

Abstract
Rationale, Aims and Objectives
Social challenges are common for young adults with autism spectrum disorder (ASD) and/or mild intellectual impairment, yet few evidence‐based interventions exist to address these challenges. PEERS®, the Program for the Education and Enrichment of Relational Skills, has been shown to be effective in improving the social skills of young adults with ASD; however, it requires a significant time commitment for parents of young adults. As such, this mixed‐methods study aimed to investigate the experiences of young adults, parents and PEERS® social coaches participating in an adapted PEERS® program, and to evaluate its acceptability and efficacy.
Method
Young adults with ASD and/or mild intellectual impairment participated in a 16‐week PEERS® program. Parents and PEERS® social coaches attended fewer, condensed sessions, where they learnt program content to support the young adults' social skill development at home and in the community. Focus groups were conducted post intervention. Quantitative pre−post assessment using the Social and Emotional Loneliness Scale for Adults, the Test of Young Adult Social Skills Knowledge, and Quality of Socialization Questionnaire‐Young Adults was completed by young adults. The Social Responsiveness Scale Second Edition was completed by young adults and their parents.
Result
Qualitative results revealed that, taken together, young adults, parents and PEERS® social coaches all felt that the adapted PEERS® program was ‘challenging, but worth it’. The program was acceptable with a 93% attendance rate across all sessions. Whilst young adults' perceptions of their own social functioning did not change post‐intervention, their knowledge of social skills content improved significantly (p < 0.05). Parent perceptions of young adults' social responsiveness also improved (p < 0.05).
Conclusions
Social skill knowledge, social responsiveness, and social engagement improved significantly following the completion of the adapted PEERS® program. It was deemed acceptable and worthwhile by young adults, their parents and PEERS® social coaches.
Keywords: autism spectrum disorder, intellectual disability, PEERS®, social skills, young adult
1. INTRODUCTION
Young people with autism spectrum disorder (ASD) and/or with mild intellectual impairment can have difficulties with social communication, social problem solving and peer interactions and relationships. 1 These limitations often become more pronounced and distressing in adolescence and young adulthood when social interactions become more complex, as individuals become more aware of their social deficits, and as caregiver coordination of interactions is no longer socially acceptable. 2
Children and young adults with ASD and/or mild intellectual impairment have been shown to participate in fewer social activities, have less social contact and experience fewer intimate relationships than their typically developing peers. 3 , 4 , 5 , 6 , 7 , 8 Young people with limited social skills often experience challenges in developing and maintaining meaningful relationships and exhibit poorer outcomes in education and employment settings. 9 Moreover, social isolation in adulthood is associated with higher rates of depression, poorer health outcomes and poorer overall well‐being. 10
PEERS®, the Program for the Education and Enrichment of Relational Skills, has been developed to teach social skills to adolescents and young adults with ASD. 11 It is a 16‐week evidence‐based, parent/caregiver‐assisted social skills program, focused on making and keeping friends, developing and maintaining romantic relationships, and managing conflict and rejection. 11
Using a cognitive‐behavioural therapy framework, PEERS® incorporates evidence‐based methods of instruction, including didactic lessons with concrete rules and steps of social skills, role‐play demonstrations, perspective‐taking questions, behavioural rehearsal exercises, performance feedback coaching and homework assignments, which utilize parents and caregivers as social coaches. 11 PEERS® was originally developed for adolescents with ASD, then later expanded to include young adults with ASD, as well as those without ASD, and has been evaluated in nearly two dozen randomized controlled trials (RCTs). Results demonstrate improvement in overall social skills, knowledge of social skills, social responsiveness, social communication, social motivation, assertion, cooperation and social engagement through hosted get‐togethers. 12 , 13 , 14 , 15 , 16 Most treatment effects are maintained at 14 weeks follow‐up, 12 with some effects improving further 1−5 years post treatment. 13
Despite PEERS® growing use internationally, it requires a considerable time commitment from parents/carers attending every session concurrently with their young adults. This time commitment may pose a significant barrier, especially for parents of young adults with a disability who are known to experience higher levels of stress managing appointments, the increased needs of their child and the everyday needs of family and other children. 17 , 18
Moreover, during this stage of emerging adulthood, young adults are beginning to develop skills of self‐determination, 19 and many young adults who have trusting relationships with mentors and/or support workers may feel more comfortable discussing topics of socializing, including bullying and dating, with them than they do with a parent or caregiver. 20 , 21
The current study aims to investigate the experiences and evaluate the acceptability and efficacy of an adapted version of the PEERS® for Young Adults Program, 11 with condensed parent involvement, and supplemented with social coaching from PEERS® social coaches. Specifically, we aimed to explore the experiences and views of young adults, parents, PEERS® social coaches and PEERS® staff in relation to the acceptability of participating in this adapted program. The study also aimed to examine the efficacy of the adapted program in improving the overall social skills, social responsiveness, knowledge of social skills, frequency and quality of social engagement, and self‐perceived loneliness among young adults with ASD and/or mild intellectual impairment. This mixed‐methods approach will, for the first time, give light to the qualitative experiences and perspectives of young adults, parents, PEERS® social coaches and PEERS® staff participating in the program.
Moreover, evaluation of the efficacy of this adapted program is critical to determine whether the positive results demonstrated by the PEERS® program can be achieved via the adapted program. Mixed‐methods program evaluations like this have been recommended for their capacity to demonstrate ‘not only whether a novel intervention works, but also how and why, or why not’, 22 p. 141.
2. MATERIAL AND METHODS
2.1. Study design
The current study reports a mixed‐methods program evaluation that combines qualitative data gathered through focus groups conducted at the end of the program, with quantitative pre−post assessments in an embedded sequential design. 23 Figure 1 provides a visual representation of the study design.
Figure 1.
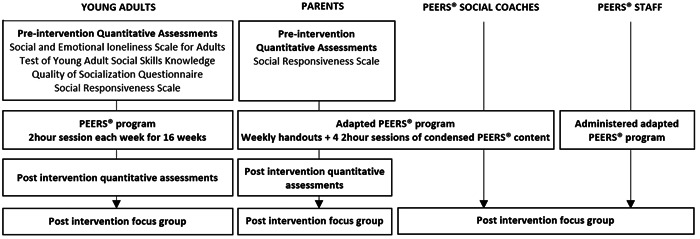
Study design
2.2. Participants
The PEERS® program was offered as a free service offering, to a convenience purposive sample of young adults with social skills difficulties who had expressed an interest in improving their social skills. They were concurrently participating in a school leaver employment support (SLES) program in Australia. The SLES program focuses on developing vocational skills such as identifying strengths and interests, curriculum vitae development, interview skills and applications for further study. SLES staff identified that some young adults experienced social skills difficulties, but that the SLES program did not offer social skill development as part of the program, and hence referred them to the adapted PEERS® program.
Eligible young adults were aged 17−23, fluent English speakers, who had a parent/caregiver who was willing and able to participate and support them in the program. Young adults who had a diagnosis of moderate to severe intellectual impairment, a history of major mental illness or moderate to severe hearing, vision or communication impairment were excluded from the study. To allow active participation in the group, the maximum number of young adults recruited was limited to eight. For pragmatic reasons, diverse primary diagnoses were accepted as long as participants met the eligibility criteria.
Young adults participating in the PEERS® program (n = 8), their parents (n = 8), PEERS® social coaches (n = 3) and PEERS® staff (n = 4) were invited to participate in a mixed‐methods research project evaluating the adapted PEERS® program. The study was conducted by a research team who were not involved in the delivery of the PEERS® program, and participants in the PEERS® program were not obliged to participate in the evaluation. Ethics approval was granted by the Cerebral Palsy Alliance Ethics Committee (EC00402), approval number: 2017‐02‐02.
2.3. Intervention
PEERS® for Young Adults 11 is a 16‐week (90‐min per week) group‐based program for young adults in which social skills are taught through didactic instruction, role‐play demonstrations, behavioural rehearsal and homework exercises. PEERS® was delivered to young adults as per manual guidelines by PEERS® Certified Providers (PEERS® staff) who underwent 24 h of comprehensive training by the program developer. Sessions focused on: appropriate conversational skills; choosing appropriate friends; appropriate use of electronic communication; appropriate use of humour; how to start, enter and exit conversations; organizing get‐togethers; developing romantic relationships; dating etiquette; handling arguments and disagreements with friends and partners; and handling rejection, teasing, bullying and rumours/gossip.
In the standard PEERS® program, parents/caregivers concurrently attend PEERS® weekly sessions to support their young adult in developing and maintaining friends and relationships. The current cohort of young adults expressed a preference for autonomy and privacy from parents, and parents commented that their own weekly attendance may be a barrier to their young adult's participation. However, repetition, rehearsal and generalization were felt to be key to the program's success by researchers; hence, an adapted PEERS® model was developed.
In this model, young adults were supported using a different process. Parents reinforced PEERS® skills and knowledge in the home environment, and PEERS® social coaches; staff (of the School Leaver Program) with whom the young adults had a good relationship and who provided one‐on‐one opportunities to practice skills and complete homework between weekly sessions. Every young adult had a PEERS® social coach, with some PEERS® social coaches working with more than one young adult.
Parents and PEERS® social coaches were invited to attend four 2‐h sessions across the course of the program (instead of weekly 90‐min sessions). These sessions included a summary of the content covered in the young adult groups and provided the opportunity to discuss and troubleshoot difficulties that may have arisen during the completion of weekly socialization homework. Young adults were also provided weekly handouts from the PEERS® manual to share with parents and PEERS® social coaches, providing a summary of course content and homework tasks. This condensed offering suited parents, who worked and lived across a large geographical area, and who expressed concerns with being able to attend weekly sessions due to work and other family commitments. PEERS® staff contact details were shared, and families were encouraged to contact the PEERS® staff if they had any questions between sessions.
2.4. Focus group methodology
Following completion of the program, three separate focus groups were held with the (1) young adults, (2) parents and (3) PEERS® staff and PEERS® social coaches. Each focus group lasted approximately 45 min and provided an opportunity for participants to provide in‐depth information about their experiences of participating in the program. The focus group guides were developed by NS and SM, who also conducted the focus groups. Questions centred around four key areas: the acceptability of the program content (i.e., ‘Was there any content that made you feel uncomfortable?’ and ‘Was there anything missing?’); feasibility of participating in the program (i.e., ‘How manageable was it to attend every week for 16 weeks/four times over the 16 weeks?’); the overall experiences of participation (i.e., ‘What did you like/dislike?’); and views on how the outcomes of the program might contribute to changes in the participants' lives in the future (i.e., ‘Have you started doing anything differently when talking to people and trying to make friends?’). Focus groups were digitally recorded and later transcribed verbatim for analysis.
2.5. Outcome measures
Young adults and parents completed the following quantitative measures 1 week before commencing the program, and at program completion (see Figure 1).
2.5.1. Social Responsiveness Scale
The Social Responsiveness Scale Second Edition (SRS‐2) 24 was completed by young adults and parents as a primary outcome measure of social functioning. The SRS‐2 is a 65‐item standardized rating scale that identifies social impairment associated with ASD. The scale is comprised of five treatment subscales: Social awareness, social cognition, social communication, social motivation and restricted interests and repetitive behaviour, and two Diagnostic and Statistical Manual of Mental Disorders (DSM‐5) compatible subscales: Social Communication and Interaction (SCI); and Restricted Interests and Repetitive Behaviour. As the PEERS® program is not designed to intervene in restricted interests and repetitive behaviours, this subdomain was not included in the analyses. Raw scores are converted to T scores (M = 50; SD = 10) for each subscale, and a total score is obtained. T scores of 59 or below indicate that the individual is unlikely to experience social difficulties consistent with ASD; T scores of 60−65 indicate mild impairments in social responsiveness; T scores of 66−75 suggest moderate impairments in social responsiveness and T scores of 76 or higher suggest severe impairments in social responsiveness and difficulties that interfere with social interactions with others.
2.5.2. Social and Emotional Loneliness Scale for Adults (SELSA)
The SELSA 25 is a 37‐item self‐report scale, completed by young adults, examining areas of social and emotional (romantic and family) loneliness. Items are rated on a 7‐point Likert scale and totals are obtained for each subdomain, with higher scores indicating greater levels of loneliness.
2.5.3. Test of Young Adult Social Skills Knowledge (TYASSK)
The TYASSK 11 is a 23‐item measure designed to assess young adult knowledge of course‐specific content before and post completion of the PEERS® intervention. Higher scores indicate greater knowledge of social skills.
2.5.4. Quality of Socialization Questionnaire‐Young Adult (QSQ‐YA)
The QSQ‐YA 11 was used to assess social engagement by way of the frequency of get‐togethers and the level of conflict experienced during get‐togethers in the past month. The QSQ‐YA is made up of three subscales: social initiation scale, social reciprocity scale and conflict scale. A conflict score of 3.5 or greater for any get‐together indicates significant conflict.
2.6. Data analysis
Qualitative data from focus groups were analysed using inductive content analysis, guided by published procedures. 26 , 27 Qualitative analysis was predominantly undertaken by N. S., with N. S., S. M. and H. S.‐S. meeting regularly throughout the course of analysis to discuss and reflect on developing themes. QSR N‐Vivo 11 software was used to manage the data and facilitate the coding process. The aim of content analysis was to attain a ‘condensed and broad description of the phenomenon’ under study. 27 The focus group transcripts formed the unit of analysis, with the entire transcripts initially reviewed, to identify meaning units relevant to the research questions. These meaning units included ‘words, sentences or paragraphs containing aspects related to each other through their content and context’. 28
Meaning units were labelled with codes, 28 for example, the meaning units ‘there's a lot to remember’ and ‘there was a lot going into our brains’ were labelled with the code ‘information overload’. In later stages of data analysis, codes were reviewed, compared based on similarities and differences, and grouped under higher order categories where relevant. 27 , 28 , 29 Categories were then grouped through a process of abstraction under four sub‐themes and an overarching theme. This process of interpretation led to an understanding of the implicit meaning, or essence of participants' experiences. 30 Finally, a ‘story line’ was developed to describe and connect the themes in a narrative, 30 as presented in the results. Strategies utilized to enhance the credibility of the qualitative findings included gathering data from multiple perspectives to ensure a rich understanding of the phenomenon, ongoing dialogue between members of the research team during analysis, and the inclusion of numerous direct quotations from transcripts within the findings. 26 , 28
Quantitative data were analysed using SPSS (Version 24). One young adult did not complete sufficient items in the SRS‐2 for inclusion in analyses and was therefore excluded from the SRS‐2 pre/post analysis. Normality was assessed using Shapiro−Wilk, visual inspection of the histogram and box plot for outliers, and paired t tests run. However, due to the small sample size, non‐parametric Wilcoxon Signed Rank Test was also conducted. Change scores were calculated. As results remained unchanged, paired t tests are discussed for ease of interpretation (Wilcoxon Signed Rank Test results reported in Supporting Information: Appendix A).
Data integration was conducted by I. H., N. S., S. M. and H. S.‐S. It occurred at the interpretation and reporting level, through narrative review in the discussion. 31
3. RESULTS
Seven PEERS® young adults (five male) aged 18−23 years, five parents, three PEERS® social coaches and four PEERS® staff provided informed consent, completed pre‐ and post‐assessments (young adults and parents) and participated in post‐intervention focus groups. One additional young adult and three parents participated in the adapted PEERS® program but were unable to attend the pre/post‐intervention session and therefore were not included in the evaluation. Four young adults had a primary diagnosis of an ASD and three had a mild intellectual impairment/disability. Participants were deemed to have a mild intellectual impairment if parent report, self‐report or clinical notes indicated a diagnosis of intellectual disability, in the context of a reasonable level of independence with activities of daily living. Total participant attendance was high with 93% (105/112) sessions attended.
3.1. Qualitative results
The overall theme identified through content analysis was PEERS® is challenging, but worthwhile. Participating in the program was challenging for a range of practical and personal reasons; however, participants believed the positive outcomes made the challenges worth overcoming. The views of young adults, parents PEERS® social coaches and PEERS® staff, which contributed to this overall theme, are represented by four sub‐themes, introduced in Figure 2. Each sub‐theme represents the juxtaposition of a challenge and the reason why participants believed that challenge was worth overcoming.
Figure 2.
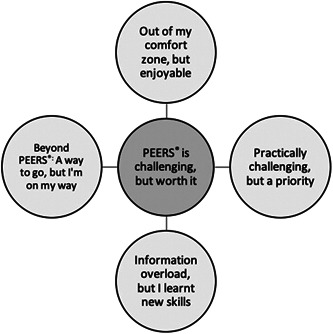
Theme and sub‐themes of qualitative analysis
3.1.1. Out of my comfort zone, but enjoyable
PEERS® put the young adult participants outside of their comfort zone in a number of ways. Initially, some young adults were ‘very anxious’ to come along to a group with people they didn't know well. For others, it was particular tasks that made them feel uncomfortable. One young adult spoke about the challenge of having to call a friend on the phone. He stated, ‘It was a bit nerve‐wracking for me. I'm not very good at talking on the phone’. Some content made young adults feel uncomfortable, in particular the content around dating. One young adult said, ‘It is just a really personal, uncomfortable subject to talk about’, while a parent mentioned that her daughter ‘found it a little bit embarrassing’. Despite these challenges, young adults enjoyed the experience of PEERS® and ‘looked forward’ to attending each week. Young adults highlighted that it was ‘fun getting to meet new people’ and ‘nice to have a laugh and be happy’. Parents expressed their surprise that their young adults were uncharacteristically happy to attend each week and to see the program through.
One parent said, ‘It's certainly amazing in my family that she'll keep coming to something’. Another parent highlighted that the group was inherently enjoyable, stating, ‘the group itself has been an enjoyable activity, as well as what he has learnt from it’.
3.1.2. Practically challenging, but a priority
Attending PEERS® every week for 16 weeks created a number of practical challenges for young adult participants and their parents, and required a high level of commitment.
Participants lived in diverse parts of Sydney, Australia, and some travelled for more than an hour each way to attend. One parent emphasized that ‘it has been a huge investment’, while others had had to ‘rearrange their work schedules’ in order for their young adult to attend. Another practical challenge related to the timing of sessions, which were held in the evening. Most young adults were not yet able to, or allowed to, travel independently on public transportation, especially at night, and thus relied on their parents for transportation. One mother said, ‘There is no way I'd have her travelling home [on public transport]’. One young adult said, ‘It is a very late night’. This was also underscored by a parent who stated, ‘It is quite a late night by the time I get home and it means staying back late at work to pick him up’. Despite these practical challenges, young adults and parents were happy to attend and recognized the program as a priority. One parent said, ‘It is hard, but it's worthwhile’, while another said, ‘I wanted him to come because I'd like him to have more of a social life…I thought he would benefit’.
3.1.3. Information overload, but I learnt new skills
Young adult participants emphasized that there was a lot of content covered within the PEERS® program, saying ‘there's a lot to remember’ and ‘there was a lot going into our brains every night’. One young adult confessed, ‘I forgot about half of it’. Despite the volume of content involved, young adults acknowledged the information was useful and were able to share a number of new skills they had practiced and remembered. These included ‘trading information’, ‘finding a common interest’, ‘starting a conversation’, and ‘resolving an argument’. Young adults recognized that the dating content was also important, despite it making some uncomfortable. With regard to dating, one young adult indicated, ‘It could happen sometime when you're ready for it to happen, and you might want to know what to do’. Having opportunities to practise in between PEERS® sessions with a PEERS® social coach was stressed as important to helping young adults implement the skills in ‘real life’. PEERS® staff also emphasized that the repetition of instruction built into the program was helpful, explaining ‘it's a very safe, predictable sort of progress’.
3.1.4. Beyond PEERS®: A way to go, but I'm on my way
Parents reflected on how they believed participating in PEERS® had influenced the young adults' lives. Some parents identified areas that their young adult was still finding difficult. One parent said, ‘I think part of it was that she could join a group…and we haven't progressed at all with that’, while another parent reflected, ‘I would have loved her to join a choir or something, but she's just too scared’. Despite these challenges, the young adults were still reported to be on their way to engaging in more social activities and building new connections. One young adult explained, ‘I'm getting out a bit more’, while another commented, ‘I have a get‐together organised’. Parents, in particular, were very positive about changes they had seen in their young adult. Examples of progress included statements like, ‘She was talking last week about a number of different groups at university that she was thinking of going to. That was good. The seed of a thought is there’. Another parent remarked, ‘He has been really proud to tell us that he organised something. There was once or twice where we would organise something and he was like “No, I can't do that because I've got other plans.” That is quite impressive’. A separate parent commented, ‘It has given him the confidence to be the initiator. Before he was just sort of waiting for some of his friends to contact him. Now, he is actually organising things, which has been good’. PEERS® staff and PEERS® social coaches also highlighted positive shifts in the young adults. One PEERS® staff reflected, ‘It's the confidence, it's the brighter eyes, it's the little smiles, it's the whole body language that changes’.
3.2. Quantitative results
No significant differences were detected in young adult perceptions of their own social functioning as assessed via self‐report on the SRS‐2 from pre‐ to post‐intervention. Interestingly, on average, young adults rated their social responsiveness within normal limits on all but one subdomain of the SRS‐2 before intervention commencement (Table 1), indicating that they felt they were unlikely to be experiencing social difficulties. However, significant differences were detected in parent perceptions of their young adult's social responsiveness from pre‐ to post‐intervention. Significant improvements were detected in SRS Total Scores, the Social Communication and Interaction subdomain, and the Social Communication subdomain (Table 1). Importantly, as seen in Figure 3, young adults were on average rated by their parents to have poor social responsiveness before the intervention on these domains; scores then significantly dropped to within normal limits following the intervention.
Table 1.
Pre‐ and post‐intervention outcome measures
| Measure/Subdomain | Pre | Post | Change statistics | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean diff | T score | p value | 95% CI | |
| SRS‐2 self‐rateda | ||||||||
| Total | 58.33 | 8.34 | 56.67 | 8.66 | 1.67 | 1.096 | 0.323 | −2.24 to 5.58 |
| SCI | 58.83 | 8.64 | 57.00 | 8.74 | 1.83 | 1.193 | 0.286 | −2.12 to 5.78 |
| Social awareness | 51.33 | 6.65 | 55.50 | 10.13 | −4.167 | −1.778 | 0.136 | −10.19 to 1.86 |
| Social cognition | 60.00 | 7.72 | 59.00 | 7.77 | 1.000 | 0.397 | 0.707 | −5.47 to 7.47 |
| Social communication | 59.50 | 10.56 | 55.50 | 10.99 | 4.000 | 2.309 | 0.069 | −0.45 to 8.45 |
| Social motivation | 58.50 | 8.55 | 55.83 | 7.65 | 2.667 | 1.360 | 0.232 | −2.37 to 7.71 |
| SRS‐2 social coach rated | ||||||||
| Total | 63.60 | 4.34 | 54.20 | 3.42 | 9.40 | 4.354 | 0.012* | 3.41–15.39 |
| SCI | 62.80 | 2.28 | 55.00 | 3.81 | 7.80 | 5.099 | 0.007* | 3.55–12.05 |
| Social awareness | 58.00 | 5.20 | 57.00 | 10.34 | 1.00 | 0.321 | 0.764 | −7.65 to 9.65 |
| Social cognition | 65.00 | 5.34 | 53.60 | 6.27 | 11.40 | 2.632 | 0.058 | −0.63 to 23.43 |
| Social communication | 61.20 | 1.30 | 53.80 | 4.27 | 7.40 | 4.230 | 0.013* | 2.54–12.26 |
| Social motivation | 62.20 | 11.67 | 55.60 | 10.24 | 6.60 | 2.012 | 0.115 | −2.51 to 15.71 |
| SELSA self‐rated | ||||||||
| Total | 115.29 | 30.91 | 111.57 | 22.90 | 3.71 | 0.683 | 0.520 | −9.59 to 17.02 |
| Romantic | 45.00 | 10.46 | 46.57 | 6.11 | −1.57 | −0.751 | 0.481 | −6.69 to 3.55 |
| Social | 38.86 | 12.68 | 37.29 | 9.41 | 1.57 | 0.575 | 0.586 | −5.12 to 8.26 |
| Family | 31.43 | 9.85 | 27.71 | 11.18 | 3.71 | 1.106 | 0.311 | −4.50 to 11.93 |
| TYASSK‐YA self‐rated | ||||||||
| Total correct | 12.14 | 1.35 | 19.00 | 3.11 | −6.86 | −8.273 | <0.001* | −8.89 to −4.83 |
Abbreviations: CI, confidence interval; SCI, Social Communication and Interaction; SD, standard deviation; SELSA, Social and Emotional Loneliness Scale for Adults; SRS‐2, Social Responsiveness Scale Second Edition; TYASSK‐YA, Test of Young Adult Social Skills Knowledge‐Young Adult.
N= 6.
Significant p ≤ 0.05.
Figure 3.
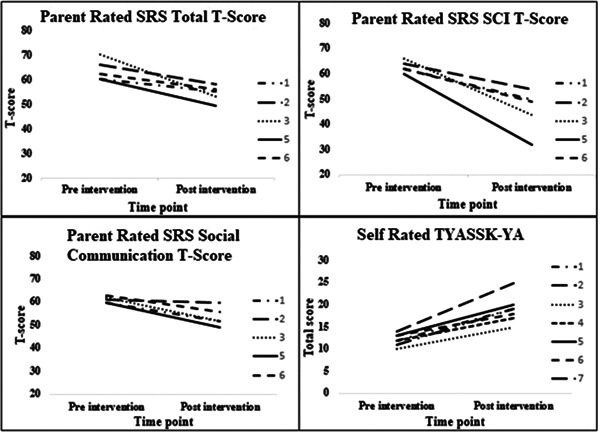
Individual participant trajectories of statistically significant results
Young adults' knowledge of social skills content, as assessed via the TYASSK‐YA, significantly improved on intervention completion, when compared to baseline knowledge (Table 1 and Figure 3).
Descriptive examination of QSQ‐A results provides insight into changes in the frequency and quality of get‐togethers on intervention completion when compared to baseline. In the month before intervention commencement, no participants hosted any get‐togethers, and only two participants were invited to one get‐together each. At intervention completion, three of the participants had hosted a total of eight get‐togethers between them in the last month, and one participant had been invited to a get‐together.
No significant differences were detected in loneliness levels, as assessed by the SELSA, at intervention completion when compared to loneliness levels before intervention commencement (Table 1).
4. DISCUSSION
Social connectedness is a key determinant of quality of life and well‐being, 32 , 33 yet many people with ASD and/or mild intellectual impairment continue to experience social skill difficulties into adulthood. 33 The present study investigated the experiences and evaluated the acceptability and efficacy of an adapted PEERS® program for young adults with ASD and/or mild intellectual impairment. Findings revealed that whilst the adapted program still required a significant time commitment from young adult participants and parents, it was deemed to be acceptable and worthwhile overall. Moreover, results suggest that the program was effective in improving aspects of social skills, including young adult social skill knowledge and parent ratings of young adults' social responsiveness.
The decision to adapt the standard PEERS® program for the current study was made for pragmatic reasons based on young adult and parent preferences. The young adults expressed a desire for autonomy from their parents, and parents anticipated that weekly session attendance would be a significant barrier to their participation. As such, parents attended fewer, condensed sessions and young adults received additional one‐on‐one support from PEERS® social coaches between the weekly PEERS® sessions to practice and implement the skills they learnt.
Whilst the original PEERS® program has been shown to be effective, with parent involvement as one of the key components thought to contribute to the generalization of skills to everyday life, it was originally developed for teenagers aged 14−18 years, and has since been adapted for young adults. 11 , 13 , 14 Young adulthood is a developmentally appropriate time to begin to execute autonomy over life areas and develop a sense of identity separate from one's parents and family. 19 Whilst this transition to adulthood for people with ASD and/or mild intellectual impairment is often delayed, providing alternative PEERS® social coaches in addition to parent coaches where this is preferred, may also support young adults to develop these important adaptive behaviours. Similarly, it is common for adolescents and young adults to refrain from sharing information on topics such as dating with parents and instead confide in a peer or mentor. The inclusion of another mentor, such as the PEERS® social coaches, provided an additional opportunity to discuss and develop skills in a safe, supportive and developmentally appropriate context.
Another key finding from investigating the young adult experience of PEERS® is that the program challenged young adults. Challenges were described in relation to the volume of content, nature of topics, nature of homework tasks and the group nature of the program. This demonstrates that the PEERS® program appears to be at the ‘just right’ challenge level, where the young adults are engaged and motivated to learn, and the material is challenging but not beyond their capacity, enabling them to comprehend, recall and implement the program content. This is further supported by quantitative results in which the young adults' knowledge of social skill content significantly increased by program completion, indicating a good ability to engage with, understand and retain program content. Whilst young adults were pushed out of their comfort zones, they were provided with the necessary information and environmental support to develop the target skills.
Support for the efficacy of the adapted program is also demonstrated by results from aspects of the quantitative measures. Parent reports at baseline revealed that young adults were exhibiting mild impairment in social responsiveness, mild impairment in social communication, and mild impairment in social and communication interaction consistent with DSM‐5 criteria on the SRS‐2, before treatment. 24 Baseline social deficits significantly improved upon program completion. Results suggest not only statistical significance, with mean improvements equivalent to approximately three quarters of a standard deviation, but perhaps more importantly, improvements reveal clinical significance, with posttreatment social responsiveness scores falling to within normal limits upon program completion.
Interestingly, young adults rated their social skills within normal limits on all domains of the SRS‐2 before the intervention, indicating that they did not feel they had clinically elevated social impairment. However, this is in contrast to discussions had with each young adult before being enrolled in the intervention, whereby social difficulties perceived by parents and young adults, and a motivation to improve these skills were necessary inclusion criteria for enrolment in the study. Results of the current study may reflect a lack of young adult insight around how certain statements and behaviours included in the SRS‐2 contribute to social skills and therefore their social skill difficulties before the PEERS® program.
While qualitative and quantitative results support the acceptability and efficacy of the adapted PEERS® program, some important limitations of the current study should be noted. The sample was a convenience, purposive sample and no control group was available. Whilst necessary for group dynamics and implementation of the program, the small number of participants limited options for quantitative statistical analysis. This small sample size, coupled with the heterogeneity of the sample in terms of primary diagnosis, prohibited any diagnosis‐specific interpretation of results. Second, young adults were concurrently participating in the SLES program. While the SLES program focused on vocational skills and did not include any specific social skill component, participation in the SELS program likely provided young adults additional ad hoc opportunities to practice social skills learnt through the adapted PEERS® program. Third, all participants lived in Sydney, a major metropolitan city in Australia. The PEERS® program was developed in the United States based on Western, English‐speaking social etiquette, but has been cross‐culturally translated and adapted into a number of languages such as Thai, 34 Japanese, 35 Dutch, 36 Korean, 37 and Hebrew. 38 The generalizability of results from the current study to regional and remote communities and culturally and linguistically diverse communities is unknown, and warrants further investigation. However, adaptations similar to those required for the cross‐cultural translation of the PEERS® program more broadly would likely be necessary, in line with local social etiquette.
In conclusion, results taken together provide support for an adapted PEERS® program with condensed parent involvement and the inclusion of PEERS® social coaches. One of the strengths of this evaluation is that the research involved a mixed‐methods design. Mixed methods combine the ‘power of stories and the power of numbers’. 39 Utilizing this approach facilitated a deeper level of insight than that offered by either quantitative or qualitative research alone and increased the rigour of the evaluation through triangulation. Given the significant investment involved in delivering this 16‐week program, it was important that an in‐depth quantitative and qualitative understanding of the adapted program outcomes were obtained. Results suggest that an adapted PEERS® program with reduced parental involvement and increased PEERS® social coach involvement is of value in improving social skills for young adults with ASD and/or mild intellectual impairment.
AUTHOR CONTRIBUTIONS
All authors have been consulted in the process of developing this manuscript to this final draft stage for submission. All authors meeting the criteria for authorship are listed under the title of the manuscript. All authors have met the eligibility criteria for inclusion as authors. Ingrid Honan, Sarah McIntyre, Nicole Sharp and Hayley Smithers‐Sheedy contributed to the research design, data collection, analysis, write up and critical review of the manuscript. Isabelle Balde, Kirsten Quinn, Marita Morgan, Sophie Rothery and Teigan Butchers were involved in research design, participant recruitment, data collection and critical manuscript review and Elizabeth. A Laugeson was involved in research design, data interpretation and critical review of the manuscript.
CONFLICT OF INTEREST
E. A. L. is the director of the UCLA PEERS® Clinic, and author of the original PEERS® Manual. I. H., N. S., S. M., H. S.‐S., I. B., K. Q., M. M., S. R. and T. B. do not have any financial interests or conflicts of interests to disclose.
Supporting information
Supplementary File: Guidelines for Good Reporting of a Mixed Methods Study (GRAMMS)40.
Supporting information.
ACKNOWLEDEGMENTS
This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors. H. S.‐S. received support through a National Health and Medical Research Council Early Career Fellowship 1144566 and the Australasian Cerebral Palsy Clinical Trials Network. S. M. received support through a National Health and Medical Research Council Early Career Fellowship 1111270. We would like to thank the young adults and parents and social coaches who participated in the project. Open access publishing facilitated by The University of Sydney, as part of the Wiley ‐ The University of Sydney agreement via the Council of Australian University Librarians.
Honan I, Sharp N, McIntyre S, et al. Program evaluation of an adapted PEERS® social skills program in young adults with autism spectrum disorder and/or mild intellectual impairment and social skills difficulties. J Eval Clin Pract. 2023;29:126‐135. 10.1111/jep.13743
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- 1. Yeates KO, Bigler ED, Dennis M, et al. Social outcomes in childhood brain disorder: a heuristic integration of social neuroscience and developmental psychology. Psychol Bull. 2007;133(3):535‐556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. White SW, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: a review of the intervention research. J Autism Dev Disord. 2007;37(10):1858‐1868. [DOI] [PubMed] [Google Scholar]
- 3. East LJ, Orchard TR. ‘Why can't I?’: an exploration of sexuality and identity among Canadian youth living with physical disabilities. J Youth Stud. 2014;17(5):559‐576. [Google Scholar]
- 4. Wiegerink DJ, Roebroeck ME, Donkervoort M, Stam HJ, Cohen‐Kettenis PT. Social and sexual relationships of adolescents and young adults with cerebral palsy: a review. Clin Rehabil. 2006;20(12):1023‐1031. 10.1177/0269215506071275 [DOI] [PubMed] [Google Scholar]
- 5. Wiegerink DJ, Roebroeck ME, van der Slot WM, Stam HJ, Cohen‐Kettenis PT. Importance of peers and dating in the development of romantic relationships and sexual activity of young adults with cerebral palsy. Dev Med Child Neurol. 2010;52(6):576‐582. 10.1111/j.1469-8749.2010.03620.x [DOI] [PubMed] [Google Scholar]
- 6. Matson JL, Hattier MA, Belva B. Treating adaptive living skills of persons with autism using applied behavior analysis: a review. Res Autism Spectr Disord. 2012;6(1):271‐276. [Google Scholar]
- 7. Reichow B, Steiner AM, Volkmar F. Social skills groups for people aged 6 to 21 with autism spectrum disorders (ASD). Campbell Syst Rev. 2012;8(1):1‐76. [DOI] [PubMed] [Google Scholar]
- 8. English B, Tickle A. Views and experiences of people with intellectual disabilities regarding intimate relationships: a qualitative metasynthesis. Sex Disabil. 2018;36(2):149‐173. [Google Scholar]
- 9. Cederlund M, Hagberg B, Billstedt E, Gillberg IC, Gillberg C. Asperger syndrome and autism: a comparative longitudinal follow‐up study more than 5 years after original diagnosis. J Autism Dev Disord. 2008;38(1):72‐85. [DOI] [PubMed] [Google Scholar]
- 10. Kapp S, Gantman A, Laugeson E. Transition to adulthood for high‐functioning individuals with autism spectrum disorders. In: Mohammadi M, ed. A Comprehensive Book on Autism Spectrum Disorders. Intech; 2011:451‐478. 10.5772/21506 [DOI] [Google Scholar]
- 11. Laugeson EA. PEERS® for Young Adults: Social Skills Training for Adults with Autism Spectrum Disorder and Other Social Challenges. Taylor and Francis; 2017. [Google Scholar]
- 12. Laugeson EA, Frankel F, Gantman A, Dillon AR, Mogil C. Evidence‐based social skills training for adolescents with autism spectrum disorders: the UCLA PEERS program. J Autism Dev Disord. 2012;42(6):1025‐1036. 10.1007/s10803-011-1339-1 [DOI] [PubMed] [Google Scholar]
- 13. Laugeson EA, Gantman A, Kapp SK, Orenski K, Ellingsen R. A randomized controlled trial to improve social skills in young adults with autism spectrum disorder: the UCLA PEERS(R) program. J Autism Dev Disord. 2015;45(12):3978‐3989. 10.1007/s10803-015-2504-8 [DOI] [PubMed] [Google Scholar]
- 14. Laugeson EA, Frankel F, Mogil C, Dillon AR. Parent‐assisted social skills training to improve friendships in teens with autism spectrum disorders. J Autism Dev Disord. 2009;39(4):596‐606. 10.1007/s10803-008-0664-5 [DOI] [PubMed] [Google Scholar]
- 15. Schohl KA, Van Hecke AV, Carson AM, Dolan B, Karst J, Stevens S. A replication and extension of the PEERS intervention: examining effects on social skills and social anxiety in adolescents with autism spectrum disorders. J Autism Dev Disord. 2014;44(3):532‐545. 10.1007/s10803-013-1900-1 [DOI] [PubMed] [Google Scholar]
- 16. Gantman A, Kapp SK, Orenski K, Laugeson EA. Social skills training for young adults with high‐functioning autism spectrum disorders: a randomized controlled pilot study. J Autism Dev Disord. 2012;42(6):1094‐1103. 10.1007/s10803-011-1350-6 [DOI] [PubMed] [Google Scholar]
- 17. Miodrag N, Hodapp RM. Chronic stress and health among parents of children with intellectual and developmental disabilities. Curr Opin Psychiatr. 2010;23(5):407‐411. [DOI] [PubMed] [Google Scholar]
- 18. Chambers HG, Chambers JA. Effects of caregiving on the families of children and adults with disabilities. Phys Med Rehabil Clin. 2015;26(1):1‐19. [DOI] [PubMed] [Google Scholar]
- 19. Curryer B, Stancliffe RJ, Dew A. Self‐determination: adults with intellectual disability and their family. J Intellect Dev Disabil. 2015;40(4):394‐399. [Google Scholar]
- 20. Ahrens K, DuBois DL, Lozano P, Richardson LP. Naturally acquired mentoring relationships and young adult outcomes among adolescents with learning disabilities. Learn Disabil Res Pract. 2010;25(4):207‐216. 10.1111/j.1540-5826.2010.00318.x [DOI] [Google Scholar]
- 21. Ryan CT, Kramer JM, Cohn ES. Exploring the self‐disclosure process in peer mentoring relationships for transition‐age youth with developmental disabilities. Intellect Dev Disabil. 2016;54(4):245‐259. 10.1352/1934-9556-54.4.245 [DOI] [PubMed] [Google Scholar]
- 22. Fetters MD, Molina‐Azorin JF. Utilizing a Mixed Methods Approach for Conducting Interventional Evaluations. Sage Publications; 2020. [Google Scholar]
- 23. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage Publications; 2017. [Google Scholar]
- 24. Constantino JN, Gruber CP. Social Responsiveness Scale: SRS‐2. Western Psychological Services; 2012. [Google Scholar]
- 25. DiTommaso E, Spinner B. The development and initial validation of the Social and Emotional Loneliness Scale for Adults (SELSA). Pers Individ Differ. 1993;14(1):127‐134. 10.1016/0191-8869(93)90182-3 [DOI] [Google Scholar]
- 26. Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: a focus on trustworthiness. SAGE Open. 2014;4(1):2158244014522633. 10.1177/2158244014522633 [DOI] [Google Scholar]
- 27. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107‐115. 10.1111/j.1365-2648.2007.04569.x [DOI] [PubMed] [Google Scholar]
- 28. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. 2004;24(2):105‐112. 10.1016/j.nedt.2003.10.001 [DOI] [PubMed] [Google Scholar]
- 29. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277‐1288. 10.1177/1049732305276687 [DOI] [PubMed] [Google Scholar]
- 30. Vaismoradi M, Jones J, Turunen H, Snelgrove S. Theme development in qualitative content analysis. J Nurs Educ Pract. 2016;6(5):100‐110. 10.5430/jnep.v6n5p100 [DOI] [Google Scholar]
- 31. Moseholm E, Fetters MD. Conceptual models to guide integration during analysis in convergent mixed methods studies. Method Innovat. 2017;10(2):2059799117703118. 10.1177/2059799117703118 [DOI] [Google Scholar]
- 32. Jose PE, Ryan N, Pryor J. Does social connectedness promote a greater sense of well‐being in adolescence over time? J Res Adolesc. 2012;22(2):235‐251. 10.1111/j.1532-7795.2012.00783.x [DOI] [Google Scholar]
- 33. Orsmond GI, Shattuck PT, Cooper BP, Sterzing PR, Anderson KA. Social participation among young adults with an autism spectrum disorder. J Autism Dev Disord. 2013;43(11):2710‐2719. 10.1007/s10803-013-1833-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Sittanomai N, Laugeson E, Chantaratin S, et al. Social skills training using the Thai version of UCLA PEERS® in Thai adolescents with autism spectrum disorder. Siriraj Med J. 2021;73(7):471‐477. 10.33192/Smj.2021.61 [DOI] [Google Scholar]
- 35. Yamada T, Miura Y, Oi M, et al. Examining the treatment efficacy of PEERS in Japan: improving social skills among adolescents with autism spectrum disorder. J Autism Dev Disord. 2020;50(3):976‐997. 10.1007/s10803-019-04325-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Jagersma GA, Idris SA, Jacobs SO, van Pelt BJ, Greaves‐Lord KI. Nederlandse hertaling van de PEERS®‐training. Wetenschappelijk Tijdschrift Autisme. 2018;17(3):31‐46. [Google Scholar]
- 37. Yoo HJ, Bahn G, Cho IH, et al. A randomized controlled trial of the Korean version of the PEERS® parent‐assisted social skills training program for teens with ASD. Autism Res. 2014;7(1):145‐161. 10.1002/aur.1354 [DOI] [PubMed] [Google Scholar]
- 38. Rabin SJ, Laugeson EA, Mor‐Snir I, Golan O. An Israeli RCT of PEERS®: intervention effectiveness and the predictive value of parental sensitivity. J Clin Child Adolesc Psychol. 2021;50(6):933‐949. 10.1080/15374416.2020.1796681 [DOI] [PubMed] [Google Scholar]
- 39. Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. 2014;35(1):29‐45. 10.1146/annurev-publhealth-032013-182440 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary File: Guidelines for Good Reporting of a Mixed Methods Study (GRAMMS)40.
Supporting information.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.