

The 22q11.2 region is known to be susceptible to chromosomal rearrangements, such as microdeletion and microduplications. Microduplication syndrome manifests with a spectrum of presentations, ranging from normal to severely affected phenotypes. 1 , 2 Dystonia has not been previously reported in association with this syndrome. In this letter, we describe a case of an 8‐year‐old girl who presented with severe generalized dystonia that significantly impaired her quality of life. Genetic investigations identified 22q11.2 microduplication as the underlying etiology. Treatment with medications was ineffective, and thus the patient underwent deep brain stimulation (DBS) targeting the globus pallidus pars interna (GPi), resulting in favorable outcomes. This letter expands the microduplication syndrome phenotype and highlights DBS's potential role in future cases.
This letter pertains to an 8‐year‐old female who was born via C‐section at 36 weeks of gestation and was discharged on the third day after delivery. The patient had been in good health until she reached the age of 1 month when she developed dystonic movements in her neck. The symptoms worsened by the age of 6 months and began to involve her arms and hands, causing gross and fine motor developmental delays. She was not able to sit or stand unsupported, and never achieved autonomous gait.
Her dystonia progressed over the next few years and she became wheelchair‐bound, by the age of 5 years old, without any functional use of her hands. Her speech was affected, but no swallowing concerns. No family history was reported. Her neurological exam showed right‐sided neck torticollis and generalized dystonia, affecting the left side of her body more than the right. The movement sub‐score of the Burke‐Fahn‐Marsden Dystonia Rating Scale 3 was 72/120 (Appendix S2). The patient did not exhibit any dysmorphic features or systemic manifestations (Video 1).
Video 1.
Pre‐DBS activation. DBS, deep brain stimulation.
Her basic blood work and metabolic screening came back normal. An MRI of her brain showed no abnormalities, but genetic testing using microarray technology revealed a microduplication at 22q11.2 (2.8 Mb in one copy of chromosome 22q at band 22q11.21.). A genetic dystonia panel (GeneDx) was negative (Appendix S1), and levodopa treatment did not significantly improve her dystonia.
At 7 years of age, the patient underwent bilateral (GPi DBS, Fig. 1). Following surgery, she looked well, the mobile component of the dystonia improved significantly in the upper and lower extremities allowing for a bit more balanced and coordinated movements, (Video 2). The DBS settings were adjusted with ventral contacts being the most effective for her symptoms (Appendix S3).
Figure 1.
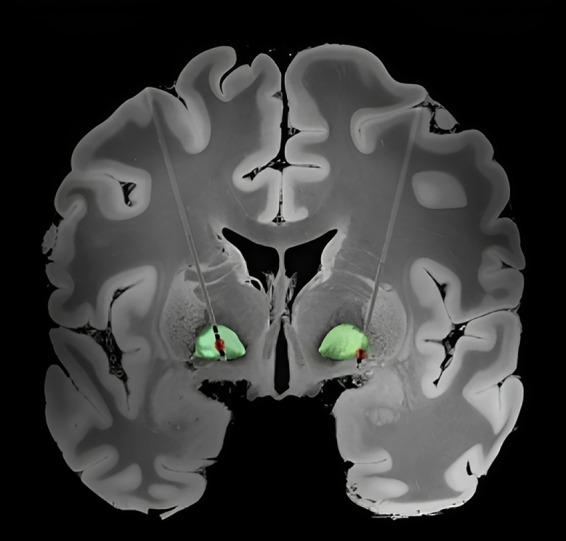
Anatomical lead localization and volume of tissue activated (VTA). The Lead‐DBS anatomical localization of implanted leads in the globus pallidus internus (GPi) for the patient. 3D reconstruction of the DBS leads was illustrated on a 100‐micron resolution, 7.0 Tesla FLASH brain in MNI152 space30. The green highlighted structure is the GPi based on the DISTAL atlas within Lead‐DBS. VTA (red) is shown based on the stimulation settings 1 year after the DBS surgery. 5
Video 2.
Post DBS. DBS, deep brain stimulation.
During the patient\s subsequent clinical encounters, and within the first 3–4 months, an amelioration of 30% was observed in the movement sub‐score of the BFMDRS scale, which now scored 50 out of 120 (Appendix S2). The patient exhibited enhanced speech clarity, augmented ambulatory capability like walking a few steps with support, and an ability to perform jumping movements. Moreover, the patient demonstrated increased manual dexterity and fine motor skills, as evidenced by her ability to operate buttons with her right hand, and to perform drawing with her toes. The evaluation of the patient's quality of life utilizing the Pediatric Quality of Life Inventory 4 showed an improvement from a baseline score of 47 to 80 one‐year post‐DBS (Video 2).
Microduplication of the 22q11.2 region refers to the presence of an additional copy at position q11.2 on chromosome 22. This condition typically presents with a broad range of symptoms, ranging from mild to severe phenotypes, such as intellectual disabilities, delayed psychomotor development, and hypotonia. Additionally, various anomalies have been associated with this condition, including hypertelorism, hearing impairment, velopharyngeal insufficiency, and seizures. 1 Recently, some literature has suggested a higher prevalence of autism spectrum and psychiatric disorders among the affected patients. 6 , 7 However, to the best of our knowledge, there have been no prior reports of dystonia associated with microduplication of 22q11.2, highlighting the importance of microarray analysis in children with suspected genetic dystonia.
There appear to be some similarities between microdeletion and microduplication syndromes. Microdeletion of 22q11.2 is a well‐established condition, characterized by a variety of dysmorphic features and involvement of multiple organ systems, including cardiovascular, endocrine, immune, psychiatric, and neurological systems. 2 Parkinson's disease and dystonia have been reported as potential associations with the condition, 8 whereas 22q11.2 duplication syndrome is more associated with hypotonia. Although our patient exhibited a relatively large duplication, her clinical presentation was limited to generalized dystonia.
Interestingly, the genes situated in the 22q11.2 region that could potentially play a role in the development of abnormal movements, include DGCR8, microRNA‐185, SEPT5, and COMT. 9
DBS has become increasingly popular in the pediatric population over the past decade, particularly in cases of genetic dystonias such as DYT‐TOR1A and DYT‐KMT2B, which have shown favorable clinical outcomes in studies. There are few reports suggesting the potential utility of DBS in ultra‐rare conditions similar to the case here. 10 Further studies are necessary to investigate the effectiveness and safety of DBS in these rare conditions and to determine the most appropriate patient selection criteria and long‐term outcomes.
Author Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript: A. Writing of the first draft, B. Review and Critique.
H.A.: 3A
S.B.: 3B.
N. W.: 3B.
A.F.: 3B.
G.I.:3B.
C.G.: 1A, 1B, 1C.
Disclosures
Ethical Approval: We confirm that the approval of an institutional review board was not required for this work, and an informed consent was obtained. Also, we confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflicts of Interest: We declare that there are no conflicts of interest relevant to this work.
Financial Disclosures for the Previous 12 Months: We declare that there are no additional disclosures to report.
Supporting information
Appendix S1. Supporting Information.
Acknowledgments
We wish to thank the health care providers who assisted in caring for this individual as well as the patient and his family.
References
- 1. Piccione M, Vecchio D, Cavani S, Malacarne M, Pierluigi M, Corsello G. The first case of myoclonic epilepsy in a child with a de novo 22q11.2 microduplication. Am J Med Genet A 2011;155(12):3054–3059. [DOI] [PubMed] [Google Scholar]
- 2. Ensenauer RE, Adeyinka A, Flynn HC, et al. Microduplication 22q11.2, an emerging syndrome: clinical, cytogenetic, and molecular analysis of thirteen patients. Am J Hum Genet 2003;73(5):1027–1040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kuiper MJ, Vrijenhoek L, Brandsma R, et al. The burke‐Fahn‐Marsden dystonia rating scale is age‐dependent in healthy children. Mov Disord Clin Pract 2016;3(6):580–586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Smyth M, Jacobson K. Paediatric quality of life inventory™ version 4.0 short form generic core scale across pediatric populations review data. Data Brief 2021;24(39):107599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Horn A, Li N, Dembek TA, et al. Lead‐DBS v2: towards a comprehensive pipeline for deep brain stimulation imaging. Neuroimage 2019;1(184):293–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Wenger TL, Miller JS, DePolo LM, et al. 22q11.2 duplication syndrome: elevated rate of autism spectrum disorder and need for medical screening. Mol Autism 2016;6(7):27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hoeffding LK, Trabjerg BB, Olsen L, et al. Risk of psychiatric disorders among individuals with the 22q11.2 deletion or duplication: a Danish Nationwide, register‐based study. JAMA Psychiatry 2017;74(3):282–290. [DOI] [PubMed] [Google Scholar]
- 8. Bayat M, Bayat A. Neurological manifestation of 22q11.2 deletion syndrome. Neurol Sci 2022;43(3):1695–1700. [DOI] [PubMed] [Google Scholar]
- 9. Butcher NJ, Kiehl T, Hazrati L, et al. Association between early‐onset Parkinson disease and 22q11 deletion syndrome. JAMA Neurol 2013;70:1359e1366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Beaulieu‐Boire I, Aquino CC, Fasano A, et al. Deep brain stimulation in rare inherited Dystonias. Brain Stimul 2016;9(6):905–910. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Supporting Information.