

Abstract
Dexterous manipulation of a multi-fingered prosthetic hand requires far more cognitive effort compared to typical 1 degree of freedom hands, which hinders their acceptance clinically. This paper presents a Myoelectrically-Operated Radio Frequency Identification (RFID) Prosthetic Hand (MORPH); an implementation of RFID with a myoelectric prosthetic hand as a means to amplify the controllable degrees of freedom. Contextual information from an object equipped with an RFID tag allows automatic preshaping along with dexterous control in an attempt to reduce the cognitive effort required to operate the terminal device. The myoelectric-RFID hybrid has been demonstrated in a proof-of-concept case study where an amputee was fitted with the device and subjected to activities adapted from the Jebsen Hand Function Test and the Smith Hand Function Evaluation with RFID-tagged and untagged items. Evaluation tests revealed that the MORPH system performed significantly better in 4 of the 8 tasks, and comparable to the control in the remainder.
I. Introduction
Although the majority of amputees are using cosmetic and body-powered prosthetic hands, more and more of these individuals are beginning to use myoelectric prostheses [1]; controlled by bioelectric signals generated by the contraction of the user’s muscles. Until recently, these prosthetic devices were little more than 3-pronged claws capable of gross open and close motions. Because of the relative simplicity of these devices, adequate control may be achieved by merely thresholding the myoelectric signals (MES) recorded from electrodes placed over an antagonistic pair of flexor and extensor muscles on the residual limb [2]. The downside of this simple decoding is that only one degree of freedom (DOF) can be controlled at a time, i.e. flexion would result in the entire hand closing while extension would cause the hand to completely open again. With further actions such as a co-contraction, it is possible to switch between additional DOFs, but this can prove inefficient for hands and arms needing higher controllability.
Recent advances in robotics have resulted in the arrival of multi-fingered prosthetic hands such as the Touch Bionics i-LIMB (Livingston, UK), and the RSLSteeper BeBionic (San Antonio, TX). These devices have far more operable DOFs than previous hands; however, they are effectively restricted to simple open and close behavior due to the continued use of traditional MES thresholding techniques.
In order to take advantage of the additional functionality offered by the i-LIMB, Touch Bionics has employed a crude method to operate various grasp types. With the i-LIMB, users can manually restrain individual fingers on the device, allowing the formation of different grips. While this solution does offer additional functionality, it requires the user to interact with some opposing force which may prove clumsy or inconvenient for bimanual tasks, and cognitively distracting in general.
Several other approaches are being investigated to enable greater functionality in these prosthetic limbs. Pattern recognition of surface MES signals has been at the forefront of prosthetic research for nearly the last two decades; resulting in progress towards up to ten different classifiable actions [3–6]. This is an active area of research but has not yet found commercial acceptability due to the repetitive training required [7], and its unreliability in real-world applications [8].
Recently, there have been some attempts at utilizing various sensors to mine information from the environment. Kyberd et al. [9] and Schneiter et al. [10] have shown prototypes of systems that utilize touch sensors to determine the right grip; but when applied to so many unpredictable shapes, there will certainly be misclassifications of the desired grasp. In addition, some investigators have used cognitive vision systems (CVS) [11, 12] in order to control lower-level dexterous movements; but these setups are large and difficult to miniaturize into prostheses.
In the paper, we describe a system that removes the cognitive effort required to manually form preshapes and eliminates the need for complicated control algorithms, expensive sensors, or bulky CVS. The central idea is to use RFID to provide contextual information such that a myoelectrically controlled hand may automatically form dexterous grips relevant to the object it is interacting with. The resultant Myoelectrically-Operated RFID Prosthetic Hand (MORPH) provides the means to program prostheses that can recognize objects and associate with them appropriate grip postures. The hand may then open and close in unique ways relevant to the task without changing the traditional one DOF myoelectric control scheme that is implemented in nearly every commercial prosthetic hand on the market. This ability to work with a one DOF control scheme expands the utility of the current and future generations of prosthetic limbs.
II. Description of the MORPH prototype
A. Radio Frequency Identification
RFID provides an ideal technology with the potential for miniaturization and incorporation in prostheses. The RFID interrogator emits radio frequency signals that have the ability to identify an RFID tag, through inductive coupling, over a relatively short range. Each RFID tag can be programmed to elicit a specific grip posture of the prosthetic hand.
B. The MORPH Prototype
The MORPH was developed to dramatically enhance the functionality of commercially available myoelectric devices while maintaining a control scheme that is robust, intuitive, and simple for the user. Contextual information provided from an identifier, e.g. RFID, can allow a simple 1 DOF thresholding system to control the capabilities of these newer arms.
The MORPH consists of two stages: an automatic RFID-controlled grip preshaping stage, and a voluntary myoelectric control stage for dexterous manipulation. When an object comes within range of the RFID antenna, there is lower-level automation to create the appropriate hand formation, i.e. for picking up a small object: flexion of the middle, ring, and pinky fingers coordinated with extension of the index and thumb. After the user has approached the object, he will generate the EMG signals typically used to fully open or close the hand which operate the relevant individual finger motors in a gripping action, i.e. for a pinch grasp: the flexion or extension of only the thumb and index while the other digits remain stationary. The state diagram for the system is illustrated in Fig. 1. Further customizations are easily implementable as with current myoelectric prosthetic hands to provide proportional control or to allow for the exit of a preshape through a muscle co-contraction.
Fig. 1.
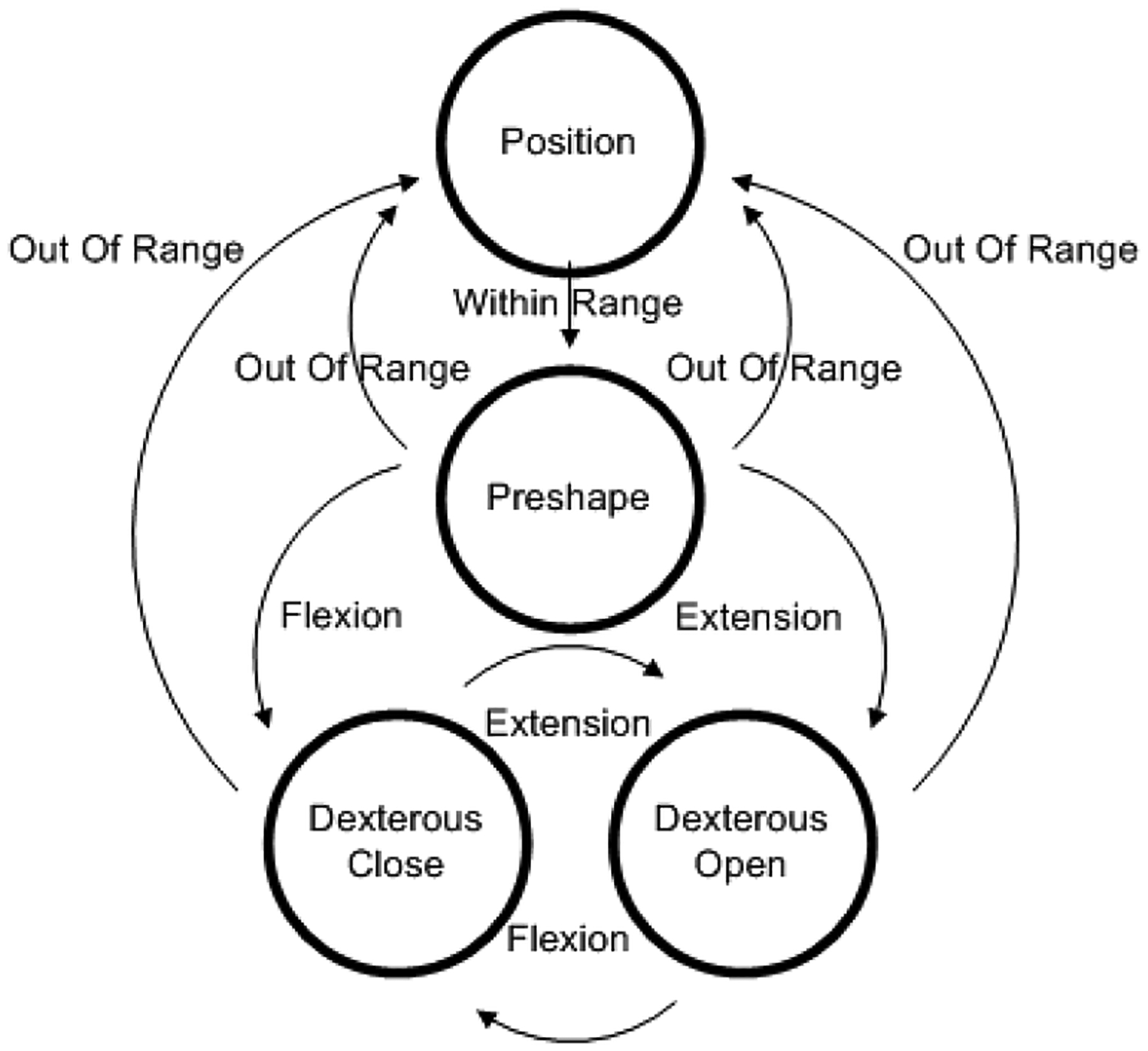
State diagram of the MORPH. Control is mediated by electromyographic input and/or successful RFID identifications.
Our experimental setup consists of a two-electrode, transradial prosthetic socket attached to a Touch Bionics i-LIMB. The MORPH system was secured to the socket by a screw that enters the rear of the coaxial connector as in Fig. 2. The MORPH circuit board was prototyped with a Roving Networks Bluetooth module (Los Gatos, CA) wired to a Microchip dsPIC (Chandler, Arizona), and an ID Innovations ID2 RFID Reader (Canning Vale, Australia) incorporating a custom built RFID antenna wound around the circuit board housed within the prosthetic wrist. The microcontroller communicates with the i-LIMB via serial peripheral interface (SPI) through the prosthetic coaxial connector. The commands travel to custom boards within the hand, capable of controlling individual digits. Although the hand is highly customized, collaboration with Touch Bionics and BeBionic are moving towards seamless integration with hands off the shelf.
Fig. 2.
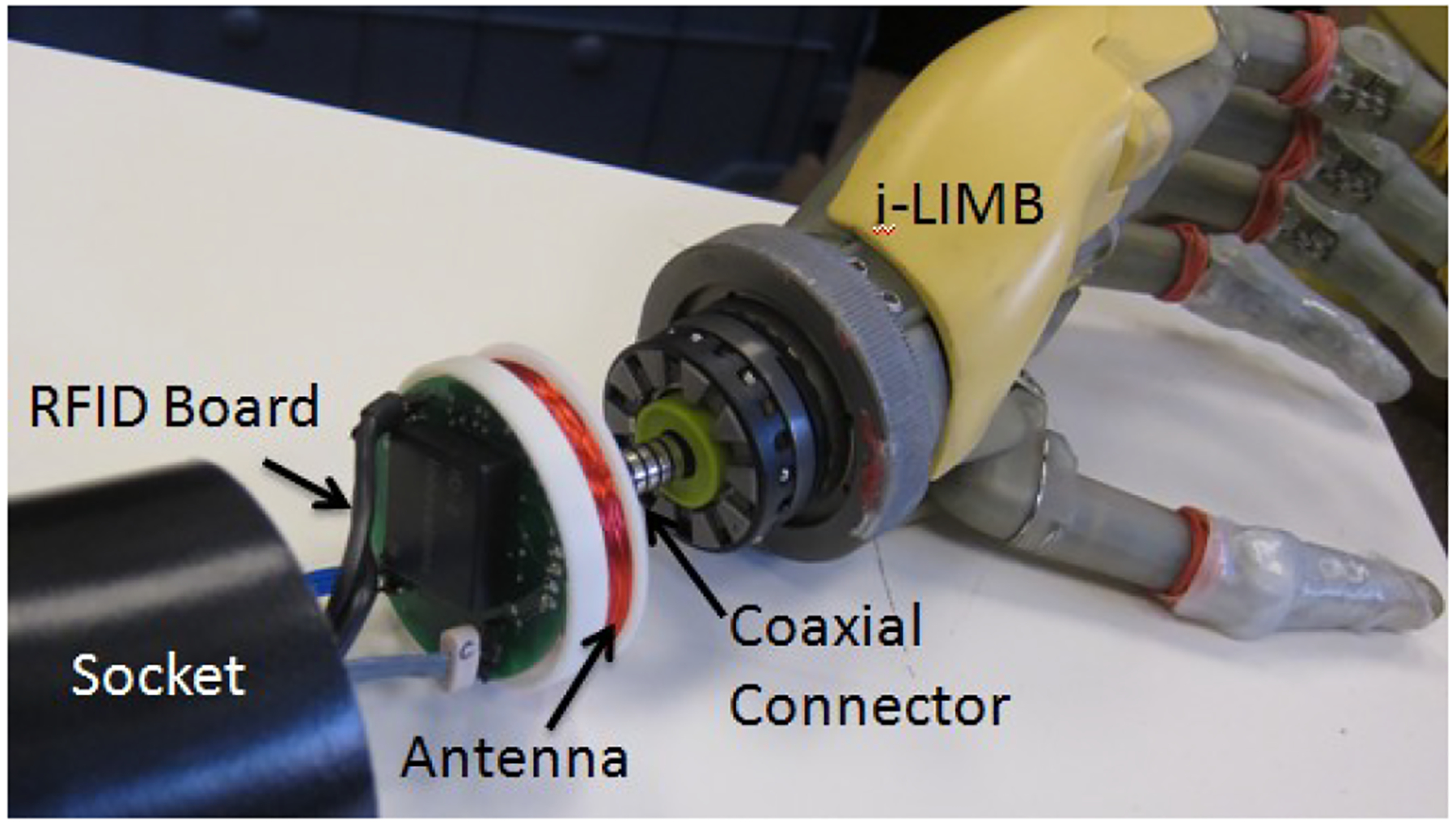
The labeled image of the MORPH prototype is shown in detail. The RFID board and antenna fit inside the socket, and is secured to the coaxial connector. The Otto Bock electrode connections along with wires running to a battery can be seen on the socket side of the PCB.
III. Methods
A. Subject
The study was a within-subject repeated-measures design. One amputee subject participated in the experiment. The subject is a male unilateral below-elbow amputee, aged 46, who lost his right hand in a construction accident in 2002. He currently has many prosthetic limbs at his disposal with a body-powered hook and an i-LIMB serving as his preferred devices.
B. The Jebsen and Smith Prosthetic Evaluation Report
In order to demonstrate that the RFID system has a significant benefit, we cannot simply measure latency and accuracy as is typical for most control schemes. It is important to be able to demonstrate functionally that an amputee equipped with this system will be more adept and have an easier time completing complicated tasks. Since the 1960s, there have been a multitude of functional tests developed and verified [13, 14]. For this experiment, we have meticulously chosen some tests from Jebsen [15] and Smith [16] to create the Jebsen and Smith Prosthetic Evaluation Report (JASPER) which focuses on the hand’s functionality in relation to forming specific dexterous grasps.
Jarus et al. [17] demonstrated that the Jebsen Hand Function Test (JHFT) and the Smith Hand Function Evaluation (SHFE) together provided a multitude of tests specifically capable of a standardized evaluation, quick and reliable administration, and easy fabrication. However, either test alone proves insufficient for our needs due to redundancy of tasks, and tests that are not particularly representative, e.g. handwriting. Jarus applied a factor analysis to a study with one hundred and sixty five volunteers performing both tests and noted which activities resulted in substantial factor loadings [17]. Eight tests highly rated by Jarus were taken from the JHFT and the SHFE to create the JASPER and can be found in Table I.
TABLE I.
Tasks in the JASPER
| Task | Type of Grasp Required | Test From |
|---|---|---|
| Large Heavy Objects | Power | JHFT |
| Large Light Objects | Power | JHFT |
| Zipper | Lateral | SHFE |
| Simulated Feeding | Lateral | JHFT |
| Blocks | Precision, 3 Jaw Chuck, Power | SHFE |
| Large Pegs | Precision | SHFE |
| Tie Knot | Precision | SHFE |
| Small Objects | Precision | JHFT |
Table I. The eight tests and the associated grasps required for performance. The tasks were chosen based off of the substantial factor loading analysis from Jarus et al. and to achieve a good representation of the four main grasps used in activities of daily living.
C. Experimental Procedures
In our experiment, we contrast our system against normal operation of the i-LIMB, i.e. manipulating the hand to stall specific motors in order to produce a particular grasp shape.
The subject was asked to perform the JASPER with the i-LIMB MORPH system which had been retrofitted into a socket the subject had donated. When tags are present, preshaping and dexterous grasping occurs, otherwise the hand operates as a normal i-LIMB. In this way, there is no bias due to a better or faster hand, or thresholding algorithm.
Each task was performed a total of ten times; alternating from with-RFID to without-RFID five times. The subject was allowed fifteen minutes to familiarize himself with different preshapes and tasks with and without RFID tags, and to practice each task 2–3 times before each trial began. The detailed protocol for each task can be found in the instructions provided by Jebsen [15] and Smith [16].
A digital stopwatch incorporating a start/stop push button and an elapsed-time readout was constructed akin to Light’s Southampton Hand Assessment Procedure [13] in order to avoid subjective assessment, and to provide a magnitude effect rather than a relative qualitative ranking. The subject will self start each iteration by pressing the button with the terminal device, followed by manipulation of the objects, and concluded by pressing the button again to stop the timer. Total summation of times or an overall functionality score are not needed because we are simply testing whether the MORPH system provides quicker and cognitively less challenging completion of these representative tasks within subject, and within each task.
D. Statistical Analysis
The median and interquartile range was determined for each of the ten unique scenarios. Additionally, a paired t-test for samples with unequal variances was used to compare the data within the subject to determine if differences in mean times were statistically significant.
IV. Results
The times for all five trials of each task with and without RFID tags is illustrated in Fig. 3. Because our objective was to determine the benefit or detriment associated with the MORPH system, it is important to note that when using the hand without RFID tags and without automatic hand preshapes, the subject was instructed to manually form the recommended preshape by restricting the flexion or extension of certain digits as is recommended for forming dexterous grips with the i-LIMB.
Fig. 3.
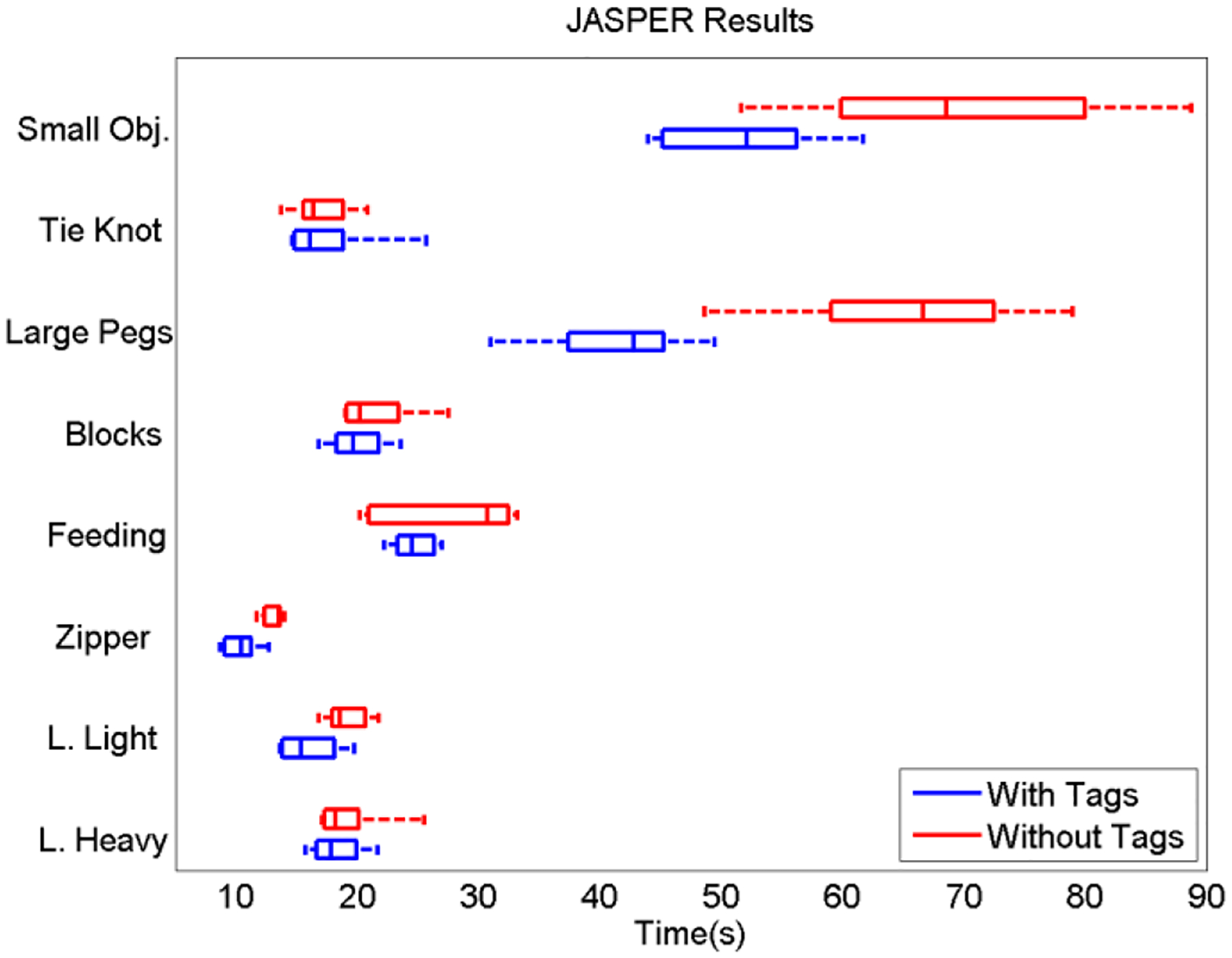
A box and whisker plot illustrating the median, and extreme values of the timed JASPER results (n=5 repetitions). Large Light Objects, Zipper, Large Pegs, and Small Objects show statistically significant quicker results with the MORPH system.
The paired t-test indicated that for Large Light Objects, the Zipper, Large Pegs, and Small Objects, the MORPH system performed significantly better (p < 0.05) than normal i-LIMB control. There were no tasks where the normal system performed statistically better.
V. Discussion
In half of the experimental tasks, the MORPH system performed significantly better, and in the rest, it had comparable mean completion times to the normal i-LIMB. The results from this subject and study are in favor of the MORPH as an improvement to traditional myoelectric control. Although this study requires additional subjects and experimental situations, we believe for numerous reasons that sharing the control of the terminal device with an automated RFID protocol will have practical benefits on the lives of amputees exceeding what these quantitative results portray.
First, the ability to automatically form the appropriate preshape when near a tagged object significantly decreases the cognitive effort required, and maintains the ability to independently perform bimanual tasks.
A second factor is that any open or close motion does not lose the original preshape or the dexterity of the manipulation. If manual interference is used to shape a terminal device into a pinch grip, and the user misses with the first close attempt, when an open command is given to try again, all fingers will extend unless a manual restriction is applied once more. The MORPH system allows for dexterous opening and closing of the relevant digits as needed until the mode is exited.
This problem was evident in the unilateral precision tasks: Small Objects and Large Pegs. For these two, the MORPH system not only outperformed the method of manual grasp formation in completion time, but there was also less variance for the task. The amount of variance within a task was noticeably related to the cognitive effort involved. There were times when it was confusing and distracting to have to continually reform the grasp shape and this added to the spread of the data.
While it is difficult to draw firm conclusions on the efficacy of the MORPH system from an experiment with limited tasks and subjects, it is worthwhile to note how this system complements or enhances the capabilities of hands in experimental phases or in the current marketplace.
There are some limitations as well. Obviously, it is not practical to tag every object an amputee may happen upon and desire to handle. The scope of this system is for a highly customized environment such as the user’s household or office work space. While outside of these situations, the hand operates exactly as it would without the MORPH system, so no functionality from the original device is lost. However, it is possible for a user to bring a tagged object when these functionalities may be needed, e.g. an eating utensil to a restaurant.
Due to manual antenna construction and a low-power RFID reader, the system has poor range. The current prototype requires the user to almost contact the RFID tag directly with the antenna located in the wrist. Future iterations of the MORPH system are intended to improve range by designing a custom RFID reader with more power, and moving the antenna to a digit extremity to make reading tags a more natural part of the reach to grasp motion.
VI. Conclusion
In this study, we introduced the MORPH control system and initiated experimentation with an amputee performing functional dexterous tasks. In these exercises, we showed that for a single subject studied, the MORPH behaved favorably and may offer a beneficial improvement to traditional myoelectric control.
The applications for the MORPH system are numerous. Beyond greatly simplifying the operation of anthropomorphic hands with many degrees of freedom, other avenues of lower-level control are feasible. The MORPH represents a technological advancement in providing lower-level control and degrees of freedom. It is also readily compatible with prosthetic system and control algorithms already on the market. Therefore, we hope that the MORPH technology presented herein will be highly relevant to improvements in prosthetic controllability and the quality of life for amputees worldwide.
Acknowledgments
This work was supported in part by the National Institutes of Health under Grant 1R44NS065495-01.
Contributor Information
Matthew S. Trachtenberg, Johns Hopkins University, Baltimore, MD 21218 USA
Girish Singhal, Machina Technologies, LLC, Baltimore, MD 21218 USA..
Rahul Kaliki, Machina Technologies, LLC, Baltimore, MD 21218 USA..
Ryan J. Smith, Johns Hopkins University, Baltimore, MD 21218 USA
Nitish V. Thakor, Johns Hopkins University, Baltimore, MD 21218 USA.
References
- [1].Biddiss EA and Chau TT, “Upper limb prosthesis use and abandonment: A survey of the last 25 years,” Prosthet. Orthot. Int, vol. 31, pp. 236–257, Sep 2007. [DOI] [PubMed] [Google Scholar]
- [2].Muzumdar A, ed. Powered upper limb prostheses: control, implementation and clinical application: Springer-Verlag, 2004. [Google Scholar]
- [3].Kuiken TA, et al. , “Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms,” JAMA, vol. 301, p. 619–628, Feb. 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Englehart K and Hudgins B, “A robust, real-time control scheme for multifunction myoelectric control,” IEEE Trans. Biomed. Eng, vol. 50, no. 7, pp. 848–854, Jul. 2003. [DOI] [PubMed] [Google Scholar]
- [5].Sebelius FC, Rosén BN, and Lundborg GN, “Refined myoelectric control in below-elbow amputees using artificial neural networks and a data glove,” J. Hand Surg. [Amer.], vol. 30, pp. 780–789, 2005. [DOI] [PubMed] [Google Scholar]
- [6].Tenore FV, et al. , “Decoding of individuated finger movements using surface electromyography,” IEEE Trans. Biomed. Eng, vol. 56, p. 1427–1434, May 2009. [DOI] [PubMed] [Google Scholar]
- [7].Tkach D, Huang H, and Kuiken TA, “Study of stability of time-domain features for electromyographic pattern recognition,” J. Neural Eng. Rehab, vol. 7, no. 21, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Zecca M, et al. , “On the control of multifunctional prosthetic hands by processing the electromyographic signal,” Crit. Rev. Biomed. Eng, vol. 30, no. 04–06 p. 459–485, 2002. [DOI] [PubMed] [Google Scholar]
- [9].Kyberd PJ and Chappell PH, “The southampton hand: an intelligent myoelectric prosthesis,” J. Rehab. Res. Dev, vol. 31, p. 326–334, 1994. [PubMed] [Google Scholar]
- [10].Schneiter JL and Sheridan TB, “An automated tactile sensing strategy for planar object recognition and localization,” IEEE Trans. Pattern Anal. Mach. Intell, vol. 12, pp. 775–786, 1990. [Google Scholar]
- [11].Došen S, et al. , “Cognitive vision system for control of dexterous prosthetic hands: Experimental evaluation,” J. Neural Eng. Rehab, vol. 7, p. 42, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Furukawa N, et al. , “Dynamic regrasping using a high-speed multifingered hand and a high-speed vision system,” Proc. of IEEE Int. Conf. on Robotics and Automation, pp. 181–187, 2006. [Google Scholar]
- [13].Light CM, Chappell PH, and Kyberd PJ, “Establishing a standardized clinical assessment tool of pathologic and prosthetic hand function: Normative data, reliability, and validity,” Arch. Phys. Med. Rehabil, vol. 83, pp. 776–783, Jun. 2002. [DOI] [PubMed] [Google Scholar]
- [14].McPhee S, “Functional hand evaluations: A review,” Amer. J. Occup. Ther, vol. 41, p. 158–163, 1987. [DOI] [PubMed] [Google Scholar]
- [15].Jebsen RH, et al. , “An objective and standardized test of hand function,” Arch. Phys. Med. Rehab, vol. 50, p. 311–319, 1969. [PubMed] [Google Scholar]
- [16].Smith HB, “Smith hand function evaluation,” Amer. J. Occup. Ther, vol. 27, pp. 24–51, 1973. [PubMed] [Google Scholar]
- [17].Jarus T and Poremba R, “Hand function evaluation: a factor analysis study,” Amer. J. Occup. Ther, vol. 47, p. 439, 1993. [DOI] [PubMed] [Google Scholar]