

Abstract
Osteochondromas are a common type of benign primary bone tumor rarely occurring in the scapula. When it is symptomatic, surgical removal is recommended. There are multiple approaches for surgical excision that can be used depending on the location and size of the tumor. We present a case of a 14-year-old female who was seen in the orthopedic clinic with right shoulder pain, mechanical symptoms and medial scapular winging due to a superomedial osteochondroma of the scapula. A novel superior approach to the superomedial ventral surface of the scapula was utilized to excise the tumor with good clinical results.
Keywords: osteochondroma, scapula, superomedial
Introduction
Osteochondromas are the most common benign primary bone tumor, typically occurring in long bones such as the proximal humerus, proximal tibia and the distal femur. Neoplasms of the scapula are rare in general and osteochondromas are the most common neoplasm of the scapula [1]. Multiple case reports and series site 3–6% as the proportion of osteochondromas that occur in the scapula however there are no large studies that have established an accepted incidence [2]. In some cases, osteochondromas of the scapula can cause pain, mechanical symptoms including scapula winging and rarely neurovascular impingement necessitating removal. Because these lesions are rare, there is little literature describing approaches to their unique locations.
For symptomatic osteochondromas of the scapula, as is the case with symptomatic osteochondromas elsewhere in the body, surgical removal remains the treatment of choice [3]. Based on the size and location of the tumor, there are different surgical approaches for excision. Scapula osteochondromas can be broadly divided into dorsal or ventral, with ventral being more common. Dorsal osteochondromas are relatively more straightforward as a direct incision is typically sufficient to expose the mass [4]. Ventral osteochondromas are predictably more complicated to access. Approaches can be divided into roughly three major categories: muscle saving, muscle detaching, and arthroscopic- or endoscopic-assisted techniques. Based on a review of the literature and the available described cases, the majority of ventral scapular osteochondromas are approached through an inferior or paramedial approach to the scapula [5]. There are few reported cases of superior medial osteochondromas, and no cases, to the authors knowledge, describe a purely superior approach to the superior medial scapula [6, 7]. Here we present a case of a patient with a superomedial osteochondroma of the scapula that necessitated a novel muscle sparing superior approach.
Case report
Here we describe a case of a 14-year-old healthy female who was referred to the orthopedic clinic reporting a 1-year history of right shoulder pain with mechanical locking symptoms. She noted discomfort and significant crepitus with shoulder abduction and overhead activities. She also noted a palpable deformity over the superior medial aspect of her shoulder. She was fully neurologically intact to her right upper extremity and her vascular exam was unremarkable. X-rays and a computed tomography scan were performed which demonstrated an osseous lesion at the superomedial ventral surface of the right scapula with cortical continuity with an associated cartilaginous cap, consistent with an osteochondroma (Fig. 1). A thorough discussion was held with the patient and her mother regarding treatment options and the decision was made to proceed with osteochondroma excision.
Figure 1.
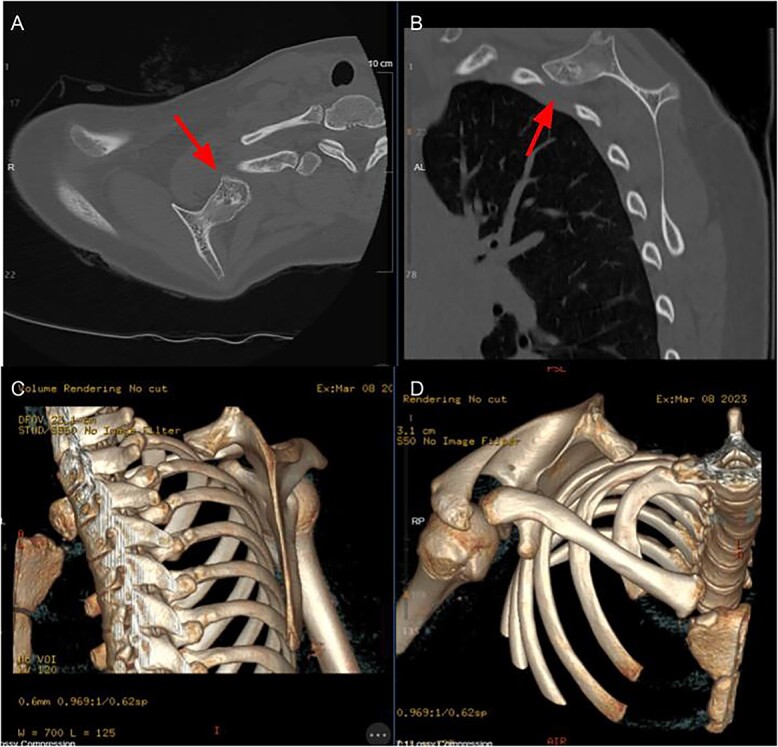
Axial (A) and sagittal (B) CT slices demonstrating lesion location, 3D reconstructions (C + D) further demonstrating morphology of lesion.
The patient was placed in the prone position on the operating table. The entire right upper extremity was draped including the entire right scapula area (Fig. 2). Fluoroscopy was used to identify the lesion and mark our planned surgical incision. A 5-cm transverse incision was made along the superior aspect of the bony lesion in line with the underlying trapezius muscle fibers.
Figure 2.

Demonstration of position and marking of the patient.
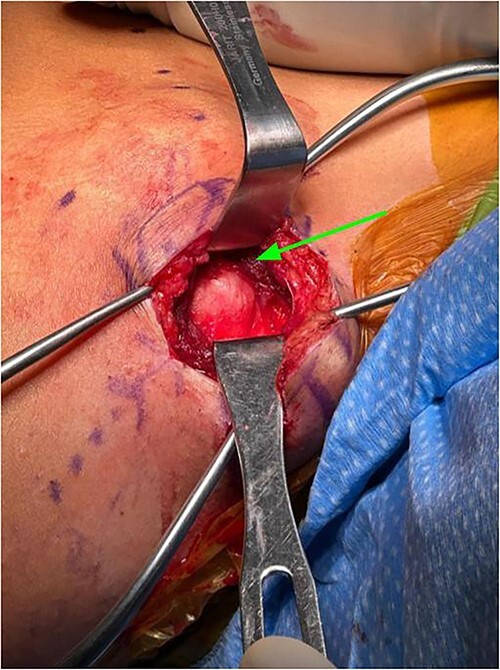
Subcutaneous tissue was divided with the electrocautery. Investing fascia over the trapezius was identified and the division between the superior and middle fibers of the trap was identified. The raphe between the superior and middle fibers was then bluntly spread in line (Fig. 3). We then encountered the superior aspect of the ventral lesion on the scapula (Fig. 4). Of note, the majority of levator scapulae fibers were medial to this lesion; however, the most lateral portion of the muscle was overlying the lesion. These lateral fibers were spread in line to expose the pedunculated mass. Blunt dissection was then taken circumferentially around the stalk of the mass to ensure all soft tissue had been freed from the area (Fig. 5). An osteotome was then carefully placed within the wound at the base of the stalk, and the tumor was then removed and sent to pathology for analysis. The stalk remnant was then filed down to a smooth and stable base with a rasp without any significant areas of potential irritation or prominence. The wound was then copiously irrigated with normal saline. Fluoroscopy images demonstrated complete resection of the bony tumor. There was no active bleeding within the wound. The fascia overlying the trapezius muscle and the skin were then closed.
Figure 3.

Exposure after superficial dissection, middle trapezius fibers (top arrow) and superior trapezius fibers (bottom arrow).
Figure 4.
Exposure after trapezius had been split between middle and superior fibers, levator scapula fibers can be seen medial to lesion (identified by arrow).
Figure 5.

Exposure after scapula has been retracted and lesion was exposed, lesion can be directly visualized.
The specimen was sent for pathologic evaluation which resulted in findings consistent with osteochondroma. The patient was followed in the orthopedic clinic post operatively for 6 months. She reported no wound complications, paresthesias or weakness of the right upper extremity. She was started in physical therapy and regained full right shoulder range of motion and strength that was symmetric to her contralateral shoulder by 3 months post operatively.
Discussion
Scapula osteochondromas are rare and literature guiding management is lacking. Here we describe a unique case of a superomedial osteochondroma that was excised through a novel transverse muscle sparing incision over the superior medial corner of the scapula. Ventral osteochondromas of the scapula, when described, are typically managed through an inferior or paramedial approach to the scapula. The superomedial corner of the scapula poses a challenge as there are few described approaches to this region as described scapula approaches, such as the Judet approach, are typically for access to the body of the scapula for fracture management [8]. This paper serves to illustrate a safe and effective approach to the superior medial border of the scapula for osteochondroma excision without detaching any muscle insertions such as the levator scapular or rhomboids.
Contributor Information
Dylan H Shafer, Department of Orthopaedic Surgery, Community Memorial Hospital, 147 N. Brent St, Ventura, CA 93003, United States.
Emilio L Robles, Department of Orthopaedic Surgery, Community Memorial Hospital, 147 N. Brent St, Ventura, CA 93003, United States.
Catherine M Linsley, Department of College of Osteopathic Medicine, Lake Erie College, 1858 W. Grandview Blvd, Erie, PA 16509, United States.
Ashley N Lamb, Department of Orthopaedic Surgery, Community Memorial Hospital, 147 N. Brent St, Ventura, CA 93003, United States.
Conflict of interest statement
None declared.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Consent
Written and verbal consent were obtained from the patient for publication of this case, clinical findings and related images. Written consent is available to the Editor-In-Chief upon request.
References
- 1. Blacksin MF, Benevenia J. Neoplasms of the scapula. Am J Roentgenol 2000;174:1729–35. 10.2214/ajr.174.6.1741729. [DOI] [PubMed] [Google Scholar]
- 2. Shahid O, Shahid M, Shaik L, et al. Rare case of osteochondroma on the dorsal aspect of the scapula. Cureus 2021;13:e17051. 10.7759/cureus.17051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Vaishya R, Dhakal S, Vaish A. A solitary osteochondroma of the scapula. Case Rep 2014;2014:bcr2013202273. 10.1136/bcr-2013-202273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bektas YE, Ozmanevra R. An unusual location of osteochondroma: dorsal scapula. Cureus 2019;11:e6464. 10.7759/cureus.6464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Prakash S, Kalra P, Khan Y, et al. Ventral scapular osteochondroma excision through ‘triangle of auscultation’: a case series. J Orthop Surg 2020;28:230949901989284. 10.1177/2309499019892848. [DOI] [PubMed] [Google Scholar]
- 6. Sivananda P, Rao BK, Kumar PV, et al. Osteochondroma of the ventral scapula causing scapular static winging and secondary rib erosion. J Clin Diagn Res JCDR 2014;8:LD03–5. 10.7860/JCDR/2014/8129.4335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Faur C, Abu-Awwad A, Patrascu JM, et al. Superomedial scapula angle osteochondroma with winging in a young female patient—case report and literature review. J Clin Med 2023;12:5106. 10.3390/jcm12155106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cole PA, Dugarte AJ. Posterior scapula approaches: extensile and modified Judet. J Orthop Trauma 2018;32:S10–1. 10.1097/BOT.0000000000001208. [DOI] [PubMed] [Google Scholar]