

Abstract
Background
Numerous studies indicate that glenoid bony augmentation raises the risk of complications during and after surgery. On the other hand, repairing the labrum alone in cases with subcritical glenoid bone loss results in recurrent instability and persistent apprehension. As a result, recent advancements in shoulder instability surgery prioritize fully restoring the anterior shoulder restraint.
Operative Technique
A novel method for treating recurrent anterior shoulder instability with subcritical glenoid bone loss and off‐track Hill‐Sachs lesion in skeletally immature patients is suggested: the use of dynamic anterior stabilization technique incorporating the long head of the biceps tendon onto the anterior glenoid rim via trans‐subscapular transfer, in conjunction with Hill‐Sachs remplissage. A practical, step‐by‐step surgical technique for a complete reconstruction of the anterior capsule‐labral‐ligamentous complex is provided. This involves utilizing a soft‐tissue dynamic anterior sling, achieved through the trans‐subscapularis transfer of the long head of the biceps tendon at the glenoid level. The procedure concludes with a Hill‐Sachs remplissage to further prevent off‐track events and alleviate apprehension.
Conclusion
Dynamic anterior stabilization is a suitable approach for addressing recurring anterior shoulder instability in skeletally immature patients who have subcritical glenoid bone loss and bipolar bone lesions.
Keywords: Anterior shoulder instability, Bankart repair, Complications in shoulder instability procedures, Dynamic anterior stabilization, Glenoid bone loss, Remplissage
The arthroscopic trans‐subscapular transfer of the long head of the biceps with tenodesis on the anterior glenoid rim, known as DAS, fills a specific indication gap between soft tissue stabilization procedures and bony procedures for subcritical glenoid bone loss. The added Hill‐Sachs remplissage also treats the humeral bone defect and brings supplementary stabilization.

Introduction
The likelihood of experiencing recurrent anterior shoulder instability subsequent to the initial episode of anterior glenohumeral dislocation is significant, particularly for young contact athletes with bipolar bone loss. 1 , 2 , 3 , 4 The decision to pursue treatment is primarily determined by the extent of damage to the capsular, ligamentous, and labral structures, as well as the degree of anterior glenoid bone loss attributable to the size of the Hill‐Sachs defect. 5 The standard surgical interventions for anterior shoulder instability usually involve arthroscopic or open Bankart repair, with or without capsulo‐tenodesis of the infraspinatus into the Hill‐Sachs defect (a technique known as remplissage), as well as Latarjet or other bone block procedures reserved for cases with large anterior defects of the glenoid. 1 , 6
The most significant risk of recurrent dislocation occurs following isolated arthroscopic Bankart stabilization. 7 In contrast, Bankart repair coupled with remplissage, or bone augmentation procedures both demonstrate superior outcomes, with fewer complications observed following Bankart repair with remplissage compared to the Latarjet procedure. 6 , 8 However, the current literature regarding recurrent anterior shoulder instability in skeletally immature patients is scarce. 3 The newly developed dynamic anterior stabilization (DAS) procedure represents a promising technique for managing recurrent anterior glenohumeral instability. 9 This approach has demonstrated its effectiveness as a viable alternative to the Latarjet procedure, which, like other bone block procedures, is known to carry a high risk of complications. 10 , 11 Moreover, DAS is more effective than an isolated Bankart repair, which may lead to recurrent instability. 9 , 11 The purpose of the study is to present a surgical strategy for treating iterative anteroinferior shoulder instability in a skeletally immature contact athlete with subcritical bipolar bone loss.
Materials and Technical Note
A 13‐year‐old male, who is right‐handed and practices boxing, experienced a traumatic anteroinferior dislocation of his right shoulder. He received a closed reduction under anesthesia in the emergency room 1.5 h following the incident. After 2 weeks of immobilization of the affected arm with a sling, he received conservative therapy at a separate medical department and attempted to return to his previous sports activities. However, at 6 months following the initial dislocation, he experienced six additional dislocations of the right shoulder and subsequently ceased participating in boxing. He ultimately dislocated his right shoulder while sleeping, and subsequently sought consultation with a shoulder surgeon.
Clinical and Imagistic Examination
Upon physical examination of the right shoulder, scapulothoracic dyskinesia was noted, and an apprehension test yielded positive results during the abducted externally rotated (ABER) position at 30°, 90°, and 140° abduction angles. Additionally, a positive hyper extension‐internal rotation (HERI) test was observed, although testing of the rotator cuff was normal, with the exception of a positive O'Brien test. 12 , 13 Magnetic resonance imaging (MRI) revealed capsulolabral and ligamentous injuries to the anteroinferior region of the shoulder, with 14% measured anterior glenoid bone loss (as depicted in Figure 1). Additionally, an engaging Hill‐Sachs lesion measuring 1 cm in width, 0.5 cm in depth, and 2 cm in height was identified.
FIGURE 1.

(A) Sagittal oblique proton density (PD)—weighted sequence depicting the amount of anterior glenoid bone loss of 3.02 / 0.42 × 100% = 13% of bone loss. (B) T2—weighted axial sequence depicting a 1.38 cm Hill‐Sachs interval.
Surgical Indication
Upon consideration of these findings, surgical intervention was recommended, which would entail reattachment of the capsulolabral and ligamentous complex via a soft tissue Bankart procedure, as well as a Hill‐Sachs remplissage. The parents and patient were informed of the possibility of a weak quality of the capsulolabral complex tissue intraoperatively due to the chronicity of the injury and repeated dislocations and the high redislocation risk and failure after soft tissue Bankart repair. Therefore, in such an event, a dynamic anterior stabilization procedure may be required. Written consent was obtained from the patient and parents for both the initial recommended procedure and the dynamic anterior stabilization, if necessary. Considering the unpredictability of the Latarjet procedure in skeletally immature patients and the limited availability of regional allografts in the event of Latarjet failure, it was determined that a soft‐tissue procedure would be the preferred option. The Latarjet technique was reserved as a potential revision option only in case of failure or postoperative redislocation.
Arthroscopic Technique with Photographic and Video Illustration
For sedation, an ipsilateral interscalene block and general anesthesia were administered. The patient was then positioned in the beach chair position. To maintain the shoulder in 30° of anterior elevation, 10° of abduction, and neutral rotation, a traction cable holding the forearm was utilized. A standard arthroscopic round diagnostic through the posterior soft spot (A) portal was then performed. The working portals were: D—anterolateral, E—anterior (corresponding to the rotator interval) and B′—inferior posterolateral for the Hill‐Sachs remplissage (Figures 2 and 3; Video S1). 14
FIGURE 2.

Step‐by‐step approach to performing dynamic anterior stabilization and Hill‐Sachs remplissage. (A) 360° arthroscopic evaluation identifies anterior disruption of the capsule‐labral complex extending to the inferior pole of the glenoid; (B) disruption of the capsule‐labrum complex can be seen at the inferior glenoid pole; (C) the anterior disruption of the inferior glenoid ligament can be identified; (D) a large Hill‐Sachs lesion can be seen and is debrided using a shaving device; (E) an all‐suture anchor is placed in the now debrided Hill‐Sachs defect in a transtendinous fashion; (F) a bird‐beak suture passer is used to pass each suture limb through the infraspinatus tendon; (G) final configuration of the Hill‐Sachs remplissage can be seen—parachute technique; (H) the repairability of the capsule‐labral complex is assessed using a grasper type instrument; (I) after assessing the repairability of the capsule‐labral complex an all‐suture anchor is placed at the 5 o'clock position and the labrum is repaired using classical Bankart repair technique; (J) before addressing the biceps tendon, the rotator interval is identified and opened but without disrupting the superior glen‐humeral ligament and anterior expansion of the rotator cable; (K) after opening the rotator interval the next step is to address the biceps tendon by releasing the transvers ligament and the rest of the biceps pulley until reaching the superior border of the pectoralis major muscle; (L) after completely releasing the biceps from its groove, a PDS suture (polyester poly p‐dioxanone) is percutaneously passed through the biceps tendon near its proximal end; (M) the PDS suture is used to shuttle a cut limb from the remplissage (economic option) and is used to create a 360° lasso loop around the biceps tendon; (N) the suture limbs of the 360° lasso loop wrapped around the biceps tendon are passed over the intact superior glen‐humeral ligament and anterior extension of the rotator cable and through the subscapularis tendon; (O) arthroscopic view from D portal, watching in front of the subscapularis: a switching stick is used to penetrate the subscapularis muscle through the posterior portal and a canulated obturator is used through the E portal to performs the subscapularis split; (P) once the canulated obturator has performed the subscapularis split, a shuttling wire is passed through it and grasped with a grasper through the posterior portal; (Q) after the shuttle wire is brought to the posterior portal its anterior end together with the 360° lasso‐loop wrapped around the biceps tendon are brought outside through the E portal, tied together and then the shuttling wire is used to pull the suture limbs through the posterior portal. While pulling the suture limbs, the biceps tendon is pushed synchronously with the grasper through the subscapularis so that the biceps tendon can penetrate the subscapularis muscle; (R) once passed through the subscapularis muscle, a tenodesis of the biceps tendon is performed as described; (S) after the biceps tenodesis, the first lasso‐loop around the capsule‐labral complex is tied; (T) the repairability of the superior labrum‐capsule complex is assessed; (U) the superior labrum‐capsule complex is deemed repairable and an all‐suture anchor is used together with a lasso‐loop using a bird‐beak suture passer; and (V) the final view shows a complete reconstruction of the anterior buttress composed of complete restoration of the labrum‐capsule complex together with the biceps tendon that serves as anterior sling and hammock.
FIGURE 3.
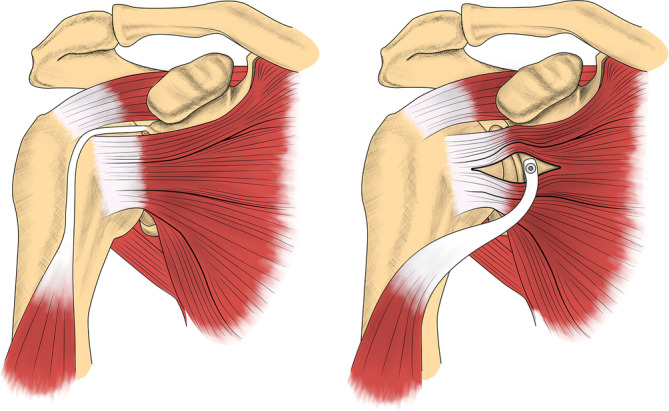
Technique illustration: the long head of the biceps tendon is tenotomies from the superior glenoid rim and transferred at the anterior glenoid at the 3 o'clock position through a subscapularis split.
The arthroscopic round‐diagnostic identified a superior labral tear (SLAP), as well as an engaging Hill‐Sachs lesion. The dynamic testing conducted during arthroscopy revealed the occurrence of anterior dislocation when passive external rotation was coupled with abduction of the arm. Detachment of the labrum was observed along the entire superior, anterior, and anteroinferior glenoid rim, with the remaining anterior labral tissue being found to be fragile, frayed, and avascular. The anterior part of the inferior glenohumeral ligament was also observed to be detached from the glenoid, with partial reduction being possible following debridement and surgical liberation of scar tissue.
Based on the findings, it was concluded that repair of the capsulo‐ligamentous‐labrum complex at the 5 o'clock position was feasible. Due to compromised structural integrity and vasculature, the remaining capsulolabral tissue above the 5 o'clock position was deemed unsuitable for an effective Bankart repair. In this context, it was deemed appropriate to perform a dynamic anterior stabilization using the long head of the biceps tendon (LHBT) to reconstruct what we call the stabilizing anterior wall of the shoulder. Additionally, given the off‐track nature of the Hill‐Sachs lesion, a remplissage procedure was also included in the surgical plan. The surgical technique and steps are depicted in the following text and Figure 2. Figure 3 represents an illustration of the original DAS technique. 15
To release the glenoid margin of scar tissue, an arthroscopic rasp was placed in the D portal and used to decorticate the bone and mobilize the capsulolabral complex. After extensive tissue mobilization from the glenoid rim and neck, a second attempt was made to check the repairability of the capsulolabral complex and this time we confirmed that it was partially reparable after shifting upwards the capsule together with labrum and ligament. A thorough bursectomy of the pre‐subscapularis compartment was performed after debriding the rotator interval.
A free suture tape (Arthrex, Naples, FL, USA) was inserted into the LHBT and a 360° pretzel like lasso was performed into and around the tendon, as demonstrated by Popescu et al. for dynamic anterior stabilization. 9 , 14 Suture ends were then retrieved through the E portal.
An all‐suture anchor (QFix, Smith and Nephew, Andover, MA, USA) was deployed at the 5 o'clock position onto the glenoid rim to achieve a partial Bankart repair. The suture limbs were passed through the corresponding viable anterior and inferior capsulolabral tissue in a lasso loop and mattress manner. The suture ends were then parked outside the shoulder in the E portal to tighten the loop, but without performing the knot. We tied the knot after the trans subscapular transfer of the LHBT at 3 o'clock position. 16 The reason is that even a partially repaired labrum might impede performing the subscapularis split for the subsequent LHBT transfer step.
The Hill‐Sachs defect was prepared by gentle debridement through the B portal with the arm in neutral position and with the humeral head slightly subluxed (anterior drawer position held by the assistant). An all‐suture anchor (Iconix Speed, Kalamazoo, MI, USA) pierced the infraspinatus tendon through the B portal and was positioned in the middle of the Hill‐Sachs lesion. A bird‐beak hook was used to pass the suture limbs through the tendon and capsule in a mattress suture fashion. By moving the arthroscope in the subacromial space, all suture limbs were retrieved together through the B portal, avoiding bursal tissue interposition. They are also put on waiting to be knotted at the end of the procedure, after the DAS and the Bankart reinsertion.
The LHBT was then released from the intertubercular groove using the ablation electrode positioned into the D portal facing posterior‐laterally, away from the subscapularis insertion. Once the bicipital groove was released, the viewing position was switched to the D portal to have a clear view behind and in front of the subscapularis (intra‐ and extra‐articular view). The remaining pre‐subscapularis bursa was resected up to the posteromedial aspect of the coracoid and the conjoint tendon to have a clear view over the anterior aspect of the subscapularis.
A Wissinger rod (switching stick) was advanced from posterior to anterior through the A portal, parallel to the glenoid, piercing the subscapularis. The piercing position was located at the inferior one‐third of the glenoid. To prepare the subscapularis tendon split for the LHBT transfer, gentle passive internal‐external rotation arm movements were conducted and a reusable arthroscopic canulated guide was pushed over the switching stick from E portal, acting as a dilatator inside the subscapularis, thus performing the subscapularis split at the musculo‐tendinous junction.
The LHBT sutures were pulled through the subscapularis split and then retrieved outside through the A portal with the help of a suture grasper. A tenotomy of the LHBT at root level was conducted. Once the LHBT was released and mobilized, the transfer was achieved by gently pulling both suture limbs through the A portal while pushing the LHBT inside the subscapularis and further into the joint from the E portal with a tissue grasper. After this step, the suture ends were recovered outside the E portal, over the subscapularis, and then charged into a knotless anchor. We performed a trans‐subscapular LHBT tenodesis using a knotless 3.5 mm Pushlock anchor (Arthrex, Naples, FL, USA) onto the anterior glenoid rim in the 3 o'clock position. Following the LHBT transfer and tenodesis, the suture ends of the 5 o'clock all‐suture anchor was tied in order to attach the remanent anteroinferior labrum underneath the transferred LHBT. A second all‐suture anchor was used to reattach remaining capsule‐labral tissue above the now transferred LHBT, thus reconstructing the whole anterior aspect of the glenoid rim. At the end, the remplissage sutures were knotted blindly through the B′ portal.
Postoperative Protocol
The shoulder was immobilized for 3 weeks in a sling with abduction pillow and neutral arm position. We recommended gradually passive mobilization and passive assisted range‐of‐motion exercises for the first 6 postoperative weeks. Shoulder shrugs, pendulum exercises and scapulothoracic rehabilitation with posture training were included from the first postoperative day. After the first 6 weeks, active‐assisted and active rehabilitation were introduced together with proprioception and strength training of the rotator cuff muscles. Tips and pitfalls, as well as key points of our technique are listed in Table 1.
TABLE 1.
Tips, pitfalls, and key points of dynamic anterior stabilization with Hill‐Sachs remplissage
| Tips | Pitfalls | Key points |
|---|---|---|
| Start with remplissage first, even before performing the anterior portals. Park all the sutures into the B portal and perform the knotting at the end of the procedure. | Poor suture management can complicate the remplissage at the end of the procedure. | Engage in comprehensive discussions with both the patient and their family regarding all available treatment alternatives, and subsequently arrive at a personalized treatment decision. |
| A thorough presubscapularis bursectomy is essential for achieving optimal visualization. | Insufficient LHBT release from its groove can render the subscapularis transfer unattainable. | Stay flexible and adapt to the intraoperative findings.
|
| Perform the LHBT release by cutting the transverse humeral ligament lateral to the tendon to avoid injuring the subscapularis insertion. | Numerous stitches in the LHBT and large penetrating tools increase the likelihood of tendon damage and longitudinal tearing. | Consider the remplissage as an aid to your anterior stabilization procedure. |
| Facilitate the transfer of the LHBT through the subscapularis using a grasper (as shown in the provided Video). | Caution must be exercised when transferring the LHBT through the subscapularis split. If too much tension is applied the biceps tendon can tear. | When possible, repair the remaining anterior‐inferior labral‐capsule‐ligament tissue. |
| Tie the knots of the anterior Bankart repair after transferring the LHBT at the glenoid rim. |
Clinical Follow‐Up at 1 Year after the Surgery
The patient progressively regained normal range of motion and strength in his operated shoulder. In Video S1 (supplementary file), after the surgical technique presentation, we demonstrate the clinical examination at 10 and at 13 months follow‐up. Apprehension is non‐existent in any degree of abduction and external rotation (ABER). HERI test became normal, rotator cuff force intact, range of motion normalized and symmetric. The patient feels confident on his shoulder and declares to be very satisfied. He returned to sport at 10 months postoperatively.
Discussion
The present operative technique presents a step‐by‐step approach to performing a complete anterior shoulder restraint reconstruction. For optimal surgical flow the remplissage is performed first without tying the knots. Then, the LHBT is transferred through a subscapularis split at the glenoid rim in the 3 o'clock position. Following this step, a Bankart repair is performed reattaching the remaining capsule‐labrum complex at the glenoid rim in the 5 and 2 o'clock position (underneath and above the DAS). Finally, the remplissage is finalized by blindly tying the knots.
Current Concepts
There is no consensus among shoulder surgeons regarding the ideal approach for the management of recurrent anterior shoulder instability with concomitant Hill‐Sachs lesion. Currently, the two most commonly used techniques are the Latarjet procedure and arthroscopic Bankart repair with or without remplissage, with the choice depending on the degree of glenoid bone loss and the size of the Hill‐Sachs defect. 1 , 6 However, the available literature on the use of bone block procedures for glenoid augmentation in young adolescents, including the Latarjet procedure, is limited and reports have identified a complication rate of up to 11%. 1 , 8 , 17
In the adult population, a significant or intermediate glenoid bone loss and engaging Hill‐Sachs lesion are often treated with a Latarjet procedure due to its higher success rate in restoring pre‐injury levels of sports with low recurrence rate. However, the procedure is associated with a higher risk of complications such as early onset arthritis, nerve injury, infection, and implant failure, particularly in cases with extensive dissection and conjoint tendon manipulation. 10 , 18 In young adolescents, literature is scarce about the use of Latarjet or other bone block procedures for glenoid augmentation, and further research is needed to assess the long‐term outcomes and potential complications in this population. 17 , 19 There are no specific contraindications for the use of glenoid augmentation procedures, including the Latarjet procedure, in the pediatric population. 17 However, there is a lack of extensive experience and clear indications for such procedures in young patients. Therefore, careful consideration of the risks and benefits should be made, and individualized treatment plans should be formulated for each patient. 3 Graft and hardware‐related complications, as well as secondary arthropathy are serious risks that still apply both in adult and in skeletally immature patients. 17 , 20
Research has shown that Bankart repair combined with remplissage results in a lower recurrence rate compared to isolated Bankart procedure while at the same time providing similar outcomes to the Latarjet procedure albeit with less reported complications. 5 , 8 , 19 , 21 However, the potential for excessive tension on the posterior capsule during the remplissage procedure could lead to limitations in external rotation and impact daily activities and sports participation. 19 On the other hand some studies suggest that an additional infraspinatus remplissage does not significantly restrict external rotation, and thus daily activities and sport level are unaffected. 22
Soft tissue stabilization procedures such as Bankart repair and Remplissage, as well as bone augmentation techniques including Latarjet and Eden‐Hybinette procedures, have shown efficacy in treating recurrent anterior shoulder instability when performed in specific indication ranges. Subcritical glenoid bone loss with an engaging Hill‐Sachs defect is still a gray area in shoulder surgery that needs to be addressed. 23 , 24 DAS fills this specific indication gap between soft tissue stabilization procedures and bony procedures, as a promising treatment for glenoid defects at or less than 20%. By transferring the LHBT at the glenoid level, where the coracoid would be fixed in a Latarjet procedure, through a trans‐subscapular split, a sling and a hammock effect is accomplished, thus dynamically stabilizing and recentering the shoulder. 15 , 25 Recent follow‐up data indicate that the LHBT has successfully healed in its relocated position, and there has been no adverse effect on the range of motion. 11 Additionally, the Hill‐Sachs remplissage creates stability by two mechanisms. First, the infraspinatus muscle opposes excessive external rotation and the engaging of the Hill‐Sachs defect and second it pulls the humeral head posteriorly thus centering the humeral head and alleviating tension from the anterior soft‐tissue buttress. 9 , 26 The first available follow‐up studies for DAS procedure display positive outcomes, with little to no reported recurrence of anterior instability and no constraints in range of motion. 11 , 27
Experience Sharing
While shoulder instability is prevalent among younger patients, there remains ongoing discussion about the most effective approach for treating skeletally immature patients. Conservative measures play an important role in this case. Nonetheless, when instability becomes recurrent, it can exacerbate shoulder damage and result in glenohumeral arthropathy, leading surgeons to now propose early surgical intervention for those at risk (throwing or contact sports athletes, young, male). 28 , 29 , 30
The opportunity to avert subsequent instability, thereby mitigating potential osseous and cartilaginous impairments, 29 supports the notion that skeletal immaturity should not be regarded as a contraindication for surgical intervention. 31 To date, the conventional Latarjet procedure and Bankart repair have constituted the main available and researched choices for addressing this population category. Given our present knowledge, this study represents the first proposition of DAS as a viable alternative for skeletally immature patients. Its safety is derived from a decreased procedural complexity in comparison to bone block augmentation techniques, thereby minimizing the potential origins of complications. 8
Our patient had several risk factors for recurrent shoulder instability: male, recurrent dislocations, young age, contact athlete. 32 The particularity of this case is represented by the subcritical glenoid bone loss in the presence of a Hill‐Sachs defect and a partially reparable anterior‐inferior labral capsular ligamentous complex. 23 , 33 It is also the authors experience that a partial Bankart repair with or without remplissage would not suffice especially in engaging bipolar lesions. The surgical solution thus provided by dynamic anterior stabilization is aimed at avoiding the complications of a coracoid transfer as well as containing the risk of recurrent instability after performing a soft tissue Bankart repair with or without an added remplissage.
The long head of the biceps tendon is a useful tool in shoulder surgery because it is a locally accessible and viable autograft that may be used to augment rotator cuff repairs and be incorporated into capsulo‐labral reconstructions in anterior shoulder instability procedures. 9 , 31 , 32 , 33
Limitations
Readers Should be Aware of the Following Limitations
Dynamic anterior stabilization is still in its early development phase, with only a limited number of studies available that report on the healing of the biceps tendon and short‐term patient‐reported outcome measures. 11 , 27
The concept of “sub‐critical” bone loss is not commonly encountered in day‐to‐day clinical practice and an important amount of heterogeneity can be encountered in the literature. 16 , 23
In the last years, it became obvious that the LHBT is useful in different types of arthroscopic reconstruction. The paradigm shift from biceps tenotomy to surgical reconstruction using the long head of the biceps has to be properly documented and be scientifically proven with long term follow up and randomized studies before being adopted in general practice. 34 , 35 , 36
Conclusion
The arthroscopic trans‐subscapularis transfer of the long head of the biceps tendon at the glenoid level, concluding with a Hill‐Sachs remplissage to further prevent off‐track events, can be taken into consideration for treating recurring anteroinferior shoulder instability in adolescents. The evaluation of potential hazards and advantages associated with this approach, in relation to conventional Latarjet surgery necessitates meticulous assessment on a case‐by‐case basis. Further long‐term follow‐up studies on arthroscopic DAS with Remplissage technique are needed.
Conflict of Interest Statement
The authors declare that they have no conflict of interests related to the subject of the article. They have not received or will receive any financial aid, in any form, for this study. The manuscript has been prepared according to the journal's style specifications and requirements.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of technical note formal consent of Ethical Committee is not required. The patient and parents signed a specific consent accepting that anonymized medical data, including video recording of the surgery, can be used for scientific and educational purposes as long as patient identity and personal data are protected.
Author Contributions
The work has not been submitted elsewhere for publication, in whole or in part, and all the authors listed contributed to the present work, have approved the manuscript and the video that is enclosed: the senior author (Popescu) developed, adapted and simplified the arthroscopic technique for feasibility and replicability, performed the surgery, edited the video, the figures, contributed to the surgical technique description, and revised the final manuscript. Nicolao and Avram prepared the main manuscript, organized the literature review, edited the video recordings and figures, and contributed to the final form of the submitted work. Simion, Obada, and Predescu contributed by conceptualizing the study, provided data curation, wrote the original draft, and reviewed the final manuscript.
Supporting information
VIDEO S1. Starting from the posterior portal, a typical round diagnostic for a right shoulder is performed. A standard soft tissue Bankart repair is carried out at the 5 o'clock position onto the anterior glenoid rim, but knot tying is postponed until the end of the procedure. The Hill‐Sachs remplissage is performed using the parachute technique, but the knot tying is done the same way, later. The long head of the biceps tendon (LHBT) is dissected and mobilized from the bicipital groove without harming the subscapularis or the supraspinatus insertions. Following proximal tenotomy, a knotless 3.5 mm anchor is used to transfer LHBT trans‐subscapular and tenodesis it on the anterior glenoid rim at the 3 o'clock position. The Bankart sutures and those for the remplissage are knotted at the end, having the option to reattach remaining capsule and labrum using a secondary all suture anchor at the 2 o'clock position.
References
- 1. Bah A, Lateur GM, Kouevidjin BT, Bassinga JYS, Issa M, Jaafar A, et al. Chronic anterior shoulder instability with significant Hill–Sachs lesion: arthroscopic Bankart with remplissage versus open Latarjet procedure. Orthop Traumatol Surg Res. 2018;104(1):17–22. 10.1016/j.otsr.2017.11.009 [DOI] [PubMed] [Google Scholar]
- 2. Watkins RA, De Borja C, Ramirez F. Common upper extremity injuries in pediatric athletes. Curr Rev Musculoskelet Med. 2022;15(6):465–473. 10.1007/s12178-022-09784-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Shanmugaraj A, Chai D, Sarraj M, Gohal C, Horner NS, Simunovic N, et al. Surgical stabilization of pediatric anterior shoulder instability yields high recurrence rates: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2021;29(1):192–201. 10.1007/s00167-020-05913-w [DOI] [PubMed] [Google Scholar]
- 4. Franklin CC, Weiss JM. The natural history of pediatric and adolescent shoulder dislocation. J Pediatr Orthop. 2019;39:S50–S52. [DOI] [PubMed] [Google Scholar]
- 5. Camus D, Domos P, Berard E, Toulemonde J, Mansat P, Bonnevialle N. Isolated arthroscopic Bankart repair vs. Bankart repair with “remplissage” for anterior shoulder instability with engaging Hill‐Sachs lesion: a meta‐analysis. Orthop Traumatol Surg Res. 2018;104(6):803–809. [DOI] [PubMed] [Google Scholar]
- 6. Hughes JL, Bastrom T, Pennock AT, Edmonds EW. Arthroscopic Bankart repairs with and without remplissage in recurrent adolescent anterior shoulder instability with hill‐Sachs deformity. Orthop J Sports Med. 2018;6(12):2325967118813981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Schwihla I, Wieser K, Grubhofer F, Zimmermann SM. Long‐term recurrence rate in anterior shoulder instability after Bankart repair based on the on‐ and off‐track concept. J Shoulder Elbow Surg. 2023;32(2):269–275. [DOI] [PubMed] [Google Scholar]
- 8. Haroun HK, Sobhy MH, Abdelrahman AA. Arthroscopic Bankart repair with remplissage versus Latarjet procedure for management of engaging Hill‐Sachs lesions with subcritical glenoid bone loss in traumatic anterior shoulder instability: a systematic review and meta‐analysis. J Shoulder Elbow Surg. 2020;29(10):2163–2174. [DOI] [PubMed] [Google Scholar]
- 9. Popescu IA, Neculau DC, Simion C, Popescu D. Modified dynamic anterior stabilization (DAS) and hill‐Sachs Remplissage for the treatment of recurrent anterior shoulder dislocation. Arthrosc Tech. 2022;11(2):e147–e152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Popescu IA, Haeni D. Complications of bony procedures for shoulder instability. In: Lafosse L, Agneskirchner J, Lafosse T, editors. Complications in Arthroscopic Shoulder Surgery. Cham: Springer International Publishing; 2020. p. 51–64. [Google Scholar]
- 11. de Campos Azevedo C, Ângelo AC. Onlay dynamic anterior stabilization with biceps transfer for the treatment of anterior glenohumeral instability produces good clinical outcomes and successful healing at a minimum 1 year of follow‐up. Arthrosc Sports Med Rehabil. 2023;5(2):e445–e457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lafosse T, Fogerty S, Idoine J, Gobezie R, Lafosse L. Hyper extension‐internal rotation (HERI): a new test for anterior gleno‐humeral instability. Orthop Traumatol Surg Res. 2016;102(1):3–12. [DOI] [PubMed] [Google Scholar]
- 13. O'Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med. 1998;26(5):610–613. [DOI] [PubMed] [Google Scholar]
- 14. Lafosse T, Kopel L, Beckers J, Lafosse L. The 360 double lasso loop for biceps tenodesis: tips and tricks. Arthrosc Tech. 2021;10(8):e1889–e1895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Collin P, Lädermann A. Dynamic anterior stabilization using the long head of the biceps for anteroinferior glenohumeral instability. Arthrosc Tech. 2018. Jan;7(1):e39–e44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Monroe EJ, Brand JC. Editorial commentary: dynamic anterior stabilization via biceps tenodesis to the glenoid is an option for anterior shoulder instability with subcritical glenoid bone loss. Art Ther. 2022;38(6):1772–1773. [DOI] [PubMed] [Google Scholar]
- 17. Domos P, Chelli M, Lunini E, Ascione F, Bercik MJ, Neyton L, et al. Clinical and radiographic outcomes of the open Latarjet procedure in skeletally immature patients. J Shoulder Elbow Surg. 2020;29(6):1206–1213. [DOI] [PubMed] [Google Scholar]
- 18. Hanson JA, Foster MJ, Pearce SS, Millett PJ. Primary Latarjet for anterior shoulder instability in adolescents: an unstable conclusion: commentary on an article by Manuel Waltenspül, MD, et al.: “long‐term results and failure analysis of the open Latarjet procedure and arthroscopic Bankart repair in adolescents”. J Bone Joint Surg Am. 2022;104(12):1129. [DOI] [PubMed] [Google Scholar]
- 19. Feng S, Chen M, Chen J, Li H, Chen J, Chen S. Patient outcomes and fear of returning to sports after arthroscopic Bankart repair with Remplissage. Orthop J Sports Med. 2021;9(4):23259671211001775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hurley ET, Schwartz LB, Mojica ES, Campbell KA, Matache BA, Meislin RJ, et al. Short‐term complications of the Latarjet procedure: a systematic review. J Shoulder Elbow Surg. 2021;30(7):1693–1699. [DOI] [PubMed] [Google Scholar]
- 21. Alkaduhimi H, Verweij LPE, Willigenburg NW, van Deurzen DFP, van den Bekerom MPJ. Remplissage with Bankart repair in anterior shoulder instability: a systematic review of the clinical and cadaveric literature. Art Ther. 2019;35(4):1257–1266. [DOI] [PubMed] [Google Scholar]
- 22. Brilakis E, Avramidis G, Malahias MA, Stathellis A, Deligeorgis A, Chiotis I, et al. Long‐term outcome of arthroscopic remplissage in addition to the classic Bankart repair for the management of recurrent anterior shoulder instability with engaging Hill–Sachs lesions. Knee Surg Sports Traumatol Arthrosc. 2019;27(1):305–313. [DOI] [PubMed] [Google Scholar]
- 23. Shaha JS, Cook JB, Song DJ, Rowles DJ, Bottoni CR, Shaha SH, et al. Redefining “critical” bone loss in shoulder instability: functional outcomes worsen with “subcritical” bone loss. Am J Sports Med. 2015;43(7):1719–1725. [DOI] [PubMed] [Google Scholar]
- 24. Boileau P, Villalba M, Héry JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006;88(8):1755–1763. [DOI] [PubMed] [Google Scholar]
- 25. Yamamoto N, Muraki T, An KN, Sperling JW, Cofield RH, Itoi E, et al. The stabilizing mechanism of the Latarjet procedure: a cadaveric study. J Bone Joint Surg Am. 2013;95(15):1390–1397. [DOI] [PubMed] [Google Scholar]
- 26. Kelly AM, Kelly JD. Editorial commentary: shoulder remplissage is a beneficial addition to Bankart or glenoid bone loss treatment: stay on track and use wisely. Art Ther. 2023;39(3):703–705. [DOI] [PubMed] [Google Scholar]
- 27. Collin P, Nabergoj M, Denard PJ, Wang S, Bothorel H, Lädermann A. Arthroscopic biceps transfer to the glenoid with Bankart repair Grants satisfactory 2‐year results for recurrent anteroinferior glenohumeral instability in subcritical bone loss. Arthroscopy. 2022;38(6):1766–1771. [DOI] [PubMed] [Google Scholar]
- 28. Roberts SB, Beattie N, McNiven ND, Robinson CM. The natural history of primary anterior dislocation of the glenohumeral joint in adolescence. Bone Joint J. 2015;97‐B(4):520–526. [DOI] [PubMed] [Google Scholar]
- 29. Clinker CE, Chalmers PN, Romeo A. Anchorless labral repair for recurrent shoulder instability in the skeletally immature. Arthrosc Tech. 2022;11(11):e2049–e2053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Longo UG, Loppini M, Rizzello G, Ciuffreda M, Maffulli N, Denaro V. Management of primary acute anterior shoulder dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy. 2014;30(4):506–522. [DOI] [PubMed] [Google Scholar]
- 31. Khan A, Samba A, Pereira B, Canavese F. Anterior dislocation of the shoulder in skeletally immature patients: comparison between non‐operative treatment versus open Latarjet's procedure. Bone Joint J. 2014;96‐B(3):354–359. [DOI] [PubMed] [Google Scholar]
- 32. Boileau P, Lemmex DB. Editorial commentary: which patients are likely to undergo redislocation after an arthroscopic Bankart repair? Preoperative instability severity index scoring over 3 points—the game is over! Art Ther. 2019;35(2):367–371. [DOI] [PubMed] [Google Scholar]
- 33. Yamamoto N, Shinagawa K, Hatta T, Itoi E. Peripheral‐track and central‐track Hill‐Sachs lesions: a new concept of assessing an on‐track lesion. Am J Sports Med. 2020;48(1):33–38. [DOI] [PubMed] [Google Scholar]
- 34. Popescu IA, Teboul F, Goubier JN, Ghazanfari A. In‐office shoulder arthroscopy and tenotomy of the long head of the biceps tendon‐a cadaveric feasibility study. Int Orthop. 2019;43(10):2361–2365. [DOI] [PubMed] [Google Scholar]
- 35. Avram GM, Neculau DC, Obada B, Pomenta Bastidas MV, Popescu D, Fiodorovas M, et al. Partial articular supraspinatus tendon avulsion repair and patch: a technical note for augmenting the supraspinatus reinsertion with the long head of the biceps tendon. Orthop Surg. 2023;15(8):2174–2180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Lädermann A. Editorial commentary: the long head of the biceps tendon is useful for shoulder reconstruction including glenohumeral stabilization: from biceps killers to biceps users. Arthroscopy. 2023;39(2):202–203. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
VIDEO S1. Starting from the posterior portal, a typical round diagnostic for a right shoulder is performed. A standard soft tissue Bankart repair is carried out at the 5 o'clock position onto the anterior glenoid rim, but knot tying is postponed until the end of the procedure. The Hill‐Sachs remplissage is performed using the parachute technique, but the knot tying is done the same way, later. The long head of the biceps tendon (LHBT) is dissected and mobilized from the bicipital groove without harming the subscapularis or the supraspinatus insertions. Following proximal tenotomy, a knotless 3.5 mm anchor is used to transfer LHBT trans‐subscapular and tenodesis it on the anterior glenoid rim at the 3 o'clock position. The Bankart sutures and those for the remplissage are knotted at the end, having the option to reattach remaining capsule and labrum using a secondary all suture anchor at the 2 o'clock position.