

Abstract
Background.
Up to 50% of midlife women report sleep problems, and cardiovascular disease (CVD) is the leading cause of death in women. How chronic poor sleep exposure over decades of midlife is related to CVD risk in women is poorly understood. Among Study of Women’s Health Across the Nation (SWAN) participants whose sleep was assessed up to 16 times over 22 years, we tested whether trajectories of insomnia symptoms or sleep duration over midlife were related to subsequent CVD events.
Methods.
SWAN participants (N=2964) at baseline were aged 42–52 years, pre- or early perimenopausal, not using hormone therapy, and free of CVD. They completed up to 16 visits, including questionnaires assessing insomnia symptoms (trouble falling asleep, waking up several times a night, or waking earlier than planned, ≥3 times/week classified as insomnia), typical daily sleep duration, vasomotor symptoms (VMS), depressive symptoms; anthropometrics; phlebotomy; and CVD event ascertainment (fatal/nonfatal myocardial infarction, stroke, heart failure, revascularization). Sleep trajectories (insomnia, sleep duration) were determined via group-based trajectory modeling. Sleep trajectories were tested in relation to CVD in Cox proportional hazards models (multivariable models: site, age, race or ethnicity, education, CVD risk factors averaged over visits; additional covariates: VMS, snoring, depression).
Results.
Four trajectories of insomnia symptoms emerged: low insomnia symptoms (n=1142, 39% of women), moderate insomnia symptoms decreasing over time (n=564, 19%), low insomnia symptoms increasing over time (n=590, 20%), and high insomnia symptoms that persisted (n=668, 23%). Women with persistently high insomnia symptoms had higher CVD risk [HR=1.71(95%CI:1.19, 2.46), p=.004, vs. low insomnia, multivariable]. Three trajectories of sleep duration emerged: persistently short (~5 h: n=363, 14%), moderate (~6 h: n=1394, 55%), and moderate-long (~8 h: n=760, 30%). Women with persistent short sleep had marginally higher CVD risk [HR=1.51(95%CI: 0.98, 2.33, p=.06, vs. moderate, multivariable]. Women who had both persistent high insomnia and short sleep had significantly elevated CVD risk [HR=1.75(95%CI: 1.03, 2.98) p=.04, vs. low insomnia/moderate or moderate-long sleep duration, multivariable]. Relations of insomnia to CVD persisted adjusting for VMS, snoring, or depression.
Conclusion.
Insomnia symptoms, when persistent over midlife and/or occurring with short sleep, are associated with higher CVD risk among women.
Keywords: sleep, cardiovascular disease, heart disease, stroke, insomnia, menopause, women
Introduction
Cardiovascular disease (CVD) is the leading cause of death in women, and approximately 30% of women will die from some form of CVD.1,2 Further, poor sleep is a major health issue for women, with women at higher risk of poorer sleep quality and insomnia disorders relative to men.3–5 Midlife, often as defined as ages 40–656 and which includes the menopause transition for women, is a critical time for both cardiovascular health and sleep. For women, midlife is often a time of accelerated accumulation of underlying vascular risk beyond the effects of aging alone.7–9 Further, midlife is a time when sleep problems become evident: up to 40–50% of women report problems with sleep at midlife.10,11
Insufficient sleep has been associated with elevated CVD risk, with the importance of sleep to cardiovascular health underscored by its recent inclusion in the American Heart Association’s Life’s Essential 8.12 Meta-analyses indicate that poor subjective sleep quality, elevated insomnia symptoms, and extreme sleep duration (i.e., short or long) are each associated with an elevated risk of CVD events.13–16 However, sleep in these studies is typically assessed only once and considered in relation to CVD events over the subsequent years. Habitual sleep patterns can change over time, particularly with aging,17 and a single assessment fails to adequately capture the patterns of or chronicity of exposure to poor sleep that may be most relevant for cardiovascular health. One notable exception is a study that examined sleep duration three times over four years and found that individuals with chronically short sleep duration were most at risk for cardiovascular events (atrial fibrillation, myocardial infarction (MI), stroke) over the subsequent 6–7 years.18 However, this study was restricted to only sleep duration, did not evaluate insomnia symptoms, implemented only three sleep assessments over four years, and had a limited follow-up period. No studies have characterized trajectories of sleep over the decades of midlife in relation to subsequent CVD events, and none have considered these associations in a racially and ethnically diverse sample of adults living in the United States.
Using data from the Study of Women’s Health Across the Nation (SWAN), a study of 3320 women whose sleep was assessed up to 16 times over 22 years during midlife, we tested how the trajectories of insomnia symptoms and sleep duration over midlife were related to subsequent incident CVD events. We considered both insomnia symptoms and sleep duration as these two sleep features have been associated with CVD risk in prior work,12–18 hypothesizing that persistent insomnia symptoms and short sleep duration would each be related to CVD risk. We also considered these sleep features together, hypothesizing that the group at greatest CVD risk would be those women who had both persistent insomnia symptoms and short sleep duration, given prior evidence that this group may be at particular risk.19 We considered associations between sleep and CVD controlling for a range of potentially confounding factors, including demographic factors, CVD risk factors, depressive symptoms, snoring, and vasomotor symptoms, which can disrupt sleep and have been associated with CVD risk in other work.20,21 Finally, as SWAN included women across five different racial and ethnic groups; racial and ethnic differences in associations between sleep and CVD were considered.
Methods
SWAN is a prospective cohort study of women conducted at seven sites in the United States (Boston, Massachusetts; Chicago, Illinois; southeast Michigan; Los Angeles, California; Newark, New Jersey; Pittsburgh, Pennsylvania; and Oakland, California).22 Each site recruited non-Hispanic White women and one racial and ethnic minority group (Black, Chinese, Hispanic, Japanese). Women were recruited from lists of names or household addresses. Select sites supplemented primary sampling frames to obtain adequate numbers of racial/ethnic minority women. Baseline eligibility criteria included being aged 42–52 years, having a uterus and at least one ovary, not being pregnant or lactating, not using oral contraceptives/hormone therapy, and having at least one menstrual cycle in the prior 3 months. Clinic assessments began in 1996–1997 and were repeated approximately annually. Protocols were approved by the institutional review boards at each site. Each participant provided written informed consent at each visit.
SWAN provides access to public use datasets that include data from SWAN screening, the baseline visit and follow-up visits (https://agingresearchbiobank.nia.nih.gov/). To preserve participant confidentiality, some, but not all, of the data used for this manuscript are contained in the public use datasets. A link to the public use datasets is also located on the SWAN web site: http://www.swanstudy.org/swan-research/data-access/. Investigators who require assistance accessing the public use dataset may contact the SWAN Coordinating Center at the following email address: swanaccess@edc.pitt.edu.
A total of 3302 women were enrolled in the SWAN cohort. For the current analyses, 92 women were excluded due to a reported history of CVD at baseline, n=190 were excluded as they did not return for any follow-up visits, n=30 were excluded due to missing data (n=4 missing data on CVD events, n=26 missing education), and n=26 were excluded due to sleep assessment completed at only one visit (precluding analysis of trajectories). This resulted in an analysis sample of N=2964 for primary insomnia symptom models. Sleep duration assessments began at SWAN visit 3. Therefore, an additional 447 women who dropped out before visit 3, had a CVD event before visit 3, or had no or inadequate sleep duration data (e.g., at only one time point) were excluded from models that included sleep duration trajectories, yielding N=2517 for these models. Consistent with exclusions, women not included in this analysis relative to those who were in the analysis were more often African American or Hispanic (relative to White), had lower education, and had a more adverse CVD risk factor profile (p’s<.0001).
Measures
Sleep
Insomnia symptoms.
At each visit, participants reported the frequency of sleep problems over the prior 2 weeks: trouble falling asleep, waking up several times a night, and waking up earlier than planned and unable to fall asleep again. Each of these responses was dichotomized as no/infrequent (≤2 times per week) or yes (≥3 times per week), consistent with prior SWAN work23,24 and DSM-5 criteria for insomnia.25 We characterized the trajectories of insomnia symptoms (≥1 sleep problem occurring ≥3 times per week vs. not) across up to 16 SWAN visits.
Sleep duration.
At four of the follow-up assessments (visits 3, 4, 12, and 13, conducted in 1999–2001, 2000–2002, 2009–2011, and 2011–2013, respectively), participants reported their typical daily sleep duration over the past month. We considered the trajectories of sleep duration over four visits, consistent with prior SWAN work.26 Further, for analyses of time-varying sleep duration, sleep was categorized as ≤5 hours, >5 to <8 hours, and ≥8 hours.
CVD events / CVD mortality
At each SWAN visit, participants reported the occurrence of CVD events [MI, cerebral vascular incident/stroke (CVA), heart failure, revascularization procedures (percutaneous coronary intervention, coronary artery bypass grafting)]. More extensive information about CVD events was obtained at SWAN visits 12, 13, and 15, and adjudication of events began at visit 15. Women were asked to provide consent to obtain medical record information, and attempts were made to obtain medical records for each CVD event. When medical records were obtained, the SWAN Coordinating Center assembled information for each event (e.g., admission history, physical exam, discharge summary, laboratory data, diagnostic test results, operative/procedure reports). Two cardiologist reviewers blinded to sleep information reviewed this information independently and returned their determination of the event status (yes, no, or indeterminate). If there was agreement between the two reviewers, the case was considered complete. If there was disagreement, a third cardiologist resolved the difference. For participants with multiple events, the first event was used.
The women in this analysis reported 179 nonfatal CVD events (MI: n=62; CVA: n=80; revascularization/percutaneous coronary intervention: n=46; heart failure: n=22; multiple events simultaneously: n=22). Of these events, 60 were confirmed through adjudication. In addition to non-fatal events, fatal CVD events were identified via systematic review of death certificates beginning at SWAN visit 15. CVD-related deaths were defined based on whether CVD was listed as an underlying cause of death on the death certificate (n=23). The primary outcome was the first non-fatal CVD event (MI, stroke, heart failure, revascularization) or fatal CVD event, which included 202 events (179 non-fatal events, 23 fatal CVD events). We additionally considered fatal/nonfatal CVA or MI/revascularization/percutaneous coronary intervention separately (the two event types with adequate numbers for analysis).
Covariates
Race and ethnicity and education (high school or less, some college/vocational, college or higher) were reported at baseline via standardized questionnaires. At each visit, age and smoking (current vs. past/never) were derived from questionnaires and clinical interviews and height, weight and blood pressure were measured. Body mass index was calculated (kg/m2) and the average of two seated measurements for systolic blood pressure and diastolic blood pressure were computed. Depressive symptoms were assessed at each visit via the Center for Epidemiologic Studies Depression scale, which was categorized according to its clinical cutpoint (≥16 indicating elevated depressive symptoms).27 Vasomotor symptoms (VMS) were assessed via a standard questionnaire, which assessed how often participants experienced hot flashes and night sweats in the past two weeks (response options: not at all, 1–5 days, 6–8 days, 9–13 days, every day); women with a response of ≥6 days/two weeks were considered to have VMS, given the relevance of this threshold to CVD in prior work.20 Symptoms of snoring (not during past month, <once/week, 1–2 times/week, ≥3 times/week, categorized as any versus no snoring in the past month) were assessed at visit 4. At visit 15, current nightshift work and prior nightshift work (of a duration of at least 3 years) were assessed via questionnaire. At each visit, medication use was ascertained by self-report and confirmed via visual inspection of pill bottles. The therapeutic class and subclass for each medication was coded according to the Iowa Drug Information System.28 Insomnia medications were classified based upon the American Academy of Sleep Medicine Clinical Practice Guideline.29
Phlebotomy was performed at each visit following overnight fasting during the early follicular phase (days 2–5 of the menstrual cycle), with blood separated, frozen at −20°C, and sent on dry ice to Medical Research Laboratories (Highland Heights, KY). For baseline through visit 7, total cholesterol and triglyceride concentrations were determined by enzymatic methods (Hitachi 747 analyzer; Boehringer Mannheim Diagnostics, Indianapolis, IN). High-density lipoprotein cholesterol (HDL-C) was quantitated following precipitation of low-density lipoprotein cholesterol (LDL-C) with heparin and manganese chloride by the modified Lipid Research Clinics procedure. Cholesterol in the supernate was measured by an automated cholesterol oxidase assay on a Hitachi 747–200 clinical analyzer using RAICHEM reagents.30,31 For subsequent visits, ADVIA assay methods were used for total cholesterol, triglycerides, and HDL.32,33 Calibration of lipid assays was based on 340 samples selected to be representative of the SWAN cohort. LDL-C was calculated by the Friedewald equation,34 and values of estimated LDL-C and triglycerides were set to missing when the triglycerides were >400mg/dl. Glucose was measured in serum by automated enzymatic assay on a Hitachi 747–200 chemistry analyzer using the hexokinase reaction and Roche Diagnostic reagents (baseline through visit 7) or by the ADVIA Chemistry Glucose Hexokinase 3 Concentrated Reagents32 (subsequent visits). Diabetes was identified by one or more of the following: (1) use of a glucose-lowering medication; (2) fasting glucose ≥7 mmol/l on two consecutive visits while not on steroids; (3) two visits with self-reported diabetes and at least one visit with fasting blood glucose ≥7 mmol/l. The atherosclerotic cardiovascular disease (ASCVD) risk score, which provides an estimate of 10-year risk of clinical CVD based upon risk factor levels (age; race; sex; systolic and diastolic blood pressure; total, LDL, and HDL cholesterol; diabetes; smoking; and statin, aspirin, and hypertension medication use), was calculated according to published guidelines.35
Data Analyses
All study variables were examined for distributions, cell sizes, and outliers. Differences between included and excluded women were determined via t-tests and chi-squared tests. To identify trajectory patterns of insomnia symptoms and sleep duration over the study, we used group-based trajectory modeling (GBTM),36 an application of finite mixture modeling designed to identify clusters of individuals following similar progressions of a feature over time.36–39 The selection of the number of trajectories was determined following published methods.38 We first considered two, three, four, or five trajectories for each sleep feature (insomnia symptoms, duration); using the Bayes Information Criterion, sample size considerations, scientific plausibility, and the prior SWAN literature23,26, we identified four trajectory groups for insomnia symptoms and three trajectory groups for sleep duration. Notably, only sleep information obtained prior to CVD events was included in the trajectories. The four insomnia symptom trajectory groups were next considered in relation to incident CVD in Cox proportional hazards models. A parallel analysis was conducted for sleep duration and incident CVD. We subsequently classified all participants as falling into the insomnia symptom and sleep duration groups in combination (e.g., short sleep and high insomnia symptoms, moderate or moderate-long sleep and high insomnia symptoms, etc.), yielding four groups; we then considered these groups in relation to incident fatal or non-fatal CVD in Cox proportional hazard models. Women were censored at the time of the first CVD event, dropout, or death from non-CVD causes. Covariates, entered into the Cox model, were site, race and ethnicity, baseline education, age, and in a separate step, ASCVD risk score. For continuous variables, the mean value across the observed follow-up visits was used, and for categorical variables (with the exception of race and ethnicity, education, and snoring, which were obtained at only one visit), the proportion of visits scoring positive for that variable. Secondary models considered the additional covariates of elevated depressive symptoms, frequent VMS, snoring, sleep medication use, and nightshift work. Interactions between insomnia symptom or sleep duration trajectories and race and ethnicity were tested. Sensitivity analyses were restricted to adjudicated CVD events. We also considered fatal/nonfatal CVA or MI/revascularization as two separate outcomes. In additional sensitivity analyses, we considered an alternate referent for sleep duration models (the moderate-high trajectory group); insomnia symptoms and sleep duration each as time-varying predictors in relation to CVD events; and insomnia symptoms or sleep duration trajectories with the posterior probabilities of group membership applied as weights in relation to CVD events in Cox proportional hazards models. Proportional hazards assumptions were met for all models. Analyses were performed with SAS v9.4 (SAS, Cary, NC).
Results
At baseline, participants were on average 46 years of age and had obtained a college education or higher (Table 1). The participants at baseline reported sleeping an average of 6.55 hours per night and over 30% had insomnia symptoms. The median follow-up time was 19.15 years (range: 0.08–21.86 years). During follow-up, there were 202 fatal or non-fatal CVD events.
Table 1.
Participant characteristics at baseline: The Study of Women’s Health Across the Nation (SWAN) (N=2964)
| Age, years, M (SD) | 45.86 (2.69) |
| Race/Ethnicity, N (%) | |
| Black | 817 (27.56) |
| White | 1421 (47.94) |
| Chinese | 241 (8.13) |
| Japanese | 274 (9.24) |
| Hispanic | 211 (7.12) |
| Education, N (%) | |
| High school or less | 691 (23.31) |
| Vocational/some college | 955 (32.22) |
| College or higher | 1318 (44.47) |
| BMI, kg/m2, M (SD) | 28.08 (7.21) |
| ASCVD risk score, M (SD) | 0.02 (0.03) |
| VMS, frequent, N (%) | 307 (10.41) |
| Depressive symptoms, high, N (%) | 689 (23.27) |
| Snoring, yes, N (%)* | 627 (25.78) |
| Sleep duration, hours, M (SD)† | 6.55 (1.21) |
| Trouble falling asleep (≥3/wk), N (%) | 288 (9.75) |
| Waking several times a night (≥3/wk), N (%) | 747 (25.32) |
| Wake up early (≥3/wk), N (%) | 356 (12.06) |
| Any insomnia symptom (≥3/wk), N (%) | 894 (30.28) |
assessed at SWAN visit 3
assessed at SWAN visit 4
BMI=body mass index; ASCVD=atherosclerotic cardiovascular disease; VMS=vasomotor symptoms
Four trajectories of insomnia symptoms emerged: persistent low insomnia symptoms (n=1142, 38.5%), moderate insomnia symptoms that declined over time (n=564, 19.0%), low insomnia symptoms that increased over time (n=590, 19.9%), and persistently high insomnia symptoms (n=668, 22.6%) over midlife (Figure 1). When insomnia trajectories were considered in relation to incident CVD events, women in the persistently high insomnia symptom trajectory had significantly higher risk for CVD (Table 2, Figure 2); associations persisted when adjusting for the ASCVD risk score.
Figure 1.
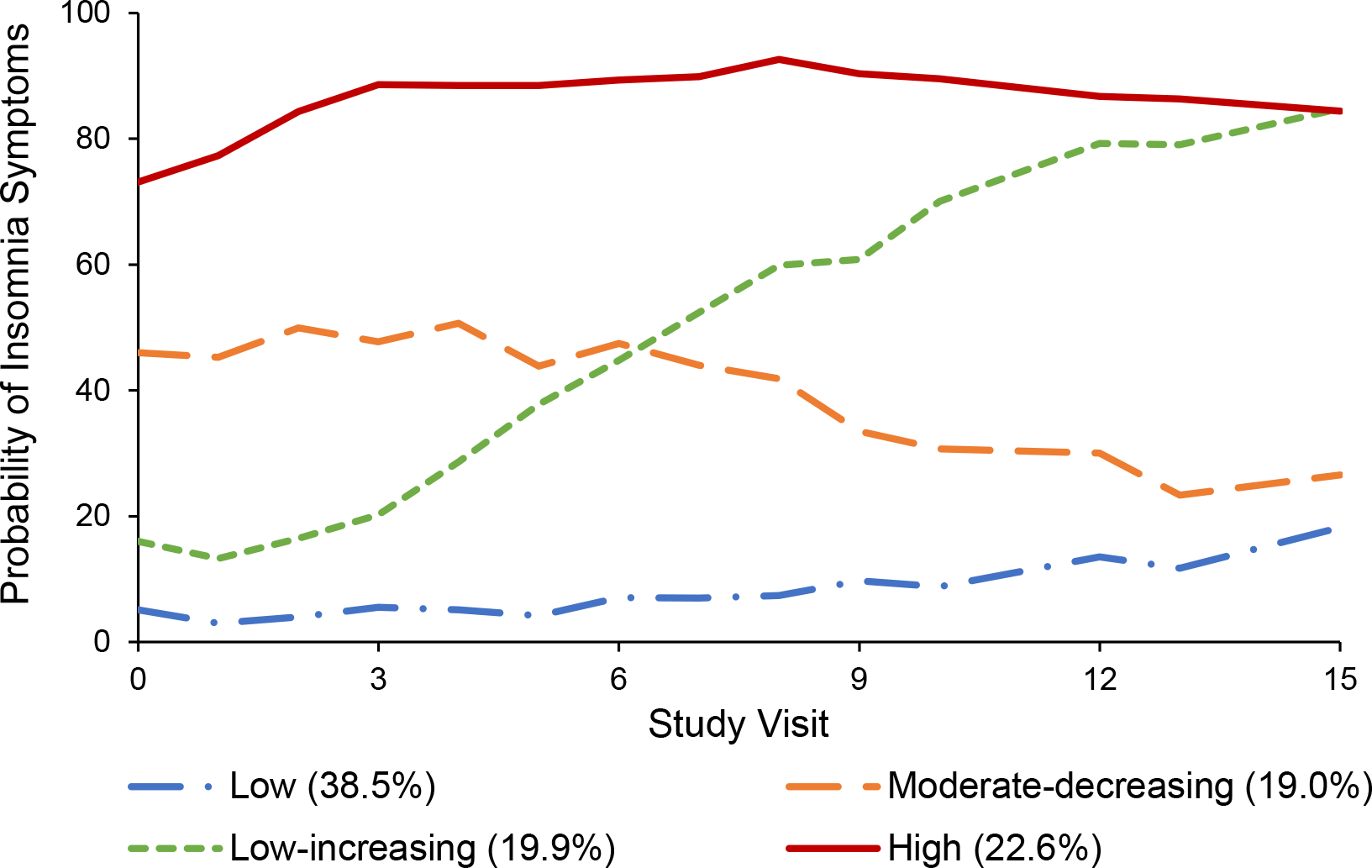
Insomnia symptom trajectories
Table 2.
Relationship between insomnia symptom trajectories and incident CVD over up to 22 years of follow up
| CVD |
||
|---|---|---|
| Model 1 | Model 2 | |
| HR (95% CI) | HR (95% CI) | |
|
| ||
| Low insomnia symptoms | (referent) | (referent) |
| Moderate-decreasing insomnia symptoms | 1.40 (0.93, 2.12) | 1.32 (0.87, 2.00) |
| Low-increasing insomnia symptoms | 1.10 (0.73, 1.67) | 1.10 (0.73, 1.68) |
| High insomnia symptoms | 1.90 (1.33, 2.71)** | 1.71 (1.19, 2.46)** |
Model 1: N=2964; Model 2: N=2960
p<.05
p<.01
Model 1: Adjusted for site, age, race/ethnicity, education
Model 2: Model 1 + atherosclerotic cardiovascular disease risk score
CVD = cardiovascular disease
Figure 2.
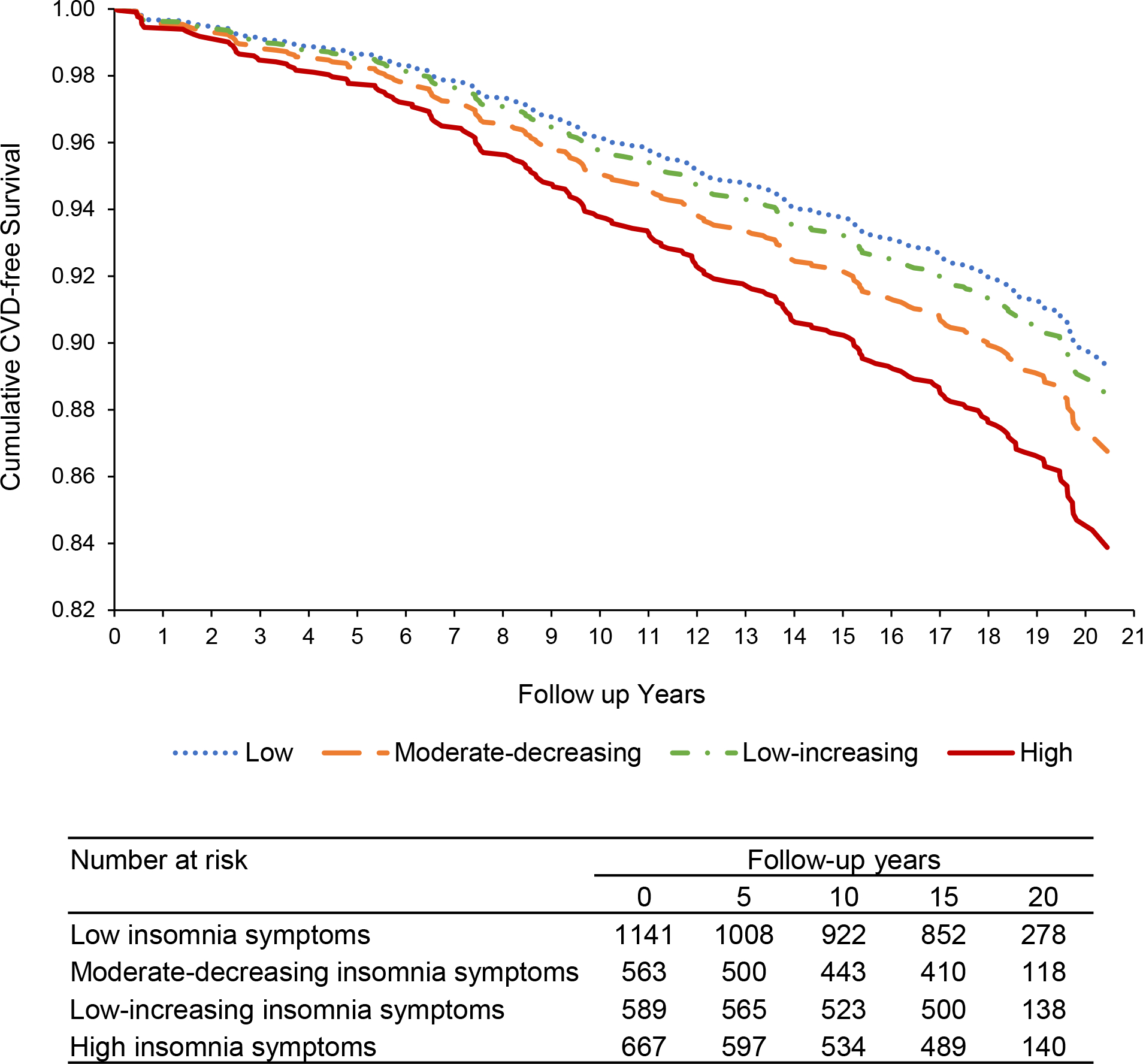
Relationship of trajectories of insomnia symptoms to incident CVD events (adjusted for site, age, race/ethnicity, education, ASCVD risk score)
We next considered sleep duration trajectories. Three trajectories of sleep duration emerged: persistently short (approximately 4.85 h/night: n=363, 14.4%), persistently moderate (approximately 6.39 h/night: n=1394, 55.4%), and persistently moderate to long (approximately 7.70 h/night: n=760, 30.2%) sleep duration (Figure S1). When these three sleep duration trajectories were considered in relation to incident CVD events, women in the persistently short sleep duration trajectory had significantly higher risk for CVD (Table 3, Figure 3). Associations were somewhat weakened when further adjusting for the ASCVD risk score.
Table 3.
Relationship between sleep duration trajectories and incident CVD events over up to 22 years of follow up
| CVD |
||
|---|---|---|
| Model 1 | Model 2 | |
| HR (95% CI) | HR (95% CI) | |
|
| ||
| Short sleep duration | 1.72 (1.13, 2.62)* | 1.51 (0.98, 2.33)† |
| Moderate sleep duration | (referent) | (referent) |
| Moderate-long sleep duration | 1.13 (0.75, 1.71) | 1.16 (0.76, 1.77) |
Model 1: N=2517; Model 2: N=2434
p<.10
p<.05
Model 1: Adjusted for site, age, race/ethnicity, education
Model 2: Model 1 + atherosclerotic cardiovascular disease risk score
CVD = cardiovascular disease
Figure 3.
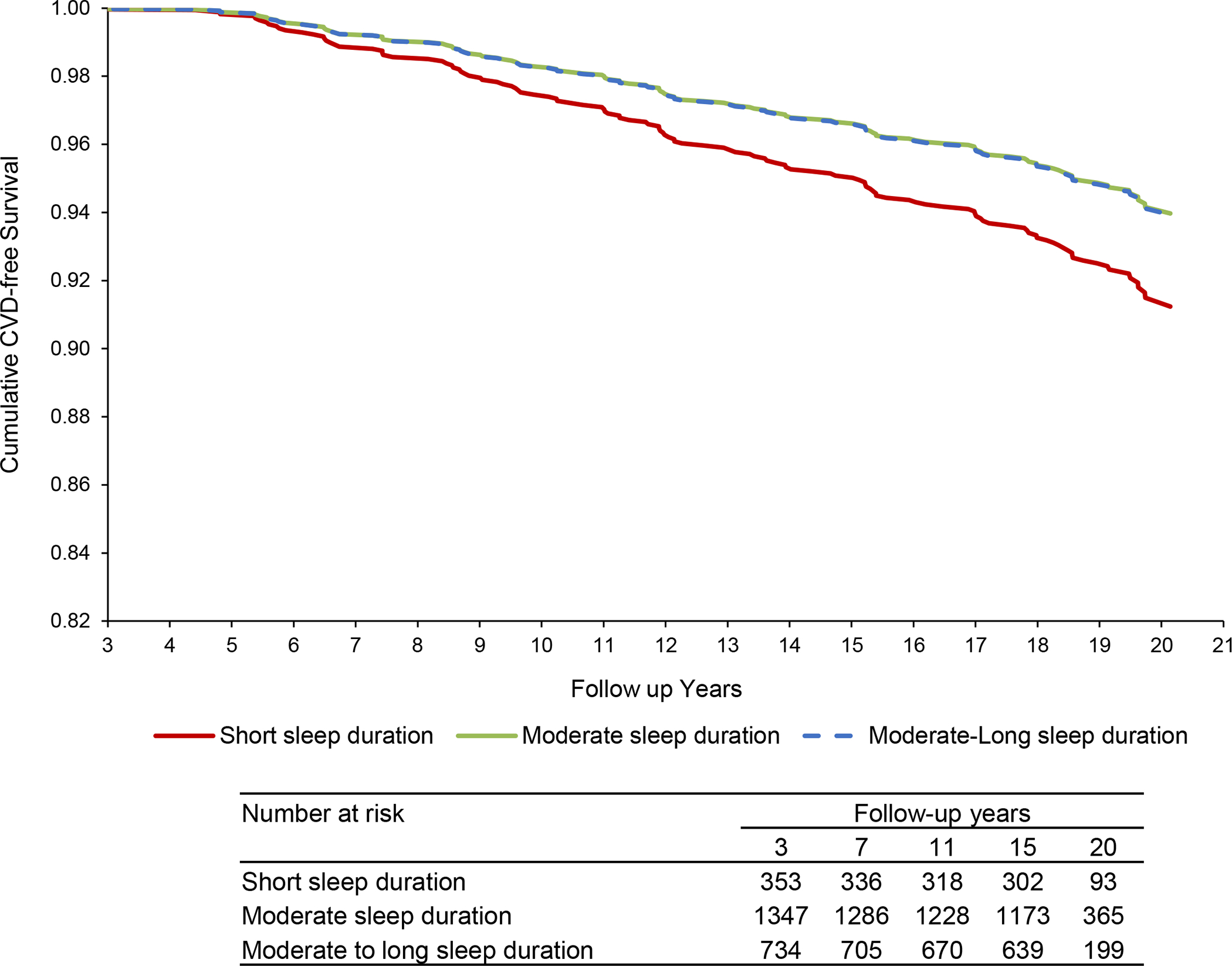
Relationship of sleep duration trajectories to CVD (adjusted for site, age, race/ethnicity, education, ASCVD risk score)
We next considered insomnia symptom and sleep duration trajectories in combination: 6.5% of women (n=164) fell into the trajectory of persistent high insomnia symptoms as well as into the trajectory of short sleep duration, 15.5% (n=390) into the trajectory of persistent high insomnia symptoms with moderate or moderate-long sleep duration, 7.9% (n=199) into the trajectory of low, moderate-decreasing, or low-increasing insomnia symptoms with short sleep duration, and 70.1% (n=1764) into the trajectory of low, moderate-decreasing, or low-increasing insomnia symptoms with moderate or moderate-long sleep duration (Figure S2). When considering these four groups in relation to CVD, while women in either of the two groups that included women with persistent high insomnia symptoms had significantly elevated risk of CVD, those in the trajectory of high insomnia symptoms in combination with short sleep duration had the highest CVD risk (Table 4; Figure 4).
Table 4.
Relationship between combined insomnia symptom-sleep duration trajectories and incident CVD events
| CVD |
||
|---|---|---|
| Model 1 | Model 2 | |
| HR (95% CI) | HR (95% CI) | |
|
| ||
| Low, moderate-decreasing, or low-increasing insomnia symptoms + moderate or moderate-long sleep duration | (referent) | (referent) |
| Low, moderate-decreasing, or low-increasing insomnia symptoms + short sleep duration | 1.70 (1.01, 2.87)* | 1.45 (0.84, 2.50) |
| High insomnia symptoms + moderate or moderate-long sleep duration | 1.80 (1.15, 2.83)* | 1.70 (1.06, 2.72)* |
| High insomnia symptoms + short sleep duration | 2.01 (1.19, 3.40)** | 1.75 (1.03, 2.98)* |
Model 1: N=2517; Model 2: N=2434
p<.05
p<.01
Model 1: Adjusted for site, age, race/ethnicity, education
Model 2: Model 1 + atherosclerotic cardiovascular disease risk score
CVD = cardiovascular disease
Figure 4.
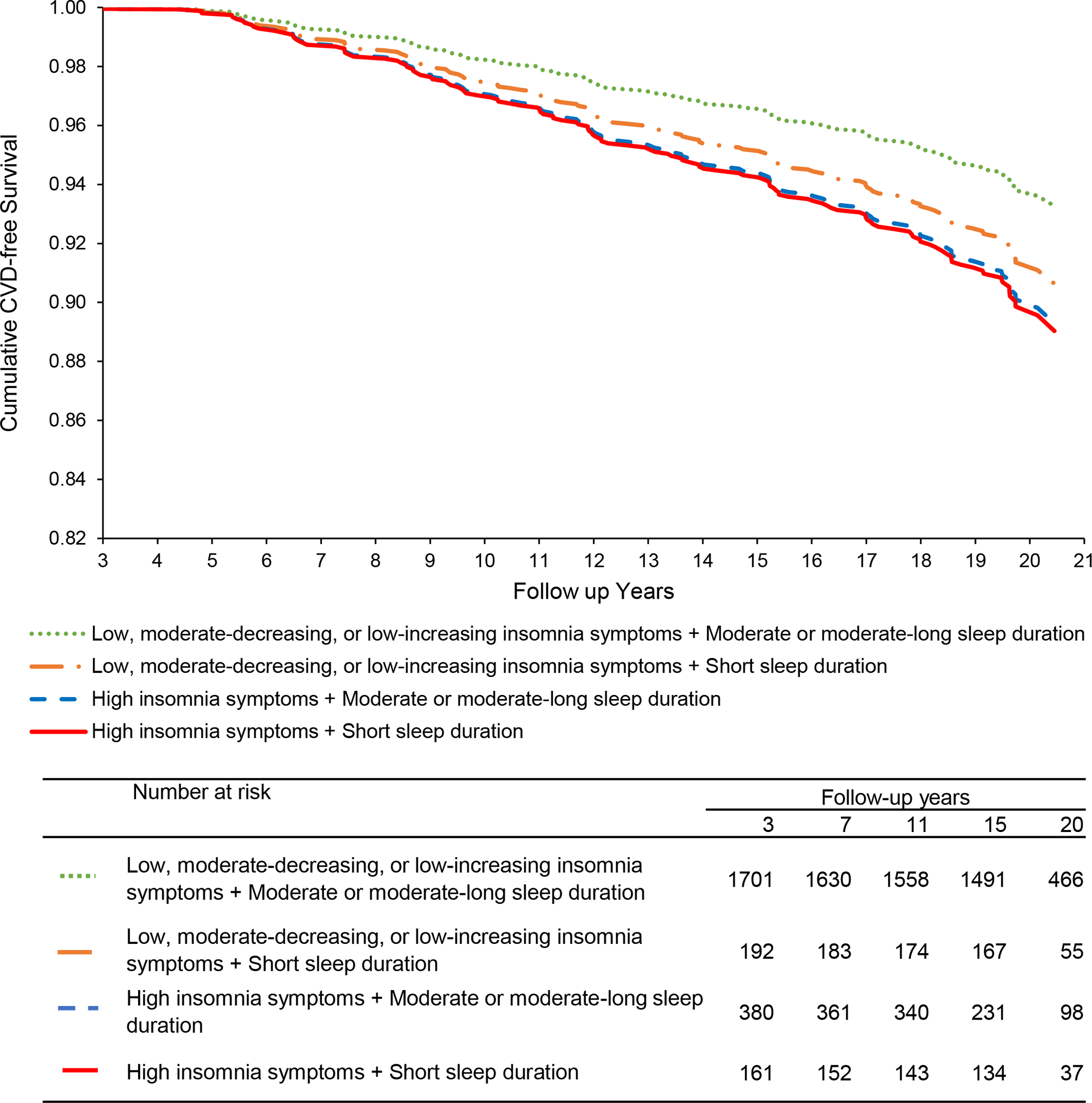
Relationship of combined insomnia symptom – sleep duration trajectories to CVD (adjusted for site, age, race/ethnicity, education, ASCVD risk score)
We conducted several additional analyses. We evaluated additional covariates (elevated depressive symptoms, frequent VMS, snoring, sleep medication use, shift work history) in models. Associations of insomnia symptom trajectories to CVD (Table S1), but not sleep duration or combined insomnia symptom-sleep duration trajectories (data not shown) in relation to CVD, persisted with additional adjustment for these covariates. We considered interactions between sleep trajectories by race and ethnicity in relation to CVD, and no statistically significant interactions were observed (each interaction p>.51; models adjusted for site, age, education, ASCVD risk score). We evaluated models restricted to adjudicated CVD events; findings were broadly consistent with the primary models [e.g., for insomnia symptoms: persistent high insomnia symptoms relative to low: HR (95%CI)=1.70 (0.96, 3.02), p=0.069; e.g., for sleep duration: persistent short duration relative to moderate: HR (95%CI)=1.87 (1.00, 3.49), p=0.050, adjusted for site, age, education, and the ASCVD risk score], although statistical significance somewhat weakened likely due to more limited numbers of events. We conducted models considering sleep trajectories in relation to fatal or nonfatal CVA and MI or revascularization separately (the two types of events in which there were adequate numbers to model); there was indication of particularly strong associations of insomnia symptoms to CVA (Tables S2a–b). We considered an alternate referent for sleep duration models (the moderate-long trajectory group), which showed findings broadly similar to primary models, although somewhat weakened (Table S3). We also considered insomnia symptoms or sleep duration trajectories with the posterior probabilities of group membership applied as weights in Cox proportional hazards models; results were consistent with primary models (Tables S4a–b). Finally, instead of modeling sleep as trajectories, we considered time-varying insomnia symptoms and time-varying sleep duration in relation to incident CVD; elevated insomnia symptoms (≥3/week) and short sleep duration (≤5 hours/night) were each associated with significantly higher risk for CVD events (Tables S5a–b).
Discussion
This study characterized the trajectories of insomnia symptoms and sleep duration over midlife and their relationship to incident CVD events in a large sample of women followed for up to two decades. Findings indicate that almost one-quarter of the women (23%) follow a trajectory of persistent insomnia symptoms over midlife and 14% of women report persistently short sleep duration over midlife. Approximately 7% of women follow a pattern of both persistent insomnia symptoms and short sleep duration over midlife. Persistent insomnia symptoms and, to a lesser extent, short sleep duration, were each associated with significantly elevated risk for subsequent CVD events. Associations between insomnia symptoms and CVD were not explained by CVD risk factors, nor were they explained by depressive symptoms, VMS, or snoring. Finally, women with both persistent insomnia symptoms and short sleep duration over midlife had a doubling of risk of CVD events. Collectively, this work underscores the high likelihood of poor sleep over midlife for women as well as its implications for their cardiovascular health as they age.
A major strength of this study was the ability to characterize trajectories of sleep based on up to 16 assessments over the course of two decades during midlife. Most prior work on the association of sleep to CVD risk has examined sleep at only one timepoint, an approach that does not adequately capture the chronicity of exposure to poor sleep. One exception is a study that considered trajectories of sleep sampled at three time points over four years in relation to cardiovascular events assessed over seven years.18 Thus, the present study is the first to characterize sleep over the full span of midlife as well as to include an extended follow-up period to characterize subsequent CVD events. This extended follow up time is critical given the older age at which women typically experience their first ASCVD event.40 This study underscores the importance of the chronicity of poor sleep for its implications for CVD risk.
Another strength of this study was the ability to consider both insomnia symptoms and sleep duration. Most studies consider only one dimension of sleep; for example, the only other study to consider sleep trajectories in relation to CVD examined only sleep duration. Other work has suggested the potential importance of the combined phenotype of insomnia and short sleep duration for women’s CVD risk,19 yet sleep was assessed only once. Other work with older women has called into question the importance of this combined phenotype.41 In the present work considering trajectories of sleep duration and insomnia symptoms over midlife, we found that women with the combined phenotype had a doubling of the risk of subsequent CVD in minimally adjusted models, and a 75% increased risk of CVD even after adjustment for CVD risk factors.
We considered a range of potential confounders and mechanisms. In models adjusted for age, site, race/ethnicity, and education, persistent insomnia symptoms and short sleep duration were each associated with greater risk of CVD. Only the association for insomnia trajectories persisted after adjusting for CVD risk factors, as well as for a range of potentially confounding factors (e.g., snoring, sleep medication use, shift work). One methodologic consideration in comparing findings between sleep duration and insomnia symptoms is that sleep duration assessments began later (visit 3 versus baseline, respectively) and occurred less frequently during follow-up (i.e., four versus 16 assessments, respectively) than did assessments for insomnia symptoms. Thus, insomnia symptoms may have been more precisely characterized than sleep duration, and models of insomnia symptoms had a somewhat larger sample size than the sleep duration models. However, our data do suggest the particular importance of insomnia symptoms for women’s cardiovascular health as they age.
This study is unique in its ability to consider these relationships across five racial/ethnic groups of women (Black, Chinese, Hispanic, Japanese, White), suggesting a consistency of associations between sleep and CVD risk across these diverse groups of women. Poor sleep, and particularly insomnia symptoms that persist over years,4 is over-represented in women relative to men,3,5 and sleep is also often worsening10 and vascular risk accumulating7,8 in an accelerated fashion over midlife and the menopause transition in women. Moreover, the menopause transition is a time of unique symptoms, such as VMS, that have implications for both women’s sleep and cardiovascular health20,21 that we were able to consider here.
Several mechanisms may explain the relationship between sleep characteristics and CVD. First, sleep problems have been associated with adverse CVD risk factors, such as hypertension and insulin resistance.42 Adjustment for CVD risk factors partially explained the association of sleep duration with CVD but did not attenuate the association to CVD we observed for insomnia symptoms. Thus, the relationship of short sleep duration, but not insomnia, on the development of clinical CVD might be partially explained by adverse CVD risk factors. Further, women at midlife often have VMS, which can disrupt sleep and which we previously associated with CVD in this cohort;20 however, associations between sleep and CVD persisted when adjusting for these symptoms. Further, sleep problems can be a feature of depression, which is related to CVD risk,43 yet associations between insomnia symptoms and CVD persisted when adjusting for elevated depressive symptoms. Moreover, we considered the role of snoring, the cardinal symptom of sleep apnea, and the associations for insomnia symptoms with CVD persisted. Other physiologic mechanisms not assessed here, such as alterations in the hypothalamic-pituitary-adrenal axis, autonomic nervous system changes, or epigenetic changes, warrant consideration in future work.44
In exploratory models, we considered the association of insomnia symptoms or sleep duration in relation to CVA or MI/revascularization considered separately. We observed particularly strong associations of insomnia symptoms with CVA, and suggestive links between short or moderate-long sleep duration and MI/revascularization. Some prior work provides suggestive evidence of particularly strong relationships of insomnia symptoms to stroke risk.45 These secondary models must be regarded with caution given their exploratory nature and limited number of specific event types. However, these data suggest the particular relevance of insomnia to stroke risk in women.
There are several limitations to this work. The sleep dimensions considered here were obtained via self-report. Self-reported sleep characteristics correlate only moderately with sleep obtained via polysomnography or other objective means.46 However, self-reported sleep is highly clinically relevant; for example, clinical insomnia diagnoses are based upon self-reported sleep. The moderate-long sleep duration trajectory group, determined empirically, averaged approximately 7.70 hours of sleep; the low prevalence of long sleep duration in this sample may have limited our ability to make conclusions about long sleep duration. Models considering the referent of the longer sleep duration group were broadly similar to primary models, although associations somewhat attenuated. Further, the moderate sleep duration trajectory group had somewhat shorter sleep (6.4 hours) than that recommended as optimal for cardiovascular health among adults.47 We considered insomnia symptoms and sleep duration but not other features of sleep (e.g., timing, regularity, efficiency) that warrant consideration in future work. Primary analyses considered self-reported CVD outcomes, yet additional analyses considered adjudicated CVD events and yielded broadly similar effect sizes. Snoring was used as a symptom for sleep apnea, and some misclassification might have occurred.48
In summary, in this study of midlife women followed over two decades, following a trajectory of persistent insomnia symptoms, alone and when accompanied by a trajectory of short sleep duration, was associated with a 70–75% increased risk of CVD over up to two decades of follow-up, after considering demographics and CVD risk factors. These findings point to the importance of considering sleep when conducting women’s CVD risk assessment and underscore the importance of chronic exposure to poor sleep for its cardiovascular implications.
Supplementary Material
Clinical Perspective:
What Is New?
Midlife, which includes the menopause transition, is a time of vulnerability to poor sleep as well as of degrading cardiovascular health for many women.
This study is the first to demonstrate that a trajectory of chronic insomnia symptoms over two decades of midlife is associated with elevated risk for CVD events later in life in women. The impact of these insomnia symptoms on CVD risk is most pronounced among women who also have chronically short sleep duration.
The relationships of insomnia symptoms to women’s cardiovascular health are not explained by CVD risk factors, sleep apnea symptoms, mood, or vasomotor symptoms.
What Are the Clinical Implications?
Insomnia symptoms and short sleep duration are common issues facing midlife women.
These findings underscore the importance of sleep problems over midlife to women’s cardiovascular health later in life.
Study findings further point to the importance of treating sleep problems to reducing women’s CVD risk as they age.
Acknowledgements
Clinical Centers: University of Michigan, Ann Arbor – Carrie Karvonen-Gutierrez, PI 2021 – present, Siobán Harlow, PI 2011 – 2021, MaryFran Sowers, PI 1994–2011; Massachusetts General Hospital, Boston, MA – Sherri-Ann Burnett-Bowie, PI 2020 – Present; Joel Finkelstein, PI 1999 – 2020; Robert Neer, PI 1994 – 1999; Rush University, Rush University Medical Center, Chicago, IL – Imke Janssen, PI 2020 – Present; Howard Kravitz, PI 2009 – 2020; Lynda Powell, PI 1994 – 2009; University of California, Davis/Kaiser – Elaine Waetjen and Monique Hedderson, PIs 2020 – Present; Ellen Gold, PI 1994 – 2020; University of California, Los Angeles – Arun Karlamangla, PI 2020 – Present; Gail Greendale, PI 1994 – 2020; Albert Einstein College of Medicine, Bronx, NY – Carol Derby, PI 2011 – present, Rachel Wildman, PI 2010 – 2011; Nanette Santoro, PI 2004 – 2010; University of Medicine and Dentistry – New Jersey Medical School, Newark – Gerson Weiss, PI 1994 – 2004; and the University of Pittsburgh, Pittsburgh, PA – Rebecca Thurston, PI 2020 – Present; Karen Matthews, PI 1994 – 2020.
NIH Program Office: National Institute on Aging, Bethesda, MD – Rosaly Correa-de-Araujo 2020 - present; Chhanda Dutta 2016- present; Winifred Rossi 2012–2016; Sherry Sherman 1994 – 2012; Marcia Ory 1994 – 2001; National Institute of Nursing Research, Bethesda, MD – Program Officers.
Central Laboratory: University of Michigan, Ann Arbor – Daniel McConnell (Central Ligand Assay Satellite Services).
Coordinating Center: University of Pittsburgh, Pittsburgh, PA – Maria Mori Brooks, PI 2012 - present; Kim Sutton-Tyrrell, PI 2001 – 2012; New England Research Institutes, Watertown, MA - Sonja McKinlay, PI 1995 – 2001.
Steering Committee: Susan Johnson, Current Chair
Chris Gallagher, Former Chair
We thank the study staff at each site and all the women who participated in SWAN.
Funding
The Study of Women’s Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR) and the NIH Office of Research on Women’s Health (ORWH) (Grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, U01AG012495, and U19AG063720). This work was also supported by the National Heart, Lung, and Blood Institute (K24HL123565). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH or the NIH.
Non-standard Abbreviations and Acronyms:
- ASCVD
atherosclerotic cardiovascular disease
- CVD
cardiovascular disease
- CVA
cerebrovascular incident/ stroke
- GBTM
group-based trajectory model
- HDL-C
high-density lipoprotein-cholesterol
- LDL-C
low-density lipoprotein cholesterol
- MI
myocardial infarction
- SWAN
Study of Women’s Health Across the Nation
- VMS
vasomotor symptoms
Footnotes
Disclosures
Dr. Thurston is a consultant and advisor for Astellas Pharma, consultant for Bayer, and on the medical advisory board for Hello Therapeutics. All other authors have no conflicts to disclose.
References
- 1.Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Beaton AZ, Boehme AK, Buxton AE, et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2023. doi: 10.1161/cir.0000000000001123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Heron M Deaths: Leading Causes for 2019. Natl Vital Stat Rep. 2021;70:1–114. [PubMed] [Google Scholar]
- 3.Boccabella A, Malouf J. How Do Sleep-Related Health Problems Affect Functional Status According to Sex? J Clin Sleep Med. 2017;13:685–692. doi: 10.5664/jcsm.6584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, Persistence, and Remission Rates of Insomnia Over 5 Years. JAMA Netw Open. 2020;3:e2018782. doi: 10.1001/jamanetworkopen.2020.18782 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zhang B, Wing YK. Sex differences in insomnia: a meta-analysis. Sleep. 2006;29:85–93. doi: 10.1093/sleep/29.1.85 [DOI] [PubMed] [Google Scholar]
- 6.Lachman ME. Handbook of midlife development. New York: Wiley; 2001. [Google Scholar]
- 7.El Khoudary SR, Wildman RP, Matthews K, Thurston RC, Bromberger JT, Sutton-Tyrrell K. Progression rates of carotid intima-media thickness and adventitial diameter during the menopausal transition. Menopause. 2013;20:8–14. doi: 10.1097/gme.0b013e3182611787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Samargandy S, Matthews KA, Brooks MM, Barinas-Mitchell E, Magnani JW, Janssen I, Hollenberg SM, El Khoudary SR. Arterial Stiffness Accelerates Within 1 Year of the Final Menstrual Period: The SWAN Heart Study. Arterioscler Thromb Vasc Biol. 2020;40:1001–1008. doi: 10.1161/atvbaha.119.313622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.El Khoudary SR, Aggarwal B, Beckie TM, Hodis HN, Johnson AE, Langer RD, Limacher MC, Manson JE, Stefanick ML, Allison MA. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020;142:e506–e532. doi: 10.1161/cir.0000000000000912 [DOI] [PubMed] [Google Scholar]
- 10.Kravitz HM, Zhao X, Bromberger JT, Gold EB, Hall MH, Matthews KA, Sowers MR. Sleep disturbance during the menopausal transition in a multi-ethnic community sample of women. Sleep. 2008;31:979–990. [PMC free article] [PubMed] [Google Scholar]
- 11.Freeman EW, Sammel MD, Lin H, Gracia CR, Pien GW, Nelson DB, Sheng L. Symptoms Associated With Menopausal Transition and Reproductive Hormones in Midlife Women. Obstet Gynecol. 2007;110:230–240. doi: 10.1097/01.Aog.0000270153.59102.40 [DOI] [PubMed] [Google Scholar]
- 12.Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, Rosamond W. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation. 2022;146:e18–e43. doi: doi: 10.1161/CIR.0000000000001078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J. 2011;32:1484–1492. doi: 10.1093/eurheartj/ehr007 [DOI] [PubMed] [Google Scholar]
- 14.Dean YE, Shebl MA, Rouzan SS, Bamousa BAA, Talat NE, Ansari SA, Tanas Y, Aslam M, Gebril S, Sbitli T, et al. Association between insomnia and the incidence of myocardial infarction: A systematic review and meta-analysis. Clin Cardiol. 2023;46:376–385. doi: 10.1002/clc.23984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kwok CS, Kontopantelis E, Kuligowski G, Gray M, Muhyaldeen A, Gale CP, Peat GM, Cleator J, Chew-Graham C, Loke YK, Mamas MA. Self-Reported Sleep Duration and Quality and Cardiovascular Disease and Mortality: A Dose-Response Meta-Analysis. J Am Heart Assoc. 2018;7:e008552. doi: 10.1161/jaha.118.008552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Krittanawong C, Tunhasiriwet A, Wang Z, Zhang H, Farrell AM, Chirapongsathorn S, Sun T, Kitai T, Argulian E. Association between short and long sleep durations and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J Acute Cardiovasc Care. 2019;8:762–770. doi: 10.1177/2048872617741733 [DOI] [PubMed] [Google Scholar]
- 17.Li J, Vitiello MV, Gooneratne NS. Sleep in Normal Aging. Sleep Med Clin. 2022;17:161–171. doi: 10.1016/j.jsmc.2022.02.007 [DOI] [PubMed] [Google Scholar]
- 18.Wang Y-H, Wang J, Chen S-H, Li J-Q, Lu Q-D, Vitiello MV, Wang F, Tang X-D, Shi J, Lu L, et al. Association of Longitudinal Patterns of Habitual Sleep Duration With Risk of Cardiovascular Events and All-Cause Mortality. JAMA Network Open. 2020;3:e205246–e205246. doi: 10.1001/jamanetworkopen.2020.5246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bertisch SM, Pollock BD, Mittleman MA, Buysse DJ, Bazzano LA, Gottlieb DJ, Redline S. Insomnia with objective short sleep duration and risk of incident cardiovascular disease and all-cause mortality: Sleep Heart Health Study. Sleep. 2018;41. doi: 10.1093/sleep/zsy047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Thurston RC, Aslanidou Vlachos HE, Derby CA, Jackson EA, Brooks MM, Matthews KA, Harlow S, Joffe H, El Khoudary SR. Menopausal Vasomotor Symptoms and Risk of Incident Cardiovascular Disease Events in SWAN. J Am Heart Assoc. 2021;10:e017416. doi: 10.1161/jaha.120.017416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thurston RC, Chang Y, Buysse DJ, Hall MH, Matthews KA. Hot flashes and Awakenings Among Midlife Women. Sleep. 2019. doi: 10.1093/sleep/zsz131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sowers M, Crawford S, Sternfeld B, Morganstein D, Gold EB, Greendale GA, Evans D, Neer R, Matthews K, Sherman S, et al. SWAN: a multicenter, multiethnic, community-based cohort study of women and the menopausal transition. In: Lobo RA, Kelsey J, Marcus R, Lobo AR, eds. Menopause: Biology and Pathology. New York: Academic Press; 2000:175–188. [Google Scholar]
- 23.Kravitz HM, Janssen I, Bromberger JT, Matthews KA, Hall MH, Ruppert K, Joffe H. Sleep trajectories before and after the final menstrual period in the Study of Women’s Health Across the Nation (SWAN). Curr Sleep Med Rep. 2017;3:235–250. doi: 10.1007/s40675-017-0084-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ciano C, King TS, Wright RR, Perlis M, Sawyer AM. Longitudinal Study of Insomnia Symptoms Among Women During Perimenopause. J Obstet Gynecol Neonatal Nurs. 2017;46:804–813. doi: 10.1016/j.jogn.2017.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Diagnostic and statistical manual of mental disorders: DSM-5™, 5th ed. Arlington, VA, US: American Psychiatric Publishing, Inc.; 2013. [Google Scholar]
- 26.Kline CE, Colvin AB, Pettee Gabriel K, Karvonen-Gutierrez CA, Cauley JA, Hall MH, Matthews KA, Ruppert KM, Neal-Perry GS, Strotmeyer ES, Sternfeld B. Associations between longitudinal trajectories of insomnia symptoms and sleep duration with objective physical function in postmenopausal women: the Study of Women’s Health Across the Nation. Sleep. 2021;44. doi: 10.1093/sleep/zsab059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. [Google Scholar]
- 28.IDIS drug vocabulary and thesaurus description. Iowa: Division of Drug Information Service, College of Pharmacy, University of Iowa; 2012. [Google Scholar]
- 29.Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13:307–349. doi: 10.5664/jcsm.6470 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Steiner PM, Freidel J, Bremner WF, Stein EA. Standardization of micro-methods for plasma cholesterol, triglyceride and HDL-cholesterol with the Lipid Research Clinics’ methodology J Clin Chem Clin Biochem. 1981;19:850. [Google Scholar]
- 31.Warnick GR, Albers JJ. A comprehensive evaluation of the heparin-manganese precipitation procedure for estimating high density lipoprotein cholesterol. J Lipid Res. 1978;19:65–76. [PubMed] [Google Scholar]
- 32.ADVIA 1800 Chemistry System. Tarrytown, NY: Siemans Healthcare Solutions Diagnostics; 2020. [Google Scholar]
- 33.Baruch L, Agarwal S, Gupta B, Haynos A, Johnson S, Kelly-Johnson K, Eng C. Is directly measured low-density lipoprotein clinically equivalent to calculated low-density lipoprotein? J Clin Lipidol. 2010;4:259–264. doi: 10.1016/j.jacl.2010.05.003 [DOI] [PubMed] [Google Scholar]
- 34.Friedewald W, Levy R, Fredrickson D. Estimation of the concentration of low density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 35.Goff DC Jr., Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S49–73. doi: 10.1161/01.cir.0000437741.48606.98 [DOI] [PubMed] [Google Scholar]
- 36.Jones BL, Nagin DS. Advances in group-based trajectory modeling and an SAS procedure for estimating them. Sociol Meth Res. 2007;35:542–571. doi: 10.1177/0049124106292364 [DOI] [Google Scholar]
- 37.Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6:109–138. doi: 10.1146/annurev.clinpsy.121208.131413 [DOI] [PubMed] [Google Scholar]
- 38.Nagin DS. Group-Based Modeling of Development. Cambridge, MA: Harvard University Press; 2005. [Google Scholar]
- 39.Nagin DS. Group-based trajectory modeling: an overview. Ann Nutr Metab. 2014;65:205–210. doi: 10.1159/000360229 [DOI] [PubMed] [Google Scholar]
- 40.Shaw LJ, Bugiardini R, Merz CN. Women and ischemic heart disease: evolving knowledge. J Am Coll Cardiol. 2009;54:1561–1575. doi: S0735-1097(09)02565-0 [pii] 10.1016/j.jacc.2009.04.098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kabat GC, Xue X, Kamensky V, Zaslavsky O, Stone KL, Johnson KC, Wassertheil-Smoller S, Shadyab AH, Luo J, Hale L, et al. The association of sleep duration and quality with all-cause and cause-specific mortality in the Women’s Health Initiative. Sleep Med. 2018;50:48–54. doi: 10.1016/j.sleep.2018.05.015 [DOI] [PubMed] [Google Scholar]
- 42.Johnson KA, Gordon CJ, Chapman JL, Hoyos CM, Marshall NS, Miller CB, Grunstein RR. The association of insomnia disorder characterised by objective short sleep duration with hypertension, diabetes and body mass index: A systematic review and meta-analysis. Sleep Med Rev. 2021;59:101456. doi: 10.1016/j.smrv.2021.101456 [DOI] [PubMed] [Google Scholar]
- 43.Low CA, Thurston RC, Matthews KA. Psychosocial factors in the development of heart disease in women: current research and future directions. Psychosom Med. 2010;72:842–854. doi: 10.1097/PSY.0b013e3181f6934f [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hall MH, Brindle RC, Buysse DJ. Sleep and cardiovascular disease: Emerging opportunities for psychology. Am Psychol. 2018;73:994–1006. doi: 10.1037/amp0000362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wu TT, Zou YL, Xu KD, Jiang XR, Zhou MM, Zhang SB, Song CH. Insomnia and multiple health outcomes: umbrella review of meta-analyses of prospective cohort studies. Public Health. 2023;215:66–74. doi: 10.1016/j.puhe.2022.11.021 [DOI] [PubMed] [Google Scholar]
- 46.Lehrer M, Yao Z, Krafty R, Evans M, Buysse D, Kravitz H, Matthew KA, Gold E, Harlow SD, Samuelsson LB, Hall MH. Comparing Polysomnography, Actigraphy, and Sleep Diary in the Home Environment: The Study of Women’s Health Across the Nation Sleep Study Sleep. 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, Gangwisch J, Grandner MA, Kushida C, et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38:843–844. doi: 10.5665/sleep.4716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Bonsignore MR, Saaresranta T, Riha RL. Sex differences in obstructive sleep apnoea. Eur Respir Rev. 2019;28. doi: 10.1183/16000617.0030-2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.