

Abstract
The stillbirth rate is among the most important indicators of access to and quality of care during pregnancy. This study investigated the factors related to the stillbirth rate in the Yazd province, Iran. The current research is descriptive and cross-sectional and the results of Shahdieh city cohort study which was conducted on 4756 women were used. Data related to the history of stillbirth, demographic characteristics, fertility history and, various female diseases were extracted from the results of the cohort study. The result shows that 7.2% of studied women had a history of stillbirth. Among the multiple variables, predictor variables including education level, marriage age, age of the first conception, number of children, consanguineous marriage, Employment status, and diseases like diabetes, hypertension, and history of depression had a significant relationship with a history of stillbirth (P ≤ .05). The stillbirth rate in Shahedieh is high compared to the global stillbirth Rate, but it is comparable with the stillbirth Rate in Yazd province. Although Yazd province, as one of the industrial hubs of Iran, has relatively acceptable indicators of income, employment, and medical and health facilities and welfare compared to other provinces, this study showed that factors such as diabetes, hypertension, low level of women’s education, consanguineous marriage, and women’s employment status and social welfare can affect Stillbirth Rate.
Keywords: stillbirth, pregnancy, socioeconomic factors, risk factors, death
What do we already know about this topic?
A lot of research has been done on the issue of stillbirth and many articles have been published.
How does your research contribute to the field?
Our study can give new dimensions to previous studies or explore the results of similar studies further.
What are your research’s implications toward theory, practice, or policy?
The results of our study make it clear that economic and social conditions affect the health of mothers, especially pregnant mothers, and, in this way, politicians and social and economic activists can be warned and informed about this.
Introduction
The global Stillbirth Rate in 2015 was 18.4 per 1000 live births 1 and based on available data, 98% of stillbirths occur in developing or underdeveloped countries, showing that this index is related to the availability of facilities such as mothers’ access to specialized care and economic and welfare facilities during pregnancy.1,2
The WHO aims to reduce the Stillbirth Rate to 12 per 1000 by 2030. 3 Numerous factors have been raised to affect women’s Stillbirth Rate across the world, including economic reasons and even the type of occupation of women so that a comparably higher percentage of mothers experiencing stillbirth have been reported to have low economic status and unfavorable relationships with their husbands.4 -6 Risk factors for stillbirth include parity, history of miscarriage, uterine abnormalities, smoking, use of certain medications, infections in pregnancy, placental problems, amniotic fluid disorders, radiation exposure, maternal underlying diseases, fetal factors, and blood incompatibility.7,8 In Iran, according to the report of the World Health Organization (WHO) in 2015, the stillbirth rate was 6.4 per 1000 births. 9
Considering that the factors related to stillbirth in Yazd province and also the cities of this industrial and immigrant-attracting province 10 have not been investigated recently.
The present study aimed to use the data of a cohort study examining the relationship between demographic characteristics, health indicators, and socio-economic status of women, and their history of stillbirth specify.
Methods
Design and Participants
This descriptive cross-sectional study was conducted using the data of a national cohort study. The Shahedieh cohort study is part of the PERSIAN (Prospective Epidemiological Research Studies of the Iranian Adults) Cohort Study conducted in 18 regions of Iran. The data from Shahedieh collected in the cohort study were used to conduct the present study.
Data Collection Instruments
The number of participants in the Shahedieh cohort was 10 194 individuals. By preliminary data review and selection of married women with a history of pregnancy and elimination of missing cases in the abortion history variable, the information of 4757 women was used to conduct the present study. The cohort study started in May 2014 and ended in September 2015.
Inclusion criteria of the PERSIAN cohort Study were the ages of 35 and 70 years, continuous residence in the city for at least 9 months before the start of the study, mental and physical ability to participate in the study, and providing consent to participate in the study and exclusion criteria included not answering the items completely and lack of volunteering to participate in the study in the interview.
Questionnaires approved by public health experts, gynecologists, nutritionists, and statisticians included items about demographic characteristics of socioeconomic status and employment status, as well as items about medical history, family medical history, smoking (cigarette, hookah, etc.). The results of the cohort have been used in other studies.11,12 Questionnaires were completed by researchers. The dependent variable was a history of stillbirth that was investigated by the self-report, yes/no item.
Other characteristics of women during the study were also asked through a questionnaire and in the form of self-report.
Information on age, age of marriage, age of pregnancy, age of menstruation and age of menopause, number of previous pregnancies, number of years of education, family marriage (relatives of husband and wife), underlying disease status (diabetes, hypertension, depression) and employment status of the individual and spouse. and, smoking status were collected.
Considering that the question of having a history of stillbirth was asked retrospectively, therefore, the main limitation of this research is that the characteristics of the examined sample are related to the time of the study and may vary with their characteristics at the time of stillbirth.
However, the study of the current characteristics also represents the previous characteristics of people, and the results obtained from the relationship between the current characteristics of people and their history of stillbirth are valuable.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For example, necessary information about the protocol of the study, the confidentiality of their data, and the purpose of the research was offered to the participants and then all the participants signed written consent form to participate in the study before they were enrolled. Besides that, the protocol of the study was approved by the Research Ethics Committee in Shahid Sadoughi University of Medical Sciences, Yazd (ethical code: IR.SSU.SPH.REC.1395.43).
Data Analysis
To conduct data analysis, Statistical Package for the Social Sciences, SPSS22 (Chicago, IL, USA), was used. Descriptive statistics including chi-square, and regression analysis were used. P value < .05 was considered a significant level.
Results
The study involved 4757 women aged 31 years or above, out of which 344 (7.2%) had a history of stillbirth. The details of these women are given in Table 1. The majority of the women (42.4%) were between 35 and 44 years old, with only 15.3% being employed. Eighty-six percent of the women had a family marriage, with 70% getting married before 18 years of age. More than half of the women (51%) had their first pregnancy before 18 years of age, and over 50% had less than 5 years of education. Approximately 20% of the women had diabetes and 26% had high blood pressure. Furthermore, more than 80% of the women had undergone more than 2 pregnancies, with 76.3% of them having 3 or more children (Table 1). ٌ While Table 2 examines the relationship between women’s characteristics and the history of stillbirth. First, the percentage of having an abortion in each of the groups of variables is given in columns 2 and 3 of the table in a cross-sectional manner, and the significance of the difference is measured using the chi-square test (significant results are indicated by the sign *). Then, in columns number 4 and 5, the correlation of each independent variable with the dependent variable in logistic regression has been measured in raw and univariate form (cOR). Finally, in column number 6 of the results of the multivariate test, the meaning variables in the previous step are given under the title of standard coefficients (aO).
Table 1.
Demographic Characteristics of Married Women Aged 35 to 70 With a History of Pregnancy Enrollment Phase of Shahedieh Cohort Study.
| Variables | N (%) | |
|---|---|---|
| Age (years) | 35-44 | 2017 (42.4) |
| 45-54 | 1493 (31.4) | |
| >55 | 1246 (26.2) | |
| Employment | Housewife | 4028 (84.7) |
| Employed | 728 (15.3) | |
| Smoke in home | No | 2896 (60.9) |
| Yes | 1855 (39) | |
| Consanguineous marriage (family marriage) | No | 652 (13.7) |
| Yes | 4085 (85.9) | |
| Age at first marriage | <18 | 3329 (70) |
| 19-25 | 1270 (26.7) | |
| 26-36 | 147 (3.1) | |
| >37 | 14 (0.3) | |
| Age at first pregnancy | <18 | 2416 (50.8) |
| 19-36 | 2326 (48.9) | |
| >37 | 10 (0.2) | |
| Education years | <5 | 2583 (54.3) |
| 6-12 | 1698 (35.7) | |
| >12 | 476 (10) | |
| Menopause age | >40 | 171 (3.6) |
| <41 | 1517 (31.9) | |
| others | 3068 (64.5) | |
| Has diabetes | No | 3781 (79.5) |
| Yes | 975 (20.5) | |
| Has hypertension | No | 3534 (74.3) |
| Yes | 1222 (25.7) | |
| Number of pregnancy | 1-2 | 813 (17.1) |
| 3-5 | 2611 (54.9) | |
| 6-20 | 1332 (28) | |
| Number of live childbirths | ≤2 | 1127 (23.7) |
| 3-5 | 2630 (55.3) | |
| >6 | 999 (21) | |
| N = 4757 |
Table 2.
Variables Related to the Probability of Stillbirth in Women Aged 35 to 70 With a History of Pregnancy Enrollment Phase of Shahedieh Cohort Study.
| Characteristics | Women with stillbirth | cOR (95% CI) | P-value | aOR (95% CI) | ||
|---|---|---|---|---|---|---|
| Column N; 1 | 2 | 3 | 4 | 5 | 6 | |
| No | Yes | |||||
| Total | n = 4413 (% = 92.8) | n = 344 (% = 7.2) | ||||
| Age (years)** | 35-44 | 1936 (96) | 80 (4.0) | 1.00 (reference) | <.001 | 1.00 (reference) |
| 45-54 | 1993 (93.2) | 102 (6.8) | 1.46 (1.05, 2.01) | 1.09 (0.71, 1.31) | ||
| >55 | 1083 (87.0) | 162 (13) | 3.4 (2.53, 4.63) | 1.24 (0.79, 1.94) | ||
| Education (years)** | <6 | 2326 (90) | 258 (10) | 1.00 (reference) | <.001 | 1.00 (reference) |
| 7-12 | 1621 (95.5) | 77 (4.5) | 0.43 (0.33, 0.55) | 0.63 (0.46, 0.86)** | ||
| >12 | 466 (98.1) | 9 (1.9) | 0.17 (0.08, 0.34) | 0.28 (0.13, 0.60)** | ||
| Employment status* | Housewife | 3708 (92.4) | 305 (7.6) | 1.00 (reference) | .012 | 1.00 (reference) |
| Employed | 691 (94.8) | 38 (5.2) | 0.67 (0.47, 0.94) | 1.09 (0.74, 1.63) | ||
| Tobacco smoking | No | 4330 (92.8) | 334 (7.2) | 1.00 (reference) | .132 | |
| Yes | 80 (89.9) | 9 (10.1) | 1.46 (0.72, 2.93) | |||
| Smoking in home | No | 2698 (93.2) | 198 (6.8) | 1.00 (reference) | .145 | |
| Yes | 1712 (92.2) | 145 (7.8) | 1.15 (0.92, 1.44) | |||
| Consanguineous marriage* (family marriage) | No | 618 (94.8) | 34 (5.2) | 0.67 (0.47, 0.97) | .022 | 0.58 (0.39, 0.85)** |
| Yes | 3780 (92.5) | 307 (7.5) | 1.00 (reference) | 1.00 (reference) | ||
| Age at first marriage** | <18 | 3062 (92) | 265 (8) | 1.00 (reference) | <.001 | 1.00 (reference) |
| 19-25 | 1198 (94.3) | 73 (5.7) | 0.71 (0.53, 0.92) | 0.95 (0.67, 1.33)* | ||
| 26-40 | 143 (97.3) | 4 (2.7) | 0.32 (0.11, 0.88) | 0.56 (0.19, 1.59) ** | ||
| >37 | 9 (100) | 0 (0) | - | - | ||
| Age at first pregnancy* | <18 | 2216 (91.7) | 200 (8.3) | 1.00 (reference) | .11 | 1.00 (reference) |
| 19-36 | 2186 (93.9) | 143 (6.1) | 0.73 (0.58, 0.90) | 0.98 (0.73, 1.31) | ||
| >37 | 11 (100) | 0 (0) | - | - | ||
| Number of live childbirths** | ≤2 | 1074 (95.3) | 53 (4.7) | 1.00 (reference) | <.001 | 1.00 (reference) |
| 3-5 | 2472 (94) | 157 (6) | 1.29 (0.93, 1.77) | 1.75 (1.51, 2.10) | ||
| 6-20 | 867 (86.6) | 134 (13.4) | 3.13 (2.25, 4.35) | 2.98 (1.61, 3.5) | ||
| Number of pregnancy** | 1-2 | 809 (99.5) | 4 (0.5) | 1.00 (reference) | <.001 | 1.00 (reference) |
| 3-5 | 2492 (95.4) | 120 (4.6) | 3.8 (2.43, 5.16) | 2.9 (1.51, 4.13)** | ||
| >6 | 1111 (83.5) | 220 (16.5) | 18.7 (5.21, 32.1) | 12.9 (2.23, 25.9)** | ||
| Depression | No | 3430 (92.7) | 272 (7.3) | 1.00 (reference) | .361 | |
| Yes | 983 (93.2) | 72 (6.8) | 0.92 (0.70, 1.20) | |||
| Diabetes** | No | 3572 (94.4) | 212 (5.6) | 1.00 (reference) | <.001 | 1.00 (reference) |
| Yes | 841 (86.4) | 132 (13.6) | 2.64 (2.10, 3.32) | 1.61 (1.24, 2.07)** | ||
| Hypertension** | No | 3356 (94.9) | 179 (5.1) | 1.00 (reference) | <.001 | 1.00 (reference) |
| Yes | 1057 (86.5) | 165 (13.5) | 2.93 (2.34, 3.65) | 1.93 (1.4, 2.56)** | ||
| Chi-square = 598, Sig < .001, Negelkerk R square = .376 | ||||||
P-value < .001. *P-value < .05.
The results of the Chi-square test show a significant difference in the percentage of having a history of stillbirth in the groups of variables, age, education, employment status, marital status, number of pregnancies and number of children born, having blood pressure and diabetes. Older women have a higher percentage of stillbirth, 13% of women over 55 have a stillbirth, and only 4% of women aged 35 to 44 have had a stillbirth. Higher education is associated with a lower percentage of stillbirth history, and only 2% of women with more than12 years had a stillbirth history, while 10% of women with less than 6 years of education had a stillbirth history. Housewives had more history of stillbirth than working women (7.6% vs 5.4%), and married women also had a higher percentage of stillbirth history (7.5%vs 5.2%). Women who married at a younger age and women who had a pregnancy at a younger age had a higher percentage of stillbirth history (8% of girls who married and got pregnant under the age of 18 had a history of stillbirth and, at older ages, the history of stillbirth is reduced). Women with a higher number of pregnancies and children have a higher percentage of stillbirth history (respectively more than 13% and 16.6% of women with more than 6 children and more than 6 pregnancies have a history of stillbirth and, a low percentage of women with less than 2 pregnancies and children had a history of stillbirth). Having diabetes and hypertension was also associated with a higher percentage of stillbirth history for women and in both groups there was about 13.5% stillbirth history compared to 5% stillbirth history for women without the disease. The results of the logistic regression in the crude stage showed a significant effect for the variables of age, education, employment status, family marriage, age of marriage and pregnancy, the number of live births and the number of pregnancies, and having diabetes and blood pressure, so all these variables in The next step is to enter the multivariable model and the standard coefficients show that in this step only the variables; Education, age at first marriage, family marriage, number of pregnancies, and having diabetes and blood pressure could have a significant effect on the probability of having a history of stillbirth for women (Table 2).
Figure 1 displays the percentage of stillbirths of women based on groups of independent variables.
Figure 1.
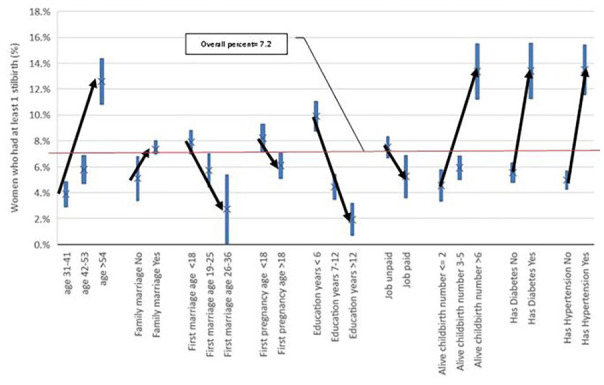
Percentage of women with a history of stillbirth at 95% confidence interval.
Discussion
Despite advances in reducing maternal and neonatal mortality and morbidity since the 1990s, the world is still a long way from achieving the goals set in the Sustainable Development Goals. The main reason for the lack of realizing this goal is not to address unsafe and poor quality care. In a study, 1 it was observed that about 98% of stillbirths occur in low- and middle-income countries, but in Yazd province, which has relatively acceptable economic, health, and cultural indicators compared to other provinces of Iran, 10 the Stillbirth Rate is relatively high compared to the national Stillbirth Rate.13,14 According to data from our participants, they have given birth to 19 377 children during their lifetime. Given 344 cases of stillbirths, the Stillbirth Rate in our study is 17.75 per 1000 births. The global stillbirth rate in 2019 was 13.9. According to the same source, the stillbirth rate in Iran is 6.9. 15 In a study conducted in Iran, the Stillbirth Rate in 2016 was obtained at 7.63 per 1000 births. 14 In another study, which was conducted almost simultaneously throughout the country, the stillbirth frequency was estimated at 4.8% of deliveries (14.8 per 1000 births). 9
One of which is that the results of the present study are terms lifelong and the rate obtained may have been affected by the previous conditions of women, while the design of the global study 15 and national study 14 is cross-sectional and their results are related to recent years and therefore the obtained stillbirth rates are comparably lower. In addition, the present study was a survey and therefore comparably more accurate information has been obtained from participants, while the global and national studies used hospital information and the number of women with a history of stillbirth may be undercounted due to lack of referring to hospital.
Based on the results, it can be argued that the majority of our participants had a low education level and did not have a paid job, and their husbands were mostly retired or were laborers (although the type of participants was reported during the study and stillbirth has already occurred, the current participant’s status is not far from the past welfare and economic status), and our participants do not seem to enjoy a good economic and welfare status in their families, as in other studies. As the role of low economic status and welfare in increasing the Stillbirth Rate has been demonstrated,9,16 the same argument can be proposed for our findings in this regard. An important point about the still birth Rate in Yazd province, including Shahedieh, can be related to the prevalence of diabetes. The high diabetes rate in Yazd province, which is one of the leading provinces in Iran, 17 can also affect the health of pregnant mothers 7 in the province.
In our study, the effect of diabetes and hypertension on stillbirth was significant. Having diabetes and high blood pressure increased the risk of miscarriage by 60% and 82%, respectively, so 13.6% of diabetic women and 13.5% of hypertensive women had experienced miscarriage, respectively. In a similar study, 26% of women with a history of stillbirth were diagnosed with hypertension.7,18 According to the results of the present study, the number of stillbirths increased with the increasing age of women, their age of marriage, and their age of giving birth to the first child. As with the results of another study, there was no significant relationship between smoking and the stillbirth rate. 2 However, the results showed that more than 98% of women did not smoke cigarettes and other tobacco and, the Stillbirth Rate was higher in women who were married or had given birth to their first child under the age of 18. This result is consistent with the results of other studies.7,16,19,20
The results of a doctoral dissertation showed that out of 1500 referred to public hospitals, 21% had stillbirths and especially pregnancies under the age of 18 had a role in increasing the Stillbirth Rate. 13 The results of another dissertation showed that the Stillbirth Rate was higher in pregnancies over 35 years and in women with low education. In the study of Khalili et al in Yazd province, the Stillbirth Rates in 2014, 2015, and 2016 were calculated at 7.31, 7.02, and 7.49, respectively. 9
According to evidence from Iran, the rates of unwanted abortions and stillbirths are higher in consanguineous marriages than in non-consanguineous marriages.19,20 In this study, over 80% of marriages among residents of the city were reported as being consanguineous the relationship between the rate of consanguineous marriages and stillbirth rate was significant. Percentages of stillbirth at a 95% confidence interval were shown in terms of various variables. The highest stillbirth rates were obtained for women over 54 years of age with less than6 years of education, and more than 6 children, with high blood pressure, diabetes and tubectomy. The inverse correlation between literacy level, employment type with fewer advantages, the number of live births, and their stillbirth rate has also been confirmed in other studies.2,9,14 Consistent with other research results, there was no significant relationship between maternal smoking and the stillbirth rate. 2 However, in the present study, more than 98% of participants reported that they did not smoke.
One of the limitations of our study was the use of second-hand (cohort) data and the lack of access to samples to garner additional information.
Conclusions
We can argue that the Stillbirth Rate in Shahedieh city is high compared to the global Stillbirth Rate, but it is comparable to the overall Stillbirth Rate in Yazd province. But since the results in this study were self-reported by women it requires more detailed studies to accurately determine the level of stillbirth in this city. Although Yazd province, as one of the industrial hubs of the country, has an acceptable index of income, and relative welfare level, this study in the small city of Yazd province shows that certain factors such as diabetes, high blood pressure, low education level of women, consanguineous marriage, and social welfare status are among the factors affecting the Stillbirth Rate in Shahedieh.
Acknowledgments
The authors are deeply indebted to all the participants in this study. This work was financially supported by Social Determinants of Health Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Footnotes
Author Contributions: Conceptualization: A.R.A, N.A, M.T.M Data curation: N.Y, T.F., D.P. Methodology: S.S.M.M., A.RA, Supervision: M.T.M, N.A. Writing – review & editing: T.F., D.P., N.Y. The authors read and approved the final manuscript.
Availability of Data and Materials: The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Shahid Sadoughi University of Medical Sciences.
Consent for Publication: Not applicable.
ORCID iD: Nahid Ardian  https://orcid.org/0000-0003-2238-4511
https://orcid.org/0000-0003-2238-4511
References
- 1. Lawn JE, Blencowe H, Waiswa P, et al. Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016;387(10018):587-603. [DOI] [PubMed] [Google Scholar]
- 2. Oğuz Kafadar Ö, Moraloğlu Tekin Ö, Çoşkun B, Güler Özgür İ, Çoşkun B. Investigating demographic, socioeconomic, and obsteric risk factors of term intrauterine stillbirth cases. Med Sci Discov. 2019;6(7):128-132. [Google Scholar]
- 3. World Health Organization. Reaching the Every Newborn National 2020 Milestones: Country Progress, Plans and Moving Forward. World Health Organization; 2017. [Google Scholar]
- 4. Perelberg RJ. Murdered father; dead father: revisiting the Oedipus complex1. Int J Psychoanal. 2009;90(4):713-732. [DOI] [PubMed] [Google Scholar]
- 5. Yasaei Fakhrolmolouk S. Investigating the causes of stillbirth based on clinical findings in Ayatollah Taleghani Hospital in 1991-2001. Sci J Forensic Med. 1996;11(1):32-35. [Google Scholar]
- 6. Alijahan R, Hazrati S, Mirzarahimi M, Pourfarzi F, Hadi P. Prevalence and risk factors associated with preterm birth in Ardabil, Iran. Iran J Reprod Med. 2014;12(1):47. [PMC free article] [PubMed] [Google Scholar]
- 7. Sarani A, Gharibi M, Noori N, Mirparsa F. Evaluation the associated factors with abortion and stillbirth in pregnant women referring to Ali-ebne Abitaleb Hospital in Zahedan, Iran. Beyhagh. 2019;24(4):13-24. [Google Scholar]
- 8. McClure EM, Saleem S, Pasha O, Goldenberg RL. Stillbirth in developing countries: a review of causes, risk factors and prevention strategies. J Matern Fetal Neonatal Med. 2009;22(3):183-190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tavousi M, Motlagh M, Eslami M, et al. Fertility desire and its correlates: a pilot study among married citizens living in Tehran, Iran. Payesh (Health Monitor). 2015;14(5):697-702. [Google Scholar]
- 10. Ardian N, Mazloomy Mahmoudabad SS, Ardian M, Karimi M. General health of foreign-origin groups and native population. Glob J Health Sci. 2014;6(5):55-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Momayyezi M, Fakhravari L, Fallahzadeh H, Mirzaei M. Prediction of hypertension based on the quantity and quality of sleep in adults: results of the first phase of Shahedieh Cohort Study 2015-2016. J Hum Environ Heal Promot. 2021;7(2):90-95. [Google Scholar]
- 12. Kazemipoor M, Owlia F, Esfandyar M, et al. Prevalence of oral mucosal lesions considering fertility status in women of Shahedieh cohort population. Jorjani Biomed J. 2019;7(2):21-30. [Google Scholar]
- 13. Alavinia Seyed Ali PM. Prevalence of Abortion and Stillbirth in Pregnant Women Referring to Bahman, Madar and Afshar Maternity Hospitals in. Shahid Sadoughi University; 1998. [Google Scholar]
- 14. Khalili N, Heidarzadeh M, Habibelahi A, et al. Stillbirth in Iran and associated factors (2014-2016): A population-based study. Med J Islam Repub Iran. 2020;34:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hug L, You D, Blencowe H, et al. Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: a systematic assessment. Lancet. 2021;398(10302):772-785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bhusal M, Gautam N, Lim A, Tongkumchum P. Factors associated with stillbirth among pregnant women in Nepal. J Prev Med Public Health. 2019;52(3):154-160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mirzaei M, Rahmaninan M, Mirzaei M, Nadjarzadeh A, Dehghani Tafti AA. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in central Iran: results from Yazd health study. BMC Public Health. 2020;20(1):166-169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Mali RV, Dalal A, Khursheed R, Gan A. Association of Stillbirths with maternal and fetal risk factors in a tertiary care hospital in South India. Obstet Gynecol Int. 2021;2021:1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Maghsoudlou S, Cnattingius S, Aarabi M, et al. Consanguineous marriage, prepregnancy maternal characteristics and stillbirth risk: a population-based case–control study. Acta Obstet Gynecol Scand. 2015;94(10):1095-1101. [DOI] [PubMed] [Google Scholar]
- 20. Ghahfarokhi M. Relationship between consanguineous marriage and spontaneous abortion and stillbirth. Payesh (Health Monitor). 2018;17(4):455-462. [Google Scholar]