

Abstract
Background
The correct management and treatment of pseudotumors due to metal-on-metal (MOM) hip arthroplasty are still debated. The purpose of this study is to analyze the surgical treatment and the clinical and radiographic 3-year outcomes of MOM arthroplasty revisions due to pseudotumor treated with a strategy of excision and revision.
Methods
Consecutive, retrospective series of 21 patients (8 males/13 females) with pseudotumor due to MOM hip arthroplasty was surgically treated at a single tertiary center. Demographic, clinical, radiological and implant-related features were collected pre-operatively. Post-revision clinical and radiographic parameters were evaluated. Chromium (Cr) and cobalt (Co) blood samples were collected before and after surgery.
Results
Three patients (14.2%) with pseudotumor underwent a resection arthroplasty due to infection (perioperative finding) and could not be reimplanted due to septic relapses. Twenty (95.2%) pseudotumors were completely resected. Revisions [2 total hip reimplantations (11.1%) and 16 isolated component revisions (88.9%)] were performed with non-MOM couplings. A clinical improvement at a mean post-revision follow-up 3.3 years [standard deviation (SD), ±2.2 years] was observed, from 50.3 (SD, ±4.6) to 88.3 (SD, ±9.2) Harris hip score (HHS) points (P<0.001). Among revisions, there were 5 complications (23.8%): 1 dislocation, 1 psoas impingement, and 3 infections (14.2%). No re-revision was carried out. Three (14.2%) pseudotumors recurred: 1 was surgically treated, 1 was treated with selective arterial embolization, and 1 clinically followed. At the final follow-up, Cr and Co blood ions beyond the threshold decreased from 85.7% cases to 0% in the seven patients that could be evaluated.
Conclusions
The one-stage strategy of radical excision and revision with non-MOM couplings in pseudotumors due to MOM hip arthroplasty achieved good 3-year outcomes. However, complications were frequent (23%). Recurrences were not rare (14%) and did not require implant re-revision.
Keywords: Adverse tissue reaction, combined anteversion, ceramic, ultraporous cup, recurrence
Highlight box.
Key findings
• One-stage complete pseudotumor resection and revision with non-MOM bearings is an effective strategy in MOM hip arthroplasties with adverse local tissue reactions, despite high complication rates and pseudotumor recurrence.
What is known and what is new?
• Pseudotumors after MOM hip arthroplasty are challenging: revision hips carry a high risk of complications and the optimal surgical strategy is still unknown.
• Complete pseudotumor resection and revision with non-MOM bearings is an effective one-stage strategy in failed MOM hip arthroplasties: clinical outcomes and metal ion blood levels significantly improved in the post-revision setting.
What is the implication, and what should change now?
• One-stage complete pseudotumor resection and revision with non-MOM bearings should be considered in MOM revisions.
Introduction
Background
Pseudotumors in metal-on-metal (MOM) arthroplasties are abnormal soft tissue reactions to metal debris, visualized intraoperatively or on imaging studies as solid and/or cystic soft tissue masses (1). Pseudotumors are consequences of MOM implant-related wear occurring at different sites (bearing surfaces, taper): necrosis, metallosis, granulomatous inflammation and aseptic lymphocytic vasculitis-associated lesions are the main histopathological features (1,2). The subtle symptomatology of these soft tissue lesions and the poor correlation with metal ion levels in serum and urine make the incidence and the behavior of pseudotumors largely unknown (3). Some papers reported that pseudotumors occurred in up to 30–50% of MOM arthroplasties, many of them becoming symptomatic over the years and requiring revisions (3,4).
Rationale and knowledge gap
There are no unanimous indications for failed MOM hip arthroplasty revisions. The decision to revise a failed implant is usually made considering the metal ion levels (whose thresholds are still debated), symptoms (which can be very subtle) and soft tissue damages (1,2,5). Despite the prevalence of pseudotumors, the surgical strategy of soft tissue mass management in failed MOM implants is not well established (5). Some authors advocated an arthroplasty revision procedure, aiming to change the main metal debris generators (6,7). Other surgeons preferred a concomitant debridement of the soft tissue lesions (8,9). A single or two step procedure was equally promoted (10,11). Generally, low post-revision outcomes were reported, with considerable rates of infections, dislocations and pseudotumor recurrence (5).
Objective
We provided a consecutive case series of 21 revision hips after pseudotumors due to failed primary MOM hip arthroplasties with a one-stage strategy of pseudotumor resection and revision. We aimed to define: (I) the clinical and radiographic outcomes; (II) complications and re-revision rates; (III) metal ion concentrations in the serum at a mean follow-up of 3 years.
We present the following article in accordance with the STROBE reporting checklist (available at https://aoj.amegroups.com/article/view/10.21037/aoj-22-45/rc).
Methods
The retrospective series includes 21 consecutive patients (8 males/13 females) affected by pseudotumors and treated surgically from 2011 to 2018 at a single tertiary center (Figure 1). The patients were clinically and radiographically followed after the revision hip arthroplasties, in a prospective fashion. Inclusion criteria were:
Figure 1.
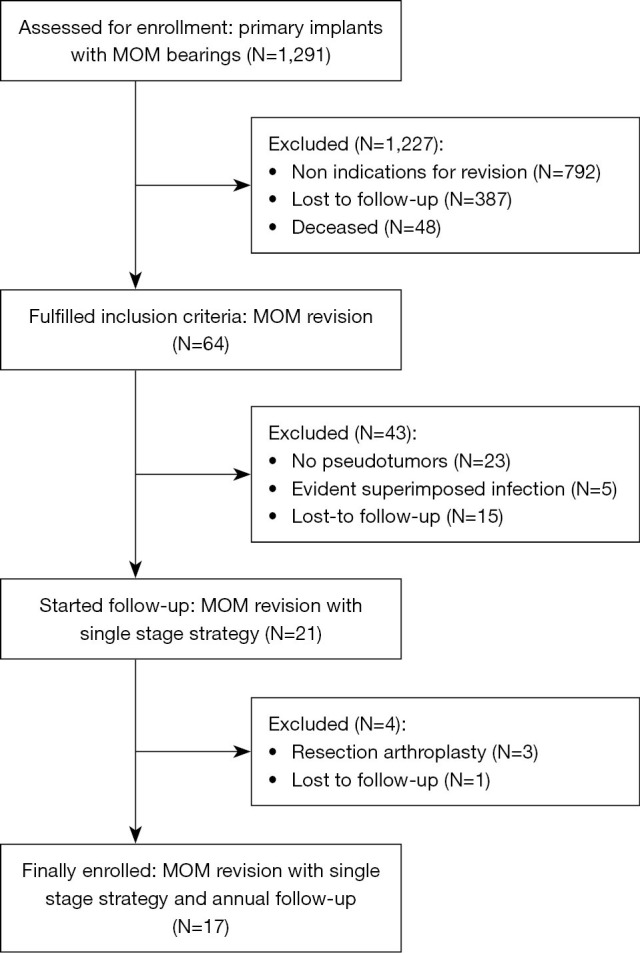
Flowchart of the study. MOM, metal-on-metal.
❖ Primary implants with MOM bearings;
❖ Evidence of pseudotumors, identified as a computed tomography (CT) scan finding of solid or cystic mass of non-infectious origin nor neoplastic in periprosthetic soft tissues;
❖ Surgical treatment of pseudotumors with a one-stage strategy of excision and revision;
❖ Adherence to post-revision clinical and radiological follow-ups (annual).
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by regional ethics committee of Comitato Etico Area Vasta Emilia Centro (CE-AVEC 433/2019/Oss/IOR) and individual consent for this retrospective analysis was waived.
Pre-revision and post-revision assessments
Pre-revision demographic and implant-related data are specified in the Table 1. The patients were clinically assessed in the pre-revision and post-revision settings using the Harris hip score (HHS). Radiological investigations were performed in all the patients before revision using anteroposterior radiographs of the pelvis and a CT scan from the fourth lumbar vertebra to the tibial plateau. The post-revision radiographic assessment included an annual anteroposterior radiograph of the pelvis.
Table 1. Demographics of the pseudotumor cohort.
| Parameters | Value |
|---|---|
| Gender, n (%) | |
| Males | 8 (38.1) |
| Females | 13 (61.9) |
| Side, n (%) | |
| Right | 15 (71.4) |
| Left | 6 (28.6) |
| ASA, n (%) | |
| I | 2 (9.5) |
| II | 9 (42.8) |
| III | 10 (47.6) |
| BMI (kg/cm2), mean ± SD | 27.9±4.6 |
| Major comorbidity, n (%) | |
| Atrial fibrillation | 1 (4.8) |
| Diabetes | 3 (14.3) |
| COPD | 1 (4.8) |
| Age at primary THA (years), mean ± SD | 56.3±11.1 |
| Primary THA survival (months), mean ± SD | 100.5±40.7 |
| Head size >36 mm, n (%) | 7 (33.3) |
| Cup type, n (%) | |
| BHR (Smith & Nephew) | 2 (9.5) |
| ASR (DePuy) | 3 (14.3) |
| Pinnacle (Depuy) | 5 (23.8) |
| Metasul (Zimmer) | 1 (4.8) |
| Recap (Biomet) | 1 (4.8) |
| Conserve Plus (Microport) | 1 (4.8) |
| Lineage (MicroPort) | 1 (4.8) |
| Unknown | 7 (33.3) |
| Stem type, n (%) | |
| Proxima (DePuy) | 3 (14.3) |
| Corail (DePuy) | 3 (14.3) |
| Conus (Zimmer) | 1 (4.8) |
| Rippen (Link) | 1 (4.8) |
| Recta (Adler) | 1 (4.8) |
| Profemur (Microport) | 1 (4.8) |
| Taperloc (Biomet) | 1 (4.8) |
| Unknown | 8 (38.1) |
| Unstemmed | 4 (19.1) |
ASA, American Society of Anesthesiologists; BMI, body mass index; SD, standard deviation; COPD, chronic obstructive pulmonary disease; THA, total hip arthroplasty; BHR, Birmingham Hip Resurfacing; ASR, articular surface replacement.
The positioning parameters of the components were measured in the pre-operative CT scans, in order to minimize magnification distortions, and in the last post-operative X-rays (the ball acting as a magnification marker). The following measurements were performed (the measurement technique was described in other papers): acetabular inclination, acetabular anteversion, stem antetorsion and combined anteversion (12). Cup loosening was diagnosed in the presence of a progressive radiolucent line greater than 2 mm and in case of migration of the cup greater than 5 mm (13). Stem loosening was placed in the presence of a sinking greater than 5 mm (13). Osteolysis was assessed according to the criteria of Engh (13). Radiolucent lines position was determined according to DeLee and Charnley (cup) and Gruen (stem) (13). Acetabular component integration was assessed according to Moore criteria (13). A good bony ingrowth was evident when at least 3 of the following 5 parameters were present: radial trabeculation, medial stress shielding, upper and lower acetabular buttresses, absence of radiolucent lines (13).
Pseudotumors were stratified in C1, C2, and C3, according to Anderson grading system (14).
Pre-revision infection survey was performed by collecting C-reactive protein (CRP) blood levels the day before surgery and performing synovial fluid needle aspirations 3 months before surgery.
Intraoperatively were collected at least 3 soft tissue samples for culture examination and frozen sections were performed.
Cobalt (Co) and chromium (Cr) ion serum levels were collected before and after the revision surgery (1 year), according to previously explained techniques. The threshold for anomalous ion levels was set at 7 µg/L according to international criteria (15).
Surgical technique and intraoperative findings
Preoperative planning was performed using a magnified anterior-posterior radiograph and a CT scan processed using the HipOp software (12).
Preoperatively, 6 patients (28.6%) underwent arterial embolization under CT guidance to reduce bleeding related to mass excision. A lateral approach was performed in 19 cases (90.5%), in 1 case (4.8%) a Smith-Petersen anterior access and in 1 case (4.8%) an anterior ileum-inguinal. A further iliofemoral anterior and pararectal approach (4.8%) were performed to completely excise the mass. The approach was chosen according to the surgeon’s experience and the pseudotumor location. After pseudotumor excision [20 (95.2%) complete eradication and 1 (4.8%) incomplete due to neurovascular proximity], the implant was dislocated and the head was removed. The stem was checked for stability. When it was well integrated and the taper was not severely damaged, an isolated acetabular reconstruction was performed (16 cases, 76.2%). In 2 cases (9.5%), a total revision was performed due to stem loosening. In 2 cases (9.5%), a resection hip arthroplasty was performed without reconstruction, in 1 case (4.8%) a cup explantation and femoral collar resection were performed. Both the procedures were performed due to intra-operative confirmation of sepsis. The cup was removed using apposite bladed instruments (Innomed Cup X, Savannah, USA). The acetabular cavity was appropriately reamed based on bone quality. Acetabular defects were evaluated according to the Paprosky classification (type I: 8 patients, 38.2%; type II: 6 patients, 28.5%; type III: 7 patients, 33.3%) (16). Morselized bone grafts were positioned to fill cavity defects (4 cases, 19.1%). Massive bone allografts were used in 6 cases (28.5%) to fill segmental defects. After placing a trial cup, the definitive cup was positioned (average size, 54.6±38.9 mm; range, 46–65 mm). Apart one iliac screw cup (Sansone, Citieffe, Italy: 5.6%), ultraporous cups were adopted in 17 cases (94.4%): 11 3D printed titanium cups (TiPor, Adler, Italy: 61.1%), and 6 tantalum sockets (Trabecular Metal, Zimmer, USA: 33.3%). A polyethylene liner was seated in 8 cases (44.4%) and ceramic Delta liner in 10 cases (55.6%). Trial reduction was performed to assess implant stability, soft tissue tension and leg length discrepancy. Based on the appropriate correction requested, a Delta revision head (9 cases, 50%) or a Delta ball head adaptation system (BioBall, Merete GmbH, Berlin, Germany; 7 cases, 38.9%) through the interposition of a titanium sleeve on the taper. In 2 cases (11.1%), a metal head was used instead. 32 mm heads and 36 mm heads were used in all revision hips except for 1 case in which a 40 mm head was used.
Pseudotumors were located along the course of the ileo-psoas muscle in 11 cases (52.4%) and paratrochanteric in 5 cases (23.8%). Metallosis, synovitis and soft tissue injuries were ubiquitous findings. Seventeen solid bone cysts (81%; 3 periacetabular, 6 paratrochanteric, and 8 both acetabular and trochanteric) were cleared.
At least 3 samples of tissue were taken for culture in 95% of patient with only 2 positive samples. Frozen section, performed in 42% of patients, were positive for acute inflammation in only 1 case (4.8%).
Statistical analysis
Patient demographics, clinical data and implant features were analyzed using descriptive statistics, such as means, ranges, and percentages. Values were compared using non-parametric tests as Fisher test and Wilcoxon-Mann-Whitney test. The threshold for significance was P=0.05. All statistical analyses were performed using R version 3.5.1.
Results
Clinical and radiographic results
An average follow-up of 3.3±2.2 years was achieved (range, 1–8 years). One patient was lost to the final follow-up. The mean age at revision was 67.4±11.9 (range, 42–83) years. The implants were revised after 100±40.6 (range, 12–180) months. The reasons for revisions were: aseptic loosening and metal ions over the threshold (47.6%, 10), pain and metal ions over the threshold (38.1%, 8). The mean postoperative HHS increased significantly to 88.3±9.2 (range, 68–97) points at final follow-up (preoperative value, 50.3±4.6 points) (P<0.001). The mean surgical time was 132±38.9 min.
Pre-revision radiographic measurements were:
❖ Cup inclination angle (°): 50.2±12.3 (range, 29–62);
❖ Cup anteversion angle (°): 8±17.6 (range, −23 to 42);
❖ Stem antetorsion (°): 8.6±16 (range, −15 to 53);
❖ Combined anteversion (°): 38% of implants reached the anteversion target of 25–50° and only 2 cups of them (10.5%) had an inclination lower than 45° (Figure 2).
Figure 2.

The combined anteversion (cup anteversion on the Y-axis, stem antetorsion on the X-axis) of the pseudotumor cohort is acceptable in less than half of the implants (in the red circle).
The pseudotumors were stratified in: C1 in 3 cases (14.2%), C2 in 9 cases (42.9%), C3 in 9 cases (42.9%) (Figure 3).
Figure 3.
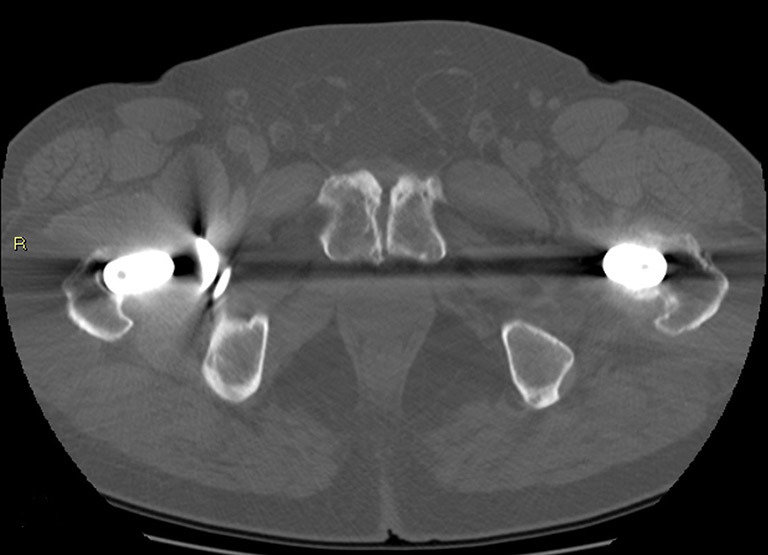
Large pseudotumor of the left MOM total hip arthroplasty with a solid component protruded anteriorly in axial image. MOM, metal-on-metal.
Post-revision radiographic measurements were:
❖ Cup inclination (°): 42.8±8.3 (range, 31–61);
❖ Cup anteversion (°): 14.3±7.2 (range, 5–22);
❖ Center of rotation height (mm): 24.7±9.8 (range, 13–43);
❖ Center of rotation medialization (mm): 35.6±7.3 (range, 24–58);
❖ Femoral offset (mm): 40.8±8.6 (range, 30–60);
❖ Leg length discrepancy (mm): 2.6±11 (range, −15 to 25).
No cup loosening occurred at the final follow-up. The radiolucent lines around the stem were stable over time (9 patients, 42.9%). The cup osseointegration was good in any cases except one (94% with more than 3 parameters): specifically, 4 (22.2%) of the cases showed all 5 signs of bone growth (Figure 4). Radiolucency around the cup was reported in 2 cases (11.1%), involving only the De Lee-Charnley B zone.
Figure 4.

Three-year outcome. (A) Right MOM total hip arthroplasty failed due to pseudotumor, high metal ions in the serum and pain. (B) The one stage revision with isolated acetabular component revision was performed with an ultraporous 3D printed cup and ceramic-on-ceramic bearings and showed successful radiographic outcomes at 3-year follow-up. MOM, metal-on-metal; 3D, three-dimensional.
Complications and re-revisions
Five complications occurred in 21 different MOM revisions (23.8%).
There were 3 (14.3%) wound infections in the first month after revision: orally administered antimicrobial therapy was successful in 2 cases, in the third surgical debridement with implant retention was needed. Two out of 3 patients are those who had previously been explanted due to a preoperative diagnosis of infection.
A dislocation occurred 5 months after the revision and was successfully treated conservatively.
One patient underwent hip arthroscopy due to psoas impingement after 6 years.
We reported 3 (14.2%) recurrences of pseudotumor. All the patients complained of local symptomatology, without evidence of metal ion level beyond the threshold. One pseudotumor recurrence was due to an incomplete excision of the mass due to the large intrapelvic extension (Anderson grading system: C3). The other two recurrences were observed in explanted patients (Anderson grading system: C2). One recurrence was surgically treated, one treated with selective arterial embolization and one followed with close follow up.
No re-revision was performed at the final follow-up.
Metal ion concentrations in serum
Samples of 13 patients preoperatively (61.9%) and 7 (33.3%) correspondent samples 1 year after surgery were available. No patient has been exposed to any other known metal ion source.
The mean post-revision Co ion value in serum was 2.7±3.1 (range, 0.2–6.7) µg/L, with a pre-revision Co ion level of 18.8±27.2 (range, 0.1–102) µg/L. In the 7 cases that could be evaluated, patients with Co ions in serum over the threshold decreased from 85.7% to 0%.
The level of Cr ions in serum was 14.3±27 (range, 0.6–103) µg/L in the pre-revision sampling and reached an average postoperative value of 2.8±2.8 (range, 0.5–6.4) µg/L. In the 7 cases that could be evaluated, patients with Cr ions in serum over the threshold decreased from 85.7% to 0%.
Discussion
Key findings
One stage surgical strategy (complete pseudotumor excision and revision hip even with isolated component reimplantation) in pseudotumors due to failed MOM arthroplasty was feasible in 85.7% of the cases and provided good clinical outcomes and dependable radiographic outcomes. Despite the high rate of complications (23.8%), no re-revision was needed at mid-term: metal ion concentrations in the serum were minimized.
Strengths and limitations
The study provided a sound surgical revision strategy for a sizeable case series of large pseudotumors in failed MOM arthroplasty. However, the retrospective design, the lack of control group, the mean 3-year follow-up after revision were the main limitations of the study. Only a small part of the cohort underwent metal ion level analysis. Moreover, the presence of many confounding factors (demographics and intraoperative) was another notable drawback: the unique features of patients, implants and pseudotumors, depicting different specific revision scenarios, preclude standard surgical treatment algorithm in adverse local tissue reactions and require tailored revision surgeries.
Comparison with similar researches and explanations of findings
The correct staging and treatment of pseudotumors are still debated. Diagnosis is often challenging: many MOM implants with massive adverse reactions can be almost asymptomatic in even half of the cases (17). The first-line diagnostic techniques, such as demographic characteristics, X-rays, and metal ion dosage, are not always effective in predicting adverse reactions (18).
However, positioning of the implants could be highly suggestive: in our case series, only 11% of the hips had an acceptable three-dimensional positioning. The improper positioning of the component is still a matter of debate: Castagnini et al. showed that over a third of the revised ASR XL implants had inadequate positioning on at least one-dimensional plane (15). The reason for the consequent inflammatory reaction can be ascribed to edge load, which induces wear debris and a consequent exuberant inflammatory response, causing a pseudotumor (15).
As already evident in literature, the study of Co ions is not always predictive of pseudotumor (3). Only 61.5% of the patients in the present series showed ions above the classic threshold value of 7 mg/L. These percentages were also observed in a retrospective series of resurfacing implants with adverse reactions: 40–50% of patients did not show high blood ions despite the pseudotumor (18). Therefore, only a high clinical suspicion and axial imaging can allow to identify patients with pseudotumor.
Surgical treatment is no less debated. A single or two step procedure was equally promoted (10,11). The reference strategy of the present case series was based on the complete pseudotumor eradication and isolated revision of the loosened component and the articular coupling (non-MOM): this strategy appears appropriate, especially if sepsis is not suspected and taper is not worn. Non-MOM couplings allow to minimize recurrence of pseudotumor due to trunnionitis or bearing surface wear. In our case series, only 85% of implants were revised, the remaining cases were explanted due to difficult septic local processes and severe local soft tissue damage. In the remaining 18 cases, at an average follow-up of 3 years, there was a significant increase of HHS but many complications occurred (23.8%). Complications mainly were dislocations, infections and hematoma: in half of these cases, a surgical procedure was required, although no re-revision occurred at the last follow-up (3-year). The most recent case series by Liow et al. on revisions of MOM hips with pseudotumor (one stage revision of the acetabular component with tantalum cups and cross-linked polyethylene/Delta coupling) showed a complication rate of 14% at 2 and a half years and a re-revision rate equal to 7% (19). The most recent implants and couplings for revision hips after pseudotumors seem to improve the clinical outcomes, however, a certain rate of complications/failures should be put into account.
We reported 3 cases (14.2%) of pseudotumor recurrence and a new surgical excision was necessary in one case. In these cases, the first removal of pseudotumor was minimal in order to reduce the invasiveness of the procedure and the damage to soft tissues, highlighting that a non-radical surgery can significantly increase the recurrence rates.
Another concern about MOM implants complicated by pseudotumors are periprosthetic infections. The pre-operative diagnosis is ineffective due to altered thresholds. In our series, infection rate was 14.2% and either blood CRP value, frozen sections and intraoperative samples demonstrated unreliable. Also, Favetti, who reported an infection rate of 30% in one-stage MOM revisions, highlighted the difficulty of anticipating infection in the pre-operative period (11). It is therefore suggested to have high threshold of suspicion. A two-stage treatment appears adequate in case of suspected sepsis.
Implications and actions needed
One stage revisions of failed MOM arthroplasty with complete pseudotumor removal showed effective outcomes: non-MOM couplings, isolated component revision with ultraporous cups and aggressive debridement are probably the gold-standard of treatment, according to the literature and the present case series. However, there is a substantial lack of comparative studies, precluding the stratification of pseudotumors and possible alternative options in some subcategories. Any definitive conclusion cannot be drawn due to the many limits of the current study (the retrospective design, the modest cohort, the lack of control group), however the technical and ethical difficulties in the conduction of comparative trails hinder obtaining higher quality findings.
Conclusions
Failed MOM prostheses with large pseudotumors present numerous pitfalls at the pre-operative, intra-operative and post-operative level. One stage surgical treatment with non-MOM couplings appears acceptable: a ceramic-polyethylene or ceramic-ceramic coupling should be implanted (Figure 2). The operating technique should be aimed at eradicating the pseudotumor as completely as possible. Several complications should be expected.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: This work was partially supported by Italian Program of Donations for Research (“5 per mille”, anno 2017–redditi 2016).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by regional ethics committee of Comitato Etico Area Vasta Emilia Centro (CE-AVEC 433/2019/Oss/IOR) and individual consent for this retrospective analysis was waived.
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://aoj.amegroups.com/article/view/10.21037/aoj-22-45/rc
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://aoj.amegroups.com/article/view/10.21037/aoj-22-45/coif). FC serves as an unpaid editorial board member of Annals of Joint from May 2022 to April 2024. The other authors have no conflicts of interest to declare.
Data Sharing Statement
Available at https://aoj.amegroups.com/article/view/10.21037/aoj-22-45/dss
References
- 1.Haddad FS, Thakrar RR, Hart AJ, et al. Metal-on-metal bearings: the evidence so far. J Bone Joint Surg Br 2011;93:572-9. 10.1302/0301-620X.93B4.26429 [DOI] [PubMed] [Google Scholar]
- 2.Natu S, Sidaginamale RP, Gandhi J, et al. Adverse reactions to metal debris: histopathological features of periprosthetic soft tissue reactions seen in association with failed metal on metal hip arthroplasties. J Clin Pathol 2012;65:409-18. 10.1136/jclinpath-2011-200398 [DOI] [PubMed] [Google Scholar]
- 3.Konan S, Duncan CP, Masri BS, et al. What Is the Natural History of Asymptomatic Pseudotumors in Metal-on-metal THAs at Mid-term Followup? Clin Orthop Relat Res 2017;475:433-41. 10.1007/s11999-016-4981-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Matharu GS, Ostlere SJ, Pandit HG, et al. What is the natural history of asymptomatic pseudotumours in metal-on-metal hip resurfacing patients? Hip Int 2016;26:522-30. 10.5301/hipint.5000387 [DOI] [PubMed] [Google Scholar]
- 5.Engh CA, Jr, Ho H, Padgett DE. The surgical options and clinical evidence for treatment of wear or corrosion occurring with THA or TKA. Clin Orthop Relat Res 2014;472:3674-86. 10.1007/s11999-014-3652-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kemp MA, Mitra A, da Costa TM, et al. Bearing exchange in the management of pseudotumours. Ann R Coll Surg Engl 2013;95:266-70. 10.1308/003588413X13511609958497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sassoon AA, Barrack RL. Pseudotumour formation and subsequent resolution in metal-on-metal total hip arthroplasty following revision: Instructional review and an illustrative case report with revision using a dual mobility design. Bone Joint J 2016;98-B:736-40. 10.1302/0301-620X.98B6.36908 [DOI] [PubMed] [Google Scholar]
- 8.De Smet KA, Van Der Straeten C, Van Orsouw M, et al. Revisions of metal-on-metal hip resurfacing: lessons learned and improved outcome. Orthop Clin North Am 2011;42:259-69, ix. 10.1016/j.ocl.2011.01.003 [DOI] [PubMed] [Google Scholar]
- 9.Wyles CC, Larson DR, Houdek MT, et al. Utility of synovial fluid aspirations in failed metal-on-metal total hip arthroplasty. J Arthroplasty 2013;28:818-23. 10.1016/j.arth.2012.11.006 [DOI] [PubMed] [Google Scholar]
- 10.Cottino U, Dettoni F, Risitano S, et al. Two-Stage Treatment of a Large Pelvic Cystic Pseudotumor in a Metal-On-Metal Total Hip Arthroplasty. Joints 2017;5:121-4. 10.1055/s-0037-1603676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Favetti F, Mazzotta G, Papalia M, et al. Contamination of revision procedures in patients with adverse tissues reaction to metal on metal implant. Eur Rev Med Pharmacol Sci 2019;23:86-93. [DOI] [PubMed] [Google Scholar]
- 12.Castagnini F, Valente G, Crimi G, et al. Component positioning and ceramic damage in cementless ceramic-on-ceramic total hip arthroplasty. J Orthop Sci 2019;24:643-51. 10.1016/j.jos.2018.12.011 [DOI] [PubMed] [Google Scholar]
- 13.Lucchini S, Castagnini F, Giardina F, et al. Cementless ceramic-on-ceramic total hip arthroplasty in post-traumatic osteoarthritis after acetabular fracture: long-term results. Arch Orthop Trauma Surg 2021;141:683-91. 10.1007/s00402-020-03711-0 [DOI] [PubMed] [Google Scholar]
- 14.Anderson H, Toms AP, Cahir JG, et al. Grading the severity of soft tissue changes associated with metal-on-metal hip replacements: reliability of an MR grading system. Skeletal Radiol 2011;40:303-7. 10.1007/s00256-010-1000-7 [DOI] [PubMed] [Google Scholar]
- 15.Castagnini F, Mariotti F, Tassinari E, et al. lsolated acetabular revisions of articular surface replacement (ASR) XL implants with highly porous titanium cups and Delta bearings. Hip Int 2021;31:250-7. 10.1177/1120700019874442 [DOI] [PubMed] [Google Scholar]
- 16.Telleria JJ, Gee AO. Classifications in brief: Paprosky classification of acetabular bone loss. Clin Orthop Relat Res 2013;471:3725-30. 10.1007/s11999-013-3264-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hart AJ, Satchithananda K, Liddle AD, et al. Pseudotumors in association with well-functioning metal-on-metal hip prostheses: a case-control study using three-dimensional computed tomography and magnetic resonance imaging. J Bone Joint Surg Am 2012;94:317-25. 10.2106/JBJS.J.01508 [DOI] [PubMed] [Google Scholar]
- 18.van der Weegen W, Sijbesma T, Hoekstra HJ, et al. Treatment of pseudotumors after metal-on-metal hip resurfacing based on magnetic resonance imaging, metal ion levels and symptoms. J Arthroplasty 2014;29:416-21. 10.1016/j.arth.2013.06.021 [DOI] [PubMed] [Google Scholar]
- 19.Liow MH, Dimitriou D, Tsai TY, et al. Preoperative Risk Factors Associated With Poor Outcomes of Revision Surgery for "Pseudotumors" in Patients With Metal-on-Metal Hip Arthroplasty. J Arthroplasty 2016;31:2835-42. 10.1016/j.arth.2016.05.034 [DOI] [PubMed] [Google Scholar]