

Abstract
Objectives
To evaluate the therapeutic efficacy and safety of obinutuzumab in remission induction for IgG4-related ophthalmic disease (IgG4-ROD) patients.
Methods
Eight IgG4-ROD patients were retrospectively enrolled. They were intravenously administered 1000 mg obinutuzumab at baseline and examined for changes in physical signs, orbital structure imaging parameters, IgG4-related disease responder index (IgG4-RD RI), serological index, and adverse events during treatment. The number of treatment sessions was based on treatment response.
Results
The mean IgG4-RD RI scores of all patients at baseline (7.75 ± 2.92) and after treatment (2.00 ± 0.76) were highly significantly different (P < 0.001). Six patients achieved complete remission (CR) (75%) and two patients achieved partial remission (25%). The mean serum IgG4 levels at baseline (9.45 ± 6.95 g/L) and after treatment (1.55 ± 1.09 g/L) showed a mean decrease of 83% (P = 0.0079). The serum IgG4 level correlated well with IgG4-RD RI at baseline and that after each treatment (r = 0.852, P < 0.01; r = 0.78, P < 0.001). In patients with CR, the serum IgG4 levels at baseline correlated positively with dose numbers required for CR (r = 0.86, P < 0.05). Five patients (62.5%) experienced infusion-related reactions (IRRs) during the first obinutuzumab infusion, while only one (12.5%) experienced IRRs during all subsequent eight infusions.
Conclusion
Obinutuzumab is a safe and promising therapeutic option for IgG4-ROD. It rapidly reduces ocular inflammation and serum IgG4 levels to avoid excessive corticosteroid usage and reduce potential risk of adverse events.
Subject terms: Outcomes research, Autoimmune diseases, Lacrimal apparatus diseases, Immunosuppression
Introduction
Immunoglobulin-G4-related disease (IgG4-RD) is an immune-mediated, multiorgan chronic inflammatory disease. The typical clinical manifestation of IgG4-RD includes significantly elevated serum IgG4 level and tumefactive lesions, and the primary histopathological manifestation is lymphoplasmacytic infiltration with predominantly IgG4-positive plasma cells, together with storiform fibrosis, obliterative phlebitis, and eosinophil infiltration [1, 2]. Ophthalmic involvement is a common manifestation of IgG4-RD, which accounts for 4–34%, and is referred to as IgG4-related ophthalmic disease (IgG4-ROD) [3].
Almost all ocular adnexa can be involved in IgG4-ROD; lacrimal gland involvement is the most common manifestation, followed by soft tissue of the eyelids, extraocular muscles, trigeminal nerve, and optic nerve involvement being commonly reported, while the involvement of the uvea, sclera, lacrimal system, and orbital bone is less common [4, 5]. Initially, because of the susceptibility of the lacrimal gland to develop inflammation, patients often present with swelling of the eyelids, even with a hard tumefactive lesion. During the active phase of the disease, the optic nerve may be involved, resulting in irreversible vision loss. In the advanced stages, tissue fibrosis occurs, which leads to a distorted appearance and varying degrees of impairment of the ocular adnexa, such as diplopia, strabismus, and xerophthalmia. The inflammation associated with chronic IgG4-ROD may also increase the risk of its progression to lymphoma [4].
Currently, the main treatment options for IgG4-ROD are glucocorticoids, csDMARDS, biologics, radiotherapy, and surgery [6]. Glucocorticoids are considered the cornerstone of IgG4-ROD treatment because of their high treatment response rate, and are recommended as the first-line treatment agent for remission induction and maintenance therapy in all patients with active, untreated IgG4-RD [7]. However, glucocorticoids often need to be used in large quantities over a prolonged period; otherwise, the disease could recur and eventually lead to adverse events [8, 9].
Therapy with Anti-CD20 monoclonal antibodies are considered a good steroid-sparing treatment strategy. Rituximab, a representative drug, has been successfully used for the induction and maintenance treatment of IgG4-RD [10–12]. Obinutuzumab is a newly developed humanized type II monoclonal antibody against the B-lymphocyte-specific antigen CD20. A recent study reported the successful use of obinutuzumab in treating a patient with IgG4-associated membranous nephropathy who was allergic to rituximab, suggesting the potential of obinutuzumab for treating IgG4-RD [13].
The present study aimed to investigate the efficacy of obinutuzumab for the remission induction treatment of IgG4-ROD and to assess changes in the serological index and patient safety during treatment. To our best knowledge, the present study is the first to report the application of obinutuzumab for treating IgG4-ROD.
Patients and methods
Study design
The present investigation was a retrospective study approved by the Review Committee of the Second Hospital of Dalian Medical University (NO. LCKY2023-135). Informed consent was received from all the participants. The study was designed in accordance with the principles of the Declaration of Helsinki for biomedical research.
Patients
This study included patients who were newly diagnosed with IgG4-ROD and were treated with obinutuzumab from December 2021 to March 2023 at the Second Hospital of Dalian Medical University. The following data were collected: demographic data, clinical data, imaging data, pathological data, and treatment data. Diagnostic criteria were based on the guidelines published by the Japanese IgG4-ROD study Group in 2014 [14]. The exclusion criteria were as follows: (1) age <18 years; (2) patients with unconfirmed diagnosis of IgG4-ROD; (3) treatment with corticosteroids, immunosuppressants, monoclonal antibodies, and other drugs before baseline; (4) surgery or radiotherapy before baseline, and (5) no complete and available clinical data.
Evaluation of disease activity
Patients were evaluated for ophthalmic disease activity by using the 2018 IgG4-RD Responder Index (IgG4-RD RI). This index is a tool to evaluate disease activity and organ damage, based on the model of Birmingham Vasculitis Activity Score for Wegener’s granulomatosis (BVAS/WG), specifically designed for IgG4-RD [15]. This tool allows the investigator to score disease activity and organ damage in 24 standard organs/sites and also include other sites involved in the disease, thus resulting in a cumulative index for the patient, with scores as follows:
0 = Unaffected or resolved
1 = Improved but persistent
2 = New or recurrence (while off of treatment) or unchanged
3 = Worse or new (despite treatment)
A score of 2 is assigned to a patient if the disease activity is newly diagnosed without treatment. A score of 1 is given when the disease improves after treatment and continues to receive 1 if the disease persists but remains improved at subsequent visits as compared to the pretreatment baseline. Correspondingly, a score of 2 remains if there is no change in disease activity, while a score of 3 is assigned for exacerbations. Moreover, in some patients, IgG4-RD may require urgent treatment to prevent severe or irreversible organ dysfunction; in such situations, the organ or site score is weighted higher by doubling.
In this study, the disease activity was evaluated based on the lacrimal gland, eyelid, extraocular muscles, trigeminal nerve, and optic nerve. The score for the optic nerve was doubled when it was affected by disease activity. Additionally, the above assessment was based on the overall condition of the bilateral eyes; the score was not considered 0 even if the same adnexa showed no disease activity in one eye after treatment but exhibited disease activity in the other eye. Patients were assessed for ocular disease activity before treatment and 1 month after each treatment on the basis of physical examination and imaging, as shown in Fig. 1.
Fig. 1. Evaluation of ocular disease activity based on physical examination and imaging.

A Changes in appearance of case 4 during treatment course. B Changes in the size of lacrimal gland based on coronal scan before and after treatment in case 5. C Changes in the largest short diameter of the extraocular muscle involved in inflammation and in the size of lesions for infraorbital nerve and maxillary sinus in case 1.
Treatment response
Treatment response was assessed 1 month after each treatment according to the changes in the IgG4-RD RI score of the patient. The response was classified as complete response (CR), partial response (PR), and no change (NC). The definition of treatment response was based on a prospective study of IgG4-RD in China [16] as follows:
CR: IgG4-RD RI <3 after a decline of ≥2.
PR: IgG4-RD RI ≥3 after a decline of ≥ 2.
NC: Lack of a significant change in the lesion size or clinical manifestations after treatment and a decline of <2 in IgG4-RD RI.
Obinutuzumab treatment protocol
At baseline, the patients were intravenously administered a 1000 mg infusion of obinutuzumab. Prior to infusion, 20 mg dexamethasone and 50 mg diphenhydramine were administered to mitigate subsequent infusion-related reactions (IRRs). All patients were reviewed 1 month after receiving the treatment, and the number of treatment sessions was determined based on the treatment response, with a 1-month interval between the doses. The indications for treatment discontinuation were as follows: (1) achievement of CR and (2) no improvement or treatment response as NC within 1 month after treatment.
Statistical analysis
SPSS 27.0 statistical software (IBM) was used, and the results were presented as mean ± standard deviation. GraphPad Prism 9.0 software was used for plotting the graphs. The Shapiro–Wilk test was performed to confirm the normality of the data. The paired design data were processed using paired samples t-test and Wilcoxon rank-sum test. Correlation analysis between the variables was performed using Spearman’s and Pearson’s correlation analyses. Differences were considered statistically significant at P < 0.05.
Results
Of the eight study patients, five were males and three were females, with a mean age of 52.00 ± 11.30 years; two patients underwent three treatment sessions, four patients underwent two treatment sessions, and two patients underwent one treatment session. Table 1 shows the detailed clinical data and treatment results for the eight patients.
Table 1.
Clinical dates and treatment outcome of 8 cases.
| Case | Sex/Age (years) | Symptom (PE) | Orbital structures involved (imaging) | Symptom duration (months) | IgG4 + /HPF | IgG4/IgG (%) | Treatment times |
Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | M/60 |
Bilateral UL and LG swelling Proptosis and Hypopsia (R) |
Bilateral LG, R side: ON, IR, LR L side: IN |
24 | 127 | 81 | 3 | CR |
| 2 | F/65 | Bilateral UL and LG swelling |
Bilateral LG L side: IN |
12 | 73 | 60 | 2 | CR |
| 3 | F/41 | Bilateral UL and LG swelling |
Bilateral LG and IN L side: LR |
8 | 24 | 45 | 2 | CR |
| 4 | M/31 | Bilateral UL and LG swelling | Bilateral LG and IN | 6 | 51 | 33 | 3 | CR |
| 5 | F/60 | Bilateral UL and LG swelling | Bilateral LG | 3 | 15 | 40 | 1 | CR |
| 6 | M/49 |
Bilateral UL and LG swelling limitation of movement (R) |
Bilateral LG R side: IR, IN |
9 | 68 | 57 | 2 | CR |
| 7 | M/53 |
Bilateral UL LG swelling (L) |
Bilateral LG L side: IN |
5 | 59 | 48 | 1 | PR |
| 8 | M/57 |
Bilateral UL, LG swelling Bilateral proptosis Hypopsia and abnormal PEP (L) |
Bilateral LG and LR L side: ON, IN, IR |
18 | 153 | 76 | 2 | PR |
PE physical examination, HPF high-power field, LG lacrimal gland, UL upper lid, IN infraorbital nerve, ON optic never, IR inferior rectus, LR lateral rectus, PEP primary eye position, CR complete remission, PR partial remission.
Treatment response
The treatment response rate was 100% for all eight patients. One patient achieved CR (12.5%) and seven patients achieved PR (87.5%) after the first treatment session. Four of the six patients (67%) who received the second treatment session achieved CR. The two patients (33%) who achieved PR after the second treatment had CR after the third treatment session. Overall, six patients eventually achieved CR (75%) and two patients achieved PR (25%) after completing the treatment course; the latter group maintained their RI scores at the follow-up.
Changes of IgG4-RD RI scores
The mean IgG4-RD RI scores of the eight patients at baseline and after the overall treatment course were 7.75 ± 2.92 and 2.00 ± 0.76, respectively. A mean decrease of 71% was observed and the difference was highly significant (P < 0.001). The IgG4-RD RI in the eight patients after the first treatment was 3.63 ± 1.06 and showed a high significant difference when compared with that at baseline (P < 0.001). In the six patients who received the second treatment session, the pre- and post-treatment IgG4-RD RI scores were 4.00 ± 0.89 and 2.17 ± 0.75, respectively (P < 0.01). In the two patients who received the third treatment session, the pre- and post-treatment IgG4-RD RI scores were 2.50 ± 0.71 and 1.50 ± 0.71, respectively (P > 0.05, Table 2, Fig. 2A).
Table 2.
Comparison of clinical parameters at baseline and after induction therapy.
| Parameter | Baseline | After induction therapy | P value |
|---|---|---|---|
| IgG (g/L) | 16.65 ± 5.43 | 7.76 ± 2.85 | 0.00055a |
| IgG4 (g/L) | 9.45 ± 6.95 | 1.55 ± 1.09 | 0.0079a |
| IgE (IU/ml) | 568.86 ± 446.51 | 209.06 ± 184.20 | 0.012a |
| Eosinophil (109/L) | 0.2675 ± 0.22 | 0.35 ± 0.16 | 0.324 |
| Neutrophil (109/L) | 4.10 ± 1.88 | 1.56 ± 0.55 | 0.0056a |
| PLT (109/L) | 235.63 ± 47.22 | 215.13 ± 53.24 | 0.173 |
| CRP (ug/ml) | 3.90 ± 2.96 | 3.17 ± 1.49 | 0.251 |
| ESR (mm/h) | 7.75 ± 6.50 | 6.73 ± 4.30 | 0.354 |
| RI | 7.75 ± 2.92 | 2.00 ± 0.76 | 0.00068a |
| LG (mm) | 6.78 ± 1.85 | 2.65 ± 0.91 | <0.0001a |
| EOM (mm) | 6.46 ± 1.79 | 3.66 ± 1.00 | 0.007a |
PLT platelets, CRP C-reactive protein, ESR erythrocyte sedimentation rate, RI responder index, LG lacrimal gland, EOM extraocularmuscles.
aStatistical significance (P < 0.05).
Fig. 2. Changes in two key parameters reflecting the effectiveness of the therapy.

A Changes of IgG4-RD RI in 8 patients during treatment course. B Changes of serum IgG4 level in 8 patients during treatment course.
Evaluation of lesions based on imaging
All lesions were observed by MRI. Based on the coronal scan, the mean largest short diameter of the lacrimal gland involved in inflammation was 6.78 ± 1.85 mm before treatment and 2.65 ± 0.91 mm after treatment, and a high significant difference in the diameters was observed (P < 0.0001). The mean largest short diameter of the extraocular muscle involved in inflammation was 6.46 ± 1.79 mm before treatment and 3.66 ± 1.00 mm after treatment, and a significant difference was noted (P < 0.01) (Table 2). The lesion disappeared in five of the seven patients with infraorbital nerve involvement, while the lesion size was reduced in two patients. In patient 1 and patient 8, the optic nerve compression due to the enlarged extraocular muscle was relieved after treatment.
Physical signs
Physical examination after treatment showed significant improvement in the swelling of the eyelids and lacrimal glands in all patients. The upward rotation of the right eye in patient 6 was mildly restricted, which was restored and aligned with that of the left eye after treatment. The proptosis of the eyes in patient 1 and patient 8 was as follows: 18 mm (R) and 14 mm (L); 16 mm (R) and 17 mm (L), respectively, before treatment and 14 mm (R) and 14 mm (L); 13 mm (R) and 15 mm (L), respectively, after treatment. The slight hypotropia of the left eye (5Δ) in patient 8 disappeared. The visual acuity of patient 1 and 8 improved from 0.3 to 1.0 and from 0.6 to 0.9, respectively. The visual field examination of patient 1 is shown in supplementary information. Furthermore, almost all patients reported improvement in subjective symptoms.
Changes in laboratory parameters
The mean serum IgG4, IgG, and IgE levels at baseline for the eight patients were 9.45 ± 6.95 g/L, 16.65 ± 5.43 g/L, and 568.86 ± 446.51 IU/mL, respectively. Following the completion of the treatment course, the serum IgG4, IgG, and IgE levels were 1.55 ± 1.09 g/L, 7.76 ± 2.86 g/L, and 209.06 ± 184.20 IU/mL, respectively. The mean percentage decrease as compared to the baseline values was 83%, 52%, and 64%, respectively (P = 0.0079, 0.00055, and 0.012, respectively). The mean values of neutrophil count, platelet (PLT) count, eosinophil count, C-reactive protein (CRP) level, and erythrocyte sedimentation rate (ESR) at baseline were 4.10 ± 1.88 ×109/L, 235.63 ± 47.22 × 109/L, 0.27 ± 0.22 × 109/L, 3.90 ± 2.96 µg/mL, and 7.75 ± 6.50 mm/h, respectively. The mean neutrophil count was significantly decreased (P < 0.01) to 1.56 ± 0.55 × 109/L after treatment completion, while the changes in the mean values of eosinophil count, CRP level, ESR, and PLT count after treatment completion were not statistically significant (all P > 0.05, Table 2, Fig. 2B).
Correlation analysis for the serum IgG4 level
At baseline, the serum IgG4 level showed a good correlation with IgG4-RD RI (r = 0.852, P < 0.01, Fig. 3A). After treatment, both IgG4-RD RI and serum IgG4 level showed a decreasing trend with a positive correlation between them (r = 0.78, P < 0.001, Fig. 3B). In the six patients who achieved CR, the serum IgG4 levels at baseline were positively correlated with the number of treatment sessions required to achieve CR (r = 0.86, P < 0.05, Fig. 3A).
Fig. 3. Correlation between serum IgG4 level and ocular disease activity.
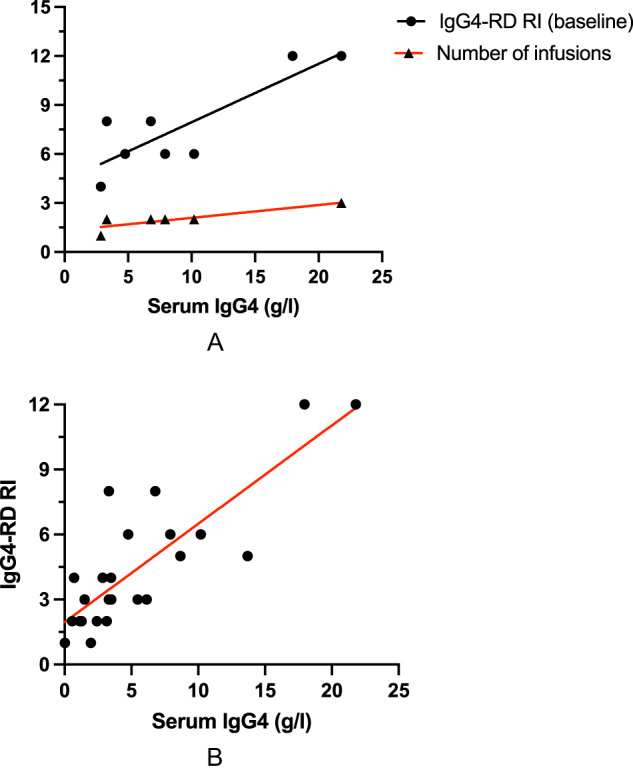
A The linear correlation showing a higher baseline serum IgG4 level leading to a higher baseline RI and a higher number of doses to achieve CR. B The linear correlation between serum IGg4 and IgG4-RD RI after each treatment.
Adverse events
Five patients (62.5%) experienced IRRs during the first treatment session with obinutuzumab. The IRRs were mainly nausea, dizziness, headache, and chest discomfort, which disappeared after the infusion was completed. In the six patients who received at least two infusions of obinutuzumab, IRR occurred in only one patient (12.5%) during all subsequent eight infusions. None of the patients experienced malignant adverse events such as bleeding or infection during or after the treatment course.
Discussion
In the present study, obinutuzumab showed a promising efficacy in patients with IgG4-ROD and significantly reduced ocular inflammation in all eight patients. Six patients (75%) achieved CR and two patients (25%) achieved PR after receiving different numbers of treatment sessions. The serum IgG4 levels decreased rapidly after treatment. Obinutuzumab also showed a high safety with no adverse events during the treatment course, except for a high incidence of IRRs at the first treatment session, which relieved after the completion of infusion.
B-cell depletion therapy with anti-CD20 monoclonal antibodies is considered an effective strategy to conserve corticosteroid use. The first prospective, open-label clinical study of rituximab for IgG4-RD in 2015 included 30 patients in active states who were treated with rituximab (1000 mg, 2 doses, two weeks apart); a total of 97% patients showed treatment response; 77% patients reached the primary study endpoint, and their RI decreased from 11 ± 7 to 1 ± 2; 60% patients achieved CR at 6 months; and 67% patients eventually achieved CR [11]. Furthermore, a case series of five steroid-resistant patients reported the use of 1000 mg intravenous infusion of rituximab twice (two weeks apart) and four doses of 375 mg/m2 (one week apart) as remission induction therapy; CR was achieved in three patients and PR in two patients after 2 months, with no relapse at an average follow-up of 33 months [12]. In the present study, all patients showed good treatment response with a mean decrease of 71% in the IgG4-RD RI score. Improvements were observed in all inflammatory ocular adnexa after treatment. The results are consistent with previous findings that CD20 monoclonal antibodies are effective in improving the clinical manifestations of IgG-RD. Our study further suggests that this effect may be more pronounced in IgG4-ROD.
A noteworthy finding is that the optic nerve in patient 1 was compressed by the enlarged lateral rectus muscle at baseline, leading to compressive optic neuropathy (CON) with acute visual loss and visual field defects. The patient reported a significant improvement in vision after treatment, as evidenced by a follow-up visual field examination; moreover, the patient’s IgG4-RD RI decreased from 12 to 2 after the completion of three treatment sessions. Glucocorticoids and emergency orbital decompression surgery are generally considered to be the mainstay of CON treatment [17, 18]; however, the tendency to recur after discontinuation of glucocorticoids limits their use in patients with severe CON. Shang et al. reported a case of an IgG4-RD patient with CON and no light perception in the involved eye due to extraocular muscle inflammation; the patient’s condition improved after receiving a high dose of methylprednisolone (1 g daily) for 72 h but again deteriorated 4 days after discontinuing the drug. Following treatment with four doses of 1 g rituximab, the condition improved, and remission was maintained for up to 9 months [19]. Therefore, in patients with optic nerve involvement, obinutuzumab treatment is a promising approach to reduce the risk of optic nerve injury and avoid orbital decompression.
Serum IgG4 has a high sensitivity and specificity in the diagnosis of IgG-RD, and a significantly elevated serum IgG4 level (>5 g/L) is considered to show 90% specificity for the disease [20]. Furthermore, numerous convincing evidence demonstrated that patients with higher levels of serum IgG4 and IgG4+ plasma cell infiltration indicated multiorgan involvement and had higher disease activity and recurrence rate [8, 21]. The quantity and proportion of IgG4+ plasma cells in local tissues correlate positively with serum IgG4 levels, reflecting the inflammatory activity of local lesions [22]. In our study, the patients showed a positive correlation between the baseline IgG4-RD RI and serum IgG4 levels prior to treatment; those patients with a higher baseline serum IgG4 level required more doses to achieve CR, thus suggesting a consistent relationship between ocular disease activity and the serum IgG4 level as noted in previous studies. The pathogenic role of IgG4 in the pathogenesis of this disease is also unclear. IgG4 may be directly involved in the disease process as a tissue-destructive immunoglobulin, or it may simply be overexpressed in response to an unknown antigen or inflammatory stimulus [2, 23]. Based on the above findings, we cautiously suggest that a reduction in serum IgG4 to low or normal levels is a necessary therapeutic goal. Khosroshah et al. reported the efficacy of two doses of 1000 mg rituximab two weeks apart in four patients; the serum IgG4 level showed a mean decrease of 65% within 2 months, and a significant improvement in clinical manifestation was noted [10]. Similarly, obinutuzumab has shown potent effect on reducing serum IgG4 levels, with a mean decrease of 83%, and a good linear correlation between serum IgG4 levels reduction and IgG4-RD RI reduction was also observed after treatment.
Elevated serum IgE levels were observed at baseline, which decreased after treatment. Actually, it has been suggested that an elevated serum IgE level may be an immunologic epiphenomenon, possibly associated with pathologically expanded IL-4-secreting follicular helper T cells that drives B lymphocyte class-switch recombination (IgG-IgE), and it is not critical for the pathogenesis due to the low level of eosinophil infiltration in tissues and lower concentration of serum IgE than that of serum IgG4 [24, 25].
Obinutuzumab exerts its efficacy through three pathways, antibody-dependent cell-mediated cytotoxicity (ADCC), complement-dependent cytotoxicity (CDC), and induction effect of direct cell death (DCD) to achieve B-cell depletion [26, 27]. Specifically, its mechanism may be based on two main aspects: (1) the depletion of all components of the B lymphocyte lineage, from the pre-B lymphocyte stage to the mature B lymphocyte stage, prevents their differentiation into plasma cells to produce IgG4 [28] and (2) B-lymphocytes can bind to specific autoantigens and present these antigens to T lymphocytes, thus maintaining the levels of effector/memory CD4+ T cells, which release inflammatory factors that induce inflammation and tissue fibrosis; this entire process is inhibited by the depletion of B lymphocytes [29].
Unlike rituximab, which is a human-mouse chimeric type I anti-CD20 monoclonal antibody, the glycosylation of the Fc segment of obinutuzumab enhances its affinity for immune effector cells, leading to a better effect of ADCC and DCD [30, 31]. In vitro studies have shown that obinutuzumab-induced ADCC is 35- to 100-fold more potent than rituximab [26]. Another study reported successful clinical and immune remission with obinutuzumab in three patients with membranous nephropathy who had failed induction therapy with rituximab [32]. Therefore, obinutuzumab may be more effective than rituximab in B-cell depletion therapy. Furthermore, in contrast to the currently recommended treatment of intravenous infusion of 375 mg/m2 of rituximab per week for four doses or an intravenous infusion of 1000 mg of rituximab for two doses at 2 weeks apart [33], the number of treatment sessions for patients in our study was dependent on the treatment response, and the remission induction treatment ended when the IgG4-RD RI score reached the criteria for CR. As for cost-effectiveness, two treatment sessions of obinutuzumab cost nearly 1/2 lower than that of rituximab according to the Chinese market price, which is more acceptable for patients. After taking the above advantages of obinutuzumab into account, we decided to choose obinutuzumab for personalized treatment rather than rituximab.
IRR is the most common adverse event during obinutuzumab infusion due to the cytokine release syndrome [34]. It is usually mild to moderate and can be effectively mitigated by premedication, slowing down the infusion rate, and suspension of infusion. In the present study, five patients experienced IRRs during the first treatment session and the incidence of IRR was significantly lower in subsequent treatments; hence, additional monitoring for IRR is required particularly at the first treatment session. Thrombocytopenia is also a common adverse effect; however, it usually occurs as a self-limiting subclinical coagulopathy, which usually resolves within a week, probably due to platelet depletion through the activation of the coagulation system by DNA molecules in the blood because of massive B-cell lysis [35]. A noteworthy finding of this study is that all eight patients showed a regular decrease in neutrophils. Late-onset neutropenia caused by obinutuzumab has been previously observed in the treatment of patients with lymphoma; however, the mechanism of its occurrence remains largely unclear and may be related to an immune response that causes dysfunction of the bone marrow hematopoietic system. The use of granulocyte colony-stimulating factor with prophylactic antimicrobial agents is necessary when there is a low level of neutrophils [36].
The present study has some limitations. First, the two patients who achieved PR declined follow-up treatment because of treatment cost; consequently, their IgG4-RD RI scores were not reduced below 3 and remained unchanged during the follow-up, which might affect our investigation results. Second, given the susceptibility of the lacrimal gland to inflammation and the certain subjectivity of physical examination for eyelids, a score of 1 was assigned to them with caution when assessing the IgG4-RD RI, which could lead to a higher score of IgG4-RD RI after treatment.
In conclusion, obinutuzumab is a safe and promising therapeutic option to relieve the manifestations of IgG4-ROD, as it can rapidly reduce ocular inflammation and serum IgG4 levels. As a remission induction agent, obinutuzumab can avoid the excessive use of corticosteroids and reduce the potential risk of adverse events. Therefore, our study further supports the benefits of using anti-CD20 antibodies for treating IgG4-RD, and obinutuzumab has the potential to play a more important role in future treatments.
Summary
What was known before
Therapy with Anti-CD20 monoclonal antibodies are considered a good steroid-sparing treatment strategy.
Rituximab has been successfully used for the induction and maintenance treatment of IgG4-ROD.
What this study adds
Obinutuzumab, as a newly developed Anti-CD20 monoclonal antibody, can be a safe and promising option for remission induction treatment of IgG4-ROD.
Obinutuzumab can rapidly reduce ocular inflammation and serum IgG4 levels to avoid the excessive use of corticosteroids and reduce the potential risk of adverse events.
Supplementary information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Author contributions
All authors contributed in data collection and participated in the writing of the manuscript.
Data availability
Data that support the findings of this study are available from the corresponding author on reasonable request.
Competing interests
The authors declare no competing interests.
Informed consent
Patient consent has been received for the publication of Fig. 1.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
The online version contains supplementary material available at 10.1038/s41433-023-02758-8.
References
- 1.Saitakis G, Chwalisz BK. The neurology of IGG4-related disease. J Neurol Sci. 2021;424:117420. doi: 10.1016/j.jns.2021.117420. [DOI] [PubMed] [Google Scholar]
- 2.Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366:539–51. doi: 10.1056/NEJMra1104650. [DOI] [PubMed] [Google Scholar]
- 3.Derzko-Dzulynsky L. IgG4-related disease in the eye and ocular adnexa. Curr Opin Ophthalmol. 2017;28:617–22. doi: 10.1097/icu.0000000000000427. [DOI] [PubMed] [Google Scholar]
- 4.McNab AA, McKelvie P. IgG4-related ophthalmic disease. Part II: clinical aspects. Ophthalmic Plast Reconstr Surg. 2015;31:167–78. doi: 10.1097/iop.0000000000000364. [DOI] [PubMed] [Google Scholar]
- 5.Wallace ZS, Deshpande V, Stone JH. Ophthalmic manifestations of IgG4-related disease: single-center experience and literature review. Semin Arthritis Rheum. 2014;43:806–17. doi: 10.1016/j.semarthrit.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 6.Detiger SE, Karim AF, Verdijk RM, van Hagen PM, van Laar JAM, Paridaens D. The treatment outcomes in IgG4-related orbital disease: a systematic review of the literature. Acta Ophthalmol. 2019;97:451–9. doi: 10.1111/aos.14048. [DOI] [PubMed] [Google Scholar]
- 7.Khosroshahi A, Wallace ZS, Crowe JL, Akamizu T, Azumi A, Carruthers MN, et al. International Consensus Guidance Statement on the management and treatment of IgG4-related disease. Arthritis Rheumatol. 2015;67:1688–99. doi: 10.1002/art.39132. [DOI] [PubMed] [Google Scholar]
- 8.Hong JW, Kang S, Song MK, Ahn CJ, Sa HS. Clinicoserological factors associated with response to steroid treatment and recurrence in patients with IgG4-related ophthalmic disease. Br J Ophthalmol. 2018;102:1591–5. doi: 10.1136/bjophthalmol-2017-311519. [DOI] [PubMed] [Google Scholar]
- 9.Akiyama M, Takeuchi T. IgG4-related disease: beyond glucocorticoids. Drugs Aging. 2018;35:275–87. doi: 10.1007/s40266-018-0534-6. [DOI] [PubMed] [Google Scholar]
- 10.Khosroshahi A, Bloch DB, Deshpande V, Stone JH. Rituximab therapy leads to rapid decline of serum IgG4 levels and prompt clinical improvement in IgG4-related systemic disease. Arthritis Rheum. 2010;62:1755–62. doi: 10.1002/art.27435. [DOI] [PubMed] [Google Scholar]
- 11.Carruthers MN, Topazian MD, Khosroshahi A, Witzig TE, Wallace ZS, Hart PA, et al. Rituximab for IgG4-related disease: a prospective, open-label trial. Ann Rheum Dis. 2015;74:1171–7. doi: 10.1136/annrheumdis-2014-206605. [DOI] [PubMed] [Google Scholar]
- 12.Wu A, Andrew NH, Tsirbas A, Tan P, Gajdatsy A, Selva D. Rituximab for the treatment of IgG4-related orbital disease: experience from five cases. Eye (Lond) 2015;29:122–8. doi: 10.1038/eye.2014.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ginthör NE, Artinger K, Pollheimer MJ, Stradner MH, Eller K. Membranous nephropathy associated with immunoglobulin G4-related disease successfully treated with obinutuzumab. Clin Kidney J. 2022;15:564–6. doi: 10.1093/ckj/sfab250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goto H, Takahira M, Azumi A. Diagnostic criteria for IgG4-related ophthalmic disease. Jpn J Ophthalmol. 2015;59:1–7. doi: 10.1007/s10384-014-0352-2. [DOI] [PubMed] [Google Scholar]
- 15.Wallace ZS, Khosroshahi A, Carruthers MD, Perugino CA, Choi H, Campochiaro C, et al. An International Multispecialty Validation Study of the IgG4-Related Disease Responder Index. Arthritis Care Res. 2018;70:1671–8. doi: 10.1002/acr.23543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zongfei J, Lijuan Z, Ying S, Dongmei L, Sifan W, Xiufang K, et al. Improved clinical outcomes of tocilizumab versus cyclophosphamide for IgG4-related disease: insights from a prospective IgG4-related disease registry. Ther Adv Chronic Dis. 2021;12:20406223211028776. doi: 10.1177/20406223211028776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Takahashi Y, Kitamura A, Kakizaki H. Bilateral optic nerve involvement in immunoglobulin G4-related ophthalmic disease. J Neuroophthalmol. 2014;34:16–9. doi: 10.1097/WNO.0b013e3182a304f4. [DOI] [PubMed] [Google Scholar]
- 18.Zhang W, Luo J, Jiao J. Optic nerve involvement in immunoglobulin G4-related disease: a case report. Exp Ther Med. 2016;12:111–4. doi: 10.3892/etm.2016.3291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen TS, Figueira E, Lau OC, McKelvie PA, Smee RI, Dawes LC, et al. Successful “medical” orbital decompression with adjunctive rituximab for severe visual loss in IgG4-related orbital inflammatory disease with orbital myositis. Ophthalmic Plast Reconstr Surg. 2014;30:e122–5. doi: 10.1097/IOP.0b013e3182a64fa4. [DOI] [PubMed] [Google Scholar]
- 20.Nagpal SJS, Chari ST. Immunoglobulin G4 Levels. JAMA. 2019;321:202–3. doi: 10.1001/jama.2018.16665. [DOI] [PubMed] [Google Scholar]
- 21.Zhao Z, Mou D, Wang Z, Zeng Q, Wang Z, Xue J, et al. Clinical features and relapse risks of IgG4-related ophthalmic disease: a single-center experience in China. Arthritis Res Ther. 2021;23:98. doi: 10.1186/s13075-021-02489-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yuan Y, Meng F, Ren H, Yue H, Xue K, Zhang R. Pathological count of IgG4-positive plasmacytes suggests extraophthalmic involvement and relapse in patients with IgG4-related ophthalmic disease: a retrospective study. Arthritis Res Ther. 2022;24:80. doi: 10.1186/s13075-022-02757-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tsang KFP, Oppong WK, Leeds SJ, Bekkali LHN, Nayar KM. Does IgG4 level at the time of diagnosis correlate with disease outcome in IgG4-Related disease? Pancreatology. 2019;19:177–81. doi: 10.1016/j.pan.2018.10.013. [DOI] [PubMed] [Google Scholar]
- 24.Perugino CA, AlSalem SB, Mattoo H, Della-Torre E, Mahajan V, Ganesh G, et al. Identification of galectin-3 as an autoantigen in patients with IgG(4)-related disease. J Allergy Clin Immunol. 2019;143:736–45.e6. doi: 10.1016/j.jaci.2018.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yoon HK, Shim YS, Kim PH, Park SR. The TLR7 agonist imiquimod selectively inhibits IL-4-induced IgE production by suppressing IgG1/IgE class switching and germline ε transcription through the induction of BCL6 expression in B cells. Cell Immunol. 2019;338:1–8. doi: 10.1016/j.cellimm.2019.02.006. [DOI] [PubMed] [Google Scholar]
- 26.Goede V, Klein C, Stilgenbauer S. Obinutuzumab (GA101) for the treatment of chronic lymphocytic leukemia and other B-cell non-hodgkin’s lymphomas: a glycoengineered type II CD20 antibody. Oncol Res Treat. 2015;38:185–92. doi: 10.1159/000381524. [DOI] [PubMed] [Google Scholar]
- 27.van Meerten T, Hagenbeek A. CD20-targeted therapy: the next generation of antibodies. Semin Hematol. 2010;47:199–210. doi: 10.1053/j.seminhematol.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 28.Anolik JH, Barnard J, Cappione A, Pugh-Bernard AE, Felgar RE, Looney RJ, et al. Rituximab improves peripheral B cell abnormalities in human systemic lupus erythematosus. Arthritis Rheum. 2004;50:3580–90. doi: 10.1002/art.20592. [DOI] [PubMed] [Google Scholar]
- 29.Mattoo H, Stone JH, Pillai S. Clonally expanded cytotoxic CD4(+) T cells and the pathogenesis of IgG4-related disease. Autoimmunity. 2017;50:19–24. doi: 10.1080/08916934.2017.1280029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mössner E, Brünker P, Moser S, Püntener U, Schmidt C, Herter S, et al. Increasing the efficacy of CD20 antibody therapy through the engineering of a new type II anti-CD20 antibody with enhanced direct and immune effector cell-mediated B-cell cytotoxicity. Blood. 2010;115:4393–402. doi: 10.1182/blood-2009-06-225979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Reddy V, Klein C, Isenberg DA, Glennie MJ, Cambridge G, Cragg MS, et al. Obinutuzumab induces superior B-cell cytotoxicity to rituximab in rheumatoid arthritis and systemic lupus erythematosus patient samples. Rheumatology. 2017;56:1227–37. doi: 10.1093/rheumatology/kex067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Klomjit N, Fervenza FC, Zand L. Successful treatment of patients with refractory PLA(2)R-associated membranous nephropathy with obinutuzumab: a report of 3 cases. Am J Kidney Dis. 2020;76:883–8. doi: 10.1053/j.ajkd.2020.02.444. [DOI] [PubMed] [Google Scholar]
- 33.Hart PA, Topazian MD, Witzig TE, Clain JE, Gleeson FC, Klebig RR, et al. Treatment of relapsing autoimmune pancreatitis with immunomodulators and rituximab: the Mayo Clinic experience. Gut. 2013;62:1607–15. doi: 10.1136/gutjnl-2012-302886. [DOI] [PubMed] [Google Scholar]
- 34.Dawson K, Moran M, Guindon K, Wan H. Managing infusion-related reactions for patients with chronic lymphocytic leukemia receiving obinutuzumab. Clin J Oncol Nurs. 2016;20:E41–8. doi: 10.1188/16.Cjon.E41-e48. [DOI] [PubMed] [Google Scholar]
- 35.Fresa A, Autore F, Innocenti I, Piciocchi A, Tomasso A, Morelli F, et al. Non-overt disseminated intravascular coagulopathy associated with the first obinutuzumab administration in patients with chronic lymphocytic leukemia. Hematol Oncol. 2021;39:423–7. doi: 10.1002/hon.2837. [DOI] [PubMed] [Google Scholar]
- 36.Shimony S, Bar-Sever E, Berger T, Itchaki G, Gurion R, Yeshurun M, et al. Late onset neutropenia after rituximab and obinutuzumab treatment - characteristics of a class-effect toxicity. Leuk Lymphoma. 2021;62:2921–7. doi: 10.1080/10428194.2021.1948037. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data that support the findings of this study are available from the corresponding author on reasonable request.