

Abstract
Background
Use of ureteral stents has become an integral part of urological practice. However, it also brought with it many complications. Double J (DJ) stent knotting is a rare stent complication, and only a few cases have been reported in the literature. Although the exact cause is unknown and, in the literature, it is generally thought that knots occur due to traction. In this case report we present for the first time that spontaneous knots can occur due to ureteral peristalsis or ureteral anomalies.
Case presentation
Two patients (67 and 35 aged-Caucasian person) with ureteral stones who presented to the emergency department with colicky pain and had no previous history of urological surgery. We observed knot formation in the routine urinary system radiographs taken before stent removal in two patients whose ureters were observed to be narrow during endoscopic ureteral stone treatment. The stents were successfully removed using gentle traction under general anesthesia.
Conclusions
We discussed the cause and solution of spontaneous knot formation. We emphasized the importance of the direct urinary system radiograph taken before DJ stent removal.
Keywords: Knotted ureteral stent, Urological complication, Ureteral stent
Introduction
The ureteral stents, which become an integral part of modern urological practice, provide urinary tract access, dilation of urinary strictures, removal of kidney stones, and temporary drainage of urine. There are various size (14–32 cm), diameter (3–8 F), hardness, body, tip shapes (pigtail, double pigtail-JJ) and coating (carbon, hydrophilic, heparin) ingredients for the purpose of use.
During their time with ureteral stents, 80% of patients report experiencing some degree of discomfort. Additionally, the use of ureteral stents may lead to serious complications such as stent migration and stent encrustation. Although spontaneous knotting of the ureteral stent has been reported before, it is one of the rare complications in the literature. There are a variety of techniques reported for the removal of a knotted double J (DJ) stent, from simple traction to open surgery.
Case report
The first case, a 67-year-old man (Caucasian), applied to our clinic with a complaint of left side pain that had been going on for a month. On physical examination, positive left costovertebral angle (CVA) tenderness was observed (Table 1). He had hypertension and diabetes. There was a stone disease in his father. The patient had no previous history of renal colic, urinary system stone disease or any surgical intervention. In the imaging performed for the patient, “Grade 2 ectasia in the upper collecting system of the left kidney, double ureter appearance on the left and suspicious stone image at the level of the left iliac crossover” was observed; ureterorenoscopy (URS) was planned for the patient. During cystoscopy, a close monitoring of the patient’s left ureteral orifice revealed an attempt to insert a sensor guide. However, it failed to transition from the middle ureter to the proximity. Then, the distal ureter was entered through the left ureteral orifice by applying ureteral balloon dilation under the guidance of a sensor guide. The ureter at the iliac cross level was passed with difficulty, but due to stenosis, it could not be advanced further proximally; 4.8 Fr 26 cm DJ was placed and it was seen that both ends were bent under fluoroscopy.
Table 1.
Timeline
| Time (t) | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Important dates | Initial presentation | After 2 weeks (URS time) | 1 day after URS | 6 weeks after URS |
Time intervals are the same for both patients
URS Ureterorenoscopy
The second case (Caucasian), aged 35, had complaints of right-side pain for four months. On physical examination, positive right CVA tenderness was observed (Table 1). The patient had no comorbidity. There was a stone disease in his family. A calculus of 3–4 mm in size was observed in the right distal ureter in the imaging performed on the patient, who had a previous history of passing spontaneous urinary system stones but did not have a previous surgical history. During the URS procedure performed 2 weeks later, annular stenosis was observed 2 cm ahead of the right orifice and was corrected with balloon dilatation. Endoscopic ureteral stone treatment was performed with holmium laser. At the end of the surgery, a 4.8 Fr 26 cm DJ was placed into the right ureter and the procedure was terminated. No perioperative or postoperative complications were observed in both cases, and the urinary system was visualized on the radiography on the first day after the operation (Fig. 1A, B).
Fig. 1.

A Case 1 direct urinary system graphic after Ureterorenoscopy. B Case 2 direct urinary system graphic after Ureterorenoscopy
In both cases, when the urinary system radiographs were repeated six weeks later for routine DJ stent removal; spontaneous knotting was observed at the proximal end of the DJ stents (Fig. 2A, B). Both of patients no bothersome symptoms were reported, and the physical examination was strictly normal. Considering the possibility that the procedure could be complicated, DJ stent removal was planned under general anesthesia. After the distal coil of the DJ stents was corrected, gentle traction was applied toward the contralateral bladder wall. DJ stents were barely removed without complications, and proximal ends were found to be coming in knotted (Fig. 3A, B). A 7Fr ureteral catheter was placed over the guide wire to the renal pelvis. The ureteral catheter was removed on postoperative day 1; After observation, the patient was discharged with nonsteroidal anti-inflammatory drug (NSAII) and antibiotic treatment.
Fig. 2.

A Case 1 direct urinary system graphic taken before Double J removal. B Case 2 direct urinary system graphic taken before Double J removal
Fig. 3.
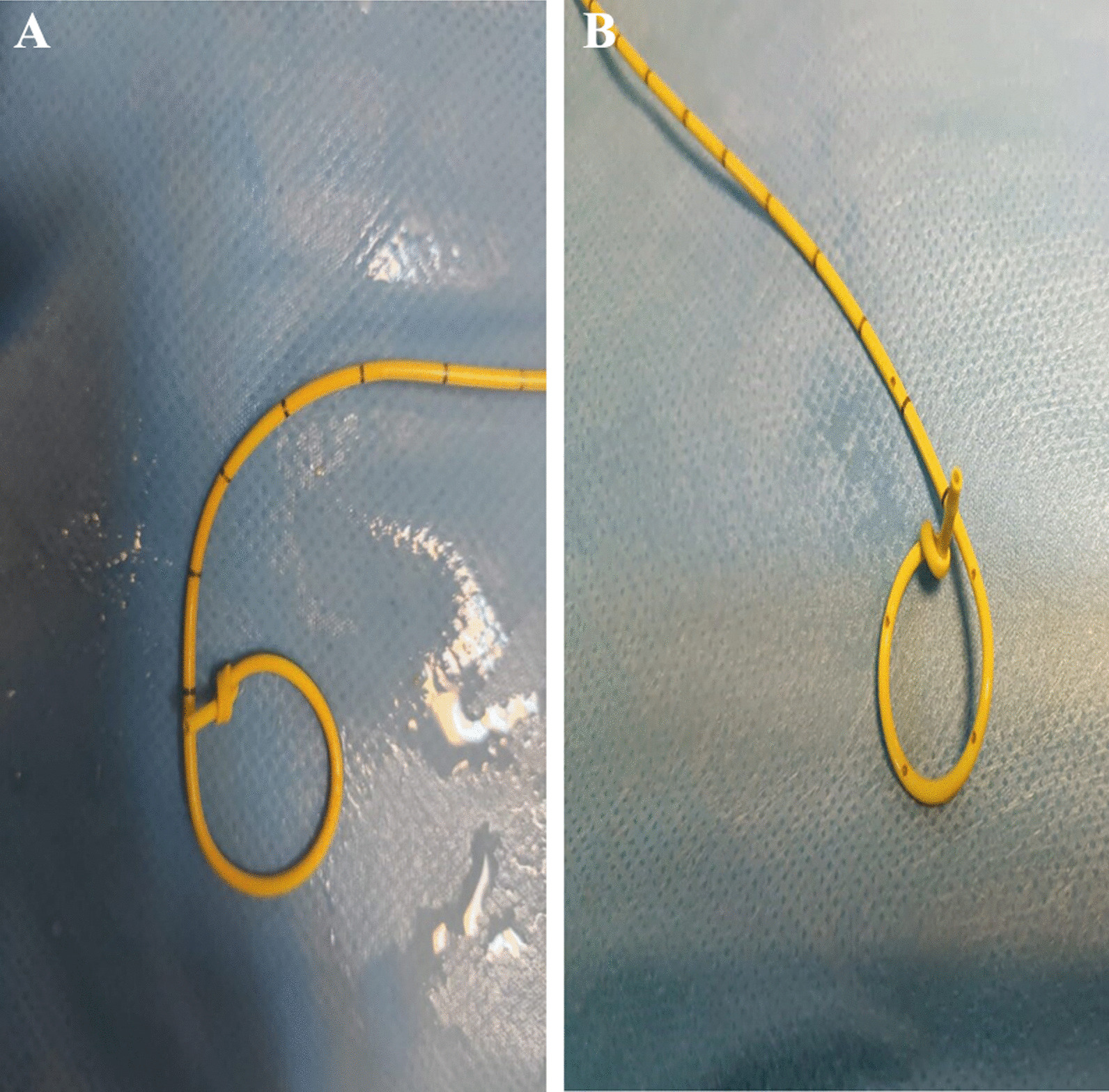
A Case 1 Double J ureteral stent with knot formation at proximal end. B Case 2 Double J ureteral stent with knot formation at proximal end
Discussion
Ureteral DJ stent complications include irritative micturition symptoms, suprapubic pain, costovertebral pain, vesicorenal reflux, stent malposition, hematuria, urinary tract infection, fever, encrustation, stent migration, stent rupture, ureteral perforation, erosion and fistulization. To our best knowledge, only a few cases have been identified in the literature since Groeneveld et al. first reported it in 1989 [1]. Table 2 summarized the previously recent published cases regarding DJ stent knotting. Knotted formation is a rare complication, with only 40 cases being described and can be vexing to manage. In the vast majority of reported cases (92.5%), knotting was observed at the proximal end of the DJ stent. In our patients and in the majority of other cases of knotting, the patients were asymptomatic and the cases typically presented with unexpected resistance during DJ stent removal.
Table 2.
Literature review of knot formation
| Case | Year | Author | Age/Gender | Location | Technique of removal |
|---|---|---|---|---|---|
| 1 | 1989 | Groeneveld et al. [1] | NA | Proximal | Gentle traction |
| 2 | 1990 | Das et al. [9] | 45/M | Distal | Gentle traction |
| 3 | 1992 | Braslis et al. [10] | 37/F | Proximal | Percutaneous nephrostomy (PCN) removal |
| 4 | 1994 | Kundagi et al. [11] | 53/M | Proximal | PCN removal |
| 5 | 1995 | Flam et al. [7] | 86/M | Proximal | 2nd DJ stent and URS |
| 6 | 1998 | Baldwinn et al. [6] | 73/M | Proximal | Guidewire (Superstiff) to untie the knot |
| 7 | 2002 | Quek M et al. [12] | 66/F | Mid | Gentle traction |
| 8 | 2005 | Sighinolfi et al. [4] | 48/M | Proximal | Continuous traction for 3 days and ESWL |
| 9 | 2005 | Kondo et al. [13] | 37/M | Proximal | Ureterotomy |
| 10 | 2006 | Eisner et al. [5] | 82/F | Proximal | Gentle traction (Valsalva) |
| 11 | 2007 | Basavaraj et al. [14] | 70/F | Proximal | PCN and gentle traction |
| 12 | 2009 | Rivalta et al. [15] | 83/M | Proximal | Gentle traction with vaseline lubrication |
| 13 | 2010 | Picozzi et al. [16] | 41/F | Proximal | Gentle traction |
| 14 | 2011 | Tempest et al. [17] | NA | Proximal | URS and Holmium laser |
| 15 | 2011 | Richards et al. [18] | 67/M | Proximal | URS and Holmium laser |
| 16 | 2012 | Moufid et al. [19] | 32/M | Proximal | 2nd DJ stent and gentle traction |
| 17 | 2012 | Karaguzel et al. [20] | 53/M | Proximal | URS and gentle traction |
| 18 | 2012 | Nettle et al. [21] | 43/M | Proximal | URS and Holmium laser |
| 19 | 2012 | Bhirud et al. [22] | 41/M | Proximal | Percutaneous removal with 26F nephroscope |
| 20 | 2015 | Ahmadi et al. [8] | 45/M | Proximal | URS and Holmium laser |
| 21 | 2015 | Ahmadi et al | 43/M | Proximal | URS and Holmium laser |
| 22 | 2015 | Ahmadi et al | 71/M | Proximal | URS and percutaneous retrieval at later date |
| 23 | 2015 | Ahmadi et al | 55/M | Proximal | URS and Holmium laser |
| 24 | 2015 | Kim et al. [23] | 53/M | Proximal | Percutaneous and Terumo Guidewire |
| 25 | 2015 | Manohar et al. [24] | 65/M | Proximal | Staged percutaneous antegrade removal |
| 26 | 2015 | Manohar et al. | 65/F | Proximal | URS and Holmium laser |
| 27 | 2015 | Manohar et al. | 55/F | Proximal | URS and Holmium laser |
| 28 | 2015 | Manohar et al. | 59/M | Proximal | Gentle traction |
| 29 | 2020 | Bradshaw et al. [3] | 57/F | Proximal | URS and dilation |
| 30 | 2020 | Cho et al. [25] | 62/M | Proximal | URS and guidewire |
| 31 | 2021 | Choo ZW et al. [26] | 73/M | Proximal | URS and Holmium laser |
| 32 | 2022 | Agarwal et al. [27] | 77/M | Proximal | Access sheath assembly |
| 33 | 2022 | Agarwal et al | 44/M | Proximal | Access sheath assembly |
| 34 | 2022 | Agarwal et al | 65/M | Proximal | Access sheath assembly |
| 35 | 2022 | Gur et al. [28] | 25/F | Mid | Guidewire |
| 36 | 2022 | Jendouzi et al. [2] | 20/M | Proximal | URS and Holmium laser |
| 37 | 2022 | Divya et al. [29] | 5/M | Proximal | Percutaneous and cystoscopically |
| 38 | 2023 | Weeratunga et al. [30] | 73/M | Proximal | Loop-snare technique |
| 39 | 2023 | Present study | 67/M | Proximal | Gentle traction |
| 40 | 2023 | Present study | 35/M | Proximal | Gentle traction |
DJ double J, ESWL extracorporeal shock wave lithotripsy, PCN percutaneous nephrostomy, URS Ureterorenoscopy
In the majority of reported cases, no abnormal appearance was detected in the urinary system radiograph taken before stent removal [2], which would suggest knotting in the DJ stent; it has been stated that the knot may form due to traction during extraction. However, in our cases, knot formation was observed to develop spontaneously immediately after URS, without any intervention or traction. This suggests that knot formation may develop due to the ureter’s own peristalsis or secondary to balloon dilatation applied to the abnormal ureter.
In approximately one-third of reported cases, the DJ stent could be removed with gentle traction and the condition was treated successfully [3]. However, this procedure carries risks for these patients as it may make the existing knot tighter and increase the degree of complications. If strong resistance is encountered during DJ stent removal, alternative interventions should be considered to avoid causing serious ureteral trauma or loss of renal function [3]. In previous years, “the use of sterile Vaseline in addition to traction” has been tried; There are suggestions such as “securing the distal end of the DJ catheter to the leg with a catheter band and providing continuous traction for 3 days” or “applying extracorporeal shock wave lithotripsy (ESWL) to the migrated area of the knotted stent” [4].
In another case where knot formation was observed twice in the same patient, no additional intervention was required to open the second knot formation; spontaneous resolution of the node has been associated with the Valsalva effect achieved by recurrent severe coughs [5]. Valsalva has been suggested as an easy and harmless treatment before invasive procedures for removing knotted stents.
Baldwin et al. used an “Amplatz 0.038 super stiff guidewire” at the proximal end of the stent to solve knot formation [6]. Flam et al. placed a second ureteral stent next to the knotted stent, and a week later, the stent was removed with 5Fr alligator forceps [7]. Endourologically, breaking down the knot formation with a holmium laser and removing the stent has been suggested in the literature as another method [8]. Removal of knot-forming stents via percutaneous or open surgery should only be performed after failure with other techniques. Urologists should be aware of the possibility of knot formation in the stent if difficulty is encountered during stent removal.
Conclusion
Although the literature shows that a knot can occur with traction during DJ stent removal, we also believe that a spontaneous node may be caused by ureteral peristalsis or ureteral anomalies. Therefore, the routine use of a urinary system graph (X) for all patients before the release of the DJ stent can prevent potential complications due to spontaneous knot formation.
Even if we do not see knot formation on the x-ray, in all cases with ureteral stent in which difficulty is experienced during removal, the possibility of stent knotting should always be kept in mind and therapy planned accordingly.
Acknowledgements
Not applicable.
Abbreviations
- CVA
Costovertebral angle
- DJ
Double J
- ESWL
Extracorporeal shock wave lithotripsy
- NSAII
Nonsteroidal anti-inflammatory drug
- PCN
Percutaneous nephrostomy
- URS
Ureterorenoscopy
Author contributions
ACK: contributed to the conception and design of the case report. ACK, SA: collection of data, Revision of the manuscript, preparing figures and performing the last evaluation. All the authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
Not applicable.
Declarations
Ethical approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patients for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Groeneveld AE. The role of ESWL in the treatment of large kidney stones. Singap Med J. 1989;30(3):249–254. [PubMed] [Google Scholar]
- 2.Jendouzi O, Lamghari A, Jamali M, Harchaoui A, Alami M, Ameur A. Knotted double J ureteral stent: a case report and literature review. Pan Afr Med J. 2022;5(43):5. doi: 10.11604/pamj.2022.43.5.34538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bradshaw J, Khan A, Adiotomre E, Burbidge S, Biyani CS. Antegrade removal of a knotted ureteric stent: case report and review of literature. Urol Ann. 2020;12(1):96–100. doi: 10.4103/UA.UA_172_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sighinolfi MC, De Stefani S, Micali S, Mofferdin A, Baisi B, Celia A, et al. A knotted multi-length ureteral stent: a rare complication. Urol Res. 2005;33(1):70–71. doi: 10.1007/s00240-004-0441-7. [DOI] [PubMed] [Google Scholar]
- 5.Eisner B, Kim H, Sacco D. Repeat knot formation in a patient with an indwelling ureteral stent. Int Braz J Urol. 2006;32(3):308–9. doi: 10.1590/S1677-55382006000300009. [DOI] [PubMed] [Google Scholar]
- 6.Baldwin DD, Juriansz GJ, Stewart S, Hadley R. Knotted ureteral stent: a minimally invasive technique for removal. J Urol. 1998;159(6):2065–2066. doi: 10.1016/S0022-5347(01)63248-8. [DOI] [PubMed] [Google Scholar]
- 7.Flam TA, Thiounn N, Gerbaud PF, Zerbib M, Debré B. Knotting of a double pigtail stent within the ureter: an initial report. J Urol. 1995;154(5):1858–1859. doi: 10.1016/S0022-5347(01)66801-0. [DOI] [PubMed] [Google Scholar]
- 8.Ahmadi N, Tran M, Elms M, Ko R. Knotted proximal loop of ureteric stents: teview of the literature and five case reports. J Clin Urol. 2015;8(6):432–437. doi: 10.1177/2051415814532810. [DOI] [Google Scholar]
- 9.Das G, Wickham JE. Knotted ureteric stent: an unusual urological complication. J R Coll Surg Edinb. 1990;35:190. [PubMed] [Google Scholar]
- 10.Braslis KG, Joyce G. Spontaneous knotting of a pigtail ureteric stent in the ureter requiring percutaneous removal. Aust N Z J Surg. 1992;62:825–826. doi: 10.1111/j.1445-2197.1992.tb06930.x. [DOI] [PubMed] [Google Scholar]
- 11.Kundargi P, Bansal M, Pattnaik PK. Knotted upper end: a new complication in the use of an indwelling ureteral stent. J Urol. 1994;151:995–996. doi: 10.1016/S0022-5347(17)35146-7. [DOI] [PubMed] [Google Scholar]
- 12.Quek ML, Dunn MD. Knot formation at the mid portion of an indwelling ureteral stent. J Urol. 2002;168(4 Pt 1):1497. doi: 10.1016/S0022-5347(05)64488-6. [DOI] [PubMed] [Google Scholar]
- 13.Kondo N, Yoshino Y, Shiono Y, Hasegawa Y. A case demonstrating knot formation at the upper end of a ureteral stent. Hinyokika Kiyo. 2005;51:385–387. [PubMed] [Google Scholar]
- 14.Basavaraj DR, Gill K, Biyani CS. Case report: knotted ureteral stent in patient with ileal conduit: conservative approach for retrieval. J Endourol. 2007;21:90–93. doi: 10.1089/end.2006.0171. [DOI] [PubMed] [Google Scholar]
- 15.Rivalta M, Sighinolfi MC, Micali S, De Stefani S, Bianchi G. Knotted ureteral catheter in an 83-year-old man: case presentation and urological non-invasive management in the elderly. Urol Res. 2009;37:261–262. doi: 10.1007/s00240-009-0209-1. [DOI] [PubMed] [Google Scholar]
- 16.Picozzi S, Carmignani L. A knotted ureteral stent: a case report and review of the literature. Urol Ann. 2010;2:80–82. doi: 10.4103/0974-7796.65108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tempest H, Turney B, Kumar S. Novel application of an established technique for removing a knotted ureteric stent. BMJ Case Rep. 2011;2011:bcr1120103528. doi: 10.1136/bcr.11.2010.3528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Richards MM, Khalil D, Mahdy A. Successful treatment of stent knot in the proximal ureter using ureteroscopy and holmium laser. Case Rep Med. 2011;2011:502191. doi: 10.1155/2011/502191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Moufid K, Touiti D, Mohamed L. “Knot stent”: AN unusual cause of acute renal failure in solitary kidney. J Clin Imaging Sci. 2012;2:36. doi: 10.4103/2156-7514.97758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Karaguzel E, Kutlu O, Kazaz IO, Gur M, Dil E, et al. Knotted ureteral stent: a rare complication of ureteral stent usage. Urol Res. 2012;40:793–795. doi: 10.1007/s00240-012-0496-9. [DOI] [PubMed] [Google Scholar]
- 21.Nettle J, Huang JG, Rao R, Costello AJ. Ureteroscopic holmium laser ablation of a knotted ureteral stent. J Endourol. 2012;26:968–970. doi: 10.1089/end.2012.0081. [DOI] [PubMed] [Google Scholar]
- 22.Bhirud P, Giridhar V, Hegde P. Midureteric knotted stent removed by percutaneous access! Urol Ann. 2012;4:106–107. doi: 10.4103/0974-7796.95557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kim MS, Lee HN, Hwang H. Knotted stents: case report and outcome analysis. Korean J Urol. 2015;56:405–408. doi: 10.4111/kju.2015.56.5.405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Manohar P, Kan WT, Ranasinghe WK, Cetti RJ, McCahy P. Knotted multilength ureteric stents: a case series. ANZ J Surg. 2016;86:413–414. doi: 10.1111/ans.12689. [DOI] [PubMed] [Google Scholar]
- 25.Cho CL. A knotted ureteral stent. Urology Case Rep. 2020;33:101327. doi: 10.1016/j.eucr.2020.101327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhou Y, Chu X, Yi Y, Lei J, Huang S, Dai Y. A knotted ureteral stent in patient withrenal transplantation: a case report and literature review. Int J Clin Exp Med. 2018;11(6):6364–6368. [Google Scholar]
- 27.Agarwal DK. A novel telescopic access sheath method to manage encrusted or knotted retained ureteral stents. J Endourol. 2022;36(7):989–995. doi: 10.1089/end.2021.0942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gur M, Eraslan A, Mohamed AH, Mohamed AI, Mohamed KA, Cimen S. Management of a patient with a double J stent knotted at the mid-portion. Urol Case Rep. 2022;16(43):102084. doi: 10.1016/j.eucr.2022.102084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Divya G, Kundal VK, Shah S, Debnath PR, Meena AK, Sen A. Complications and management of retained double-J stents in children during the coronavirus disease-2019 pandemic. J Indian Assoc Pediatr Surg. 2022;27(6):735–740. doi: 10.4103/jiaps.jiaps_67_22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Weeratunga GN, Yuan L, Yassaie O, Caswell-Smith P. Case report: retrieval of knotted ureteric stent causing obstructive urosepsis. Urol Case Rep. 2023;4(46):102316. doi: 10.1016/j.eucr.2023.102316. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.