

Abstract
Background:
While cross-sectional studies have suggested that HIV-related stigma and depression symptoms may result in poor HIV treatment and health outcomes, few studies have investigated potential longitudinal mechanisms in these relationships. Furthermore, longitudinal effects of HIV-related stigma on health outcomes have not been examined in people with HIV (PWH) newly initiating HIV clinical care. We examined longitudinal associations between experienced and perceived community stigma and health outcomes (ART adherence and viral load), mediated by internalized stigma and depression symptoms among new-to-care PWH in the United States.
Setting/Methods:
Data were obtained from 371 PWH who initiated HIV medical care at four HIV sites at baseline and 48 weeks later between December 2013 and 2018. Validated measures were used to assess experienced stigma, perceived community stigma, internalized stigma, depression symptoms, and ART adherence; and viral load was obtained from medical records at final study visit.
Results:
Serial mediation models revealed significant indirect effects of experienced stigma and perceived community stigma on ART adherence and on viral suppression, first through internalized stigma, and then through depression symptoms.
Conclusions:
These results suggest that PWH may tend to internalize HIV-related stigma when they experience acts of stigmatization or perceive negative attitudes in society, which in turn may result in negative effects on psychological and physical well-being. These findings about how stigma in society may be an antecedent mechanism for PWH to develop internalized stigma, which in turn affects individual health outcomes, can be used to tailor both individual-level and community-level interventions.
Keywords: Experienced stigma, Perceived community stigma, Internalized stigma, Depression symptoms, ART adherence, Viral Suppression
Introduction
Linkage to HIV care, adherence to antiretroviral therapy (ART), and adherence to HIV care visits is crucial for people with HIV (PWH) to achieve and maintain viral suppression and optimal health outcomes.1–3 In the United States, 59–66% of PWH newly diagnosed are engaged in HIV care1,2 and only 55–65% are virally suppressed.4,5 In recent years, the rates of PWH who initially engage in HIV care following HIV diagnosis has increased (80–88%),6,7 yet retention in HIV care and ART adherence among PWH is still an important challenge. Thus, it is important to elucidate factors associated with lower treatment adherence or non-suppressed viral load to develop targeted interventions, particularly when treatment adherence issues are salient for PWH who have newly initiated HIV care.
One major barrier to achieving optimal HIV health outcomes is stigma. In the context of HIV, stigma—a damaging social process—includes prejudice, devaluation, negative attitudes, and discrimination towards PWH.8–10 Conceptual frameworks and empirical work suggest that HIV-related stigma is a multidimensional construct, including experienced (i.e., exposure to actual acts of discrimination, devaluation, prejudice, and abuse), anticipated (i.e., fears of experiencing stigma), perceived community (perception of public attitudes about PWH), and internalized stigma (i.e., negative self-image, when PWH internalize negative attitudes about PWH that exist in society and apply these to themselves).8,11–13 Existing studies have consistently provided evidence for the deleterious effects of HIV-related stigma on ART adherence, visit adherence, and viral load suppression.14–17
The literature also suggests that dimensions of HIV-related stigma are interrelated and may affect one another.12,18 Theoretically, when PWH experience stigma and/or discrimination from others in the society, whether actual or perceived, this can lead to feelings of shame, self-blame, and low self-esteem, possibly causing them to internalize stigma and accept and endorse negative societal evaluations about having HIV.19,20 In turn, the internalization of stigma may have adverse effects on physical and psychological health for PWH, such as increased depression symptoms and non-adherence to treatment regimens.18,21 For instance, one study reported that perceived community stigma leads to internalized stigma and anticipated stigma. These stigma dimensions, in turn, were associated with poorer ART adherence.18 In another study, experienced stigma in healthcare settings was found to be associated with diminished trust in physicians through the pathways of internalized stigma and anticipated stigma from healthcare workers.22 Additionally, the association between experienced stigma in healthcare settings and trust in health care providers — a significant predictor of suboptimal health outcomes (e.g., higher viral load, lower medication adherence)23,24 — was found to be mediated by internalized stigma and anticipated stigma from the community.22 Thus, research provides initial support for the theoretical hypothesis that stigma that starts in the community (“external” to PWH) can get under the skin and be internalized by PWH. However, these studies were all cross-sectional, which underscores the importance of testing the mediating role of internalized stigma in the effects of other stigma dimensions using longitudinal data.
Furthermore, effects of HIV-related stigma dimensions on health behaviors and outcomes may be mediated by mental health factors. Several studies suggested that depression mediates the association between HIV-related stigma and medication adherence.15,16,25,26 Although various mechanisms through which HIV-related stigma affects adherence and HIV outcomes have been established, there is a scarcity of research that has empirically evaluated potential longitudinal mechanisms over time. One study with women living with HIV reported that internalized stigma at baseline leads to depressive symptoms 18 months after the baseline, which in turn leads to poorer ART adherence at follow-up (two years after the baseline).27 Another study conducted with African American women receiving HIV treatment found that HIV stigma was associated with subsequent viral load but neither depression nor social support mediated this association.28 However, much of the limited research up to now has focused on PWH in research cohort studies who have been in HIV care for many years. Thus, more research is warranted to determine the magnitude of these complex mechanisms longitudinally starting with initiating HIV care and elucidate temporal relationships to provide further evidence for causality.
In the first year following HIV care initiation, new-to-care PWH are a vulnerable group, with significant challenges of adjustment to a life-changing health condition, adherence to HIV treatment recommendations, dealing with stigma, and associated adverse physical and psychological health symptoms. Thus, understanding barriers to ART adherence and viral suppression among PWH who are newly entering HIV medical care can have profound implications for individual health and health outcomes in the short- and longer-term.
In this study, we hypothesized that experienced stigma as well as perceived community stigma at the time of initiating care (i.e., at baseline) leads to suboptimal ART adherence or non-suppressed viral load at 48 weeks (follow-up), mediated by internalized stigma and depression symptoms at 48 weeks. More specifically, PWH who experience stigma and discrimination from others or who believe the existence of stigmatizing attitudes in the community may endorse and accept stigmatizing beliefs about PWH and apply these beliefs to themselves (i.e., internalize stigma), which subsequently results in depression symptoms. Depression symptoms, in turn, may lead to poorer ART adherence or non-suppressed viral load. Knowledge obtained in this area will lead to a deeper understanding of longitudinal links between dimensions of stigma, ART adherence, and viral suppression, which can be used for intervention development and service provision. Given the importance of both linkage to and sustained adherence to HIV care and treatment, elucidating the effects of HIV-related stigma on outcomes, especially when PWH first start HIV care, is important in terms of developing effective and responsive treatments.
Methods
Participants and Procedure
The sample consisted of 371 PWH who recently initiated outpatient HIV care and participated in a multi-site study called “integrating ENGagement and Adherence Goals upon Entry (iENGAGE)” at four HIV clinical sites in the United States: Johns Hopkins University, University of Alabama at Birmingham, University of North Carolina at Chapel Hill, and University of Washington. All participants were enrolled in this study within 14 days of their first outpatient HIV medical care visit at one of these study sites and data were collected between December 2013 and December 2018. Participants were asked to complete a computer-assisted survey for self-reported measures and clinic data were extracted from medical records. All measures were collected at baseline and 48 weeks later, except for the outcome variables adherence and viral load, which were measured only at the 48-week assessment. The study was approved by the Institutional Review Board of each HIV clinical site.
Measures
HIV-related Stigma Measures
Experienced, perceived community, and internalized stigma were assessed using three subscales (experienced stigma, concern with public attitudes, and negative self-image) of the HIV Stigma Scale.11 The experienced stigma subscale includes 11 items (e.g., “People have physically backed away from me because I have HIV/AIDS”), the perceived community stigma subscale includes six items (e.g., “Most people are uncomfortable around someone with HIV/AIDS”), and the internalized stigma subscale includes seven items (e.g., “Having HIV/AIDS makes me feel that I’m a bad person”). The items were rated on a 4-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree). All three subscales have good psychometric properties.8,11 Mean scores on each stigma subscale are calculated by taking the mean of the corresponding items. Higher mean scores on each subscale indicate higher stigma. Cronbach’s alpha was .92 for experienced stigma at baseline, .84 for perceived community stigma at baseline, and .81 for internalized stigma at 48-week follow-up.
Depression Symptoms
The Patient Health Questionnaire (PHQ-8) (Kroenke et al., 2009), which has eight items rated on a four point-Likert scale (0 =not at all, 3= every day), was used to measure depression symptoms over the past two weeks. A composite score is calculated by using the mean of non-missing items. Higher scores indicate higher depression symptoms. In the current study, Cronbach’s alpha was .80 for depression symptoms at 48-week follow-up.
ART Adherence
ART adherence was assessed with the single question4 asking participants’ ability in the past 4 weeks to take their anti-HIV medications prescribed by the doctor. Participants used ratings with a six point-Likert scale (1=very poor, 2=poor, 3=fair, 4=good, 5=very good, 6=excellent). This is a validated measure of ART adherence.5 This measure was dichotomized as “less than excellent” for those who checked options other than “excellent” vs. “excellent adherence” for those who checked “excellent” in response to the question.
Viral Load
Data on viral load were taken from the most recent clinic record of participants at the final visit. This measure was dichotomized as “suppressed” (<200 c/mL) vs. “not suppressed” (≥200 c/mL).
Statistical Analyses
In order to preserve the temporal sequence between the independent variable and the mediator and outcome variable, we tested the indirect effect of experienced stigma as well as perceived community stigma (independent variables) at the time of initiating care (i.e., at baseline) on the outcome variables suboptimal ART adherence and non-suppressed viral load at 48 weeks (follow-up) through internalized stigma and depression symptoms (mediators) at 48 weeks (Figures 1–4). For the hypothesized serial mediation models, we tested indirect effects using 2000 bootstrapped resamples with 95% confidence interval in Process Macro for IBM SPSS.29 An indirect effect is considered significant if the confidence interval does not include zero, which is evidence for mediation. In each model, age, gender, race, and viral load at baseline (only in the models where viral suppression at follow-up was the outcome) were entered as covariates. The iENGAGE is an intervention study aimed at fostering adjustment to living with HIV and adherence to HIV care through focusing on problem solving, affect management, and communication skills. PHW were either assigned to intervention or control group. Thus, in the present study, study arm was also used as a control variable. In all of the models, unstandardized beta (B) values were reported.
Results
Descriptive statistics are presented in Table 1. Participants mostly defined their race/ethnicity as Black or African American (62.3%). Two hundred and ninety-four participants (79.2%) described their gender as male and 94.6% described their ethnicity as non-Hispanic. 46.9% reported their insurance status as public insurance. The mean age of the participants was 35.71 (SD = 11.91). Mean scores were 2.18 (SD = 0.73; range: 1–4) for experienced stigma at baseline, 2.69 (SD = 0.68; range: 1–4) for perceived community stigma at baseline, 2.17 (SD = 0.73; range: 1–4) for internalized stigma at 48-week follow-up, and 5.83 (SD = 5.86; range: 0–23) for depression symptoms at 48-week follow-up.
First, we tested the serial (chain) mediation model from experienced stigma or perceived community stigma at baseline to ART adherence at the 48-week follow-up, mediated by internalized stigma and depression symptoms at the 48-week follow-up (see Figures 1 and 2). The total effect of experienced stigma on ART adherence was significant when internalized stigma and depression symptoms were not in the model (B = −.42, SE = .19, p = .026). The serial indirect effect of experienced stigma on ART adherence through first internalized stigma and then depression symptoms was significant (B = −.08, SE = .04, 95% CI [−.162, −.009]), suggesting that experienced stigma leads to internalized stigma (B = .33, p = .000), which leads to depression symptoms (B = 3.56, p = .000), which in turn leads to lower ART adherence (B = −.06, p = .016) (see Figure 1). On the other hand, the total effect of perceived community stigma on ART adherence was not significant when internalized stigma and depression symptoms were not in the model (B = −.18, SE = .20, p = .359). The serial indirect effect of perceived community stigma on ART adherence first through internalized stigma and then through depression symptoms was also significant (B = −.09, SE =.04, 95% CI [−.191, −.028]), suggesting that perceived community stigma leads to internalized stigma (B = .31, p = .000), which leads to depression symptoms (B = 3.71, p = .000), which in turn leads to lower ART adherence (B = −.08, p = .004) (see Figure 2).
Figure 1.
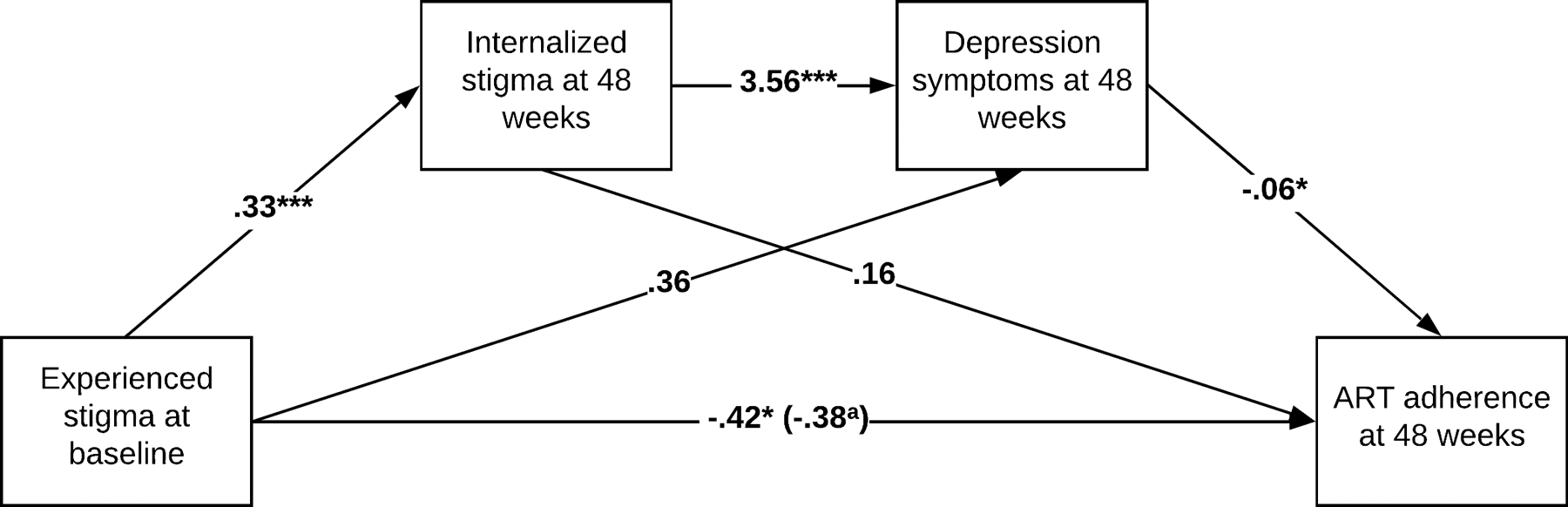
Serial mediation model in the association between experienced stigma and ART adherence. aWhen internalized stigma and depression symptoms are in the model. *p < 0.05; ***p < 0.001.
Figure 2.
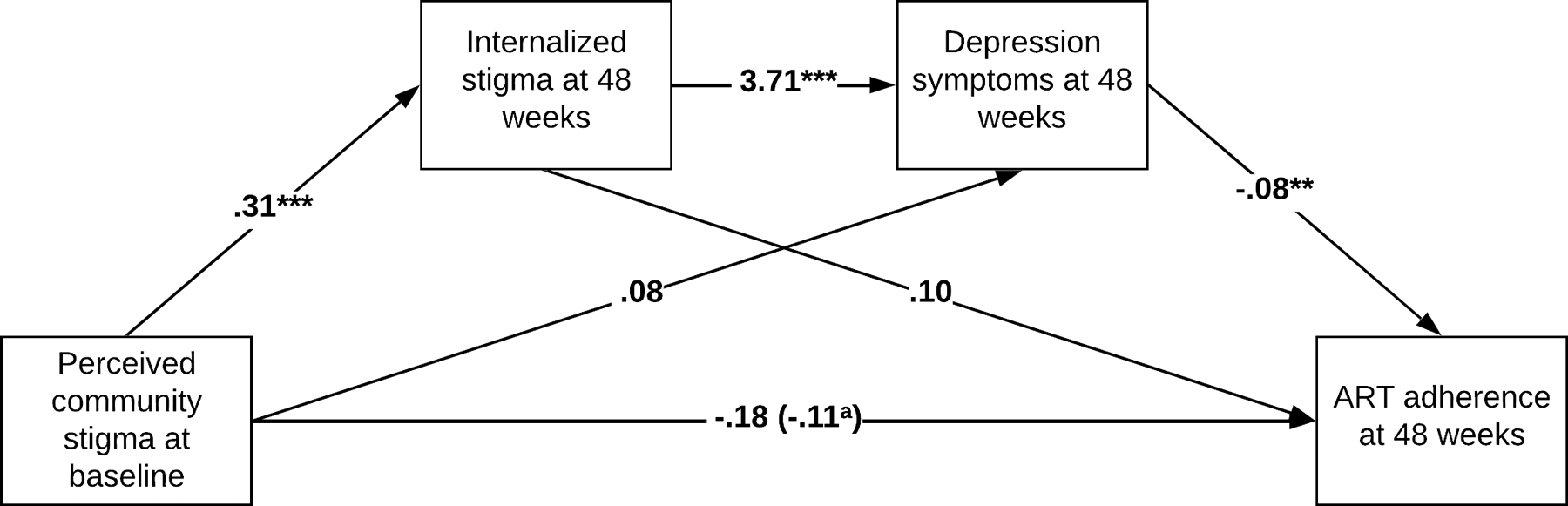
Serial mediation model in the association between perceived community stigma and ART adherence. aWhen internalized stigma and depression symptoms are in the model. **p < 0.01; ***p < 0.001.
Finally, we tested the same serial mediation models from experienced or perceived community stigma first through internalized stigma and then through depression symptoms with viral suppression at 48-week follow-up as the outcome. The total effect of experienced stigma on viral load suppression was not significant (before adding internalized stigma and depression symptoms to the model; B = −.27, SE = .27, p = .321). The serial indirect effect of experienced stigma on viral suppression was significant (B = −.10, SE = .05, 95% CI [−.233, −.012]), suggesting that experienced stigma leads to internalized stigma (B = .32, p = .000), which leads to depression symptoms (B = 3.67, p = .000), which in turn lead to lower odds of viral suppression (B = −.09, p = .015) (see Figure 3). The total effect of perceived community stigma on viral load suppression was not significant (B = −.13, SE = .29, p = .653). The serial indirect effect of perceived community stigma on viral suppression was significant (B = −.11, SE = .06, 95% CI [−.252, −.009]), suggesting that perceived community stigma leads to internalized stigma (B = .34, p = .000), which leads to depression symptoms (B = 3.93, p = .000), which in turn lead to lower odds of viral suppression (B = −.08, p = .022) (see Figure 4).
Figure 3.
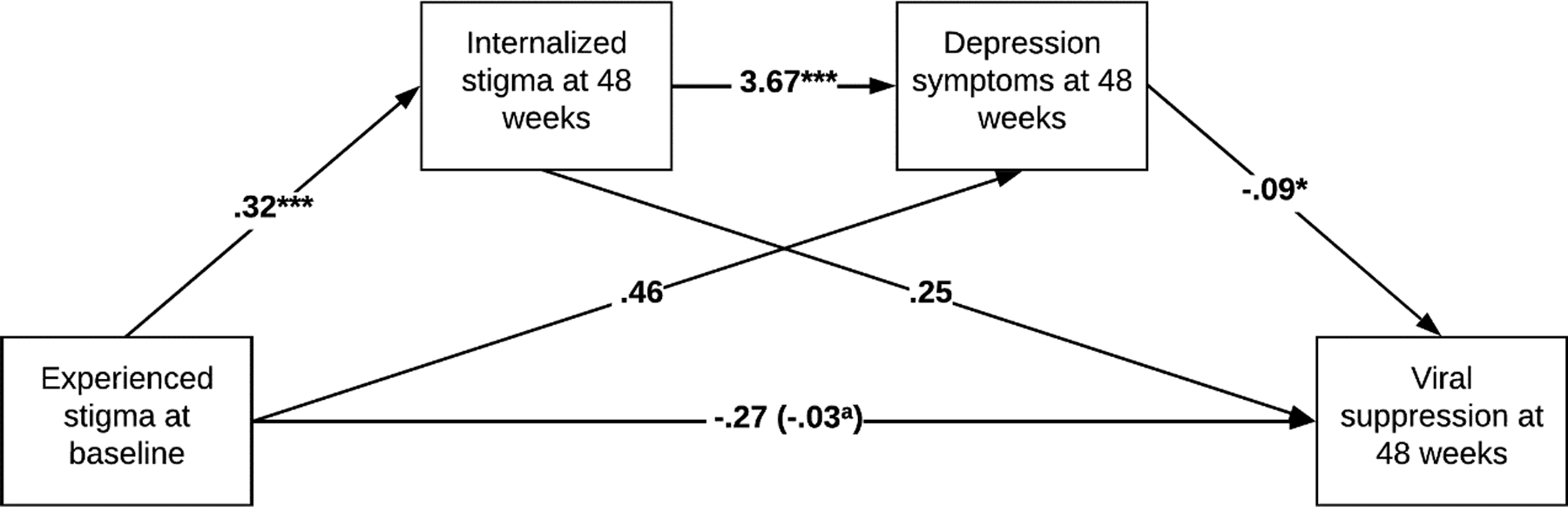
Serial mediation model in the association between experienced stigma and viral suppression. aWhen internalized stigma and depression symptoms are in the model. *p < 0.05; ***p < 0.001.
Figure 4.
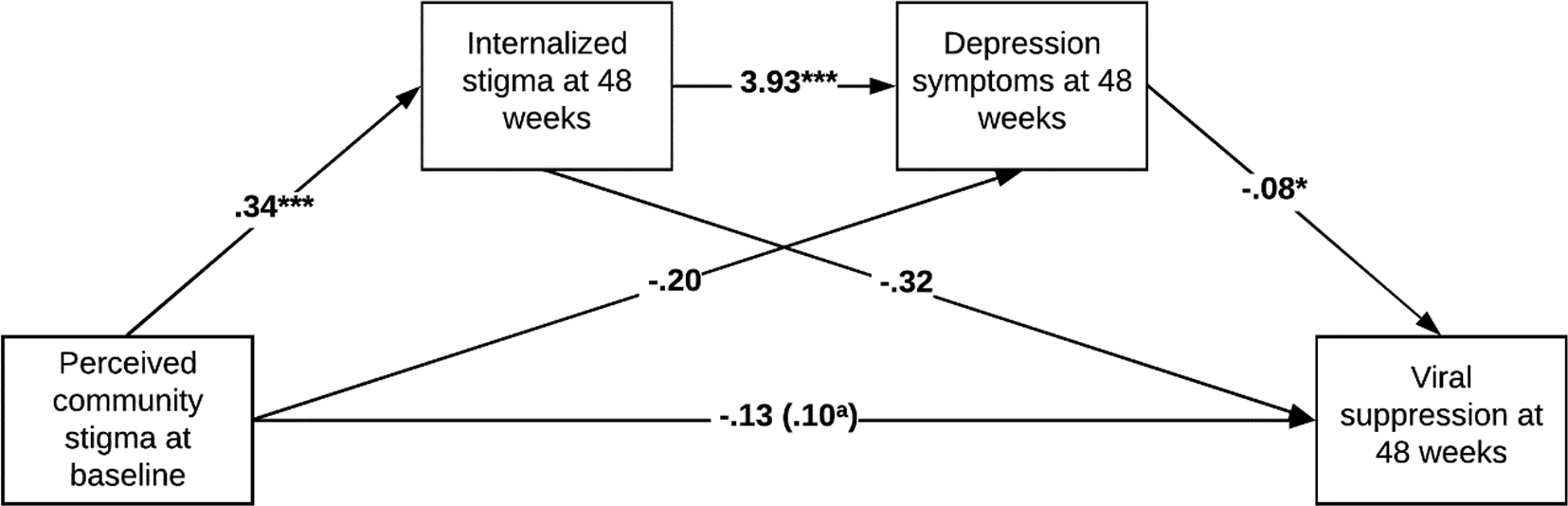
Serial mediation model in the association between perceived community stigma and viral suppression. aWhen internalized stigma and depression symptoms are in the model. *p < 0.05; ***p < 0.001.
Discussion
The present study examined the longitudinal effects of HIV-related experienced and perceived community stigma (stigma dimensions with a source external to PWH) on ART adherence and viral load through the pathways of internalized stigma and depression symptoms. We found that internalized stigma and depression symptoms mediate the associations between both experienced stigma and perceived community stigma and key HIV indicators including ART adherence and viral suppression. Despite cross-sectional studies revealing plausible connections between HIV-related stigma and HIV health outcomes, research examining these connections longitudinally is scarce. Furthermore, there are a limited number of studies examining mechanisms through which HIV-related stigma leads to adverse HIV clinical outcomes among PWH new to care. Thus, our results extend prior work on HIV-related stigma by exploring potential longitudinal mechanisms and providing important information to inform and strengthen interventions at this vulnerable time following HIV care entry.
One important finding of this study is that perceived community stigma was associated with internalized stigma, which in turn was associated with depression symptoms, resulting in sub-optimal ART adherence and lower odds of viral suppression. We also found that experienced stigma was associated with internalized stigma, which was associated with depression symptoms, which in turn were associated with poor ART adherence and lower odds of viral suppression. These findings corroborate and extend previous findings from cross-sectional and longitudinal studies with PWH who have been in treatment for a while15,18,22,30 suggesting that internalized stigma and/or depression mediates the association between perceived community stigma (or perceived discrimination) and suboptimal health outcomes.
Given that studying the mediating role of internalized stigma in the effects of other stigma dimensions stemming from the community is a relatively new area in HIV research, the findings of the current study have important implications. The finding that experienced stigma and perceived community stigma may affect health outcomes through internalized stigma and depression symptoms suggests that improving adherence to HIV care and viral suppression as well as improved mental health for PWH may not be achievable when only targeting one individual-level dimension of HIV-related stigma as the bulk of previous research attempted. Rather, targeting different dimensions of stigma simultaneously can be more effective in achieving desired health outcomes for PWH, taking into consideration how one dimension may lead to another dimension. Our results suggest that community-level stigmas may be antecedent factors that are likely to cause PWH to develop internalized stigma, with downstream effects on health outcomes. Thus, community-level interventions addressing stigma in society may be a more effective long-term solution. Additionally, at the individual level, addressing internalized stigma may be another strategy since internalized stigma emerges as the most powerful and proximal stigma dimension in predicting suboptimal health outcomes for PWH. In this sense, existing interventions, including cognitive behavioral therapy, acceptance and commitment therapy, and problem-solving therapy, might be helpful for targeting internalized stigma and improving adherence to HIV treatment by challenging negative cognitions and emotions regarding stigma and preventing internalization of stigma in the society.31,32
Depression symptoms emerged as a mediating mechanism of the association between experienced or perceived community stigma and ART adherence through the pathway of internalized stigma. This finding is in accord with previous studies indicating that PWH are at great risk for having depressive symptoms because of stigmatization and/or discrimination33,34 and that depression and/or internalized stigma mediates the relationship between perceived or experienced stigma and health outcomes.16,18,22,35 PWH may internalize stigma, particularly when they experience actual acts of discrimination and abuse (i.e., experienced stigma), and when they perceive negative attributions and attitudes in the community (i.e., perceived community stigma). In turn, the experience of internalizing stigma leads to depression symptoms, ultimately resulting in undesired health outcomes, such as poor ART adherence and detectable viral load. At this point, our findings suggest that focusing upon or prioritizing depression symptom management in addition to stigma dimensions can maximize the effectiveness of adherence interventions, particularly considering overlapping aspects of internalized stigma and depression, such as negative self-image, self-blame, worthlessness, self-devaluation, and feelings of negativity.
This study had several limitations. The sample size of the study is relatively small, and study measures were taken only at two time points: baseline and 48 weeks (follow-up). The sample included participants from an intervention study, who received either an intervention or standard of care (for the details, see Yigit et al.’s study36), which might have affected our findings, even though we adjusted for the effect of study arm. The current study did not assess other intersectional stigmas, such as poverty stigma, racism, sexism, and heterosexism, which may also be important determinants of the outcomes. The participants might not be representative of all PWH because they were recruited from four well-resourced sites affiliated with major academic health centers in the U.S., which is likely to limit generalizability of our findings to other clinical settings. Furthermore, our data included a small number of people of Latino ethnicity, which could be also taken as a limitation for generalizability since this population compromise a considerable percentage of individuals newly diagnosed with HIV. Additionally, despite having been validated in prior studies, using a single item for adherence could be considered a potential limitation. Finally, we assessed experienced stigma that PWH might face in the broader society and did not address experienced stigma within healthcare settings, which further research may address.
Future research should address several key areas to overcome the limitations highlighted in this study. First, conducting longitudinal studies with larger and more diverse samples could provide a more comprehensive understanding of the complex relationship between HIV-related stigma and adverse health outcomes among PWH. Employing measures at multiple time points would allow for a better grasp of the dynamic nature of the effects of HIV-related stigma on health outcomes over time. Furthermore, investigating intersectional stigmas, such as racism, sexism, and stigma related to poverty, in conjunction with HIV stigma could reveal crucial determinants of health outcomes. Considering the influence of healthcare settings in perpetuating stigma and its impact on health outcomes for PWH, future studies should delve into stigma experienced within these environments. Additionally, to enhance the generalizability of findings, research should aim to recruit more representative samples, including larger proportions of populations, such as Latino individuals, who represent a significant portion of new HIV diagnoses. Moreover, employing more robust measures for adherence and examining the impact of stigma on suboptimal health outcomes within diverse clinical settings would provide a more nuanced understanding. Addressing these avenues in future research could better inform the development of targeted interventions to mitigate the negative effects of stigma on the health and well-being of PWH, especially those new to care, thereby improving overall health outcomes in this population. Finally, it is crucial to highlight that a substantial amount of additional research, particularly longitudinal research, is necessary to develop effective interventions designed to diminish HIV-related stigma and enhance health outcomes for PWH.
Notwithstanding these limitations, the current study contributes to existing knowledge of HIV stigma and its effects on health outcomes for PWH by elucidating mediating pathways and providing evidence for potential links over time. Our findings suggest that different forms of HIV stigma, including experienced, perceived, and internalized stigma, can negatively impact ART adherence and viral suppression as well as psychological well-being. By focusing on stigma particularly among PWH new to care who are an understudied and vulnerable group, our findings provide valuable information about the crucial initial phase of HIV treatment and care.
Conflict of Interest and Source of Funding:
The authors declare that there is no conflict of interest. This work was supported by the National Institutes of Allergy and Infectious Diseases (NIAID) [grant numbers R01AI103661, 3R01AI103661-03S1, and R03DA052180]. This research was also supported by the University of Alabama at Birmingham (UAB) Center for AIDS Research CFAR, and a National Institutes of Health funded program [P30 AI027767] that was made possible by the following institutes: NIAID, NCI, NICHD, NHLBI, NIDA, NIA, NIDDK, NIGMS, and OAR. M. J. M. has received grant support (to the University of Alabama at Birmingham) from Merck Foundation.
Footnotes
NCT Identifier: NCT01900236
References
- 1.Gardner EM, McLees MP, Steiner JF, Del Rio C, Burman WJ. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clinical infectious diseases. 2011;52(6):793–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clinical infectious diseases. 2013;57(8):1164–1171. [DOI] [PubMed] [Google Scholar]
- 3.Kitahata MM, Gange SJ, Abraham AG, et al. Effect of early versus deferred antiretroviral therapy for HIV on survival. New England Journal of Medicine. 2009;360(18):1815–1826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nwangwu‐Ike N, Saduvala N, Watson M, Panneer N, Oster AM. HIV diagnoses and viral suppression among US women in rural and nonrural areas, 2010–2017. The Journal of Rural Health. 2020;36(2):217–223. [DOI] [PubMed] [Google Scholar]
- 5.Sackoff JE, Hanna DB, Pfeiffer MR, Torian LV. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Annals of internal medicine. 2006;145(6):397–406. [DOI] [PubMed] [Google Scholar]
- 6.Johnson AS, Johnson SD, Hu S, et al. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data: United States and 6 dependent areas, 2017. 2019;
- 7.Lyons SJ, Johnson AS, Hu X, et al. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data: United States and 6 dependent areas, 2018. 2020;
- 8.Earnshaw VA, Chaudoir SR. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS and Behavior. 2009;13(6):1160–1177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Herek GM, Capitanio JP. AIDS stigma and contact with persons with AIDS: Effects of direct and vicarious contact. 1. Journal of Applied Social Psychology. 1997;27(1):1–36. [Google Scholar]
- 10.Link BG, Phelan JC. Conceptualizing stigma. Annual review of Sociology. 2001;27(1):363–385. [Google Scholar]
- 11.Berger BE, Ferrans CE, Lashley FR. Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale¶. Research in nursing & health. 2001;24(6):518–529. [DOI] [PubMed] [Google Scholar]
- 12.Turan B, Hatcher AM, Weiser SD, Johnson MO, Rice WS, Turan JM. Framing mechanisms linking HIV-related stigma, adherence to treatment, and health outcomes. American Journal of Public Health. 2017;107(6):863–869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Earnshaw VA, Smith LR, Chaudoir SR, Amico KR, Copenhaver MM. HIV stigma mechanisms and well-being among PLWH: a test of the HIV stigma framework. AIDS and Behavior. 2013;17(5):1785–1795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sweeney SM, Vanable PA. The association of HIV-related stigma to HIV medication adherence: a systematic review and synthesis of the literature. AIDS and Behavior. 2016;20(1):29–50. [DOI] [PubMed] [Google Scholar]
- 15.Turan B, Rogers AJ, Rice WS, et al. Association between perceived discrimination in healthcare settings and HIV medication adherence: mediating psychosocial mechanisms. AIDS and Behavior. 2017;21(12):3431–3439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Turan B, Smith W, Cohen MH, et al. Mechanisms for the negative effects of internalized HIV-related stigma on antiretroviral therapy adherence in women: the mediating roles of social isolation and depression. Journal of acquired immune deficiency syndromes. 2016;72(2):198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Seghatol-Eslami VC, Dark HE, Raper JL, Mugavero MJ, Turan JM, Turan B. Interpersonal and intrapersonal factors as parallel independent mediators in the association between internalized HIV stigma and ART adherence. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2017;74:e18–e22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS and Behavior. 2017;21(1):283–291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Goffman E Stigma: Notes on the management of spoiled identity. Simon and Schuster; 2009. [Google Scholar]
- 20.Turan B, Crockett KB, Buyukcan-Tetik A, et al. Buffering Internalization of HIV Stigma: Implications for Treatment Adherence and Depression. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2019;80(3):284–291. doi: 10.1097/qai.0000000000001915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fazeli PL, Turan JM, Budhwani H, et al. Moment-to-moment within-person associations between acts of discrimination and internalized stigma in people living with HIV: An experience sampling study. Stigma and health. 2017;2(3):216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kay ES, Rice WS, Crockett KB, Atkins GC, Batey DS, Turan B. Experienced HIV-related stigma in healthcare and community settings: Mediated associations with psychosocial and health outcomes. Journal of acquired immune deficiency syndromes (1999). 2018;77(3):257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dale SK, Bogart LM, Wagner GJ, Galvan FH, Klein DJ. Medical mistrust is related to lower longitudinal medication adherence among African-American males with HIV. Journal of health psychology. 2016;21(7):1311–1321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brincks AM, Shiu-Yee K, Metsch LR, et al. Physician mistrust, medical system mistrust, and perceived discrimination: associations with HIV care engagement and viral load. AIDS and Behavior. 2019;23(10):2859–2869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Turan B, Rice WS, Crockett KB, et al. Longitudinal association between internalized HIV stigma and antiretroviral therapy adherence for women living with HIV: the mediating role of depression. Aids. 2019;33(3):571–576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yigit I, Bayramoglu Y, Weiser SD, et al. Changes in internalized stigma and HIV health outcomes in individuals new to HIV care: The mediating roles of depression and treatment self-efficacy. AIDS Patient Care and STDs. 2020;34(11):491–497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Turan B, Rice WS, Crockett KB, et al. Longitudinal association between internalized HIV stigma and antiretroviral therapy adherence for women living with HIV: The mediating role of depression. AIDS (London, England). 2019;33(3):571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kemp CG, Lipira LL, David H, et al. HIV stigma and viral load among African-American women receiving treatment for HIV: A longitudinal analysis. AIDS (London, England). 2019;33(9):1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford publications; 2017. [Google Scholar]
- 30.Van Der Kooij YL, Kupková A, Den Daas C, et al. Role of self-stigma in pathways from HIV-related stigma to quality of life among people living with HIV. AIDS Patient Care and STDs. 2021;35(6):231–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Skinta MD, Lezama M, Wells G, Dilley JW. Acceptance and compassion-based group therapy to reduce HIV stigma. Cognitive and Behavioral Practice. 2015;22(4):481–490. [Google Scholar]
- 32.Tshabalala JVM. Developing a cognitive behavioural therapy model to assist women to deal with HIV and stigma. South African Journal of Psychology. 2011;41:17–28. [Google Scholar]
- 33.Rueda S, Mitra S, Chen S, et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses. BMJ open. 2016;6(7):e011453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ayano G, Solomon M, Abraha M. A systematic review and meta-analysis of epidemiology of depression in people living with HIV in east Africa. BMC psychiatry. 2018;18(1):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rao D, Feldman BJ, Fredericksen RJ, et al. A structural equation model of HIV-related stigma, depressive symptoms, and medication adherence. AIDS and Behavior. 2012;16(3):711–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yigit I, WEISER SD, JOHNSON MO, MUGAVERO MJ, TURAN JM, TURAN B. Effects of an intervention on internalized HIV-related stigma for individuals newly entering HIV care. AIDS (London, England). 2020;34(Suppl 1):S73. [DOI] [PMC free article] [PubMed] [Google Scholar]