

Abstract
Riedel’s lobe of the liver is a rare anatomical variant often incidentally found on imaging or through the presence of hepatomegaly on physical examination. While patients are usually asymptomatic, the presentation of this condition can vary, ranging from nonspecific symptoms to more severe issues such as torsion, obstruction, rupture, and bleeding. We present a case of a patient with asymptomatic hepatomegaly who was incidentally found to have Riedel’s lobe of the liver, accompanied by an elevated IgG mitochondrial antibody. The range of symptoms associated with this rare anatomical variation underscores its importance in diagnosis and surveillance within this patient population.
Keywords: Accessory hepatic lobe, case report, incidental finding, liver abnormality, liver anatomy
Introduction
The liver, the largest internal organ in the human body, may present with anatomical variations. Riedel’s lobe of the liver is a rare anatomical variation, described as a downward tongue-like projection of the anterior edge of the right liver lobe to the right of the gallbladder.[1] The incidence of Riedel’s lobe varies depending on diagnostic criteria and methods but has been reported to be between 3.3% and 14.5%.[2] We report a case of a 43-year-old female with an incidental finding of non-palpable Riedel’s lobe.
Case Report
A 43-year-old female was referred for evaluation of hepatomegaly, which was revealed on MRI and CT scans dating back to 2016. Her medical history was notable for Irritable Bowel Syndrome (IBS), uterine fibroids, and a history of tumor removal from her right breast. The patient denied any history of alcohol, illicit drug use, hepatotoxic medications, or pre-existing liver disease. The physical exam was unremarkable, and the abdominal exam did not reveal any mass or abnormalities.
Routine blood examination was within normal limits, as were liver function tests, which showed preserved hepatic synthetic function and normal iron studies. The Hepatitis panel (A, B, C), anti-smooth muscle antibody, and LKM-1 IgG antibody were negative. ANA, alpha-1 antitrypsin, and tissue transglutaminase were also negative. The only lab abnormality was an elevated IgG mitochondrial M2 antibody at 54.5 (normal less than 20 units).
CT, MRI, venous duplex, and liver biopsy were all performed. A CT abdomen performed in 2016 showed an enlarged liver, measuring up to 197.3 mm in the sagittal plane (Fig. 1). A CT abdomen performed in 2020 was significant for an enlarged liver with the right lobe extending into the pelvis and “not completely included in the study” (Fig. 2). As shown in Figure 2, the liver measured up to 215.4 mm in the sagittal plane. An MRI of the abdomen revealed a markedly enlarged liver measuring up to 23.8 cm in its craniocaudal dimension with extension into the pelvis, with the pancreas deviated to the left, likely secondary to the prominent hepatomegaly. Venous duplex was significant for normal directional flow in the portal and hepatic veins with no evidence of portal hypertension. Liver biopsy revealed signs of sinusoidal dilatation nonspecific for veno-occlusive outflow obstruction with no signs of inflammation, steatosis, or fibrosis.
Figure 1.
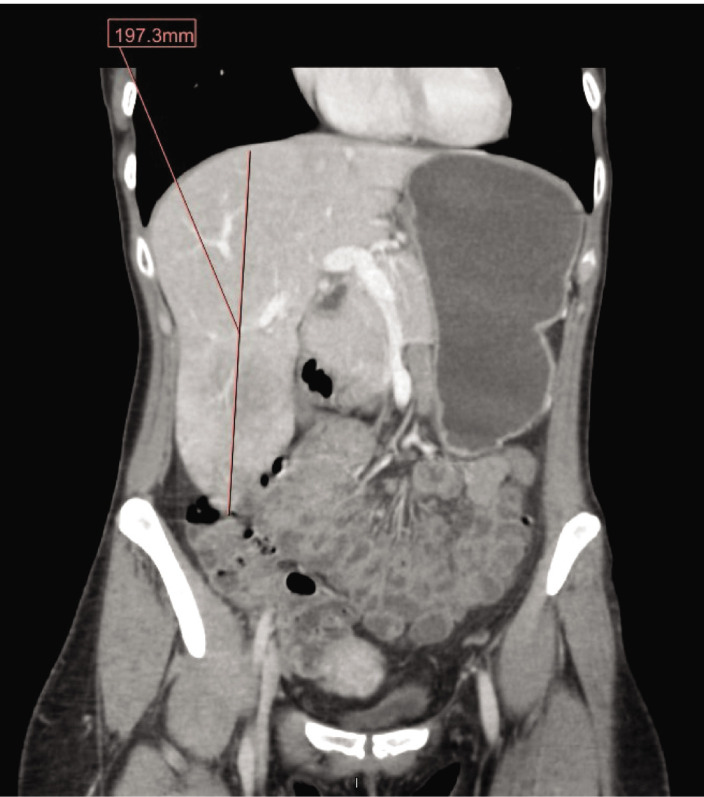
Liver measuring up to 197.3 mm in the sagittal plane on a computed tomography (CT) scan of the abdomen and pelvis in 2016.
Figure 2.

Liver measuring up to 215.4 mm in the sagittal plane on a CT scan of the abdomen and pelvis in 2020.
The patient was diagnosed with Riedel’s lobe of the liver. She was discharged from the hospital without treatment, with a recommendation to repeat an MRI in 1 year, as torsion is a reported complication of Riedel’s lobe over time. The patient will be recommended to repeat LFTs and anti-mitochondrial antibody to determine progression/significance prior to follow-up in 6 months.
Discussion
Riedel’s lobe is an extremely rare hepatic morphological variant, first described by Corbin in 1830 and defined by Riedel in 1888 as a “round tumor on the anterior side of the liver, near the gallbladder, to its right”.[3] The etiology of Riedel’s lobe has been suggested to be either congenital or acquired. The congenital origin is thought to result from a dysmorphic anomaly in the development of a hepatic bud, leading to the formation of accessory lobes in the infrahepatic space.[4,5] These accessory lobes, composed of normal liver parenchyma, can be connected directly to the original liver, by mesentery, or by a pedicle.[6]. Patients with accessory hepatic lobes may have a history of omphalocele or gastroschisis, suggesting a relation to a malformation involving the foregut and abdominal wall.[7] Conversely, Riedel’s lobe may result from acquired risk factors, such as intrapelvic inflammatory conditions. Riedel originally postulated that inflammation in nearby structures, like the gallbladder or appendix, could lead to the elongation of the liver.[3]
The formation of accessory hepatic lobes is extremely rare, with an estimated prevalence of 1%.[2,8] These lobes have been predominantly discovered in adults but have been reported in patients as young as 2 months to as old as 79 years.[7,9] The prevalence of Riedel’s lobe in the general population varies, depending on diagnostic criteria and imaging techniques, but ranges from 3.3% to 14.5%.[2] It has been shown to be higher in women (4.5–19.4%) compared to men (2.1–6.1%).[2] A radiologic series reported a higher prevalence of Riedel’s lobe (31%) and showed no statistical difference between genders,[5] highlighting the variations in diagnostic criteria and methods. Our case represents this unique finding in a middle-aged woman.
Patients with Riedel’s lobe can present with palpable or non-palpable hepatomegaly. Differential diagnoses for palpable hepatomegaly include emphysema, congestive heart failure, and other causes of liver disease such as hepatitis, cirrhosis, and malignancy. Imaging techniques, such as hepatobiliary ultrasonography, abdominal CT, and MRI, are utilized for differentiation and diagnosis. While most patients with Riedel’s lobe are asymptomatic, it can lead to abdominal discomfort, nausea, bloating, and constipation in the event of torsion or external compression of the lobe. Approximately 20–30 cases report mechanical complications, such as torsion of the accessory lobe. Other severe complications reported include gastric outlet obstruction, bleeding, and rupture. Interestingly, cases of malignancy involving Riedel’s lobe have been reported, including primary hepatocellular carcinoma and metastatic nodules. In our case, the patient presented without symptoms and denied any history of complications caused by the accessory lobe.
Conclusion
Our patient was referred after incidental detection of hepatomegaly. Although she was asymptomatic at presentation and denied any history of complications due to Riedel’s lobe, knowledge and surveillance of the accessory lobe are important as it may not always remain clinically latent. Interestingly, our patient was found to have elevated IgG mitochondrial M2 antibody (AMA-M2). AMA-M2 is usually associated with primary biliary cirrhosis (PBC) but can also be found in patients with autoimmune hepatitis. Anti-smooth muscle antibody was negative in our patient. Antimitochondrial antibody is highly sensitive and specific for PBC. Positive results in the setting of normal liver function tests (LFTs) indicate an increased risk of future PBC development.[10] Our patient presented without prior symptoms, normal LFTs, and liver biopsy showed mild sinusoidal dilatation with no signs of inflammation, steatosis, fibrosis, or pathognomonic bile duct lesions. Taking into account our patient’s history, workup thus far, and the limited knowledge about Riedel’s lobe, we will repeat an MRI, AMA-M2, and LFTs prior to follow-up in 1 year.
Footnotes
How to cite this article: Patel AH, Amin R, Abdelsayed G. Congenital Riedel’s lobe of the liver: A case report. Hepatology Forum 2024; 5(2):87–89.
Author Contributions
Concept – AHP, RA, GA; Design – AHP, RA, GA; Supervision – GA; Fundings – GA; Materials – GA; Data Collection and/or Processing – AHP, RA; Analysis and/or Interpretation – AHP; Literature Search – AHP; Writing – AHP; Critical Reviews – AHP, RA, GA.
Conflict of Interest
The authors have no conflict of interest to declare.
Informed Consent
Written informed consent was obtained from the patient for the publication of the case report and the accompanying images.
Use of AI for Writing Assistance
Not declared.
Financial Disclosure
The authors declared that this study has received no financial support.
Peer-review
Externally peer-reviewed.
References
- 1.Zamfir R, Braşoveanu V, Boroş M, Herlea V, Popescu I. Hepatocellular carcinoma in Riedel’s lobe. Chirurgia (Bucur) 2008;103(1):121–123. [PubMed] [Google Scholar]
- 2.Glenisson M, Salloum C, Lim C, Lacaze L, Malek A, Enriquez A, et al. Accessory liver lobes: anatomical description and clinical implications. J Visc Surg. 2014;151(6):451–455. doi: 10.1016/j.jviscsurg.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 3.Riedel I. Uber den zungenformigen Forsarz des rechten Leberlappens und seine pathognostische Bedeutung fur die Erkrankung der Gallenblase nebst Bemerkungen uber Gallenstein Operationen. Berl Klin Wochenschr. 1888;29:577–581. [Google Scholar]
- 4.Couinaud C. 1989. Surgical anatomy of the liver revisited C. Couinaud. [Google Scholar]
- 5.Gillard JH, Patel MC, Abrahams PH, Dixon AK. Riedel’s lobe of the liver: fact or fiction? Clin Anat. 1998;11(1):47–49. doi: 10.1002/(SICI)1098-2353(1998)11:1<47::AID-CA7>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 6.Sommariva A, Pasquali S, Stramare R, Montesco M, Tropea S, Rossi C. Laparoscopic Diagnosis and Treatment of a Twisted Accessory Liver Lobe. CRSLS 11/01. 2014.
- 7.Jambhekar K, Pandey T, Kaushik C, Shah HR. Intermittent torsion of accessory hepatic lobe: An unusual cause of recurrent right upper quadrant pain. Indian J Radiol Imaging. 2010;20(2):135–137. doi: 10.4103/0971-3026.63046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Salisbury SM, Yi CE, Merianos DJ, Sapra A, Anselmo DM. Laparoscopic resection of a torsed accessory hepatic lobe: Case report and literature review. J Pediatric Surg Case Rep. 2013;1(8):214–217. [Google Scholar]
- 9.Hundal RS, Ali J, Korsten MA, Khan AM. Torsion and infarction of an accessory liver lobe. Z Gastroenterol. 2006;44(12):1223–1226. doi: 10.1055/s-2006-926847. [DOI] [PubMed] [Google Scholar]
- 10.Metcalf JV, Mitchison HC, Palmer JM, Jones DE, Bassendine MF, James OF. Natural history of early primary biliary cirrhosis. Lancet. 1996;348(9039):1399–402. doi: 10.1016/S0140-6736(96)04410-8. [DOI] [PubMed] [Google Scholar]