

Abstract
The traditional Chinese herb hawthorn is gaining attention for its potential to lower lipid levels due to its active components that positively influence lipid metabolism. Our meta-analysis of fourteen randomized controlled trials compared traditional Chinese medicine containing hawthorn with conventional lipid-lowering drugs for hyperlipidemia. Hawthorn-based medicine showed promise in reducing total cholesterol and triglycerides while increasing high-density lipoprotein cholesterol levels, albeit less effective than standard drugs in lowering low-density lipoprotein cholesterol. However, caution is needed due to methodological limitations in some trials, emphasizing the importance of further well-designed studies to clarify hawthorn’s efficacy in managing hyperlipidemia.
Keywords: hyperlipidemias, meta-analysis, traditional Chinese medicine, hawthorn
Introduction
Hyperlipidemia involves an imbalance in cholesterol levels, including low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) in the blood. LDL-C and HDL-C regulate the body’s cholesterol content, and an imbalance can increase the risk of cardiovascular diseases, including myocardial infarction and stroke. Other forms of hyperlipidemia include hypertriglyceridemia and mixed hyperlipidemia, where both cholesterol and triglyceride levels are elevated. An increase in LDL-C may lead to the accumulation of plaques in the arteries and is associated with an increased risk of atherosclerotic cardiovascular diseases (ASVD), including coronary artery disease or stroke. This underscores the importance of managing hyperlipidemia to maintain a balanced cholesterol level, thereby reducing the risk of cardiovascular diseases. Timely interventions, through lifestyle changes and medication, are crucial for managing hyperlipidemia and preserving cardiovascular health.1 In the United States, over 100 million people (approximately 53% of the adult population) have elevated LDL-C levels. However, fewer than 50% of individuals with elevated LDL-C receive treatment to lower their levels, and among those undergoing treatment, less than 35% achieve appropriate control. Additionally, around 31 million American adults have total cholesterol levels exceeding 240 mg/dL, putting them at about twice the risk compared to those who have achieved their target cholesterol levels. These statistics highlight the widespread prevalence of elevated cholesterol levels in the U.S. population and underscore the need for improved management and control to mitigate the associated health risks.2,3
Seven statins are presently FDA-approved for hyperlipidemia treatment in conjunction with a heart-healthy diet. In general, statins can lower LDL-C by approximately 20% to 65%, with more significant reductions observed with atorvastatin, rosuvastatin, and pitavastatin; moderate decreases with lovastatin and simvastatin; and the smallest decreases with fluvastatin and pravastatin.4–11 Except for pitavastatin, all have indications for patients with FH. While statins are generally well tolerated, they are linked to various adverse effects, including gastrointestinal events, musculoskeletal pain, respiratory infections, and headaches.4–11 Consequently, researchers have been actively seeking better, safer, and more natural alternatives.
For thousands of years, Eastern countries have been using herbal medicine to treat diseases. In the past two decades, these remedies have gained increasing popularity in the West.12 Currently, the lipid-lowering effects of traditional Chinese medicine have garnered significant attention worldwide. The National Medical Products Administration has approved 57 traditional Chinese medicines for the treatment of hyperlipidemia. Among these, hawthorn or formulations containing hawthorn constitute over 50% of prescriptions, making it the most popular traditional Chinese medicine for treating hyperlipidemia.13 Herbal formulations, primarily composed of hawthorn, which work to resolve phlegm and clarify turbidity, are the most widely used means for treating hyperlipidemia.
Hawthorn, a renowned traditional Chinese medicine, is employed for the management of dyspepsia syndrome, cardiovascular disease, and hyperlipidemia. Hawthorn belongs to the Crataegus species within the Rosaceae family. In China, hawthorn is primarily represented by two varieties, C. pinnatifida Bge. and C. pinnatifida Bge. var. major N, E. Br. (C. pinnatifida), prevalent in Northeast and North China. “Shanzha” is the designation for C. pinnatifida Bge., and “shanlihong” for C. pinnatifida Bge. var. major N, E. Br.14 Both are extensively utilized domestically and internationally, particularly in China. The fruit of C. pinnatifida is referred to as “Crataegi fructus” in the Chinese Pharmacopoeia, boasting a history of over 2,000 years of both edible and medicinal use in China.15 According to the British Herbal Pharmacopoeia (1983), Hawthorn (C. pinnatifida) has been historically utilized for the treatment of myocardial dysfunction, hypertension, and atherosclerosis. Additionally, in China, it has been employed to address blood circulation issues.16
Hawthorn has a complex composition. Animal experimental studies, establishing hyperlipidemic rat models through a high-fat diet, involved the collection of plasma samples for biochemical and metabolomic analyses. The results indicate that hawthorn n-butanol and ethyl acetate extracts show the highest efficacy in hyperlipidemic rats. The most effective components in hawthorn extracts can reverse the metabolic disturbances in the plasma of hyperlipidemic rats. Hawthorn Pectin Oligosaccharides (POSs) have been added to functional foods to prevent hyperlipidemia and dyslipidemia.17 Hawthorn POS has been reported to have beneficial effects against a high-fat diet. It significantly reduces the total liver fat content, as well as levels of hepatic pro-inflammatory factors, tumor necrosis factor-A, and interleukin-6 (IL-6), while increasing the level of anti-inflammatory interleukin-10 (IL-10). In comparison to the high-fat control group, Hawthorn POS significantly reduces the protein expression of nuclear factor kappa B (NF-κB). It also lowers mRNA receptor levels associated with proteins such as receptor-interacting protein 1 (RIP1), NF-κB-inducing kinase (NIK), inhibitor of nuclear factor kappa-B kinase subunit alpha (IKα), mitochondrial transcription factor A (MTFA), tumor necrosis factor receptor 1 (TNfr1), and telomere-related factors 2 (TRF2) interactions.18 However, despite some studies on hawthorn’s effects on hyperlipidemia, the results are inconsistent, requiring more comprehensive analyses to determine its actual effectiveness.
Materials and methods
Study registration
The protocol of this study was registered in the PROSPERO international prospective register of systematic reviews (https://www.crd.york. ac.uk/PROSPERO).
Qualification criteria
This study employed the PICOS framework, encompassing five key elements: Participants (P); Intervention (I); Comparator (C); Outcomes (O); and Study Design (S).
Inclusion criteria
Study Type. All randomized controlled clinical trials (RCTs) assessing the impact of traditional Chinese medicine containing hawthorn on hyperlipidemia are included, with no language restrictions. This also encompasses all modified combinations of traditional Chinese medicine containing hawthorn. No restrictions are placed on participant characteristics, language, or publication type. Participant types include patients diagnosed with hyperlipidemia according to the “Guiding Principles for Clinical Research of New Chinese Medicines,"19 as well as any other studies deemed reasonable, irrespective of participant age, gender, or ethnicity.
Intervention and Control Types. The control group adopts traditional Chinese medicine or Western medical treatment measures, while the observation group uses traditional Chinese medicine containing hawthorn. There are no restrictions on the duration, dosage, or administration route of the intervention. If the experimental group undergoes combined treatment with traditional Chinese medicine containing hawthorn and other therapies, then the control group must receive the same treatment.
Results Measurement. This primarily includes total cholesterol (TC), triglycerides (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL), assessing changes in lipid levels from baseline to the end of treatment. Secondary outcome indicators include the effective rate. Included studies should have at least one outcome. The time point for measuring the efficacy is at the end of treatment. The criteria for efficacy assessment are primarily determined by the “Guiding Principles for Clinical Research of New Chinese Medicines.” Clinical Control: Clinical symptoms disappear, and lipid indicators return to normal. Marked Effect: Clinical symptoms disappear, and lipid indicators meet any of the following: TC decrease ≥20%, TG decrease ≥40%, HDL-C increase ≥0.26 mmol/L. Effective: Lipid indicators meet any of the following: TC decrease ≥10% but <20%, TG decrease ≥20% but <40%, HDL-C increase ≥0.104 mmol/L but <0.26 mmol/L. Invalid: No improvement in clinical symptoms after treatment, and lipid indicators do not meet the above criteria or show no significant improvement. In this study, the clinical total effective rate is calculated as [(total number of patients—invalid) / total number of patients] × 100%.
Exclusion criteria
Animal experiments, duplicate data, incomplete data, incorrect data that cannot be extracted, or data that cannot be obtained in full even after contacting the original authors.
Search strategy
A systematic search was conducted in eight databases, including PubMed, Embase, Cochrane Central Register of Controlled Trials, Web of Science (ISI), China National Knowledge Infrastructure, Wanfang Database, Chinese Scientific Journals Full-Text Database (VIP), and others, from our institutional repository up to February, 2021, for published RCT reports. No predefined restrictions were set for the publication status. Additionally, we manually searched the WHO Trial Register, Google Scholar, Chinese Clinical Trial Register, Baidu, and other search engines to identify unpublished articles. The search terms typically consisted of three groups: Clinical conditions (e.g. “hyperlipidemia”, “hyperlipidemias”, “hyperlipidemia”, “lipidemia”, “lipidemias”, “lipemia”, “lipemias”); Types of intervention (e.g. “crataegus”, “crataegus laevigata”, “crataegus monogyna”, “hawthorn”, “hawthorns”); Study type: a randomized controlled trial.
Study selection and data extraction
Two independent researchers conducted literature screening based on inclusion and exclusion criteria. Duplicate articles were removed using EndNote (Version: X9.3.313966). Initial screening was performed by reading titles and abstracts to exclude literature that did not meet the inclusion criteria. After making the final selection by reading the full text, researchers will use a standardized data abstraction form to independently extract basic study information, research methods, intervention and control measures, results, and other detailed and quantitative data about the studies. Any discrepancies regarding the eligibility of specific studies will be resolved through discussion with a third researcher. Qualified study information will be independently extracted by two researchers using a standardized data extraction form. The standard data extraction form will include at least the following items: Basic information about the study: title, detailed author information, and publication date; Basic characteristics of patients: age, gender, sample size, and diagnosis; Basic characteristics of the study: study design, recruitment strategy, methodological quality, intervention measures for the experimental and control groups, composition, dosage, treatment duration, administration method; Primary and secondary outcome measurements. If necessary, we will contact the corresponding authors via email and telephone for additional information.
Quality assessment
Two researchers will independently assess the risk of bias in the selected studies using the bias risk assessment tool from Cochrane Handbook version 5.3.0.20 The assessment will primarily focus on 7 aspects:
1. Random sequence generation (selection bias); 2. Allocation concealment (selection bias); 3. Blinding of participants and personnel (performance bias); 4. Blinding of outcome data (detection bias); 5. Incomplete outcome data (attrition bias); 6. Selective reporting (reporting bias); 7. Other biases. The evaluation results will be categorized as “low risk,” “unclear risk,” and “high risk” for each of the seven aspects. This comprehensive evaluation aims to provide a thorough understanding of bias in the studies and assess their reliability in drawing conclusions.
Data analysis
Data analysis was conducted using RevMan 5.3 software (ver. 5.3 RevMan, Copenhagen, Denmark). For binary outcome variables, the odds ratio (OR) was calculated, and for continuous variables, the weighted mean difference (WMD) was calculated, each with a corresponding 95% confidence interval (CI). Heterogeneity among trials was assessed using the chi-square (χ2) test. In the presence of acceptable homogeneity (P > 0.1, I2 ≤ 50%), a fixed-effects model was employed for meta-analysis. In cases of significant heterogeneity (P ≤ 0.1, I2 > 50%), a random-effects model was utilized.
Results
Description of studies
Initially, 410 relevant articles were retrieved. After screening and removing duplicate records, 294 articles remained. During the title and abstract screening, 222 articles were excluded. Among these, 117 were excluded due to animal experiments, reviews, or conference reports, 2 were excluded due to unavailability, and 103 were excluded because their research focus was not hyperlipidemia. After reviewing the full articles, 58 articles were excluded. Among these, 18 were excluded as they were graduate theses, 35 were excluded because patients had comorbidities, and 5 were excluded because the experimental group did not receive a single drug. Finally, 14 studies were included in the final analysis. The flowchart of this process is illustrated in Fig. 1.
Fig. 1.

Study flow diagram traditional Chinese medicine containing hawthorn.
These 14 randomized controlled trials were all conducted in China and published in Chinese between the establishment of the database and February 2021. The characteristics of these randomized trials are summarized in Table 1. A total of 1,448 patients participated in these 14 trials, using five different diagnostic criteria. Among them, 6 trials21–26 used the diagnostic criteria for hyperlipidemia outlined in the “Guidelines for Clinical Research of New Chinese Medicines,"19 3 trials27–29 used the “Chinese Adult Dyslipidemia Prevention Guide,"30 1 trial31 referred to the diagnostic criteria for hyperlipidemia in the undergraduate textbook “Internal Medicine” (Fifth Edition) of Chinese higher medical institutions,32 1 trial33 followed the recommendations for adjusting lipid-lowering drugs in the “Suggestions for Prevention and Treatment of Lipid Abnormalities” (1997, Chinese Journal of Cardiovascular Diseases Editorial Board Lipid Abnormalities Prevention and Treatment Special Group).34 The remaining 3 trials35–37 only described patients with hyperlipidemia without mentioning specific diagnostic criteria. All included trials used traditional Chinese medicine containing hawthorn as the sole treatment. The duration of treatment varied among the 14 trials, with 5 trials lasting for 4 weeks,23,26–28,35 1 trial lasting for 5 weeks,21 2 trials lasting for 6 weeks,22,37 and 6 trials lasting for 8 weeks.24,25,29,31,33,36 For further details, refer to Table 2.
Table 1.
Characteristics of included studies.
| Study | Sample (T/C) |
Age (T/C) |
Gender M:F(T/C) | Intervention | Control | Course (week) |
Outcome measur | Effective rate(T/C) |
|---|---|---|---|---|---|---|---|---|
| Deng XJ 200721 | 80(40/40) | (55.64 ± 8.82)/(56.31 ± 8.76) | (28:12)/(27:13) | danxiang erchen decoction for lipid regulation | duoyikang capsules | 5 | CRE,TC,TG,HDL,LDL | (37:3)/(29:11) |
| He SW et al 200522 | 120(60/60) | 61/60 | (41:19)/(36:24) | compound portulaca oleracea capsules | diaoxin xinxuekang capsules | 6 | CRE,TC,TG,HDL,LDL | (47:13)/(43:17) |
| Liu GX et al. 201323 | 75(40/35) | (53. 8 ± 10. 3)/(55.3 ± 10. 8) | (29:11)/(26:9) | modified liu jun zi tang decoction | duoyi kang capsules | 4 | CRE,TC,TG,HDL | (34:6)/(25:10) |
| Jing H et al 200524 | 114(70/44) | 36–70 | (38:32)/(23:21) | modified wuling san | simvastatin | 8 | CRE,TC,TG,HDL,LDL | (57:9)/(37:5) |
| He JX et al 200225 | 270(180/90) | 49.5/49.8 | (118:62)/(61:29) | lipid-lowering capsules | inositol nicotinic acid acetate tablets | 8 | CRE,TC,TG,HDL | (168:12)/(62:28) |
| Liu YK 200526 | 60(40/20) | 53.2/51.6 | (27:13)/(13:7) | lipid pulse-calming capsules | xuezhi kang | 4 | CRE,TC,TG,HDL,LDL | (39:1)/(17:3) |
| Yang L 201727 | 60(30/30) | 18–85 | (12:18)/(14:16) | lipid-lowering powder | atorvastatin calcium | 4 | CRE | (27:3)/(21:9) |
| Li RZ 201528 | 66(33/33) | 40–75/40–74 | (20:13)/(19:14) | lipid-lowering decoction | simvastatin | 4 | CRE | (29:4)/(21:11) |
| Tang JR et al 201929 | 70(43/43) | >50 | (26:17)/(32:11) | individually formulated lipid-lowering prescription | atorvastatin | 8 | CRE,TC,TG,HDL,LDL | (33:10)/(31:12) |
| Rao H 201231 | 140(72/68) | 52 | (42:30)/(38:30) | polygonum multiflorum and hawthorn lipid-lowering pills | fenofibrate tablets | 8 | CRE | (70:2)/(50:18) |
| Zhang T 201233 | 115(70/45) | (51.28 ± 8.26)/(52.07 ± 0.15) | (42:28)/(28:17) | invigorating qi and blood circulation, resolving turbidity decoction | zhibituo tablets | 8 | CRE | (63:7)/(31:14) |
| Jin BL 199435 | 88(51/37) | 40–60 | (38:13)/(23:14) | compound rhubarb and polygonum cuspidatum powder | maitong jiaowan pills | 4 | CRE,TC,TG | (74.5%:25.5%)/(48.6%:51.4%) |
| Liu YY et al 201936 | 120(60/60) | 62 ± 3.2 | 76:44 | gynostemma pentaphyllum lipid-lowering tea formula | atorvastatin tablets | 8 | CRE,TC,TG,HDL,LDL | (54:6)/(50:10) |
| Ma H 201137 | 70(35/35) | 40–60 | 38:42 | traditional chinese medicine formula granules | fluvastatin capsules | 6 | TC,TG, | NMT |
Notes: T/C: treatment group/control group; M/F: male/female; TC: total cholesterol; TG: triglycerides; LDL: low-density lipoprotein cholesterol; HDL: high-density lipoprotein cholesterol; NMT: not mentioned.
Table 2.
Intervention details of included studies.
| Study | Formula | Prescriptio | Taking instruction |
|---|---|---|---|
| Deng XJ 200721 | danggui erchen tang for lipid regulation | Salvia Miltiorrhiza 15 g, Ligusticum Wallichii 15 g, Atractylodes Macrocephala 15 g, Angelica Sinensis 10 g, Paeonia Lactiflora 10 g, Earthworm 10 g, Tangerine Peel 12 g, Cyperus Rotundus 12 g, Poria Cocos 12 g, Hawthorn 12 g | decoction, oral taken, twice a day |
| He SW et al 200522 | compound formula of portulaca oleracea | Portulaca Oleracea 40 g, Cassia Obtusifolia 15 g, Fried Hawthorn 15 g, Pueraria Root 15 g, Red Amaranth 12 g, Ligusticum Wallichii 12 g | decoction, oral taken,three times a day |
| Liu GX et al. 201323 | modified liu junzi tang | Tangerine Peel 10 g, Pinellia Ternata 10 g, Codonopsis Pilosula 15 g, Poria Cocos 15 g, Atractylodes Macrocephala 15 g, Zingiber Officinale (processed) 6 g, Pueraria Root 15 g, Hawthorn 15 g, Salvia Miltiorrhiza 20 g, Rehmannia Glutinosa 15 g, Polygonum Multiflorum 15 g, Lotus Leaf 10 g | decoction, oral taken, twice a day |
| Jing H et al 200524 | modified wu ling san | Poria Cocos 12 g, Alisma Orientale 15 g, Atractylodes Macrocephala 9 g, Poria Cocos (Powder) 12 g, Cinnamomum Cassia (Powder) 6 g, Atractylodes Macrocephala (Powder) 16 g, Job’s Tears Seed (Powder) 16 g, Hawthorn 20 g | decoction, oral taken, twice a day |
| He JX et al 200225 | lipid-lowering capsules | Hawthorn, Cassia Seed, Polygonum Multiflorum, Alisma Rhizome, Processed Rhubarb, Chinese Angelica, Goji Berry | decoction, oral taken, twice a day |
| Liu YK 200526 | zhimaining capsules | Hawthorn, Leech,Salvia Miltiorrhiza (Chinese Sage or Danshen), Alisma Rhizome | decoction, oral taken,three times a day |
| Yang L 201727 | lipid-lowering powder | Raw Hawthorn 100 g, Raw Rhubarb 60 g, Gynostemma Pentaphyllum 100 g, Tangerine Peel 100 g | decoction, oral taken, twice a day |
| Li RZ 201528 | lipid-lowering decoction | Hirudo 10 g, Prepared Rehmannia 15 g, Coix Seed 10 g, Alisma Orientale 15 g, Cinnamomum Cassia 6 g, Tangerine Peel 10 g, Processed Polygonum Multiflorum 12 g, Poria Cocos 10 g, Hawthorn 15 g, Dodder Seed 8 g, Cassia Seed 20 g | decoction, oral taken, twice a day |
| Tang JR et al 201929 | personally formulated lipid-lowering formula | Medicated Leaven 20 g,Pinellia Tuber, 20 g,Hawthorn, 20 g, White Atractylodes Rhizome, 15 g, Poria, 15 g Apricot Kernel, 15 g | decoction, oral taken,three times a day |
| Rao H 201231 | polygonum multiflorum and hawthorn lipid-lowering pills | Hawthorn 30 g, Polygonum Multiflorum 18 g, Rhizoma Polygonati 18 g, Panax Notoginseng (Powder) 9 g, Cassia Seed (Powder) 18 g, Alisma Orientale 12 g, White Atractylodes 15 g, Poria Cocos 15 g, Radish Seed 15 g, Coix Seed 15 g, Lotus Leaf 15 g, Salvia Miltiorrhiza 18 g, Pinellia Ternata 12 g, White Peony Root 15 g, Lotus Leaf 10 g, Licorice 6 g | decoction, oral taken,three times a day |
| Zhang T 201233 | promote qi, activate blood, and dispel turbidity decoction | Angelica Sinensis 15 g, Paeonia Lactiflora 15 g, Ligusticum Wallichii 10 g, Peach Kernel 10 g, Safflower 15 g, Hirudo 6 g, Wine-Processed Rhubarb 10 g, Alisma Orientale 12 g, Hawthorn 30 g, Gynostemma Pentaphyllum 30 g, Tangerine Peel 10 g, Polygonum Multiflorum 30 g, Poria Cocos 15 g, Salvia Miltiorrhiza 15 g | decoction, oral taken, twice a day |
| Jin BL 199435 | compound powder of rhubarb and amomum | Raw Hawthorn, Raw Rhubarb, Radish Seed, Salvia Miltiorrhiza, Polygonum Multiflorum, Chrysanthemum Flower, Safflower | decoction, oral taken,three times a day |
| Liu YY et al 201936 | gynostemma pentaphyllum lipid-lowering tea formula | Gynostemma Pentaphyllum 10 g, Cassia Seed 10 g, Hawthorn 10 g, Lotus Leaf 10 g, Chinese Yam 10 g | decoction, oral taken, twice a day |
| Ma H 201137 | traditional chinese medicine formula granules | Gastrodia Elata 15 g, Uncaria Rhynchophylla 15 g, Lysimachia Christinae 30 g, Lophatherum Gracile 15 g, Parasitic Loranthus 20 g, Astragalus Membranaceus 20 g, Hawthorn 30 g, Atractylodes Macrocephala 15 g, Salvia Miltiorrhiza 15 g, Panax Notoginseng | decoction, oral taken, twice a day |
Risk of bias in included studies
After evaluation, all included studies were found to have a high risk of bias and were considered to be of poor methodological quality. Although all trials claimed that participants were randomly assigned, only two studies31,33 explicitly stated the specific method of random number generation, using a random number table. The other 12 trials did not provide detailed information, making it impossible to assess the adequacy of their methods. In all trials, allocation concealment was not mentioned, and only one trial22 mentioned blinding of participants and personnel. One trial24 provided information about dropouts or withdrawals. All included studies seemed to have a sufficient and acceptable level of compliance. Due to the inability to access study protocols, selective reporting is often unclear. Other biases may exist, but due to insufficient evidence, confirmation is not possible (Figs 2 and 3).
Fig. 2.
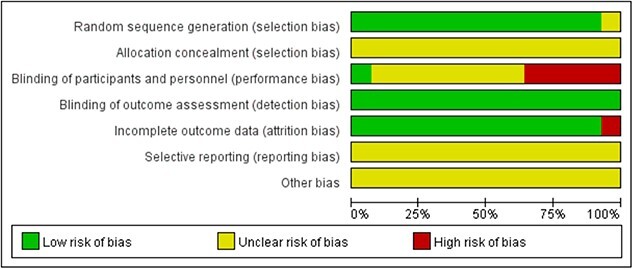
Risk of bias graph.
Fig. 3.
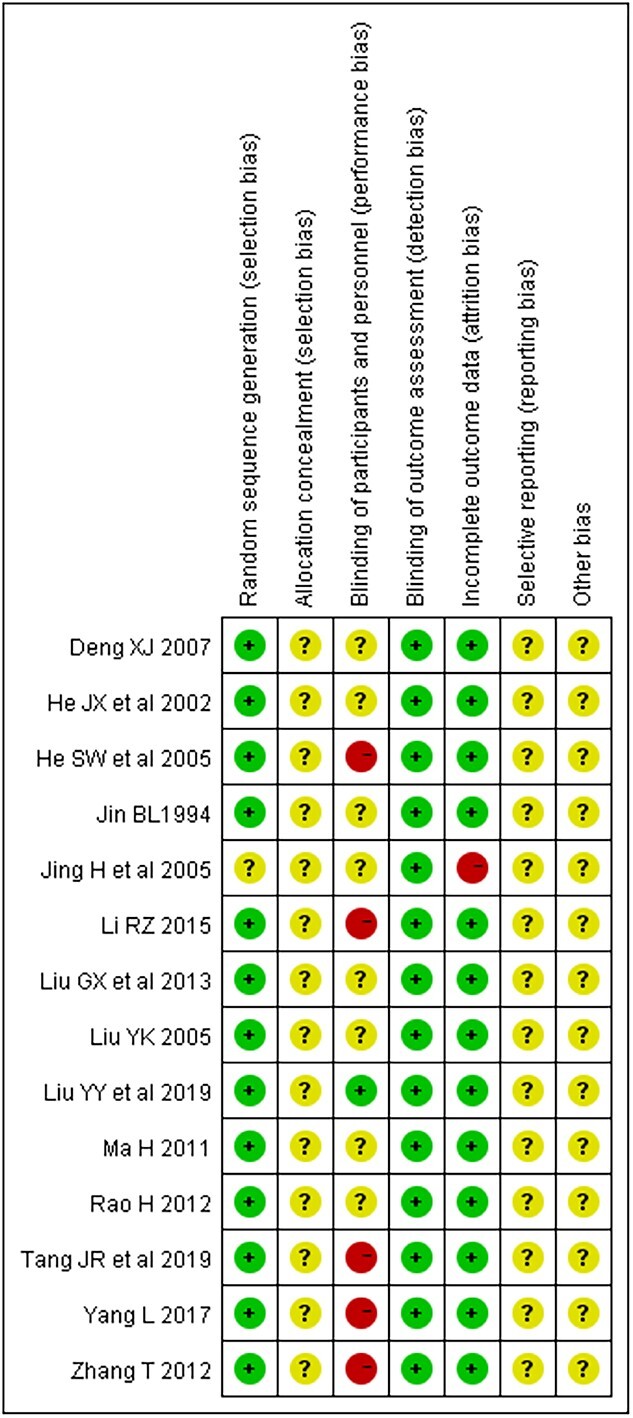
Risk of bias graph.
Effective rate
All 14 trials utilized Chinese medicine containing hawthorn as the treatment group, comparing it with lipid-lowering drugs as the control group. Among these, 12 trials21–29,31,33,36 assessed the effective rate as the outcome, but the criteria for defining effectiveness were not entirely consistent. In the studies by Deng, Liu, He, Rao,21,23,25,31 effectiveness was defined as “reaching one of the following criteria: TC reduction ≥10% but <20%, TG reduction ≥20% but <40%, HDL-C increase ≥0.104mmol/L but <0.26mmol/L.” In the studies by He, Zhang, Jing,22,24,33 the criteria were “serum total cholesterol decrease of 10%~20%, or triglycerides decrease of 20%~40%, or high-density lipoprotein cholesterol increase of 0.104~0.260 mmol/L”; while in Li’s study,28 the standard was “clinical symptoms improving to a certain extent, symptom score reduced by ≥30%.” In Liu’s study,36 the standard was “effective TC reduction by 10%–20%, and/or TG reduction by 20%–40%, HDL increase by 0.1–0.2 mmol/L, LDL decrease by 0.1–0.02 mmol/L.” In Liu’s study,26 the standard was “TC reduction ≥10%~19%, TG reduction 30%~39%, or HDL increase 0.1mmol/L.” Tan’s study29 defined effectiveness as “when the patient’s TC decreases by 10%~15%, TG decreases by 25%~38%, LDL increases by 0.1~0.2mmol, it is considered effective.” In Yang’s study,27 the criteria were “TC reduction >10%, <20%, TG reduction ≥20%, <40%, HDL-C increase 4~10mg/dL, TC-HDL-C/HDL-C decrease >10%, <20%.” In Jin’s study,35 the criteria were “two lipid parameters returning to the normal range, while the third remains above normal; two parameters increasing before treatment, and one decreasing to the normal range after treatment.” The results of these 12 independent trials showed heterogeneity (P = 0.002, I2 = 62%). After sensitivity analysis, we excluded the study by Jing.24 The data subsequently showed acceptable homogeneity (P = 0.12, I2 = 35%), and thus, a fixed-effects model was used to pool the data, confirming a significant improvement in clinical effective rate for Chinese medicine containing hawthorn compared to the control group (OR = 2.55; 95%CI = [1.82,3.57]) (Fig. 4).
Fig. 4.

Effective rate of traditional Chinese medicine containing hawthorn versus lipid-lowering drugs.
TC
Nine studies21–26,36,37 29compared the effect of the treatment group and the control group on reducing TC, but they exhibited heterogeneity (P < 0.00001, I2 = 88%). We used a random-effects model to analyze the data, and the forest plot indicates that the treatment group is significantly more effective than the control group [(MD = −0.43; 95% CI = (−0.67, −0.19)] (Fig. 5).
Fig. 5.

Total cholesterol of traditional Chinese medicine containing hawthorn versus lipid-lowering drugs.
TG
Nine studies21–26,36,37measured TG as an outcome, but they showed significant heterogeneity (P < 0.00001; I2 = 98%). A random-effects model was used for statistical analysis. The effect of Chinese medicine containing hawthorn in reducing TG was superior to lipid-lowering drugs [MD = −1.04; 95% CI = (−1.62, −0.45)] (Fig. 6).
Fig. 6.

Total triglyceride of traditional Chinese medicine containing hawthorn versus lipid-lowering drugs.
HDL
Seven studies21,22,24–26,29,36 reported the comparison of HDL levels between the treatment and control groups after intervention. The data from these seven trials showed homogeneity (P = 0.58, I2 = 0%). Therefore, a fixed-effects model was used. The meta-analysis indicated that traditional Chinese medicine containing hawthorn was more effective than lipid-lowering drugs in increasing HDL [MD = 0.12; 95% CI = (0.09, 0.16)] (Fig. 7).
Fig. 7.

High-density lipoprotein cholesterol of traditional Chinese medicine containing hawthorn versus lipid-lowering drugs.
LDL
Six studies21,22,24,26,29,36 compared the effect of reducing LDL levels between the treatment and control groups after intervention. The data exhibited significant heterogeneity (P < 0.00001, I2 = 98%), so a random-effects model was employed for data analysis. The results indicated that traditional Chinese medicine containing hawthorn was not more effective than lipid-lowering drugs in reducing LDL [MD = −0.23; 95% CI = (−0.70, 0.24)] (Fig. 8).
Fig. 8.

Low-density lipoprotein of traditional Chinese medicine containing hawthorn versus lipid-lowering drugs.
Publication bias
A funnel plot was used for a bias analysis of the 12 studies21–29,31,33,36 describing the overall effective rate. The inverted funnel plot shows an asymmetric and skewed distribution of data points, as depicted in Fig. 8. This suggests the presence of publication bias in the included literature, possibly due to the overall low quality of the studies where negative results might have remained unpublished. Additionally, the asymmetry in the funnel plot could be related to the small sample size in the trials(Fig. 9).
Fig. 9.
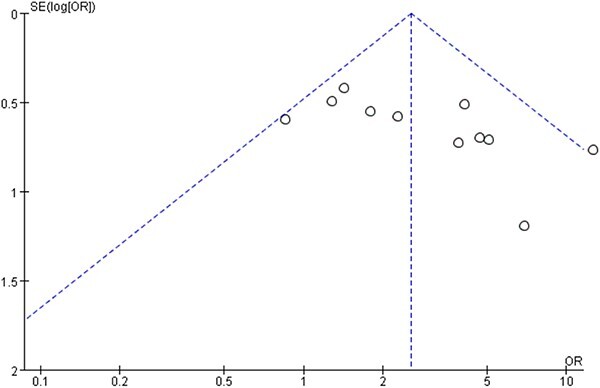
Total effective rate funnel chart.
Discussion
This is a summary of a meta-analysis involving 14 RCTs with 1,448 participants. The data and forest plots from the meta-analysis suggest that traditional Chinese medicine containing hawthorn might be more effective than traditional medications for treating hyperlipidemia. Preliminary conclusions from the meta-analysis indicate a significant improvement in the clinical effectiveness of traditional Chinese medicine containing hawthorn compared to the control group. Traditional Chinese medicine containing hawthorn appears to be more effective in reducing total cholesterol TC and triglycerides TG while increasing high-density lipoprotein HDL. In a recent 2015 study, the anti-obesity effects of a combination of C. pinnatifida leaf and Citrus unshiu peel extracts (HTO48) were explored in male Sprague Dawley rats. Divided into chow diet and high-fat diet (HFD) groups, the rats showed that 0.2% and 0.6% concentrations of HTO48 for 12 weeks reduced serum TC by 14.4% and 16.3% and TG levels by 33.7% and 31.9% in HFD-fed rats compared to the HFD control group.38 Another study used C. pinnatifida (Shan zha) fruit extracts to examine their impact on obesity and dyslipidemia in hamsters on a high-fat diet. In this study with male Syrian golden hamsters, those receiving 250 mg/kg of Shan zha (dissolved in water) exhibited a 15% lower plasma total cholesterol level, a 20% decrease in LDL, and a 27% increase in HDL after 7 days of treatment.39
However, in reducing LDL, traditional Chinese medicine containing hawthorn is not more effective than lipid-lowering drugs. In 2014, Hu et al. conducted a study on the effects of a multiherbal preparation containing C. pinnatifida and other herbs like Alisma orientalis, Stigma maydis, Ganoderma lucidum, Polygonum multiflorum, and Morus alba on dyslipidemia. Participants took four capsules in the morning and evening for 12 weeks. The study concluded that the multiherbal formulation showed only marginal beneficial effects on LDL-C levels.40
This is the first systematic review and meta-analysis aimed at evaluating the efficacy of traditional Chinese medicine containing hawthorn in treating hyperlipidemia. The study adhered to the PRISMA statement and followed a standardized protocol registered in PROSPERO (registration number: CRD42015019428), an international prospective register of systematic reviews. The literature search was comprehensive and rigorously assessed the methodological quality of the included trials.
There are several limitations in this meta-analysis. The included trials exhibit poor methodological quality. Only 2 studies reported the randomization procedures, while the other 12 trials merely stated that patients were randomly divided into two groups. Due to a lack of necessary information in the articles, we cannot determine if randomization was conducted appropriately. All 14 studies lacked information regarding allocation concealment, with one study mentioning blinding of assessments for participants and staff. One study reported patient dropout or loss of follow-up, while all studies failed to mention intention-to-treat analysis and pre-trial sample size estimation. Information on quality control and qualitative testing of traditional Chinese medicine preparations is lacking, a common issue in Chinese clinical trials. In the analysis of effective rates in this meta-analysis, funnel plot analysis identified publication bias, and due to insufficient quantity, we were unable to perform funnel plot analysis for other indicators, potentially indicating underlying publication bias as well.
In summary, the included trials and the results of the meta-analysis suggest that traditional Chinese medicine containing hawthorn may be more effective than lipid-lowering drugs in treating hyperlipidemia. However, the evidence obtained from this study is not sufficient to draw a definitive conclusion about the benefits of traditional Chinese medicine containing hawthorn in treating hyperlipidemia. Due to methodological limitations in the included trials, positive findings should be interpreted cautiously. More well-designed clinical trials are needed to validate the efficacy and safety of traditional Chinese medicine containing hawthorn in treating hyperlipidemia. This meta-analysis provides insights for future clinical research. Sample size estimation should be conducted before recruitment. Adequate information about methods, such as randomization, allocation concealment, and blinding, should be provided. Intention-to-treat analysis and patient dropout during the trial should be clearly described. Follow-ups should be conducted to assess the long-term effectiveness and safety of the intervention. Reporting of adverse events should receive increased attention. Additionally, clinical trials should be registered in advance on the World Health Organization International Clinical Trials Registry Platform and follow the CONSORT statement or CONSORT extension for herbal interventions, providing detailed information.
Contributor Information
Xiaoli Zhou, Department of Spine Surgery, Tianjin Hospital, Tianjin University, No. 406 Jiefang South Road, Hexi District, Tianjin 300211, China; Department of Toxicology, Tianjin Centers for Disease Control and Prevention, No. 6, Huayue Road, Hedong District, Tianjin 300011, China.
Chun Chen, Tianjin Key Laboratory of Agricultural Animal Breeding and Healthy Husbandry, College of Animal Science and Veterinary Medicine, Tianjin Agricultural University, Jinjing Road No. 22, Xiqing District, Tianjin 300392, China.
Zheng Gao, Department of Toxicology, Tianjin Centers for Disease Control and Prevention, No. 6, Huayue Road, Hedong District, Tianjin 300011, China.
Zhiyong Qian, Department of Toxicology, Tianjin Centers for Disease Control and Prevention, No. 6, Huayue Road, Hedong District, Tianjin 300011, China.
Jun Miao, Department of Spine Surgery, Tianjin Hospital, Tianjin University, No. 406 Jiefang South Road, Hexi District, Tianjin 300211, China.
Author contributions
Xiaoli Zhou collected documents and wrote the manuscript; Chun Chen helped to collected some literature and improve the manuscript; Zheng Gao and Jun Miao revised the manuscript for important content; Zhiyong Qian contributed significantly to the manuscript preparation and modification.
Funding
This work was supported by Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-026A).
Conflict of interest statement: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
- 1. Cooney MT, Dudina A, de Bacquer D, Wilhelmsen L, Sans S, Menotti A, de Backer G, Jousilahti P, Keil U, Thomsen T, et al. HDL cholesterol protects against cardiovascular disease in both genders, at all ages and at all levels of risk. Atherosclerosis. 2009:206(2):611–616. [DOI] [PubMed] [Google Scholar]
- 2. Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, Ferranti S, Després J-P, et al. Heart disease and stroke Statistics-2016 update: a report from the American Heart Association [published correction appears in circulation. 2016 Apr 12;133(15):e599]. Circulation. 2016:133(4):e38–e360. [DOI] [PubMed] [Google Scholar]
- 3. Centers for Disease Control and Prevention (CDC) . Vital signs: prevalence, treatment, and control of high levels of low-density lipoprotein cholesterol--United States, 1999-2002 and 2005-200. MMWR Morb Mortal Wkly Rep. 2011:60(4):109–114. [PubMed] [Google Scholar]
- 4. Pfizer, Inc . Lipitor [package insert]. New York, NY; 2015. [Google Scholar]
- 5. Novartis Pharmaceuticals Corporation . Lescol/Lescol XL [package insert]. East Hanover, NJ; 2012. [Google Scholar]
- 6. Mylan Pharmaceuticals, Inc . Mevacor [package insert]. Morgantown, WV; 2014. [Google Scholar]
- 7. Bristol-Myers Squibb Company . Pravachol [package insert]. Princeton, NJ; 2016. [Google Scholar]
- 8. Merck & Co, Inc . Zocor [package insert]. Whitehouse Station, NJ; 2015. [Google Scholar]
- 9. Davidson M, McKenney J, Stein E, Schrott H, Bakker-Arkena R, Fayyad R, Black D. Comparison of one-year efficacy and safety of atorvastatin versus lovastatin in primary hypercholesterolemia. Atorvastatin study group I. Am J Cardiol. 1997:79(11):1475–1481. [DOI] [PubMed] [Google Scholar]
- 10. Livalo [package insert]. Montgomery, AL: Kowa Pharmaceuticals America, Inc.; 2016. [Google Scholar]
- 11. AstraZeneca Pharmaceuticals, LP . Crestor [package insert]. Wilmington, DE; 2016. [Google Scholar]
- 12. Tachjian A, Maria V, Jahangir A. Use of herbal products and potential interactions in patients with cardiovascular diseases. J Am Coll Cardiol. 2010:55(6):515–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Xie W, Zhao Y, Du L. Emerging approaches of traditional Chinese medicine formulas for the treatment of hyperlipidemia. J Ethnopharmacol. 2012:140(2):345–367. [DOI] [PubMed] [Google Scholar]
- 14. Chinese Academy of Sciences Editorial Committee . Flora of China. Beijing: Science Press; 1974. [Google Scholar]
- 15. Zhao P, Qiu S, Hou ZL, Xue XB, Yao GD, Huang XX, Song SJ. Sesquineolignans derivatives with neuroprotective activity from the fruits of Crataegus pinnatifida. Fitoterapia. 2020:143:104591. [DOI] [PubMed] [Google Scholar]
- 16. Chen J, Xue B, Li K, Shi J, Krempin D, Zhu M, Garland C. The effects of an instant haw beverage on lipid levels, antioxidant enzyme, and immune function in hyperlipidemia patients. Zhonghua Yu Fang Yi Xue Za Zhi. 2002:36(3):172–175. [PubMed] [Google Scholar]
- 17. Zeng L, Luo L, Xue Q, He Q, Chen X, Meng J, Wang S, Liang S. LC-MS based plasma metabolomics study of the intervention effect of different polar parts of Hawthorn on hyperlipidemia rats. J Sep Sci. 2021:44(5):963–972. [DOI] [PubMed] [Google Scholar]
- 18. Li T, Chen X, Huang Z, Xie W, Tong C, Bao R, Sun X, Li W, Li S. Pectin oligosaccharide from hawthorn fruit ameliorates hepatic inflammation via NF-κB inactivation in high-fat diet fed mice. J Funct Foods. 2019:57:345–350. [Google Scholar]
- 19. Ministry of Health of the People's Republic of China . Guiding principles for clinical research of new traditional Chinese medicine drugs. 2nd ed. Beijing: People’s Medical Publishing House; 1995. p. 171.
- 20. Deeks JJ, Higgins JP, Altman DG. Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of interventions version 6.1.0. U.K.: The Cochrane Collaboration; 2020. [Google Scholar]
- 21. Deng XJ. Observation on the therapeutic effect of Danxiang Erchen decoction in treating 40 cases of phlegm-dampness stasis type hyperlipidemia. J Qiqihar Med College. 2007:28(19):2. [Google Scholar]
- 22. He SW, He SG, Zhao RH, Li SH, Li GZ. Effects of compound Portulaca oleracea on blood lipids, lipoproteins, and hemorheology in patients with hyperlipidemia. Chin Clin Rehabil. 2005:31:009. [Google Scholar]
- 23. Liu GX, Deng YH, Pan GQ. Treatment of hyperlipidemia with modified Liu-Jun-Zi-tang: a study of 40 cases. Guangming Tradit Chin Med. 2013:28(9):2. [Google Scholar]
- 24. Jing H, Liu H. The lipid-regulating effects of modified Wu Ling san on primary hyperlipidemia. Chin Patent Med. 2005:27(1):4. [Google Scholar]
- 25. He JX, Liu CK, Lu GP, Liu RM, Sun X. Observation on the therapeutic effect of lipid-lowering capsules in the treatment of 180 cases of hyperlipidemia. J Jilin Tradit Chin Med. 2002:1:9–10. [Google Scholar]
- 26. Liu YK. Clinical study on the effects of Zhi-Mai-Ning capsules on lipid metabolism, antioxidant, and hemorheology in patients with hyperlipidemia. New Chin Med. 2005:37(10):3. [Google Scholar]
- 27. Yang L. Randomized parallel control study of Jiangzhi san in the treatment of hyperlipidemia. J Pract Tradit Chin Intern Med. 2017:31(2):2. [Google Scholar]
- 28. Li RZ. Randomized parallel control study of Jiangzhi tang in the treatment of hyperlipidemia. J Pract Tradit Chin Intern Med. 2015:6:2. [Google Scholar]
- 29. Tan JR, Li D. Observation on the efficacy of self-formulated lipid-lowering prescription in the treatment of hyperlipidemia. Mod Med Health. 2019:35(10):2. [Google Scholar]
- 30. Joint Committee for Developing Chinese Guidelines on Prevention and Treatment of Dyslipidemia in Adults . Chinese guidelines on prevention and treatment of dyslipidemia in adults. Chin J Cardiovasc Dis. 2007:35(5):390–419. [PubMed] [Google Scholar]
- 31. Rao H. Clinical study on Shouwu Shanzha Jiangzhi pill in the treatment of hyperlipidemia. Chin J Tradit Chin Med. 2012:27(12):2. [Google Scholar]
- 32. Ye RG. Internal medicine. 5th ed. Beijing: People's Health Publishing House; 2002. pp. 827–828 [Google Scholar]
- 33. Zhang T. Clinical study on the treatment of qi and blood stasis type Hyperlipidemia with Liqi Huoxue Huazhuo decoction. Chin J Tradit Chin Med. 2012:27(4):2. [Google Scholar]
- 34. Editorial Board of the Chinese Journal of Cardiovascular Diseases, Lipid Abnormalities Prevention and Treatment Special Group . Recommendations for the prevention and treatment of lipid abnormalities. Chin J Cardiovasc Dis. 1997:25(3):169–175. [Google Scholar]
- 35. Jin BL. Report on the treatment of 51 cases of Hyperlipidemia with compound Shanzha Dahuang powder. Inner Mongolia Med J. 1995:2:015. [Google Scholar]
- 36. Liu YY, Liu W, Zhao YY, Gao XQ, Wu KM. Clinical study on the treatment of 60 cases of Hyperlipidemia with Gouqulan lipid-lowering tea. World Latest Med Inf Abstr. 2019:92:2. [Google Scholar]
- 37. Ma H. Clinical efficacy observation of traditional Chinese medicine granules "Teng Ma Tiao Zhi yin" in the treatment of 35 cases of Hyperlipidemia. Chin Tradit Med Inf. 2011:3(8):2. [Google Scholar]
- 38. Ali AT, Hochfeld WE, Myburgh R, Pepper MS. Adipocyte and adipogenesis. Eur J Cell Biol. 2013:92(6–7):229–236. [DOI] [PubMed] [Google Scholar]
- 39. Kuo DH, Yeh CH, Shieh PC, Cheng KC, Chen FA, Cheng JT. Effect of shanzha, a Chinese herbal product, on obesity and dyslipidemia in hamsters receiving high-fat diet. J Ethnopharmacol. 2009:124(3):544–550. [DOI] [PubMed] [Google Scholar]
- 40. Hu M, Zeng W, Tomlinson B. Evaluation of a crataegus-based multiherb formula for dyslipidemia: a randomized, double-blind, placebo-controlled clinical trial. Evid Based Complement Alternat Med. 2014:2014:365742. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.