

Abstract
Objective
The aim of this study was to investigate the bactericidal effect of various concentrations of triple antibiotic paste (TAP) against Enterococcus faecalis (E. faecalis) in dentinal tubules using a bacterial culture assay and confocal laser scanning microscope (CLSM).
Methods
Ninety human teeth were contaminated with E. faecalis (ATCC 29212) and randomly allocated into 5 groups; the negative control (without TAP), 1 mg/ml, 5 mg/ml, 7.5 mg/ml and 10 mg/ml TAP (n=18). After a 3-week TAP treatment, samples were collected from the root canal space, root dentin at 100-μm and 200-μm depth. The collected samples were subjected to a bacterial culture assay (n=10). Eight roots from each group underwent CLSM analysis to determine the live/dead bacterial cells.
Results
The bacterial culture assay results indicated that the negative control samples were all culturable. The number of culture-positive samples decreased after TAP treatment at 1, 5, 7.5 and 10 mg/ml, with 2, 2, 1 and 0 culturable samples, respectively. However, there was no significant difference among the TAP treatments. Surprisingly, the CLSM analysis demonstrated live bacteria in the dentinal tubules in all samples. The negative control had 52.36%±3.24 live bacteria. TAP treatment at 10 mg/ml had the lowest percentage of live bacterial cells (40.58%±5.40), followed by 7.5 mg/ml (44.14%±6.03), 5 mg/ml (46.31%±5.32) and 1 mg/ml (52.55%±8.82). The percentage of live cells in the 10 mg/ml, 7.5 mg/ml and 5 mg/ml TAP groups were significantly lower than the 1 mg/ml TAP and negative control groups.
Conclusion
TAP treatment significantly decreased the percentage of viable E. faecalis cells in the dentinal tubules and its bactericidal effect was dose-dependent.
Keywords: Dentinal tubule contamination, enterococcus faecalis, live/dead assay, triple antibiotic paste
HIGHLIGHTS
This is the first study that used a dentinal tubule contamination method in human teeth to evaluate the bactericidal effect of TAP.
Although 1, 5, 7.5 and 10 mg/ml of TAP decreased the culture-positive root canal samples, the differences between groups were not significant.
The bacterial culture assay results indicated that only the high concentration of TAP (10 mg/ml) completely eradicated E. faecalis in the dentinal tubules.
The CLSM analysis revealed that, including at a high TAP concentration (10 mg/ml), live bacteria were detected in the dentinal tubules.
INTRODUCTION
Disinfection during Regenerative Endodontic Procedures (REPs) is challenging and is required for tissue regeneration to occur (1). Due to the thin root canal wall of immature teeth, mechanical instrumentation must be minimized. Therefore, irrigation and medication are vital for canal disinfection. Calcium hydroxide (Ca(OH)2) is used as an intracanal medication because its high pH kills most endodontic bacteria, with no detrimental effect on stem cells (2). However, some bacteria that can survive in extreme alkaline pH, such as the gram-positive facultative anaerobe Enterococcus faecalis (E. faecalis), show resistance to Ca(OH)2 (3, 4). Thus, triple antibiotic paste (TAP) is recommended as the medication of choice in REPs (5).
TAP, a combination of metronidazole, ciprofloxacin and minocycline, is a broad-spectrum antibacterial that is used as a medication in mixed-species endodontic infections. TAP disinfects the bacteria in carious dentine and pulpal lesions (6, 7). In vitro studies found that TAP penetrates through root dentine, and reaches the outer surface of the root within 48 h (6). These characteristics make TAP an interesting choice in REPs, which require an aseptic environment (5). Studies have evaluated the appropriate concentration of TAP used for REPs, however, the results were inconclusive. The reported minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) of TAP are far less than the concentrations used clinically (8).
In root canal model studies, which are more related to the clinical situation, high concentrations of TAP (>10 mg/ml) exhibited high bactericidal efficacy by completely eradicating E. faecalis within 1–4 weeks, however, these concentrations were cytotoxic to stem cells, which could adversely affect regeneration (9–11). One mg/ml TAP resulted in ~50% stem cells from the apical papilla survival and 10 mg/ml demonstrated <10% cell survival (11). Similar results were obtained from dental pulp stem cells; 0.125 mg/ml TAP was not cytotoxic (10). However, lower concentrations of TAP can reduce, but not completely eradicate, the number of bacteria. Alyas et al. (12) found that 1 mg/ml TAP combined with methylcellulose as a vehicle completely eradicated E. faecalis biofilm in root canal blocks. At 1.5 mg/ml, TAP almost eliminated E. faecalis biofilm in the root canal after 7 d and eliminated it after 14 d (8). A confocal laser scanning analysis demonstrated similar results with >99% reduction in E. faecalis after treatment with 1.5 mg/ml TAP for 1 week (13). Lower TAP concentrations (0.01 and 0.1 mg/ml) reduced, but not completely eradicated, the number of bacteria (9).
For REPs, stem cell survivability is the key for successful outcomes. The appropriate TAP concentration should minimize the damage to stem cells; therefore, the TAP concentration used in REPs should balance its antibacterial effect and cell cytotoxicity (9–11). The American Association of Endodontists (AAE) guideline recommends 1–5 mg/ml TAP or DAP for REPs. However, the optimal concentrations of TAP (between 1 and 10 mg/ml) that can eliminate E. faecalis in the root canal remains unknown.
The aim of this study was to investigate the bactericidal effect of various TAP concentrations against E. faecalis that penetrated into the dentinal tubules using the bacterial culture assay and confocal laser scanning microscopy (CLSM). The null hypothesis of this study was that there is no significant difference in bactericidal effect among various TAP concentrations.
MATERIALS AND METHODS
The study protocol was approved by the Faculty of Dentistry and Faculty of Pharmacy, Mahidol University, Institutional Review Board (MU-DT/PY-IRB 2022/029.2705).
Tooth Selection
Single-rooted mandibular premolars, extracted from orthodontic reasons, were used. The root length was ≥10 mm from the cemento-enamel junction to the root apex. Teeth with root caries, root fractures, cracks, root resorption, existing crown restoration or previous endodontic treatment were excluded. Pre-operative radiographs (mesio-distal and bucco-lingual) of each tooth were taken. Teeth with multiple root canals or calcified canals on the radiographs were also excluded. The selected teeth were stored in 0.1% thymol until used.
Bacterial Strain and Culture
E. faecalis ATCC 29212 was used for the root canal and dentinal tubule contamination. The bacterial cells were grown on Brain Heart Infusion (BHI) agar plates and incubated at 37°C for 24 h (Heraeus B 5060 EK-CO2, Heraeus, Hanau, Germany). The bacterial inoculum was prepared by suspending 2–3 isolated E. faecalis colonies in BHI broth and incubating the broth at 37°C for 24 h. Prior to the experiment, the number of bacteria was adjusted to McFarland standard No.1 (3×108 CFU/mL) as measured from the turbidity of the cell suspension using a densitometer (DEN-1B densitometer, Bio San, Riga, Latvia).
TAP Preparation
The freshly mixed TAP was prepared from United States Pharmacopeia Convention (USP) grade powder of each antibiotic, i.e., minocycline, ciprofloxacin and metronidazole (Sigma Pharmaceutical, North Liberty, Iowa, USA). Macrogol and propylene glycol (MP) served as the drug vehicle. To prepare the initial concentration, 10 mg/ml TAP, 5 mg of each antibiotic powder was mixed in MP (M:P ratio = 1:1 by volume). The vehicle was gradually added into the mixture until reaching a final volume of 1.5 ml. Other concentrations were prepared by diluting the initial concentration in MP.
Tooth Preparation
The total of 91 teeth were used in this study. The calculus and soft tissue remnants on the root surfaces were removed using a periodontal curette. The teeth were cut using a diamond disc under water coolant 3 mm from the root apex. The teeth were cut 8 mm coronally from the new apex to obtain open-ended cylindrical root specimens. The root canal was sequentially enlarged with No. 1–3 peeso reamers (Dentsply Meillefer, USA). Irrigation was performed during canal enlargement with sterile normal saline solution to remove the dentine debris. The apical end was sealed with 2 mm resin composite (Filtek™ Z350 XT 3M ESPE, USA) with total etch bonding (Single Bond Universal, 3M ESPE, USA) to create a closed-end cylindrical tube. The smear layer was removed as previously described (14). The canals were dried with paper points before subjected to dentinal tubule contamination.
Dentinal Tubule Contamination
The specimens were sterilized by autoclaving (HICLAVE HVA-85, Hirayama, Saitama, Japan) for 20 min at 121°C. Each specimen was transferred to 1.5 ml-microcentrifuge tube (Costar®, Corning, New York, USA) containing 800 μl BHI broth and subjected to ultrasonic activation (B9500E–DTH, VWR International, USA) for 15 min to allow the culture medium to penetrate into the dentinal tubules. All specimens were incubated at 37°C for 24 h to confirm that they were sterile. E. faecalis contamination was created in the dentinal tubules as previously described (15). The protocol, including bacterial inoculation and medium replacement procedures, was completed in 4 d. The procedures were performed under aseptic conditions and the specimens were maintained at 37°C. Briefly, bacterial inoculation was performed on the 1st and the 3rd day, while the medium was replaced on the 2nd and 4th day. On the first day, after removing the BHI broth from each microcentrifuge tube containing the specimen, 800 μl bacterial suspension was added. All specimens were subjected to centrifugation (Eppendorf 5417C, Eppendorf AG, Hamburg, Germany) at 25°C, 1,400g, 2,000g, 3,600g and 5,600g, for 5 min each. At the end of each centrifugation step, 800 μl bacterial suspension added to the tube. Centrifugation was performed for 2 cycles. The specimens were incubated at 37°C for 24 h. The culture medium was replaced on the second day by adding 800 μl fresh BHI broth and centrifuging the tube at 25°C, 3,600g for 5 min. The specimens were incubated at 37°C for 24 h. The same procedure was repeated on the 3rd and the 4th day.
After bacterial contamination, one specimen was randomly selected to confirm the bacterial biofilm formation in the dentinal tubules using CLSM (Stellaris 8, Leica Microsystem, Wetzlar, Germany). The tooth was cross-sectionally cut by a diamond saw (Isomet 1000, Buhler, New York, USA) with copious irrigation with normal saline at the mid-root portion to obtain a 0.3 mm thick dentine disc. The disc was rinsed with 1% phosphate buffered saline under ultrasonic activation for 15 min to remove the smear layer. The disc was stained with 100 μl LIVE/DEAD® stain for 20 min. The LIVE/DEAD® stain contains SYTO 9® dye and propidium iodide (PI) dye, which stains the live and dead bacteria green and red, respectively.
Twenty X magnification was used in the scanning process. Four sequential images were taken from each disc with a resolution of 1024×1024 pixels on the diagonal sides of the root canal wall (Fig.1). These images were analysed with Leica Application Suite X (LAS X) software to quantify the amount of live (green) and dead (red) bacteria. The disc should have at least half of the analysed field showing live bacteria inside the tubules to confirm the success of the bacterial contamination method.
Experimental Groups and Medication Procedures
Ninety contaminated root specimens were randomly divided into 5 groups (n=18), negative control (no TAP), 1 mg/ml, 5 mg/ml, 7.5 mg/ml and 10 mg/ml TAP. The TAP was applied to the root canals in a laminar hood (NU-126-300E, NUAIRE, Minnesota, USA). Each specimen was removed from the microcentrifuge tube and the entire root canal was dried with marked sterile paper points. Eight μl TAP or vehicle alone was placed into the root canal using a micropipette. The orifice of each specimen was sealed with sterile PTFE tape and put in a new microcentrifuge tube. The specimens were incubated at 37°C in a humidified atmosphere for 3 weeks. Ten specimens from each group were subjected to the bacterial culture assay, while 8 specimens were subjected to CLSM for evaluating the presence of bacteria in the dentinal tubules.
Bacterial Culture Test
After a 3-week TAP treatment, the bacteria surviving in the root canals were determined. The PTFE tape was removed and 8 μl BHI broth was placed in the root canal. To collect the bacteria in the root canal space, a sterile paper point was placed at the working length for 1 min and then placed into a sterile glass tube containing 10 ml BHI broth. The bacteria in dentinal tubules at 100 μm and 200 μm depth were collected using a Gates-glidden drill (Dentsply Sirona, North Carolina, USA) No. 5 and 6, respectively. After the Gates-glidden drill was applied at the working length at 1,000 rpm, a sterile paper point was then placed at the working length for 1 min to collected the remaining dentine chip. Each Gates-glidden drill and paper point were transferred to a tube containing BHI broth. The tubes were vortexed for 1 min and incubated at 37°C for 1 week. Bacterial growth, indicated by the turbidity of the BHI broth, was evaluated every day. The positive samples were cultured and the presence of E. faecalis was confirmed by colony morphology, gram stain and bile esculin assay.
LIVE/DEAD Assay by CLSM
To investigate the presence of bacteria in the dentinal tubules, eight specimens from each group were subjected to the LIVE/DEAD assay using CLSM. The images from four areas of interest were captured and analysed as described above. The mean percentage of live cells in each group (n=8) were reported. The percentage of live bacteria was calculated using the following equation:
Statistical Analysis
The data were analysed using SPSS version 23.0.0.0 (SPSS Inc., IL, USA). The bactericidal effect of TAP was evaluated using the Chi-square test to compare the number of positive samples between the different drug concentrations at each depth. The CLSM data were analysed by linear regression. The significance level was set at p<0.05.
RESULTS
Confirmation of Bacterial Contamination in the Dentinal Tubules
One root sample was randomly selected for CLSM after the contamination process to confirm the presence of bacteria in the dentinal tubules. The green signals (SYTO9) represented live bacterial cells and the red signals (PI) represented dead cells (Fig. 2). Live bacteria were present in more than half of the analysed field, confirming the success of the bacterial contamination method. Moreover, the depth of bacterial penetration in the dentinal tubules was at least 500 μm.
Figure 2.

CLSM images of the root sample after bacterial contamination. The red color (PI) represents dead bacterial cells, while the green color (SYTO9) represents live bacterial cells
Figure 1.
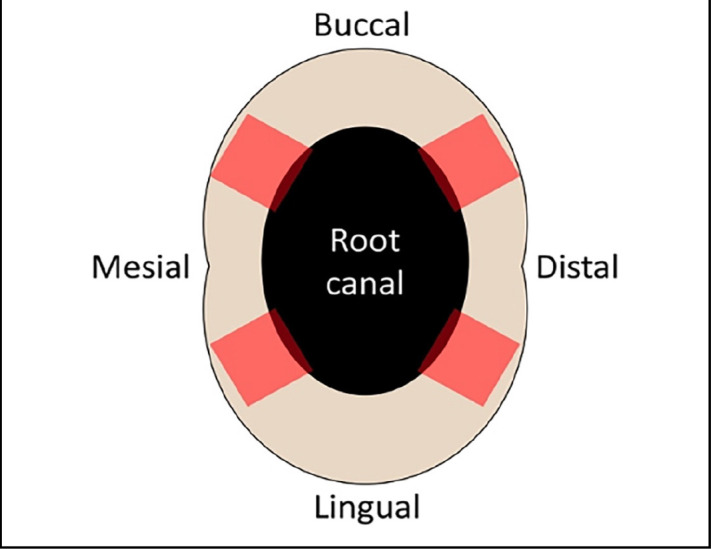
The schematic illustration showed four diagonal sides (red area) of the root canal wall that were captured for CLSM analysis.
CLSM: Confocal laser scanning microscope
Bactericidal Effect of TAP against E. faecalis
After treating the infected root canal with 1–10 mg/ml TAP, samples from the root canal and 100 μm and 200 μm deep into the dentinal tubules were collected for detecting the viable bacteria using the bacterial culture assay. The number of culturable samples in each group are displayed in Table 1. All negative control samples (no TAP) were culturable and contained E. faecalis. In contrast, no culturable sample was found at 10 mg/ml TAP. At lower TAP concentrations were used, the number of culturable samples varied. TAP at 7.5 mg/ml had no culturable samples from the dentinal tubules, and 1 culturable sample from the root canal. Similar results were observed from 1 mg/ml and 5 mg/ml TAP that had 2 culturable samples from the root canals and 1 sample from 200 µm deep into root dentine. The number of culturable samples among the experiment groups in each depth were similar (p>0.05).
TABLE 1.
The number of culturable samples in each experimental group and depth (n=10)
| Experimental groups (n=10) | Number of culturable samples | ||
|---|---|---|---|
| Root canal | 100 µm | 200 µm | |
| Neg control (No TAP) | 10 | 10 | 10 |
| 1 mg/ml TAP | 2 | 0 | 1 |
| 5 mg/ml TAP | 2 | 0 | 1 |
| 7.5 mg/ml TAP | 1 | 0 | 0 |
| 10 mg/ml TAP | 0 | 0 | 0 |
The LIVE/DEAD assay revealed the mean percentage of live bacteria in each experimental group (Fig. 3). Ten mg/ml TAP exhibited the lowest percentage of live cells (40.58±5.40%), followed by 7.5 mg/ml (44.14±6.03%), 5 mg/ml (46.31±5.32%) and 1 mg/ml TAP (52.55±8.82%). The percentage of live cells in the 10 mg/ml, 7.5 mg/ml and 5 mg/ml TAP groups were significantly lower than the 1 mg/ml TAP and the negative control group (52.36±3.24) (p<0.05). There were no significant differences among the 5, 7.5 and 10 mg/ml TAP groups. The representative CLSM PI, SYTO9 and merged images are shown in Figure 4. More intense red fluorescent signals were detected in the 5 mg/ml, 7.5 mg/ml and 10 mg/ml TAP groups compared with the 1 mg/ml TAP and the negative control groups.
Figure 3.

Mean percentage (±SD) of live bacteria in the root canal dentine obtained from various concentrations of TAP medication. Superscript A and B indicate significant differences among the groups (p<0.05)
TAP: Triple antibiotic paste
Figure 4.

Representative CLSM images of live and dead bacteria in the root canal dentine obtained from various concentrations of TAP medication. The red color (PI) represents dead bacterial cells, while the green color (SYTO9) represents live bacterial cells
DISCUSSION
TAP has demonstrated the bactericidal efficacy by completely eradicating E. faecalis in infected root canals (9, 10). However, high TAP concentration showed cytotoxicity to stem cells, which might affect the success of regenerative endodontic procedures (11). Therefore, the aim of this study was to determine the optimal concentration that can eliminate E. faecalis in the root canal. From our results, the null hypothesis is rejected.
Although the antibacterial effect of the antibiotics in TAP has been shown by the standard antimicrobial susceptibility tests, e.g. agar diffusion, these methods do not mimic their antibacterial effect exerted in endodontic infections. The bacteria colonize the root canal wall and penetrate into the dentinal tubules, which might impair the bactericidal effect of antibiotics. Moreover, the mixed bacterial species form biofilms that can tolerate medications via numerous drug resistant mechanisms, including protection from drug penetration, gene transfer, and slow growth or moving into the stationary phase (16). Therefore, the specimens from extracted human teeth and the dentinal tubule contamination method were used in current study (15). This method simulates dentinal tubule contamination more quickly compared with the traditional bacterial contamination that requires 21–30 d. Moreover, high percentage of live bacteria and deeper penetration of bacterial cells in the dentinal tubules were achieved.
The CLSM results revealed the colonization of E. faecalis on the root canal walls and the presence of the bacteria equally distributed in the dentinal tubules more than 500 μm deep. In contrast, a study using the traditional contamination method had less penetration depth and the bacteria were mostly accumulated at the superficial root canal dentine (17). Furthermore, this study found a slightly lower percentage of live bacterial cells compared with other studies that used the dentinal bacterial contamination method (18–20). These differences might be due to the type of the teeth and incubation time used between studies. To the best of our knowledge, our study is the first to use human teeth instead of bovine teeth. These tooth types differ in the size and the density of the dentinal tubules (21, 22). The dentinal tubules in human teeth near the pulp side are generally larger and fewer than those in bovine teeth. Moreover, the fewer live cells in our study might be due to the 3-week incubation time after TAP treatment. A previous study demonstrated the presence of starved bacterial cells after 3 weeks of incubation (17).
The bacterial culture assay was used evaluate the efficiency of various TAP concentrations to eradicate E. faecalis in the root canal and dentinal tubules. No culturable samples were detected in the 10 mg/ml TAP group, which corresponded to other studies where 10 mg/ml and higher TAP concentrations eliminated E. faecalis biofilm (9, 12, 23). Two (20%) root canal samples treated with 1 mg/ml and 5 mg/ml TAP demonstrated incomplete E. faecalis elimination. Another study also found complete eradication of E. faecalis biofilm after direct contact with 1 mg/ml TAP (12). In addition, only 1 (10%) root canal sample treated with 7.5 mg/ml TAP showed incomplete E. faecalis elimination. There is no report on the bactericidal activity of 1–10 mg/ml TAP.
Regarding the bacterial penetration depth, some culturable samples were detected from the samples collected 200 μm into the dentine. These might due to the varying concentration of TAP and the number of bacteria in the root canal and dentine. In the deeper dentine (200 μm), although the number of penetrated bacteria is less, the TAP concentration of TAP might also be lower based on the distance from the root canal. Thus, TAP could not effectively kill the bacteria 200 μm deep into root dentine. It is also possible that the number of bacteria introduced in dentine by centrifugation was greater than those present in clinical infections. At 100 μm deep, there were no culturable samples, indicating the optimal concentration of TAP that effectively eradicated the bacteria present. Dentine samples more than 200 μm deep could not be collected due to the thin dentine on the mesial-distal side of the root.
Surprisingly, CLSM revealed the presence of live E. faecalis in all samples. The TAP treatment results demonstrated decreased live bacteria inside the dentinal tubules in a dose-dependent manner. At the lowest concentration, 1 mg/ml TAP, the percentage of live cells was similar to the negative control. However, the culture test results indicated that only a few samples were culturable. The possible explanation may be that E. faecalis can adapt into a viable, but nonculturable (VBNC), state when exposed to some environmental stresses, and can be resuscitated later in a suitable environment (24). Previous studies indicated that E. faecalis entered a VBNC state within 2 weeks and remained viable for at least 2 months (25, 26). When entering the VBNC state, the E. faecalis shape changed from coccoid to irregular, and it lost its ability to break down lactose, D-mannitol and D-sorbitol (24). Furthermore, the cells can still attach to dentine and Type I collagen fibres, but cannot penetrate the dentinal tubules (25). These situations might lower the pathogenicity of the bacteria; however, the resuscitated cells can initiate infection after recovery. However, some antibiotics can block the bacterial resuscitation processes, either directly or by binding to a molecule that mediates resuscitation (27). From the result of bacteria culture test, E. faecalis in the dentinal tubules might entered a VBNC state and TAP treatment might block E. faecalis resuscitation as indicated by the nonculturable samples.
To the best of knowledge, this is the first study that used the dentinal tubule contamination method to evaluate the antimicrobial effect of TAP. Although TAP, including at low concentration (1 mg/ml), inhibited the growth of E. faecalis in the dentinal tubules, whether the bacterial cells in the dentinal tubules are in a VBNC state remains to be elucidated. Residual TAP after treatment and its cytotoxic effect should be investigated to minimize the adverse effects of TAP before initiating the regeneration processes. Moreover, the limitation of this study is the utilisation of monospecies biofilm which may not accurately replicate the complexity of polymicrobial infections observed in clinical situation.
CONCLUSION
This study found that 1, 5, 7.5 and 10 mg/ml TAP markedly decreased the number of culture-positive root canal samples. Moreover, the bactericidal effect of TAP in the dentinal tubules was dose-dependent. However, CLSM revealed remaining live bacteria in the dentinal tubules of all specimens.
Footnotes
Please cite this article as: Thasanakit A, Kaewprag J, Srisatjaluk R. Bactericidal Effect of Triple Antibiotic Paste against Enterococcus faecalis in Dentinal Tubules: An Ex Vivo Study. Eur Endod J 2024; 9: 161-6
Disclosures
Acknowledgements
We would like to express our gratitude for Dr. Sittichoke Osiri (Department of Operative Dentistry and Endodontics, Faculty of Dentistry, Mahidol University, Thailand) for his kind assistance in statistical analysis.
Ethics Committee Approval
The study was approved by the Faculty of Dentistry and Faculty of Pharmacy, Mahidol University Ethics Committee (no: MU-DT/PY-IRB 2022/029.2705, date: 27/05/2022).
Authorship Contributions
Concept – J.K.; Design – J.K., R.S.; Supervision – J.K., R.S.; Funding – J.K., R.S.; Materials – J.K., R.S.; Data collection and/or processing – A.T.; Data analysis and/or interpretation – A.T., J.K., R.S.; Literature search – A.T.; Writing – A.T., J.K., R.S.; Critical review – A.T., J.K., R.S.
Conflict of Interest
All authors declared no conflict of interest.
Use of AI for Writing Assistance
Not declared.
Financial Disclosure
This study was supported by research grant for residency training program, Faculty of Dentistry, Mahidol University, Thailand.
Peer-review
Externally peer-reviewed.
References
- 1.Myers WC, Fountain SB. Dental pulp regeneration aided by blood and blood substitutes after experimentally induced periapical infection. Oral Surg Oral Med Oral Pathol. 1974;37(3):441–50. doi: 10.1016/0030-4220(74)90119-4. [DOI] [PubMed] [Google Scholar]
- 2.Althumairy RI, Teixeira FB, Diogenes A. Effect of dentin conditioning with intracanal medicaments on survival of stem cells of apical papilla. J Endod. 2014;40(4):521–5. doi: 10.1016/j.joen.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 3.Evans M, Davies JK, Sundqvist G, Figdor D. Mechanisms involved in the resistance of Enterococcus faecalis to calcium hydroxide. Int Endod J. 2002;35(3):221–8. doi: 10.1046/j.1365-2591.2002.00504.x. [DOI] [PubMed] [Google Scholar]
- 4.McHugh CP, Zhang P, Michalek S, Eleazer PD. pH required to kill Enterococcus faecalis in vitro. J Endod. 2004;30(4):218–9. doi: 10.1097/00004770-200404000-00008. [DOI] [PubMed] [Google Scholar]
- 5.Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod. 2004;30(4):196–200. doi: 10.1097/00004770-200404000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Sato I, Ando-Kurihara N, Kota K, Iwaku M, Hoshino E. Sterilization of infected root-canal dentine by topical application of a mixture of ciprofloxacin, metronidazole and minocycline in situ. Int Endod J. 1996;29(2):118–24. doi: 10.1111/j.1365-2591.1996.tb01172.x. [DOI] [PubMed] [Google Scholar]
- 7.Hoshino E, Kurihara-Ando N, Sato I, Uematsu H, Sato M, Kota K, et al. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int Endod J. 1996;29(2):125–30. doi: 10.1111/j.1365-2591.1996.tb01173.x. [DOI] [PubMed] [Google Scholar]
- 8.Abbaszadegan A, Dadolahi S, Gholami A, Moein MR, Hamedani S, Ghasemi Y, et al. Antimicrobial and cytotoxic activity of cinnamomum zeylanicum, calcium hydroxide, and triple antibiotic paste as root canal dressing materials. J Contemp Dent Pract. 2016;17(2):105–13. doi: 10.5005/jp-journals-10024-1811. [DOI] [PubMed] [Google Scholar]
- 9.Frough Reyhani M, Rahimi S, Fathi Z, Shakouie S, Salem Milani A, Soroush Barhaghi MH, et al. Evaluation of antimicrobial effects of different concentrations of triple antibiotic paste on mature biofilm of Enterococcus faecalis. J Dent Res Dent Clin Dent Prospects. 2015;9(3):138–43. doi: 10.15171/joddd.2015.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sabrah AH, Yassen GH, Liu WC, Goebel WS, Gregory RL, Platt JA. The effect of diluted triple and double antibiotic pastes on dental pulp stem cells and established Enterococcus faecalis biofilm. Clin Oral Investig. 2015;19(8):2059–66. doi: 10.1007/s00784-015-1423-6. [DOI] [PubMed] [Google Scholar]
- 11.Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A. Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod. 2012;38(10):1372–5. doi: 10.1016/j.joen.2012.06.018. [DOI] [PubMed] [Google Scholar]
- 12.Alyas SM, Fischer BI, Ehrlich Y, Spolnik K, Gregory RL, Yassen GH. Direct and indirect antibacterial effects of various concentrations of triple antibiotic pastes loaded in a methylcellulose system. J Oral Sci. 2016;58(4):575–82. doi: 10.2334/josnusd.16-0384. [DOI] [PubMed] [Google Scholar]
- 13.Zancan RF, Cavenago BC, Oda DF, Bramante CM, Andrade FB, Duarte MAH. Antimicrobial activity and physicochemical properties of antibiotic pastes used in regenerative endodontics. Braz Dent J. 2019;30(6):536–41. doi: 10.1590/0103-6440201902613. [DOI] [PubMed] [Google Scholar]
- 14.Haapasalo M, Orstavik D. In vitro infection and disinfection of dentinal tubules. J Dent Res. 1987;66(8):1375–9. doi: 10.1177/00220345870660081801. [DOI] [PubMed] [Google Scholar]
- 15.Andrade FB, Arias MP, Maliza AG, Duarte MA, Graeff MS, Amoroso-Silva PA, et al. A new improved protocol for in vitro intratubular dentinal bacterial contamination for antimicrobial endodontic tests: standardization and validation by confocal laser scanning microscopy. J Appl Oral Sci. 2015;23(6):591–8. doi: 10.1590/1678-775720140261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sharma D, Misba L, Khan AU. Antibiotics versus biofilm: an emerging battleground in microbial communities. Antimicrob Resist Infect Control. 2019;8:76. doi: 10.1186/s13756-019-0533-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Smittiset B, Banomyong D, Ruangsawasdi N, Kaewprag J. In vitro bactericidal efficacy of a new triple antibiotic paste formulation against Enterococcus faecalis biofilm. Aust Endod J. 2022 Sep 8; doi: 10.1111/aej.12683. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 18.Pereira TC, da Silva Munhoz Vasconcelos LR, Graeff MSZ, Ribeiro MCM, Duarte MAH, de Andrade FB. Intratubular decontamination ability and physicochemical properties of calcium hydroxide pastes. Clin Oral Investig. 2019;23(3):1253–62. doi: 10.1007/s00784-018-2549-0. [DOI] [PubMed] [Google Scholar]
- 19.de Andrade FB, da Silva Munhoz Vasconcelos LR, Pereira TC, Garcia RB, Bramante CM, Duarte MAH. Ultrasonic agitation reduces the time of calcium hydroxide antimicrobial effect and enhances its penetrability. J Mater Sci Mater Med. 2021;32(12):150. doi: 10.1007/s10856-021-06607-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lei L, Shao M, Yang Y, Mao M, Yang Y, Hu T. Exopolysaccharide dispelled by calcium hydroxide with volatile vehicles related to bactericidal effect for root canal medication. J Appl Oral Sci. 2016;24(5):487–95. doi: 10.1590/1678-775720160014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schilke R, Lisson JA, Bauss O, Geurtsen W. Comparison of the number and diameter of dentinal tubules in human and bovine dentine by scanning electron microscopic investigation. Arch Oral Biol. 2000;45(5):355–61. doi: 10.1016/s0003-9969(00)00006-6. [DOI] [PubMed] [Google Scholar]
- 22.Lopes MB, Sinhoreti MA, Gonini Junior A, Consani S, McCabe JF. Comparative study of tubular diameter and quantity for human and bovine dentin at different depths. Braz Dent J. 2009;20(4):279–83. doi: 10.1590/s0103-64402009000400003. [DOI] [PubMed] [Google Scholar]
- 23.Zargar N, Rayat Hosein Abadi M, Sabeti M, Yadegari Z, Akbarzadeh Baghban A, Dianat O. Antimicrobial efficacy of clindamycin and triple antibiotic paste as root canal medicaments on tubular infection: An in vitro study. Aust Endod J. 2019;45(1):86–91. doi: 10.1111/aej.12288. [DOI] [PubMed] [Google Scholar]
- 24.Oliver JD. The viable but nonculturable state in bacteria. J Microbiol. 2005;43:93–100. [PubMed] [Google Scholar]
- 25.E J, Jiang YT, Yan PF, Liang JP. Biological changes of Enterococcus faecalis in the viable but nonculturable state. Genet Mol Res. 2015;14(4):14790–801. doi: 10.4238/2015.November.18.44. [DOI] [PubMed] [Google Scholar]
- 26.Lleo MM, Bonato B, Tafi MC, Signoretto C, Boaretti M, Canepari P. Resuscitation rate in different enterococcal species in the viable but non-culturable state. J Appl Microbiol. 2001;91(6):1095–102. doi: 10.1046/j.1365-2672.2001.01476.x. [DOI] [PubMed] [Google Scholar]
- 27.Lleo MM, Benedetti D, Tafi MC, Signoretto C, Canepari P. Inhibition of the resuscitation from the viable but non-culturable state in Enterococcus faecalis. Environ Microbiol. 2007;9(9):2313–20. doi: 10.1111/j.1462-2920.2007.01345.x. [DOI] [PubMed] [Google Scholar]