

Abstract
目的
探讨老年原发性高血压(essential hypertension,EH)合并不稳定型心绞痛(unstable angina,UA)患者血清γ-谷氨酰基转移酶与血小板比值(γ-glutamyl transferase-to-platelet ratio,GPR)、单核细胞与高密度脂蛋白胆固醇比值(monocyte count to high-density lipoprotein ratio,MHR)的水平及意义。
方法
选取2018年9月至2019年9月承德医学院附属医院心脏内科以EH收入院且年龄≥60岁并行冠状动脉造影的患者218例,根据是否合并UA分为EH+UA组(n=113)和EH组(n=105),另选择疑诊冠心病入院冠状动脉造影正常的患者为对照组(n=106)。比较各组患者的一般资料、血生化指标、GPR及MHR的差异,并进行偏相关分析及受试者工作特征(receiver operator characteristic,ROC)曲线分析。
结果
与对照组相比,EH+UA组、EH组患者体重指数(body mass index,BMI)、三酰甘油(tyiglyceride,TG)、GPR、MHR均升高,高密度脂蛋白胆固醇(high-density lipoprotein-cholesterol,HDL-C)降低(均 P<0.05);EH+UA组患者白细胞计数、丙氨酸转氨酶(alanine aminotransferase,ALT)、尿酸水平均升高(均P<0.05);与EH组相比,EH+UA组患者GPR、MHR均升高(均P<0.05)。偏相关分析显示:在控制降压药及降脂药后,GPR与BMI、白细胞计数、ALT、TG、尿酸均呈正相关(分别r=0.160、0.111、0.205、0.250、0.154,均P<0.05),与HDL-C呈负相关(r=-0.238,P<0.05);MHR与BMI、ALT、TG、尿酸、GPR均呈正相关(分别r=0.186、0.307、0.157、0.141、0.223,均P<0.05),与HDL-C呈负相关(r=-0.610,P<0.001)。ROC曲线分析表明GPR具有较高特异性和阳性预测价值,而MHR具有较高的敏感度,当两指标联合检测时,敏感度及阳性预测价值更高。
结论
GPR、MHR与EH+UA存在相关性,且两指标联合检测对老年EH+UA具有一定的辅助诊断价值。
Keywords: γ-谷氨酰基转移酶与血小板比值, 单核细胞与高密度脂蛋白胆固醇比值, 原发性高血压, 不稳定型心绞痛
Abstract
Objective
To investigate the level and significance of serum γ-glutamyl transferase-to-platelet ratio (GPR) and monocyte count to high-density lipoprotein ratio (MHR) in patients with essential hypertension (EH) and unstable angina (UA).
Methods
A total of 218 patients with coronary angiography aged ≥60 years, who were admitted to the EH hospital of the Department of Cardiac Medicine, Affiliated Hospital of Chengde Medical College, were selected from September 2018 to September 2019. They were divided into an EH+UA group (n=113) and an EH group (n=105). In addition, 106 patients with normal coronary angiography who were diagnosed with coronary heart disease were selected as a control group. The general data, blood biochemical indicators, GPR and MHR in each group were compared, and partial correlation analysis and receiver operator characteristic (ROC) curve analysis were performed.
Results
Compared with the control group, patients in the EH+UA group and the EH group had higher body mass index (BMI), tyiglyceride (TG), GPR, and MHR, and lower high-density lipoprotein-cholesterol (HDL-C) (all P<0.05); and patients in the EH+UA group had higher white blood cell counts, alanine aminotransferase (ALT), and uric acid (all P<0.05). Compared with the EH group, patients in the EH+UA group had higher GPR and MHR (both P<0.05). Partial correlation analysis showed that after controlling the antihypertensive drugs and lipid-lowering drugs, GPR was found to be positively correlated with BMI, white blood cell count, ALT, TG, and uric acid (r=0.160, 0.111, 0.205, 0.250, 0.154, respectively, all P<0.05), which was negatively correlated with HDL-C (r=-0.238, P<0.05); MHR was positively correlated with BMI, ALT, TG, uric acid, and GPR (r=0.186, 0.307, 0.157, 0.141, 0.223, respectively, all P<0.05), and negatively correlated with HDL-C (r=-0.610, P<0.001). ROC curve analysis showed that GPR had higher specificity and positive predictive value, while MHR had higher sensitivity. When the two indicators were combined, the sensitivity and positive predictive value were higher.
Conclusion
There is a correlation between GPR, MHR and EH combined with UA pectoris, and the combined detection of the two indicators has adjuvant diagnostic value for elderly EH combined with UA.
Keywords: γ-glutamyl transferase to platelet ratio, monocyte count to high density lipoprotein ratio, essential hypertension, unstable angina
目前,我国心血管病患病率及病死率总体处于上升阶段。据推算我国冠心病现患人数约1 100万,原发性高血压(essential hypertension,EH)现患人数约2.4亿[1]。冠心病是危害我国人民健康的重要疾病,也是导致死亡的首要原因。2016年我国农村心脏病病死率为151.18/10万,城市心脏病病死率为138.70/10万[2]。高血压是主要的心血管疾病之一,也是冠心病的独立危险因素。据统计我国约71.8%的冠心病患者合并高血压[3]。当冠心病与高血压同时存在时,心血管事件发生率明显增加。γ-谷氨酰基转移酶(γ-glutamyl transferase,GGT)与血小板比值(γ-glutamyl transferase to platelet ratio,GPR)不仅是肝纤维化或肝癌的独立预测因子[4-5],还是冠心病患者经皮冠脉介入术(percutaneous coronary intervention,PCI)远期不良预后的独立预测指标[6]。单核细胞计数与高密度脂蛋白胆固醇比值(monocyte count to high-density lipoprotein ratio,MHR)是预测慢性肾脏疾病和心房颤动(atrial fibrillation,AF)术后心血管疾病恶化的一项新指标[7-8],它与急性心肌梗死PCI预后有关[9]。但GPR、MHR与冠心病合并高血压的关系尚未见相关报道。本研究旨在探讨GPR、MHR与EH合并不稳定型心绞痛(unstable angina,UA)的相关性。
1. 对象与方法
1.1. 对象
选取2018年9月至2019年9月承德医学院附属医院(以下简称我院)心脏内科以EH收入院且年龄≥ 60岁并行冠状动脉造影的患者218例,根据是否合并UA分为EH+UA组(n=113)和EH组(n=105),另选择疑诊冠心病入院冠状动脉造影正常患者为对照组(n=106)。本研究经承德医学院附属医院医学伦理委员会批准,研究对象均知情同意。纳入标准:1)年龄≥ 60岁;2)符合EH诊断标准[10];3)符合UA诊断标准[11]。排除标准:1)继发性高血压患者;2)心脏瓣膜病患者;3)呼吸睡眠暂停综合征患者;4)原发性肺动脉高压患者;5)心功能不全患者;6)恶性肿瘤患者;7)肝肾功能不全患者;8)内分泌系统疾病及风湿免疫疾病患者。
1.2. 临床基本资料收集
记录所有患者的性别、年龄、身高、体重、体重指数(body mass index,BMI)、吸烟史、饮酒史、是否服用降压药、是否服用降脂药。所有研究对象于入院次日清晨抽取5 mL空腹静脉血,在我院检验科进行血常规、肝功能、肾功能、血脂等指标检测,计算GPR、MHR。
1.3. 统计学处理
采用SPSS 25.0统计学软件对数据进行分析,计量资料以均数±标准差( ±s)表示,3组比较采用单因素方差分析(F检验);组间比较采用Bonferroni检验;计数资料用率(%)表示,组间比较采用χ2检验。GPR、MHR与各指标的相关性采用偏相关分析。采用受试者工作特征(receiver operator characteristic,ROC)曲线评估GPR、MHR及两指标联合对EH+UA患者的诊断效能,以P<0.05为差异有统计学意义。
2. 结 果
2.1. 基本资料
3组的性别、年龄、吸烟、饮酒比较,差异均无统计学意义(均P>0.05),服用降压药、服用降脂药、BMI、白细胞计数、ALT、TG、HDL-C、尿酸、GPR、MHR比较,差异均有统计学意义(均P<0.05)。经两两比较分析发现:EH+UA组、EH组BMI、TG、GPR、MHR均高于对照组,HDL-C均低于对照组(均P<0.05);EH+UA组白细胞计数、ALT、尿酸均高于对照组(均P<0.05);EH+UA组GPR、MHR均高于EH组(均P<0.05,表1)。
表1.
3组基本资料的比较
Table 1 Comparison of basic data among the 3 groups
| 组别 | n | 男/女 | 年龄/岁 | 吸烟/[例(%)] | 饮酒/[例(%)] |
|---|---|---|---|---|---|
| EH+UA组 | 113 | 63/50 | 68.23±5.42 | 59(52.2) | 47(41.6) |
| EH组 | 105 | 53/52 | 67.52±4.60 | 57(54.3) | 43(41.0) |
| 对照组 | 106 | 61/45 | 67.99±4.42 | 50(47.2) | 45(42.5) |
| F/χ2 | 1.152 | 0.586 | 1.135 | 0.049 | |
| P | 0.562 | 0.557 | 0.567 | 0.976 |
| 组别 | 服用降压药/[例(%)] | 服用降脂药/[例(%)] | BMI/(kg·m-2) | 白细胞/(×109·L-1) | ALT/(U·L-1) |
|---|---|---|---|---|---|
| EH+UA组 | 75(66.4) | 52(46.0) | 25.79±3.34* | 6.70±1.51* | 36.52±36.45* |
| EH组 | 78(74.3) | 15(14.3) | 25.40±3.62* | 6.31±1.29 | 29.26±12.76 |
| 对照组 | ― | ― | 24.23±2.33 | 6.08±1.75 | 25.63±12.11 |
| F/χ2 | 142.326 | 74.482 | 7.164 | 4.608 | 6.003 |
| P | <0.001 | <0.001 | 0.001 | 0.011 | 0.003 |
2.2. GPR、MHR与相关指标的相关性分析
采用偏相关分析,在控制降压药及降脂药后发现:GPR与BMI、白细胞计数、ALT、TG、尿酸均呈正相关,与HDL-C呈负相关;MHR与BMI、ALT、TG、尿酸均呈正相关,与HDL-C呈负相关;GPR与MHR呈正相关(均P<0.05,表2)。
表2.
在控制降压药及降脂药后,GPR及MHR与一般资料、血生化资料的相关性
Table 2 Correlation between GPR, MHR and general data, blood biochemical data after controlling antihypertensive drugs and lipid-lowering drugs
| 组别 | TG/(mmom·L-1) | HDL-C/(mmom·L-1) | 尿酸/(μmol·L-1) | GPR | MHR |
|---|---|---|---|---|---|
| EH+UA组 | 1.92±1.18* | 1.06±0.22* | 326.62±70.10* | 0.33±0.14*† | 6.85±2.36*† |
| EH组 | 1.97±1.67* | 1.10±0.25* | 312.90±72.10 | 0.25±0.29* | 6.17±1.92* |
| 对照组 | 1.47±1.05 | 1.29±0.30 | 291.09±87.63 | 0.17±0.11 | 4.99±1.71 |
| F/χ2 | 6.232 | 25.857 | 5.913 | 18.522 | 23.518 |
| P | 0.002 | <0.001 | 0.003 | <0.001 | <0.001 |
UA:不稳定型心绞痛;BMI:体重指数;ALT:丙氨酸转氨酶;TG:三酰甘油;HDL-C:高密度脂蛋白胆固醇;GPR:γ谷氨酰基转移酶与血小板比值;MHR:单核细胞与高密度脂蛋白胆固醇比值;与对照组比较,*P<0.05;与EH组比较, †P<0.05。
表2.
在控制降压药及降脂药后,GPR及MHR与一般资料、血生化资料的相关性
Table 2 Correlation between GPR, MHR and general data, blood biochemical data after controlling antihypertensive drugs and lipid-lowering drugs
| 指标 | 统计量 | GPR | MHR | 年龄 | BMI | 白细胞 | ALT | TG | HDL-C | 尿酸 |
|---|---|---|---|---|---|---|---|---|---|---|
| GPR | r | ― | 0.223 | -0.051 | 0.160 | 0.111 | 0.205 | 0.250 | -0.238 | 0.154 |
| P | ― | <0.001 | 0.364 | 0.004 | 0.046 | <0.001 | <0.001 | <0.001 | 0.006 | |
| MHR | r | 0.223 | ― | 0.013 | 0.186 | 0.015 | 0.307 | 0.157 | -0.610 | 0.141 |
| P | <0.001 | ― | 0.814 | 0.001 | 0.787 | <0.001 | 0.005 | <0.001 | 0.012 |
GPR:γ谷氨酰基转移酶与血小板比值;MHR:单核细胞与高密度脂蛋白胆固醇比值;BMI:体重指数;ALT:丙氨酸转氨酶;TG:三酰甘油;HDL-C:高密度脂蛋白胆固醇。
2.3. ROC曲线分析
GPR、MHR、GPR+MHR诊断EH+UA的ROC曲线下面积(area under curve,AUC)分别为0.846、0.749、0.871。选取约登指数最大值为阈值,GPR、MHR、GPR+MHR诊断EH+UA的最佳截断值分别为0.176、4.566、0.294,所对应的灵敏度分别为89.4%、91.2%、97.3%,特异度分别为68.9%、48.1%、63.2%(图1)。
图1.
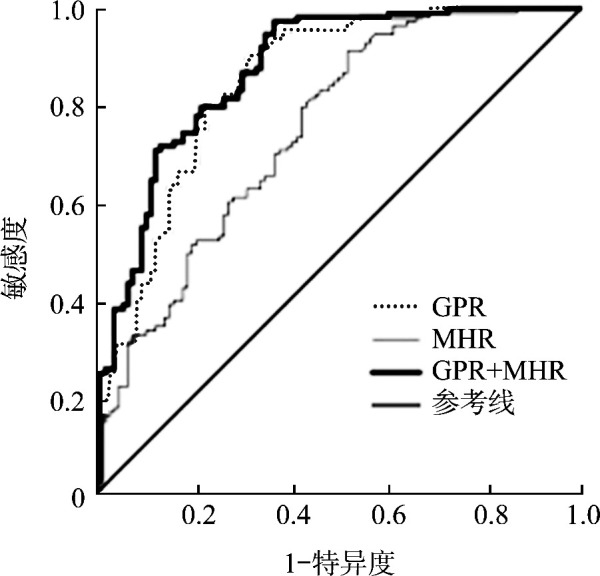
GPR、MHR、GPR+MHR诊断EH+UA的ROC曲线
Figure 1 ROC curve of diagnosing EH+UA by GPR, MHR, and GPR+MHR
3. 讨 论
高血压是冠心病的独立危险因素,收缩压每升高20 mmHg(1 mmHg=0.133 kPa)或舒张压每升高 10 mmHg,心脑血管病发生的风险倍增[10]。动脉粥样硬化是一种慢性炎症过程,也是高血压和冠心病共同的病理机制。
动脉粥样硬化是由于氧化和抗氧化系统之间不平衡引起的氧化应激反应[12]。GGT是肝病和过量饮酒的敏感指标,对谷胱甘肽的调节和降解以及氧化应激的产生具有重要作用。GGT参与细胞外氧自由基的产生,导致低密度脂蛋白胆固醇(low-density lipoprotein-cholesterol,LDL-C)氧化,因此GGT是评估氧化应激和心血管风险的有前途的生物标志物[13]。GPR是最新发现的一种新型生物标志物,既往研究[4-5, 14-15]表明GPR与肝纤维化、肝硬化、肝癌以及肝衰竭具有明显的相关性。而Zheng等[6]通过对5 636名接受PCI的冠心病患者进行回顾性研究,发现GPR是冠心病患者PCI术后长期不良预后新的独立预测指标。本研究结果表明:EH+UA组、EH组GPR水平明显高于对照组,EH+UA组明显高于EH组。这提示GPR与心血管疾病及严重程度的发生有关,其可能通过影响体内脂质氧化应激来促进动脉粥样硬化的形成,进而导致高血压、冠心病的发生。相关性分析显示GPR与BMI、TG、白细胞计数呈正相关,与HDL-C呈负相关,进一步说明GPR与脂质代谢以及炎症反应有关,但GPR与脂质代谢及体内炎症反应的确切作用机制尚未完全明确,仍需要进一步的基础实验研究。ROC曲线分析表明GPR对老年EH+UA具有一定的诊断预测价值,根据约登指数计算得出GPR为0.176时对老年EH+UA诊断预测价值最高。
炎症在动脉粥样硬化和动脉粥样硬化斑块破裂中起重要作用,这是急性冠状动脉综合征病理生理的主要机制。单核细胞的激活是动脉粥样硬化过程的始动环节。作为组织巨噬细胞和泡沫细胞的来源,循环中单核细胞的计数被认为是新斑块发展的先兆[16]。内皮功能障碍是动脉粥样硬化发展的第一阶段。当内皮细胞功能障碍时,单核细胞开始向内皮聚积,然后牢固地黏附于内皮上,再逐渐迁移到内皮下,在一些酶的作用下成为巨噬细胞,最终分化为泡沫细胞[17]。HDL具有抗炎、抗氧化和抗血栓形成的作用[18],它能逆向转运巨噬细胞内的胆固醇,同时抑制内皮细胞黏附分子表达和防止单核细胞聚集到动脉壁,还可通过直接作用于单核细胞来预防炎症反应。研究[9]表明MHR升高与全身性炎症和内皮功能障碍有关,被定义为心血管疾病中一种基于炎症的新型预后标志物。Kanbay等[7]研究发现MHR可作为慢性肾脏病患者心血管事件的独立预测因子,并随着估算的肾小球滤过率(estimated glomerular filtration rate,eGFR)的降低而增加。Canpolat等[19]研究发现在慢血流患者中MHR升高,且证明MHR升高与缓慢冠状动脉血流之间有相关性。Cetin等[20]认为MHR可能是急性冠状动脉综合征患者冠状动脉疾病严重程度的独立预测指标。Arısoy等[21]报道:在ST段抬高的心肌梗死患者中,高血栓负荷患者的MHR高于低血栓负荷患者。MHR可能是血栓负荷的独立预测因子。本研究表明:EH+UA组、EH组MHR水平明显高于对照组,EH+UA组高于EH组,提示MHR与心血管疾病的发生以及疾病复杂程度有关。相关性分析显示MHR与BMI、TG呈正相关,与HDL-C呈负相关,说明MHR影响体内脂质代谢过程。ROC曲线分析进一步表明MHR可以预测老年EH+UA的发生,但特异度不高(48.1%),根据约登指数计算MHR为4.566时有一定的诊断预测价值。进一步将GPR、MHR两指标联合检测,结果显示其对老年EH+UA的诊断敏感度明显升高(97.3%)。表明两指标联合对预测老年EH+UA的发生较单一指标敏感度明显提高。
综上所述,GPR、MHR与EH+UA存在相关性,EH+UA患者GPR及MHR明显高于对照组及EH组,同时两指标联合检测可提高老年EH+UA辅助诊断的敏感度,因此GPR、MHR有望成为临床辅助诊断EH+UA的一种廉价且易获取的炎症指标。但本研究为单中心、小样本、横断面研究,病例入选过程中可能存在偏倚,一些较轻或较重的病例未入选,影响代表性,同时未进一步探究GPR、MHR对EH+UA患者不同病变支数是否有影响,因此,尚需要多中心、大样本、前瞻性研究加以证实。
基金资助
承德市技术研究与发展计划(201801A026)。
This work was supported by the Technology Research and Development Program from Chengde City, China (201801A026).
利益冲突声明
作者声称无任何利益冲突。
原文网址
http://xbyxb.csu.edu.cn/xbwk/fileup/PDF/202104373.pdf
参考文献
- 1. 胡盛寿, 高润霖, 刘力生, 等. 《中国心血管病报告2018》概要[J]. 中国循环杂志, 2019, 34(3): 209-220. [Google Scholar]; HU Shengshou, GAO Runlin, LIU Lisheng, et al. Summary of the 2018 report on cardiovascular diseases in China[J]. Chinese Circulation Journal, 2019, 34(3): 209-220. [Google Scholar]
- 2. 国家卫生和计划生育委员会 . 中国卫生和计划生育统计年鉴-2017[M]. 北京: 中国协和医科大学出版社, 2017. [Google Scholar]; National Health and Family Planning Commission . China health and family planning statistical yearbook-2017[M]. Beijing: Peking Union Medical College Publishing House, 2017. [Google Scholar]
- 3. 张威, 朱航, 姚思宇, 等. 不稳定性心绞痛合并高血压患者血压昼夜节律研究[J]. 中华心血管病杂志, 2017, 45(7): 585-590. [DOI] [PubMed] [Google Scholar]; ZHANG Wei, ZHU Hang, YAO Siyu, et al. Circadian blood pressure characteristics in hospitalized unstable angina pectoris patients with hypertension[J]. Chinese Journal of Cardiology, 2017, 45(7): 585-590. [DOI] [PubMed] [Google Scholar]
- 4. Lemoine M, Shimakawa Y, Nayagam S, et al. The gamma-glutamyl transpeptidase to platelet ratio (GPR) predicts significant liver fibrosis and cirrhosis in patients with chronic HBV infection in West Africa[J]. Gut, 2016, 65(8): 1369-1376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Park YE, Kim BK, Park JY, et al. Gamma-glutamyl transpeptidase-to-platelet ratio is an independent predictor of hepatitis B virus-related liver cancer[J]. J Gastroenterol Hepatol, 2017, 32(6): 1221-1229. [DOI] [PubMed] [Google Scholar]
- 6. Zheng YY, Wu TT, Chen Y, et al. Gamma-glutamyl transferase-to-platelet ratio as a novel predictor of long-term adverse outcomes in patients after undergoing percutaneous coronary intervention: a retrospective cohort study[J]. Thromb Haemost, 2019, 119(6): 1021-1030. [DOI] [PubMed] [Google Scholar]
- 7. Kanbay M, Solak Y, Unal HU, et al. Monocyte count/HDL cholesterol ratio and cardiovascular events in patients with chronic kidney disease[J]. Int Urol Nephrol, 2014, 46(8): 1619-1625. [DOI] [PubMed] [Google Scholar]
- 8. Canpolat U, Aytemir K, Yorgun H, et al. The role of preprocedural monocyte-to-high-density lipoprotein ratio in prediction of atrial fibrillation recurrence after cryoballoon-based catheter ablation[J]. Europace, 2015, 17(12): 1807-1815. [DOI] [PubMed] [Google Scholar]
- 9. Karataş MB, Çanga Y, Özcan KS, et al. Monocyte to high-density lipoprotein ratio as a new prognostic marker in patients with STEMI undergoing primary percutaneous coronary intervention[J]. Am J Emerg Med, 2016, 34(2): 240-244. [DOI] [PubMed] [Google Scholar]
- 10. 中国高血压防治指南修订委员会 . 中国高血压防治指南2010[J]. 中华心血管病杂志, 2011, 39(7): 579-616. [PubMed] [Google Scholar]; Revision Committee of China Guidelines for Prevention and Treatment of Hypertension . 2010 Chinese guidelines for the management of hypertension [J]. Chinese Journal of Cardiology, 2011, 39(7): 579-616.22088239 [Google Scholar]
- 11. 中华医学会心血管病学分会 . 非ST段抬高型急性冠状动脉综合征诊断和治疗指南(2016)[J]. 中华心血管病杂志, 2017, 45(5): 359-376. [DOI] [PubMed] [Google Scholar]; Branch of Cardiovascular Diseases of Chinese Medical Association . Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndrome (2016)[J]. Chinese Journal of Cardiology, 2017, 45(5): 359-376.28511320 [Google Scholar]
- 12. Mao Y, Qi XL, Xu WJ, et al. Serum gamma-glutamyl transferase: A novel biomarker for coronary artery disease[J]. Med Sci Monit, 2014, 30(20): 706-710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Bharani V, Ramesh V, Rao RN, et al. Evaluation of gamma glutamyl transferase as a marker of cardiovascular risk, in 200 angiographically proven coronary artery disease patients[J]. Indian Heart J, 2017, 69(3): 325-327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ke MY, Zhang M, Su Q, et al. Gamma-glutamyl transpeptidase to platelet ratio predicts short-term outcomes in hepatocellular carcinoma patients undergoing minor liver resection[J]. J Surg Res, 2018, 231: 403-410. [DOI] [PubMed] [Google Scholar]
- 15. Liu LG, Lan Q, Lin L, et al. Gamma-glutamyl transpeptidase-to-platelet ratio predicts the prognosis in HBV-associated acute-on-chronic liver failure[J]. Clin Chim Acta, 2018, 476: 92-97. [DOI] [PubMed] [Google Scholar]
- 16. Gratchev A, Sobenin I, Orekhov A, et al. Monocytes as a diagnostic marker of cardiovascular diseases[J]. Immuno-biology, 2012, 217(5): 476-482. [DOI] [PubMed] [Google Scholar]
- 17. Karabacak M, Kahraman F, Sert M, et al. Increased plasma monocyte chemoattractant protein-1 levels in patients with isolated low high-density lipoprotein cholesterol[J]. Scand J Clin Lab Invest, 2015, 75(4): 327-332. [DOI] [PubMed] [Google Scholar]
- 18. Akboga MK, Yayla C, Balci KG, et al. Relationship between serum albumin level and monocyte-to-high-density lipoprotein cholesterol ratio with saphenous vein graft disease in coronary bypass[J]. Thorac Cardiovasc Surg, 2017, 65(4): 315-321. [DOI] [PubMed] [Google Scholar]
- 19. Canpolat U, Çetin EH, Cetin S, et al. Association of monocyte-to-HDL cholesterol ratio with slow coronary flow is linked to systemic inflammation[J]. Clin Appl Thromb Hemost, 2016, 22(5): 476-482. [DOI] [PubMed] [Google Scholar]
- 20. Cetin MS, Ozcan Cetin EH, Kalender E, et al. Monocyte to HDL cholesterol ratio predicts coronary artery disease severity and future major cardiovascular adverse events in acute coronary syndrome[J]. Heart Lung Circ, 2016, 25(11): 1077-1086. [DOI] [PubMed] [Google Scholar]
- 21. Arısoy A, Altunkaş F, Karaman K, et al. Association of the monocyte to HDL cholesterol ratio with thrombus burden in patients with ST-segment elevation myocardial infarction[J]. Clin Appl Thromb Hemost, 2017, 23(8): 992-997. [DOI] [PubMed] [Google Scholar]