

Abstract
Social adaptive functioning is notably compromised and may be further impaired by aggressive behavior in children with autism spectrum disorder (ASD). This study examined the association between aggressive behavior and social adaptive skills in children with ASD and the contribution of aggressive behavior to social adaptive skills in a combined sample of children with and without ASD. Participants consisted of children, ages 8 to 15 years, with ASD (n = 52) and who were typically developing (n = 29). Results indicate that aggressive behavior is negatively associated with social adaptive skills in children with ASD and that it contributes to reduced social adaptive functioning above and beyond ASD diagnosis. Findings underscore the importance of considering the role of aggressive behavior when evaluating and promoting social functioning in children with ASD.
Keywords: autism spectrum disorders, functional skills, independence, social skills, socialization
Adaptive functioning, or the ability to operate independently and competently in one’s environment, is commonly impaired in children with autism spectrum disorder (ASD) (Kanne et al., 2011). Adaptive functioning includes skills related to a variety of behaviors, including engaging in interpersonal interactions, completing self-care tasks, and operating in the community (Pugliese et al., 2015). The Vineland Adaptive Behavior Scales, recently updated from the second edition (Vineland-II; Sparrow, Cicchetti, & Balla, 2005) to the third edition (Vineland-3; Sparrow, Cicchetti, & Saulnier, 2016), are the most widely used measure of adaptive functioning. Adaptive skills are divided into three domains on Vineland-II and Vineland-3: Communication, Socialization, and Daily Living Skills (Sparrow et al., 2005; Sparrow et al., 2016). Across all three domains, children with ASD demonstrate adaptive behaviors below the level which would be expected based on cognitive ability, leading to compromised daily functioning and impaired ability to carry out everyday tasks in a manner commensurate with same-age peers (Kanne et al., 2011).
Social difficulties are especially prominent in children with ASD, as reflected in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria for the disorder, which include impairments in social communication and interaction (APA, 2013). These impairments, including difficulty engaging in interpersonal interactions, problems with nonverbal communication, and difficulty understanding interpersonal relationships, often translate into problems with everyday social adaptive behaviors, such as getting along with others and maintaining relationships. The Vineland Socialization domain serves as a widely used measure of social adaptive behaviors. Children with ASD demonstrate the lowest levels of adaptive behavior in the domain of Socialization relative to the other Vineland domains (Kenworthy et al., 2010; Klin et al., 2007). Klin and colleagues reported in their 2007 paper that 12-year-old children with ASD had an average Vineland-II Socialization age-equivalent score of 4.5 years. While an average 4.5-year-old may have the ability to take turns, apologize for small mistakes, and talk with others about shared interests, areas of challenge are likely to include competencies such as asking permission when taking others’ belongings and engaging in conversations about nonpreferred topics.
Compounding these social difficulties, children with ASD tend to show declines in social adaptive behavior over time (Pugliese et al., 2015), as they acquire social skills at a rate slower than same-age peers (Tomaszewski et al., 2020). This increased lagging behind of peers has significant ramifications for the transition toward more independent functioning. As expectations for social behavior increase and youth with ASD encounter difficulty navigating complex social interactions and relationships, they are less likely to meet normative interpersonal and educational milestones (e.g., maintaining friends, dating, graduating from high school, going to college), reducing their chances of success in future social and occupational settings.
Elevated levels of irritability and aggression occur in almost half of children with ASD (Lecavalier et al., 2019). Both irritability, which refers to proneness to anger and frustration (Brotman et al., 2017), and aggression, which refers to behaviors that cause risk of harm to self or others, can cause substantial impairment in children with ASD (Sukhodolsky et al., 2019). Aggressive behavior is an especially prevalent and troubling concern that often occurs across settings. More than two thirds of children were reported to have displayed aggression to caregivers in a study of 1,389 children with ASD, and about half were reported to have to displayed aggression to non-caregivers. Rates of aggression were higher among children who were younger, who had more restricted and repetitive behaviors, and who had more social communication difficulties (Kanne & Mazurek, 2011). Several other studies have also demonstrated a link between communication deficits and aggressive behavior in children with ASD (Boonen et al., 2014; Hartley et al., 2008) and are consistent with the notion that aggressive tendencies may serve a communicative function in children who lack more adaptive ways of communicating feelings of frustration and anger (Lindgren et al., 2020).
The negative association between aggression and social functioning is well documented in the literature on children who are typically developing (TD) (e.g., Evans et al., 2015). Children who engage in aggressive behavior are less likely to engage in prosocial behavior, are more likely to be perceived negatively by peers, and are more likely to have difficulty making friends (Ettekal & Ladd, 2015; Lansford et al., 2010). Aggressive behavior is especially likely to interfere with social functioning in a variety of ways for children with ASD. First, aggressive behavior in children with ASD tends to be more reactive than proactive in nature, thus more commonly arising in response to provocation than due to purposeful, goal-directed behavior (Farmer et al., 2015). As such, aggressive behavior in children with ASD may arise abruptly in social situations and may be difficult for others to anticipate. A child who becomes frustrated easily in social situations, such as those requiring sharing or flexibility, and escalates to verbally aggressive behavior (e.g., arguing, threatening) is likely to be viewed by others as difficult or hostile. Whether these situations involve peers, family members, or other adults, such experiences are likely to impact the quality of social interactions negatively and limit the child’s ability to maintain positive interpersonal relationships (Robb, 2010). In addition, aggressive behavior in children with ASD often takes physical forms (e.g., hitting, kicking) and can lead to injury of others (Farmer et al., 2015; McDougle et al., 2008). Physical aggression, which is reported in about 50% of children with ASD (Mazurek et al., 2013), is especially likely to place a strain on interpersonal relationships, including those within the family (Sikora et al., 2013) and with peers (Zaidman-Zait et al., 2021). Family and friends may limit or avoid interactions with children with ASD and aggression in response to physically aggressive behavior, resulting in decreased opportunities for them to engage with others and continue to build social adaptive skills.
Furthermore, when communication deficits accompany and/or give rise to aggressive behavior, children with ASD may be at a particularly heightened risk of social difficulties. When faced with a challenging social situation, children with communication deficits may experience added frustration resulting from difficulty articulating their wants and needs and, as a result, may engage in more aggressive forms of communication (e.g., yelling, hitting). These more aggressive forms of communication are likely not only to isolate others but also to be further compounded by a lack of social communication abilities (e.g., expressing regret, apologizing) that are integral to the development and maintenance of positive social relationships.
Despite the prevalence of aggressive behavior in children with ASD, only two studies have directly examined the link between aggressive behavior and social adaptive skills in this population. Mazurek and colleagues (2013), in their study of 1,584 children with ASD, reported that children with higher levels of physical aggression had lower Vineland-II Socialization scores (Mazurek et al., 2013). Similarly, in a study on the effect of parent training and risperidone on aggression in young children with ASD, Scahill and colleagues (2012) found that reductions in aggression were associated with gains in Vineland-II Socialization scores (Scahill et al., 2012).
Given the lack of research on aggression and social adaptive skills in children with ASD, further study of this issue is needed. First, a better understanding of the association between aggression and social functioning in ASD is likely to improve clinical conceptualizations of children with ASD who present with challenges in these areas. Second, increased awareness of the link between aggression and socialization is likely to contribute to more nuanced assessments of these challenges in ASD, with the potential for more targeted and useful interventions.
This study investigated the association between aggression and social adaptive behavior in a sample of children with ASD and co-occurring anxiety. Children with ASD and anxiety represent a valuable group in whom to examine this association for multiple reasons. First, due to the high prevalence of anxiety disorders in children with ASD, utilizing a sample of children with this set of comorbidities is likely to further understandings of aggression and adaptive behavior in a relevant population of children with ASD. Second, in children with ASD, high levels of anxiety and aggressive behavior tend to co-occur (Sullivan et al., 2019), and thus children with ASD and comorbid anxiety are more likely to display aggressive behavior pronounced enough to impact social adaptive behavior. As such, children with ASD and comorbid anxiety are a group of children from whom much can be learned regarding aggression and its impact on social adaptive skills. Furthermore, they are a subset of children who are at increased risk of challenges with aggression and its consequences for everyday functioning.
The first aim of this study was to examine the association between aggression and social adaptive behavior in children with ASD. It was predicted that aggression would be negatively associated with social adaptive behavior. The second aim was to examine the difference in social adaptive behavior between children with and without clinically significant levels of aggressive behavior. It was predicted that children with clinically significant levels of aggressive behavior would have lower levels of social adaptive behavior than those without clinically significant levels of aggression. The third aim was to examine the contributions of aggressive behavior and ASD diagnosis to social adaptive behavior. The existing sample of children with ASD was combined with a sample of TD children for this aim, to allow for examination of the contribution of ASD diagnosis to social adaptive behavior, both as separate from and in combination with aggressive behavior. It was predicted that both ASD diagnosis and aggressive behavior would influence social adaptive skills, with higher levels of aggressive behavior contributing to lower social adaptive skills above and beyond the effect of ASD diagnosis.
Method
Participants and Procedures
Participants were two groups of U.S. children (ages 8–15 years): 52 children with ASD and co-occurring anxiety disorders (ASD group) and 29 matched TD healthy controls (TD group). Children in the ASD and TD groups were matched by group at the time of recruitment based on age, gender, and IQ, as these characteristics may be related to the associations of ASD with adaptive functioning and comorbid disorders. Demographics and clinical characteristics are reported in the online supplemental material.
Autism spectrum disorder diagnosis was based on the Autism Diagnostic Interview–Revised (ADI-R; Le Couteur et al., 2003) and the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012) for children in the ASD group, and both measures were administered by a doctorate-level research-reliable clinician trained to fidelity. Full-scale IQ was measured using the Differential Ability Scales, Second Edition (DAS-II; Elliott, 2007) for children in both the ASD and TD groups. Full-scale IQ scores for all children ranged from 65 to 155 (M = 103.80, SD = 19.77). Co-occurring psychiatric disorders were assessed using the Anxiety Disorders Interview Schedule for Children and Parents (ADIS-C/P; Silverman & Albano, 1996) for children in both the ASD and TD groups. The ADIS was administered by a master’s level clinician with extensive expertise in childhood anxiety disorders and ADIS administration, with interrater reliability in the adequate to excellent range (Cohen’s κ, .62 to 1.0; Kalvin et al., 2020).
Social adaptive behavior was assessed using the Socialization domain of the Vineland Adaptive Behavior Scales, Third Edition (Vineland-3; Sparrow et al., 2016), administered via interview with the primary caregiver. Aggressive behavior was assessed using the Aggressive Behavior scale of the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001), completed via parent-report. Finally, anxiety was assessed using the Multidimensional Anxiety Scale for Children, Second Edition (MASC-2), completed via parent-report. A more detailed description of each of these measures, as well as the ADI-R and ADOS-2, can be found in the online supplemental material.
The parents of all children provided demographic and medical history information, participated in clinical assessments of children’s adaptive functioning, and completed questionnaires regarding children’s symptoms of aggressive behavior and anxiety.
Children in the ASD group were recruited from a U.S. university autism program and were seeking services for comorbid anxiety. All children in the ASD group participated in a study of cognitive behavioral therapy (CBT). The current study reported baseline data (i.e., data collected prior to study intervention) of these participants. Children in the TD group were recruited from the local community. Parents of all children provided written informed consent, and all children provided assent prior to data collection. To ensure data integrity and reliability, a trained research assistant reviewed and entered data on a customized clinical research platform (OnCore). The study principal investigator (PI) had regular meetings with the research assistant to review the quality of data entry and check for inconsistencies, omissions, and errors in the data. All study procedures were approved by the university Institutional Review Board and complied with ethical standards of the American Psychological Association.
Data Analyses
Data analyses were conducted using SPSS v24. Chi-square tests and t tests were conducted to examine group differences in demographic and clinical characteristics. Next, to examine the association between aggressive behavior and social adaptive skills in children with ASD, a zero-order correlation between CBCL Aggressive Behavior and Vineland-3 Socialization in the ASD group (n = 52) was conducted. Zero-order correlations between CBCL Aggressive Behavior, Vineland-3 Socialization, MASC-2 Total Anxiety, age, gender, IQ, and ASD symptom severity variables (measured by the ADOS-2 and ADI-R) were also conducted in this group to explore associations of aggressive behavior and social adaptive behavior with anxiety and demographic and clinical characteristics. Given the small sample size, this additional set of correlations was conducted for exploratory purposes and not corrected for multiple comparisons.
Children in the ASD group were divided into two groups to compare levels of social adaptive skills between children with ASD with and without clinically significant aggressive behavior. The two groups were children with CBCL Aggressive Behavior T scores ≥65 (n = 12) and children with CBCL Aggressive Behavior T scores <65 (n = 40). T scores ≥65 on the CBCL Aggressive Behavior scale represent 1.5 SDs above the mean and reflect a cutoff for clinically significant levels of aggressive behavior. An analysis of covariance (ANCOVA) was conducted to compare levels of social adaptive behavior between the high and low aggressive behavior groups, with IQ as a covariate and Vineland-3 Socialization as the dependent variable. Finally, a hierarchical linear regression predicting Vineland-3 Socialization was conducted in the full sample (ASD and TD groups, N = 81) to examine the contribution of aggressive behavior and ASD diagnosis to social adaptive behavior. Controlling for age and IQ, the effects of diagnostic group (ASD vs. TD) and CBCL Aggressive Behavior on Vineland-3 Socialization were examined.
Results
Analyses were conducted to examine group differences between the ASD and TD groups. There were no differences in age, gender, race, ethnicity, or IQ between children in the two groups. However, between the two groups, there were significant differences in aggressive behavior and anxiety, with higher scores in the ASD group, and in social adaptive skills, with higher scores in the TD group. Vineland Socialization scores in the TD group were on average 2 SDs above Vineland Socialization scores in the ASD group. Demographic and clinical characteristics of each group can be found in the online supplemental material.
Among children in the ASD group, aggressive behavior and social adaptive skills were negatively associated (r = −.35, p = .01). Age, gender, IQ, anxiety, and indices of ASD symptom severity were not associated with aggressive behavior or social adaptive behavior. These correlations are reported in the online supplemental material.
Children in the ASD group were divided into two subgroups representing those with and without clinically significant levels of aggressive behavior for the next set of analyses. Using the CBCL T score cutoff ≥65, 12 children had clinically significant levels of aggressive behavior (eight boys, four girls; CBCL Aggressive Behavior T-score M = 71.42, SD = 5.33), and 40 children had aggressive behavior below this threshold (30 boys, 10 girls; CBCL Aggressive Behavior T score M = 56.10, SD = 4.52). Children with ASD and clinically significant aggressive behavior had lower social adaptive skills than children with ASD without aggressive behavior. Specifically, children with ASD and clinically significant aggressive behavior had Vineland-3 Socialization scores (M = 60.37, SE = 4.30) that fell 10 points below the scores of children with ASD without aggressive behavior (M = 70.36, SE = 2.34), controlling for IQ, F = 4.13, p < .05, η2p =.78. This group difference in social adaptive skills is depicted in Figure 1.
Figure 1.
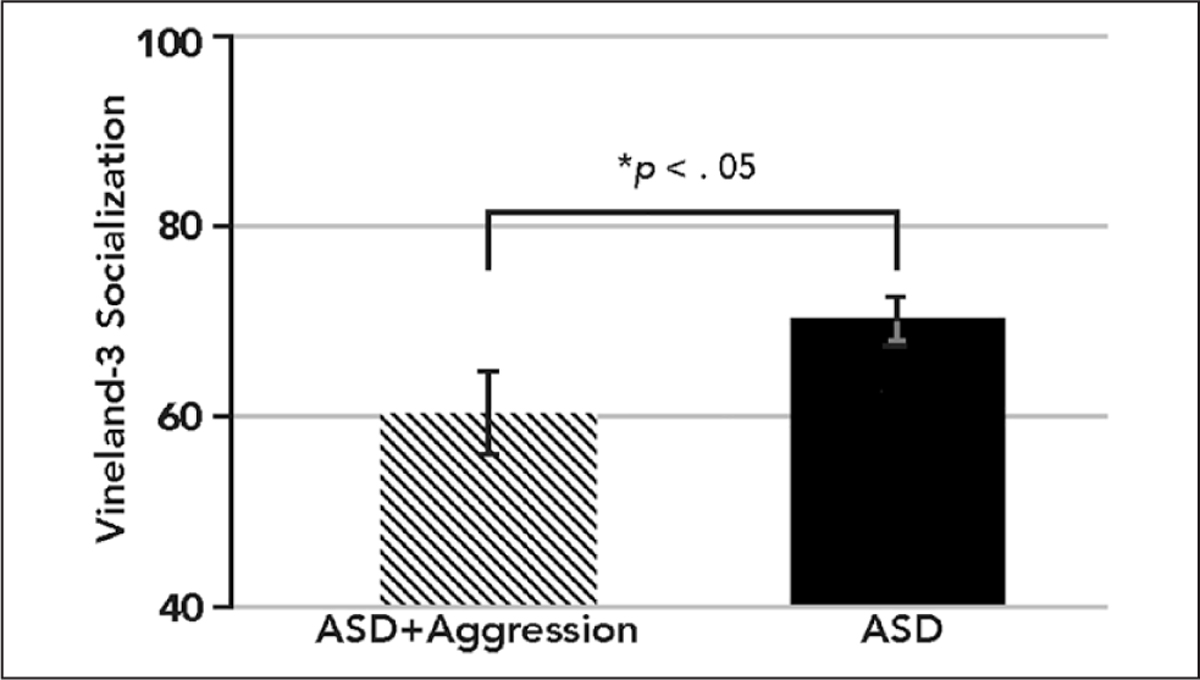
Vineland-3 Socialization Standard Scores in children with autism spectrum disorder (ASD) without aggressive behavior (n = 40) versus children with ASD and clinically significant aggressive behavior (ASD + Aggression; n = 12).
The hierarchical linear regression predicting Vineland-3 Socialization in the full sample was conducted in three steps. First, diagnostic group (ASD vs. TD) was entered in the first step. Age and IQ were entered in the second step to control for heterogeneity conferred by these variables. Finally, to examine the effect of aggressive behavior on social adaptive skills, aggressive behavior was entered in the third step. The results of these analyses are presented in Table 1. Diagnostic group significantly contributed to the model and accounted for 46% of the variance in Vineland-3 Socialization scores, with status in the ASD (vs. TD) group associated with lower Socialization scores (β = −.68, p < .001). Aggressive behavior negatively predicted social adaptive skills after accounting for diagnostic group, age, and IQ, with aggressive behavior accounting for 4% of the variance in Vineland-3 Socialization scores (β = −.24, p < .05). Overall, this pattern of results signifies that, over and above the effects of ASD diagnosis, age, and IQ, higher levels of aggressive behavior contribute to lower levels of adaptive functioning in the area of Socialization.
Table 1.
Hierarchical Regression Analysis of Socialization as a Function of Aggressive Behavior in the Total Sample.
| Variable | R2 | β | ΔF |
|---|---|---|---|
|
| |||
| Step 1 | .46 | 68.15*** | |
| Diagnostic group | −.68*** | ||
| Step 2 | .47 | .40 | |
| Age | −.05 | ||
| IQ | .05 | ||
| Step 3 | .51 | 6.16* | |
| Aggressive behavior | −.24* | ||
Note. Sample N = 81. Diagnostic group = ASD (autism spectrum disorder) group versus TD (typically developing) group.
p < .05.
p < .001.
Discussion
This study examined social adaptive behavior and its association with aggression in a sample of children with ASD. Consistent with previous research conducted with the earlier, second edition of the Vineland (Kanne et al., 2011), children with ASD in this sample had social adaptive skills 2 SDs below the population mean, reflecting significant impairment. This finding underscores the prominent difficulties that children with ASD, including those with intellectual abilities in the average range, have in the area of daily social functioning (Klin et al., 2007; Pugliese et al., 2015).
The first aim of the study was to examine the association between aggression and social adaptive behavior in children with ASD. As expected, aggressive behavior and social adaptive skills demonstrated a moderate negative association. That is, among the children in this sample with ASD, children with higher levels of aggressive behavior demonstrated lower social adaptive behavior. This finding is consistent with research documenting a negative association between aggressive behavior and adaptive functioning in children with ASD (Farmer et al., 2015; Stringer et al., 2020), suggesting that elevated levels of aggressive behavior may limit the ability of children with ASD to function independently and effectively in their daily lives. Furthermore, the present findings specifically indicate that aggressive behavior is associated with lower levels of functioning in the area of social adaptive behavior and parallel findings from the study conducted by Mazurek and colleagues (2013) documenting a negative association between physical aggression and social adaptive skills, measured with Vineland-II, in children with ASD (Mazurek et al., 2013). Given that aggressive behavior occurs in about half of children with ASD (Mayes et al., 2012), this association between aggression and social adaptive skills is an important finding that warrants attention.
The second aim of the study was to examine the difference in social adaptive behavior between children with ASD with and without co-occurring aggressive behavior. Consistent with expectations, children with ASD and clinically significant levels of aggressive behavior demonstrated lower social adaptive skills than children with ASD without clinically significant levels of aggressive behavior, controlling for IQ. Specifically, while children with ASD without aggressive behavior had social adaptive skills about 2 SDs below the population mean, children with ASD with aggressive behavior had social adaptive skills about 2.66 SDs below the population mean. Furthermore, the results indicate that the difference in social adaptive behavior between these two subgroups could not be accounted for by intellectual ability. This finding builds upon our previous finding by indicating not only that higher levels of aggression are associated with lower social adaptive skills among children with ASD, but specifically that, among this population, clinically elevated levels of aggression are associated with substantial impairment in social adaptive skills.
Although little research has examined the specific link between aggression and social adaptive functioning, measured with the Vineland, in children with ASD, the problematic features and potential consequences of aggressive behavior in ASD are well documented and shed light on our current findings. Aggressive behavior among children with ASD is often more reactive than proactive (Farmer et al., 2015) and occurs in social contexts, thus making it difficult for children with ASD to sustain positive daily social interactions (e.g., playing a game with peers, engaging in an ongoing conversation). In addition, aggressive behavior in children with ASD may be physical in nature, which can be threatening and/or injurious to others (Farmer et al., 2015; McDougle et al., 2008), making it challenging for children with ASD and aggression to maintain positive interpersonal relationships, both in and outside of the family (Robb, 2010; Sikora et al., 2013). Furthermore, among children with ASD who already have difficulties with social communication and interaction, the presence of aggressive behavior and its consequences may make it more challenging to navigate interpersonal interactions independently. A child with ASD who often becomes upset and aggressive when plans with peers do not go as anticipated, for example, might necessitate adult support during peer engagements to engage with peers more adaptively. Tendencies toward aggressive behavior are likely to be problematic especially for children with clinically significant aggressive behavior that is beyond the normative range, as such behavior is likely to compromise children’s ability to interact competently with others and in ways commensurate with same-age peers.
The third aim of the study was to examine contributions of aggressive behavior and ASD diagnosis to social adaptive skills in a combined sample of children with ASD and TD children. Consistent with expectations, while ASD diagnosis was associated with lower social adaptive skills, aggressive behavior was negatively associated with social adaptive skills after accounting for ASD diagnosis. These findings suggest that, while having ASD places children at risk of lower social adaptive skills, aggressive behavior may influence social adaptive behavior negatively in ways not accounted for by ASD alone. Taken together with the previous finding demonstrating that children with ASD and aggressive behavior had lower Vineland Socialization scores relative to children with ASD without aggressive behavior, these results underscore the way in which children with ASD plus high levels of aggression are at particularly elevated risk of impairment in social adaptive skills. Together, these findings parallel prior research documenting poorer daily social functioning in children with ASD (Kenworthy et al., 2010), as well as in children with ASD and aggressive behavior (Mazurek et al., 2013). In addition, the present finding that aggression is negatively associated with social adaptive skills in this combined ASD and TD sample, above and beyond ASD diagnosis, suggests that aggression may be problematic for social functioning not only in children with ASD, but also in TD children. That aggressive behavior is associated with poorer social functioning for children without ASD is consistent with research highlighting the link between aggression and social difficulties, such as peer rejection, in TD youth (Lansford et al., 2010).
The results from this study extend previous research in several ways. Most studies on aggressive behavior and adaptive functioning in children with ASD to date have looked at adaptive skills broadly using the Vineland-II or Vineland-3 Adaptive Behavior Composite (Farmer et al., 2015; Stringer et al., 2020) and have not individually examined the domain of social adaptive behavior. Given that social adaptive skills represent the area of adaptive functioning which is most impaired in children with ASD (Klin et al., 2007; Pugliese et al., 2015), better understanding of the link between aggressive behavior and social adaptive skills in particular is important. This study adds to the literature in this area by specifically demonstrating a link between aggressive behavior and impaired social adaptive behavior, measured via Vineland Socialization scores, in a sample of children with ASD.
This study also adds to the literature on aggression and social adaptive functioning in children with ASD by utilizing a sample of children with comorbid anxiety disorders, which is a common co-occurring condition in children with ASD (van Steensel & Heeman, 2017) that may heighten the risk of aggressive behavior. Heightened levels of anxiety and aggressive behavior tend to co-occur in children with ASD (Sullivan et al., 2019), and the presence of comorbid anxiety and disruptive behaviors has been linked to higher levels of functional impairment in this population (Storch et al., 2012). However, despite research linking anxiety to aggression and impairment in children with ASD, it is noteworthy that in the sample of children with ASD in this study, anxiety, as measured by MASC-2 parent ratings, was not associated with CBCL parent ratings of aggressive behavior or Vineland Socialization scores. Future studies are needed to continue to explore potential associations of anxiety with aggression and social adaptive behavior in children with ASD.
The present findings have notable implications for clinical practice. First, that aggressive behavior was associated with lower social adaptive skills in this study suggests the potential utility of assessing problems in both of these areas (i.e., aggression, social functioning) when problems in one area are present. If a clinician is conducting an assessment of a child with ASD who has difficulty sustaining positive interactions with family members and peers, for example, it may be helpful for the clinician to gather information about potential aggressive behavior. Similarly, when assessment of problem behavior occurs in the school setting, it may be helpful to expand the scope of the assessment to include information gathering about social functioning. If a school psychologist is observing a child during a daily lesson to collect data on the child’s aggressive behaviors in the classroom, it could be helpful to observe less structured social situations, such as lunch or recess, to learn about the child’s social adaptive skills. Even if the aggressive behavior appears to be unique to the classroom setting, by expanding the assessment to include a wider range of social interactions, additional information about aggressive behaviors and associations with social functioning may be gleaned. Furthermore, when assessing aggressive behavior, including an assessment of the social contextual factors (e.g., type of social interaction, people present, demands of social situation, predictably of social situations/routines) that coincide with aggression is likely to enhance understanding of the aggressive behavior and inform the development of treatment plans aimed at preventing and reducing aggression and replacing it with more adaptive behavior.
When a child exhibits both aggressive behavior and delays in social adaptive functioning, clinical interventions aimed at the reduction of aggressive behavior may aid in the promotion of social adaptive functioning. Behavioral interventions for childhood aggressive behavior, including parent training (Bearss et al., 2015) and CBT (Sukhodolsky & Scahill, 2012), may be useful in this capacity. Scahill and colleagues’ (2012) study of parent training, which emphasizes the reinforcement of appropriate, non-aggressive behaviors, found that children with ASD demonstrated improvements in social adaptive skills that were directly associated with reductions in aggression (Scahill et al., 2012).
When aggressive behavior in children with ASD is associated with communication deficits, interventions focusing on the development of functional communicative skills, such as functional communication training (Carr & Durand, 1985), are likely to be helpful. Functional communication training, which is an intervention that teaches children new communication strategies with which to replace problem behavior (Chezan et al., 2018; Wu et al., 2022), has been widely used in children with ASD (Lindgren et al., 2020; Reichle & Wacker, 2017). When a child engages in aggressive behavior that serves a communicative function (e.g., hitting a parent who takes away a toy communicates the message “I do not like what you are doing!”), replacing the aggressive behavior with more appropriate forms of communicative behavior (e.g., using the words “I do not like that” or “I want my toy” to communicate this message) is likely to augment the development of more adaptive social behaviors.
The results of this study also suggest that interventions for enhancing social functioning in children with ASD, such as social skills training, may be augmented by including a focus on aggressive behavior. Furthermore, when different service providers are delivering interventions focused on aggressive behavior and social adaptive skills separately, collaboration between providers is likely to enhance the treatment plan across settings. When a child with ASD is receiving social skills training in school and attending outpatient CBT for aggressive behaviors at home, for example, collaboration between the providers might result in a plan to replace aggressive behaviors at home with specific social skills taught at school. Similarly, strategies used for the prevention of aggressive behavior at home may be used to augment the utilization of social skills with peers in the classroom.
Several limitations of this study warrant attention. First, the study sample, and the TD subsample in particular, was small in size, as the ability to recruit TD participants was limited by budgetary considerations. This small sample size limited the power to detect effects. Future studies should include larger samples to continue to examine the association between aggression and social adaptive skills in children with ASD. Second, children with ASD who participated in this study were seeking clinical services for comorbid anxiety at a specialty autism program. While children with ASD and comorbid anxiety are more likely to have aggressive behaviors and thus represent an important group for studying co-occurring concerns such as aggression, the current findings may not generalize to non-treatment-seeking populations. Third, boys constituted the majority of the current sample, and thus the extent to which the present findings generalize to girls with ASD is uncertain. Fourth, the children in this sample were predominately White, and the results may not generalize to other racial and ethnic groups. Fifth, while aggression and social adaptive skills were treated as independent constructs, there is likely some conceptual overlap between the two constructs. Aggressive behavior, for example, may be seen as the outcome of a social skill deficit in certain social situations (e.g., a child who is waiting in line for a snack shoves the child in front of him because he has not learned how to wait his turn). Nevertheless, as evidenced by socially skilled children who engage in aggression, as well as non-aggressive children with social skill deficits, aggression and social adaptive behavior are best understood as distinct, albeit associated, dimensions.
Relatedly, while not included in the present analyses, communication abilities represent another construct which may be associated with aggression and social adaptive behavior in children with ASD. Future studies of aggressive behavior in children with ASD should include developmentally appropriate measures of communication. Finally, given the study’s cross-sectional design, definitive conclusions about the direction of the association between aggressive behavior and social adaptive skills are precluded. While the current findings were interpreted to suggest that aggressive behavior contributes to poorer social functioning, it is also plausible that deficits in social skills may render children unequipped to deal with social challenges in prosocial ways (e.g., talking, negotiating) and thus heighten the likelihood of engagement in aggressive responses. Longitudinal studies are warranted to better explain the direction of effects between aggression and social functioning in children with ASD over time.
This study adds to the limited literature on aggressive behavior and social adaptive functioning in children with ASD. Results indicated that aggression is negatively associated with social adaptive skills and that children with ASD with clinically significant aggressive behavior demonstrate particularly low levels of social adaptive skills relative to children with ASD without aggressive behavior. In addition, higher levels of aggressive behavior are associated with reduced social adaptive skills, above and beyond the effects of ASD diagnosis, age, and IQ. Findings underscore the potentially negative effects of aggressive behavior on social adaptive skills in children with ASD and suggest that addressing aggressive behavior is likely to aid in the promotion of social functioning in this population.
Supplementary Material
Funding
This work was supported by National Institute of Child Health and Human Development (NICHD) grant R01HD083881 (D.G.S.). C.B.K. is a Fellow of the Translational Developmental Neuroscience Training Program (T32 MH18268) directed by Dr. Michael Crowley.
Footnotes
Declaration of Conflicting Interests
Dr. Sukhodolsky receives royalties from Guilford Press for a treatment manual on CBT for anger and aggression in children. Other authors (C.B.K., R.J., S.R., A.L.W. and K.I.) have no biomedical financial interests or potential conflicts of interest to declare related to this study.
Supplemental Material
Supplemental material for this article is available on the Focus on Autism website with the online version of this article.
References
- Achenbach TM, & Rescorla LA (2001). Manual for the ASEBA school-age forms & profiles: An integrated system of multi-informant assessment. University of Vermont, Research Center for Children, Youth, & Families. [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). [Google Scholar]
- Bearss K, Johnson C, Smith T, Lecavalier L, Swiezy N, Aman M, . . . Minshawi, N. (2015). Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: A randomized clinical trial. Journal of the American Medical Association, 313(15), 1524–1533. 10.1001/jama.2015.3150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boonen H, Maljaars J, Lambrechts G, Zink I, Van Leeuwen K, & Noens I (2014). Behavior problems among school-aged children with autism spectrum disorder: Associations with children’s communication difficulties and parenting behaviors. Research in Autism Spectrum Disorders, 8(6), 716–725. 10.1016/j.rasd.2014.03.008 [DOI] [Google Scholar]
- Brotman MA, Kircanski K, & Leibenluft E (2017). Irritability in children and adolescents. Annual Review of Clinical Psychology, 13, 317–341. 10.1146/annurev-clinpsy-032816-044941 [DOI] [PubMed] [Google Scholar]
- Carr EG, & Durand VM (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, 18, 111–126. 10.1901/jaba.1985.18-111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chezan LC, Wolfe K, & Drasgow E (2018). A meta-analysis of functional communication training effects on problem behavior and alternative communicative responses. Focus on Autism and Other Developmental Disabilities, 33(4), 195–205. 10.1177/1088357617741294 [DOI] [Google Scholar]
- Elliott CD (2007). The Differential Abilities Scales, Second Edition (DAS-II). Pearson Education. [Google Scholar]
- Ettekal I, & Ladd GW (2015). Developmental pathways from childhood aggression–disruptiveness, chronic peer rejection, and deviant friendships to early-adolescent rule breaking. Child Development, 86(2), 614–631. 10.1111/cdev.12321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans SC, Fite PJ, Hendrickson ML, Rubens SL, & Mages AK (2015). The role of reactive aggression in the link between hyperactive–impulsive behaviors and peer rejection in adolescents. Child Psychiatry & Human Development, 46(6), 903–912. 10.1007/s10578-014-0530-y [DOI] [PubMed] [Google Scholar]
- Farmer C, Butter E, Mazurek MO, Cowan C, Lainhart J, Cook EH, . . . Aman M. (2015). Aggression in children with autism spectrum disorders and a clinic-referred comparison group. Autism, 19(3), 281–291. 10.1177/1362361313518995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartley SL, Sikora DM, & McCoy R (2008). Prevalence and risk factors of maladaptive behaviour in young children with autistic disorder. Journal of Intellectual Disability Research, 52(10), 819–829. 10.1111/j.1365-2788.2008.01065.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalvin CB, Marsh CL, Ibrahim K, Gladstone TR, Woodward D, Grantz H, . . . Sukhodolsky DG. (2020). Discrepancies between parent and child ratings of anxiety in children with autism spectrum disorder. Autism Research, 13(1), 93–103. 10.1002/aur.2220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kanne SM, Gerber AJ, Quirmbach LM, Sparrow SS, Cicchetti DV, & Saulnier CA (2011). The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. Journal of Autism and Developmental Disorders, 41(8), 1007–1018. 10.1007/s10803-010-1126-4 [DOI] [PubMed] [Google Scholar]
- Kanne SM, & Mazurek MO (2011). Aggression in children and adolescents with ASD: Prevalence and risk factors. Journal of Autism and Developmental Disorders, 41(7), 926–937. 10.1007/s10803-010-1118-4 [DOI] [PubMed] [Google Scholar]
- Kenworthy L, Case L, Harms MB, Martin A, & Wallace GL (2010). Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 40(4), 416–423. 10.1007/s10803-009-0911-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klin A, Saulnier CA, Sparrow SS, Cicchetti DV, Volkmar FR, & Lord C (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal of Autism and Developmental Disorders, 37(4), 748–759. 10.1007/s10803-006-0229-4 [DOI] [PubMed] [Google Scholar]
- Lansford JE, Malone PS, Dodge KA, Pettit GS, & Bates JE (2010). Developmental cascades of peer rejection, social information processing biases, and aggression during middle childhood. Development and Psychopathology, 22(3), 593–602. 10.1017/S0954579410000301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lecavalier L, McCracken CE, Aman MG, McDougle CJ, McCracken JT, Tierney E, . . . Scahill L. (2019). An exploration of concomitant psychiatric disorders in children with autism spectrum disorder. Comprehensive Psychiatry, 88, 57–64. 10.1016/j.comppsych.2018.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Couteur A, Lord C, & Rutter M (2003). The autism diagnostic interview-revised (ADI-R). Western Psychological Services. [Google Scholar]
- Lindgren S, Wacker D, Schieltz K, Suess A, Pelzel K, Kopelman T, . . . O’Brien M. (2020). A randomized controlled trial of functional communication training via telehealth for young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50 (12), 4449–4462. 10.1007/s10803-020-04451-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore PC, Risi S, Gotham K, & Bishop SL (2012). Autism diagnostic observation schedule: ADOS-2. Western Psychological Services. [Google Scholar]
- Mayes SD, Calhoun SL, Aggarwal R, Baker C, Mathapati S, Anderson R, & Petersen C (2012). Explosive, oppositional, and aggressive behavior in children with autism compared to other clinical disorders and typical children. Research in Autism Spectrum Disorders, 6(1), 1–10. 10.1016/j.rasd.2011.08.001 [DOI] [Google Scholar]
- Mazurek MO, Kanne SM, & Wodka EL (2013). Physical aggression in children and adolescents with autism spectrum disorders. Research in Autism Spectrum Disorders, 7(3), 455–465. 10.1016/j.rasd.2012.11.004 [DOI] [Google Scholar]
- McDougle CJ, Stigler KA, Erickson CA, & Posey DJ (2008). Atypical antipsychotics in children and adolescents with autistic and other pervasive developmental disorders. The Journal of Clinical Psychiatry, 69, 15–20. 10.1007/s00213-013-3068-y [DOI] [PubMed] [Google Scholar]
- Pugliese CE, Anthony L, Strang JF, Dudley K, Wallace GL, & Kenworthy L (2015). Increasing adaptive behavior skill deficits from childhood to adolescence in autism spectrum disorder: Role of executive function. Journal of Autism and Developmental Disorders, 45(6), 1579–1587. 10.1007/s10803-014-2309-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reichle J, & Wacker D (2017). Functional communication training for problem behavior. Guilford Press. [Google Scholar]
- Robb AS (2010). Managing irritability and aggression in autism spectrum disorders in children and adolescents. Developmental Disabilities Research Reviews, 16(3), 258–264. 10.1002/ddrr.118 [DOI] [PubMed] [Google Scholar]
- Scahill L, McDougle CJ, Aman MG, Johnson C, Handen B, Bearss K, . . . Arnold LE. (2012). Effects of risperidone and parent training on adaptive functioning in children with pervasive developmental disorders and serious behavioral problems. Journal of the American Academy of Child & Adolescent Psychiatry, 51(2), 136–146. 10.1016/j.jaac.2011.11.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sikora D, Moran E, Orlich F, Hall TA, Kovacs EA, Delahaye J, . . . Kuhlthau K. (2013). The relationship between family functioning and behavior problems in children with autism spectrum disorders. Research in Autism Spectrum Disorders, 7(2), 307–315. 10.1016/j.rasd.2012.09.006 [DOI] [Google Scholar]
- Silverman W, & Albano AM (1996). Anxiety disorders interview schedule for DSM-IV, child version. Oxford University Press. [Google Scholar]
- Sparrow SS, Cicchetti DV, & Balla DA (2005). Vineland adaptive behavior scales, second edition (Vineland-II). Pearson Clinical Assessment. [Google Scholar]
- Sparrow SS, Cicchetti DV, & Saulnier CA (2016). Vineland adaptive behavior scales, third edition (Vineland-3). Pearson Clinical Assessment. [Google Scholar]
- Storch EA, Arnold EB, Jones AM, Ale CM, Wood JJ, Ehrenreich-May J, . . . Murphy TK. (2012). The role of co-occurring disruptive behavior in the clinical presentation of children and adolescents with anxiety in the context of autism spectrum disorders. Child Psychiatry and Human Development, 43, 734–746. 10.1007/s10578-012-0294-1 [DOI] [PubMed] [Google Scholar]
- Stringer D, Kent R, Briskman J, Lukito S, Charman T, Baird G, . . . Simonoff E. (2020). Trajectories of emotional and behavioral problems from childhood to early adult life. Autism, 24(4), 1011–1024. 10.1177/1362361320908972 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sukhodolsky DG, Gladstone TR, Marsh CL, & Cimino KR (2019). Behavioral interventions for irritability in children and adolescents. In Roy AK, Brotman M, & Leibenluft E(Eds.), Irritability in pediatric psychopathology (pp. 255–275). Oxford University Press. [Google Scholar]
- Sukhodolsky DG, & Scahill L (2012). Cognitive-behavioral therapy for anger and aggression in children. Guilford Press. [Google Scholar]
- Sullivan MO, Gallagher L, & Heron EA (2019). Gaining insights into aggressive behaviour in autism spectrum disorder using latent profile analysis. Journal of Autism and Developmental Disorders, 49, 4209–4218. 10.1007/s10803-019-04129-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomaszewski B, Hepburn S, Blakeley-Smith A, & Rogers SJ (2020). Developmental trajectories of adaptive behavior from toddlerhood to middle childhood in autism spectrum disorder. American Journal on Intellectual and Developmental Disabilities, 125(3), 155–169. 10.1352/1944-7558-125.3.155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Steensel FJA, & Heeman EJ (2017). Anxiety levels in children with autism spectrum disorder: A meta-analysis. Journal of Child and Family Studies, 26(7), 1753–1767. 10.1007/s10826-017-0687-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu J, Kopelman TG, & Miller K (2022). Using functional communication training to reduce problem behavior. Intervention in School and Clinic, 57, 343–347. 10.1177/10534512211032628 [DOI] [Google Scholar]
- Zaidman-Zait A, Mirenda P, Szatmari P, Duku E, Smith IM, Zwaigenbaum L, . . . Waddell C. (2021). Profiles and predictors of academic and social school functioning among children with autism spectrum disorder. Journal of Clinical Child & Adolescent Psychology, 50, 656–668. 10.1080/15374416.2020.1750021 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.