

Abstract
Purpose:
Black men face a higher incidence of high-risk prostate cancer (PCa) compared with non-Black men. While the 4Kscore is a widely utilized commercial test for PCa risk assessment, it does not currently account for racial differences. The aim of this study is to describe and validate a prespecified race coefficient for the 4Kscore with the goal of improving the accuracy of this test for Black men.
Materials and Methods:
Using data from 85 Black men from the initial US prospective validation study, a race coefficient of 0.6 on the log-odds scale was pre-specified. We calculated discrimination, calibration, and clinical utility of the 4Kscore with and without this coefficient for Black race in our primary analysis cohort of 205 Black men undergoing biopsy for PCa in a Veterans Affairs (VA) institution. We performed a sensitivity analysis using a combined cohort from the US prospective validation and the VA studies.
Results:
The mean probability of high-grade PCa from the 4Kscore in the primary cohort increased from 25% to 37% with race coefficient addition. Incorporating the race coefficient improved 4Kscore’s calibration in Black men, with consequent improvements in clinical utility based on decision curve analysis. Model discrimination was maintained (AUC 0.825 vs 0.828, p = 0.14) in the combined cohort of Black and non-Black men from the US prospective and VA studies and the calibration remained largely unchanged.
Conclusions:
Incorporating a prespecified coefficient for Black race improved calibration and clinical utility of the 4Kscore among Black men and should be added to the 4Kscore.
Keywords: African Americans, biomarkers, prostate neoplasm
Introduction
Prostate specific antigen (PSA) screening reduces prostate cancer (PCa) mortality but results in a significant number of men being subjected to unnecessary prostate biopsies or under-detection of clinically significant cancers. The 4Kscore test is a widely used panel of 4 serum kallikreins (total PSA, free PSA, intact PSA, and human kallikrein 2) combined with clinical information (age, prior negative biopsy, digital rectal exam) to provide a probability of high-grade PCa, defined as Grade Group 2 or higher. The test was extensively tested in Europe1 and prospectively validated in the United States2 to enhance pre-prostate biopsy decision making.
In these studies, most participants were White. However, men who self-report as Black race are known to be at increased risk for high-grade PCa.3 With this rationale in mind, the 4Kscore was validated in a Veterans Affairs (VA) study which consisted of a cohort with majority (56%) Black men.4 In this study, the calibration of the 4Kscore in the entire cohort was good but the specific calibration for Black men was not investigated. Given the significantly increased incidence of prostate cancer in Black men we sought to assess the 4Kscore’s performance in the sub-cohort of Black men from the VA study.
A pre-specified race coefficient was developed to adjust the 4Kscore for the increased risk of high-grade PCa in Black men before any patients were enrolled in the VA trial. Here, our primary objective is to report the performance of the 4Kscore with and without the race coefficient in an independent cohort of Black men from the VA trial. Our secondary objective was to assess the performance in a combined cohort more representative of the US population.
Material and Methods
Study populations
This study used data from two existing studies of the 4Kscore: the initial US prospective study2 and the VA study,4 and the recruitment criteria and laboratory methods were previously described. The initial prospective 4Kscore validation study included 1,012 US men, of whom 85 (8.4%) were Black. Two statisticians (AV and DD) assessed the calibration of the 4Kscore for detecting high-grade disease in these 85 men. Based on these data and a review of the literature, they prespecified that the 4Kscore to be tested would include a coefficient of 0.6 on the log-odds scale (an odds ratio of 1.82) for men self-identifying as Black, with no change for men of other races. The coefficient was finalized in the signed and dated statistical analysis plan before any data from the VA study was available. The VA study consisted of 366 men, of whom 205 (56%) were Black, referred for prostate biopsy from 8 VAs across the country.
Statistical analysis
We compared the performance of the 4Kscore with and without the Black race coefficient of 0.6 on the log odds scale in the 205 Black men from the VA study. We also compared the performance of the race coefficient in a combined cohort of Black and non-Black men from both the initial prospective validation and the VA studies, a cohort more representative of the US population. We chose this as a sensitivity analysis on the grounds that the data from the Black men in the US prospective validation study were available to the study investigators before the Black coefficient was finalized. This is even though the prespecified race coefficient was not that found in the US validation study, calculated as 0.45 (95% CI 0.14, 1.03). We assessed model calibration using calibration plots, model discrimination by area under the receiver operating curve (AUC), and net benefit using decision curve analysis. We explored the clinical consequences of using the 4Kscore algorithm at various biopsy thresholds. These results were compared with the performance of the unmodified 4Kscore. Where warranted, the AUCs of the modified and unmodified 4Kscores were compared using DeLong’s method.5 All analyses were conducted using R version 4.2.0 with tidyverse (v1.3.1), dcurves (0.3.0) and gtsummary (v1.6.1) packages.
Results
Among Black men in the VA study, the rate of high-grade PCa was 40%. In the combined cohort, the rate of high-grade PCa was higher among Black men compared with non-Black men (38% vs 23%). Black men had higher PSA levels at biopsy (6.8ng/mL [IQR4.8-10.3]) compared with non-Black men (5.2ng/mL [IQR 3.7-7.5]). Age and rate of prior negative biopsy were not different between study and race cohorts (Table 1).
The median probability of high-grade PCa as determined by the 4Kscore in Black men from the VA study was 25% and increased to 37% after adjusting the 4Kscore by the race coefficient. Including the coefficient improved the 4Kscore’s calibration with slopes approaching the ideal 45° line in clinically relevant thresholds (Figure 1A). When stratified by race the actual rate of clinically significant cancer is similar to the predicted rate (Table 2). When examining Black men from both cohorts the race coefficient still improved the calibration (Figure 1B).
Figure 1.

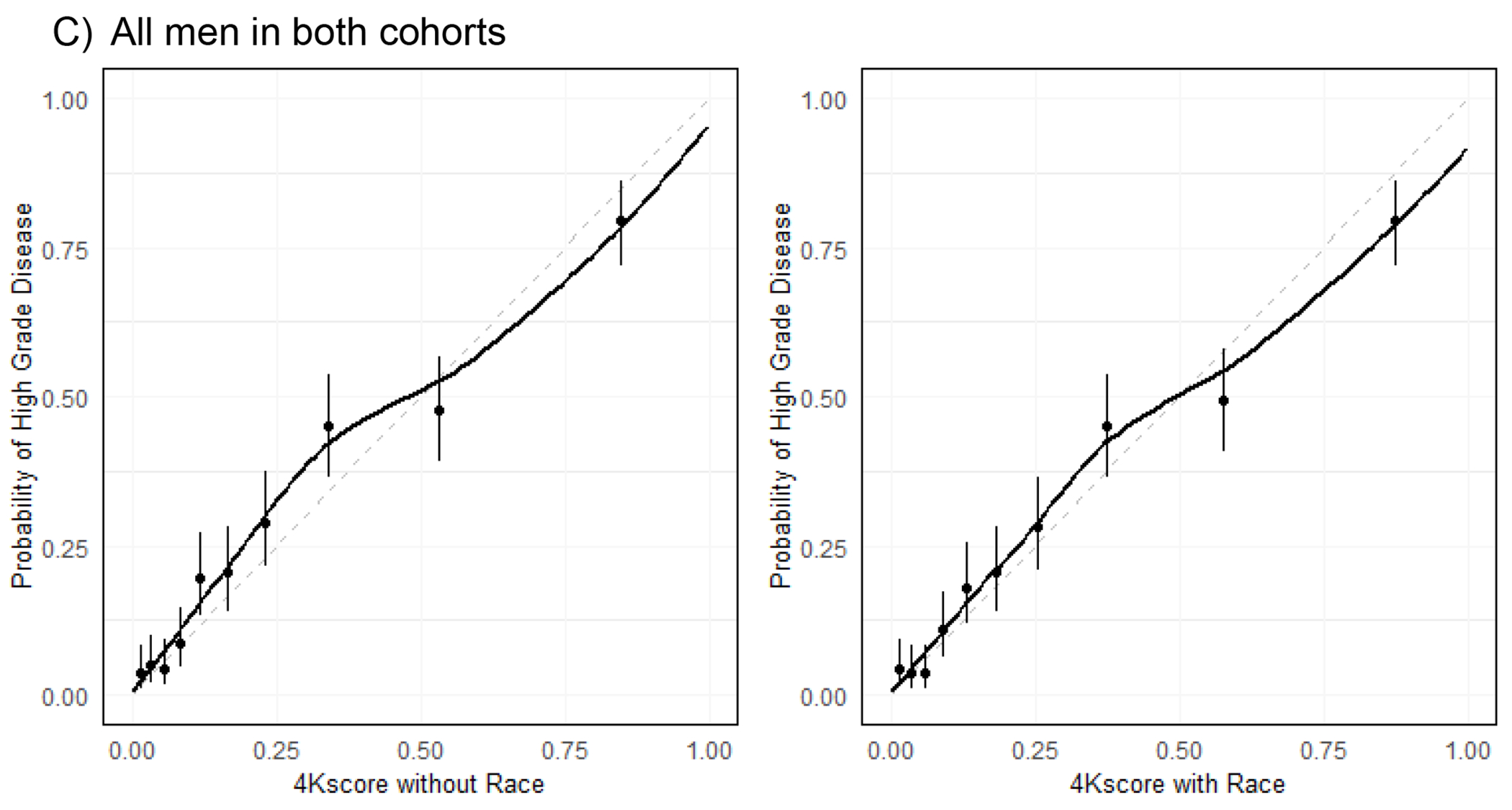
Calibration of the 4Kscore before and after application of the race coefficient
A) represents calibration before and after the race coefficient adjustment in 205 men in the VA cohort. B) represents calibration before and after race coefficient in black men from both cohorts (N= 290). C) represents calibration before and after race coefficient in all men in both studies (N=1,378). A calibration curve slope of 45 degrees is ideal.
The race coefficient also improved clinical utility: The decision curves analysis of the primary validation cohort of Black VA patients showed a higher net benefit within accepted threshold probabilities for performing a biopsy (Figure 2). Table 3 illustrates specific clinical consequences using results standardized to 1,000 patients. For example, at a biopsy threshold of 9%, the modified 4Kscore resulted in a reduction of 15 biopsies per 1,000 men, while delaying the diagnosis of only 5 patients with high grade cancers. At the same biopsy threshold, the unmodified 4Kscore delayed the diagnosis of three times as many men with high grade cancers while increasing the number of biopsies avoided by only about 50%. Calibration plots from non-black patients in both cohorts (Supp. Fig. 1) and race stratified decision curves from the primary validation cohort (Supp. Fig. 2) are also provided.
Figure 2.

Decision curve analysis of 4Kscore among primary validation cohort (VA cohort)
Explanation for net benefit: Curve with highest net benefit at any biopsy threshold results in best clinical results. Red curve represents biopsy in all patients. Green curve represents biopsy in no patients. Purple curve represents biopsy decision using the 4Kscore without race coefficient. Blue curve presents biopsy decision using 4Kscore with race coefficient.
In the combined cohort, model discrimination was maintained (AUC 0.825 vs 0.828, p = 0.14), and overall calibration improved slightly and remained close to ideal (Figure 1c). In the VA cohort, the AUC was 0.813 without the race coefficient and 0.820 with the race coefficient.
Discussion
Despite having a higher risk of aggressive PCa, Black men have been underrepresented in biomarker studies.1 The VA study provided the opportunity to take a closer look at the performance of the 4KScore test specifically in Black men and to validate our pre-specified coefficient for Black race.4 Black race-specific cutoffs for PSA and other biomarkers have been suggested,6,7 but thus far no biomarker to our knowledge has introduced a race specific coefficient to adjust model calibration and validated its performance in an independent cohort of Black men. In this study, we generate and validate the performance of a race-specific coefficient to improve the calibration and clinical utility of the 4Kscore for Black men.
We acknowledge that using race as a correlate for biology is not ideal and there is increased hesitancy to use it as a monolithic variable to calculate risk.8 Race is a social construct incorporating complex interactions between genetic, clinical, and environmental factors. The increased prostate cancer incidence and higher adverse risk seen in Black men are primarily underlined by genomic factors.9–11 Certain genomic variations, such as HOXB13 are predominantly found in West Africa where most Black Americans can trace their ancestry due to slave trade. This variant, in contrast, has low prevalence in East Africa. Using race as a monolithic variable obscures the heterogeneity within a broadly-defined racial group, especially as US immigration patterns change over time.
Despite the inherent simplification of using race as a variable, the current state of the matter is that the incidence of prostate cancer, and especially high-risk prostate cancer, is higher among Blacks in the US.12 And we do not have a comprehensive understanding of the underlying genomics for this increased risk. In fact, in certain populations, self-reported Black race was a stronger predictor of PCa diagnosis compared with genetic ancestry.3 Thus, until we have a test based on genomics that may better capture ancestry, we will continue to rely on self-reported race as a surrogate to adjust the 4Kscore for the increased risk of high-grade PCa in Black men.
Incorporating this coefficient shifts the risk such that a higher number of biopsies are performed overall, and the number of biopsies avoided is lower. Thus, the risk of using this coefficient would be the overdiagnosis of low-risk prostate cancer and procedure-related risks associated with prostate biopsy in the Black population. This limitation may be offset by the increased number of clinically significant cancers found when incorporating the coefficient. Balancing these benefits and risks are not trivial and this study found that adding the race coefficient provides a more accurate prediction of high-grade prostate cancer and better clinical utility in biopsy decision making among Black men. A more sensitive screening or risk assessment regimen may in the future address the increased incidence of prostate cancer in Black patients and thus reduce downstream treatment disparities in this population.
In addition to the complexities of using race as monolithic variable, there are additional limitations of the study. In the VA study men underwent biopsy as part of a shared decision making process that may have varied across the 8 VA sites of care instead of on a standard protocol. This likely contributed to the higher PSA in the Black group. Moreover, studies have shown that Black men have higher PSAs compared with White men.6 In addition, the US military population upon which the VA study is based has a higher incidence of prostate cancer compared with the general population based on SEER studies.13 While this difference may be attributable to certain risk exposures in the military, an equally likely explanation for this difference is the higher rate of screening in this population which has more equitable access to care.14 Furthermore, incorporating the coefficient in Black patients from both cohorts still improved the calibration. Another limitation is that the available sample size did not allow for multiple iterations to optimally calibrate the model. As such, we took a pragmatic approach of prespecifying the coefficient which was accurate. The lack of central pathology review was also a limitation in this study that derived data from multiple VA centers. Lastly, we don’t have information on pre-biopsy prostate magnetic resonance imaging (MRI) which is now becoming a standard of care and often used in conjunction with biomarkers in the pre-biopsy setting.
Currently, the 4Kscore test is a widely-used biomarker to decide on the need for prostate biopsy, with approximately 75,000 tests ordered every year in clinical practice (personal communication, OPKO diagnostics). In our study, use of the race coefficient provides a more accurate prediction of cancer risk among Black men. This could improve prostate cancer detection rates in the Black population.
Conclusions
We report the independent validation of a prespecified race coefficient to improve the performance of a widely used pre-prostate biopsy risk stratification test, the 4Kscore, in Black men. Incorporation of the race coefficient into the 4Kscore algorithm maintained good discrimination and resulted in near perfect calibration in Black men, allowing for more reliable shared decision making regarding the need for a biopsy. This evidence suggests the 4Kscore test should incorporate the race coefficient. Further research should examine whether genetic markers could replace the use of self-identified race in the 4Kscore algorithm.
Supplementary Material
Funding:
This work was supported in part by the National Institutes of Health/National Cancer Institute (NIH/NCI) with a Cancer Center Support Grant to Memorial Sloan Kettering Cancer Center (P30 CA008748) and Sylvester Cancer Center (P30CA240139). SP has additional support from NIH/NCI (U01CA239141, 1R01CA272766) and Paps Corps Champions for Cancer Research.
Appendix
Table 1.
Patient characteristics of patients with 4Kscore undergoing biopsy based on race and study cohort
| Cohort by race | Cohort by study | ||||
|---|---|---|---|---|---|
| Characteristics | VA study Black men (N = 205) | Black (N = 290) | Non-Black (N = 1,088) | US Prospective Cohort (N = 1,012) | VA Cohort (N = 366) |
| Biopsy GG≥2 | 82 (40%) | 109 (38%) | 253 (23%) | 231 (23%) | 131 (36%) |
| Biopsy GG | |||||
| Negative | 70 (34%) | 114 (39%) | 578 (53%) | 542 (54%) | 150 (41%) |
| 1 | 53 (26%) | 67 (23%) | 257 (24%) | 239 (24%) | 85 (23%) |
| 2 | 36 (18%) | 49 (17%) | 118 (11%) | 108 (11%) | 59 (16%) |
| 3 | 13 (6.3%) | 21 (7.2%) | 55 (5.1%) | 59 (5.8%) | 17 (4.6%) |
| 4 | 25 (12%) | 27 (9.3%) | 43 (4.0%) | 35 (3.5%) | 35 (9.6%) |
| 5 | 8 (3.9%) | 12 (4.1%) | 37 (3.4%) | 29 (2.9%) | 20 (5.5%) |
| Age, years | 64 (59, 68) | 64 (59, 68) | 65 (60, 70) | 65 (59, 70) | 66 (61, 69) |
| Prior negative biopsy | 40 (20%) | 57 (20%) | 215 (20%) | 199 (20%) | 73 (20%) |
| 4Kscore w/o coefficient | 25% (10, 52) | 20% (7, 48) | 13% (5, 30) | 12% (5, 27) | 24% (9, 56) |
| 4Kscore w/ coefficient | 37% (17, 66) | 31% (12, 63) | 13% (5, 30) | 12% (5, 28) | 30% (12, 65) |
| Total PSA, ng/ml | 7 (5, 11) | 6.8 (4.8, 10.3) | 5.2 (3.7, 7.5) | 4.9 (3.5, 7.2) | 7.2 (5.4, 10.1) |
| Free PSA, ng/ml | 1.01 (0.66, 1.55) | 0.98 (0.65, 1.55) | 0.89 (0.60, 1.31) | 0.88 (0.59, 1.30) | 1.01 (0.68, 1.53) |
| Intact PSA, ng/ml | 0.46 (0.30, 0.71) | 0.47 (0.31, 0.75) | 0.45 (0.30, 0.67) | 0.45 (0.30, 0.67) | 0.47 (0.29, 0.71) |
| hK2, ng/ml | 0.08 (0.05, 0.12) | 0.08 (0.05, 0.12) | 0.08 (0.05, 0.13) | 0.08 (0.05, 0.12) | 0.09 (0.05, 0.13) |
| Cohort | |||||
| US Prospective Study | 85 (29%) | 927 (85%) | 1,1012 (100%) | 0 (0%) | |
| VA Study | 205 (100%) | 205 (71%) | 161 (15%) | 0 (0%) | 366 (100%) |
| Race/ethnicity | |||||
| White | 1,015 (93%) | 869 (86%) | 146 (40%) | ||
| Black | 205 (100%) | 290 (100%) | 0 (0%) | 85 (8.4%) | 205 (56%) |
| Hispanic or Latino | 39 (3.6) | 36 (3.6%) | 3 (0.8%) | ||
| Other | 34 (3.1) | 22 (2.2%) | 12 (3.3%) | ||
Abbreviations: VA, Veterans Affairs; GG, grade group; PSA, prostate-specific antigen
Categorical variables expressed as n (%), continuous variables as median (25%, 75%)
Table 2.
Race-stratified predicted probabilities and observed proportion of men with GG2-5 prostate cancer categorized by 4Kscore of the primary validation cohort (VA cohort)
| Categorized 4Kscore | ||||||
|---|---|---|---|---|---|---|
| 0-9.99% (95% CI) | 10-19.99% (95% CI) | 20-29.99% (95% CI) | 30-39.99% (95% CI) | 40-49.99% (95% CI) | >=50% (95% CI) | |
| Black | ||||||
| Biopsy Grade Group ≥2 | 3.3% (0.58%, 13%) | 18% (8.7%, 33%) | 26% (14%, 42%) | 41% (24%, 61%) | 57% (35%, 76%) | 67% (57%, 76%) |
| 4Kscore with Race | 5.4% | 15% | 25% | 35% | 45% | 77% |
| Not Black | ||||||
| Biopsy Grade Group ≥2 | 5.2% (3.4%, 7.7%) | 19% (14%, 25%) | 26% (19%, 35%) | 43% (32%, 55%) | 48% (34%, 62%) | 66% (57%, 73%) |
| 4Kscore | 4.7% | 14% | 24% | 35% | 45% | 74% |
CI: confidence interval
Table 3.
Clinical consequences of 4Kscore with and without race coefficient in the primary validation cohort (VA study)
| Gleason Grade for Delayed Dx | |||||||
|---|---|---|---|---|---|---|---|
| Biopsy Threshold | Biopsies Performed | Biopsies Avoided | High Grade Cancer Found | High Grade Dx Delayed | 2 | 3 | 4 |
| 4Kscore with Race | |||||||
| 0% | 1,000 | 0 | 400 | 0 | 0 | 0 | 0 |
| 6% | 907 | 93 | 395 | 5 | 0 | 5 | 0 |
| 9% | 849 | 151 | 395 | 5 | 0 | 5 | 0 |
| 12% | 815 | 185 | 395 | 5 | 0 | 5 | 0 |
| 15% | 771 | 229 | 390 | 10 | 5 | 5 | 0 |
| 4Kscore without Race | |||||||
| 0% | 1,000 | 0 | 400 | 0 | 0 | 0 | 0 |
| 6% | 829 | 171 | 395 | 5 | 0 | 5 | 0 |
| 9% | 766 | 234 | 385 | 15 | 10 | 5 | 0 |
| 12% | 693 | 307 | 366 | 34 | 24 | 5 | 5 |
| 15% | 629 | 371 | 346 | 54 | 34 | 5 | 15 |
Results are standardized to 1,000 patients.
Footnotes
Ethics statement: All human subjects provided written informed consent with guarantees of confidentiality
Conflicts of interest: Andrew Vickers is a co-inventor of the 4Kscore, a commercial test for predicting prostate biopsy outcome. He receives royalties from sales of the test. He owns stock options in Opko, which offers the test.
References
- 1.Zappala SM, Scardino PT, Okrongly D, et al. : Clinical Performance of the 4Kscore Test to Predict High-grade Prostate Cancer at Biopsy: A Meta-analysis of US and European Clinical Validation Study Results. Rev. Urol 2017; 19: 149–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Parekh DJ, Punnen S, Sjoberg DD, et al. : A Multi-institutional Prospective Trial in the USA Confirms that the 4Kscore Accurately Identifies Men with High-grade Prostate Cancer. Eur. Urol 2015; 68: 464–470. [DOI] [PubMed] [Google Scholar]
- 3.Nettey OS, Walker AJ, Keeter MK, et al. : Self-reported Black race predicts significant prostate cancer independent of clinical setting and clinical and socioeconomic risk factors. Urol. Oncol. Semin. Orig. Investig 2018; 36: 501.e1–501.e8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Punnen S, Freedland SJ, Polascik TJ, et al. : A Multi-Institutional Prospective Trial Confirms Noninvasive Blood Test Maintains Predictive Value in African American Men. J. Urol 2018; 199: 1459–1463. [DOI] [PubMed] [Google Scholar]
- 5.DeLong ER, DeLong DM and Clarke-Pearson DL: Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988; 44: 837. [PubMed] [Google Scholar]
- 6.Morgan TO, Jacobsen SJ, McCarthy WF, et al. : Age-Specific Reference Ranges for Serum Prostate-Specific Antigen in Black Men. N. Engl. J. Med 1996; 335: 304–310. [DOI] [PubMed] [Google Scholar]
- 7.Babajide R, Carbunaru S, Nettey OS, et al. : Performance of Prostate Health Index in Biopsy Naïve Black Men. J. Urol 2021; 205: 718–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kessler L, Watts K and Abraham N: Should We Correct the Use of Race in Urological Risk Calculators? J. Urol 2023; 209: 17–20. [DOI] [PubMed] [Google Scholar]
- 9.Darst BF, Wan P, Sheng X, et al. : A Germline Variant at 8q24 Contributes to Familial Clustering of Prostate Cancer in Men of African Ancestry. Eur. Urol 2020; 78: 316–320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jaratlerdsiri W, Chan EKF, Gong T, et al. : Whole-Genome Sequencing Reveals Elevated Tumor Mutational Burden and Initiating Driver Mutations in African Men with Treatment-Naïve, High-Risk Prostate Cancer. Cancer Res. 2018; 78: 6736–6746. [DOI] [PubMed] [Google Scholar]
- 11.Petrovics G, Price DK, Lou H, et al. : Increased frequency of germline BRCA2 mutations associates with prostate cancer metastasis in a racially diverse patient population. Prostate Cancer Prostatic Dis. 2019; 22: 406–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.DeSantis CE, Miller KD, Goding Sauer A, et al. : Cancer statistics for African Americans, 2019. CA. Cancer J. Clin 2019; 69: 211–233. [DOI] [PubMed] [Google Scholar]
- 13.Zhu K, Devesa SS, Wu H, et al. : Cancer Incidence in the U.S. Military Population: Comparison with Rates from the SEER Program. Cancer Epidemiol. Biomarkers Prev 2009; 18: 1740–1745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ross LE, Berkowitz Z and Ekwueme DU: Use of the Prostate-Specific Antigen Test among U.S. Men: Findings from the 2005 National Health Interview Survey. Cancer Epidemiol. Biomarkers Prev 2008; 17: 636–644. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.