG: 30 (18) | IG: 16.9 (1.5); CG: 16.3 (1.5) | MVPA (min/d) | Sedentary time (min/d) | |||||||||
|
|
Pace-Internet for Diabetes Prevention Intervention (PACEi-DP) | Patrick et al [44], 2013 | RCT | United States | Adolescents with overweight and obesity at risk of type 2 DMk | IG1 (Wl): 26 (16); IG2 (WSMSm): 14 (12); IG3 (WGn): 26 (18); CG: 25 (18) | IG1 (W): 14.1 (1.4); IG2 (WSMS): 14.3 (1.8); IG3 (WG): 14.3 (1.5); CG: 14.5 (1.5) | MVPA (min/wk) | Sedentary time (h/d) | |||||||||
|
|
— | Ruotsalainen et al [33], 2015 | RCT | Finland | Adolescents with overweight and obesity | IG1 (FB+Acto): 15 (10); IG2 (FB): 16 (11); CG: 15 (11) | IG1 (FB+Act): 14.8 (0.8); IG2 (FB): 14.8 (0.8); CG: 15 14.7 (0.8) | Light PA (min/d) and MVPA (min/d) | Sedentary time (min/d) | |||||||||
|
|
— | Thompson et al [45], 2016 | RCT | United States | Healthy adolescents | IG: 40 (17); CG: 40 (20) | 14 to 17 | Steps/d and MVPA (min/d) | — | |||||||||
| Telephone-delivered interventions | ||||||||||||||||||
|
|
Healthy Eating and Activity Today study | Wright et al [46], 2013 | RCT | United States | Children with obesity | IG: 24 (9); CG: 26 (12) | IG: 10.9 (1.3); CG: 10.5 (1.2) | — | Screen time (h/d) | |||||||||
| Text messages intervention | ||||||||||||||||||
|
|
— | Newton et al [47], 2009 | RCT | New Zealand | Adolescents with type 1 DM | IG: 38 (22); CG: 40 (20) | 14.4 (2.37) | Steps/d and MVPA (min/wk) | — | |||||||||
|
|
— | Shapiro et al [48], 2008 | Pilot RCT | United States | Healthy adolescents | IG: 18 (13); CG: 22 (13) | IG: 8.4 (2.3); CG: 8.5 (2.3) | Steps/d | Screen time (min/d) | |||||||||
| Web-based intervention | ||||||||||||||||||
|
|
Rheumates@Work | Armbrust et al [49], 2017 | RCT | The Netherlands | Children with juvenile idiopathic arthritis | IG: 28 (21); CG: 21 (12) | IG: 9.9 (0.78) CG: 10 (0.45) | Light PA (min/d) and MVPA (min/d) | — | |||||||||
|
|
Activ-O-Meter HELENA study | de Bourdeaudhuij et al [50], 2010; Cook et al [51], 2014 | Clustered RCT | Europe | Healthy adolescents | 1050 (515); IG: 581 (NRp); CG: 469 (NR) | 14.5 (1.4) | MVPA (min/wk) | — | |||||||||
|
|
FATaintPHAT | Ezendam et al [52], 2012 | Clustered RCT | The Netherlands | Healthy adolescents | IG: 485 (198); CG: 398 (200) | IG: 12.7 (0.7); CG: 12.6 (2.7) | Steps/d | Screen time (min/d) | |||||||||
|
|
Families Reporting Every Step to Health | Guagliano et al [53], 2020 | Pilot RCT | United Kingdom | Healthy children | IG: 30 (15); CG: 29 (14) | IG: 10.1 (2.8); CG: 8.9 (0.6) | MVPA (min/d) | Sedentary time (min/d) | |||||||||
|
|
— | Haerens et al [54], 2006; Haerens et al [55], 2007 | Clustered RCT | Belgium | Healthy children | IG1: 1194 (479); IG2: 911 (142); CG: 735 (432) | IG1: 13 (0.8); IG2: 13.2 (0.9); CG: 12.9 (0.7) | Light PA (min/d) and MVPA (min/d) | Sedentary time (min/d) | |||||||||
|
|
— | Slootmaker et al [56], 2010 | RCT | The Netherlands | Healthy adolescents | IG: 41 (26); CG: 46 (29) | IG: 15.4 (1.1); CG: 14.9 (1.3) | Light PA (min/wk) and MVPA (min/wk) | Sedentary time (min/wk) | |||||||||
aPA: physical activity.
bAIMFIT: Apps for Improving Fitness.
cRCT: randomized controlled trial.
dIG: intervention group.
eCG: control group.
fPAQ-A: Physical Activity Questionnaire for Adolescents.
gPACES: perceived enjoyment using the Physical Activity Enjoyment Scale.
hMVPA: moderate to vigorous physical activity.
iNot available.
jATLAS: Active Teen Leaders Avoiding Screen-time.
kDM: diabetes mellitus.
lW: website only group.
mWSMS: website and SMS group.
nWG: website, monthly group sessions, and follow-up calls group.
oFB+Act: Facebook-delivered lifestyle counseling+physical activity self-monitoring group
pNR: not reported.
The sample size of the included studies ranged from 37 to 2840 participants (with a mean of 2436/4978, 58.7% female participants), whose ages ranged from 8.4 to 17 years; these studies were performed in children 6-12 years (5/20, 25%) and adolescents 13-17 years (15/20, 75%). Most studies included healthy children or adolescents (11/20, 55%), although several studies included children with physical health problems (overweight or obesity, 5/20, 25%; survivors of cancer, 2/20, 10%; and type 1 diabetes mellitus, 1/20, 5%).
Studies were classified according to the type of eHealth delivering the intervention (mobile apps, 1/20, 5%; exergames, 2/20, 10%; multicomponent interventions, 8/20, 40%; telephone-delivered interventions, 1/20, 5%; text messages, and 2/20, 10%; web-based interventions, 6/20, 30%). With regard to intervention content, most interventions were based on self-determination and social cognitive theories (5/20, 25% and 6/20, 30%, respectively), and included, in most cases, several of the following components: coaching (9/20, 45%), counseling (8/20, 40%), parental counseling (2/20, 10%), monitoring (2/20, 10%) and self-monitoring (3/20, 15%), group sessions (5/20, 25%), and goal setting (4/20, 20%). The duration of the interventions ranged from 8 to 96 weeks, and the dosage was left undetermined owing to the characteristics of the intervention. Most interventions required clinicians’ assistance (13/20, 65%); 20% (4/20) of the interventions were autonomous and 15% (3/20) of the interventions involved the school setting.
For the comparison, most studies used usual behavior (6/20, 30%), waitlist control (5/20, 25%), or no intervention (4/20, 20%). However, minimal interventions such as printed information, 1 group session, or generic advice were also used as control in 25% (5/20) of the studies.
Outcomes measured with objective measures such as accelerometers or pedometers were steps (4/20, 20%), counts (3/20, 15%), LPA (6/20, 30%), MVPA (13/20, 65%), sedentary time (6/20, 30%), and screen time (2/20, 10%). Several outcomes were also measured with self-reported instruments as questionnaires (screen time, 6/20, 30%; sedentary time, 2/20, 10%; or MVPA, 2/20, 10%).
Further details on intervention characteristics and outcome measurement methods are shown in Table S3 in Multimedia Appendix 1.
RoB2 Tool
According to the Cochrane Collaboration’s tool for assessing the RoB, RoB2 for RCTs, 43% (6/14) of the trials showed a high RoB for overall bias, and 43% (6/14) the trials showed some concerns. By domain, no trial showed a high risk for the randomization process, missing outcome data, or selection of the reported result. Only 1 trial showed high risk for assignment to the intervention. The most compromised domain was measurement of the outcome, where 43% (6/14) showed a high RoB, probably owing to the nature of the interventions (Figure S1 in Multimedia Appendix 1).
Cluster RCTs RoB was assessed using a specific version of the RoB2 tool with additional considerations. According to the results, only 6% (1/16) of the trials showed a high RoB owing to a compromise in the measurement of the outcome domain, whereas the rest of the trials showed some concerns for the overall RoB (Figure S2 in Multimedia Appendix 1).
Quality of Evidence
According to the GRADE summary of findings, the main limitations were the high RoB, the substantial heterogeneity, and imprecision among the RCTs included. Therefore, the level of certainty of the findings was very low for counts per minute, LPA, and sedentary time and low for steps per day, MVPA, and screen time (Table S4 in Multimedia Appendix 1).
Meta-Analyses
When analyzing trials with several reports, the most recent and complete objectively measured data were considered for the quantitative synthesis. One study did not report sufficient numerical data to be included in the meta-analysis [57]. Only 1 of the included cluster RCTs [52] did not report an appropriate analysis to avoid “unit-of-analysis error” and did not report sufficient data to perform the inflated SEs method and was therefore excluded from the meta-analysis. Raw data and all conversions are reported in Multimedia Appendix 1.
To minimize the unit-of-analysis errors, studies with similar intervention arms were combined into 1 arm, as in the AIMFIT [34] study (combining IG1 and IG2), the PACEi-DP study [44] (combining IG1, IG2, and IG3), the studies by Haerens et al [54,55] combining IG1 and IG2, and the study by Slootmaker et al [56] combining boys and girls that had been analyzed separately.
None of the included studies reported change score SDs, and the exact correlation coefficients were only available for 1 study [49] for MVPA and LPA outcomes. However, because of the specific characteristics of the population included in this study, such coefficients were not used, and we assumed a correlation coefficient of 0.5 for the calculation of change score SDs.
The pooled MD for counts per minute (Figure 2 [34,37,41,45,47]) was −16.11 counts per minute (95% CI −122.76 to 90.53), with the number of trials (k=3) and number of participants (n=402) favoring control. For steps per day (Figure 2), MD was 593.46 steps (95% CI −2102.27 to 3289.19; k=2; n=152; favoring intervention [FI]). Both had substantial and insignificant heterogeneity values (I2=69% for counts/min I2=0%, for steps/d). The trial by Shapiro et al [48] was excluded from the steps per day analysis owing to its lack of a control group for this parameter.
Figure 2.
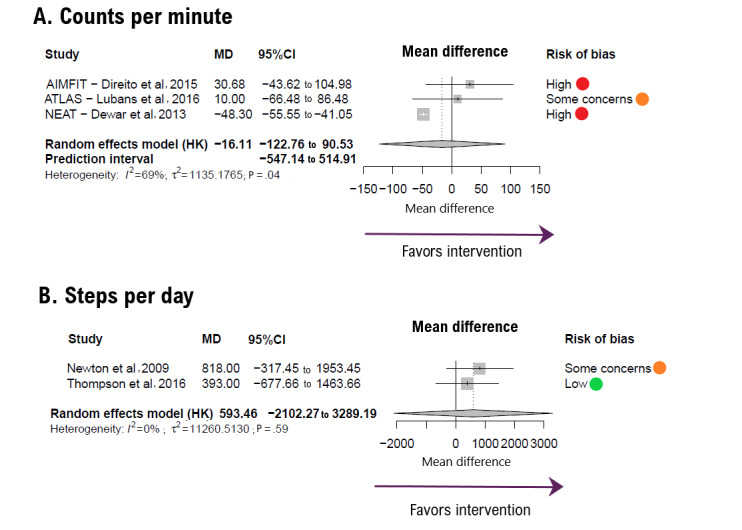
Forest plot showing the effect size for (A) counts per minute and (B) steps per day outcomes. Positive mean difference (MD) values favor intervention. Bold values highlight pooled effects (MD, 95% CI) and their respective prediction intervals. HK: Hartung-Knapp method.
The pooled MD for MVPA (Figure 3 [33,34,36,39,40,43, 45,47,49,50,53,54,56,57]) was −1.99 minute per day (95% CI −8.95 to 4.96; k=14; n=2336; favoring control). After extracting data for the analysis, 1 study [43] showed log transformed data for MVPA and was consequently excluded from the analysis. For LPA (Figure 3), MD was 3.28 minute per day (95% CI −15.48 to 22.04; k=5; n=355; FI). The heterogeneity values were substantial to considerable (I2=86% for MVPA and I2=67%, for LPA).
Figure 3.
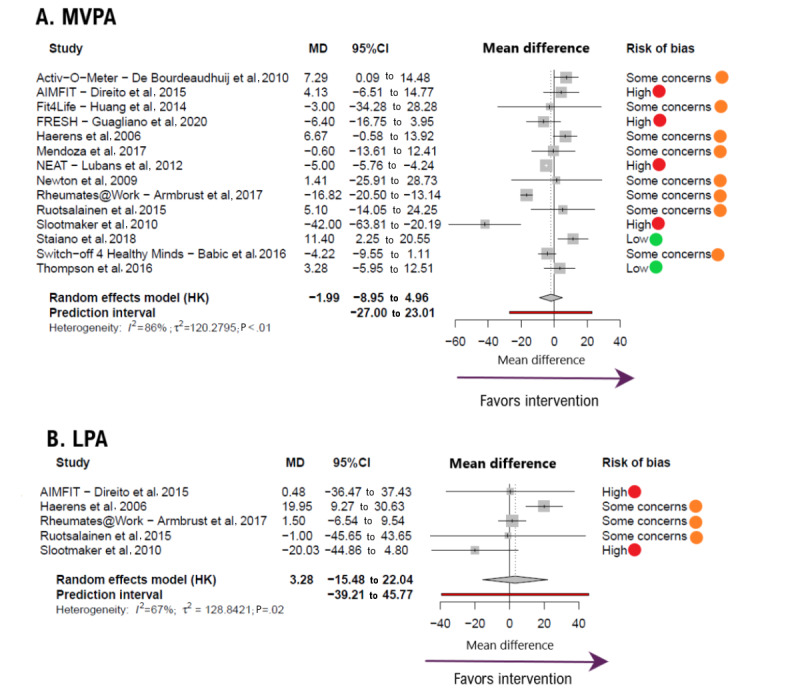
Forest plot showing the effect size for (A) moderate to vigorous physical activity (MVPA) and (B) light physical activity (LPA) outcomes. Positive mean difference (MD) values favor intervention. Bold values highlight pooled effects (MD, 95% CI) and their respective prediction intervals.
For sedentary behavior parameters, the pooled MD for screen time (Figure 4 [33,34,36-38,41,43,44,46,48,53,54,56]) was −31.48 minute per day (95% CI −68.62 to 5.65; k=5; n=904, FI). For sedentary time (Figure 3), the MD was −33.12 minute per day (95% CI −57.27 to −8.97; k=8; n=819; FI). There were no substantial heterogeneity estimates (I2=0% for screen time and I2=75%, for sedentary time).
Figure 4.
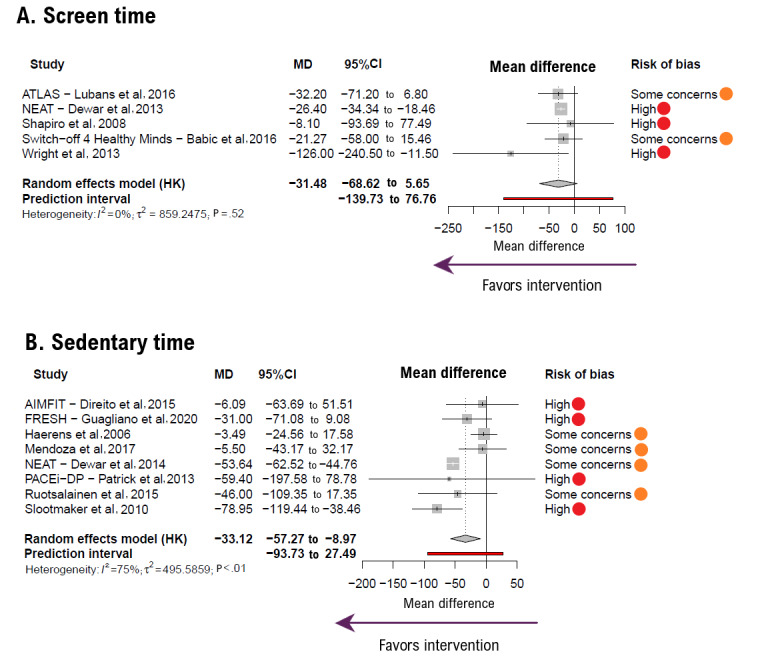
Forest plot showing the effect size for (A) screen time and (B) sedentary time outcomes. Negative mean difference (MD) values favor intervention. Bold values highlight pooled effects (MD, 95% CI) and their respective prediction intervals. HK: Hartung-Knapp method.
Sensitivity Analysis
After evaluating skewness to check for normality of primary data, evidence of skewness was found for several reports in steps per day, MVPA, screen time, and sedentary time analyses, and taking into account the nature of the data, a sensitivity analysis excluding skewed data was performed. Such analysis showed no significant statistical differences from the main analyses, except for the loss of statistical significance in the sedentary time MD (Table 2).
Table 2.
Sensitivity analysis results.
| Outcome | Number of trials | Pooled MDa estimates (95% CI) | I2 (%) | |||
| Pooled MD estimates excluding skewed data | ||||||
|
|
Steps per day | k=1 [44] | 393 (−677.66 to 1463.66) | —b | ||
|
|
MVPAc (min/d) | k=3 [38,48,56] | −18.89 (−63.09 to 25.32) | 95.9 | ||
|
|
Screen time (min/d) | k=1 [36] | −48.30 (−55.55 to −41.05)d | — | ||
|
|
Sedentary time (min/d) | k=4 [33,37,54,56] | −36.69 (−93.97 to 20.58) | 86.9 | ||
| Pooled MD estimates excluding high risk of bias data | ||||||
|
|
Counts per minute | k=1 [40] | 10 (−66.48 to 86.48) | — | ||
|
|
MVPA (min/d) | k=10 [34,35,39,42,44,48,50,54,56,67] | 0.54 (−6.07 to 7.14) | 88.4 | ||
|
|
LPAe (min/d) | k=3 [48,54,67] | 9.27 (−19.10 to 37.65) | 73.3 | ||
|
|
Screen time (min/d) | k=2 [35,40] | −26.41 (−95.73 to 42.91) | 0.0 | ||
|
|
Sedentary time (min/d) | k=4 [37,42,54,67] | −27.08 (−70.79 to 16.63) | 86.8 | ||
| Pooled MD estimates excluding nonobjectively measured data | ||||||
|
|
MVPA (min/d) | k=11 [33-35,38,39,42,44,48,53,54,67] | −1.33 (−7.02 to 4.35) | 85.6 | ||
|
|
LPA (min/d) | k=4 [33,48,54,67] | 8.57 (−8.37 to 25.51) | 60.7 | ||
|
|
Screen time | k=0 | — | — | ||
|
|
Sedentary time (min/d) | k=6 [33,37,42,53,54,67] | −26.45 (−51.80 to −1.10) | 79.8 | ||
| Pooled MD estimates excluding converted data | ||||||
|
|
Counts per minute | k=1 [33] | 10.00 (−66.48 to 86.48) | — | ||
|
|
Steps per day | k=0 | — | — | ||
|
|
MVPA (min/d) | k=6 [33,34,39,50,53,67] | 3.66 (−2.17 to 9.50) | 7.3 | ||
|
|
LPA (min/d) | k=3 [33,54,67] | 14.94 (−11.52 to 41.40) | 0.0 | ||
|
|
Screen time (min/d) | k=2 [45,47] | −60.32 (−804.46 to 683.81) | 61.7 | ||
|
|
Sedentary time (min/d) | k=4 [33,53,54,67] | −15.23 (−44.22 to 13.75) | 0.0 | ||
| Pooled MD estimates including only healthy population | ||||||
|
|
Steps per day | k=1 [44] | 393 (−677.66 to 1463.66) | — | ||
|
|
MVPA (min/d) | k=8 [33,35,38,44,50,53,54,56] | −2.86 (−14.45 to 8.74) | 81.4 | ||
|
|
LPA (min/d) | k=3 [33,54,56] | 2.66 (−50.21 to 55.54) | 77.4 | ||
|
|
Screen time (min/d) | k=4 [35,36,40,47] | −26.20 (−31.06 to −21.34) | 0.0 | ||
|
|
Sedentary time (min/d) | k=5 [33,37,53,54,56] | −35.81 (−74.77 to 3.14) | 82.9 | ||
aMD: mean difference.
bNot available.
cMVPA: moderate to vigorous physical activity.
dItalicized values indicate statistical significance (P≤.05).
eLPA: light physical activity.
In addition, exploratory sensitivity analyses were conducted, excluding trials classified as high RoB and those using nonobjective measurement methods. These results did not significantly differ from the main analyses but differed for sedentary time (Table 2).
Furthermore, owing to the different formats of primary data, an exploratory sensitivity analysis was performed by analyzing only primary data reported as means (SD), which did not significantly differ from the main analysis for the loss of statistical significance in the sedentary time MD (Table 2).
Moreover, studies were removed one at a time from each analysis to examine their individual impact on pooled MD estimates, which were not significantly modified in magnitude or direction when each trial was removed in any of the outcomes.
When performing an exploratory sensitivity analysis including only children and adolescents reported as healthy, only screen time was statistically significantly modified (k=4; –26.20 min/d, 95% CI –31.06 to –21.34).
Meta-Regression and Multiple Group Analysis
Exploratory random effects meta-regression models showed that neither the age of the participants nor the percentage of female participants included in the samples could have influenced the pooled standardized MD estimates for any of the outcomes studied (Table S5 in Multimedia Appendix 1).
Table S6 in Multimedia Appendix 1 shows the results of exploratory multigroup analyses, which, although there were not enough studies to have a meaningful impact on our results, were included along with tests for subgroup differences to show how evidence was distributed between the different types of eHealth interventions. Furthermore, it is important to note that these analyses are derived from observations and lack sufficient statistical power.
Publication Bias
After visually examining the funnel plots (Figures S3-S8 in Multimedia Appendix 1) and performing the Egger tests for each parameter (Table S7 in Multimedia Appendix 1), no evidence of significant publication bias was found.
Discussion
Principal Findings
This systematic review and meta-analysis provides a quantitative analysis of the effects of eHealth interventions on the different parameters of PA and sedentary behavior in children and adolescents. Overall, our results showed that eHealth interventions aimed at increasing PA and decreasing time spent in sedentary behaviors in children did not have a significant effect on increasing PA or decreasing screen time. However, they showed a statistically significant reduction in time spent on sedentary behavior that was not robust to any sensitivity analysis, highlighting the need for further research to confirm these findings.
According to our results, eHealth interventions aimed at promoting PA showed a greater effect on reducing some sedentary behavior parameters, such as time spent in sedentary behaviors or screen time, than on increasing PA, especially MVPA. These findings are in line with the results of previous systematic reviews and meta-analyses [21-23], and considering the importance of PA, especially MVPA for a healthy development [10], the lack of effect of increasing MVPA highlights one of the main limitations of this type of intervention. However, further research is required to elucidate whether more specific interventions or modified interventions could improve MVPA.
The statistically significant reduction in sedentary time, which has not been shown previously when analyzing only mHealth interventions [26], is particularly important because sedentary behaviors, especially screen-associated sedentary behaviors such as screen time, have been recognized as significant contributors to adverse health [69]. Moreover, eHealth interventions have been previously questioned owing to their potentially adverse consequences of increased sedentary screen time and decreased focused attention owing to technology use [70]; hence, our results suggest the possibility of benefits outweighing potential harm. Although it is true that our estimates are based on data from only a few studies and are not robust to sensitivity analyses performed, they need to be confirmed by subsequent studies.
Although the results of previous meta-analyses in older people raise expectations about the usefulness of eHealth interventions for increasing PA [71-73], the results in children have not shown strong beneficial effects on daily waking activities [19-30]. Our findings are in line with previous systematic reviews and meta-analyses [21-23,25-27], as the heterogeneity of the designs, small sample sizes, and variety of outcomes and devices analyzed suggest that further research is needed. This is particularly important given the rapid growth of eHealth technologies, which, considering the high replacement rate, makes studies obsolete in a short period and consequently challenges research to keep pace [74].
Several reasons could be hypothesized to explain these contradictory differences in the effect of eHealth technologies on children and older people, including the following: (1) most interventions in children lack a behavioral change model, or the model is inappropriate; (2) because children are “born connected,” they are assumed to have a literacy in the use of these technologies that may be lacking or may not be sufficient for appropriate use; (3) the use of these technologies may require a change in children’s daily routines, thus requiring parental involvement; and (4) owing to intervention strategies being unable to meet children’s needs, it may be difficult to achieve and maintain motivation and benefit perception to preserve adherence.
In view of these results, should we discard any hope that such interventions are effective in promoting PA? It seems logical that to answer this question, studies must first be conducted to overcome the aforementioned shortcomings (small number of studies, small sample sizes, high heterogeneity, and poor quality) of the studies conducted to date.
eHealth interventions promoting PA, despite controversies about their effectiveness, are described as acceptable, usable, and feasible, with benefits such as cost-effectiveness, potential for real-time data collection, feedback capability, minimized participant burden, and increased dissemination capability [70]. Thus, they are postulated as promising alternatives to truly scalable interventions; however, such benefits must be confirmed through studies involving larger sample sizes. Hence, future research should focus on developing eHealth interventions adapted to the pediatric population, which could be tested in large RCTs with a clearer and comparable methodology.
Limitations
Our results should be interpreted cautiously, as our study has some limitations that should be acknowledged. First, the paucity of comparable RCTs, RCTs registered but not yet published, or gray literature that may have been overlooked in our systematic search may have affected the magnitude of our estimates. Second, the heterogeneity of some of the included interventions owing to differences in their components, length, main outcomes, or measurement instruments may also have affected our findings. Third, the small sample size of some of the included studies decreased the precision of our estimates. Fourth, challenges arise in estimating the independent effect of each component when analyzing multicomponent interventions or interventions whose primary objective is not promoting PA. Fifth, approximately 50% (6/14) of the included trials showed a high RoB, which could compromise the consistency of our findings. Sixth, several exploratory multigroup analyses were performed, even knowing that the Cochrane Handbook for Systematic Reviews of Interventions [32] recommends that these analyses should include at least 10 studies for the same outcome, recognizing the threat it poses to the inferences based on our estimates. Finally, none of the included studies used the mHealth evidence reporting and assessment checklist [75].
Conclusions
Our results provide a comprehensive quantitative analysis of the effects of eHealth interventions on PA and sedentary behavior parameters in children and adolescents according to PRISMA standards (Multimedia Appendix 2). We did not find evidence of an effect of PA-targeted eHealth interventions on PA parameters, but the very low certainty of evidence suggests that eHealth interventions may reduce sedentary time in children and adolescents. Our findings may have an important scientific impact as they highlight that fast-paced advancements in eHealth interventions aimed at promoting PA lack robust supporting evidence.
Acknowledgments
This study was funded by the European Regional Development Fund. CPM was supported by a grant from the University of Castilla-La Mancha (2018-CPUCLM-7939).
Abbreviations
- FI
favoring intervention
- GRADE
Grading of Recommendations Assessment, Development, and Evaluation
- IG
intervention group
- LPA
light physical activity
- MD
mean difference
- mHealth
mobile health
- MVPA
moderate to vigorous physical activity
- PA
physical activity
- PICO
patient, intervention, comparison, and outcomes
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
randomized controlled trial
- RoB
risk of bias
- RoB2
Risk of Bias 2
Supplementary material including in-depth step-by-step analyses.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Footnotes
Conflicts of Interest: None declared.
References
- 1.GBD 2015 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct 08;388(10053):1659–724. doi: 10.1016/S0140-6736(16)31679-8. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(16)31679-8 .S0140-6736(16)31679-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, Edwards P, Woodcock J, Brage S, Wijndaele K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018 Sep;33(9):811–29. doi: 10.1007/s10654-018-0380-1. https://europepmc.org/abstract/MED/29589226 .10.1007/s10654-018-0380-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Katzmarzyk PT, Friedenreich C, Shiroma EJ, Lee IM. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br J Sports Med. 2022 Jan;56(2):101–6. doi: 10.1136/bjsports-2020-103640. https://europepmc.org/abstract/MED/33782046 .bjsports-2020-103640 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yavuz HM, van Ijzendoorn MH, Mesman J, van der Veek S. Interventions aimed at reducing obesity in early childhood: a meta-analysis of programs that involve parents. J Child Psychol Psychiatry. 2015 Jun;56(6):677–92. doi: 10.1111/JCPP.12330. doi: 10.1111/JCPP.12330. [DOI] [PubMed] [Google Scholar]
- 5.Garrido-Miguel M, Cavero-Redondo I, Álvarez-Bueno C, Rodríguez-Artalejo F, Moreno LA, Ruiz JR, Ahrens W, Martínez-Vizcaíno V. Prevalence and trends of overweight and obesity in European children from 1999 to 2016: a systematic review and meta-analysis. JAMA Pediatr. 2019 Oct 01;173(10):e192430. doi: 10.1001/jamapediatrics.2019.2430. https://europepmc.org/abstract/MED/31381031 .2747328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013 Jan 02;309(1):71–82. doi: 10.1001/jama.2012.113905. https://europepmc.org/abstract/MED/23280227 .1555137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Juhola J, Magnussen CG, Viikari JS, Kähönen M, Hutri-Kähönen N, Jula A, Lehtimäki T, Åkerblom HK, Pietikäinen M, Laitinen T, Jokinen E, Taittonen L, Raitakari OT, Juonala M. Tracking of serum lipid levels, blood pressure, and body mass index from childhood to adulthood: the cardiovascular risk in young Finns study. J Pediatr. 2011 Oct;159(4):584–90. doi: 10.1016/j.jpeds.2011.03.021. doi: 10.1016/j.jpeds.2011.03.021.S0022-3476(11)00277-0 [DOI] [PubMed] [Google Scholar]
- 8.Juonala M, Lewis S, McLachlan R, Hammarberg K, Kennedy J, Saffery R, McBain J, Welsh L, Cheung M, Doyle LW, Amor DJ, Burgner DP, Halliday J. American Heart Association ideal cardiovascular health score and subclinical atherosclerosis in 22-35-year-old adults conceived with and without assisted reproductive technologies. Hum Reprod. 2020 Jan 01;35(1):232–9. doi: 10.1093/humrep/dez240. doi: 10.1093/humrep/dez240.5675532 [DOI] [PubMed] [Google Scholar]
- 9.Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, Carty C, Chaput JP, Chastin S, Chou R, Dempsey PC, DiPietro L, Ekelund U, Firth J, Friedenreich CM, Garcia L, Gichu M, Jago R, Katzmarzyk PT, Lambert E, Leitzmann M, Milton K, Ortega FB, Ranasinghe C, Stamatakis E, Tiedemann A, Troiano RP, van der Ploeg HP, Wari V, Willumsen JF. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020 Dec 25;54(24):1451–62. doi: 10.1136/bjsports-2020-102955. http://bjsm.bmj.com/lookup/pmidlookup?view=long&pmid=33239350 .bjsports-2020-102955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, Jago R, Ortega FB, Katzmarzyk PT. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. Int J Behav Nutr Phys Act. 2020 Nov 26;17(1):141. doi: 10.1186/s12966-020-01037-z. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-020-01037-z .10.1186/s12966-020-01037-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tremblay MS, Gray C, Akinroye K, Harrington D, Katzmarzyk P, Lambert EV, Liukkonen J, Maddison R, Ocansey RT, Onywera VO, Prista A, Reilly JJ, Rodríguez Martínez MP, Sarmiento Duenas OL, Standage M, Tomkinson G. Physical activity of children: a global matrix of grades comparing 15 countries. J Phys Act Health. 2014 May;11 Suppl 1:S113–25. doi: 10.1123/jpah.2014-0177. https://journals.humankinetics.com/doi/10.1123/jpah.2014-0177 . [DOI] [PubMed] [Google Scholar]
- 12.Tremblay MS, Aubert S, Barnes J, Saunders T, Carson V, Latimer-Cheung A, Chastin SF, Altenburg TM, Chinapaw MJ. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act. 2017 Jun 10;14(1):75. doi: 10.1186/s12966-017-0525-8. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-017-0525-8 .10.1186/s12966-017-0525-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010 May 11;7:40. doi: 10.1186/1479-5868-7-40/. doi: 10.1186/1479-5868-7-40/.1479-5868-7-40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wu XY, Han LH, Zhang JH, Luo S, Hu JW, Sun K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS One. 2017 Nov 09;12(11):e0187668. doi: 10.1371/journal.pone.0187668. https://dx.plos.org/10.1371/journal.pone.0187668 .PONE-D-17-21727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, Goldfield G, Connor Gorber SC. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011 Sep 21;8:98. doi: 10.1186/1479-5868-8-98. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-8-98 .1479-5868-8-98 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nooijen CF, Galanti MR, Engström K, Möller J, Forsell Y. Effectiveness of interventions on physical activity in overweight or obese children: a systematic review and meta-analysis including studies with objectively measured outcomes. Obes Rev. 2017 Feb;18(2):195–213. doi: 10.1111/obr.12487. doi: 10.1111/obr.12487. [DOI] [PubMed] [Google Scholar]
- 17.Lau PW, Lau EY, Wong DP, Ransdell L. A systematic review of information and communication technology-based interventions for promoting physical activity behavior change in children and adolescents. J Med Internet Res. 2011 Jul 13;13(3):e48. doi: 10.2196/jmir.1533. https://www.jmir.org/2011/3/e48/ v13i3e48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Monitoring and evaluating digital health interventions. World Health Organization. 2016. Dec 12, [2024-02-06]. https://www.who.int/publications/i/item/9789241511766 .
- 19.McIntosh JR, Jay S, Hadden N, Whittaker PJ. Do e-health interventions improve physical activity in young people: a systematic review. Public Health. 2017 Jul;148:140–8. doi: 10.1016/j.puhe.2017.04.001. doi: 10.1016/j.puhe.2017.04.001.S0033-3506(17)30138-5 [DOI] [PubMed] [Google Scholar]
- 20.Norman GJ, Zabinski MF, Adams MA, Rosenberg DE, Yaroch AL, Atienza AA. A review of eHealth interventions for physical activity and dietary behavior change. Am J Prev Med. 2007 Oct;33(4):336–45. doi: 10.1016/j.amepre.2007.05.007. https://europepmc.org/abstract/MED/17888860 .S0749-3797(07)00363-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Böhm B, Karwiese SD, Böhm H, Oberhoffer R. Effects of mobile health including wearable activity trackers to increase physical activity outcomes among healthy children and adolescents: systematic review. JMIR Mhealth Uhealth. 2019 Apr 30;7(4):e8298. doi: 10.2196/mhealth.8298. https://mhealth.jmir.org/2019/4/e8298/ v7i4e8298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.He Z, Wu H, Yu F, Fu J, Sun S, Huang T, Wang R, Chen D, Zhao G, Quan M. Effects of smartphone-based interventions on physical activity in children and adolescents: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2021 Feb 01;9(2):e22601. doi: 10.2196/22601. https://mhealth.jmir.org/2021/2/e22601/ v9i2e22601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Darling KE, Sato AF. Systematic review and meta-analysis examining the effectiveness of mobile health technologies in using self-monitoring for pediatric weight management. Child Obes. 2017 Oct;13(5):347–55. doi: 10.1089/chi.2017.0038. doi: 10.1089/chi.2017.0038. [DOI] [PubMed] [Google Scholar]
- 24.Shin Y, Kim SK, Lee M. Mobile phone interventions to improve adolescents' physical health: a systematic review and meta-analysis. Public Health Nurs. 2019 Nov;36(6):787–99. doi: 10.1111/phn.12655. doi: 10.1111/phn.12655. [DOI] [PubMed] [Google Scholar]
- 25.Turner T, Spruijt-Metz D, Wen CK, Hingle MD. Prevention and treatment of pediatric obesity using mobile and wireless technologies: a systematic review. Pediatr Obes. 2015 Dec;10(6):403–9. doi: 10.1111/ijpo.12002. https://europepmc.org/abstract/MED/25641770 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Baumann H, Fiedler J, Wunsch K, Woll A, Wollesen B. mHealth interventions to reduce physical inactivity and sedentary behavior in children and adolescents: systematic review and meta-analysis of randomized controlled trials. JMIR Mhealth Uhealth. 2022 May 11;10(5):e35920. doi: 10.2196/35920. https://mhealth.jmir.org/2022/5/e35920/ v10i5e35920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Langarizadeh M, Sadeghi M, As'habi A, Rahmati P, Sheikhtaheri A. Mobile apps for weight management in children and adolescents; an updated systematic review. Patient Educ Couns. 2021 Sep;104(9):2181–8. doi: 10.1016/j.pec.2021.01.035. doi: 10.1016/j.pec.2021.01.035.S0738-3991(21)00062-8 [DOI] [PubMed] [Google Scholar]
- 28.Yau KW, Tang TS, Görges M, Pinkney S, Kim AD, Kalia A, Amed S. Effectiveness of mobile apps in promoting healthy behavior changes and preventing obesity in children: systematic review. JMIR Pediatr Parent. 2022 Mar 28;5(1):e34967. doi: 10.2196/34967. https://pediatrics.jmir.org/2022/1/e34967/ v5i1e34967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ludwig K, Arthur R, Sculthorpe N, Fountain H, Buchan DS. Text messaging interventions for improvement in physical activity and sedentary behavior in youth: systematic review. JMIR Mhealth Uhealth. 2018 Sep 17;6(9):e10799. doi: 10.2196/10799. https://mhealth.jmir.org/2018/9/e10799/ v6i9e10799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rose T, Barker M, Maria Jacob C, Morrison L, Lawrence W, Strömmer S, Vogel C, Woods-Townsend K, Farrell D, Inskip H, Baird J. A systematic review of digital interventions for improving the diet and physical activity behaviors of adolescents. J Adolesc Health. 2017 Dec;61(6):669–77. doi: 10.1016/j.jadohealth.2017.05.024. https://europepmc.org/abstract/MED/28822682 .S1054-139X(17)30253-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Page MJ, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. Hoboken, NJ: Wiley; 2019. Sep 20, [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ruotsalainen H, Kyngäs H, Tammelin T, Heikkinen H, Kääriäinen M. Effectiveness of Facebook-delivered lifestyle counselling and physical activity self-monitoring on physical activity and body mass index in overweight and obese adolescents: a randomized controlled trial. Nurs Res Pract. 2015;2015:159205. doi: 10.1155/2015/159205. doi: 10.1155/2015/159205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Direito A, Jiang Y, Whittaker R, Maddison R. Apps for improving fitness and increasing physical activity among young people: the AIMFIT pragmatic randomized controlled trial. J Med Internet Res. 2015 Aug 27;17(8):e210. doi: 10.2196/jmir.4568. https://www.jmir.org/2015/8/e210/ v17i8e210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Staiano AE, Marker AM, Beyl RA, Hsia DS, Katzmarzyk PT, Newton RL. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr Obes. 2017 Apr;12(2):120–8. doi: 10.1111/ijpo.12117. https://europepmc.org/abstract/MED/26918815 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Babic MJ, Smith JJ, Morgan PJ, Lonsdale C, Plotnikoff RC, Eather N, Skinner G, Baker AL, Pollock E, Lubans DR. Intervention to reduce recreational screen-time in adolescents: outcomes and mediators from the 'Switch-Off 4 Healthy Minds' (S4HM) cluster randomized controlled trial. Prev Med. 2016 Oct;91:50–7. doi: 10.1016/j.ypmed.2016.07.014. doi: 10.1016/j.ypmed.2016.07.014.S0091-7435(16)30190-6 [DOI] [PubMed] [Google Scholar]
- 37.Dewar DL, Morgan PJ, Plotnikoff RC, Okely AD, Collins CE, Batterham M, Callister R, Lubans DR. The nutrition and enjoyable activity for teen girls study: a cluster randomized controlled trial. Am J Prev Med. 2013 Sep;45(3):313–7. doi: 10.1016/J.AMEPRE.2013.04.014. doi: 10.1016/J.AMEPRE.2013.04.014.S0749-3797(13)00335-8 [DOI] [PubMed] [Google Scholar]
- 38.Dewar DL, Morgan PJ, Plotnikoff RC, Okely AD, Batterham M, Lubans DR. Exploring changes in physical activity, sedentary behaviors and hypothesized mediators in the NEAT girls group randomized controlled trial. J Sci Med Sport. 2014 Jan;17(1):39–46. doi: 10.1016/J.JSAMS.2013.02.003. doi: 10.1016/J.JSAMS.2013.02.003.S1440-2440(13)00035-2 [DOI] [PubMed] [Google Scholar]
- 39.Lubans DR, Morgan PJ, Okely AD, Dewar D, Collins CE, Batterham M, Callister R, Plotnikoff RC. Preventing obesity among adolescent girls: one-year outcomes of the nutrition and enjoyable activity for teen girls (NEAT Girls) cluster randomized controlled trial. Arch Pediatr Adolesc Med. 2012 Sep 01;166(9):821–7. doi: 10.1001/ARCHPEDIATRICS.2012.41. doi: 10.1001/ARCHPEDIATRICS.2012.41.archpediatrics.2012.41 [DOI] [PubMed] [Google Scholar]
- 40.Huang JS, Dillon L, Terrones L, Schubert L, Roberts W, Finklestein J, Swartz MC, Norman GJ, Patrick K. Fit4Life: a weight loss intervention for children who have survived childhood leukemia. Pediatr Blood Cancer. 2014 May;61(5):894–900. doi: 10.1002/pbc.24937. https://europepmc.org/abstract/MED/24436138 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lubans DR, Smith JJ, Plotnikoff RC, Dally KA, Okely AD, Salmon J, Morgan PJ. Assessing the sustained impact of a school-based obesity prevention program for adolescent boys: the ATLAS cluster randomized controlled trial. Int J Behav Nutr Phys Act. 2016 Aug 20;13:92. doi: 10.1186/s12966-016-0420-8. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-016-0420-8 .10.1186/s12966-016-0420-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Smith JJ, Morgan PJ, Plotnikoff RC, Dally KA, Salmon J, Okely AD, Finn TL, Lubans DR. Smart-phone obesity prevention trial for adolescent boys in low-income communities: the ATLAS RCT. Pediatrics. 2014 Sep;134(3):e723–31. doi: 10.1542/PEDS.2014-1012. doi: 10.1542/PEDS.2014-1012.peds.2014-1012 [DOI] [PubMed] [Google Scholar]
- 43.Mendoza JA, Baker KS, Moreno MA, Whitlock K, Abbey-Lambertz M, Waite A, Colburn T, Chow EJ. A Fitbit and Facebook mHealth intervention for promoting physical activity among adolescent and young adult childhood cancer survivors: a pilot study. Pediatr Blood Cancer. 2017 Dec;64(12) doi: 10.1002/pbc.26660. doi: 10.1002/pbc.26660. [DOI] [PubMed] [Google Scholar]
- 44.Patrick K, Norman GJ, Davila EP, Calfas KJ, Raab F, Gottschalk M, Sallis JF, Godbole S, Covin JR. Outcomes of a 12-month technology-based intervention to promote weight loss in adolescents at risk for type 2 diabetes. J Diabetes Sci Technol. 2013 May 01;7(3):759–70. doi: 10.1177/193229681300700322. https://europepmc.org/abstract/MED/23759410 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Thompson D, Cantu D, Ramirez B, Cullen KW, Baranowski T, Mendoza J, Anderson B, Jago R, Rodgers W, Liu Y. Texting to increase adolescent physical activity: feasibility assessment. Am J Health Behav. 2016 Jul;40(4):472–83. doi: 10.5993/AJHB.40.4.9. https://europepmc.org/abstract/MED/27338994 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wright JA, Phillips BD, Watson BL, Newby PK, Norman GJ, Adams WG. Randomized trial of a family-based, automated, conversational obesity treatment program for underserved populations. Obesity (Silver Spring) 2013 Sep;21(9):E369–78. doi: 10.1002/oby.20388. https://europepmc.org/abstract/MED/23512915 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Newton KH, Wiltshire EJ, Elley CR. Pedometers and text messaging to increase physical activity: randomized controlled trial of adolescents with type 1 diabetes. Diabetes Care. 2009 May;32(5):813–5. doi: 10.2337/dc08-1974. https://europepmc.org/abstract/MED/19228863 .dc08-1974 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Shapiro JR, Bauer S, Hamer RM, Kordy H, Ward D, Bulik CM. Use of text messaging for monitoring sugar-sweetened beverages, physical activity, and screen time in children: a pilot study. J Nutr Educ Behav. 2008;40(6):385–91. doi: 10.1016/j.jneb.2007.09.014. https://europepmc.org/abstract/MED/18984496 .S1499-4046(07)00995-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Armbrust W, Bos GJ, Wulffraat NM, van Brussel M, Cappon J, Dijkstra PU, Geertzen JH, Legger GE, van Rossum MA, Sauer PJ, Lelieveld OT. Internet program for physical activity and exercise capacity in children with juvenile idiopathic arthritis: a multicenter randomized controlled trial. Arthritis Care Res (Hoboken) 2017 Jul;69(7):1040–9. doi: 10.1002/acr.23100. doi: 10.1002/acr.23100. [DOI] [PubMed] [Google Scholar]
- 50.de Bourdeaudhuij I, Maes L, de Henauw S, de Vriendt T, Moreno LA, Kersting M, Sarri K, Manios Y, Widhalm K, Sjöstrom M, Ruiz JR, Haerens L. Evaluation of a computer-tailored physical activity intervention in adolescents in six European countries: the Activ-O-Meter in the HELENA intervention study. J Adolesc Health. 2010 May;46(5):458–66. doi: 10.1016/j.jadohealth.2009.10.006. doi: 10.1016/j.jadohealth.2009.10.006.S1054-139X(09)00595-3 [DOI] [PubMed] [Google Scholar]
- 51.Cook TL, de Bourdeaudhuij I, Maes L, Haerens L, Grammatikaki E, Widhalm K, Kwak L, Plada M, Moreno LA, Zampelas A, Tountas Y, Manios Y. Moderators of the effectiveness of a web-based tailored intervention promoting physical activity in adolescents: the HELENA Activ-O-Meter. J Sch Health. 2014 Apr;84(4):256–66. doi: 10.1111/josh.12140. doi: 10.1111/josh.12140. [DOI] [PubMed] [Google Scholar]
- 52.Ezendam NP, Brug J, Oenema A. Evaluation of the web-based computer-tailored FATaintPHAT intervention to promote energy balance among adolescents: results from a school cluster randomized trial. Arch Pediatr Adolesc Med. 2012 Mar;166(3):248–55. doi: 10.1001/ARCHPEDIATRICS.2011.204. doi: 10.1001/ARCHPEDIATRICS.2011.204.archpediatrics.2011.204 [DOI] [PubMed] [Google Scholar]
- 53.Guagliano JM, Armitage SM, Brown HE, Coombes E, Fusco F, Hughes C, Jones AP, Morton KL, van Sluijs EM. A whole family-based physical activity promotion intervention: findings from the families reporting every step to health (FRESH) pilot randomised controlled trial. Int J Behav Nutr Phys Act. 2020 Sep 22;17(1):120. doi: 10.1186/s12966-020-01025-3. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-020-01025-3 .10.1186/s12966-020-01025-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Haerens L, Deforche B, Maes L, Cardon G, Stevens V, de Bourdeaudhuij I. Evaluation of a 2-year physical activity and healthy eating intervention in middle school children. Health Educ Res. 2006 Dec;21(6):911–21. doi: 10.1093/HER/CYL115. doi: 10.1093/HER/CYL115.cyl115 [DOI] [PubMed] [Google Scholar]
- 55.Haerens L, de Bourdeaudhuij I, Maes L, Cardon G, Deforche B. School-based randomized controlled trial of a physical activity intervention among adolescents. J Adolesc Health. 2007 Mar;40(3):258–65. doi: 10.1016/J.JADOHEALTH.2006.09.028. doi: 10.1016/J.JADOHEALTH.2006.09.028.S1054-139X(06)00389-2 [DOI] [PubMed] [Google Scholar]
- 56.Slootmaker SM, Chinapaw MJ, Seidell JC, van Mechelen W, Schuit AJ. Accelerometers and internet for physical activity promotion in youth? feasibility and effectiveness of a minimal intervention [ISRCTN93896459] Prev Med. 2010 Jul;51(1):31–6. doi: 10.1016/J.YPMED.2010.03.015. doi: 10.1016/J.YPMED.2010.03.015.S0091-7435(10)00111-8 [DOI] [PubMed] [Google Scholar]
- 57.Staiano AE, Beyl RA, Hsia DS, Katzmarzyk PT, Newton RL. Twelve weeks of dance exergaming in overweight and obese adolescent girls: transfer effects on physical activity, screen time, and self-efficacy. J Sport Health Sci. 2017 Mar;6(1):4–10. doi: 10.1016/j.jshs.2016.11.005. https://europepmc.org/abstract/MED/28491483 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Tremblay MS, Carson V, Chaput JP. Introduction to the Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016 Jun;41(6 Suppl 3):iii–iv. doi: 10.1139/apnm-2016-0203. [DOI] [PubMed] [Google Scholar]
- 59.Sterne JA, Savović J, Page M, Elbers R, Blencowe N, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JP. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;366:l4898. doi: 10.1136/bmj.l4898. https://eprints.whiterose.ac.uk/150579/ [DOI] [PubMed] [Google Scholar]
- 60.Minozzi S, Cinquini M, Gianola S, Gonzalez-Lorenzo M, Banzi R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J Clin Epidemiol. 2020 Oct;126:37–44. doi: 10.1016/j.jclinepi.2020.06.015. doi: 10.1016/j.jclinepi.2020.06.015.S0895-4356(20)30181-5 [DOI] [PubMed] [Google Scholar]
- 61.Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the journal of clinical epidemiology. J Clin Epidemiol. 2011 Apr;64(4):380–2. doi: 10.1016/j.jclinepi.2010.09.011. doi: 10.1016/j.jclinepi.2010.09.011.S0895-4356(10)00329-X [DOI] [PubMed] [Google Scholar]
- 62.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005 Apr 20;5:13. doi: 10.1186/1471-2288-5-13. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-5-13 .1471-2288-5-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Whiting-O'Keefe QE, Henke C, Simborg DW. Choosing the correct unit of analysis in medical care experiments. Med Care. 1984 Dec;22(12):1101–14. doi: 10.1097/00005650-198412000-00005. [DOI] [PubMed] [Google Scholar]
- 64.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MW, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions, Second Edition. Hoboken, NJ: John Wiley & Sons; 2019. Including variants on randomized trials. [Google Scholar]
- 65.IntHout J, Ioannidis JP, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. 2014 Feb 18;14:25. doi: 10.1186/1471-2288-14-25. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-14-25 .1471-2288-14-25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002 Jun 15;21(11):1539–58. doi: 10.1002/sim.1186. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 67.Sterne JA, Egger M, Smith GD. Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ. 2001 Jul 14;323(7304):101–5. doi: 10.1136/bmj.323.7304.101. https://europepmc.org/abstract/MED/11451790 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Lelieveld OT, Armbrust W, Geertzen JH, de Graaf I, van Leeuwen MA, Sauer PJ, van Weert E, Bouma J. Promoting physical activity in children with juvenile idiopathic arthritis through an internet-based program: results of a pilot randomized controlled trial. Arthritis Care Res (Hoboken) 2010 May;62(5):697–703. doi: 10.1002/acr.20085. https://onlinelibrary.wiley.com/doi/10.1002/acr.20085 . [DOI] [PubMed] [Google Scholar]
- 69.Saunders TJ, Chaput J, Tremblay M. Sedentary behaviour as an emerging risk factor for cardiometabolic diseases in children and youth. Can J Diabetes. 2014 Mar;38(1):53–61. doi: 10.1016/j.jcjd.2013.08.266. doi: 10.1016/j.jcjd.2013.08.266.S1499-2671(13)01214-8 [DOI] [PubMed] [Google Scholar]
- 70.Tate EB, Spruijt-Metz D, O'Reilly G, Jordan-Marsh M, Gotsis M, Pentz MA, Dunton GF. mHealth approaches to child obesity prevention: successes, unique challenges, and next directions. Transl Behav Med. 2013 Dec;3(4):406–15. doi: 10.1007/s13142-013-0222-3. https://europepmc.org/abstract/MED/24294329 .222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kwan RY, Salihu D, Lee PH, Tse M, Cheung DS, Roopsawang I, Choi KS. The effect of e-health interventions promoting physical activity in older people: a systematic review and meta-analysis. Eur Rev Aging Phys Act. 2020;17:7. doi: 10.1186/s11556-020-00239-5. https://eurapa.biomedcentral.com/articles/10.1186/s11556-020-00239-5 .239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Núñez de Arenas-Arroyo S, Cavero-Redondo I, Alvarez-Bueno C, Sequí-Domínguez I, Reina-Gutiérrez S, Martínez-Vizcaíno V. Effect of eHealth to increase physical activity in healthy adults over 55 years: a systematic review and meta-analysis. Scand J Med Sci Sports. 2021 Apr;31(4):776–89. doi: 10.1111/SMS.13903. doi: 10.1111/SMS.13903. [DOI] [PubMed] [Google Scholar]
- 73.Martin A, Fitzsimons C, Jepson R, Saunders DH, van der Ploeg HP, Teixeira PJ, Gray CM, Mutrie N. Interventions with potential to reduce sedentary time in adults: systematic review and meta-analysis. Br J Sports Med. 2015 Aug;49(16):1056–63. doi: 10.1136/BJSPORTS-2014-094524. doi: 10.1136/BJSPORTS-2014-094524.bjsports-2014-094524 [DOI] [PubMed] [Google Scholar]
- 74.Lee AM, Chavez S, Bian J, Thompson LA, Gurka MJ, Williamson VG, Modave F. Efficacy and effectiveness of mobile health technologies for facilitating physical activity in adolescents: scoping review. JMIR Mhealth Uhealth. 2019 Mar 12;7(2):e11847. doi: 10.2196/11847. https://mhealth.jmir.org/2019/2/e11847/ v7i2e11847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Agarwal S, LeFevre AE, Lee J, L'Engle K, Mehl G, Sinha C, Labrique A. Guidelines for reporting of health interventions using mobile phones: mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ. 2016 Mar 17;352:i1174. doi: 10.1136/bmj.i1174. doi: 10.1136/bmj.i1174. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material including in-depth step-by-step analyses.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.