

Abstract
Background
Gastrointestinal stromal tumor (GIST) is a common mesenchymal tumor of the gastrointestinal system. They originate from the interstitial cells of Cajal located within the muscle layer and are characterized by over-expression of the tyrosine kinase receptor KIT.
Methods
Data from the Surveillance Epidemiology, and End Results (SEER) database of 1,213 patients diagnosed with GIST between 2010 and 2019 were dichotomized into a modeling set and a validation set at a 2:1 ratio. For the modeling set, both univariate and multivariate Cox regression analyses were used to identify independent prognostic factors. A nomogram was then constructed based on these determinants. Model efficacy was tested using receiver operating characteristic (ROC) curves, calibration curves, clinical decision curves, and risk stratification analysis in both subsets.
Results
Identified prognostic determinants included age, sex, pathological differentiation level, tumor-node-metastasis (TNM) stage, surgical intervention, radiotherapy, and marital status. The constructed nomogram showed area under the ROC curve (AUC) values of 0.822, 0.793, and 0.779 for 1-, 3-, and 5-year overall survival (OS) in the modeling set, respectively, while in the validation set, the values were 0.796, 0.823, and 0.806, respectively. Calibration plots from both sets confirmed the concordance between predicted and observed survival. Decision curve analysis (DCA) indicated significant clinical utility for the nomogram. Risk stratification of the patient data revealed distinct survival differences between high-risk and low-risk cohorts in both sets (P<0.001).
Conclusions
A novel and potent nomogram for the prognosis of GIST has been introduced. This model’s precision offers crucial insights for clinical decisions, yet further external validation remains essential.
Keywords: Gastrointestinal stromal tumor (GIST); nomogram; prognostic; Surveillance Epidemiology, and End Results database (SEER database)
Highlight box.
Key findings
• The nomogram for the prognosis of gastrointestinal stromal tumor (GIST) has been introduced.
What is known and what is new?
• GISTs are rare tumors of the digestive system, which have poor prognosis. At present, there is no standard to evaluate the prognosis of patients with GIST. tumor-node-metastasis stage is a well-known prognostic factor.
• We found new prognostic factors, such as age, sex, pathological differentiation level, surgical intervention, radiotherapy, and marital status.
What is the implication, and what should change now?
• Leveraging this nomogram offers clinicians a reliable tool, enhancing the precision of their judgments. Nevertheless, performing broader external validations remains a crucial next step.
Introduction
Gastrointestinal stromal tumors (GISTs) are rare tumors of the digestive system and include gastrointestinal stromal sarcoma (GISS) (1). Stemming from pluripotent mesenchymal cells, GISTs can evolve into the interstitial cells of Cajal (ICCs), pivotal pacemaker entities nestled between the circular and longitudinal muscular layers of the gastrointestinal tract’s muscular propria (2). For patients with non-metastatic GISTs, laparoscopic surgical removal remains the primary therapeutic approach (3). In advanced GIST cases, clinicians typically resort to tyrosine kinase inhibitors (TKIs), such as imatinib, sunitinib, and regorafenib. These pharmaceutical agents demonstrate efficacy against certain GIST subtypes, yet their challenges persist, necessitating innovative therapeutic strategies (4). The recurrence rate remains high for GIST due to its rarity, even after intensive treatment (5). The literature regarding this malignancy primarily encompasses case studies and limited-scope retrospective analyses. Typically, prognostic assessments for GIST rely heavily on clinical expertise. Hence, the creation of a visual nomogram for survival prediction can offer clinicians an enhanced tool for individual prognosis assessments. We present this article in accordance with the TRIPOD reporting checklist (available at https://jgo.amegroups.com/article/view/10.21037/jgo-24-27/rc).
Methods
Data source
In this investigation, we utilized a retrospective approach with data sourced from the Surveillance Epidemiology, and End Results (SEER) database. Utilizing SEER*Stat software, information based on histological and pathological assessments from 2010–2019 was extracted. The dataset incorporated factors such as age, sex, primary location of the tumor, pathological grading, and staging (T, N, M, and overall), along with treatment methods, tumor dimensions, marital status, and ethnicity. Eligibility for inclusion encompassed (I) diagnoses between 2010 and 2019; (II) tumors primarily situated in the stomach; (III) confirmation of GIST via ICD-O-3 pathology; and (IV) availability of comprehensive follow-up details. On the other hand, exclusion criteria included (I) the presence of multiple primary tumors; (II) incomplete or unverified histological/pathological data; (III) ambiguous surgical details; (IV) lack of clarity regarding tumor categorization, differentiation level, and staging; (V) uncertain survival duration; and (VI) mortality linked to other malignancies or undetermined origins. After screening, we identified a cohort of 1,213 patients. These individuals were subsequently distributed into modeling and validation cohorts at a 2:1 ratio, resulting in 809 participants in the modeling subset, with the residual 404 assigned to the validation subset. Within the scope of inclusion criteria, we randomly selected a part of people as the validation cohort and the training. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Statistical analysis
Dataset fundamentals were articulated as percentages. Chi-square tests were used to compare rates, with significance acknowledged when P<0.05. Lasso regression was applied for formative steps on the modeling group’s data. This allowed for the identification of substantial prognostic elements, which then entered the multifaceted analysis via the Cox proportional hazard regression model, presenting their respective hazard ratios (HRs) and 95% confidence intervals (95% CIs). Survival rates at distinct intervals—1, 3, and 5 years—were illustrated graphically. The discriminatory ability of the model was gauged through the area under the receiver operating characteristic (ROC) curve (AUC). Calibration curves were used to further this analysis by juxtaposing predictions against tangible outcomes. Concurrently, a clinical decision curve analysis (DCA) illuminated the clinical utility of the nomogram. Based on inherent prognostic components, risk stratifications for GIST patients emerged. Employing R language, we generated survival state scatter plots. The Kaplan-Meier approach was applied to distinguish disparities between risk tiers, high and low. R language software, version 4.1.3, was used to craft all relevant visualizations and tables.
Results
Patient baseline characteristics
In our investigation, we sourced eligible patients diagnosed with GIST from 2010 to 2019 using the SEER database. The distribution between the modeling and validation groups was set at a 2:1 ratio as detailed in Table 1. A comparative analysis between these two groups revealed no significant variances in their clinical characteristics (P>0.05), ensuring the robustness and reliability of our model.
Table 1. Clinical characteristics of gastrointestinal stromal tumor patients.
| Characteristic | Training cohort (n=809) | Validation cohort (n=404) | P |
|---|---|---|---|
| Age (years) | 0.531 | ||
| <60 | 252 (20.8) | 118 (9.7) | |
| ≥60 | 557 (45.9) | 286 (23.6) | |
| Sex | 0.902 | ||
| Female | 387 (31.9) | 191 (15.7) | |
| Male | 422 (34.8) | 213 (17.6) | |
| Primary site | 0.033 | ||
| Body | 86 (7.1) | 30 (2.5) | |
| Cardia | 65 (5.4) | 31 (2.6) | |
| Fundus | 132 (10.9) | 79 (6.5) | |
| Greater curvature | 100 (8.2) | 60 (4.9) | |
| Lesser curvature | 84 (6.9) | 59 (4.9) | |
| Overlapping lesion | 34 (2.8) | 22 (1.8) | |
| Pylorus | 61 (5.0) | 25 (2.1) | |
| Stomach | 247 (20.4) | 98 (8.1) | |
| Grade | 0.171 | ||
| I | 174 (14.3) | 69 (5.7) | |
| II | 83 (6.8) | 45 (3.7) | |
| III | 20 (1.6) | 18 (1.5) | |
| IV | 38 (3.1) | 18 (1.5) | |
| Unknown | 494 (40.7) | 254 (20.9) | |
| T | 0.053 | ||
| T1 | 134 (11.0) | 54 (4.5) | |
| T2 | 244 (20.1) | 136 (11.2) | |
| T3 | 204 (16.8) | 85 (7.0) | |
| T4 | 143 (11.8) | 93 (7.7) | |
| TX | 84 (6.9) | 36 (3.0) | |
| N | 0.208 | ||
| N0 | 776 (64.0) | 394 (32.5) | |
| N1 | 33 (2.7) | 10 (0.8) | |
| M | 0.983 | ||
| M0 | 695 (57.3) | 348 (28.7) | |
| M1 | 114 (9.4) | 56 (4.6) | |
| Stage | 0.173 | ||
| I | 354 (29.2) | 165 (13.6) | |
| II | 79 (6.5) | 57 (4.7) | |
| III | 55 (4.5) | 33 (2.7) | |
| IV | 131 (10.8) | 59 (4.9) | |
| Unknown | 190 (15.7) | 90 (7.4) | |
| Surgery | 0.637 | ||
| No | 196 (16.2) | 108 (8.9) | |
| Local surgery | 80 (6.6) | 39 (3.2) | |
| Gastrectomy | 533 (43.9) | 257 (21.2) | |
| Radiation | >0.99 | ||
| None/unknown | 806 (66.4) | 402 (33.1) | |
| Yes | 3 (0.2) | 2 (0.2) | |
| Chemotherapy | 0.899 | ||
| No/unknown | 464 (38.3) | 234 (19.3) | |
| Yes | 345 (28.4) | 170 (14.0) | |
| Systemic treatment | 0.673 | ||
| No | 578 (47.7) | 291 (24.0) | |
| Before surgery | 44 (3.6) | 28 (2.3) | |
| After surgery | 147 (12.1) | 67 (5.5) | |
| Both before and after surgery | 40 (3.3) | 18 (1.5) | |
| Months from diagnosis to treatment | 0.414 | ||
| <1 | 382 (31.5) | 179 (14.8) | |
| ≥1 | 345 (28.4) | 175 (14.4) | |
| Unknown | 82 (6.8) | 50 (4.1) | |
| Tumor size (cm) | 0.275 | ||
| <5 | 125 (10.3) | 64 (5.3) | |
| ≥5 | 150 (12.4) | 60 (4.9) | |
| Unknown | 534 (44.0) | 280 (23.1) | |
| Marital status | 0.644 | ||
| Married | 450 (37.1) | 214 (17.6) | |
| Single | 7 (0.6) | 6 (0.5) | |
| Divorced/widowed/separated | 310 (25.6) | 163 (13.4) | |
| Unknown | 42 (3.5) | 21 (1.7) | |
| Race recode | 0.699 | ||
| White | 484 (39.9) | 229 (18.9) | |
| Black | 166 (13.7) | 93 (7.7) | |
| Other | 154 (12.7) | 80 (6.6) | |
| Unknown | 5 (0.4) | 2 (0.2) |
Univariate and multivariate Cox regression analyses
Single-factor analysis indicated that variables such as age, pathological differentiation, stages T, N, M, and tumor-node-metastasis (TNM) as well as surgical intervention radiation treatment, systemic treatments, post-diagnosis therapy duration, and marital status played a pivotal role in influencing the overall survival (OS) of patients. From an examination of both single-factor and multifactor analysis for the modeling group, it became evident that age, gender, pathological grading, TNM staging, surgical procedures, radiation exposure, and marital status stood out as autonomous determinants of an unfavorable prognosis for those diagnosed with GIST. This is elaborated upon in Table 2.
Table 2. Univariate and multivariate analyses for prognosis of gastrointestinal stromal tumor patients in the modeling group.
| Characteristics | Total | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| Hazard ratio (95% CI) | P value | Hazard ratio (95% CI) | P value | |||
| Age (years) | <0.001 | <0.001 | ||||
| <60 | 252 | Reference | ||||
| ≥60 | 557 | 2.111 (1.502–2.968) | <0.001 | 2.414 (1.678–3.472) | <0.001 | |
| Sex | 0.046 | 0.029 | ||||
| Female | 387 | Reference | ||||
| Male | 422 | 1.267 (1.059–1.673) | 0.046 | 1.413 (1.039–1.921) | 0.028 | |
| Primary site | 0.097 | 0.475 | ||||
| Fundus | 132 | Reference | ||||
| Body | 86 | 0.864 (0.513–1.453) | 0.580 | 1.256 (0.731–2.158) | 0.408 | |
| Lesser curvature | 84 | 0.849 (0.513–1.404) | 0.524 | 1.043 (0.610–1.784) | 0.878 | |
| Stomach | 247 | 1.372 (0.956–1.969) | 0.086 | 1.239 (0.843–1.822) | 0.276 | |
| Cardia | 68 | 1.090 (0.628–1.892) | 0.760 | 0.773 (0.430–1.387) | 0.387 | |
| Overlapping lesion | 34 | 1.260 (0.873–1.485) | 0.760 | 0.837 (0.574–1.175) | 0.387 | |
| Greater curvature | 100 | 1.294 (0.673–2.488) | 0.440 | 1.214 (0.614–2.400) | 0.577 | |
| Pylorus | 61 | 0.599 (0.294–1.221) | 0.159 | 0.684 (0.329–1.420) | 0.308 | |
| Grade | 0.037 | 0.044 | ||||
| I | 174 | Reference | ||||
| II | 83 | 1.277 (0.719–2.270) | 0.404 | 1.437 (0.788–2.622) | 0.237 | |
| III | 20 | 1.880 (0.782–4.518) | 0.158 | 2.167 (0.855–5.494) | 0.103 | |
| IV | 38 | 2.281 (1.227–4.242) | 0.009 | 1.660 (0.787–3.504) | 0.183 | |
| Unknown | 494 | 1.673 (1.125–2.488) | 0.011 | 0.832 (0.521–1.330) | 0.443 | |
| T | <0.001 | 0.305 | ||||
| T1 | 134 | Reference | ||||
| T2 | 244 | 0.941 (0.580–1.526) | 0.806 | 0.925 (0.558–1.534) | 0.764 | |
| T3 | 204 | 1.139 (0.763–1.699) | 0.524 | 1.124 (0.727–1.738) | 0.599 | |
| T4 | 143 | 1.558 (1.024–2.371) | 0.038 | 1.700 (0.987–2.928) | 0.056 | |
| TX | 84 | 3.253 (2.143–4.936) | <0.001 | 1.339 (0.790–2.268) | 0.278 | |
| N | 0.013 | 0.232 | ||||
| N0 | 776 | Reference | ||||
| N1 | 33 | 1.970 (1.144–3.392) | 0.014 | 0.598 (0.260–1.375) | 0.226 | |
| M | <0.001 | 0.370 | ||||
| M0 | 695 | Reference | ||||
| M1 | 114 | 2.692 (1.967–3.686) | <0.001 | 0.599 (0.199–1.797) | 0.360 | |
| Stage | <0.001 | 0.040 | ||||
| I | 354 | Reference | ||||
| II | 79 | 0.499 (0.239–1.039) | 0.063 | 0.458 (0.201–1.041) | 0.062 | |
| III | 55 | 1.765 (1.021–3.051) | 0.042 | 1.345 (0.660–2.738) | 0.414 | |
| IV | 131 | 3.328 (2.342–4.730) | <0.001 | 2.896 (0.892–9.396) | 0.077 | |
| Unknown | 190 | 2.081 (1.446–2.995) | <0.001 | 1.080 (0.673–1.734) | 0.749 | |
| Surgery | <0.001 | 0.031 | ||||
| No | 196 | Reference | ||||
| Local surgery | 80 | 0.343 (0.215–0.549) | <0.001 | 0.632 (0.221–1.803) | 0.391 | |
| Gastrectomy | 533 | 0.231 (0.172–0.310) | <0.001 | 0.407 (0.154–1.077) | 0.070 | |
| Radiation | 0.002 | 0.008 | ||||
| None/unknown | 806 | Reference | ||||
| Yes | 3 | 6.988 (1.721–28.382) | 0.007 | 8.783 (1.796–42.940) | 0.007 | |
| Chemotherapy | 0.069 | 0.487 | ||||
| No/unknown | 464 | Reference | ||||
| Yes | 345 | 1.292 (0.980–1.704) | 0.069 | 1.410 (0.542–3.666) | 0.481 | |
| Systemic treatment | 0.025 | 0.349 | ||||
| No | 578 | Reference | ||||
| Before surgery | 44 | 0.986 (0.520–1.870) | 0.966 | 1.014 (0.308–3.335) | 0.982 | |
| After surgery | 147 | 0.557 (0.373–0.833) | 0.004 | 0.554 (0.209–1.467) | 0.235 | |
| Both before and after surgery | 40 | 0.614 (0.272–1.389) | 0.242 | 0.693 (0.192–2.506) | 0.576 | |
| Months from diagnosis to treatment | <0.001 | 0.248 | ||||
| <1 | 345 | Reference | ||||
| ≥1 | 82 | 2.949 (1.999–4.352) | <0.001 | 2.024 (0.795–5.152) | 0.139 | |
| Unknown | 382 | 0.877 (0.645–1.192) | 0.402 | 1.197 (0.849–1.688) | 0.306 | |
| Tumor size (cm) | 0.540 | 0.637 | ||||
| <5 | 125 | Reference | ||||
| ≥5 | 150 | 1.388 (0.674–2.859) | 0.374 | 0.889 (0.413–1.917) | 0.764 | |
| Unknown | 534 | 1.401 (0.768–2.556) | 0.272 | 1.137 (0.607–2.129) | 0.688 | |
| Marital status | 0.004 | 0.007 | ||||
| Married | 450 | Reference | ||||
| Single | 7 | 0.739 (0.103–5.301) | 0.763 | 1.156 (0.156–8.544) | 0.887 | |
| Divorced/widowed/separated | 310 | 1.670 (1.257–2.219) | <0.001 | 1.765 (1.281–2.431) | <0.001 | |
| Unknown | 42 | 1.399 (0.728–2.687) | 0.313 | 1.166 (0.581–2.338) | 0.666 | |
| Race | 0.081 | 0.508 | ||||
| White | 484 | Reference | ||||
| Black | 166 | 1.405 (1.010–1.957) | 0.044 | 1.313 (0.926–1.862) | 0.127 | |
| Other | 154 | 0.887 (0.605–1.298) | 0.536 | 1.085 (0.728–1.617) | 0.687 | |
| Unknown | 5 | 0.000 (0.000–Inf) | 0.993 | 0.000 (0.000–Inf) | 0.993 | |
CI, confidence interval.
Construction and validation of the prognostic nomogram
Based on the significance of various parameters from the multifactorial assessment, we allocated distinct scores to each. By summing these scores, we generated a comprehensive prognosis evaluation for patients. In our modeling cohort, the multivariate investigation identified age, sex, pathological grade, TNM classification, surgical intervention, radiation therapy, and marital status as pivotal factors determining the outcome in GIST cases. Using the aforementioned seven criteria, we devised a nomogram to project survival outcomes, particularly focusing on the 1-, 3-, and 5-year OS probabilities; details can be observed in Figure 1. For the ROC analysis, the AUC metrics for the 1-, 3-, and 5-year survival probabilities in the modeling cohort were 0.822, 0.793, and 0.779, respectively, while those for the validation cohort were respectively 0.796, 0.823, and 0.806, suggesting robust model precision (refer to Figure 2). Furthermore, a calibration curve was formulated to reaffirm the predictive efficiency of our model. In this curve, the X-axis illustrates the survival probabilities as per the nomogram, while the Y-axis shows the actual patient outcomes. The congruence between the dotted and solid trajectories within the diagram denotes the nomogram’s precision. Intriguingly, the calibration curve’s observed versus projected values for the 1-, 3-, and 5-year survival probabilities in both the modeling and validation cohorts were notably aligned (see Figure 3). Additionally, our clinical DCA reaffirmed the efficacy of our model in both groups, indicating its potential clinical utility and patient benefit (displayed in Figure 4).
Figure 1.
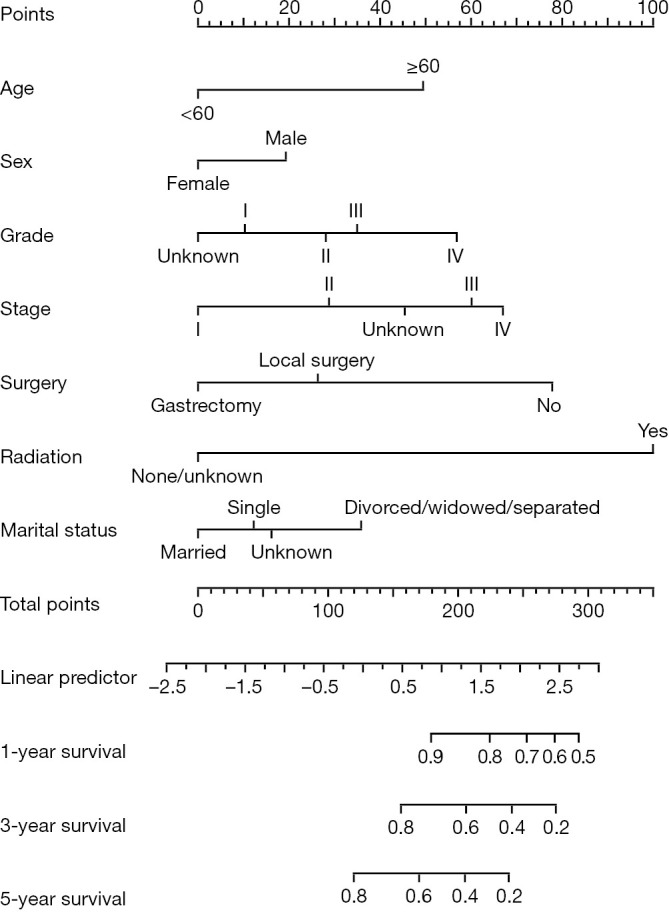
Nomogram chart forecasting 1-, 3-, and 5-year OS outcomes in gastrointestinal stromal tumor patients. OS, overall survival.
Figure 2.

ROC curves evaluating the nomogram’s precision for 1-, 3-, and 5-year projections. (A,C,E) The modeling cohort; (B,D,F) the validation cohort. TPR, true positive rate; FPR, false positive rate; AUC, area under the receiver operating characteristic curve; CI, confidence interval; ROC, receiver operating characteristic.
Figure 3.

Calibration plots for the nomogram’s 1-, 3-, and 5-year OS predictions. The x-axis represents the predicted OS, while the y-axis indicates the observed OS. (A,C,E) The modeling cohort; (B,D,F) the validation cohort. OS, overall survival.
Figure 4.

Decision curve analyses illustrating the net benefits of the nomogram’s 1-, 3-, and 5-year OS predictions. (A,C,E) The modeling group; (B,D,F) the validation set. OS, overall survival.
Risk stratification analysis
Utilizing the predictive indicators present in the nomogram, we categorized the individuals from both the modeling and validation cohorts into high-risk and low-risk segments. With R language, we graphically represented the survival patterns of these subgroups (refer to Figure 5). Evidently, the scatterplot elucidated a higher mortality rate among high-risk participants than among their low-risk counterparts. A subsequent Kaplan-Meier survival evaluation revealed that the low-risk segment demonstrated a substantially elevated survival trajectory in both cohorts relative to the high-risk segment. The marked discrepancy in the OS trajectories between these risk divisions was underpinned by a significant difference (P<0.001), reinforcing the adept predictive caliber of our constructed nomogram (see Figure 6).
Figure 5.

Diagrams presenting risk factors for both cohorts. (A) The modeling group; (B) the validation group. 0 means alive, 1 means dead.
Figure 6.

Depiction of survival curves for both groups. (A) The modeling cohort; (B) the validation group. HR, hazard ratio.
Discussion
Over the decade from 2010 to 2019, our investigation encompassed 1,213 cases diagnosed with GIST. This expansive dataset allowed for a robust assessment of the survival metrics, specifically at the 1-, 3-, and 5-year marks. From our evaluations, several variables emerged as key independent prognostic indicators: age, sex, pathological differentiation, TNM stage, surgical intervention, radiotherapy, and marital status.
The literature suggests that individuals around the age of 60 are predominantly diagnosed with this condition (6,7). Aligning with these findings, we utilized 60 years as a critical age threshold, deducing age’s profound impact on prognosis. In a unique revelation of this study, gender was identified as an influential prognostic factor, with females in China exhibiting a heightened predisposition toward soft tissue sarcomas (8). Furthermore, marital status’s role in cancer prognosis has been underscored in various retrospective evaluations (9,10). Our multivariate analysis echoes these sentiments, reinforcing marital status as a pivotal prognostic element, likely attributed to the emotional and psychological support offered through marital bonds. Beyrouti and colleagues elucidated the rarity of stomach sarcoma and the dependence of its prognosis on varied parameters (11). Consistent with prior research, this study accentuates the inverse relationship between the AJCC staging post-GIST resection and the 5-year disease-free survival (DFS) rate (12). The prognosis of GIST is significantly influenced by TNM stage. Surgical interventions remain paramount in managing GIST. Shannon et al. pinpointed augmented OS in older patients undergoing resection, albeit with notable mortality risks (13). Peiper et al. highlighted the favorable outcomes following an extensive initial resection (14). Meanwhile, a study by Gronchi et al. underscored the disparities in OS among patients with varied resection extents (15). Our data included some ambiguities regarding surgical methodologies. However, we broadly categorized surgical intervention as a binary factor, underscoring its profound positive influence on prognosis. Traditionally, GIST treatments seldom involve radiotherapy. However, scholars in certain studies propose its potential benefits (16,17). Zhang et al. conducted a comprehensive review, suggesting radiotherapy’s efficacy in selecting advanced GIST cases, albeit without discernible survival enhancements (18). Our research posits radiotherapy as an influential prognostic factor, albeit indicative of an adverse prognosis. Further prospective evaluations are warranted to delve deeper into this association.
Our investigations demonstrate that the nomogram model holds promise in accurately forecasting the survival outcomes of individuals with GIST, thereby enhancing the precision of clinical judgments. Nevertheless, the limitations of this study also need to be noted. First, the SEER database, a prominent clinical cancer repository in the U.S., predominantly represents Black and White populations, leaving the Asian demographic underrepresented. Second, inherent to its retrospective nature, this work may encompass unforeseen selection biases. Last, our validation was internally confined; expanded validation through alternate databases or prospective evaluations remains paramount. For those diagnosed with GIST, early surgical intervention combined with reinforced psychological support is pivotal. However, large-sample, multicenter retrospective and prospective studies are still needed to provide better guidance on whether postoperative adjuvant radiotherapy should be performed and what kind of surgery should be followed by adjuvant radiotherapy. The original data in SEER database did not contain these clinical characteristics (e.g., mitotic rate, depth of invasion), so statistics could not be made. The study does not show any effect of tumor size, which may be related to the insufficient number of cases and the lack of external validation, and further research is needed. Factors such as type of driver mutations, germline vs. sporadic, and variant mutations within specific exons, allow selecting the type of targeted therapy that would benefit the most patients with advanced disease or patients at increased risk for recurrence. The proposed nomogram ignores the most important advances in the prognostication and therapy of GISTs. This is a limitation of this study, and further research is needed.
Conclusions
Our research is pioneering in devising a survival prognosis tool for individuals diagnosed with GIST. Leveraging this nomogram offers clinicians a reliable tool, enhancing the precision of their judgments. Nevertheless, performing broader external validations remains a crucial next step.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: The work was supported by Cohort and Clinical Research Program of Wuxi Medical Center, Nanjing Medical University (No. WMCC202319) and Wuxi Health Commission scientific research (suitable technology promotion) (No. M202108).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Footnotes
Reporting Checklist: The authors have completed the TRIPOD reporting checklist. Available at https://jgo.amegroups.com/article/view/10.21037/jgo-24-27/rc
Peer Review File: Available at https://jgo.amegroups.com/article/view/10.21037/jgo-24-27/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-24-27/coif). The authors have no conflicts of interest to declare.
References
- 1.Ueyama T, Guo KJ, Hashimoto H, et al. A clinicopathologic and immunohistochemical study of gastrointestinal stromal tumors. Cancer 1992;69:947-55. [DOI] [PubMed] [Google Scholar]
- 2.Khan J, Ullah A, Waheed A, et al. Gastrointestinal Stromal Tumors (GIST): A Population-Based Study Using the SEER Database, including Management and Recent Advances in Targeted Therapy. Cancers (Basel) 2022;14:3689. 10.3390/cancers14153689 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mazer L, Worth P, Visser B. Minimally invasive options for gastrointestinal stromal tumors of the stomach. Surg Endosc 2021;35:1324-30. 10.1007/s00464-020-07510-x [DOI] [PubMed] [Google Scholar]
- 4.Klug LR, Khosroyani HM, Kent JD, et al. New treatment strategies for advanced-stage gastrointestinal stromal tumours. Nat Rev Clin Oncol 2022;19:328-41. 10.1038/s41571-022-00606-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Beham AW, Schaefer IM, Schüler P, et al. Gastrointestinal stromal tumors. Int J Colorectal Dis 2012;27:689-700. 10.1007/s00384-011-1353-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Piso P, Schlitt HJ, Klempnauer J. Stromal sarcoma of the stomach: therapeutic considerations. Eur J Surg 2000;166:954-8. 10.1080/110241500447128 [DOI] [PubMed] [Google Scholar]
- 7.Irving JA, Lerwill MF, Young RH. Gastrointestinal stromal tumors metastatic to the ovary: a report of five cases. Am J Surg Pathol 2005;29:920-6. 10.1097/01.pas.0000155161.55915.c3 [DOI] [PubMed] [Google Scholar]
- 8.Yang Z, Zheng R, Zhang S, et al. Incidence, distribution of histological subtypes and primary sites of soft tissue sarcoma in China. Cancer Biol Med 2019;16:565-74. 10.20892/j.issn.2095-3941.2019.0041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Krajc K, Miroševič Š, Sajovic J, et al. Marital status and survival in cancer patients: A systematic review and meta-analysis. Cancer Med 2023;12:1685-708. 10.1002/cam4.5003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhou R, Yan S, Li J. Influence of marital status on the survival of patients with gastric cancer. J Gastroenterol Hepatol 2016;31:768-75. 10.1111/jgh.13217 [DOI] [PubMed] [Google Scholar]
- 11.Beyrouti MI, Beyrouti R, Ben Amar M, et al. Gastric sarcoma. Presse Med 2008;37:e60-6. 10.1016/j.lpm.2007.05.004 [DOI] [PubMed] [Google Scholar]
- 12.Rutkowski P, Wozniak A, Dębiec-Rychter M, et al. Clinical utility of the new American Joint Committee on Cancer staging system for gastrointestinal stromal tumors: current overall survival after primary tumor resection. Cancer 2011;117:4916-24. 10.1002/cncr.26079 [DOI] [PubMed] [Google Scholar]
- 13.Shannon AB, Song Y, Fraker DL, et al. Surgical resection of gastric gastrointestinal stromal tumors (GIST) in octogenarians. Am J Surg 2022;223:325-30. 10.1016/j.amjsurg.2021.03.062 [DOI] [PubMed] [Google Scholar]
- 14.Peiper M, Schröder S, Zornig C. Stromal sarcoma of the stomach--a report of 20 surgically treated patients. Langenbecks Arch Surg 1998;383:442-6. 10.1007/s004230050157 [DOI] [PubMed] [Google Scholar]
- 15.Gronchi A, Bonvalot S, Poveda Velasco A, et al. Quality of Surgery and Outcome in Localized Gastrointestinal Stromal Tumors Treated Within an International Intergroup Randomized Clinical Trial of Adjuvant Imatinib. JAMA Surg 2020;155:e200397. 10.1001/jamasurg.2020.0397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ozkan EE. Radiotherapy for Gastrointestinal Stromal Tumors. Chin Med J (Engl) 2018;131:235-40. 10.4103/0366-6999.222344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Corbin KS, Kindler HL, Liauw SL. Considering the role of radiation therapy for gastrointestinal stromal tumor. Onco Targets Ther 2014;7:713-8. 10.2147/OTT.S36873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang H, Jiang T, Mu M, et al. Radiotherapy in the Management of Gastrointestinal Stromal Tumors: A Systematic Review. Cancers (Basel) 2022;14:3169. 10.3390/cancers14133169 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as