

Abstract
目的
总结腓肠神经营养血管皮瓣修复跖骨中点连线以远前足创面的临床经验,比较该皮瓣修复跖骨中点连线以远及以近创面的临床疗效。
方法
回顾性分析2002年4月至2020年4月间修复小腿中下段、踝及足部皮肤软组织缺损的425例腓肠神经营养血管皮瓣的临床资料。以跖骨中点连线为界,将腓肠神经营养血管皮瓣分为前足组(皮瓣最远端位于该连线以远的皮瓣)和踝周组(皮瓣最远端位于该连线以近的皮瓣)。
结果
前足组皮瓣部分坏死率(14.5%,10/69)高于踝周组(7.0%,25/356),两组比较差异有统计学意义(P<0.05)。前足组和踝周组单独应用该皮瓣或联合简单二期处理覆盖创面的成功率分别为98.6%(68/69)和97.8%(348/356),两组比较差异无统计学意义(P>0.05)。
结论
腓肠神经营养血管皮瓣是修复跖骨中点连线以远的前足皮肤软组织缺损的一种较理想的方法,该皮瓣修复跖骨中点连线以近创面的成活可靠性优于修复跖骨中点连线以远创面。
Keywords: 外科皮瓣, 腓肠神经, 穿支皮瓣, 腓动脉
Abstract
Objectives
To summarize our experience with the sural neurofasciocutaneous flap for reconstructing the soft tissue defects over the forefoot distal to the connecting line of midpoints in the metatarsal bones, and to compare the outcomes between the flap for resurfacing the defects distal and proximal to the connecting line.
Methods
The clinical data of 425 sural neurofasciocutaneous flaps for repairing the soft tissue defects in the middle and lower leg, ankle, and foot between Apr. 2002 and Apr. 2020 were reviewed. Based on the connecting line of midpoints of the metatarsals, the sural neurofasciocutaneous flaps were divided into a forefoot group (flaps with furthest edges distal to the connecting line) and a peri-ankle group (flaps with the furthest edges proximal to the connecting line).
Results
The partial necrosis rate in the forefoot group (14.5%, 10/69) was significantly higher than that in the peri-ankle group (7.0%, 25/356), with significant difference (P<0.05). Using the flap alone or in combination with a simple salvage treatment, the ratio of successful coverages of the defects was 98.6% (68/69) in the forefoot group, and 97.8% (348/356) in the peri-ankle group, respectively, with no statistical difference (P>0.05).
Conclusion
The sural neurofasciocutaneous flap is a better choice for covering the soft tissue defects over the forefoot distal to the connecting line of midpoints of the metatarsal bones. The survival reliability of the sural neurofasciocutaneous flap reconstructing the soft tissue defect proximal to the connecting line is superior to that of the flap reconstructing the defect distal to the connecting line.
Keywords: surgical flap, sural nerve, perforator flap, peroneal artery
腓肠神经营养血管皮瓣已广泛应用于修复小腿中下段、踝及足部皮肤软组织缺损[1-3]。目前该皮瓣修复足部缺损的范围仍有争议,有学者[4-5]认为该皮瓣不宜修复前足创面,但也有学者[6]报道应用该皮瓣成功修复前足创面。在临床实践中,作者观察到腓肠神经营养血管皮瓣修复跖骨中点以远前足创面时,皮瓣出现远端部分坏死的可能性增大[7]。迄今为止,大样本量腓肠神经营养血管皮瓣修复跖骨中点连线以远前足创面少见报道,该皮瓣修复跖骨中点连线以远及以近创面的临床疗效比较罕见报道。2002年4月至2020年4月作者行腓肠神经营养血管皮瓣修复小腿中下段、踝及足部创面425例,其中69例皮瓣修复跖骨中点连线以远前足创面,获得较好临床效果。本研究旨在总结腓肠神经营养血管皮瓣修复跖骨中点连线以远前足皮肤软组织缺损的临床经验,比较该皮瓣修复跖骨中点连线以远及以近创面的临床疗效。
1. 资料与方法
1.1. 一般资料
对419例患者(其中6例患者行双侧皮瓣,故总皮瓣数为425例)行腓肠神经营养血管皮瓣修复小腿中下段、踝及足部皮肤软组织缺损,回顾性分析这些患者的临床资料。纳入标准:皮瓣均为远端蒂腓肠神经营养血管皮瓣,皮瓣筋膜蒂基底部包含腓动脉最远端或其上方穿支。排除标准:1)顺行的腓肠神经营养血管皮瓣;2)穿支蒂腓肠神经营养血管皮瓣;3)皮瓣基底部包含跟外侧动脉穿支或外踝后动脉穿支的低旋转点腓肠神经营养血管皮瓣。本研究获得中南大学湘雅二医院临床研究伦理委员会批准[审批号:(2020)伦审[临研]第(k021)号]。所有患者均签署知情同意书。
患者中,男328例,女91例;年龄为36.6(1.0~81.0)岁。皮肤软组织缺损原因如下:外伤为338例,慢性骨髓炎伴有窦道形成或者慢性溃疡为61例,不稳定性疤痕或疤痕挛缩为9例,肿瘤为17例。皮肤软组织缺损最近端位于小腿中段,最远端位于足趾区域。皮瓣大小5.0 cm×4.0 cm~20.0 cm×15.0 cm。皮瓣旋转点位于外踝尖上方3.5~19.0 cm,其中外踝尖上方3.5~4.5 cm 4例(均为2.0~5.0岁儿童)、5.0~7.0 cm 294例、7.5~9.5 cm 60例、10.0~12.0 cm 54例、12.5~14.0 cm 8例、15.0~19.0 cm 5例。所有创面均合并骨、关节、肌腱和/或内固定外露。
1.2. 分组与评价指标
1.2.1. 分组
以跖骨中点连线为界,将小腿中下段、踝及足部分为前足(跖骨中点连线以远区域)和踝周(跖骨中点连线以近的足部、踝及小腿中下段)两个区域(图1)。将腓肠神经营养血管皮瓣分为前足组(皮瓣转位后最远端位于跖骨中点连线以远的皮瓣)和踝周组(皮瓣转位后最远端位于跖骨中点连线以近的皮瓣)。
图1.
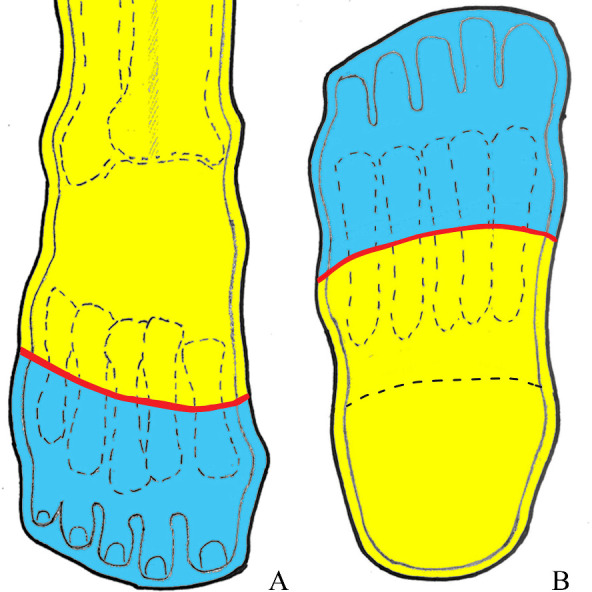
前足及踝周划分示意图
Figure 1 Illustration of demarcation of forefoot and peri-ankle
A: Anterior view; B: Planta pedis view. With the connecting line (red line) of midpoints of metatarsals as boundary, the middle and lower leg, ankle and foot are divided into two regions: forefoot region (distal to the connecting line, blue area) and peri-ankle region (proximal to the connecting line, yellow area).
1.2.2. 皮瓣部分坏死及其危险因素的评价指标
皮瓣完全成活或皮瓣远端坏死长度<1 cm定义为皮瓣成活。皮瓣远端坏死长度≥1 cm定义为皮瓣部分坏死。皮瓣的筋膜蒂长和宽、瓣部长和宽、总长、长宽比及近端位置等指标的描述见文献[8]。
1.3. 两组皮瓣部分坏死率及其危险因素、覆盖创面 成功率比较
比较前足组和踝周组皮瓣的部分坏死率及其可能的危险因素,并比较两组单独应用腓肠神经营养血管皮瓣或联合简单二期处理(包括换药、植皮和二期缝合)覆盖创面的成功率。
1.4. 手术方法
皮瓣采用顺逆结合法[9]切取。前足组皮瓣设计前,可用1根直径3.0 mm斯氏针从足底外侧穿过跖骨基底至胫骨,将踝关节固定于背屈位,以减少旋转点至创面近端的距离,缩短皮瓣筋膜蒂的长度,进而减少皮瓣发生部分坏死的可能性。术后2~3周拔除斯氏针。修复小腿下段胫前纵向创面或跟踝部横向创面时,皮瓣瓣部采用皮岛倾斜的改良设计,以增加修复这些创面皮瓣的成活可靠性[10]。设计、切取皮瓣筋膜蒂时,筋膜蒂表面携带1.5~2.5 cm宽的皮条,皮瓣均通过明通道转位,使通道两侧的皮肤与皮条缝合,以避免蒂部卡压。
1.5. 统计学处理
使用SPSS 21.0统计学软件进行数据分析。计量资料以均数±标准差( ±s)表示,组间比较采用t检验;计数资料以率(构成比)表示,组间比较采用χ 2检验或Fisher确切概率法检验。P<0.05为差异有统计学意义。
2. 结 果
2.1. 皮瓣成活及创面愈合情况
在前足组69例中,皮瓣成活59例(85.5%;图2,3),创面顺利愈合;皮瓣部分坏死10例(14.5%),其中1例二期缝合,8例植皮,1例局部皮瓣转位后残留创面愈合。
图2.

53岁男性患者外伤致左足背皮肤软组织缺损(缺损最远端位于前足)
Figure 2 Fifty-three year-old man suffered from a traumatic soft tissue defect in dorsum of left foot (locating forefoot of the furthest end)
A: Defect after debridement; B: Design of a sural neurofasciocutaneous flap after left ankle was temporarily fixed in dorsiflexion position with a Steinmann pin (red arrow); C: Completely survived flap at the 3th week postoperatively, with the furthest end over dorsal of the 4th and 5th proximal phalanges.
图3.

29岁男性患者外伤致右足背及足底外侧皮肤软组织缺损(缺损最远端位于跖骨中点连线以远的前足)
Figure 3 Twenty-nine year-old man suffered from a traumatic soft tissue defect in lateral dorsum and planta of right foot (the furthest end of the defect locates in the forefoot distal to connecting line of midpoints of metatarsal bones)
A: Flap design after debridement, with a skinstrip overlying adipofascial pedicle; B: Flap appearance at 4 months postoperatively, with the furthest end approaching the 5th metatarsophalangeal joint.
在踝周组356例中,皮瓣成活331例(93.0%,图4);皮瓣部分坏死25例(7.0%),其中1例伤口换药,4例二期缝合,12例植皮,5例局部皮瓣转位后残留创面愈合,剩余3例截肢(2例严重感染未得到控制,另1例术后病理检查为慢性溃疡合并癌变)。前足组皮瓣部分坏死率高于踝周组(χ 2=4.268,P<0.05)。
图4.

54岁女性患者外伤致左小腿下段胫前纵向皮肤软组织缺损
Figure 4 Fifty-four year-old woman suffered from a traumatic longitudinal soft tissue defect in right distal pretibial region
A: Defect after debridement; B: Modified design of a sural neurofasciocutaneous flap with sloped skin island, region surrounded by dotted line represents routinely-designed skin island; C: Flap appearance at the 10th month postoperatively, with the furthest end inperi-ankle.
单独应用腓肠神经营养血管皮瓣或联合简单二期处理(包括换药、植皮和二期缝合,不包括局部皮瓣转位和截肢)覆盖创面的成功率前足组为98.6%(68/69)、踝周组为97.8%(348/356),两者差异无统计学意义(χ 2=0.000,P>0.05)。
所有患者均获随访,随访时间为术后2周~156个月(平均8.1个月)。随访期内创面感染均得到控制,患者对皮瓣的功能和外形满意。固定踝关节于背屈位的斯氏针拔除后,患者踝关节活动无明显影响。
2.2. 两组皮瓣部分坏死的可能危险因素比较
前足组与踝周组的年龄、性别及病因差异均无统计学意义(均P>0.05)。皮瓣近端位置位于第8~第9区段和位于第9区段的构成比,前足组均大于踝周组(χ2 =62.291,P<0.01;χ 2=17.330,P<0.01)。前足组的皮瓣长宽比≥5꞉1构成比及皮瓣瓣部宽≥8 cm的构成比均大于踝周组(均P<0.05,表1)。
表1.
两组皮瓣计数资料的比较
Table 1 Comparison of categorical variables of flaps between the 2 groups
| 组别 | n | 年龄/[例(%)] | 性别/[例(%)] | 病因/[例(%)] | |||||
|---|---|---|---|---|---|---|---|---|---|
| ≤40岁 | >40岁 | 男 | 女 | 外伤 | 慢性溃疡 | 肿瘤 | 不稳定瘢痕 | ||
| 前足组 | 69 | 33(47.8) | 36(52.2) | 53(76.8) | 16(23.2) | 58(84.1) | 8(11.6) | 1(1.4) | 2(2.9) |
| 踝周组 | 356 | 194(54.5) | 162(45.5) | 281(78.9) | 75(21.1) | 280(78.7) | 53(14.9) | 16(4.5) | 7(1.9) |
| χ 2 | 1.033 | 0.155 | 2.587 | ||||||
| P | 0.309 | 0.694 | 0.460 | ||||||
| 组别 | 皮瓣近端位置/[例(%)] | 长宽比/[例(%)] | 瓣部宽/[例(%)] | |||||
|---|---|---|---|---|---|---|---|---|
| 第6区段及以下区段 | 第7区段 | 第8区段 | 第9区段 | <5꞉1 | ≥5꞉1 | <8 cm | ≥8 cm | |
| 前足组 | 0 | 0 | 48(69.6) | 21(30.4) | 15(21.7) | 54(78.3) | 19(27.5) | 50(72.5) |
| 踝周组 | 52(14.6) | 131(36.8) | 133(37.4) | 40(11.2) | 233(65.4) | 123(34.6) | 154(43.3) | 202(56.7) |
| χ 2 | 64.388 | 51.085 | 5.919 | |||||
| P | <0.01 | <0.01 | 0.015 | |||||
前足组皮瓣旋转点低于踝周组皮瓣(P<0.05);前足组皮瓣筋膜蒂长、筋膜蒂宽、瓣部长、瓣部宽、皮瓣总长及长宽比均长于或大于踝周组皮瓣(均P<0.05,表2)。
表2.
两组皮瓣计量资料的比较( ±s)
Table 2 Comparison of continuous variables of flaps between the 2 groups ( ±s)
| 组别 | n | 筋膜蒂/cm | 瓣部/cm | 旋转点/cm | 皮瓣总长/cm | 长宽比 | ||
|---|---|---|---|---|---|---|---|---|
| 长 | 宽 | 长 | 宽 | |||||
| 前足组 | 69 | 9.93±3.77 | 4.30±0.58 | 13.03±3.41 | 8.84±1.71 | 6.90±1.50 | 22.98±4.09 | 5.39±0.91 |
| 踝周组 | 356 | 7.64±2.44 | 4.06±0.45 | 10.87±3.36 | 8.22±2.52 | 7.72±2.09 | 18.52±3.75 | 4.57±0.84 |
| t | -4.861 | -3.248 | -4.875 | -2.539 | 3.864 | -8.908 | -7.309 | |
| P | <0.001 | 0.002 | <0.001 | 0.012 | <0.001 | <0.001 | <0.001 | |
3. 讨 论
本研究采用顺逆结合法切取腓肠神经营养血管皮瓣,皮瓣远端筋膜蒂基底部均包含腓动脉穿支;该皮瓣具有双重的动脉供血和静脉回流,其中穿支血管起主要作用,筋膜蒂起次要作用[11]。
皮肤穿支血管间的连接有choke吻合和真性吻合两种方式,人体体被组织穿支血管间多数通过choke吻合方式连接。当穿支间连接为choke吻合时,一个穿支可以向任意方向上的一个相邻穿支血管供血,皮瓣坏死常发生在第2个choke连接区附近;当穿支间的连接为真性吻合时,皮瓣成活长度增加,相当于该皮瓣已行延迟术[12-13]。
作者前期的解剖学研究[14]观察到:腓肠神经营养动脉链从踝间线至腘窝横纹是通过真性吻合连接的,腓动脉远端2~3个穿支间通过纵向分支真性吻合连接,这些穿支通过横向或斜向的分支与腓肠神经营养动脉链真性吻合连接。这些真性吻合的解剖学特点是远端蒂腓肠神经营养血管皮瓣血供可靠,成活较长,可跨6~7个穿支体区存活[14]。
研究[2, 8, 15]报道腓肠神经营养血管皮瓣的部分坏死率为3.8%~36.0%。本研究前足组69例的皮瓣成活率为85.5%,10例(14.5%)皮瓣发生部分坏死,经植皮或二期缝合简单处理后9例皮瓣残留创面被成功覆盖。前足组单独应用腓肠神经营养血管皮瓣或联合简单二期处理(植皮或二期缝合)覆盖创面的成功率为98.6%(68/69),与踝周组的成功率(97.8%,348/356)差异无统计学意义,提示腓肠神经营养血管皮瓣修复跖骨中点连线以远的前足创面是可行的,且临床疗效较好。
修复前足创面有很多方法,如交腿皮瓣[16]、局部筋膜皮瓣[17]、游离皮瓣(包括游离穿支皮瓣)[18-20]、小腿带蒂皮瓣(如胫后动脉穿支筋膜蒂皮瓣[7, 21]、外踝上皮瓣[22]),每种方法各有其优点、缺点及适应证。前足创面也可采用蒂部包含外踝后动脉或跟外侧动脉穿支的低旋转点腓肠神经营养血管皮瓣修复[23]。本研究前足组皮瓣旋转点低于踝周组皮瓣,但所有皮瓣不包括上述低旋转点皮瓣。前足组皮瓣多数以位于外踝尖上方5.0~7.0 cm的腓动脉最远端穿支处为旋转点。4例旋转点位于外踝尖上方3.5~4.5 cm的患者均为2~5岁儿童,这些皮瓣基底部的穿支均为腓动脉最远端穿支。
腓肠神经营养血管皮瓣具有操作简单、无需吻合血管、不损伤小腿主干血管、血运丰富、成活较长、修复范围较广、可修复中到大面积的皮肤软组织缺损及皮瓣厚薄适中等优点,但该皮瓣用于修复肥胖人群的创面时,皮瓣可能相对较臃肿。
综合上述腓肠神经营养血管皮瓣修复前足创面的疗效、解剖学特点和临床优点,作者认为腓肠神经营养血管皮瓣是修复前足皮肤软组织缺损的一种较理想的方法。
虽然前足组与踝周组单独应用腓肠神经营养血管皮瓣或联合简单二期处理覆盖创面的成功率差异无统计学意义,但结果显示前足组的皮瓣部分坏死率为14.5%,高于踝周组的皮瓣部分坏死率(7.0%),提示在腓肠神经营养血管皮瓣的成活可靠性方面,该皮瓣修复跖骨中点连线以近创面优于修复跖骨中点连线以远的前足创面。
本研究前足组的筋膜蒂长、瓣部长及皮瓣总长均长于踝周组,前足组的皮瓣近端位置位于第8~第9区段或第9区段、长宽比≥5꞉1和瓣部宽≥8 cm的构成比均大于踝周组。前足组有较高的皮瓣部分坏死率,这可能主要与该组这些负面的皮瓣因素[8]有关。
为提高前足组皮瓣成活率,皮瓣筋膜蒂宜稍宽,皮条宽度也应相应增加;本研究前足组筋膜蒂宽度大于踝周组。腓动脉最远端穿支通常较外踝后动脉及跟外侧动脉穿支粗大,故尽量选择腓动脉最远端穿支处为皮瓣的旋转点设计、切取皮瓣。设计皮瓣前,以斯氏针将踝关节固定于背屈位,可缩短旋转点至创面近端的距离,有利于缩短皮瓣筋膜蒂长度和皮瓣总长,从而降低皮瓣远端发生部分坏死的可能性。
由于本研究是回顾性临床研究,不能做到随机、双盲、对照。虽然本研究的病例数相对较多,但前足组与踝周组的样本量相差较大,这种非对称性样本可能使研究结果出现偏差。
综上所述,腓肠神经营养血管皮瓣天然存在的真性吻合连接的解剖学特性使该皮瓣具有血运可靠、存活较长的特点。腓肠神经营养血管皮瓣是修复跖骨中点连线以远的前足皮肤软组织缺损可行且较理想的方法,该皮瓣修复跖骨中点连线以近创面的成活可靠性优于修复跖骨中点连线以远的前足创面。
基金资助
国家自然科学基金(81672188)。
This work was supported by the National Natural Science Foundation of China (81672188).
利益冲突声明
作者声称无任何利益冲突。
作者贡献
刘立宏 论文构想和撰写;陶世斌 数据采集、病例收集、统计分析;董忠根 手术操作、研究指导;魏建伟 手术操作、研究指导、论文修改;罗兆彪 统计分析;戴宇 文章构思、论文修改。
原文网址
http://xbyxb.csu.edu.cn/xbwk/fileup/PDF/20220179.pdf
参考文献
- 1. Perumal R, Bhowmick K, Reka K, et al. Comparison of reverse sural artery flap healing for traumatic injuries above and below the ankle joint[J]. J Foot Ankle Surg, 2019, 58(2): 306-311. 10.1053/j.jfas.2018.08.057. [DOI] [PubMed] [Google Scholar]
- 2. Daar DA, Abdou SA, David JA, et al. Revisiting the reverse sural artery flap in distal lower extremity reconstruction: A systematic review and risk analysis[J]. Ann Plast Surg, 2020, 84(4): 463-470. 10.1097/SAP.0000000000002041. [DOI] [PubMed] [Google Scholar]
- 3. Stevanovic GR, Dakovic-Bjelakovic MZ, Paravina JM, et al. Reliability and versatility of reverse sural island neurofasciocutaneous leg flaps[J]. Ann Plast Surg, 2020, 85(6): 656-660. 10.1097/SAP.0000000000002350. [DOI] [PubMed] [Google Scholar]
- 4. Chang SM, Li XH, Gu YD. Distally based perforator sural flaps for foot and ankle reconstruction[J]. World J Orthop, 2015, 6(3): 322-330. 10.5312/wjo.v6.i3.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Zhu YL, Wang Y, He XQ, et al. Foot and ankle reconstruction: an experience on the use of 14 different flaps in 226 cases[J]. Microsurgery, 2013, 33(8): 600-604. 10.1002/micr.22177. [DOI] [PubMed] [Google Scholar]
- 6. Lee HI, Ha SH, Yu SO, et al. Reverse sural artery island flap with skin extension along the pedicle[J]. J Foot Ankle Surg, 2016, 55(3): 470-475. 10.1053/j.jfas.2015.07.014. [DOI] [PubMed] [Google Scholar]
- 7. Luo Z, Lv G, Wei J, et al. Comparison between distally based peroneal and posterior tibial artery perforator-plus fasciocutaneous flap for reconstruction of the lower extremity[J]. Burns, 2020, 46(1): 225-233. 10.1016/j.burns.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 8. Wei JW, Dong ZG, Ni JD, et al. Influence of flap factors on partial necrosis of reverse sural artery flap: a study of 179 consecutive flaps[J]. J Trauma Acute Care Surg, 2012, 72(3): 744-750. 10.1097/TA.0b013e31822a2f2b. [DOI] [PubMed] [Google Scholar]
- 9. Dong ZG, Wei JW, Ni JD, et al. Anterograde-retrograde method for harvest of distally based sural fasciocutaneous flap: report of results from 154 patients[J]. Microsurgery, 2012, 32(8): 611-616. 10.1002/micr.22049. [DOI] [PubMed] [Google Scholar]
- 10. Wei JW, Ni JD, Dong ZG, et al. A modified technique to improve reliability of distally based sural fasciocutaneous flap for reconstruction of soft tissue defects longitudinal in distal pretibial region or transverse in heel and ankle[J]. J Foot Ankle Surg, 2016, 55(4): 753-758. 10.1053/j.jfas.2016.02.011. [DOI] [PubMed] [Google Scholar]
- 11. Mehrotra S. Perforator-plus flaps: a new concept in traditional flap design[J]. Plast Reconstr Surg, 2007, 119(2): 590-598. 10.1097/01.prs.0000239570.18647.83. [DOI] [PubMed] [Google Scholar]
- 12. Taylor GI, Corlett RJ, Dhar SC, et al. The anatomical (angiosome) and clinical territories of cutaneous perforating arteries: development of the concept and designing safe flaps[J]. Plast Reconstr Surg, 2011, 127(4): 1447-1459. 10.1097/PRS.0b013e318208d21b. [DOI] [PubMed] [Google Scholar]
- 13. Taylor GI, Chubb DP, Ashton MW. True and 'choke' anastomoses between perforator angiosomes: part i. anatomical location[J]. Plast Reconstr Surg, 2013, 132(6): 1447-1456. 10.1097/PRS.0b013e3182a80638. [DOI] [PubMed] [Google Scholar]
- 14. 陶世斌, 董忠根, 魏建伟, 等. 腓肠神经营养血管皮瓣的真性吻合连接及修复前足创面的疗效[J]. 中国临床解剖学杂志, 2020, 38(4): 450-454. 10.13418/j.issn.1001-165x.2020.04.016. [DOI] [Google Scholar]; TAO Shibin, DONG Zhonggen, WEI Jianwei, et al. True anastomosis connections of sural neuro-vascular flap and outcomes of the flap for reconstructing soft tissue defect in forefoot[J]. Chinese Journal of Clinical Anatomy, 2020, 38(4): 450-454. 10.13418/j.issn.1001-165x.2020.04.016. [DOI] [Google Scholar]
- 15. Wei JW, Ni JD, Dong ZG, et al. Distally based perforator-plus sural fasciocutaneous flap for soft-tissue reconstruction of the distal lower leg, ankle, and foot: comparison between pediatric and adult patients[J]. J Reconstr Microsurg, 2014, 30(4): 249-254. 10.1055/s-0033-1357274. [DOI] [PubMed] [Google Scholar]
- 16. Liang W, Tan BK. Use of the cross-leg distally based sural artery flap for the reconstruction of complex lower extremity defects[J]. Arch Plast Surg, 2019, 46(3): 255-261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. 张景僚, 蔡俊雅, 张海瑞, 等. 足背内侧皮神经营养血管皮瓣逆行修复前足软组织缺损[J]. 中华创伤杂志, 2016, 32(4): 310-312. 10.3760/cma.j.issn.1001-8050.2016.04.007. [DOI] [Google Scholar]; ZHANG Jingliao, CAI Junya, ZHANG Hairui, et al. Reversed cutaneous neurovascular flap of medial dorsalis pedis for reconstruction of the defect in the forefoot[J]. Chinese Journal of Truama, 2016, 32(4): 310-312. 10.3760/cma.j.issn.1001-8050.2016.04.007. [DOI] [Google Scholar]
- 18. Fitzgerald O'Connor E, Ruston J, Loh CYY, et al. Technical refinements of the free medial sural artery perforator (MSAP) flap in reconstruction of multifaceted ankle soft tissue defects[J]. Foot Ankle Surg, 2020, 26(2): 233-238. 10.1016/j.fas.2019.02.003. [DOI] [PubMed] [Google Scholar]
- 19. Noaman HH, Soroor YO. Foot salvage using microsurgical free muscle flaps in severely crushed foot with soft tissue defects [J]. Injury, 2019, 50 (Suppl 5): S17-S20. 10.1016/j.injury.2019.10.040. [DOI] [PubMed] [Google Scholar]
- 20. Jiga LP, Jandali Z, Merwart B, et al. The free vastus lateralis muscle flap. A smart less used flap for soft tissue reconstruction of the weight-bearing foot[J]. Injury, 2020, 51 (Suppl 4): S34-S40. 10.1016/j.injury.2020.03.019. [DOI] [PubMed] [Google Scholar]
- 21. 许良, 王楠, 王利祥. 胫后动脉穿支联合隐神经营养血管筋膜蒂皮瓣修复足底内侧创面[J]. 中华显微外科杂志, 2020, 43(1): 10-14. 10.3760/cma.j.issn.1001-2036.2020.01.004. [DOI] [Google Scholar]; XU Liang, WANG Nan, WANG Lixiang. Distally based posterior tibial artery perforator-plus saphenous nerve fasciocutaneous Flap for reconstruction of defect in the medial plantar[J]. Chinese Journal of Microsurgery, 2020, 43(1): 10-14. 10.3760/cma.j.issn.1001-2036.2020.01.004. [DOI] [Google Scholar]
- 22. 李俊明, 李艳华, 黄贺军, 等. 优化的外踝上皮瓣修复足踝部皮肤软组织缺损[J]. 中华整形外科杂志, 2021, 37(2): 171-177. 10.3760/cma.j.cn114453-20200207-00030. [DOI] [Google Scholar]; LI Junming, LI Yanhua, HUANG Hejun, et al. The lateral supramalleolar perforator pedicle flap was optimized to repair the soft tissue defect offoot and ankle[J]. Chinese Journal of Plastic Surgery, 2021, 37(2): 171-177. 10.3760/cma.j.cn114453-20200207-00030. [DOI] [Google Scholar]
- 23. 张发惠, 宋一平, 林松庆, 等. 腓肠神经营养血管远端蒂皮瓣修复足前部软组织缺损[J]. 中华解剖与临床杂志, 2014, 19(01): 46-48. 10.3760/cma.j.issn.2095-7041.2014.01.012. [DOI] [Google Scholar]; ZHANG Fahui, SONG Yiping, LIN Songqing, et al .The distally based sural neurouascular flap for reconstruction of the forefoot soft tissue defect[J]. Chinese Journal of Anatomy and Clinics, 2014, 19(01): 46-48. 10.3760/cma.j.issn.2095-7041.2014.01.012. [DOI] [Google Scholar]