

Abstract
Urinary incontinence (UI) is a disorder of micturition that can occur in dogs of any age, sex, and breed depending on the underlying cause and time of onset. Diagnosis and treatment for various causes of UI in dogs have been described by multiple comprehensive single author review articles, but large prospective clinical trials comparing treatment outcomes in veterinary medicine are lacking. The objectives of this consensus statement therefore are to provide guidelines on both recommended diagnostic testing and treatment for various causes of UI in dogs. Specifically, pathophysiology directly related to the canine urinary system will be reviewed and diagnostic and therapeutic challenges will be addressed. A panel of 12 experts in the field (8 small animal internists [L. Adams, J. Bartges, A. Berent, J. Byron, J. Foster, A. Kendall, S. Vaden, J. Westropp], 2 neurologists [J. Coates, N. Olby], 1 radiologist [G. Oetelaar], and 1 surgeon [C. Adin]) was formed to assess and summarize evidence in the peer‐reviewed literature and to complement it with consensus recommendations using the Delphi method. Some statements were not voted on by all panelists. This consensus statement aims to provide guidance for management of both male and female dogs with underlying storage or voiding disorders resulting in UI.
Keywords: canine, incontinence, urinary
Abbreviations
- 2D
2‐dimensional
- 3D
3‐dimensional
- ABUC
aerobic bacterial urine culture
- Ach‐m
acetylcholine muscarinic receptor
- Ach‐n
acetylcholine nicotinic receptor
- AUS
abdominal ultrasound
- AVMA
American Veterinary Medical Association
- BPH
benign prostatic hyperplasia
- CA‐EU
cystoscopic ablation of ectopic ureters
- CMG
cystometrogram
- CNS
central nervous system
- CT
computed tomography
- CUI‐S
canine urinary incontinence survey
- DUD
detrusor urethral dyssynergia
- EMG
electromyography
- EU
ectopic ureter(s)
- FOO
functional outflow obstruction
- GI
gastrointestinal
- ICS
International Continence Society
- IM
intramuscular
- ISCAID
International Society for Companion Animal Infectious Diseases
- IVDH
intervertebral disc herniation
- LPP
leak point pressure
- LUT
lower urinary tract
- MOO
mechanical outflow obstruction
- MRI
magnetic resonance imaging
- MUCP
maximum urethral closure pressure
- OAB
overactive bladder
- OHE/OVE
ovariohysterectomy/ovariectomy
- PCCL
percutaneous cystolithotomy
- PPA
phenylpropanolamine
- PU/PD
polyuria/polydipsia
- PVRV
post void residual volume
- TURBT
transurethral resection of bladder tumor
- UC
urothelial carcinoma
- UI
urinary incontinence
- UPP
urethral pressure profile
- US
ultrasound
- USG
urine specific gravity
- USMI
urethral sphincter mechanism incompetence
- UTI
urinary tract infection
- VVSR
vestibulovaginal septal remnant
1. INTRODUCTION
There are many disorders of micturition, which can occur in dogs of any age, sex, and breed. Urinary incontinence (UI) is a disorder of micturition characterized by the passive, involuntary leakage of urine. Although the exact prevalence of acquired UI in dogs is unknown, studies have reported a prevalence of 3% to 20% in spayed female dogs. 1 , 2 , 3 , 4 , 5 The prevalence of acquired UI in male dogs is much lower and the underlying causes are less well understood. 6
Prospective clinical trials for diagnostic testing and management of UI in small animal medicine are limited. The use of terminology and diagnostic algorithms from the human medical literature may be inappropriate in veterinary medicine because of anatomical differences. Therefore, an expert panel was convened to provide clinicians the necessary diagnostic testing information to identify the most appropriate treatments for dogs with UI. Pathophysiology related to micturition in dogs will be reviewed and diagnostic and therapeutic challenges addressed. Contributions to this Consensus Statement were provided by members of the Consensus Panel including input from members of the American Society of Veterinary Nephrology and Urology.
2. PHYSIOLOGY
Normal function of the lower urinary tract (LUT) includes storage and voiding of urine. 7 , 8 , 9 The detrusor reflex is involved with the evacuation of urine in response to stretch of the bladder whereas the micturition reflex involves a coordinated and sustained contraction of the detrusor muscle (the detrusor reflex) along with simultaneous relaxation of the urethra. These reflexes are coordinated by autonomic and somatic segmental spinal cord pathways and supraspinal pathways involving the brainstem, cerebellum, and cerebral cortex. The sympathetic and somatic nervous systems govern urine storage whereas the parasympathetic nervous system governs the voiding phase. Coordination of all 3 systems is required for micturition to occur appropriately.
2.1. Lower urinary tract anatomy
The LUT consists of the bladder and urethra. The bladder functions as a reservoir whereas the urethra functions as a sphincter. The bladder is divided into a neck (trigone) and body with a wall composed of 3 interwoven layers of smooth muscle (detrusor muscle) accompanied by mucosal, submucosal, and serosal layers. In the bladder and urethra, the muscle is surrounded by collagen‐rich connective tissue. The proportion of collagen varies between 40% and 70% of the total tissue mass depending upon the region of the LUT and sex of the dog. 10 , 11 Collagen influences the structural properties of the LUT, and the muscle fibers are responsible for contractile activity.
Umbrella cells with tight junctions form the first layer of stratified uroepithelium that lines the mucosal surface of the bladder, ureters and renal pelvis and undergo large conformational changes during bladder filling and emptying. 12 In the normal animal, intra‐abdominal pressure is transmitted to both the bladder and the proximal urethra, assisting in maintaining continence.
The urethral musculature is composed of 2 layers: an inner layer of smooth muscle (internal urethral sphincter) and an outer layer of striated muscle (external urethral sphincter). 10 , 11 The smooth muscle consists of outer and inner longitudinal and middle circular layers that begin at the bladder neck and extend distally. In the female dog, the bladder neck is augmented by a smooth muscle sphincter which encircles the cranial half of the urethra and gradually becomes incorporated with the striated muscle caudal to the vagina (Figure 1). 11 , 13 , 14 Although the predominant constituents of the female urethra are collagenous and elastic fibers, smooth muscle is distributed uniformly throughout the length of the urethra. 13 At the external urethral orifice, striated muscle (urethralis muscle) encloses all but the dorsal surface of the urethra and is interwoven proximally with the urethral smooth muscle to form a prominent sphincter at the external orifice. 15 , 16 Regardless of neuter status, female dogs have a higher proportion of collagen and lower proportion of muscle relative to males.
FIGURE 1.
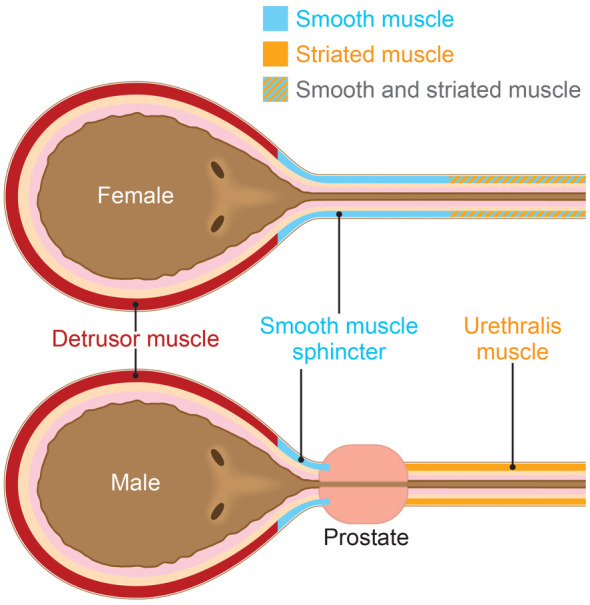
Diagram depicting location of smooth and striated muscle in the male and female bladder and urethra. Source: Image by Tim Vojt, MA. Used with permission from The Ohio State University.
The smooth muscle sphincter is weakly developed in the male urethra and is limited to the prostatic and cranial half of the membranous urethra, comprising only 9% of the wall (Figure 1). 10 , 17 , 18 However, the circular layer of smooth muscle of the bladder neck is thicker in male dogs. 18 The external striated muscle in the membranous urethra comprises >50% to 70% of the urethral wall along the length of the urethra; its circular orientation indicates sphincteric function. 10 , 18
The “urethral sphincter mechanism” responsible for continence is made up of the urethral components described above and their supporting structures. Also included are the neural pathways that activate and inhibit the muscular elements along the urethra.
2.2. Storage phase
As the bladder fills, the intravesicular pressure increases minimally because of the stretch properties of the bladder wall and active relaxation of the detrusor muscle. During low‐level bladder distension, afferent signals that increase in strength are conducted via the pelvic nerve to neurons located in the periaqueductal gray (Figure 2). The periaqueductal gray is a pivotal neuronal pool between the brain and bladder. 19 It can both pass information about the bladder to higher brain centers and receive information from the cerebrum to suppress or enhance storage and voiding. Excitatory axons from the L region, the pontine urine storage center, facilitates urine storage through excitatory synaptic connections with nicotinic cholinergic motor neurons of Onuf's nucleus (located in S1 and S2 segments) that innervate the external urethral sphincter via the pudendal nerve (Figure 2). 20 , 21 , 22 The pudendal nerve stimulates the urethral sphincter to remain tightly closed, allowing closure pressure to exceed the bladder pressure during urine storage to maintain continence.
FIGURE 2.
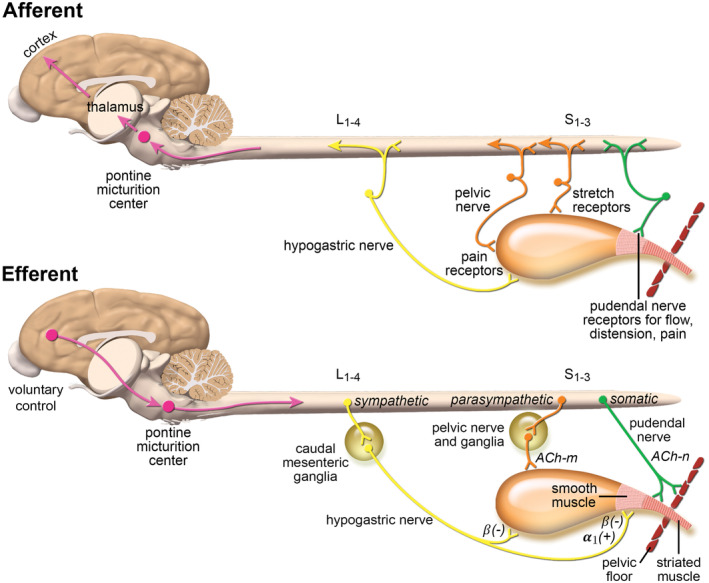
Afferent and efferent bladder innervation and signal pathways. Ach‐n, acetylcholine nicotinic receptor; Ach‐m, acetylcholine muscarinic receptor; α: alpha‐adrenergic receptors; β, beta‐adrenergic receptors. (+) denotes stimulation of muscular contraction, and (−) denotes inhibition of muscular contraction. L1‐4 refers to lumbar spinal cord segments 1 to 4. S1‐3 refers to sacral spinal cord segments 1 to 3. Source: Image adopted Veterinary Clinics: Small Animal Practice, Volume 45, Issue 4, p. 769‐782. Used with permission from author.
Pelvic nerve projections also stimulate pathways to maintain continence: sympathetic neurons of the hypogastric nerve to the bladder outlet and pudendal neurons to the external urethral sphincter. Preganglionic sympathetic neurons to the bladder are in the intermediolateral cell column located between L1 and L4 in the dog (Figure 2). 21 , 23 , 24 These preganglionic fibers course as the lumbar splanchnic nerves to synapse with nicotinic cholinergic receptors on the cell bodies of the caudal mesenteric ganglion or within the bladder wall. Postganglionic axons continue as the hypogastric nerve to the pelvic plexus to innervate the inhibitory beta‐3 adrenergic receptors of the detrusor muscle and the excitatory alpha‐1A adrenergic receptors of the bladder trigone. 25 , 26 The net effect of this involuntary process is bladder wall relaxation and urethral sphincter contraction.
2.3. Voiding phase
Urine voiding is an active, voluntary process coordinated by supraspinal centers and parasympathetic transmission. The voiding phase starts when a critical bladder volume has been reached, which triggers a micturition reflex through Aδ afferents that transmit signals from mechanoreceptors in the bladder wall. Afferent signals in the pelvic nerve activate spinal‐brainstem‐spinal reflex pathways that pass through the periaqueductal gray and the M region of the pontine micturition center, which in turn provides descending output to the sacral spinal nuclei (Figure 2). 27 The preganglionic parasympathetic axons course via the pelvic nerve through the ventral branches of the sacral spinal nerves. The pelvic nerve continues to the pelvic plexus and synapses on cell bodies either of postganglionic axons in the pelvic plexus ganglion or within the bladder wall. Mediated by acetylcholine, the M3 receptors, located within the body and neck of the bladder musculature, are involved in excitatory transmission to cause detrusor muscle contraction and urethral relaxation. Under normal conditions, the voluntary voiding phase is initiated if time and place are appropriate. Disruption of connections between muscle fibers and detrusor atony might occur when the bladder is overdistended.
3. CLASSIFICATION
Statement
Urinary incontinence should be divided into 2 main categories: disorders of storage and disorders of voiding. These can further be subdivided into major causes according to the diagram in Figure 3.
Panel vote
12 of 12 (100%) members strongly agreed with this statement.
FIGURE 3.
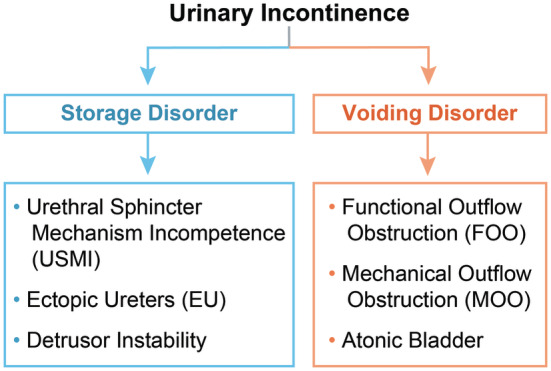
Common causes of urinary incontinence in dogs. Refer to Table 1 for a complete list of differentials.
Disorders of urine storage are characterized by UI with normal postvoiding residual volume (PVRV; see Section 4.3) and further subdivided into functional and mechanical causes (Table 1). Although direct comparison studies still are needed, female dogs are more likely to experience storage disorders whereas male dogs have equal prevalence of storage and voiding disorders. 28 In several studies, some breeds were overrepresented in the UI group, either with urethral sphincter mechanism incompetence (USMI) or ectopic ureter (EU; Box 1). 4 , 5 , 29 , 30
TABLE 1.
Complete list of differentials for urinary incontinence in dogs.
| Disorders of storage |
|---|
|
Nonneurogenic
Neurogenic
|
| Disorders of voiding |
|---|
|
Nonneurogenic
Neurogenic
|
Note: Please note that many neurogenic disorders may result in both disorders of storage and/or disorders of voiding.
Abbreviations: IVDH, intervertebral disc herniation; S1, sacral spinal segment 1.
Indicates most common causes.
BOX 1. The following is a list of breeds identified as overrepresented in developing USMI or EU.
| USMI | EU |
| German shepherd dog | Siberian husky |
| Rottweiler | Labrador retriever |
| Doberman pinscher | Golden Retriever |
| Giant schnauzer | Newfoundland |
| Old English sheepdog | Miniature and toy poodle |
| Boxer | Bulldog |
| English springer spaniel | French bulldog |
| Weimaraner | West Highland white terrier |
| Irish setter | Fox terrier |
| Soft‐coated wheaten terrier | Skye terrier |
| “Doodle” mix | |
| Soft‐coated wheaten terrier |
Urethral sphincter mechanism incompetence is the most common functional urine storage disorder in dogs and is usually, but not always, associated with alterations in sex hormones after neutering of female and male dogs. Hormonally‐related USMI is an acquired disorder, although some dogs might have congenital urethral dysfunction before neutering. Other causes of functional urine storage disorders include sacral spinal cord injury affecting the pudendal or pelvic nerves or both, and dysautonomia; these disorders are related to the spinal cord or cauda equina and are beyond the scope of this discussion. Although common in women, functional UI because of overactive bladder (OAB) or detrusor instability is difficult to definitively confirm in dogs because of limited availability of urodynamic testing (see Section 4.5). In dogs, detrusor instability probably is associated with urinary tract infections (UTI) or advanced age but because of the difficulty in diagnosis is termed idiopathic.
Mechanical causes of storage failure usually involve anatomic abnormalities caused by congenital defects or secondary to surgical modification or injury. These include EU, a short urethra resulting in a pelvic bladder, or a combination of these. A short or dilated urethra decreases the functional profile length (ie, the length of urethra where urethral pressure exceeds bladder pressure) and increases the pressure required to maintain continence. A short urethra and EU might indicate other abnormalities with the urethral sphincter mechanism that involve muscle fiber function and anatomic orientation. Thus, correction of this anatomic abnormality might not fully correct the incontinence.
Disorders of voiding are characterized by UI with a larger PVRV with or without secondary overflow UI (Table 1). Disorders of voiding are subdivided into functional and mechanical causes. Functional disorders of voiding result in inability to pass urine from the bladder to the external environment because the bladder fails to effectively contract, the urethra fails to relax, or a combination of both. The term functional outflow obstruction (FOO) has been adopted by this panel to globally characterize this functional voiding disorder when a defined central nervous system (CNS) abnormality is not identified. Mechanical outflow obstruction (MOO) results from luminal, intramural, or extramural obstruction of the urinary outflow tract. Both FOO and MOO can result in overflow UI when bladder pressure exceeds urethral pressure, which most often occurs when the dog is resting or after attempting to urinate.
4. DIAGNOSTICS
4.1. History and pattern recognition
Statement
The first step for categorizing UI into a storage or voiding disorder is to obtain a thorough history from the client as well as direct observation or video review of the dog's UI and conscious voiding behaviors. This approach also facilitates pattern recognition.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
When obtaining a history from a client (Box 2), the priority is to determine if the dog has UI or is consciously voiding. Understanding where the UI occurs in the house and making note of the dog's activities (eg, sleeping, playing) surrounding the episodes is helpful for pattern recognition. Ideally, the owner will have witnessed the UI at home and can describe its timing, frequency, and severity. Use of a motion‐activated camera could be considered to assist in the diagnosis.
BOX 2. Important history questions that should be asked when assessing a patient with urinary incontinence.
Is the dog aware of inappropriate urination (is it really incontinence?)
How long has the problem been present?
Was the problem present before neuter?
Is the dog able to urinate normally?
Is the dog able to empty its bladder completely?
Is there a change in the frequency of normal urination?
Is the dog polyuric/polydipsic?
Can the dog produce a normal urine stream?
Is the dog straining when it urinates?
Is the dog able to posture appropriately to urinate?
Does the dog have a history of neurologic disease or orthopedic/spinal pain or lameness?
Has the dog ever had fecal incontinence?
Does the dog drip urine after it voids normally?
Does the dog have any lower urinary tract signs such as pollakiuria, hematuria, or malodorous urine?
Does the dog show a sense of urgency to urinate prior to leaking urine?
For female dogs, pattern recognition delineated from the history often leads to a presumptive diagnosis, particularly for dogs with USMI (Figure 4). Disorders of storage present as involuntary leakage but the dog retains the ability to void normally. Understanding the activity associated with the UI is helpful in distinguishing USMI, EU, and detrusor instability. Female dogs with USMI most commonly experience UI when lying down or at rest because the increasing intravesicular pressure overcomes the weakened urethral sphincter mechanism. Female dogs with EU generally are juvenile and often continually leak urine, during activity and at rest, because of the anatomical position of the ureters bypassing the urethral sphincter mechanism. Detrusor instability often presents with increased frequency, dribbling urine postvoiding and difficulty retaining urine in the bladder.
FIGURE 4.
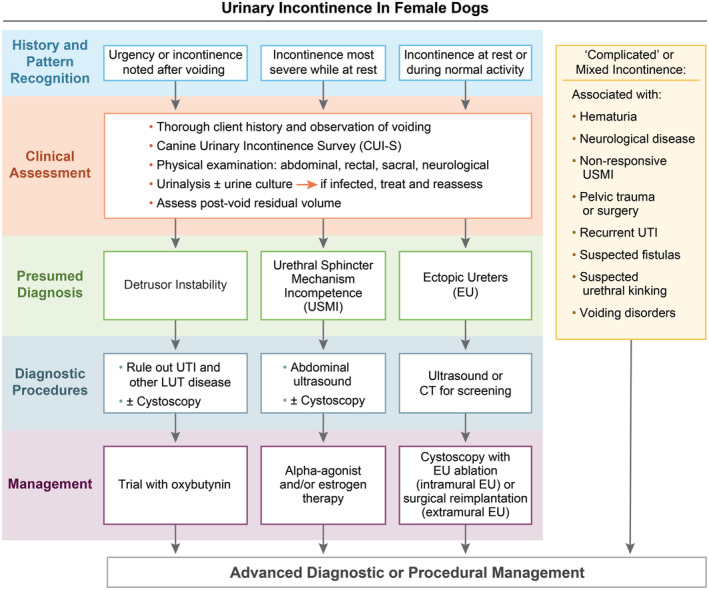
Visual aid for diagnosis and management of urinary incontinence in female dogs based on initial pattern recognition. Image adopted from the International Continence Society (ICS). Please note that the diagnosis and management should be tailored to the individual dog and the presumed diagnoses listed are not an exhaustive list.
A thorough history of voiding patterns also is warranted in male dogs, but pattern recognition is less useful in establishing a presumptive diagnosis with storage disorders because of anatomical differences in their urethral sphincter and length (Figure 5). A history of posturing with a weak, interrupted stream toward the end of urination and increased PVRV is characteristic of FOO. Stranguria with a weak or no urine stream may indicate complete obstruction, more commonly caused by MOO. Functional outflow obstruction more often causes pronounced stranguria; however, most animals still have some, although decreased, ability to generate a urine stream. Young to middle‐aged large and giant breed male dogs are most often identified with FOO and secondary overflow incontinence. 31 This disorder is likely more prevalent than USMI in males and must be ruled out before a disorder of storage is diagnosed. Male dogs can dribble urine postvoiding with both outflow obstruction and preputial abnormalities.
Statement
Subjective changes in water intake and urine volume should be noted for all UI patients because PU/PD can exacerbate UI.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
FIGURE 5.
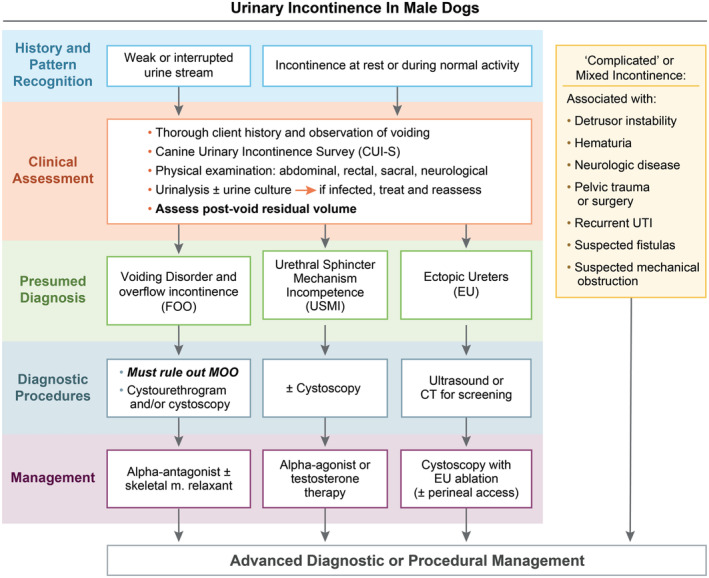
Visual aid for diagnosis and management of urinary incontinence in male dogs based on initial pattern recognition. Image adopted from the International Continence Society (ICS). Please note that pattern recognition is less reliable in male dogs, the diagnosis and management should be tailored to the individual dog, and the presumed diagnoses listed are not an exhaustive list.
Polyuria and polydipsia (PU/PD) might exacerbate UI secondary to increased urine production because the urethra must exert higher pressure to counter the increased bladder volume and pressure. Management of UI is likely to be more successful if the underlying cause of PU/PD is diagnosed and treated appropriately.
Statement
A standardized canine urinary incontinence survey (CUI‐S) is highly recommended at every visit to assess the severity and pattern of UI as well as the response to therapeutic interventions.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
Several published UI questionnaires or severity indices exist for dogs. The consensus panel combined many of these to create a single standardized survey (Supplemental Table 1).
4.2. Physical examination
In addition to obtaining a thorough history regarding the dog's urinary behavior, observing the dog urinate or viewing a video capture can be beneficial. Urine stream, presence or absence of stranguria, duration of voiding, and presence or absence of involuntary leakage of urine immediately after urinating all should be noted. Distal urethral obstruction can cause distension or pulsating of the perineal urethra, which might be observed in the perineal region during micturition. In addition, the posture and perceived discomfort of the dog should be noted. Orthopedic and neurologic disease can prevent an animal from posturing appropriately and lead to urine retention and overflow UI. Neurologic causes of UI are beyond the scope of this discussion but are provided in Supplemental Table 2.
Statement
A thorough general physical examination should be performed in all dogs with UI, including a rectal examination with urethral palpation, bladder palpation, and focused neurological examination that assesses behavior, gait, hindlimb postural reactions, spinal reflexes, tail tone and presence or absence of back pain (Figure 6).
Panel vote
12 of 12 (100%) panelists agreed with this statement.
FIGURE 6.
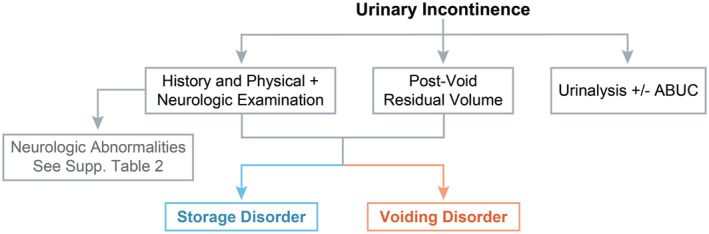
Recommended initial diagnostic steps for storage and voiding disorders. ABUC, aerobic bacterial urine culture.
In addition to watching the dog urinate, all dogs should be assessed for evidence of UI during the examination as well as urine and feces on the perineal hair. In male dogs, extrude the penis and examine the urethral orifice at the tip of the penis. The preputial opening in relation to the penis should be evaluated. A preputial opening that is too small can be associated with urination into the prepuce and urine leaking after voiding. Palpate along the length of the urethra, especially at the base of the os penis, a common site for urethral calculi. Palpation of the perineum should be performed for masses that could result in urethral obstruction. Rectal examination should be performed in all dogs regardless of age or reproductive status. The urethra can be palpated on midline, dorsal to the pubic symphysis and the prostate may be palpable cranial to the pubis. Vulvar anatomy should be inspected in female dogs, noting any evidence of perivulvar dermatitis, saliva staining, or degree of excessive perivulvar skin (ie, vulvar hooding).
The urinary bladder can be palpated in most dogs unless it is empty, or if the animal is obese or very large. Care should be taken to note the position of the urinary bladder in the abdomen, the degree of distention, the presence of pain, and if UI occurs during palpation. In dogs, the thickness of the bladder wall, and the presence of intramural masses (eg, neoplasms) or intraluminal structures (eg, calculi) should be noted. The size of the urinary bladder should be recorded prevoiding and postvoiding. Presence of a large bladder postvoiding suggests a voiding disorder, whereas a small bladder postvoiding suggests a storage disorder. A bladder that is empty may not be palpable.
A focused neurological examination should be performed including assessment of behavior, level of consciousness, cranial nerve examination, gait evaluation, postural reaction testing, and presence of spinal pain. Dogs with diffuse forebrain disease might exhibit inappropriate urination, and urge incontinence has been associated with cerebellar disease. Dysautonomia results in severe overflow UI and voiding dysfunction and often is accompanied by additional signs of autonomic dysfunction that can be detected on the neurological examination. Further information regarding neurological disorders and UI can be found in Supplemental Table 2.
In dogs without overt neurological signs on physical examination, the presence of fecal incontinence, spinal pain, or a disconnected forelimb and hindlimb gait should trigger a complete neurological examination, and ideally magnetic resonance imaging (MRI) of the spine.
4.3. Postvoiding residual volume
Statement
Postvoiding residual volume should be assessed in all dogs, especially males, presenting with UI in addition to direct observation of voiding. Increased PVRV could signify a disorder in voiding whereas normal PVRV with UI suggests a urine storage disorder (Figure 6).
Panel vote
12 of 12 (100%) panelists agreed with this statement.
Measurement of PVRV is a noninvasive tool that should be used during initial diagnostic testing to assist in categorizing the underlying causes for the dog presenting with UI (Figure 6). Techniques used to measure PVRV in dogs include urinary bladder palpation, 2‐dimensional (2D) B‐mode ultrasound (US) calculations, and 3‐dimensional (3D) US measurements. Based on recommendations in humans, dogs, and clinical experience, the following are recommended for dogs with storage and voiding disorders: a PVRV of 0.2 to 1.0 mL/kg can be considered normal for dogs, a PVRV >3 mL/kg is abnormal and signifies urine retention, and a PVRV of 1 to 3 mL/kg should be interpreted based on the signalment and other clinical signs of the dog. 32 , 33 Postvoiding residual volume should be measured within 10 minutes of voiding for accuracy and the dog should be given ample time to fully urinate outside, 34 particularly in male dogs that may not voluntarily void during a single posture and may need multiple attempts. When available, 2D B‐mode US or a 3D US (bladder scanner) should be used instead of urinary catheterization because this approach is less invasive and avoids potential catheter‐associated UTI, which has been reported in 8% to 32% of dogs. 35 , 36 , 37 , 38 When using 2D ultrasonography, the formula V = length × width × height × 0.52 has been shown to be the most accurate in both humans and dogs. 39 , 40 , 41
4.4. Urinalysis and urine culture
Statement
Urinalysis and aerobic bacterial urine culture (ABUC) should be evaluated in all dogs presented for UI and in dogs with relapsing UI (Figure 6). If urine sediment examination is suggestive for infection, an appropriately collected urine sample should be submitted for quantitative ABUC with antimicrobial susceptibility testing. Alternatively, cage‐side, rapid screening for bacteriuria could be performed and, if positive, urine should be submitted for ABUC.
Panel vote
12 of 12 (100%) panel members agreed with this statement.
The classical LUT signs of dogs with UTI include pollakiuria, stranguria, hematuria, and pain upon voiding. Associations between bacteriuria and UI (both storage and voiding disorders) have been reported in dogs 42 , 43 and in women with stress urinary incontinence, 44 a disorder that has many similarities to USMI in dogs. In most cases, bacteriuria is a result of impaired host defense mechanisms associated with the UI.
Statement
If ABUC is positive for microbial growth, antimicrobials, ideally based on susceptibility test results, should be administered to the dog for 5 days, and the dog's UI should be monitored for improvement.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
The recommended antimicrobial treatment duration is derived from published International Society for Companion Animal Infectious Diseases (ISCAID) guidelines. 45 If clinical signs persist, further diagnostic testing and use of CUI‐S are recommended to determine the underlying cause for the UI. 46
Statement
A urinalysis and ABUC should be evaluated in all dogs before interventional urinary procedures. If the urinalysis results are consistent with infection or the ABUC is positive for bacterial growth, antimicrobials should be administered for a period of 24 hours before or at the time of anesthesia induction. Post‐procedure antibiotics should be tailored to the dog, procedure, and clinical signs.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
The ISCAID working group recommends that most dogs with subclinical bacteriuria not be given antimicrobials 45 except before interventional urinary procedures or diagnostic testing. Ideally, a negative urine culture is documented before referral or before the evaluation for an interventional procedure. In extenuating circumstances, a urinalysis alone can be acceptable, considering the risk of false negative results.
4.5. Urodynamic testing
Statement
Urodynamic studies are not considered necessary in dogs that initially present for voiding or storage disorders but might provide further information regarding the cause of UI in refractory cases.
Panel vote
12 of 12 (100%) panelists agreed with this statement.
Urodynamic testing, including urethral pressure profile (UPP), cystometrogram (CMG), leak point pressure (LPP), electromyography (EMG), or a combination of these studies can be considered for dogs with UI. Diagnosis of the most common storage disorder in dogs, USMI, usually is established based on appropriate signalment, history, absence of abnormalities on physical examination, and response to appropriate therapeutic drug trials. However, if concurrent disorders are present (eg, EU), a UPP/CMG can be considered. Data suggests these studies might help identify concurrent functional abnormalities of the urinary bladder and urethra in dogs with EU and might help predict postoperative outcome. 47 , 48
Cystometry can be considered to evaluate bladder threshold volume, pressure, and compliance in animals suspected of having detrusor muscle abnormalities such as detrusor instability. 49 As the bladder fills, the rate of pressure increase accelerates in several stages, leading to spontaneous or intentional voiding. Alterations in this pattern might indicate decreased compliance (increased stiffness) of a diseased bladder or a problem with pelvic nerve transmission. Before CMG, a urine culture should be obtained and treatment with proper antimicrobials administered if the culture is positive for growth.
The type of urodynamic equipment and protocols must be standardized to gain the most accurate information and for proper interpretation. Protocols for performing these diagnostic tests, including anesthetic regimens and bladder fill rates, are beyond the scope of this discussion. 50 All anesthetic agents will alter (usually decrease) the maximum urethral closure pressure (MUCP) and the capability for the dog to have a normal detrusor reflex during a CMG. 51 , 52 , 53 Urodynamic studies might provide further information regarding the cause for refractory UI, which could alter treatment. However, these diagnostic tests are not always practical because of limited availability and the standardized anesthetic regimens required to perform them.
4.6. Diagnostic imaging
Diagnostic imaging provides a global overview of urogenital anatomy, identifies conditions that may be relevant to UI, and can identify comorbidities that might impact the treatment and prognosis of the dog. The primary imaging modalities utilized are radiography (survey and contrast radiography), fluoroscopy, ultrasonography (US), and computed tomography (CT). Radiography and fluoroscopy are similar in their applications, but radiography provides better spatial resolution and fluoroscopy demonstrates in real‐time the anatomy, pathology, and visualization of dynamic processes. Although MRI is the most useful modality when a neurologic cause of UI is suspected, other less expensive, more accessible imaging modalities are used to assess the lower urinary tract (LUT).
Statement
Evaluation of survey abdominal radiographs (including the entire urethra) may be considered during initial presentation for a voiding disorder.
Panel vote
12 of 12 panelists (100%) agreed with this statement.
Survey radiography is critical to exclude mechanical voiding disorders such as uroliths (including urate and cystine calculi) in many instances, 54 mineralized mural lesions of the lower urinary tract, or lesions of the os penis. 55 , 56 , 57 Radiographs also are useful to note bladder position. Radiographs should include the entirety of the pelvis and perineum, and in male dogs the pelvis and pelvic limbs should be extended cranially to expose more of the penile urethra. 58 A radiolucent implement (eg, wooden spoon) can be used to compress the abdomen, displacing viscera from the urinary tract and decreasing tissue thickness to increase the likelihood of identifying uroliths. 59
Statement
Retrograde urography (cystourethrography in male dogs or both vaginourethrography and cystourethrography in female dogs) with or without concurrent cystoscopy is recommended for dogs suspected to have voiding disorders.
Panel vote
10 of 10 (100%; 8 SAIM diplomates, CA, and GO) panelists agreed with this statement.
Retrograde positive contrast studies help to outline the bladder, urethra, vagina, and vestibule, and in some instances the distal portions of the ureters. Retrograde urography provides information about the lower urinary tract and is recommended if short urethra, 60 , 61 bladder hypoplasia, 62 , 63 patent urachus or vesicourachal diverticula, 63 , 64 , 65 fistulae (ureterovaginal, vesicovaginal, urethrovaginal, urethrorectal), 61 , 66 vestibulovaginal stenosis or septal remnants, 67 , 68 urethral strictures or mural lesions, 58 or caudal sliding of the bladder 69 are suspected. Furthermore, elimination of these differential diagnoses can be used as support for a diagnosis of idiopathic FOO. Ultimately, retrograde positive contrast studies are recommended in conjunction with cystoscopy.
Retrograde urography requires use of a standardized protocol, with particular attention given to the extent of urinary bladder distension. For females, a cystourethrogram is performed using catheterization to fill the bladder and then manual compression of the bladder to fill the urethra once the catheter is withdrawn. Maximal bladder distension is recommended in all instances but particularly when surveying for short urethra, bladder hypoplasia, and urethral lesions. Normal urinary bladder capacity in dogs is approximately 10 mL/kg. However, manual palpation during infusion of contrast medium or direct visualization during video fluoroscopy should be used to determine when maximal distension has been achieved.
Contrast studies have been utilized for diagnosis of pelvic bladder and bladder hypoplasia, both storage disorders, although their relationship to UI is unknown. Pelvic bladder is defined as a bladder neck caudal to the pubic brim at maximal distension. 67 In female dogs, pelvic bladders are associated with shorter urethras, 67 , 70 but this association has not been demonstrated in male dogs. 71 Although significant associations between pelvic bladder and UI in female and male dogs have been identified, it is important to note that pelvic bladders can be found in continent dogs. 67 , 71 , 72 , 73 , 74 , 75 Bladder position alone is only 68% specific and 76% sensitive in female dogs and 75% specific and 65% sensitive in male dogs in predicting UI. 71 , 75 It therefore is recommended to investigate for a pelvic bladder in the diagnostic evaluation of UI but equally important to investigate other causes of UI (eg, USMI) even if a pelvic bladder is identified.
Bladder hypoplasia or fibrosis are uncommon conditions that are defined radiographically by identifying a bladder that requires only a small amount of contrast to reach maximal distension. Additional anomalies often coexist with these conditions, and other causes of UI should be investigated if bladder hypoplasia or fibrosis is diagnosed. 62 , 63
Statement
Abdominal ultrasonography (US) is a reasonable non‐invasive imaging modality for screening dogs suspected of having EU before cystoscopy and can identify upper urinary tract comorbidities.
Panel vote
10 of 10 panelists (100%; 8 SAIM diplomates, CA, and GO) agreed with this statement.
Abdominal US has good sensitivity and specificity (sensitivities of 87.8%‐93.6% and specificities of 86.2%‐100% relative to cystoscopy 76 ) for detecting EU and does not require ionizing radiation, but US infrequently determines the location of the ureteral entrance into the urogenital tract. 76 , 77 Confidence in the diagnosis of EU can be increased by administration of furosemide because it will increase the likelihood of identifying ureterovesicular junctions by increasing ureteral diameter, ureteral peristalsis, and urine jet production (Figure 7). 76 , 78 , 79 Ultrasonography also is excellent for assessing the remainder of the urogenital tract such as the kidneys (eg, renal dysplasia that can occur with EU), excluding those components obscured by the pelvis. Because the sensitivity of US is lower than cystoscopy, cystoscopy still should be pursued if pattern recognition is consistent with EU because it cannot be entirely ruled out based on US, and the possibility of misdiagnosis of intra vs extramural EU exists.
Statement
Cystoscopy and CT are the most sensitive and specific imaging modalities for establishing a diagnosis of EU. However, cystoscopy is more sensitive and definitive, and allows for ablation of intramural ectopic ureters when present and is, therefore, the preferred modality.
Panel vote
10 of 10 (100%; 8 SAIM diplomates, CA, and GO) panelists agreed with this statement.
FIGURE 7.
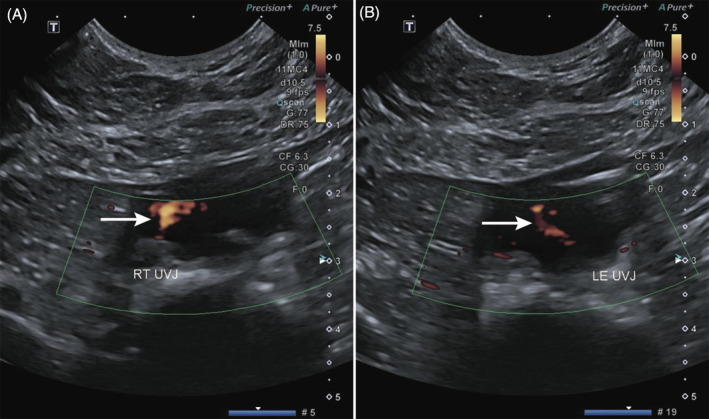
Doppler color flow indicating urine jets from right (A) and left (B) ureteral vesicular junctions (UVJ) using 2D B‐mode ultrasound. LE, left; RT, right.
Computed tomography can be used with excretory urography or retrograde urography to yield similar information as described with radiography and has the advantage of circumventing anatomic superimposition, which is particularly relevant for EU. Strong agreement has been demonstrated between CT and cystoscopic, surgical, or necropsy diagnosis of EU (with sensitivity of 73%‐100% and specificity of 90.2%‐100%) and CT outperformed radiographic or fluoroscopic excretory urography. 80 , 81 , 82 Furthermore, CT provides a detailed overview of urogenital anatomy and can disclose potential comorbidities of EU (such as renal agenesis, pyelonephritis, or ureteral duplication). However, CT is less sensitive than cystoscopy in diagnosing EU and certain important features of EU (eg, intra vs extramural course, ureteral troughs, ureteral fenestrations, branched ureters), that are evident by cystoscopy and cannot be identified by any imaging modality. Therefore, cystoscopy is the preferred technique for establishing a definitive diagnosis of EU. Moreover, once an intramural EU is identified by cystoscopy, laser or cautery ablation can be performed during the same procedure.
4.7. Endourology
Statement
Cystoscopy is recommended to confirm the presence or absence of EU but also can be considered for dogs with refractory storage disorders to evaluate the anatomy of the LUT and facilitate interventional treatment such as administration of urethral bulking agents or ablation of EU.
Panel vote
10 of 10 panelists (100%; 8 SAIM diplomates, CA, and GO) agreed with this statement.
In cases of storage disorders that are refractory to medical management, cystoscopy is recommended to evaluate the anatomy of the LUT and confirm the presence or absence of EU. If intramural EU are diagnosed during cystoscopy, laser or electrocautery ablation of the intramural ectopic ureter can be performed during the same procedure. 83 , 84 , 85 Also during cystoscopy, anatomy of the urethra and vaginal vestibule are evaluated.
Statement
A causal relationship between vestibular vaginal septal remnants (VVSR) and UI has not been established but these remnants should be ablated during cystoscopy whenever possible.
Panel vote
10 of 10 panelists (100%; 8 SAIM diplomates, CA, and GO) agreed with this statement.
Many dogs with EU have an abnormality of the vaginal vestibule called a VVSR which is a broad tissue band dividing the vaginal opening into 2 parts and lifting the urethral opening dorsally (Figure 8). 86 The VVSR should be corrected by laser or electrocautery ablation at the time of ectopic ureter correction. 86 These bands also have been noted in dogs without EU or UI and therefore the causal relationship between VVSR and UI has not been established.
Statement
Before treatment with testosterone, flexible cystoscopy should be considered in the diagnostic evaluation of male dogs with storage disorders that have failed to respond to phenylpropanolamine (PPA).
Panel vote
9 of 10 panelists (90%; 8 SAIM diplomates, CA, and GO) agreed with this statement.
FIGURE 8.
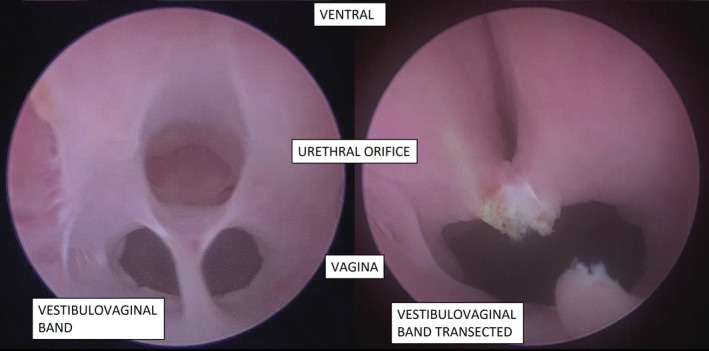
Cystoscopic image of vestibulovaginal band or vestibulovaginal septal remnant (VVSR) before and after transection. Please note the position and confirmation of the external urethral orifice before and after transection.
Cystoscopy can confirm if LUT anatomy is normal in addition to evaluating the urethra for any causes of partial mechanical urethral obstruction before initiating testosterone treatment.
A full review of treatments for both storage and voiding disorders is presented in Figures 9 and 10. For differences in male and female dogs, please refer to Figures 4 and 5. Use of these diagnostic tests should be tailored to the individual dog, financial constraints of the owner, and availability of the various diagnostic test procedures available.
FIGURE 9.
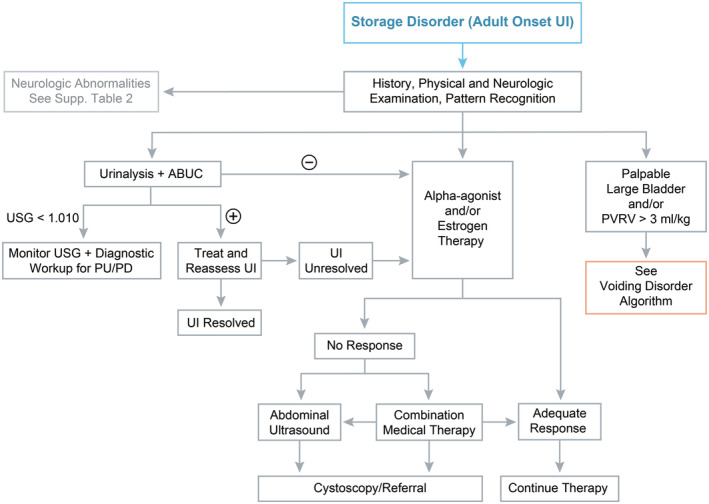
Flow diagram depicting diagnostic steps for urinary incontinence due to a disorder in urine storage. Please note, that dogs presenting with urinary incontinence since birth should be investigated for ectopic ureters (EU) prior to following this flow diagram. The ⊕ symbol refers to positive growth on ABUC. ABUC, aerobic bacterial urine culture; LUT, lower urinary tract; PU/PD, polyuria/polydipsia; PVRV, post void residual volume; UI, urinary incontinence; USG, urine specific gravity.
FIGURE 10.
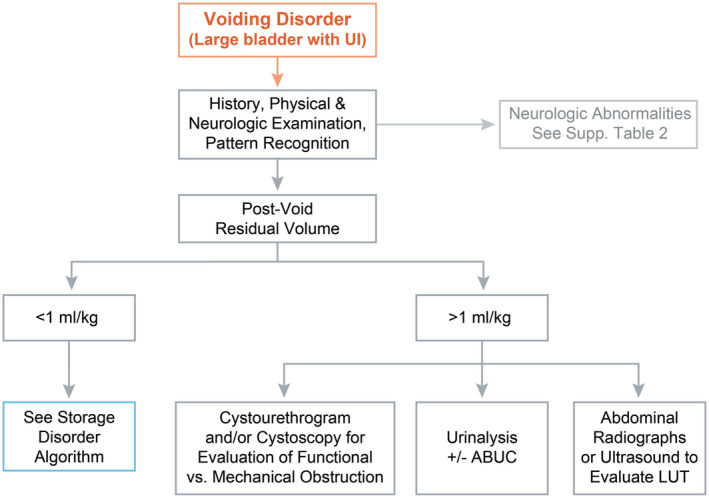
Flow diagram depicting diagnostic steps for urinary incontinence due to a disorder in voiding. Please note that the diagnostic options for an increased postvoid residual volume should be tailored to the individual dog and pattern recognition. ABUC, aerobic bacterial urine culture; UI, urinary incontinence.
5. TREATMENT
Treatment of UI in the dog should be tailored to storage vs voiding disorders and the underlying cause. If a thorough diagnostic evaluation fails to provide a definitive diagnosis, a treatment trial can be initiated and response recorded. This section describes medical, interventional, and surgical treatment options for the most common causes of storage and voiding disorders in dogs.
5.1. Treatment of storage disorders
5.1.1. Urethral sphincter mechanism incompetence
Medical management of USMI
Statement
An alpha‐agonist (eg, PPA) or administration of estrogen compounds (eg, diethylstilbestrol, estriol) is recommended as the initial treatment for USMI in female dogs. An alpha‐agonist (PPA) is recommended as the initial treatment for USMI in male dogs.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Alpha‐agonists stimulate the adrenergic receptors of the internal urethral sphincter whereas estrogens may upregulate expression of such receptors as well as have trophic effects on the urethral sphincter mechanism (Table 2). Consensus by the panel is that either may be used as a first‐line treatment in female dogs, with attention to the impact of potential adverse effects in individual dogs. Although direct comparisons of treatment efficacy between PPA and estrogens for treatment of USMI have not been performed, 8 of 8 panelists (100%; 8 SAIM diplomates) choose PPA as initial treatment. A minimum of 28 days is recommended to assess response to treatment with PPA. 87 In dogs that do not respond to PPA, 6 of 8 panelists (75% of SAIM diplomates) choose estriol as their next treatment of choice and 2 of 8 panelists choose diethylstilbestrol. A single study showed no evidence of synergistic activity between PPA and estrogens, but anecdotal experience suggests there may be a benefit for some dogs that do not respond to either drug alone or the combination may decrease the dosage of either drug alone. 88
TABLE 2.
Summary of medications, doses, and potential adverse effects for treating storage disorders.
| Drug | Class | Mechanism of action | Indication | Dose | Potential adverse effects |
|---|---|---|---|---|---|
| Phenylpropanolamine | α‐Agonist | Direct stimulation of α and some β receptors | USMI | 2 mg/kg PO q8‐12h | Hypertension, restlessness, GI effects |
| Estriol | Estrogen | Binds to estrogen receptors within sphincter cells resulting in increased responsiveness to norepinephrine. May also sensitize the urethral sphincter to α‐adrenergic stimulation | USMI (females) | 2 mg/dog PO q24h × 14 days, then reduce to 1 mg q24h | Attractiveness to males, mammary/vulvar swelling, behavioral changes |
| Diethylstilbestrol | Estrogen | Binds to estrogen receptors within sphincter cells resulting in increased responsiveness to norepinephrine. May also sensitize the urethral sphincter to α‐adrenergic stimulation | USMI (females) | 0.1‐1 mg/dog PO q24h for 3–5 days then weekly or as needed | Myelosuppression (rare at these doses), attractiveness to males, mammary/vulvar swelling, behavioral changes |
| Testosterone cypionate | Androgen | Exact mechanism unknown. Suspected to maintain tone of urethra and bladder smooth muscle. May also cause hypertrophy of the prostate, which increases urethral resistance | USMI (males) | 2.2 mg/kg IM q4‐8 weeks | Behavior changes, aggression, perianal adenoma, prostatic hyperplasia |
| Methyltestosterone | Androgen | Exact mechanism unknown. Suspected to maintain tone of urethra and bladder smooth muscle. May also cause hypertrophy of the prostate, which increases urethral resistance | USMI (males) | 0.5 mg/kg PO q24h; if effective, recommend change to testosterone cypionate | Behavior changes, aggression, perianal adenoma, prostatic hyperplasia |
| Oxybutynin | Antimuscarinic, antispasmodic | Antagonization of parasympathetic control of the bladder, reducing the frequency of contractions | Detrusor instability | 0.2‐0.3 mg/kg q8‐12h | GI effects, urine retention, hypersalivation, sedation |
Abbreviations: α, alpha‐adrenergic receptors; β, beta‐adrenergic receptors; GI, gastrointestinal; h, hours; IM, intramuscular; PO, per os; q, every; USMI, urethral sphincter mechanism incompetence.
Adverse effects of estrogen treatment can include mammary and vulvar swelling, uterine stump enlargement and attractiveness to male dogs. These adverse effects are often dose‐dependent and emphasize the need for individual dose management. There also are reports of bone marrow suppression secondary to estrogen use in dogs, but these events occurred primarily with estradiol cypionate or high‐dose diethylstilbestrol. 89 The adverse effects of PPA (eg, aggression, hyporexia, hypertension) and estriol generally resolve when the medication is decreased or stopped.
The use of estrogen in prepubertal intact females is controversial. The panel advises against such treatment because of potential risk of developing uterine enlargement or pyometra, although clear evidence implicating estrogen is lacking. In a case series, 50% of the 14 dogs receiving estriol had vulvar changes reported on their physical examinations, but only 3 of 14 (21%) had uterine stump abnormalities mentioned on the ultrasonographic reports. 90 Routine screening, including vaginoscopy and ultrasonography, usually is not indicated for dogs receiving estriol, but can be tailored to the individual dog. No dogs had any clinical consequences because of the abnormalities noted on physical examination or ultrasonographic findings. 90
Statement
Treatment with testosterone is recommended for castrated male dogs with USMI that are refractory to PPA.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
For male dogs that do not respond to PPA, the diagnostic evaluation (including PVRV) for a voiding disorder should be repeated. If PVRV is normal and other storage disorders such as EU have been excluded, treatment with injectable testosterone cypionate or PO methyltestosterone is recommended (Table 2). In a small study evaluating 8 male dogs with USMI, treatment with 1.5 mg/kg testosterone cypionate IM every 4 weeks resulted in a good to excellent response in 3 dogs and a slight response in 1 dog. 91 A poor response was noted in the other dogs but no adverse effects were reported, suggesting this treatment might be an option for male dogs with USMI.
Statement
Ideally, systolic blood pressure should be measured both before initiating and periodically during administration of PPA because hypertension is a potential, albeit uncommon, adverse effect of alpha agonists.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Phenylpropanolamine causes norepinephrine release 92 but also inhibits norepinephrine reuptake by nerve endings. 93 It is a nonselective α‐agonist and therefore has the potential to increase systemic blood pressure because of an increase in total peripheral resistance. Hypertension, tachycardia, restlessness, aggression, decreased appetite, and insomnia have been reported as adverse effects in dogs treated with PPA. In a prospective, cross‐over, double‐blinded study evaluating PPA in 7 healthy beagle dogs, significant increases in systolic, diastolic, and mean blood pressure occurred in dogs that received 2 and 4 mg/kg of PPA. No significant increase in blood pressure was noted at 1 mg/kg in this 7‐day study. A significant decrease in heart rate was noted in all groups that received PPA, but not in the placebo group. The maximal increase in blood pressure was documented 2 hours after administration of 2 mg PPA/kg with an average increase in systolic blood pressure of 8.0 mm Hg. 94 Estrogen compounds should be considered as first‐line treatment in dogs with documented hypertension and could be used for dogs with comorbidities that predispose to hypertension. If alpha agonists are administered to these dogs, blood pressure should be monitored more often.
Interventional and surgical procedures for USMI
Urethral bulking agents
Options for dogs that have medically‐unresponsive USMI, normal cystoscopy, and negative bacterial urine culture include surgical procedures, urethral bulking, stem cell therapy, and placement of hydraulic urethral sphincter or transobturator vaginal tape (see Section 5.1.1 for a discussion of surgical procedures).
Statement
Urethral bulking agents or surgical placement of an artificial urethral sphincter should be considered for dogs that are found to be refractory to all medical management and have undergone cystoscopy.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Urethral bulking involves cystoscopically injecting a bulking agent submucosally in the proximal urethra. Currently, a single veterinary urethral bulking agent is available in the United States, an insoluble crosslinked collagen product (ReGain; Avalon Medical, Stillwater, MN). Over 80% of dogs achieve continence with bulking agents but incontinence recurs in many dogs within 1 year. 95
Other bulking agents used in humans include calcium dextranomer/hyaluronic acid copolymer, polydimethylsiloxane, and hydroxyapatite. Although studies in dogs have been promising, none of these products currently is available for use in veterinary medicine. Dextranomer/hyaluronic acid copolymer used in dogs resulted in a mean duration of continence of 20.5 months (range, 12‐48 months) with a 58% success rate at 6 months. 96 Polydimethylsiloxane resulted in 21 of 22 dogs becoming continent and 1 dog exhibiting improved continence, 8 dogs requiring retreatment between 3 and 8 months, an overall continence rate of 91% at 12 months, and 80% of dogs remaining continent at 2 years. 97 No data exists for the use of hydroxyapatite in dogs.
Autologous skeletal muscle progenitor cells also have been evaluated in dogs in 3 studies, 1 involving client‐owned dogs with USMI and 2 involving an experimental model of USMI in dogs. The clinical study involved injecting 100 million cells per milliliter into 15 client‐owned dogs with USMI and resulted in improvement in median continence scores at 3, 6, 12, and 24 months. Thirteen of the 15 dogs had complete continence with additional medical treatment. Therefore, skeletal muscle progenitor cells may be a useful adjunct with medical treatment to achieve continence in female dogs with USMI, but currently the treatment is technically challenging, time‐consuming, and not widely available. 98
Panelists were divided between recommending urethral bulking agents vs surgical procedures as the first line treatment in female dogs with refractory USMI. The primary determining factor for decision making was the age of the dog. For older female dogs that are refractory to treatment, the consensus panel recommends injectable bulking agents. Although bulking agents can have a limited duration of effect, they could be appropriate for this population. However, the panelists have found that bulking agent injections are not as successful or durable in dogs with concurrent anatomical anomalies such as a short or dilated urethra or EU. Bulking agents are most effective in urethral coaptation in dogs with anatomically normal urethral lumens (eg, acquired USMI). Placement of an artificial urethral sphincter has been found to be the most successful long‐term treatment option, and might be considered more often for young dogs with USMI that are refractory to medical management and in those with EU that have persistent UI despite repositioning of the ureteral opening to the bladder.
Artificial urethral sphincter
Surgical procedures can be used in male and female dogs that have functional storage disorders (USMI) or persistent UI after anatomical correction of EU. Before 2004, colposuspension was the most commonly reported technique to treat UI in female dogs. This technique involves placing sutures from the vagina to the prepubic tendon to apply cranial traction on the urogenital tract, effectively lengthening and compressing the urethra. Although relatively high success rates were achieved in female dogs during the first 2 months after surgery, continence rates decreased to 50% after 6 months and 12% at 1 year. 99 , 100 In male dogs, analogous approaches to the repositioning of the lower urinary tract using vas deferentopexy and prostatopexy had limited success. 101 , 102
In the last 2 decades, the majority of reports in both male and female dogs have focused on the use of a permanent artificial urethral sphincter (AUS)—a percutaneously‐adjustable hydraulic cuff that is placed around the urethra through a caudal midline abdominal approach. 103 , 104 , 105 , 106 , 107 , 108 , 109 , 110 , 111 Good to excellent continence (score of ≥8 out of 10) was documented in 82% to 92% of dogs after placement of the AUS, 103 , 105 , 109 , 110 with the maintenance of improved continence extending as long as follow‐up was performed (2‐3 years). 105 , 110 , 111 Aside from the inherent invasiveness of open surgery, clients should be advised that the AUS implant requires follow‐up visits for adjustments of the device. Potential complications include lower urinary obstruction because of the development of an extraluminal urethral stricture that requires device removal in 0% to 17% of dogs 103 , 105 , 108 , 109 and, in others, urethral balloon dilation. 103 Urethral sling procedures, which are now the standard approach in women, have been reported in a limited number of female dogs and may offer another durable treatment in the future, although the procedure requires specialized training and the initial continence rates were lower than described for the AUS in a single long‐term study. 112 , 113 , 114
Surgical implants enhance the risk of postoperative infections by enabling the formation of bacterial biofilm. Although the diagnosis of classical implant‐associated infection is rare after application of the AUS in dogs, occult infections may be a problem because the device is extraluminal and not exposed to the dog's urine. A recent retrospective study showed that 6 of 6 dogs that developed urethral strictures at the site of AUS implantation had evidence of bacterial contamination based on positive cultures of either the fibrous tissue around the implant or the implant itself. 115 In another study, 39% of explanted AUS devices from people had evidence of subclinical bacterial contamination. 116 Based on the available information, the consensus group recommends IV administration of a first‐generation cephalosporin within 20 minutes of induction of anesthesia. There is no evidence to support postoperative antimicrobial administration in the absence of documented bacteriuria. Such AUS implant‐associated infections are rare and can involve either the SC port or the hydraulic urethral sphincter. The approach to infected implants follows general principles used in both human and veterinary surgery, including removal of the affected device and antimicrobial treatment based on culture and susceptibility results. 117 When indicated, a new device can be placed after a washout period. Most dogs continue to experience improved continence after removal of the AUS, especially with the addition of PPA or estriol treatment. 109 , 115
Failure to achieve continence after inflation of the AUS can be caused by manufacturing defects, damage to the balloon or tubing, kinks in the access tubing, placement of an oversized device, or urethral atrophy or other anatomic anomalies. 117 Because of the collapsible silicone tubing that is used in the AUS for dogs and incorporation of air bubbles into the system during surgical implantation, it often is impossible to aspirate the full volume of saline solution that has been injected into the device. 118 Although rare, when mechanical failure of the AUS is suspected, contrast injection under fluoroscopic guidance is the most accurate method to detect leakage from the device and identify any mechanical kinking of the access tubing. 118 The AUS is emptied and then injected with sterile iodinated contrast medium to the total filling volume (typically 1‐4 mL).
5.1.2. Ectopic ureters
No successful medical management for treatment of EU is available. Ablation is the treatment of choice for intramural EU whereas surgical reimplantation is required for extramural EU, although this surgical treatment is beyond the scope of this discussion because of the rarity of extramural EU (<5%). 119
Interventional procedures for EU
Statement
Cystoscopic EU ablation is the preferred treatment modality for dogs (male and female) with intramural EU. Dogs for which EU is the most likely diagnosis should be evaluated by cystoscopy at a facility that can ablate the EU during the same procedure.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Cystoscopic‐guided ablation of EU (CA‐EU) can be performed using a diode laser, holmium YAG laser, or electrocautery. 83 , 84 , 85 , 120 , 121 , 122 Multiple studies comparing outcomes between CA‐EU and open surgical correction of EU are not available. In a retrospective study, there were fewer complications and less recurrence of UI in dogs treated using CA‐EU compared to neoureterostomy. 121 Urinary continence after CA‐EU is variably reported from 47% to 72% without additional medical management. 83 , 84 Medical management for concurrent USMI, injection of bulking agents, or AUS placement after CA‐EU further increased continence rates to 77% to 82%. 83 , 84 , 85 Concurrent USMI is estimated to occur in approximately 47% to 67% of female dogs with EU. 47 , 83 , 84
In some dogs, confirmation of an intramural EU can be challenging and may require a retrograde contrast ureterogram with concurrent cystoscopy and fluoroscopy. Although some hospitals routinely perform retrograde contrast ureterography during CA‐EU, doing so is not required. The consensus panel was divided between using fluoroscopy (5 of 8 SAIM diplomates) or visual inspection (3 of 8 SAIM diplomates) during CA‐EU, the individual decision based on availability and experience. Placement of an open‐ended ureteral catheter over a flexible urologic guide wire into the ureteral lumen facilitates identification of the path of the ureter and provides additional safety during ablation of the wall between the urethral lumen and parallel ureteral lumen. Cystoscopic ablation of ectopic ureters should be performed to move the new ureteral orifice to a location approximately 1 to 2 cm within the urinary bladder. Failing to move the ureteral orifice into the urinary bladder is a relatively common reason for continued UI. For this reason, individuals without extensive endourologic experience generally should refrain from performing CA‐EU to avoid unnecessary additional expense and repeat anesthetic events.
In male dogs, CA‐EU resolved UI in 4 of 4 male dogs. 123 Although larger studies are not available to evaluate outcomes in male dogs, concurrent USMI appears to be less common in male dogs compared to female dogs with EU. Therefore, male dogs managed by CA‐EU may have a higher success rate for establishing continence compared with female dogs. In male dogs, CA‐EU may be performed transurethrally using a flexible ureteroscope and laser ablation 123 or via temporary percutaneous perineal access using a rigid cystoscope and laser or electrocautery ablation. 124
Extramural EU must be surgically corrected by transection of the ureter distally and implantation of the ureter into the urinary bladder (ie, neoureterostomy).
5.1.3. Detrusor instability
Medical management for detrusor instability
Statement
A therapeutic trial of oxybutynin is suggested for dogs that have not responded to standard USMI treatment and have a urination pattern consistent with detrusor instability.
Panel vote
9 of 10 panelists (90%) agreed with this statement.
Medical treatment of suspected detrusor instability generally involves antimuscarinic medications (Table 2). Oxybutynin, a broad antimuscarinic, is most widely used although its effectiveness on detrusor relaxation is not well reported. 125 Because documentation of detrusor instability via CMG is challenging as a result of limited availability, empirical treatment with oxybutynin and continued monitoring of the clinical signs is reasonable.
5.2. Treatment of voiding disorders
5.2.1. Functional outflow obstruction
Thoracolumbar spinal cord dysfunction and other neurological disorders may lead to lack of inhibition of the pudendal and hypogastric nerves and result in voiding disorders, especially in male dogs. Clinical signs usually are characterized by stranguria, inability to urinate, large PVRV, bladder atony, overflow UI, or a combination of these signs. 7 Treatment for these dogs requires appropriate medical intervention and efforts to keep the urinary bladder small by intermittent urinary catheterization, which is preferred over an indwelling urinary catheter. 35 Adjunct medical management also may be required.
Idiopathic FOO, formerly known as reflex dyssynergia or detrusor urethral dyssynergia (DUD), also can occur. 31 , 126 , 127 The latter 2 terms are discouraged because DUD specifically describes functional urethral obstruction resulting from CNS disease in humans 128 and a definitive diagnosis of DUD requires urodynamic testing. 128 Because urodynamic studies are not widely available and can be challenging to perform and interpret (see Section 4.5), the term FOO is recommended until further information regarding the etiology of this disease is determined. Idiopathic FOO occurs most commonly in large breed, middle‐aged, male (neutered or intact) dogs. 31 , 126 Dyssynergic voiding patterns might be observed in which a relatively normal urine stream is initiated that rapidly becomes attenuated or tapered to intermittent spurts and is accompanied by increased PVRV. 129 To diagnose FOO, mechanical causes for outflow obstruction (eg, urethroliths, mass lesions) must be excluded by cystourethrogram or cystoscopy. Referral to a neurologist should be considered if overt neurological deficits or spinal pain are noted, especially in female dogs.
Statement
The recommended initial treatment in dogs with FOO is administration of an alpha‐antagonist with or without a skeletal muscle relaxant. Alterations in drug dosing with or without urinary diversion procedures are recommended for dogs with FOO. Response to treatment should be based on client communications (ideally utilizing a CUI‐S), visualization of improving urine stream, and decrease in PVRV.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Increased sympathetic or somatic tone or a combination is considered when recommending treatment for presumed FOO. Therefore, the most common management includes alpha‐antagonists and skeletal muscle relaxants (Table 3). Localization of FOO to the smooth or striated muscle sphincter can be determined by evaluating response to treatment. It is recommended to begin treatment with smooth muscle relaxants considering the musculature of the male dog urethra. Treatment using an alpha‐antagonist, either prazosin or tamsulosin, should be initiated. Six of 8 (75%) SAIM panelists recommended the use of tamsulosin because of its wide safety margin and anecdotally better outcomes. Combined treatment with a skeletal muscle relaxant, either diazepam or alprazolam, is recommended initially or if initial response to an alpha‐antagonist alone is poor. Six of 8 (63%) panelists recommended use of diazepam because of clinical experience and positive response. 130
Statement
For dogs diagnosed with FOOD and without chronic bladder over‐distention, additional medications to increase bladder contractility (eg, parasympathomimetics) can be administered, however efficacy of these agents has not been established.
Panel vote
9 of 10 panelists (90%) agreed with this statement.
TABLE 3.
Summary of medications, doses, and potential adverse effects for treating voiding disorders.
| Drug | Class | Mechanism of action | Indication | Dose | Potential adverse effects |
|---|---|---|---|---|---|
| Tamsulosin hydrochloride | α‐Antagonist | Smooth muscle relaxant | FOO | 0.4‐0.8 mg (400 mcg)/dog, PO, q 24 h; escalation of dose and to q 12‐8 h has been anecdotally recommended | Hypotension |
| Prazosin | α‐Antagonist | Smooth muscle relaxant | FOO | 0.5‐3 mg/dog PO q8‐12h | Hypotension, weakness, syncope, GI upset |
| Phenoxybenzamine | α‐Antagonist | Smooth muscle relaxant | FOO | 0.5 mg/kg/day, PO, used daily or divided into twice daily | Hypotension, tachycardia, weakness |
| Diazepam | Benzodiazepine | Skeletal muscle relaxant | FOO | 0.04‐0.8 mg/kg/day, PO, divided q8‐12h; recommended 30 minutes prior to a walk | Sedation, ataxia |
| Lorazepam | Benzodiazepine | Skeletal muscle relaxant | FOO | 0.02‐0.2 mg/kg PO q8‐12h | Sedation, behavior changes |
| Acepromazine | Phenothiazine derivative | Skeletal muscle relaxant | FOO | 0.5‐2.2 mg/kg PO q6‐8h | Sedation, hypotension |
| Dantrolene sodium | Postsynaptic muscle relaxant | Skeletal muscle relaxant | FOO | 1‐2.7 mg/kg/day, PO, divided q8‐12h | Sedation, weakness, hepatotoxicity |
| Alprazolam | Benzodiazepine | Skeletal muscle relaxant | FOO | 0.02‐0.1 mg/kg, PO, q 12 h | Sedation, increased appetite |
| Bethanechol | Cholinergic—muscarinic | Stimulates detrusor contraction via stimulation of postganglionic parasympathetic receptors | Detrusor atony | 2.5‐25 mg/dog PO q8‐24h | Diarrhea, salivation |
Abbreviations: α, alpha‐adrenergic receptors; β, beta‐adrenergic receptors; FOO, functional outflow obstruction; GI, gastrointestinal; h, hours; PO, per os; q, every.
Parasympathomimetic drugs can be considered if secondary bladder atony, evidenced by high PVRV in the presence of urethral relaxation, is present. However, these drugs have unknown efficacy, and adverse effects (most commonly diarrhea) can prohibit long‐term use (Table 3). Anti‐inflammatory drugs and glucocorticoids have been prescribed anecdotally, but the working group does not recommend these medications for this disease unless secondary urethral inflammation, pain associated with urinary catheterizations, or pain during posturing is noted. In a retrospective study, bacteriuria was observed in several dogs with FOO but none of the dogs had resolution of their stranguria after appropriate antimicrobial treatment. 131 Antimicrobials could be considered at the initial presentation if bacteriuria is noted and suspected to be contributing to clinical signs, and the clinician should monitor for clinical improvement of the voiding disorder. If no improvement is observed, long‐term antimicrobials likely is not warranted.
Controlled trials and a standardized outcome score are necessary before further recommendations can be made. For dogs with intermittent episodes or known anxiety, anxiolytics are recommended although published evidence supporting their use is lacking.
For dogs that are refractory to medical management of FOO, intermittent urinary catheterization or tube cystostomy catheters could be considered. Urethral balloon dilation was unsuccessful in improving 1 dog's clinical signs. 132
5.2.2. Mechanical outflow obstruction
Statement
Treatment for MOO should be considered an emergency. Interventional treatment utilizing cystoscopy with or without fluoroscopy is recommended to decrease morbidity and risk of subsequent urethral stricture. Treatment modality depends on the type and chronicity of obstruction as well as regional availability.
Panel vote
10 of 10 panelists (100%) agreed with this statement.
Mechanical obstruction to urine flow results in increased pressure in the bladder and urethra proximal to the site of obstruction. Mechanical obstruction in dogs most often is intraluminal or extramural, including urolithiasis, bladder or urethral neoplasia or both, proliferative urethritis, urethral strictures, urethral foreign bodies, urethral blood clots, and prostatic disease. Extramural diseases are less likely to cause complete or partial urethral obstruction and can include caudal abdominal, perineal, or penile tumors and trauma, particularly of the pelvic canal or penis (Table 4).
TABLE 4.
Differentials/causes of mechanical outflow obstruction (MOO).
| Intraluminal | Intramural | Extraluminal |
|---|---|---|
| Urolithiasis | Neoplasia | Prostatic disease (excluding BPH) |
| Pyelonephrosis/cystitis‐related inflammatory debris | Proliferative urethritis | Caudal abdominal/perineal tumors |
| Blood clot | Stricture from previous trauma/surgery | Trauma |
| Urethral foreign bodies |
Abbreviation: BPH, benign prostatic hyperplasia.
Treatment for mechanical obstructions should be considered an emergency because both systemic and local effects can be detrimental. Dogs with an acute obstruction should be evaluated for azotemia, hyperkalemia, and metabolic acidosis. Additionally, urethral obstruction may lead to detrusor atony, mucosal damage, urine retention, and urethral or urinary bladder rupture. Chronic obstruction results in decreased detrusor muscle contractility and partial denervation. 133 , 134 , 135 Factors associated with decreased detrusor contractility include decreased muscarinic receptor density, decrease in smooth muscle cell myofilaments, weak contractions of hyperplastic cells, and decreased propagation of action potentials through the detrusor muscle secondary to intercellular (tight junction) disruption. 136 , 137 , 138 Release of obstruction within 6 days may allow full return of detrusor function. Release after 14 days may restore 50% to 65% function. Release after 30 days of obstruction may restore up to 30% of function. Obstruction for >4 weeks may result in permanent detrusor damage. 139
Interventional treatment utilizing cystoscopy (with or without fluoroscopy) is the recommended treatment to decrease morbidity and risk of subsequent urethral stricture formation associated with urethral surgery. Treatment modality depends on the cause of the obstruction and chronicity. Relief of urolithiasis can be done using cystoscopic basket retrieval or laser lithotripsy using a Holmium: YAG laser or antegrade calculi removal using an approach through the apex of the bladder (PCCL). Placement of a self‐expanding metallic stent under cystoscopic or fluoroscopic guidance has been the minimally invasive treatment of choice for dogs with urethral urothelial carcinoma (UC) 140 , 141 and also has been described in dogs with benign obstructions such as urethral strictures. 142 Urethral stents are reliable, rapidly placed, and successful in relieving obstruction in 97.6% of dogs. 140 The major complication of urethral stenting is continued incontinence, reported in 26% to 41% of dogs. 140 , 141 Alternatively, balloon dilation of the urethra for malignant UC, proliferative urethritis, and benign strictures has been described in dogs. 143 , 144 , 145 Balloon dilation offers a good alternative to relieve obstruction without the ongoing severe UI seen in some dogs with stents. It can be a suitable treatment option for dogs with urethral UC while they are undergoing radiation therapy for their disease, but dogs with prostatic carcinoma are less responsive to balloon dilation. Temporary urethral stents have been used to treat neoplasia or proliferative urethritis. 145 , 146 Transurethral resection of bladder tumor (TURBT) is the first‐line treatment in human patients with early tumors of the urethra. This procedure uses a resectoscope with continuous irrigation and a resection loop electrode to gently cut away and cauterize the tumor, thus relieving the immediate obstruction. Ablation with or without ultrasound guidance in combination with chemotherapy has been used in dogs with UC. 147
The use of cystostomy catheters, either temporary or permanent, also is recommended for urinary diversion when a stent or balloon is not immediately available or while awaiting a response to medical management. Percutaneous placement can be used as a temporary method of stabilization or surgical placement can be considered as a long‐term method if the client cannot access a specialist, with careful consideration of complications and disadvantages of this technique.
Follow‐up after relief of obstruction should include visualization of the dog's urine stream, measurement of PVRV, and repeat laboratory testing to monitor improvement in electrolyte or acid base disturbances. If PVRV remains persistently increased after relief of obstruction, treatment for functional outflow obstruction should be pursued (see Section 5.2.1).
6. GONADECTOMY
Statement
Ovariohysterectomy or ovariectomy should be delayed until at least after the first estrus in breeds that are at risk for UI or in prepubertal female dogs with UI. The timing should be tailored to the individual dog and client.
Consider the dog's signalment, intended use, household environment, and temperament in accordance with guidelines established by the American Veterinary Medical Association (AVMA).
Panel vote
11 of 12 panelists (90%) agreed with this statement.
The recommendation of this consensus panel is to delay OHE/OVE until at least the first estrus in breeds at risk of UI or in prepubertal female dogs that already have UI. No current evidence suggests a similar timeline for neutering in male dogs. However, the panel recommends that intact male dogs with voiding disorders be neutered to decrease prostatic size and prevent androgen‐related disorders (eg, idiopathic FOO).
Some evidence suggests that neutering is associated with development of acquired UI, specifically storage disorders (ie, USMI) in female dogs. A meta‐analysis found only weak evidence to support this risk and many studies had moderate to high risk of bias. 148 However, several studies published since this meta‐analysis repeatedly showed an increased risk of UI associated with neutering. 4 , 5 , 149 This risk, however, only pertains to female dogs, and castration was not associated with increased risk of UI in male dogs. 6
Other factors have been associated with an increased risk of acquired UI such as breed and weight of the dog. 3 , 4 , 5 , 149 , 150 Neutering also can increase the risk of UI in large breed dogs (>25 kg) but not in smaller breeds, suggesting several variables might have effects. 150 Many studies have failed to document a substantial association between timing of spaying and the risk of developing UI. 2 , 3 , 5 , 151
7. FOLLOW‐UP AND MONITORING
Statement
All dogs with UI should be evaluated regularly and routine use of CUI‐S should be used for objective evaluation of improvement or regression over time. Any adverse events treatment should be recorded.
Panel vote
12 of 12 panelists (100%) agreed with this statement.
Standardizing the response scores to specific treatments can aid in identifying cause and ideal treatment. Dogs that do not respond well to treatment should be evaluated for a different underlying cause of UI or concurrent UI disorders such as EU and USMI. Factors to consider when animals relapse include noncompliant clients, resistance to medication, development of a comorbidity (eg, PU/PD, high salt diet, osteoarthritis, UTI) or incorrect initial diagnosis.
8. FUTURE DIRECTIONS
Future developments in the diagnosis and treatment of UI in dogs should be led by continued understanding of the underlying pathophysiology and the use of prospective controlled clinical trials. Direct treatment comparisons to assess drug dosage and efficacy for underlying causes of UI, such as USMI and FOO, are needed. In addition, outcome predictors for response to treatment could help tailor treatment and help understanding of relapse vs resistance to medications.
Understanding urinary incontinence in male dogs including underlying causes and treatment response is warranted. Prevalence studies of storage or voiding disorders in male dogs will help with diagnosis and empirical medical management.
It is the hope of the consensus panel that publication of this consensus statement will guide future studies and foster active interest in this field.
CONFLICT OF INTEREST DECLARATION
Authors declare no conflict of interest.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Authors declare no IACUC or other approval was needed.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
Supporting information
Supplemental Table 1. Canine urinary incontinence survey.
Supplemental Table 2. Clinical signs of urinary incontinence associated with neurologic dysfunction. Note that motor and proprioceptive deficits are usually prominent when there is an underlying neurologic etiology. However, the presence of spinal pain, of fecal incontinence, or a disconnected forelimb hindlimb gait in the absence of clear motor and proprioceptive deficits should alert the clinician to the possibility of a neurologic etiology.
ACKNOWLEDGMENT
No funding was received for this study. The authors acknowledge Dr Marilyn Dunn DMV, MVSc, DACVIM and the American Society of Veterinary Nephrology and Urology for their contributions. The authors thank Tim Vojt for illustrations and Ivy Leventhal for manuscript preparation.
Kendall A, Byron JK, Westropp JL, et al. ACVIM consensus statement on diagnosis and management of urinary incontinence in dogs. J Vet Intern Med. 2024;38(2):878‐903. doi: 10.1111/jvim.16975
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provide the veterinary community with up‐to‐date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. The ACVIM Board of Regents oversees selection of relevant topics, identification of panel members with the expertise to draft the statements, and other aspects of assuring the integrity of the process. The statements are derived from evidence‐based medicine whenever possible and the panel offers interpretive comments when such evidence is inadequate or contradictory. A draft is prepared by the panel, followed by solicitation of input by the ACVIM membership which may be incorporated into the statement. It is then submitted to the Journal of Veterinary Internal Medicine, where it is edited prior to publication. The authors are solely responsible for the content of the statements.
REFERENCES
- 1. Arnold S, Arnold P, Hubler M, Casal M, Rüsch P. Urinary incontinence in spayed female dogs: frequency and breed disposition. Schweiz Arch Tierheilkd. 1989;131:259‐263. [PubMed] [Google Scholar]
- 2. Thrusfield MV, Holt PE, Muirhead RH. Acquired urinary incontinence in bitches: its incidence and relationship to neutering practices. J Small Anim Pract. 1998;39:559‐566. [DOI] [PubMed] [Google Scholar]
- 3. Forsee KM, Davis GJ, Mouat EE, Salmeri KR, Bastian RP. Evaluation of the prevalence of urinary incontinence in spayed female dogs: 566 cases (2003‐2008). J Am Vet Med Assoc. 2013;242:959‐962. [DOI] [PubMed] [Google Scholar]
- 4. O'Neill DG, Riddell A, Church DB, Owen L, Brodbelt DC, Hall JL. Urinary incontinence in bitches under primary veterinary care in England: prevalence and risk factors. J Small Anim Pract. 2017;58:685‐693. [DOI] [PubMed] [Google Scholar]
- 5. Pegram C, Brodbelt DC, Church DB, et al. Associations between neutering and early‐onset urinary incontinence in UK bitches under primary veterinary care. J Small Anim Pract. 2019;60:723‐733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hall JL, Owen L, Riddell A, Church DB, Brodbelt DC, O'Neill DG. Urinary incontinence in male dogs under primary veterinary care in England: prevalence and risk factors. J Small Anim Pract. 2019;60:86‐95. [DOI] [PubMed] [Google Scholar]
- 7. Byron JK. Micturition disorders. Vet Clin North Am Small Anim Pract. 2015;45:769‐782. [DOI] [PubMed] [Google Scholar]
- 8. Lorenz MD, Coates J, Kent M, ScienceDirect . Handbook of Veterinary Neurology. 5th ed. London: Elsevier Health Sciences; 2010. [Google Scholar]
- 9. de Groat WC, Yoshimura N. Anatomy and physiology of the lower urinary tract. Handb Clin Neurol. 2015;130:61‐108. [DOI] [PubMed] [Google Scholar]
- 10. Cullen WC, Fletcher TF, Bradley WE. Histology of the canine urethra II. Morphometry of the male pelvic urethra. Anat Rec. 1981;199:187‐195. [DOI] [PubMed] [Google Scholar]
- 11. Cullen WC, Fletcher TF, Bradley WE. Histology of the canine urethra. I. Morphometry of the female urethra. Anat Rec. 1981;199:177‐186. [DOI] [PubMed] [Google Scholar]
- 12. Carattino MD, Prakasam HS, Ruiz WG, et al. Bladder filling and voiding affect umbrella cell tight junction organization and function. Am J Physiol Renal Physiol. 2013;305:F1158‐F1168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Augsburger HR, Cruz‐Orive LM, Arnold S. Morphology and stereology of the female canine urethra correlated with the urethral pressure profile. Acta Anat (Basel). 1993;148:197‐205. [DOI] [PubMed] [Google Scholar]
- 14. Augsburger HR, Cruz‐Orive LM. Morphological, histochemical and stereological analysis of the female canine M. urethralis. Histochemistry. 1994;102:373‐382. [DOI] [PubMed] [Google Scholar]
- 15. Hermanson JW, DeLahunta A, Evans HE. Miller and Evans' Anatomy of the Dog. Vol xxi. 5th ed. St Louis, MO: Elsevier; 2020:981 Illustrations (chiefly colour). [Google Scholar]
- 16. Stolzenburg JU, Neuhaus J, Liatsikos EN, Schwalenberg T, Ludewig E, Ganzer R. Histomorphology of canine urethral sphincter systems, including three‐dimensional reconstruction and magnetic resonance imaging. Urology. 2006;67:624‐630. [DOI] [PubMed] [Google Scholar]
- 17. Stolzenburg JU, Schwalenberg T, Do M, et al. Is the male dog comparable to human? A histological study of the muscle systems of the lower urinary tract. Anat Histol Embryol. 2002;31:198‐205. [DOI] [PubMed] [Google Scholar]
- 18. Van der Werf BA, Creed KE. Mechanical properties and innervation of the smooth muscle layers of the urethra of greyhounds. BJU Int. 2002;90:588‐595. [DOI] [PubMed] [Google Scholar]
- 19. de Groat WC, Griffiths D, Yoshimura N. Neural control of the lower urinary tract. Compr Physiol. 2015;5:327‐396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Oliver J, Bradley W, Fletcher T. Spinal cord distribution of the somatic innervation of the external urethral sphincter of the cat. J Neurol Sci. 1970;10:11‐23. [DOI] [PubMed] [Google Scholar]
- 21. Purinton PT, Oliver JE Jr. Spinal cord origin of innervation to the bladder and urethra of the dog. Exp Neurol. 1979;65:422‐434. [DOI] [PubMed] [Google Scholar]
- 22. Thuroff JW, Bazeed MA, Schmidt RA, et al. Functional pattern of sacral root stimulation in dogs. II. Urethral closure. J Urol. 1982;127:1034‐1038. [DOI] [PubMed] [Google Scholar]
- 23. Petras JM, Cummings JF. Sympathetic and parasympathetic innervation of the urinary bladder and urethra. Brain Res. 1978;153:363‐369. [DOI] [PubMed] [Google Scholar]
- 24. Purinton PT, Oliver JE Jr, Bradley WE. Differences in routing of pelvic visceral afferent fibers in the dog and cat. Exp Neurol. 1981;73:725‐731. [DOI] [PubMed] [Google Scholar]
- 25. Ye G, Jin X. Action of autonomic drugs on the in vivo bladder base and proximal urethra in dog. Chin Med J (Engl). 1997;110:173‐176. [PubMed] [Google Scholar]
- 26. Takeda M, Araki I, Kamiyama M, Takihana Y, Komuro M, Furuya Y. Diagnosis and treatment of voiding symptoms. Urology. 2003;62:11‐19. [DOI] [PubMed] [Google Scholar]
- 27. Blok BF, Holstege G. The central control of micturition and continence: implications for urology. BJU Int. 1999;83(Suppl 2):1‐6. [DOI] [PubMed] [Google Scholar]
- 28. Slead T, Vaden S, Harris T, Kendall A. Urinary incontinence in male dogs. American College of Veterinary Internal Medicine Forum. Philadelphia, PA; 2023:NU15. [Google Scholar]
- 29. Hart BL, Hart LA, Thigpen AP, Willits NH. Assisting decision‐making on age of neutering for 35 breeds of dogs: associated joint disorders, cancers, and urinary incontinence. Front Vet Sci. 2020;7:388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Holt PE, Thrusfield MV. Association in bitches between breed, size, neutering and docking, and acquired urinary incontinence due to incompetence of the urethral sphincter mechanism. Vet Rec. 1993;133:177‐180. [DOI] [PubMed] [Google Scholar]
- 31. Diaz Espineira MM, Viehoff FW, Nickel RF. Idiopathic detrusor‐urethral dyssynergia in dogs: a retrospective analysis of 22 cases. J Small Anim Pract. 1998;39:264‐270. [DOI] [PubMed] [Google Scholar]
- 32. Atalan G, Barr FJ, Holt PE. Frequency of urination and ultrasonographic estimation of residual urine in normal and dysuric dogs. Res Vet Sci. 1999;67:295‐299. [DOI] [PubMed] [Google Scholar]
- 33. Vasquez EJ, Kendall A, Musulin S, Vaden SL. Three‐dimensional bladder ultrasound to measure daily urinary bladder volume in hospitalized dogs. J Vet Intern Med. 2021;35:2256‐2262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Haylen BT, Lee J. The accuracy of post‐void residual measurement in women. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:603‐606. [DOI] [PubMed] [Google Scholar]
- 35. Bubenik LJ, Hosgood GL, Waldron DR, Snow LA. Frequency of urinary tract infection in catheterized dogs and comparison of bacterial culture and susceptibility testing results for catheterized and noncatheterized dogs with urinary tract infections. J Am Vet Med Assoc. 2007;231:893‐899. [DOI] [PubMed] [Google Scholar]
- 36. Bubenik L, Hosgood G. Urinary tract infection in dogs with thoracolumbar intervertebral disc herniation and urinary bladder dysfunction managed by manual expression, indwelling catheterization or intermittent catheterization. Vet Surg. 2008;37:791‐800. [DOI] [PubMed] [Google Scholar]
- 37. Smarick SD, Haskins SC, Aldrich J, et al. Incidence of catheter‐associated urinary tract infection among dogs in a small animal intensive care unit. J Am Vet Med Assoc. 2004;224:1936‐1940. [DOI] [PubMed] [Google Scholar]
- 38. Biertuempfel PH, Ling GV, Ling GA. Urinary tract infection resulting from catheterization in healthy adult dogs. J Am Vet Med Assoc. 1981;178:989‐991. [PubMed] [Google Scholar]
- 39. Dicuio M, Pomara G, Menchini Fabris F, et al. Measurements of urinary bladder volume: comparison of five ultrasound calculation methods in volunteers. Arch Ital Urol Androl. 2005;77:60‐62. [PubMed] [Google Scholar]
- 40. Kendall A, Keenihan E, Kern ZT, et al. Three‐dimensional bladder ultrasound for estimation of urine volume in dogs compared with traditional 2‐dimensional ultrasound methods. J Vet Intern Med. 2020;34:2460‐2467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Hvarness H, Skjoldbye B, Jakobsen H. Urinary bladder volume measurements: comparison of three ultrasound calculation methods. Scand J Urol Nephrol. 2002;36:177‐181. [DOI] [PubMed] [Google Scholar]
- 42. Grant DC, Nappier MT, Corrigan VK. Diagnostic accuracy of a point‐of‐care test using voided urine samples for detection of bacteriuria in dogs with signs of lower urinary tract disease. J Vet Intern Med. 2021;35:993‐996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Llido M, Vachon C, Dickinson M, Beauchamp G, Dunn M. Transurethral cystoscopy in dogs with recurrent urinary tract infections: retrospective study (2011‐2018). J Vet Intern Med. 2020;34:790‐796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Zhang RQ, Xia MC, Cui F, et al. Epidemiological survey of adult female stress urinary incontinence. BMC Womens Health. 2021;21:172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Weese JS, Blondeau J, Boothe D, et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet J. 2019;247:8‐25. [DOI] [PubMed] [Google Scholar]
- 46. Khandelwal C, Kistler C. Diagnosis of urinary incontinence. Am Fam Physician. 2013;87:543‐550. [PubMed] [Google Scholar]
- 47. Lane IF, Lappin MR, Seim HB 3rd. Evaluation of results of preoperative urodynamic measurements in nine dogs with ectopic ureters. J Am Vet Med Assoc. 1995;206:1348‐1357. [PubMed] [Google Scholar]
- 48. Koie H, Yamaya Y, Sakai T. Four cases of lowered urethral pressure in canine ectopic ureter. J Vet Med Sci. 2000;62:1221‐1222. [DOI] [PubMed] [Google Scholar]
- 49. Goldstein RE, Westropp JL. Urodynamic testing in the diagnosis of small animal micturition disorders. Clin Tech Small Anim Pract. 2005;20:65‐72. [DOI] [PubMed] [Google Scholar]
- 50. Byron JK, March PA, DiBartola SP, et al. Comparison of the effect of propofol and sevoflurane on the urethral pressure profile in healthy female dogs. Am J Vet Res. 2003;64:1288‐1292. [DOI] [PubMed] [Google Scholar]
- 51. Oliver JE Jr, Young WO. Evaluation of pharmacologic agents for restraint in cystometry in the dog and cat. Am J Vet Res. 1973;34:665‐668. [PubMed] [Google Scholar]
- 52. Rawlings CA, Barsanti JA, Chernosky AM, Oliver JE. Results of cystometry and urethral pressure profilometry in dogs sedated with medetomidine or xylazine. Am J Vet Res. 2001;62:167‐170. [DOI] [PubMed] [Google Scholar]
- 53. Johnson CA, Beemsterboer JM, Gray PR, Slusser PG, Goullaud EL. Effects of various sedatives on air cystometry in dogs. Am J Vet Res. 1988;49:1525‐1528. [PubMed] [Google Scholar]
- 54. Nell E, Garofolo SQ, Ober C. Pure cystine and urate calculi can be clearly visible using survey digital radiography. Can Vet J. 2021;62:605‐607. [PMC free article] [PubMed] [Google Scholar]
- 55. Johnston GR, Feeney DA. Localization of feline urethral obstruction. Vet Clin North Am Small Anim Pract. 1984;14:555‐566. [DOI] [PubMed] [Google Scholar]
- 56. Mirkovic TK, Shmon CL, Allen AL. Urinary obstruction secondary to an ossifying fibroma of the os penis in a dog. J Am Anim Hosp Assoc. 2004;40:152‐156. [DOI] [PubMed] [Google Scholar]
- 57. Burchell RK, Kirberger RM, Janse van Rensberg DD. Haemangiosarcoma of the os penis in a dog: the most common neoplasm of the canine penis. J S Afr Vet Assoc. 2014;85:e1‐e4. [DOI] [PubMed] [Google Scholar]
- 58. Ackerman N. Urethrography: Interpretation of the Study. California Veterinarian. Sacramento, CA; 1979. [Google Scholar]
- 59. Thrall DE. Principles of radiographic interpretation of the abdomen. In: Thrall DE, ed. Textbook of Veterinary Diagnostic Radiology. 7th ed. W.B. Saunders. Philadelphia, PA; 2018:754‐763. [Google Scholar]
- 60. Webbon PM. The radiological investigation of congenital urinary incontinence in the bitch. Vet Annu. 1982;22:199‐206. [Google Scholar]
- 61. Holt P, Gibbs C, Latham J. An evaluation of positive contrast vaginourethrography as a diagnostic aid in the bitch. J Small Anim Pract. 1984;25:531‐549. [Google Scholar]
- 62. Holt PE, Moore AH. Canine ureteral ectopia: an analysis of 175 cases and comparison of surgical treatments. Vet Rec. 1995;136:345‐349. [DOI] [PubMed] [Google Scholar]
- 63. Holt P. Urinary incontinence in the dog. In Pract. 1983;5(162–164):169‐173. [DOI] [PubMed] [Google Scholar]
- 64. Wilson JW, Kurtz HJ, Leipold HW, Lees GE. Spina bifida in the dog. Vet Pathol. 1979;16:165‐179. [DOI] [PubMed] [Google Scholar]
- 65. Groesslinger K, Tham T, Egerbacher M, Lorinson D. Prevalence and radiologic and histologic appearance of vesicourachal diverticula in dogs without clinical signs of urinary tract disease. J Am Vet Med Assoc. 2005;226:383‐386. [DOI] [PubMed] [Google Scholar]
- 66. Pearson H, Gibbs C. Urinary incontinence in the dog due to accidental vagino‐ureteral fistulation during hysterectomy. J Small Anim Pract. 1980;21:287‐291. [DOI] [PubMed] [Google Scholar]
- 67. Holt PE. Importance of urethral length, bladder neck position and vestibulovaginal stenosis in sphincter mechanism incompetence in the incontinent bitch. Res Vet Sci. 1985;39:364‐372. [PubMed] [Google Scholar]
- 68. Crawford JT, Adams WM. Influence of vestibulovaginal stenosis, pelvic bladder, and recessed vulva on response to treatment for clinical signs of lower urinary tract disease in dogs: 38 cases (1990‐1999). J Am Vet Med Assoc. 2002;221:995‐999. [DOI] [PubMed] [Google Scholar]
- 69. Benzimra C, Decome M, Maurey C, et al. Intermittent urethral obstruction secondary to caudal sliding of a pelvic bladder in 3 dogs. Can Vet J. 2020;61:267‐273. [PMC free article] [PubMed] [Google Scholar]
- 70. Gregory SP, Parkinson TJ, Holt PE. Urethral conformation and position in relation to urinary incontinence in the bitch. Vet Rec. 1992;131:167‐170. [DOI] [PubMed] [Google Scholar]
- 71. Power SC, Eggleton KE, Aaron AJ, Holt PE, Cripps PJ. Urethral sphincter mechanism incompetence in the male dog: importance of bladder neck position, proximal urethral length and castration. J Small Anim Pract. 1998;39:69‐72. [DOI] [PubMed] [Google Scholar]
- 72. Adams WM, DiBartola SP. Radiographic and clinical features of pelvic bladder in the dog. J Am Vet Med Assoc. 1983;182:1212‐1217. [PubMed] [Google Scholar]
- 73. Johnston GR, Osborne CA, Jessen CR, Feeney DA. Effects of urinary bladder distention on location of the urinary bladder and urethra of healthy dogs and cats. Am J Vet Res. 1986;47:404‐415. [PubMed] [Google Scholar]
- 74. Mahaffey MB, Barsanti JA, Barber DL, Crowell WA. Pelvic bladder in dogs without urinary incontinence. J Am Vet Med Assoc. 1984;184:1477‐1479. [PubMed] [Google Scholar]
- 75. Gregory SP, Cripps PJ, Holt PE. Comparison of urethral pressure profilometry and contrast radiography in the diagnosis of incompetence of the urethral sphincter mechanism in bitches. Vet Rec. 1996;138:58‐61. [DOI] [PubMed] [Google Scholar]
- 76. Taylor O, Knight R, Genain MA, Owen L. Ultrasonography as a sensitive and specific diagnostic modality for the detection of ectopic ureters in urinary incontinent dogs. Vet Radiol Ultrasound. 2022;63:328‐336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Lamb CR, Gregory SP. Ultrasonographic findings in 14 dogs with ectopic ureter. Vet Radiol Ultrasound. 1998;39:218‐223. [DOI] [PubMed] [Google Scholar]
- 78. Secrest S, Essman S, Nagy J, Schultz L. Effects of furosemide on ureteral diameter and attenuation using computed tomographic excretory urography in normal dogs. Vet Radiol Ultrasound. 2013;54:17‐24. [DOI] [PubMed] [Google Scholar]
- 79. Oh H, Kim S, Kim S, et al. Evaluation of the ureteral jet in dogs by using color Doppler ultrasonography. J Vet Sci. 2017;18:399‐406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Samii VF, McLoughlin MA, Mattoon JS, et al. Digital fluoroscopic excretory urography, digital fluoroscopic urethrography, helical computed tomography, and cystoscopy in 24 dogs with suspected ureteral ectopia. J Vet Intern Med. 2004;18:271‐281. [DOI] [PubMed] [Google Scholar]
- 81. Fox AJ, Sharma A, Secrest SA. Computed tomographic excretory urography features of intramural ectopic ureters in 10 dogs. J Small Anim Pract. 2016;57:210‐213. [DOI] [PubMed] [Google Scholar]
- 82. Schwarz T, Bommer N, Parys M, et al. Four‐dimensional CT excretory urography is an accurate technique for diagnosis of canine ureteral ectopia. Vet Radiol Ultrasound. 2021;62:190‐198. [DOI] [PubMed] [Google Scholar]
- 83. Berent AC, Weisse C, Mayhew PD, Todd K, Wright M, Bagley D. Evaluation of cystoscopic‐guided laser ablation of intramural ectopic ureters in female dogs. J Am Vet Med A. 2012;240:716‐725. [DOI] [PubMed] [Google Scholar]
- 84. Hoey C, Friend E, Meakin LB, Chanoit GP. Long‐term outcome of female dogs treated for intramural ectopic ureters with cystoscopic‐guided laser ablation. Vet Surg. 2021;50:1449‐1462. [DOI] [PubMed] [Google Scholar]
- 85. Hooi KS, Vachon C, Martel DV, Dunn M. Retrospective evaluation of cystoscopic‐guided laser ablation of intramural ectopic ureters in female dogs. J Vet Intern Med. 2022;36:156‐163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Burdick S, Berent AC, Weisse C, Langston C. Endoscopic‐guided laser ablation of vestibulovaginal septal remnants in dogs: 36 cases (2007‐2011). J Am Vet Med Assoc. 2014;244:944‐949. [DOI] [PubMed] [Google Scholar]
- 87. Scott L, Leddy M, Bernay F, Davot JL. Evaluation of phenylpropanolamine in the treatment of urethral sphincter mechanism incompetence in the bitch. J Small Anim Pract. 2002;43:493‐496. [DOI] [PubMed] [Google Scholar]
- 88. Hamaide AJ, Grand JG, Farnir F, et al. Urodynamic and morphologic changes in the lower portion of the urogenital tract after administration of estriol alone and in combination with phenylpropanolamine in sexually intact and spayed female dogs. Am J Vet Res. 2006;67:901‐908. [DOI] [PubMed] [Google Scholar]
- 89. Sontas HB, Dokuzeylu B, Turna O, Ekici H. Estrogen‐induced myelotoxicity in dogs: a review. Can Vet J. 2009;50:1054‐1058. [PMC free article] [PubMed] [Google Scholar]
- 90. Mathews KD, Hardy B, Johnson EG, Westropp JL. Ultrasonographic evaluation of uterine stump size in ovariohysterectomized dogs receiving estriol compared to control dogs. Top Companion Anim Med. 2020;38:100370. [DOI] [PubMed] [Google Scholar]
- 91. Palerme JS, Mazepa A, Hutchins RG, Ziglioli V, Vaden SL. Clinical response and side effects associated with testosterone cypionate for urinary incontinence in male dogs. J Am Anim Hosp Assoc. 2017;53:285‐290. [DOI] [PubMed] [Google Scholar]
- 92. Nair R, Dyer DC. Pharmacological characterization of alpha 1‐adrenoceptors in porcine uterine artery. Eur J Pharmacol. 1996;312:45‐51. [DOI] [PubMed] [Google Scholar]
- 93. Levitt M, Cumiskey WR, Shargel L. Studies on the physiologic disposition and activity of phenylpropanolamines in the mouse. Drug Metab Dispos. 1974;2:187‐193. [PubMed] [Google Scholar]
- 94. Segev G, Westropp JL, Kulik C, Lavy E. Changes in blood pressure following escalating doses of phenylpropanolamine and a suggested protocol for monitoring. Can Vet J. 2015;56:39‐43. [PMC free article] [PubMed] [Google Scholar]
- 95. Chen H, Shipov A, Segev G. Evaluation of cross‐linked gelatin as a bulking agent for the management of urinary sphincter mechanism incompetence in female dogs. J Vet Intern Med. 2020;34:1914‐1919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Luttmann K, Merle R, Nickel R. Retrospective analysis after endoscopic urethral injections of glutaraldehyde‐cross‐linked‐collagen or dextranomer/hyaluronic acid copolymer in bitches with urinary incontinence. J Small Anim Pract. 2019;60:96‐101. [DOI] [PubMed] [Google Scholar]
- 97. Bartges JWCA. Polydimethylsiloxane Bulking Agent (PDMS UGA) Injection for Treatment of Female Canine Urinary Incontinence—Preliminary Results. Denver, CO: American College of Veterinary Medicine Forum; 2011. [Google Scholar]
- 98. Vaden SL, Mathews KG, Yoo J, et al. The use of autologous skeletal muscle progenitor cells for adjunctive treatment of presumptive urethral sphincter mechanism incompetence in female dogs. J Vet Intern Med. 2022;36:1686‐1692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Holt PE. Long‐term evaluation of colposuspension in the treatment of urinary incontinence due to incompetence of the urethral sphincter mechanism in the bitch. Vet Rec. 1990;127:537‐542. [PubMed] [Google Scholar]
- 100. Rawlings C, Barsanti JA, Mahaffey MB, Bement S. Evaluation of colposuspension for treatment of incontinence in spayed female dogs. J Am Vet Med Assoc. 2001;219:770‐775. [DOI] [PubMed] [Google Scholar]
- 101. Holt PE, Coe RJ, Hotston MA. Prostatopexy as a treatment for urethral sphincter mechanism incompetence in male dogs. J Small Anim Pract. 2005;46:567‐570. [DOI] [PubMed] [Google Scholar]
- 102. Weber UT, Arnold S, Hubler M, Kupper JR. Surgical treatment of male dogs with urinary incontinence due to urethral sphincter mechanism incompetence. Vet Surg. 1997;26:51‐56. [DOI] [PubMed] [Google Scholar]
- 103. Currao RL, Berent AC, Weisse C, Fox P. Use of a percutaneously controlled urethral hydraulic occluder for treatment of refractory urinary incontinence in 18 female dogs. Vet Surg. 2013;42:440‐447. [DOI] [PubMed] [Google Scholar]
- 104. Adin CA, Farese JP, Cross AR, Provitola MK, Davidson JS, Jankunas H. Urodynamic effects of a percutaneously controlled static hydraulic urethral sphincter in canine cadavers. Am J Vet Res. 2004;65:283‐288. [DOI] [PubMed] [Google Scholar]
- 105. Delisser PJ, Friend EJ, Chanoit GP, Parsons KJ. Static hydraulic urethral sphincter for treatment of urethral sphincter mechanism incompetence in 11 dogs. J Small Anim Pract. 2012;53:338‐343. [DOI] [PubMed] [Google Scholar]
- 106. Fournet A, Maurey C, Decambron A, Viateau V, Manassero M. Treatment of urinary incontinence in a cat with genitourinary dysplasia using an urethral sphincter occluder. J Small Anim Pract. 2021;62:391‐396. [DOI] [PubMed] [Google Scholar]
- 107. Luckring EJ, Ham K, Adin CA, McLoughlin MA, Stull JW. Laparoscopic placement and urodynamic effects of an artificial urethral sphincter in cadaveric dogs. Vet Surg. 2016;45:O20‐O27. [DOI] [PubMed] [Google Scholar]
- 108. Morgan K, Milner HR, Tikekar A, Smith HL, Coomer AR. Long term use of hydraulic artificial urethral sphincters in nine dogs from New Zealand with urethral sphincter mechanism incompetence. N Z Vet J. 2018;66:205‐209. [DOI] [PubMed] [Google Scholar]
- 109. Reeves L, Adin C, McLoughlin M, Ham K, Chew D. Outcome after placement of an artificial urethral sphincter in 27 dogs. Vet Surg. 2013;42:12‐18. [DOI] [PubMed] [Google Scholar]
- 110. Rose SA, Adin CA, Ellison GW, et al. Long‐term efficacy of a percutaneously adjustable hydraulic urethral sphincter for treatment of urinary incontinence in four dogs. Vet Surg. 2009;38:747‐753. [DOI] [PubMed] [Google Scholar]
- 111. Wilson KE, Berent AC, Weisse CW. Use of a percutaneously controlled hydraulic occluder for treatment of refractory urinary incontinence in three female cats. J Am Vet Med Assoc. 2016;248:544‐551. [DOI] [PubMed] [Google Scholar]
- 112. Claeys S, de Leval J, Hamaide A. Transobturator vaginal tape inside out for treatment of urethral sphincter mechanism incompetence: preliminary results in 7 female dogs. Vet Surg. 2010;39:969‐979. [DOI] [PubMed] [Google Scholar]
- 113. Claeys S, Noël S, Hamaide A. Acquired urinary incontinence in the bitch: update and perspectives from human medicine. Part 3: the urethral component and surgical treatment. Vet J. 2010;186:25‐31. [DOI] [PubMed] [Google Scholar]
- 114. Hamon M, Hamaide AJ, Noël SM, Claeys S. Long‐term outcome of the transobturator vaginal tape inside out for the treatment of urethral sphincter mechanism incompetence in female dogs. Vet Surg. 2019;48:29‐34. [DOI] [PubMed] [Google Scholar]
- 115. Kopecny L, Palm CA, Culp WTN. Diagnosis, management, and outcome of urethral obstruction secondary to the capsule associated with the artificial urethral sphincter device. J Vet Intern Med. 2022;36:1016‐1023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Ziegelmann MJ, Linder BJ, Avant RA, Elliott DS. Bacterial cultures at the time of artificial urinary sphincter revision surgery in clinically uninfected devices: a contemporary series. J Urol. 2019;201:1152‐1157. [DOI] [PubMed] [Google Scholar]
- 117. Khouri RK Jr, Ortiz NM, Dropkin BM, et al. Artificial urinary sphincter complications: risk factors, workup, and clinical approach. Curr Urol Rep. 2021;22:30. [DOI] [PubMed] [Google Scholar]
- 118. Tong K, Nelson LL, Hauptman J, Nelson NC. Evaluation of percutaneously adjustable hydraulic urethral sphincters with and without induced mechanical failure. Vet Surg. 2013;42:774‐782. [DOI] [PubMed] [Google Scholar]
- 119. McLoughlin MA, Chew DJ. Diagnosis and surgical management of ectopic ureters. Clin Tech Small Anim Pract. 2000;15:17‐24. [DOI] [PubMed] [Google Scholar]
- 120. Smith AL, Radlinsky MG, Rawlings CA. Cystoscopic diagnosis and treatment of ectopic ureters in female dogs: 16 cases (2005‐2008). J Am Vet Med Assoc. 2010;237:191‐195. [DOI] [PubMed] [Google Scholar]
- 121. Dekerle B, Maurice E, Decambron A, Viateau V, Maurey C, Manassero M. Outcomes of 25 female dogs treated for ectopic ureters by open surgery or cystoscopic‐guided laser ablation. Vet Surg. 2022;51:568‐575. [DOI] [PubMed] [Google Scholar]
- 122. Burbaitė E, Sabūnas V, Stankus V, et al. Monopolar electrocautery use in minimally invasive urosurgery: case report of ectopic ureter management in a bitch. Open Vet J. 2022;12:182‐187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Berent AC, Mayhew PD, Porat‐Mosenco Y. Use of cystoscopic‐guided laser ablation for treatment of intramural ureteral ectopia in male dogs: four cases (2006‐2007). J Am Vet Med Assoc. 2008;232:1026‐1034. [DOI] [PubMed] [Google Scholar]
- 124. Morgan M, Forman M. Cystoscopy in dogs and cats. Vet Clin North Am Small Anim Pract. 2015;45:665‐701. [DOI] [PubMed] [Google Scholar]
- 125. Noel S, Massart L, Hamaide A. Urodynamic investigation by telemetry in beagle dogs: validation and effects of oral administration of current urological drugs: a pilot study. BMC Vet Res. 2013;9:197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Stilwell C, Bazelle J, Walker D, Stanzani G, Florey J. Detrusor urethral dyssynergy in dogs: 35 cases (2007‐2019). J Small Anim Pract. 2021;62:468‐477. [DOI] [PubMed] [Google Scholar]
- 127. Lane IF, Fischer JR, Miller E, Grauer GF, Lappin MR. Functional urethral obstruction in 3 dogs: clinical and urethral pressure profile findings. J Vet Intern Med. 2000;14:43‐49. [DOI] [PubMed] [Google Scholar]
- 128. Stoffel JT. Detrusor sphincter dyssynergia: a review of physiology, diagnosis, and treatment strategies. Transl Androl Urol. 2016;5:127‐135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Lane IF. Diagnosis and management of urinary retention. Vet Clin North Am Small Anim Pract. 2000;30(25–57):v‐57. [DOI] [PubMed] [Google Scholar]
- 130. Mawby DI, Meric SM, Crichlow EC, Papich MG. Pharmacological relaxation of the urethra in male cats: a study of the effects of phenoxybenzamine, diazepam, nifedipine and xylazine. Can J Vet Res. 1991;55:28‐32. [PMC free article] [PubMed] [Google Scholar]
- 131. Mathews K, Toedebusch C, Palm C, Kendall A, Westropp JL. Idiopathic functional urinary outflow tract obstruction in dogs, a retrospective case series (2010‐2021): 31 cases. J Vet Intern Med. 2023;37:2211‐2218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Gookin JL, Bunch SE. Detrusor‐striated sphincter dyssynergia in a dog. J Vet Intern Med. 1996;10:339‐344. [DOI] [PubMed] [Google Scholar]
- 133. Sibley GN. The physiological response of the detrusor muscle to experimental bladder outflow obstruction in the pig. Br J Urol. 1987;60:332‐336. [DOI] [PubMed] [Google Scholar]
- 134. Speakman MJ, Sethia KK, Fellows GJ, Smith JC. A study of the pathogenesis, urodynamic assessment and outcome of detrusor instability associated with bladder outflow obstruction. Br J Urol. 1987;59:40‐44. [DOI] [PubMed] [Google Scholar]
- 135. Speakman MJ, Brading AF, Gilpin CJ, Dixon JS, Gilpin SA, Gosling JA. Bladder outflow obstruction—a cause of denervation Supersensitivity. J Urol. 1987;138:1461‐1466. [DOI] [PubMed] [Google Scholar]
- 136. Ghoniem GM, Regnier CH, Biancani P, Johnson L, Susset JG. Effect of vesical outlet obstruction on detrusor contractility and passive properties in rabbits. J Urol. 1986;135:1284‐1289. [DOI] [PubMed] [Google Scholar]
- 137. Levin RM, High J, Wein AJ. The effect of short‐term obstruction on urinary bladder function in the rabbit. J Urol. 1984;132:789‐791. [DOI] [PubMed] [Google Scholar]
- 138. Lloyd‐Davies RW, Hinman F Jr. Constant flow in the female dog. V. Effect of raised intraperitoneal pressure on exit velocity. J Urol. 1971;105:802‐806. [DOI] [PubMed] [Google Scholar]
- 139. Brace JJ. Urinary tract obstruction. In: Bojrab M, ed. Pathophysiology of Small Animal Surgery. Philadephia: Lea & Febiger; 1981:288. [Google Scholar]
- 140. Blackburn AL, Berent AC, Weisse CW, Brown DC. Evaluation of outcome following urethral stent placement for the treatment of obstructive carcinoma of the urethra in dogs: 42 cases (2004‐2008). J Am Vet Med Assoc. 2013;242:59‐68. [DOI] [PubMed] [Google Scholar]
- 141. McMillan SK, Knapp DW, Ramos‐Vara JA, et al. Outcome of urethral stent placement for management of urethral obstruction secondary to transitional cell carcinoma in dogs: 19 cases (2007‐2010). J Am Vet Med Assoc. 2012;241:1627‐1632. [DOI] [PubMed] [Google Scholar]
- 142. Hill TL, Berent AC, Weisse CW. Evaluation of urethral stent placement for benign urethral obstructions in dogs. J Vet Intern Med. 2014;28:1384‐1390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Gin TE, Secoura P, Harris T, Vaden S. Outcomes following balloon dilation of benign urethral strictures in dogs: eight cases (2005‐2018). J Am Anim Hosp Assoc. 2020;56:23‐29. [DOI] [PubMed] [Google Scholar]
- 144. Kim S, Hosoya K, Takagi S, Okumura M. Outcomes following balloon dilation for management of urethral obstruction secondary to urothelial carcinoma in dogs: 12 cases (2010‐2015). J Am Vet Med Assoc. 2019;255:330‐335. [DOI] [PubMed] [Google Scholar]
- 145. Emanuel M, Berent AC, Weisse C, Donovan T, Lamb KE. Retrospective study of proliferative urethritis in dogs: clinical presentation and outcome using various treatment modalities in 11 dogs. J Vet Intern Med. 2021;35:312‐320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Lulich JP. Evaluation of temporary urethral stents in the management of malignant and nonmalignant urethral diseases in dogs. Vet Sci. 2022;9:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Upton ML, Tangner CH, Payton ME. Evaluation of carbon dioxide laser ablation combined with mitoxantrone and piroxicam treatment in dogs with transitional cell carcinoma. J Am Vet Med Assoc. 2006;228:549‐552. [DOI] [PubMed] [Google Scholar]
- 148. Beauvais W, Cardwell JM, Brodbelt DC. The effect of neutering on the risk of urinary incontinence in bitches—a systematic review. J Small Anim Pract. 2012;53:198‐204. [DOI] [PubMed] [Google Scholar]
- 149. Pegram C, O'Neill DG, Church DB, Hall J, Owen L, Brodbelt DC. Spaying and urinary incontinence in bitches under UK primary veterinary care: a case‐control study. J Small Anim Pract. 2019;60:395‐403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150. Byron JK, Taylor KH, Phillips GS, Stahl MS. Urethral sphincter mechanism incompetence in 163 neutered female dogs: diagnosis, treatment, and relationship of weight and age at neuter to development of disease. J Vet Intern Med. 2017;31:442‐448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. de Bleser B, Brodbelt DC, Gregory NG, Martinez TA. The association between acquired urinary sphincter mechanism incompetence in bitches and early spaying: a case‐control study. Vet J. 2011;187:42‐47. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Table 1. Canine urinary incontinence survey.
Supplemental Table 2. Clinical signs of urinary incontinence associated with neurologic dysfunction. Note that motor and proprioceptive deficits are usually prominent when there is an underlying neurologic etiology. However, the presence of spinal pain, of fecal incontinence, or a disconnected forelimb hindlimb gait in the absence of clear motor and proprioceptive deficits should alert the clinician to the possibility of a neurologic etiology.