

Abstract
Rifampicin and rifabutin can activate the pregnane X receptor (PXR, NR1I2), thereby inducing pharmacokinetically important genes/proteins and reducing exposure to co-administered drugs. Because induction effects vary considerably between these antibiotics, differences could be due to unequal rifamycin-induced activation or tissue expression of the three major NR1I2 splice variants, PXR.1 (NM_003889), PXR.2 (NM_022002), and PXR.3 (NM_033013). Consequently, PXR activation (PXR reporter gene assays) and mRNA expression levels of total NR1I2, PXR.1, PXR.2, and PXR.3 were investigated by polymerase chain reaction in colon and liver samples from eleven surgical patients, in LS180 cells, and primary human hepatocytes. Compared to the colon, total NR1I2 mRNA expression was higher in the liver. Both tissues showed similar expression levels of PXR.1 and PXR.3, respectively. PXR.2 was not quantifiable in the colon samples. Rifampicin and rifabutin similarly enhanced PXR.1 and PXR.2 activity when transfected into LS180 cells, while PXR.3 could not be activated. In LS180 cells, rifampicin (10 μM) reduced total NR1I2 and PXR.3 expression 2-fold after 24 h, while rifabutin (10 μM) increased total NR1I2, PXR.1, PXR.2, and PXR.3 mRNA by approx. 50% after 96-h exposure. In primary human hepatocytes, rifampicin (10 μM) suppressed total NR1I2, PXR.1, and PXR.3 after 48-h exposure, and rifabutin (10 μM) had no significant impact on total NR1I2 or any of the splice variants studied. In conclusion, both antibiotics activated the studied PXR splice variants similarly but modified their expression differently. While rifampicin can suppress mRNA of PXR forms, rifabutin rather increases their expression levels.
Supplementary Information
The online version contains supplementary material available at 10.1007/s00210-023-02768-z.
Keywords: Pregnane X receptor, Splice variant, Expression, Rifampicin, Rifabutin, Primary human hepatocytes
Introduction
Rifampicin and rifabutin are antibiotics mostly used against mycobacterial infections. Their use is complicated by the high risk of reducing the exposure to co-administered drugs by increasing the intestinal and hepatic expression and activity of proteins being involved in drug metabolism (e.g., cytochrome P-450 isozyme 3A4, CYP3A4) and drug transport (e.g., by P-glycoprotein (P-gp), encoded by ABCB1). The risk of drug-drug interactions between rifampicin and rifabutin and other drugs has been known for decades, but the reasons for the considerable differences between the individual rifamycins have not yet been clarified. In general, rifabutin is considered a weaker inducer than rifampicin (Baciewicz et al. 2008; Finch et al. 2002), but detailed comparisons are scarce or misleading because clinical trials always compared the standard doses of 300 mg/day rifabutin with 600 mg/day rifampicin and did not regard the effects of resulting plasma concentrations. Meaningful comparisons of the pharmacodynamics of induction between rifabutin and rifampicin are thus difficult to obtain (e.g., dose-dependent or concentration-dependent CYP3A4 induction). In vitro, we have recently shown that rifabutin poorly enhances CYP3A4 mRNA or activity when compared to rifampicin, after normalization of effects to intracellular rifamycin concentrations (Nilles et al. 2023). This data thus suggests that molecular differences between the two drugs may explain their unequal inducer properties.
The pregnane X receptor (PXR, encoded by NR1I2) is an important nuclear transcription factor that enhances the expression of CYP3A4 and ABCB1 upon activation by rifampicin or rifabutin (Chen & Raymond 2006). Besides polymorphisms of the NR1I2 gene (Svärd et al. 2010; Lamba et al. 2008), transcript variants originating from alternative splicing have been reported. Three major PXR variants have mostly been described (Brewer & Chen 2016): PXR.1 (NM_003889; NP_003880; 434 amino acids) and PXR.2 (NM_022002; NP_071285; 473 amino acids) share exon 2 to 9. The relevant structural difference is that PXR.2 starts from exon 1b (compared to exon 1a in PXR.1), resulting in an additional 39 amino acids at the N-terminus compared to PXR.1. Functionally, these two splice forms are considered comparable (Lin et al. 2009). PXR.3 (NM_033013; NP_148934; 397 amino acids; misleadingly called PXR.2 in Lin et al. 2009) is a truncated protein that harbors an altered ligand-binding domain. Consequently, activation of PXR.3 by rifampicin is weaker than the activation of PXR.1 (“wild-type”). In addition, PXR.3 can counteract the effects of PXR.1 (Lin et al. 2009). Thus far, the variable response of the different splice forms to rifampicin and rifabutin has never been compared as a possible cause of the differences in their drug interaction potential. Finally, there is limited information on the interindividual (Breuker et al. 2014; Liu et al. 2009) variability of mRNA expression levels of NR1I2 splice variants in LS180 cells, primary hepatocytes, or in major drug-metabolizing human tissues such as the liver.
In consequence, the in vitro activation of PXR.1 to PXR.3 by rifampicin or rifabutin was compared through reporter gene assays. Effects of drug treatment on expression levels in LS180 cells and primary human hepatocytes were assessed. Finally, matched samples of colon and liver specimens were evaluated for mRNA expression levels to record interindividual variability of the splice form expression levels.
Materials and methods
Materials
Dulbecco’s modified Eagle’s medium (DMEM) and fetal calf serum (FCS) were purchased from PAN-Biotech (Aidenbach, Germany) and Livetech (Monticello d’Alba, Italy). Phosphate-buffered saline (PBS), medium supplements for LS180 cell culture (glutamine, non-essential amino acids, penicillin/streptomycin), β-mercaptoethanol, dexamethasone, extracellular matrix (ECM) from Engelbreth-Holm-Swarm murine sarcoma, trypan blue solution, and Williams’ medium E were purchased from Sigma-Aldrich (Taufkirchen, Germany). Cryopreserved Hepatocyte Recovery Medium (CHRM) was purchased from Invitrogen (Carlsbad, CA). Phosphate-buffered saline and L-glutamine (GlutaMAX, 100X) were purchased from Thermo Fisher Scientific (Waltham, MA), and insulin-transferrin-selenious acid (ITS), ITS+ (supplemented with bovine serum albumin, 100X), and BD BioCoat collagen I-coated plates were obtained from BD Biosciences (San Jose, CA, USA). Rifampicin and dimethyl sulfoxide (DMSO) were purchased from AppliChem (Darmstadt, Germany) and Sigma-Aldrich (Taufkirchen, Germany). Rifabutin was purchased from Santa Cruz Biotechnology (Heidelberg, Germany) and Cayman Chemicals (Ann Arbor, MI). The Dual-Glo Luciferase Assay System, the pGL4.21 vector, the pGL4.74 [hRluc/TK] Renilla vector, the FuGene® HD Transfection reagent, and the CytoTox ONE™ Homogeneous Membrane Integrity Assay were purchased from Promega Corporation (Madison, WI, USA). The NR1I2 (NM_003889, NM_022002, NM_033013) human cDNA TrueClone® vectors (containing the cDNA of the NR1I2 splice variant) were obtained from OriGene (Rockville, MD, USA). Qiazol, the RDD buffer, DNAse, the RNeasy Micro Kit (50), and QIAshredder columns were purchased from Qiagen (Hilden, Germany). The High-Capacity Reverse Transcription Kit was obtained from Applied Biosystems (Foster City, CA, USA). Absolute ethanol was purchased from Riedel de Haen (Seelze, Germany). Cell culture flasks and white 96-well plates with white bottom were obtained from Greiner (Frickenhausen, Germany).
Stock solutions
For experiments with LS180 cells, rifampicin and rifabutin (100 mM stock solutions) were dissolved in DMSO. The stock solutions were diluted with supplemented medium prior to the experiments. The DMSO concentrations in the assays did not exceed 0.1%. For primary human hepatocyte incubations, rifampicin and rifabutin were initially dissolved in ACN/MeOH (1:2) to obtain a 25 mM stock solution. Subsequently, rifamycins were diluted with ACN/MeOH (1:2) to obtain a 5 mM solution. Prior to the treatments, rifamycin solutions were diluted with hepatocyte cell culture medium without supplemented FCS to obtain the final concentration of 10 μM. All stock solutions were freshly prepared prior to the induction experiments. Dexamethasone for hepatocyte cell culture was dissolved in DMSO to obtain a 1 mM solution and was stored at −20 °C.
LS180 cell culture
LS180 cells originate from a human colon adenocarcinoma and are available at ATCC (Manassas, VA, USA). This cell line shows activity and inducibility of PXR-driven genes or proteins (e.g., CYP3A4 or P-gp) and has consequently been used in many experiments investigating the PXR-mediated induction of drug metabolism or drug transport (Weiss et al. 2013; Harmsen et al. 2008; Gupta et al. 2008; Harper et al. 1991). Moreover, it has been used to assess PXR activation or inhibition through luciferase-based reporter gene assays (Nilles et al. 2022; Weiss et al. 2013). LS180 cells were cultured under standard conditions with DMEM supplemented with 10% FCS, 2 mM glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin sulfate, and 0.1 mM non-essential amino acids.
Primary human hepatocyte culture
Commercial primary human hepatocytes were purchased from BioIVT (West Sussex, UK; donors: OQA (male), QBU (male), CRT (male)) and Lonza (Basel, Switzerland; donors: HUM183121 (male), HUM190171 (female)). Culturing, quality assessment, and drug treatment were performed as described below. Briefly, cryopreserved hepatocytes were briefly prewarmed and transferred into CHRM thawing medium. Death cells were removed by centrifuging the CHRM medium containing floating cells at 100 g for 10 min at room temperature with braking function set off. Williams’ medium E was supplemented with ITS+ (final concentrations: 6.25 μg/mL insulin, 6.25 μg/mL transferrin, 6.25 ng/mL selenious acid, 5.35 μg/mL linoleic acid, 1.25 mg/mL bovine serum albumin), dexamethasone (final concentration: 0.01 μM), penicillin/streptomycin, and L-glutamine to obtain the primary hepatocyte cell culture medium. A Neubauer chamber was used for cell counting and cell viability was assessed by trypan blue exclusion (only viabilities > 80% were accepted). The cell number was adjusted with hepatocyte plating medium (+ 6% FCS and 0.1 μM dexamethasone) to 550,000 cells/mL (= 55,000 cells/well). Afterwards, cells were seeded on a 96-well collagen I-coated plate and were incubated for 4 h at 37 °C with 5% CO2 and 95% humidity. After incubation, an overlay with ECM gel (0.25 mg/mL protein in culture medium with 0.01 μM dexamethasone; 0.1 μM for HUM183121 donor) was performed to generate the final hepatocyte sandwich culture.
Clinical samples of benign liver and colon tissue
The clinical tissue samples of healthy liver and matched colon had been obtained during the surgical treatment of carcinoma of the rectum or colon, or its metastases. Ethics approval was obtained from the responsible Ethics Committee of the Medical Faculty of Heidelberg University (ethical approval number S-649/2012). All patients gave their written informed consent before being enrolled in the study; their characteristics are listed in Table 1. RNA was isolated as published previously (Shen et al. 2020). Briefly, tissue samples were dispensed with 1 mL Qiazol and stainless-steel beads, and disintegrated using a tissue lyser. The lysate was incubated with 200 μL chloroform for 6 min and centrifuged at 14,800 g for 15 min at 4 °C. Five-hundred microliters of the supernatant was transferred into a new tube, mixed with 500 μL isopropanol, and stored overnight at −20 °C. After centrifugation (14,800 g, 15 min, 4 °C), the supernatant was discarded, and the pellet was washed with ice-cold ethanol (75%), and pelleted again by centrifugation. After drying the sample, the pellet was resuspended with 30 μL distilled water and incubated at 60 °C for 10 min. After adding 3 μL of RDD buffer and 1 μL DNAse, the sample was incubated for 20 min at 37 °C. After centrifugation (14,800 g for 1 min at 4 °C), the RNA contained in the supernatant was transferred into a new tube. Afterwards, RNA concentrations and purity of the samples were determined. The transcriptase-based RevertAid™ H Minus First Strand cDNA Synthesis Kit was used to transfer isolated RNA into cDNA.
Table 1.
Demographic data of patients the liver and colon samples were obtained from
| Patient # | Sex | Age (y) | Neoplastic diagnosis | TNM-classification (8th edition) | Neoadjuvant chemotherapy | Adjuvant chemotherapy | Comorbidity |
|---|---|---|---|---|---|---|---|
| 1 | Female | 55 | Rectum carcinoma | pT3pN1M0 | No | Yes | Hypothyroidism, bronchial asthma |
| 2 | Female | 56 | Metastasized rectum carcinoma | pT3pN1M1 | Yes | Yes | Hypertension |
| 3 | Male | 58 | Metastasized rectum carcinoma | pT2pN1M1 | No | Yes | Hypertension, cervix carcinoma |
| 4 | Female | 73 | Metastasized colon carcinoma | pT3pN2M1 | No | No | Chronic obstructive pulmonary disease |
| 5 | Male | 70 | Metastasized rectum carcinoma | pT4pN2M1 | No | Yes | Acoustic neuroma |
| 6 | Male | 87 | Metastasized rectum carcinoma | pT3pN2M1 | No | Yes | Hypertension |
| 7 | Female | 64 | Metastasized colon carcinoma | pT2pN1M1 | Yes | Yes | Hypertension |
| 8 | Female | 55 | Metastasized rectum carcinoma | pT2pN2M1 | No | Yes | Epilepsy |
| 9 | Female | 76 | Metastasized colon carcinoma | pT4pN2M1 | No | Yes | Type 2 diabetes mellitus |
| 10 | Male | 58 | Metastasized caecum carcinoma | pT1pN1M1 | Yes | Yes | Hypertension, coronary heart disease, non-alcoholic fatty liver disease, obesity |
| 11 | Male | 60 | Metastasized colon carcinoma | pT3pN0M1 | Yes | Yes | Hypertension, coronary heart disease |
Growth inhibition assay
Because growth-inhibiting effects can confound the results obtained in cell culture, potential antiproliferative effects of rifamycins were investigated in LS180 cells prior to incubation experiments by crystal violet staining as published previously (Peters et al. 2006). Briefly, seeded cells were exposed to different rifamycin concentrations for 24 h, 96 h, or 144 h. After incubation, cells were washed with PBS and subsequently stained with 50 μL crystal violet for 15 min at room temperature on a rotary shaker. Afterwards, cells were washed thrice with double distilled water to remove unbound dye. Experiments were performed in three independent biological replicates with quadruplets for each concentration. Absorption of crystal violet (555 nm) was recorded after dissolving the wells with 200 μL methanol (SpectraMax iD3 from Molecular Devices, Wokingham, UK), and mean background values were subtracted from the measured absorbance values of the cell samples. The proliferation of untreated cells was set to 100%. Only rifamycin concentrations below the IC20 value were used in all subsequent experiments.
Lactate dehydrogenase assay
Possible cytotoxic effects of the rifamycins on primary human hepatocytes were evaluated with the CytoTox ONE™ Homogeneous Membrane Integrity Assay (Promega Corporation, Madison, WI, USA) according to the manufacturer’s instructions. This fluorescence-based system detects lactate dehydrogenase activity (LDH) in the supernatant when the cell membrane is disrupted. Briefly, 50 μL of cell culture supernatant was transferred after the treatment period to a black 96-well plate, and 50 μL of CytoTox ONE™ reagent (including LDH substrate) was added. After brief shaking, plates were incubated for 7 min at room temperature under light protection. Fluorescence was recorded with a Tecan Spark plate reader (excitation: 545 nm, emission: 590 nm) after adding 25 μL stop solution. A lysis control, provided by the manufacturer, served as a positive control. To determine cytotoxic effects, the mean background values of the background fluorescence were subtracted from the measured fluorescence values of the samples. Untreated cells were set to 100%. Cytotoxic effects were assessed for each sample/well.
PXR activity assay
The methodology of the PXR reporter gene assay has been described previously (Weiss et al. 2013; Nilles et al. 2022). Seeded cells (50,000 LS180 cells per well) were transfected with 20 ng of the respective PXR splice variant expression vector, 80 ng of the reporter vector (PXR response elements of the CYP3A4 gene, cloned upstream of the firefly luciferase open reading frame), and 10 ng of the Renilla vector (pGL4.74 [hRluc/TK]), used for signal normalization. Twenty-four hours after transfection, cells were treated with rifampicin or rifabutin for 72 h, and the resulting luminescence (firefly and Renilla) was recorded with the SpectraMax iD3 luminometer, using the Dual-Glo Luciferase assay system according to the manufacturer’s instructions. Experiments were performed in three independent biological replicates with quadruplets for each concentration. Because preliminary control experiments had demonstrated variable antiproliferative effects of PXR transfection (PXR.1 through PXR.3) and drugs (rifampicin, rifabutin), the distinct exposure concentrations were adapted accordingly to prevent toxic adverse effects and thus differ between the experiments.
Sample preparation of LS180 cells
LS180 cells were seeded (500,000 cells/flask) and allowed to grow for 3 days. Afterwards, cells were induced with 10 μM rifampicin or rifabutin for 24, 96, and 144 h. After each induction period, total RNA was isolated using the GenElute™ Mammalian Total RNA Miniprep Kit according to the manufacturer’s instructions. The transcriptase-based RevertAid™ H Minus First Strand cDNA Synthesis Kit was used to transfer isolated total RNA into cDNA. Experiments were performed in four independent biological replicates.
Sample preparation of primary human hepatocytes
One day after the ECM overlay, primary human hepatocytes were exposed to 10 μM rifampicin or rifabutin for 48 h. After 24 h of incubation, the induction medium was replaced with freshly prepared rifamycin-containing medium. After the entire induction period (48 h), possible cytotoxic effects were assessed with the LDH cytotoxicity assay. Then, total RNA was isolated using the RNeasy Micro Kit according to the manufacturer’s instructions with minor changes. Briefly, cells were lysed with 60 μL RLT buffer (provided by the manufacturer) containing 10 μL/mL β-mercaptoethanol. Three independent replicates were pooled to obtain one final sample with a sufficient amount of total RNA (total lysis volume: 180 μL/replicate). Then, the lysate was transferred to a QIAshredder column and was centrifuged for 2 min at 14,000 rpm to gain optimal RNA extraction. The isolation procedure also included the optional DNase I incubation. Total RNA was eluted with 14 μL RNAse-free water. Subsequently, 150 ng total RNA was applied to synthesize the cDNA using the High-Capacity Reverse Transcription Kit with a final volume of 20 μL. Twenty microliters of RNAse-free water was then added and cDNA was stored at −20 °C.
Evaluation of PXR splice variant expression levels
NR1I2 splice variant expression levels were quantified by real-time reverse transcription (RT) polymerase chain reaction (PCR) with the LightCycler® 480 (Roche Applied Science, Mannheim, Germany). Primers (sequence, nucleotide position) used are listed in Table 2 and the approximate location of the primers is depicted in Fig. 1. In LS180 cells, hypoxanthine-guanine phosphoribosyltransferase was the most stable housekeeping gene under the experimental conditions (tested with geNorm, version 3.4, Center for Medical Genetics, Ghent, Belgium) and was thus used for normalization. For human colon and liver tissue samples and the primary hepatocytes, the human acidic ribosomal protein and the ribosomal protein L13 were used for normalization. Data were analyzed as described previously (Albermann et al. 2005). Analysis of primary hepatocytes (untreated and treated) and tissue samples was performed in two technical replicates. LS180 cell analysis was performed in four independent experiments for each treatment and analyzed with two technical replicates.
Table 2.
Sequences and nucleotide positions of primer pairs for the detection of total NR1I2 and the three NR1I2 splice variants PXR.1, PXR.2, and PXR.3
| Name | Primer sequence | Nucleotide position# | Reference |
|---|---|---|---|
| PXR.1-forward | 5′-ACT TAC CAC CAA GCA GTC C-3′ | 185 to 203 | * |
| PXR.1-reverse | 5′-TCA AAG AGC ACA GAT CTT TCC-3′ | 830 to 850 | * |
| PXR.2-forward | 5′-AAG GAC AGC AGC ATG ACA G-3′ | 37 to 55 | * |
| PXR.2-reverse | 5′-CAA AGT CAG CAT GGT TCC AG-3′ | 189 to 208 | * |
| PXR.3-forward | 5′-TCA AGA ATT TCC GGG TCT CTC-3′ | 728 to 748 | Lamba et al. (2004) |
| PXR.3-reverse | 5′-CGA TGG GCA AGT CCC TGA AG-3′ | 900 to 919 | Lamba et al. (2004) |
| Total NR1I2-forward | 5′- CCC AGC CTG CTC ATA GGT TC- 3′ | 1367 to 1386 | Svecova et al. (2008) |
| Total NR1I2-reverse | 5′-CTG TGA TGC CGA ACA ACT CC-3′ | 1500 to 1519 | Svecova et al. (2008) |
#Primer positions were evaluated by the online tool available at https://www.bioinformatics.org/sms2/primer_map.html using the respective cDNA sequences available at https://blast.ncbi.nlm.nih.gov/Blast.cgi?PROGRAM=blastn&PAGE_TYPE=BlastSearch&LINK_LOC=blasthome
*Primers were designed for this study by means of the online tool available at https://eurofinsgenomics.eu/de/ecom/tools/pcr-primer-design/
Fig. 1.

Structure of the three NR1I2 mRNA transcripts (PXR.1, PXR.2, PXR.3) and binding sites of the respective primer pairs. Exons 2 through 9 are represented as gray rectangles, the alternative exon 1 (1a or 1b) is shown in white. The region of exon 5 that is only expressed in PXR.1 and PXR.2 is highlighted in black. The primer pair for total NR1I2 (NR1I2-for; NR1I2-rev; gray arrows) binds to exon 8/9 (forward primer) and 9 (reverse primer). Primer pair combinations only for NR1I2 splice variants bind to regions being selectively present in the respective transcript variant. PXR.1-for recognizes PXR.1 and PXR.3; PXR.1-rev recognizes PXR.1 and PXR.2; PXR2-for recognizes only PXR.2; PXR.2-rev recognizes PXR.1-3; PXR.3-for recognizes only PXR.3; PXR.3-rev recognizes PXR1-3. The combination of PXR.1-for/rev, PXR.2-for/rev, and PXR.3-for/rev is thus selective for only one splice variant
Statistics
Statistical analysis was performed using GraphPad Prism version 9.1 (GraphPad Software Inc., La Jolla, CA, USA). Differences in the pharmacodynamics (EC50, Emax of reporter gene assay) of rifampicin and rifabutin were evaluated by non-parametric Mann-Whitney test. The impact of drug treatment on NR1I2 or its splice variant expression in primary hepatocytes or LS180 cells was evaluated by non-parametric Kruskal-Wallis test and Dunn’s test, correcting for multiple comparisons. Differences of NR1I2 or its splice variant expression in colon vs. liver samples were evaluated by non-parametric Wilcoxon matched-pairs signed-rank test. Outliers in the clinical sample data set were identified by ROUT testing at a Q-level of 1% and were subsequently excluded from analysis.
Results
Rifamycin-mediated activation of NR1I2 splice variants
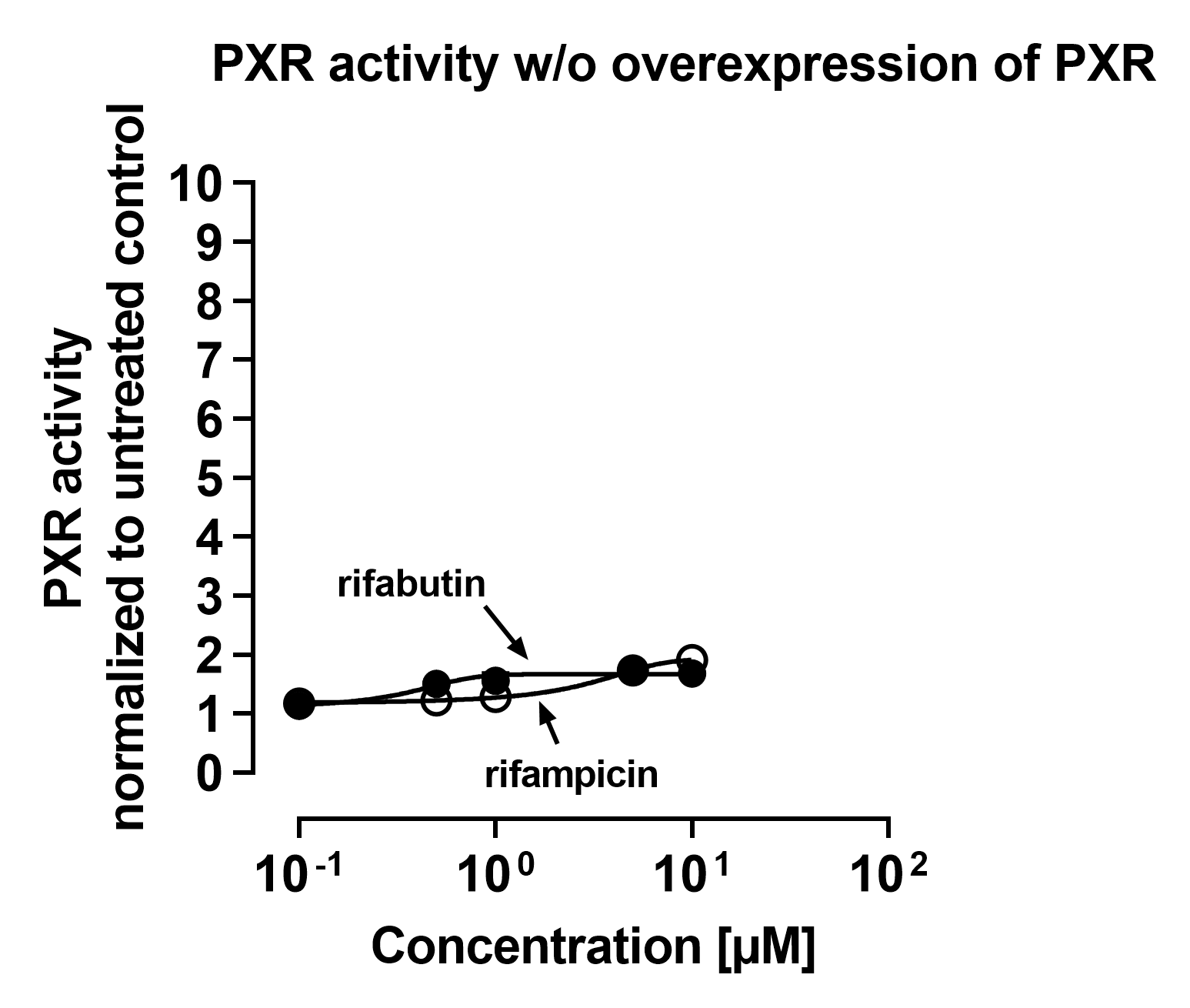
In LS180 cells transfected with the PXR.1 overexpression vector, both rifampicin (EC50: 0.37 ± 0.01 μM) and rifabutin (EC50: 1.54 ± 1.0 μM) enhanced the reporter signal (Emax) approximately 5-fold compared to untreated cells (Fig. 2). Overexpression of PXR.2 yielded similar activation dynamics, which were comparable and non-significantly different to PXR.1 (rifampicin EC50: 0.47 ± 0.05 μM; rifabutin EC50: 1.4 ± 0.78 μM; Emax values approximately 4-fold compared to untreated cells). In contrast, the reporter signals weakly but statistically significantly increased when PXR.3-transfected cells were treated with rifampicin (80% increase in Emax, P = 0.0016), while rifabutin had no effect. The poor activation by rifampicin resembled the activation dynamics of reporter assays without PXR overexpression (endogenous PXR only; 90% increase in Emax compared to untreated control) (Suppl. Fig. S1), suggesting that PXR.3 overexpression did not functionally contribute to the cell’s overall PXR activity.
Fig. 2.

Relative PXR reporter activity in LS180 cells after selective overexpression of NR1I2 splice variants (PXR.1, PXR.2, or PXR.3) and subsequent 72-h exposure to rifampicin (open circles) or rifabutin (closed circles). Data shown is the mean ± S.D. of three independent biological replicates with triplicates for each concentration. Data were fitted according to an Emax model (4-parameter logistic equation; variable with slope)
NR1I2 mRNA expression in LS180 cells
LS180 cells were exposed for 24, 96, and 144 h to 10 μM of each rifamycin. Total NR1I2 mRNA expression was reduced by 40% after 24-h treatment with rifampicin (P = 0.009), while rifabutin enhanced the expression by 46% after 96-h exposure (P = 0.009) (Fig. 3). The mRNA expression of the NR1I2 splice variant PXR.1 was increased by 58% after 96-h treatment with rifabutin (P = 0.007). Likewise, rifabutin enhanced the mRNA expression of PXR.2 by 46% after 96 h (P = 0.048) and by 82% after 144 h (P = 0.029). PXR.3 mRNA expression was reduced by 45% after 24-h treatment with rifampicin (P = 0.016), but was increased by 46% after rifabutin exposure for 96 h (P = 0.046).
Fig. 3.

Impact of 10 μM rifampicin (white bars) or rifabutin (gray bars) for 24 h, 96 h, or 144 h on mRNA expression of total NR1I2 or its splice variants in LS180 cells, normalized to solvent control (black bars). Data shown is the mean ± S.D. of four independent biological replicates. Statistical significance was evaluated by non-parametric Kruskal-Wallis test and Dunn’s test, correcting for multiple comparisons
NR1I2 mRNA expression in primary human hepatocytes
NR1I2 splice variant mRNA expression was also evaluated in primary human hepatocytes from different donors after 48-h treatment with 10 μM rifampicin or rifabutin and compared to solvent controls (Fig. 4). Among the different donors, expression levels differed substantially at baseline (solvent control). Rifampicin lowered the expression of total NR1I2 (P < 0.0001, Fig. 4A), PXR.1 (P = 0.036), and PXR.3 (P = 0.002), whereas rifabutin had no effects. There was no significant impact on PXR.2 expression after rifamycin treatment (Fig. 4B).
Fig. 4.

Relative mRNA expression of total NR1I2 (A) or its splice variants (B) in primary human hepatocytes after treatment with rifampicin or rifabutin (both 10 μM) for 48 h. Data points shown are the mean ± S.D. of hepatocyte samples (pooled from three independent experiments), evaluated by two technical replicates (PCR runs). Statistical significance was evaluated by non-parametric Kruskal-Wallis test and Dunn’s test (correcting for multiple comparisons), comparing all solvent control hepatocyte samples with all rifampicin-treated or rifabutin-treated hepatocyte samples
NR1I2 mRNA expression in samples of healthy liver and colon tissue
In 8 of 9 individuals, total NR1I2 mRNA expression was lower in the colon than in the corresponding hepatic samples of the respective patient (P = 0.008) (Fig. 5A). This difference is likely caused by high hepatic PXR.2 expression, whereas the colon expressed PXR.2 below the detection limit. There were no differences in the tissue-specific expression of PXR.1 or PXR.3 mRNA (Fig. 5B). When comparing the mRNA expression levels of the PXR splice forms, PXR.1 mRNA expression levels were the lowest both in the liver (hepatic PXR.1 vs. hepatic PXR.2: P = 0.009; hepatic PXR1. vs. hepatic PXR.3: P = 0.049) and colon samples (colon PXR.1 vs. colon PXR.3: P = 0.031). In addition, hepatic PXR.2 and hepatic PXR.3 mRNA expression levels were similar.
Fig. 5.

Relative mRNA expression of total NR1I2 (A) or its splice variants (B) in matched samples of healthy liver and colon. Data points shown are the mean relative expression of each sample, evaluated by two technical replicates (PCR runs). Statistical significance was evaluated by non-parametric Wilcoxon matched-pairs signed-rank test. Samples with unreliable housekeeping gene expression or outliers identified by ROUT testing (Q-level at 1%) were excluded from the analysis
Discussion
We have recently shown that rifabutin has considerably fewer effects on CYP3A4 and ABCB1 than rifampicin, especially when normalized to actual intracellular rifamycin concentrations (Nilles et al. 2023). In order to clarify the possible molecular mechanisms leading to the different inductive effects of rifampicin and rifabutin, we investigated three hypotheses on the pharmacology of PXR:
First, rifampicin might be a more potent activator of certain NR1I2 splice variants than rifabutin, leading to a higher overall cellular PXR-activating effect and thus greater induction of CYP3A4 or ABCB1. However, selective overexpression of PXR.1, PXR.2, or PXR.3 and subsequent reporter gene assays did not reveal pharmacodynamic differences between the two antibiotics, suggesting that variable activation of PXR splice forms was not the reason of unequal drug disposition gene inductions by these two compounds. Furthermore, the data confirmed that PXR.3 can hardly be activated by rifampicin (Lin et al. 2009; Hustert et al. 2001) and revealed that this is also true for rifabutin. After PXR.3 transfection (= overexpression), firefly luminescence in fact increased upon rifampicin treatment, but this signal likely resulted from the cells’ endogenous functional PXR (e.g., endogenous PXR.1).
The second tested hypothesis was that rifampicin might be the stronger CYP3A4 or ABCB1 inducer through concurrently enhancing the transcription and thus the expression of the PXR gene or its activatable splice variants (fast-forward mechanism). Consequently, mRNA expression levels in LS180 cells and primary human hepatocytes were assessed after exposure to 10 μM rifampicin or rifabutin for variable exposure times. Rifampicin however lowered the mRNA expression of total NR1I2 and PXR.3 in both primary human hepatocytes and LS180 cells, especially after 24 h of treatment, clearly contradicting the hypothesized fast-forward mechanism. This rifampicin-mediated suppression of total NR1I2 after 24-h drug treatment is consistent with previously reported data (Smutny et al. 2020, Bailey et al. 2011) and seems to be (at least in part) mediated by the PXR.3 suppression because PXR.1 and PXR.2 remained unaffected in LS180 cells. In contrast, rifabutin enhanced the mRNA expression of total NR1I2 in LS180 cells after 96-h drug treatment, which was likely due to enhancements of all three splice variants evaluated. The rifabutin-mediated enhancement of PXR.3 in LS180 cells might have functional consequences because the protein encoded by PXR.3 can hardly be activated or can even out-balance activation of PXR.1 (Lin et al. 2009). For instance, when cells had been co-transfected with a fixed amount of a PXR.1-encoding plasmid (10 ng) plus variable amounts of a PXR.3-encoding plasmid and subsequently treated with rifampicin, the PXR.1 activation was “dose-dependently” compensated by increasing amounts of PXR.3 plasmids (Lin et al. 2009). Accordingly, our data suggest that by concurrently enhancing PXR.3 expression, rifabutin might weaken its activation of PXR.1, partly explaining rifabutin’s weaker net effect on CYP3A4 or ABCB1 in LS180 cells (Nilles et al., 2023). However, this might only be of relevance when NR1I2 and its splice variants are expressed in vivo at all.
Accordingly, our third hypothesis was that the drug-responsive PXR forms are differentially expressed in the liver, a major site of drug metabolism. Moreover, we additionally evaluated expression levels in the colon, a little-studied site of PXR expression (van de Kerkhof 2008). Our data confirmed that total NR1I2 expression levels vary considerably among individuals (Gardner-Stephen et al. 2004) and showed that its expression level in the colon is significantly lower than in the liver. This is in line with previous findings on the PXR target genes. For instance, CYP3A4 and P-gp are highly expressed in the liver but only small amounts of the respective mRNA or protein were detected in the colon (Canaparo et al. 2007; Berggren et al. 2007; McKinnon et al. 1995). The PXR splice variants also tended to be less strongly expressed in the colon than in the liver, but the difference was not statistically significant. Together, the liver certainly is a major site of drug disposition gene induction given its high expression of PXR (mainly driven by high expression of activatable PXR.2). In contrast, the colon expresses less functional PXR, making the colon a less likely site of induction-mediated drug-drug interactions (Huppertz et al. 2019).
This study has its strengths and weaknesses. A major limitation is that expression was not studied in small intestinal tissue, which is as important as the liver for induction-related drug-drug interactions for orally administered drugs (Thelen & Dressman 2009; Galetin et al. 2008; Gorski et al. 2003). In addition, we have only assessed mRNA (but no protein) levels of the NR1I2 splice variants. However, splicing occurs at the level of pre-mRNA and eventually quantifying the mature mRNA forms through PCR thus seems an appropriate approach. Another limitation is the unequal expression of housekeeping genes in the liver and colon samples, so comparative conclusions about the respective expression levels should be taken with caution. The strength of this study is that well-designed, specific primer sequences and their binding sites were used. Previous primer sequences were in fact published (Fukuen et al. 2002; He et al. 2006), but during the establishment of our PCR protocols, these sequences seemed to lead to amplification side products (detected during melting curve analysis), and splice variant sequences were partly overlapped or were not specific. In contrast, the primers indicated here demonstrably led to distinct single PCR products and yielded first information on mRNA expression levels of three major NR1I2 splice variants in matched samples of healthy liver and colon. Another strength is the use of different cell systems (cell line, primary cells, and liver and colon specimens) which allows the drawing of profound conclusions.
Conclusion
While rifampicin and rifabutin activated PXR splice variants similarly, rifampicin tended to decrease the expression of NR1I2 splice variants and rifabutin rather increased them, including the non-activatable PXR.3 splice form. However, these changes appear too small to explain the observed in vivo and in vitro differences in CYP3A4 and P-gp induction by rifampicin or rifabutin.
Supplementary information
{kind=link}
(PNG 56 kb)
(DOCX 13 kb)
Acknowledgements
The authors thank Corina Mueller for excellent assistance with the PCR analysis of all samples. We also thank Dr. Thomas Ebner from Boehringer Ingelheim Pharma GmbH & Co. KG and Prof. Dr. Gerd Mikus from Heidelberg University Hospital for their valuable advices and helpful suggestions throughout the study.
Abbreviations
- PXR
Pregnane X receptor
- CYP3A4
Cytochrome P-450 isozyme 3A4
- P-gp
P-Glycoprotein
Author contributions
JN, MM, DT, JW, and SR performed the experiments, data collection, and analysis. JW developed the qRT-PCR methods. CT and MJS provided clinical samples and demographic data. JN and DT wrote the first draft of the manuscript. WEH discussed the data and commented on the previous versions of the manuscript. The authors declare that all data were generated in-house and that no paper mill was used.
Funding
Open Access funding enabled and organized by Projekt DEAL. Julie Nilles receives an allowance from Boehringer Ingelheim Pharma GmbH & Co. KG.
Data availability
Data is available upon request.
Declarations
Ethical approval
Ethics approval was obtained from the responsible Ethics Committee of the Medical Faculty of Heidelberg University (ethical approval number S-649/2012).
Consent to participate
All patients gave their written informed consent before being enrolled in the study.
Consent for publication
All authors read and approved the manuscript for submission.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Albermann N, Schmitz-Winnenthal FH, Z'graggen K, Volk C, Hoffmann MM, Haefeli WE, Weiss J. Expression of the drug transporters MDR1/ABCB1, MRP1/ABCC1, MRP2/ABCC2, BCRP/ABCG2, and PXR in peripheral blood mononuclear cells and their relationship with the expression in intestine and liver. Biochem Pharmacol. 2005;70:949–958. doi: 10.1016/j.bcp.2005.06.018. [DOI] [PubMed] [Google Scholar]
- Baciewicz AM, Chrisman CR, Finch CK, Self TH. Update on rifampin and rifabutin drug interactions. Am J Med Sci. 2008;335:126–136. doi: 10.1097/MAJ.0b013e31814a586a. [DOI] [PubMed] [Google Scholar]
- Bailey I, Gibson GG, Plant K, Graham M, Plant N. A PXR-mediated negative feedback loop attenuates the expression of CYP3A in response to the PXR agonist pregnenalone-16α-carbonitrile. PLoS One. 2011;6:16703. doi: 10.1371/journal.pone.0016703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berggren S, Gall C, Wollnitz N, Ekelund M, Karlbom U, Hoogstraate J, Schrenk D, Lennernäs H. Gene and protein expression of P-glycoprotein, MRP1, MRP2, and CYP3A4 in the small and large human intestine. Mol Pharm. 2007;4:252–257. doi: 10.1021/mp0600687. [DOI] [PubMed] [Google Scholar]
- Breuker C, Planque C, Rajabi F, Nault JC, Couchy G, Zucman-Rossi J, Evrard A, Kantar J, Chevet E, Bioulac-Sage P, Ramos J, Assenat E, Joubert D, Pannequin J, Hollande F, Pascussi JM. Characterization of a novel PXR isoform with potential dominant-negative properties. J Hepatol. 2014;61:609–616. doi: 10.1016/j.jhep.2014.04.030. [DOI] [PubMed] [Google Scholar]
- Brewer CT, Chen T. PXR variants: the impact on drug metabolism and therapeutic responses. Acta Pharm Sin B. 2016;6:441–449. doi: 10.1016/j.apsb.2016.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canaparo R, Nordmark A, Finnström N, Lundgren S, Seidegård J, Jeppsson B, Edwards RJ, Boobis AR, Rane A. Expression of cytochromes P450 3A and P-glycoprotein in human large intestine in paired tumour and normal samples. Basic Clin Pharmacol Toxicol. 2007;100:240–248. doi: 10.1111/j.1742-7843.2006.00023.x. [DOI] [PubMed] [Google Scholar]
- Chen J, Raymond K. Roles of rifampicin in drug-drug interactions: underlying molecular mechanisms involving the nuclear pregnane X receptor. Ann Clin Microbiol Antimicrob. 2006;5:3. doi: 10.1186/1476-0711-5-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finch CK, Chrisman CR, Baciewicz AM, Self TH. Rifampin and rifabutin drug interactions: an update. Arch Intern Med. 2002;162:985–992. doi: 10.1001/archinte.162.9.985. [DOI] [PubMed] [Google Scholar]
- Fukuen S, Fukuda T, Matsuda H, Sumida A, Yamamoto I, Inaba T, Azuma J. Identification of the novel splicing variants for the hPXR in human livers. Biochem Biophys Res Commun. 2002;298:433–438. doi: 10.1016/s0006-291x(02)02469-5. [DOI] [PubMed] [Google Scholar]
- Galetin A, Gertz M, Houston JB. Potential role of intestinal first-pass metabolism in the prediction of drug-drug interactions. Expert Opin Drug Metab Toxicol. 2008;4:909–922. doi: 10.1517/17425255.4.7.909. [DOI] [PubMed] [Google Scholar]
- Gardner-Stephen D, Heydel JM, Goyal A, Lu Y, Xie W, Lindblom T, Mackenzie P, Radominska-Pandya A. Human PXR variants and their differential effects on the regulation of human UDP-glucuronosyltransferase gene expression. Drug Metab Dispos. 2004;32:340–347. doi: 10.1124/dmd.32.3.340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorski JC, Vannaprasaht S, Hamman MA, Ambrosius WT, Bruce MA, Haehner-Daniels B, Hall SD. The effect of age, sex, and rifampin administration on intestinal and hepatic cytochrome P450 3A activity. Clin Pharmacol Ther. 2003;74:275–287. doi: 10.1016/S0009-9236(03)00187-5. [DOI] [PubMed] [Google Scholar]
- Gupta A, Mugundu GM, Desai PB, Thummel KE, Unadkat JD. Intestinal human colon adenocarcinoma cell line LS180 is an excellent model to study pregnane X receptor, but not constitutive androstane receptor, mediated CYP3A4 and multidrug resistance transporter 1 induction: studies with anti-human immunodeficiency virus protease inhibitors. Drug Metab Dispos. 2008;36:1172–1180. doi: 10.1124/dmd.107.018689. [DOI] [PubMed] [Google Scholar]
- Harmsen S, Koster AS, Beijnen JH, Schellens JHM, Meijerman I. Comparison of two immortalized human cell lines to study nuclear receptor-mediated CYP3A4 induction. Drug Metab Dispos. 2008;36:1166–1171. doi: 10.1124/dmd.107.017335. [DOI] [PubMed] [Google Scholar]
- Harper PA, Prokipcak RD, Bush LE, Golas CL, Okey AB. Detection and characterization of the Ah receptor for 2,3,7,8-tetrachlorodibenzo-p-dioxin in the human colon adenocarcinoma cell line LS180. Arch Biochem Biophys. 1991;290:27–36. doi: 10.1016/0003-9861(91)90587-9. [DOI] [PubMed] [Google Scholar]
- He P, Court MH, Greenblatt DJ, von Moltke LL. Human pregnane X receptor: genetic polymorphisms, alternative mRNA splice variants, and cytochrome P450 3A metabolic activity. J Clin Pharmacol. 2006;46:1356–1369. doi: 10.1177/0091270006292125. [DOI] [PubMed] [Google Scholar]
- Huppertz A, Ott C, Bruckner T, Foerster KI, Burhenne J, Weiss J, Zorn M, Haefeli WE, Czock D. Prolonged-release tacrolimus is less susceptible to interaction with the strong CYP3A inhibitor voriconazole in healthy volunteers. Clin Pharmacol Ther. 2019;106:1290–1298. doi: 10.1002/cpt.1529. [DOI] [PubMed] [Google Scholar]
- Hustert E, Zibat A, Presecan-Siedel E, Eiselt R, Mueller R, Fuss C, Brehm I, Brinkmann U, Eichelbaum M, Wojnowski L, Burk O. Natural protein variants of pregnane X receptor with altered transactivation activity toward CYP3A4. Drug Metab Dispos. 2001;29:1454–1459. [PubMed] [Google Scholar]
- Lamba J, Lamba V, Strom S, Venkataramanan R, Schuetz E. Novel single nucleotide polymorphisms in the promoter and intron 1 of human pregnane X receptor/NR1I2 and their association with CYP3A4 expression. Drug Metab Dispos. 2008;36:169–181. doi: 10.1124/dmd.107.016600. [DOI] [PubMed] [Google Scholar]
- Lamba V, Yasuda K, Lamba JK, Assem M, Davila J, Strom S, Schuetz EG (2004) PXR (NR1I2): splice variants in human tissues, including brain, and identification of neurosteroids and nicotine as PXR activators.Toxicol Appl Pharmacol 199(3):251–265. 10.1016/j.taap.2003.12.027 [DOI] [PubMed]
- Lin YS, Yasuda K, Assem M, Cline C, Barber J, Li CW, Kholodovych V, Ai N, Chen JD, Welsh WJ, Ekins S, Schuetz EG. The major human pregnane X receptor (PXR) splice variant, PXR.2, exhibits significantly diminished ligand-activated transcriptional regulation. Drug Metab Dispos. 2009;37:1295–1304. doi: 10.1124/dmd.108.025213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu Y, Ji W, Yin Y, Fan L, Zhang J, Yun H, Wang N, Li Q, Wei Z, Ouyang D, Zhou HH. The effects of splicing variant of PXR PAR-2 on CYP3A4 and MDR1 mRNA expressions. Clin Chim Acta. 2009;2009(403):142–144. doi: 10.1016/j.cca.2009.02.006. [DOI] [PubMed] [Google Scholar]
- McKinnon RA, Burgess WM, Hall PM, Roberts-Thomson SJ, Gonzalez FJ, McManus ME. Characterisation of CYP3A gene subfamily expression in human gastrointestinal tissues. Gut. 1995;36:259–267. doi: 10.1136/gut.36.2.259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nilles J, Weiss J, Sauter M, Haefeli WE, Ruez S, Theile D. Comprehensive in vitro analysis evaluating the variable drug-drug interaction risk of rifampicin compared to rifabutin. Arch Toxicol. 2023;97:2219–2230. doi: 10.1007/s00204-023-03531-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nilles J, Weiss J, Haefeli WE, Ruez S, Theile D. How to avoid misinterpretation of dual reporter gene assay data affected by cell damage. Arch Toxicol. 2022;96:2501–2510. doi: 10.1007/s00204-022-03323-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters T, Lindenmaier H, Haefeli WE, Weiss J. Interaction of the mitotic kinesin Eg5 inhibitor monastrol with P-glycoprotein. Naunyn Schmiedebergs Arch Pharmacol. 2006;372:291–299. doi: 10.1007/s00210-005-0022-5. [DOI] [PubMed] [Google Scholar]
- Shen Y, Wang X, Lu J, Salfenmoser M, Wirsik NM, Schleussner N, Imle A, Freire Valls A, Radhakrishnan P, Liang J, Wang G, Muley T, Schneider M, Ruiz de Almodovar C, Diz-Muñoz A, Schmidt T. Reduction of liver metastasis stiffness improves response to bevacizumab in metastatic colorectal cancer. Cancer Cell. 2020;37:800–17.e7. doi: 10.1016/j.ccell.2020.05.005. [DOI] [PubMed] [Google Scholar]
- Svärd J, Spiers JP, Mulcahy F, Hennessy M. Nuclear receptor-mediated induction of CYP450 by antiretrovirals: functional consequences of NR1I2 (PXR) polymorphisms and differential prevalence in whites and sub-Saharan Africans. J Acquir Immune Defic Syndr. 2010;55:536–549. doi: 10.1097/QAI.0b013e3181f52f0c. [DOI] [PubMed] [Google Scholar]
- Svecova L, Vrzal R, Burysek L, Anzenbacherova E, Cerveny L, Grim J, Trejtnar F, Kunes J, Pour M, Staud F, Anzenbacher P, Dvorak Z, Pavek P. Azole antimycotics differentially affect rifampicin-induced pregnane X receptor-mediated CYP3A4 gene expression. Drug Metab Dispos. 2008;36:339–348. doi: 10.1124/dmd.107.018341. [DOI] [PubMed] [Google Scholar]
- Smutny T, Dusek J, Hyrsova L, Nekvindova J, Horvatova A, Micuda S, Gerbal-Chaloin S, Pavek P. The 3'-untranslated region contributes to the pregnane X receptor (PXR) expression down-regulation by PXR ligands and up-regulation by glucocorticoids. Acta Pharm Sin B. 2020;10:136–152. doi: 10.1016/j.apsb.2019.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thelen K, Dressman JB. Cytochrome P450-mediated metabolism in the human gut wall. J Pharm Pharmacol. 2009;61:541–558. doi: 10.1211/jpp/61.05.0002. [DOI] [PubMed] [Google Scholar]
- van de Kerkhof EG, de Graaf IA, Ungell AL, Groothuis GM. Induction of metabolism and transport in human intestine: validation of precision-cut slices as a tool to study induction of drug metabolism in human intestine in vitro. Drug Metab Dispos. 2008;36:604–613. doi: 10.1124/dmd.107.018820. [DOI] [PubMed] [Google Scholar]
- Weiss J, Theile D, Spalwisz A, Burhenne J, Riedel K, Haefeli WE. Influence of sildenafil and tadalafil on the enzyme- and transporter-inducing effects of bosentan and ambrisentan in LS180 cells. Biochem Pharmacol. 2013;85:265–273. doi: 10.1016/j.bcp.2012.11.020. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PNG 56 kb)
(DOCX 13 kb)
Data Availability Statement
Data is available upon request.