

Abstract
Background
Quality cancer care necessitates opportunities for patient participation, supposedly recognizing the individual's preferences and experiences for being involved in their health and healthcare issues. Previous research shows that surgical cancer patients wish to be more involved, requiring professionals to be sensitive of patients' needs.
Aims
To explore preference‐based patient participation in surgical cancer care.
Methods
A cross‐sectional study was conducted. The Patient Preferences for Patient Participation tool (4Ps) was used, which includes 12 attributes of preferences for and experiences of patient participation. Data were analyzed with descriptive and comparative statistical methods.
Results
The results are based on a total of 101 questionnaires. Having reciprocal communication and being listened to by healthcare staff were commonly deemed crucial for patient participation. While 60% of the patients suggested that taking part in planning was crucial for their participation, they had experienced this only to some extent. Learning to manage symptoms and phrasing personal goals were items most often representing insufficient conditions for preference‐based patient participation.
Linking Evidence to Action
To support person‐centered surgical care, further efforts to suffice preference‐based participation are needed, including opportunities for patients to share their experiences and engage in the planning of healthcare activities.
Keywords: cancer care, involvement, patient participation, patient preferences, person‐centered care, surgical care
INTRODUCTION
Patient participation is highly important for numerous reasons (World Health Organization, 2013); for example, it is associated with improved recovery, treatment outcomes, and rehabilitation (Arnetz et al., 2004), as well as increased motivation, better treatment outcomes, and greater satisfaction with the given care (Vahdat et al., 2014). Many countries, including Sweden, encourage patient participation by means of legislations and standards (Nolte et al., 2020). Yet, even if patient participation is advocated throughout health care, it comes with a varying conceptualization (Cahill, 1996; Larsson et al., 2011; Longtin et al., 2010; Sahlsten et al., 2008). For person‐centered health care to be provided, patient participation should be defined with recognition to semantic, ethical, and conceptual perspectives, including patients' experience of the phenomenon (Eldh et al., 2010; Finset, 2017). More recent research suggests a wider understanding of the concept than what health professionals may think, including that patient participation comprises a mutual sharing of experiences, engaging in self‐care activities, in addition to being involved in planning and procedures (Årestedt et al., 2019; Kvæl et al., 2018; Nilsson et al., 2019;). A further need to better understand patients' preferences for participation remains, including to what extent and in what way patients wish to engage. This is vital both to facilitate person‐centered care and to utilize healthcare resources more efficiently, including staff time and efforts to match patients' needs and conditions (Eldh, 2019; Nolte et al., 2020).
Patients with cancer in the liver, bile ducts, or pancreas are a very vulnerable patient group with a tough situation. The patients often experience a lot of symptoms both prior to surgery and in the postoperative phase. The surgery and stress from the situation cause great stress to the body, and it often takes 2 months (or more) before the patient begins to feel fully recovered after the surgical treatment. Major surgeries are associated with pain, nausea, fatigue, postoperative ileus, and postoperative complications. Further, because of shorter hospital stays, these patients need strong self‐care abilities to cope with the symptoms and minimize the risks of complications; sometimes, the self‐care even includes managing their own wound drains at home (Ibrahim et al., 2019; Kehlet & Wilmore, 2008). Nevertheless, most patients with pancreatic cancer have been found to prefer surgery rather than palliative chemotherapy considering the possibility of cure and potential risks (Molinari et al. 2020). Consequently, patients should have opportunities to participate, that is, to engage in discussing their treatment options (Dumitra et al., 2021).
Previous studies among patients who had surgery for liver, bile ducts or pancreas cancer have suggested the need for further improvements regarding patient participation (Ibrahim et al., 2019; Larnebratt et al., 2019). Ibrahim et al. (2019) found that even when patients had received information preoperatively, they felt that the provision of the information in a single event could be overwhelming. Currently, limited attention is given to patient participation consistent with the needs and resources of the individual, that is, preference‐based patient participation, among patient groups undergoing surgery for upper abdominal cancer. Rather, previous studies have shown that patients favor more information and the visibility of care goals and planning during the surgical cancer care period (Ibrahim et al., 2019; Larnebratt et al., 2019). Even though healthcare professionals in surgical cancer care also rate the provision of information as the most important issue for patient participation, they often lack the time to provide the information, as the prioritization of other work activities hampers an ideal situation of patient participation (Andersson et al., 2021).
Consequently, professionals can provide more ideal conditions for patients to partake in health and healthcare‐related matters according to their participation preferences (Eldh et al., 2010). Surgical cancer patients have been found to desire more involvement, calling for a need for professionals to be sensitive to patients' participation preferences (Ibrahim et al., 2019; Larnebratt et al., 2019; Molinari et al. 2020). Yet, there is a knowledge gap and paucity of studies concerning the extent to which patients experience preference‐based patient participation in surgical cancer care. To better meet the needs of patients with malignant tumors in the liver, bile ducts, pancreas, or stomach, further studies on their preferences for and experiences of participation when treated with curative elective cancer surgery are recommended.
Aim
This study explored preference‐based patient participation in surgical cancer care via two research questions:
What are the patients' views regarding preferences and experiences of their patient participation?
What are the patients' levels of preference‐based patient participation?
METHODS
Design
A cross‐sectional quantitative study was conducted.
Ethics
The study was performed in accordance with the ethical principles of the Declaration of Helsinki (World Medical Association, 2013), and approved by the Regional Ethics Review Board (No. 2018/413–32).
Setting, Sample, and Data Collection.
The patients were recruited from one university hospital in Sweden with a catchment area of about 1‐million inhabitants. A consecutive selection procedure was used for the inclusion of patients who underwent surgery for upper abdominal cancer in a specialist surgery clinic between May 2019 and March 2020.
The inclusion criteria were patients over 18 years of age with malignant tumors in the liver, bile ducts, pancreas, or stomach who were treated with curative elective cancer surgery. The exclusion criteria were patients with cognitive impairment or who did not have mastery of the Swedish language (determined by a research nurse). The patient selection and data collection process are illustrated in Figure 1. No patients were recruited in July 2019 due to logistical issues, that is, few patients were admitted during this common summer holiday month.
FIGURE 1.
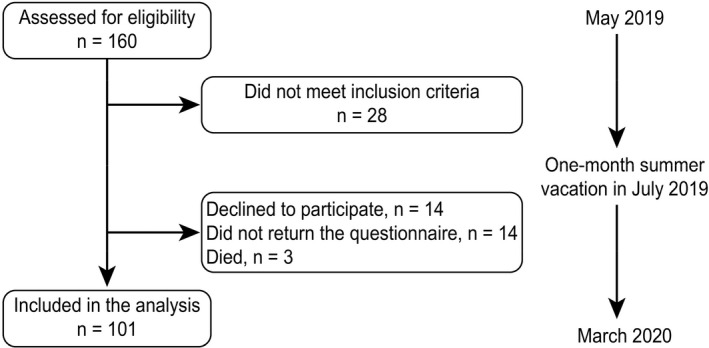
Flowchart of the inclusion process
One‐hundred and thirty‐two patients provided informed consent and were included in the study. These patients received the Patient Preferences for Patient Participation tool (4Ps) via regular mail 2–3 weeks after their discharge, along with a prepaid return envelope. Reminders were sent to non‐respondents one week later.
Measure
Per contemporary evidence, the 4Ps comprise 12 attributes conceptualizing patient participation (Eldh et al., 2015). The 4Ps are valid and appropriate for conceptualizing patient participation (Eldh et al., 2015; Luhr et al., 2018; Luhr et al., 2019) and deemed relevant for capturing patient preferences for engagement (Jerofke‐Owen et al., 2020).
The 4Ps consists of two sections, which were completed jointly in this study. Both sections employ the 12 items, presented in the following order: being listened to (by the healthcare staff); one's experiences being recognized; having reciprocal communication; telling about (my) symptoms/issues; having explanations as for one's symptoms/issues; having explanations for what is done/planned; partaking in planning; phrasing one's (health) goals; knowing how to manage symptoms/issues; managing (prescribed) treatment/procedures; and performing self‐care.
When completing the 4Ps, in section 1, the patient indicates the extent to which each item represents his or her preferences for patient participation using one of four response alternatives: that the attribute is “unimportant,” “somewhat important,” “very important,” or “crucial” (for me to experience participation).
In section 2, the patient defines the extent to which he or she has experienced patient participation. For each attribute, the patient conveys whether this occurred “not at all,” “to some extent,” “to a large extent,” or “entirely.”
Statistical analysis
The demographic variables were presented as descriptive statistics with counts and proportions. All patients' preferences and experiences were presented as proportions. Analyzed together, these responses provided a measure of preference‐based patient participation (Eldh et al., 2020). To assess whether the responses in sections 1 and 2 indicated “good” conditions for patient participation, the degree to which the patient's responses for each item matched or mismatched between the two sections was determined. The higher the match between the response alternative for each item, the more preference‐based patient care. The match scores were categorized into three levels of preference‐based patient participation, as outlined in Figure 2:
Insufficient provision of preference‐based patient participation, calling for significant improvement (levels 0–1),
Fair provision, indicating room and need for improvement (levels 2–3), and
Sufficient provision, signifying a complete or near match between patient preferences and experiences (levels 4–5).
FIGURE 2.
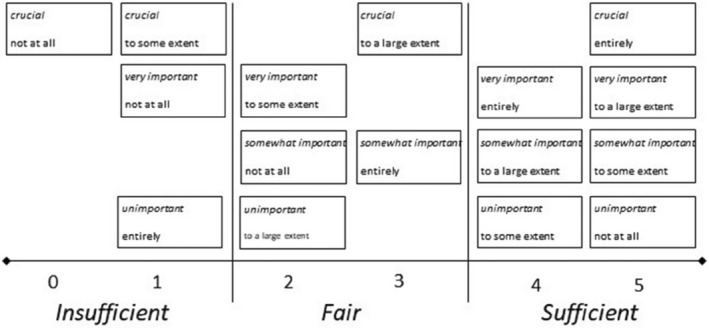
Scores and Levels of Matches and Mismatches Between Patient Preferences and Experiences of Patient Participation. Note. Originally published by Eldh et al. 2020
The levels of preference‐based patient participation were related to each other, therefore, multivariate analysis was performed.
Individual multivariate confidence intervals for proportions with Bonferroni’s adjustment were calculated for two of the levels, insufficient and sufficient. In this analysis, only the patients who answered all the items in both the preferences and the experiences sections were included.
The two items with the highest frequency and the two items with the lowest frequency of “crucial” patient ratings were identified. The results of the comparison of attributes rated as “crucial” for participation with the patients' responses regarding their experiences of these attributes were described as proportions with confidence intervals with Bonferroni’s adjustment within each item to cover multiple comparisons.
The 95% confidence intervals were presented. The diagrams present the items in the same order as they appear in the questionnaire. All analyses were carried out in IBM SPSS Statistics version 27.
RESULTS
A total of 101 unique completions of the 4Ps were returned (response rate 77%). Most of the returned 4Ps were from men, age 70 or older, and operated on for liver tumors. All details regarding demographics are shown in Table 1.
TABLE 1.
Patient characteristics
| Variable | n (%) |
| Sex | |
| Female | 48 (47.5) |
| Male | 53 (52.4) |
| Age | |
| −59 | 15 (14.9) |
| 60–69 | 35 (34.6) |
| 70– | 51 (50.5) |
| Education | |
| Compulsory school through grade 9 | 33 (35.1) |
| Two years of high school, trade school | 14 (14.9) |
| High school, 3–4 years/University, college | 44 (46.8) |
| Other | 3 (3.2) |
| Missing | 7 |
| Marital status | |
| Married/partner | 75 (76.5) |
| Single | 22 (22.4) |
| Other | 1 (1) |
| Missing | 3 |
| Children | |
| Yes | 84 (87.5) |
| No | 12 (12.5) |
| Missing | 5 |
| Tumour | |
| Pancreas | 41 (40.6) |
| Liver | 50 (49.5) |
| Bile duct | 9 (8.9) |
| Stomach | 1 (1) |
Preferences of patient participation
Regarding patients' preferences for participation, the items “having reciprocal communication” and “being listened to by the healthcare staff” were most often considered crucial for patient participation. In addition, “learning about what is planned for me” was a commonly preferred attribute of participation, more so than “having explanations of my symptoms/issues” and “learning to manage symptoms.” The attributes found to be least preferred for participation were “phrasing personal goals,” “my experiences being recognized,” “managing self‐care,” and “taking part in planning.” All details in terms of the patients' preferences for patient participation are presented in Figure 3a.
FIGURE 3.
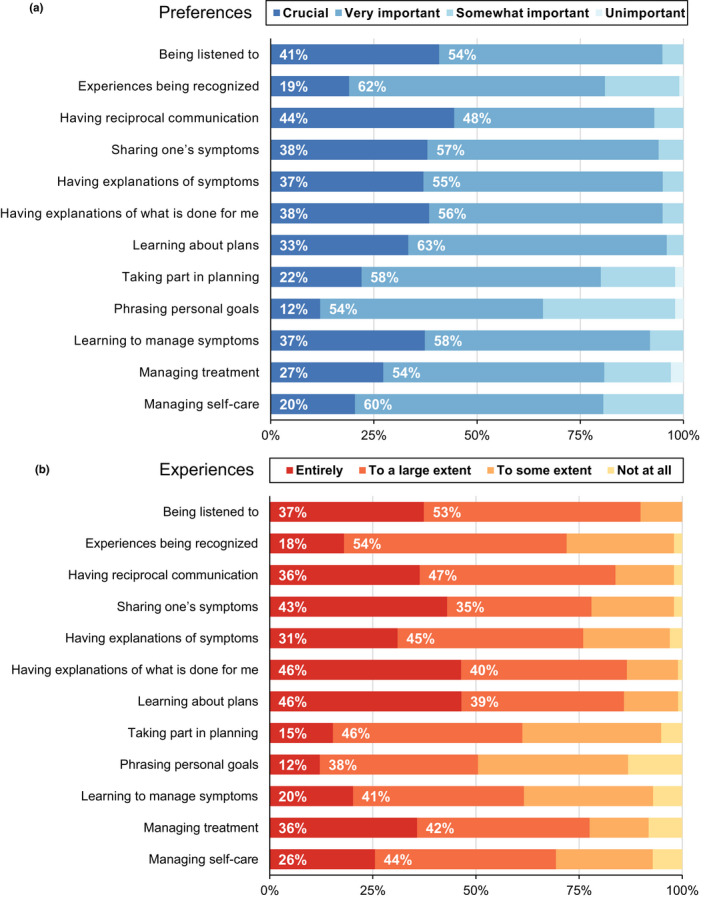
Patients Preferences for and Experiences of Patient Participation for Each Attribute. Note. The items are presented in the same order as they are presented in the 4Ps tool
Experiences of patient participation
As summarized in Figure 3b, the patients reported experiencing the highest levels of patient participation (i.e., experiencing the attribute entirely or to a large extent) for the following four items: “being listened to,” “having reciprocal communication,” “having explanations of what is done for me,” and “learning of plans.” The four items with the lowest levels of patient participation were “taking part in planning,” “phrasing personal goals,” “learning to manage symptoms,” and “managing self‐care.”
Levels of preference‐based patient participation
The comparison of the patients' preferences and experiences indicated the levels of preference‐based patient participation that had been achieved with the patients. As illustrated in Figure 4, the highest match was identified for “being listened to” by healthcare staff: 73% of the patients had experiences that matched their preferences. On the other hand, for “learning to manage my symptoms,” almost one‐fifth of the patients had an insufficient match; there was a 19% mismatch between preferences for and experiences of participation. The two attributes most often considered crucial for participation, “being listened to by the healthcare staff” and “having reciprocal communication,” were also the two attributes with the lowest proportions of insufficient levels of preference‐based patient participations, but these results were not significant.
FIGURE 4.
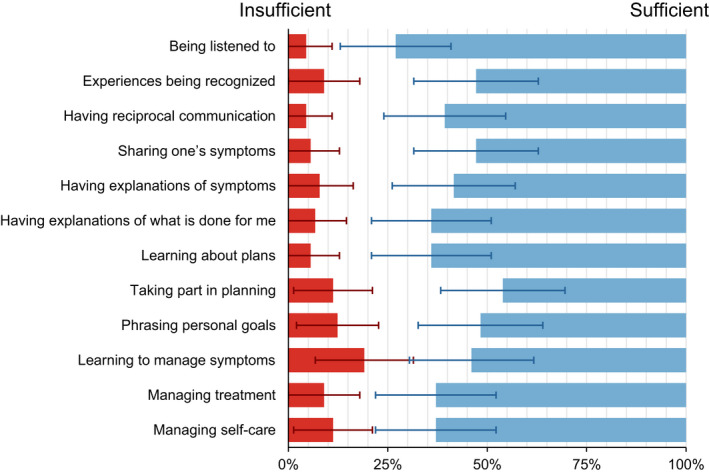
Insufficient and Sufficient Levels of Preference‐Based Patient Participation. Note. Figure also includes the individual multivariate 95% confidence intervals with Bonferroni’s adjustment (n = 89)
The four items with the highest percentages of insufficient preference‐based patient participation are presented in Figure 5. Only patients experiencing an insufficient match between preferences and experiences for the different attributes were included in this analysis (10 to 19 patients out of 101). “Learning to manage symptoms” had the highest percentage (63%) of insufficient preference‐based patient participation (crucial for participation yet experienced only to some extent). 62% of the patients rated the item “phrasing personal goals” as very important for my sense of participation but had not experienced any conditions for this attribute at all. Regarding “managing self‐care,” 58% stated that this attribute was “crucial” for sensing that he or she participated, yet the patients experienced this condition only to some extent during the care period. In addition, 60% of the patients had a high preference for “taking part in planning” (i.e., indicated that the item was crucial for patient participation), but they experienced this attribute only to some extent.
FIGURE 5.
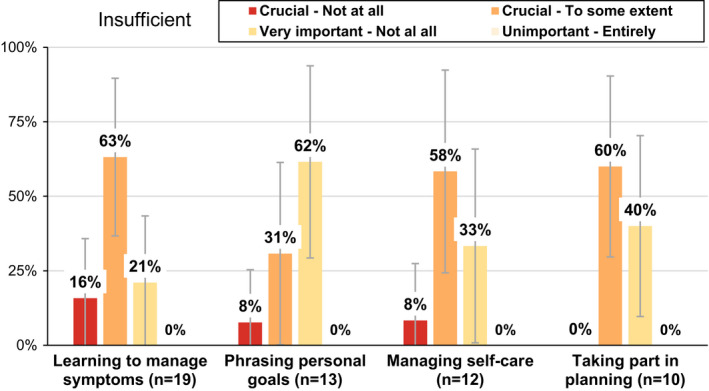
The Four Attributes of Patient Participation with the Largest Percentages of Insufficient Preference‐Based Patient Participation. Note. Figure also includes the 95% confidence interval with Bonferroni’s adjustment for each item
Most patients considered “having reciprocal communication” to be crucial for their participation, and 94% of the patients also experienced conditions matching their preferences, experiencing reciprocal communication either to a large extent (fair) or entirely (sufficient). “Being listened to by the healthcare staff” was the item that had the second‐largest percentage of patients who considered this attribute to be crucial (preference for participation) and experienced this attribute “to a large extent” (a fair level of preference‐based patient participation) or “entirely” (sufficient preference‐based participation); 91% had a sufficient or fair match between their preferences and experiences. Furthermore, the attributes “my experiences being recognized” and “phrasing personal goals” had the lowest matches between preferences and experiences, with only 32% and 33% of the patients having sufficient preference‐based patient participation for these attributes, respectively (Figure 6).
FIGURE 6.
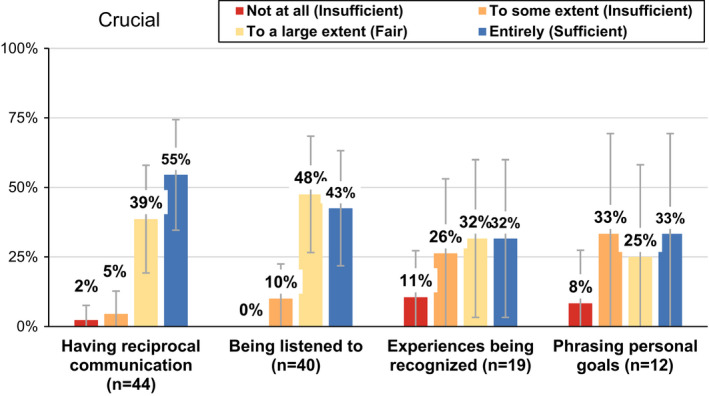
The Two Attributes Rated as Crucial for Participation with the Highest Percentages of Sufficient Matches and the Two Attributes Rated as Crucial for Participation with the Lowest Percentages of Sufficient Matches. Note. Figure also includes the 95% confidence interval with Bonferroni’s adjustment for each item
DISCUSSION
This study aimed to investigate and explore preference‐based patient participation in surgical upper abdominal cancer care based on patient's reports of their preferences and experiences of patient participation. “Having reciprocal communication” and “being listened to by the healthcare staff” were the attributes identified as most important for this group of patients in terms of their participation. Furthermore, these preferences were also best matched with the patients' experiences. This finding indicates that the specific surgical cancer care unit may provide preference‐based patient participation. However, whether the provision of such participation is unintentional requires further investigation.
The patients in the study reported the lowest preferences and experiences for “phrasing personal goals” and “taking part in planning.” These results may be related to their short time in the hospital and may also be associated with the care process, which is often conducted according to standardized programs (e.g., enhanced recovery after surgery) in which goal targets are set for diagnosis or surgical intervention. Goals and fast track planning are usually most visible to staff but may need to be clarified, made visible, and communicated with patients to a greater extent. A previous study has indicated that although phrasing goals corresponds to the concept of patient participation, it is difficult to execute, particularly in patients with severe conditions (Vahdat et al., 2014).
The results show that “learning to manage symptoms,” “taking part in planning,” and “phrasing personal goals” are areas that require further attention to meet patients' preferences. “Learning to manage symptoms” was the attribute with the highest proportion of insufficient matches, and “phrasing personal goals” also had a relatively high percentage of mismatches in this study. These may be important attributes to improve in the specific clinical practice context, especially as previous studies have shown that proper monitoring of the needs of patients with cancer can enhance their ability to cope with the stressful situation and improve their health‐related quality of life (Abu Sharour et al., 2020). Furthermore, there are indications that although professionals aim to provide information relevant to the patient, this effort does not always correspond with the patient's need for information (Fruijtier et al., 2020). There are opportunities to better understand patients' preferences for patient participation by means of a more mutual mode in healthcare professionals' communication (D'Agostino et al., 2017).
The items “learning to manage symptoms” and “phrasing personal goals” were generally considered by the patients to be very important for participation, but the patients did not have experiences that matched their preferences. This result is consistent with a previous study that described patient involvement in cancer surgery as being stimulated by patient‐centered care and the provision of support in asking questions and good communication (Thaysen et al., 2019).
“Being listened to by the healthcare staff” was sufficiently matched between preferences and experiences for 73% of the patients, which is a relatively high percentage. However, 27% of patients did not have a match between their preferences and actual experiences for being listened to; in person‐centered cancer surgical care, all patients should be listened to on their own terms. Creating a better match between preferences and experiences requires addressing the potential barriers in the healthcare context and those of the individual, including a recognition of the patient's health literacy and prior knowledge and experience (Parnell et al., 2019). However, this vulnerable group of patients with a severe cancer diagnosis may have a lot of mental distress and existential concerns. When it comes to health literacy, it can be dynamic and greatly affected by stress and worry. Previous studies have shown that health literacy and communication interaction ability played a prominent role for patients with cancer to be involved in treatment decision‐making (Kuijpers et al., 2021).
“Managing self‐care” was rated as crucial or very important for a sense of participation by 80% of the patients, and 70% also indicated that they had experienced this attribute entirely or to a large extent. Studies have shown that healthcare professionals' assessment of patients' self‐care needs is an unmet care need at each stage of the cancer trajectory to support patients in managing symptoms and self‐care (Gustavell et al., 2020; Lee et al., 2020).
The present study has its strengths and limitations. Considering the vulnerability of this group of patients, the 77% response rate is good, and there were few internal missing values. The sample size seemed to fulfill the aim and research questions due to the descriptive cross‐sectional design. No analysis comparing the included and excluded patients was done, which may be a limitation calling for further research efforts. Those that declined inclusion stated that a lack of energy and time was the reason for not participating. These non‐participants may have been more vulnerable than the included patients. However, the sample included more patients with pancreatic and liver malignancies than patients with bile duct or gastric cancer, but this distribution was representative of the patients who underwent cancer surgery during the enrollment period. It may be a limitation that patients responded to the questionnaire after discharge as this could have led to recall bias of how patient participation was experienced. But, on the other hand, the patients had more time for reflection when responding to the tool after discharge. Furthermore, the 4Ps tool is a relatively new tool, though valid and promising for capturing preferences for patient participation (Jerofke‐Owen et al., 2020). Despite the tool's novelty, it is one of the few available that fully conceptualizes patient participation, including the patient's lived experience. The tool also has more recently been used in other studies (Luhr et al., 2019; Martinsson et al., 2021). Therefore, we suggested the 4Ps for this study to reflect a broader notion of patient participation, corresponding to person‐centered patient participation (Pettersson et al., 2018).
Although patient participation is considered vital, there are challenges to meeting each patient's needs. Participation through decision involvement raises ethical issues with the Swedish Cancer Strategy (Castro et al., 2016), including the choice to have surgery or not. Previous studies among patients who had surgery for upper abdominal cancer have suggested further improvements regarding patient participation (Ibrahim et al., 2019; Larnebratt et al., 2019). For example, despite receiving information preoperatively, the provision of information in a single event could be stressful and overwhelming.
Even though healthcare professionals in the same surgical cancer clinic as this study rate the provision of information as the most important issue for patient participation, they often lack time to provide the information, as the prioritization of other activities hinders an ideal patient participation situation (Andersson et al., 2021). But it still emerges in the Swedish Cancer Strategy, which highlights that patients should be involved, well informed, and active in their treatment and that the treatment should be given based on a clear and well‐functioning individual care plan and in a standardized care path. Person‐centered communication should address listening, perspective and preference taking, and assessing and satisfying patients' information needs (Street et al., 2019). A review highlights that most patients with cancer prefer active participation, while only some patients prefer a passive role (Noteboom et al., 2021). However, it is useful to investigate patients' preferences in both clinical encounters and research to be able to adapt participation to the individual, providing opportunities for more person‐centered patient participation.
Linking Evidence to Action.
While preference‐based patient participation was achieved primarily for the item being listened to by the healthcare staff, healthcare staff need to recognize the need to also provide for opportunities to manage one's symptoms, taking part in planning, and phrasing personal goals in congruence with patients' preferences for participation.
Further studies of interventions facilitating a recognition of patients' preferences for, and experiences of participation are essential to enhance person‐centered surgical cancer care.
Implementation of preference‐based patient participation means and procedures are required, calling for co‐production initiatives with patient and staff representatives and management engagement at all levels of surgical care.
Patient participation needs to shift from being stated as a policy to an enactment in everyday health care, entailing that staff and patients come together in a shared dialogue of the preferences for and experiences of participation for the individual.
CLINICAL IMPLICATIONS
Professionals should work with a holistic approach in cancer surgical care to achieve optimal person‐centered care with high levels of patient participation. Although patient participation is considered vital, there are challenges to meeting each patient's personal needs. The findings of our study may provide a basis for further clinical implications of sufficient preference‐based patient participation in cancer surgical care. It may be useful to investigate patients' preferences with a tool in the clinical practice to be able to adapt participation to the individual. This could lead to an optimized degree of preference‐based patient participation.
CONCLUSION
Due to both the matches and mismatches between patients' preferences for and experiences of patient participation in surgical cancer care, there is potential for professionals to recognize both what works and what needs to be improved to adopt a more holistic approach to person‐centered care. Having opportunities for reciprocal communication and being listened to by the healthcare staff were rated as critical attributes by patients within the cancer care trajectory.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
Supporting information
TableS1
Drott, J. , Fomichov, V. , Nordén, M. , Larsson, A.L. , Sandström, P. & Björnsson, B. et al. (2022) Patient preferences and experiences of participation in surgical cancer care. Worldviews on Evidence‐Based Nursing, 19, 405–414. Available from: 10.1111/wvn.12589
Funding information
This work was supported by grants from the Medical Research Council of Southeast Sweden (FORSS‐862001)
REFERENCES
- Abu Sharour, L. , Malak, M. , Subih, M. & Bani Salameh, A. (2020) Quality of life, care needs, and information needs among patients diagnosed with cancer during their treatment phase. Psychology, Health & Medicine, 25(25), 252–258. 10.1080/13548506.2019.1699660 [DOI] [PubMed] [Google Scholar]
- Andersson, Å. , Wilhelmsson, M. , Fomichov, V. , Larsson, A. , Bjornsson, B. , Sandström, P. et al. (2021) Patient involvement in surgical care – health care personnel views and behaviour regarding patient involvement. Scandinavian Journal of Caring Science, 35(1), 96–103. 10.1111/scs.12823 [DOI] [PubMed] [Google Scholar]
- Årestedt, L. , Martinsson, C. , Hjelm, C. , Uhlin, F. , & Eldh, AC. (2019). Patient participation in dialysis care‐a qualitative study of patients' and health professionals' perspectives. Health Expectations, 22(6), 285–1293. 10.1111/hex.12966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnetz, J.E. , Almin, I. , Bergström, K. , Franzén, Y. & Nilsson, H. (2004) Active patient involvement in the establishment of physical therapy goals: effects on treatment outcome and quality of care. Advances in Physiotherapy, 6(2), 50–69. 10.1080/14038190310017147 [DOI] [Google Scholar]
- Cahill, J. (1996) Patient participation: a concept analysis. Journal of Advanced Nursing, 24, 561–571. 10.1046/j.1365-2648.1996.22517.x [DOI] [PubMed] [Google Scholar]
- Castro, E.M. , Van Regenmortel, T. , Vanhaecht, K. , Sermeus, W. & Van Hecke, A. (2016) Patient empowerment, patient participation and patient‐centeredness in hospital care: a concept analysis based on a literature review. Patient Education and Counseling, 99(12), 1923–1939. 10.1016/j.pec.2016.07.026 [DOI] [PubMed] [Google Scholar]
- D'Agostino, T.A. , Atkinson, T.M. , Latella, L.E. , Rogers, M. , Morrissey, D. , DeRosa, A.P. et al. (2017) Promoting patient participation in healthcare interactions through communication skills training: a systematic review. Patient Education and Counseling, 100(7), 1247–1257. 10.1016/j.pec.2017.02.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dumitra, T. , Ganescu, O. , Hu, R. , Fiore, J.F., Jr. , Kaneva, P. , Mayo, N. et al. (2021) Association between patient activation and health care utilization after thoracic and abdominal surgery. JAMA Surgery, 156(1), e205002. 10.1001/jamasurg.2020.5002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eldh, A.C. (2019) Facilitating patient participation by embracing patients' preferences‐a discussion. Journal of Evaluation in Clinical Practice, 25(6), 1070–1073. 10.1111/jep.13126 [DOI] [PubMed] [Google Scholar]
- Eldh, A.C. , Ekman, I. & Ehnfors, M. (2010) A comparison of the concept of patient participation and patients' descriptions as related to healthcare definitions. International Journal of Nursing Terminolofies and Classifications, 21(1), 21–32. 10.1111/j.1744-618x.2009.01141.x [DOI] [PubMed] [Google Scholar]
- Eldh, A.C. , Luhr, K. & Ehnfors, M. (2015) The development and initial validation of a clinical tool for patients' preferences on patient participation‐‐the 4Ps. Health Expectations, 18(6), 2522–2535. 10.1111/hex.12221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eldh, A.C. , Holmefur, M. , Luhr, K. & Wenemark, M. (2020) Assessing and reporting patient participation by means of patient preferences and experiences. BMC Health Services Research, 20(1), 702. 10.1186/s12913-020-05574-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finset, A. (2017) Patient participation, engagement and activation: increased emphasis on the role of patients in healthcare. Patient Education and Counseling, 100(7), 1245–1246. 10.1016/j.pec.2017.05.011 [DOI] [PubMed] [Google Scholar]
- Fruijtier, A.D. , Visser, L.N.C. , Bouwman, F.H. , Lutz, R. , Schoonenboom, N. , Kalisvaart, K. et al. (2020) What patients want to know, and what we actually tell them: the ABIDE project. Alzheimer's & Dementia, 6(1), e12113. 10.1002/trc2.12113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gustavell, T. , Sundberg, K. & Langius‐Eklöf, A. (2020) Using an interactive app for symptom reporting and management following pancreatic cancer surgery to facilitate person‐centered care: descriptive study. JMIR mHealth and uHealth, 8(6), e17855. 10.2196/17855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ibrahim, F. , Sandström, P. , Björnsson, B. , Larsson, A.L. & Drott, J. (2019) 'I want to know why and need to be involved in my own care…': a qualitative interview study with liver, bile duct or pancreatic cancer patients about their experiences with involvement in care. Supportive Care in Cancer, 27(7), 2561–2567. 10.1007/s00520-018-4548-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jerofke‐Owen, T. , Garnier‐Villarreal, M. , Fial, A. & Tobiano, G. (2020) Systematic review of psychometric properties of instruments measuring patient preferences for engagement in health care. Journal of Advanced Nursing. 10.1111/jan.14402 Epub ahead of print [DOI] [PubMed] [Google Scholar]
- Kehlet, H. & Wilmore, D.W. (2008) Evidence‐based surgical care and the evolution of fast‐track surgery. Annals of Surgery, 248(2), 189–198. 10.1097/sla.0b013e31817f2c1a [DOI] [PubMed] [Google Scholar]
- Kuijpers, M.M.T. , van Veenendaal, H. , Engelen, V. , Visserman, E. , Noteboom, E.A. , Stiggelbout, A.M. et al. (2021) Shared decision making in cancer treatment: a Dutch national survey on patients' preferences and perceptions. European Journal of Cancer Care, 31(1), e13534. 10.1111/ecc.13534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kvæl, L.A.H. , Debesay, J. , Langaas, A. , Bye, A. & Bergland, A. (2018) A concept analysis of patient participation in intermediate care. Patient Education and Counseling, 101, 1337–1350. 10.1016/j.pec.2018.03.005 [DOI] [PubMed] [Google Scholar]
- Larnebratt, A. , Fomichov, V. , Björnsson, B. , Sandström, P. , Lindhoff Larsson, A. & Drott, J. (2019) Information is the key to successful participation for patients receiving surgery for upper gastrointestinal cancer. European Journal of Cancer Care, 28(2), e12959. 10.1111/ecc.12959 [DOI] [PubMed] [Google Scholar]
- Larsson, I.E. , Sahlsten, M.J. , Segesten, K. & Plos, K.A. (2011) Patients' perceptions of nurses' behaviour that influence patient participation in nursing care: a critical incident study. Nursing Research Practice, 2011, 534060. 10.1155/2011/534060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, J.Y. , Jang, Y. , Kim, S. & Hyung, W.J. (2020) Uncertainty and unmet care needs before and after surgery in patients with gastric cancer: a survey study. Nursing & Health Science, 22(2), 427–435. 10.1111/nhs.12677 [DOI] [PubMed] [Google Scholar]
- Longtin, Y. , Sax, H. , Leape, L.L. , Sheridan, S.E. , Donaldson, L. & Pittet, D. (2010) Patient participation: current knowledge and applicability to patient safety. Mayo Clinic Proceedings, 85(1), 53–62. 10.4065/mcp.2009.0248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luhr, K. , Eldh, A.C. , Nilsson, U. & Holmefur, M. (2018) Patient preferences for patient participation: psychometric evaluation of The 4Ps tool in patients with chronic heart or lung disorders. Nordic Journal of Nursing Research, 38, 68–76. 10.1177/2057158517713156 [DOI] [Google Scholar]
- Luhr, K. , Eldh, A.C. , Theander, K. & Holmefur, M. (2019) Effects of a self‐management programme on patient participation in patients with chronic heart failure or chronic obstructive pulmonary disease: a randomized controlled trial. European Journal of Cardiovascular Nursing, 18(3), 185–193. 10.1177/1474515118804126 [DOI] [PubMed] [Google Scholar]
- Martinsson, C. , Uhlin, F. , Wenemark, M. & Eldh, A.C. (2021) Preference‐based patient participation for most, if not all: a cross‐sectional study of patient participation amongst persons with end‐stage kidney disease. Health Expectations, 24(5), 1833–1841. 10.1111/hex.13323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molinari, M. , El‐Tawil, K. , Swaid, F. , Fiorentini, G. , Bou‐Samra, P. , Sharma, C. et al. (2020) Patients' treatment preferences for potentially resectable tumors of the head of the pancreas. HPB, 22(2), 265–274. 10.1016/j.hpb.2019.06.015 [DOI] [PubMed] [Google Scholar]
- Nilsson, M. , From, I. & Lindwall, L. (2019) The significance of patient participation in nursing care ‐ a concept analysis. Scandinavian Journal of Caring Science, 33(1), 244–251. 10.1111/scs.12609 [DOI] [PubMed] [Google Scholar]
- Nolte, E. , Merkur, S. & Anell, A. (2020) Achieving person‐centred health systems: evidence, strategies and challenges. England: Cambridge University Press, European Observatory on Health Systems and Policies. [Google Scholar]
- Noteboom, E.A. , May, A.M. , van der Wall, E. , de Wit, N.J. & Helsper, C.W. (2021) Patients' preferred and perceived level of involvement in decision making for cancer treatment: a systematic review. Psychooncology, 30(10), 1663–1679. 10.1002/pon.5750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parnell, T.A. , Stichler, J.F. , Barton, A.J. , Loan, L.A. , Boyle, D.K. & Allen, P.E. (2019) A concept analysis of health literacy. Nursing Forum, 54(3), 315–327. 10.1111/nuf.12331 [DOI] [PubMed] [Google Scholar]
- Pettersson, M.E. , Öhlén, J. , Friberg, F. , Hydén, L.C. , Wallengren, C. , Sarenmalm, E.K. et al. (2018) Prepared for surgery ‐ communication in nurses' preoperative consultations with patients undergoing surgery for colorectal cancer after a person‐centred intervention. Journal of Clinical Nursing, 27, 2904–2916. [DOI] [PubMed] [Google Scholar]
- Sahlsten, M.J. , Larsson, I.E. , Sjöström, B. & Plos, K.A. (2008) An analysis of the concept of patient participation. Nursing Forum, 43(1), 2–11. 10.1111/j.1744-6198.2008.00090.x [DOI] [PubMed] [Google Scholar]
- Street, R.L. , Spears, E. , Madrid, S. & Mazor, K.M. (2019) Cancer survivors' experiences with breakdowns in patient‐centered communication. Psychooncology, 28(2), 423–429. 10.1002/pon.4963 [DOI] [PubMed] [Google Scholar]
- Thaysen, H.V. , Lomborg, K. & Seibaek, L. (2019) Patient involvement in comprehensive, complex cancer surgery: perspectives of patients, relatives and health professionals. European Journal of Cancer Care, 28(4), e13071. 10.1111/ecc.13071 [DOI] [PubMed] [Google Scholar]
- Vahdat, S. , Hamzehgardeshi, L. , Hessam, S. & Hamzehgardeshi, Z. (2014) Patient involvement in health care decision making: a review. Iranian Red Crescent Medical Journal, 16(1), e12454. 10.5812/ircmj.12454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . (2013) Exploring patient participation in reducing health‐care‐ related safety risks. WHO Regional Office for Europe. https://apps.who.int/iris/handle/10665/326442 [Google Scholar]
- World Medical Association . (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA, 310(20), 2191–2194. 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
TableS1