

Summary
Few studies have examined racial/ethnic differences in rates and correlates of insomnia among veterans. This study compared rates of insomnia and interest in sleep treatment among veterans of diverse racial/ethnic backgrounds. Consistent with the 3P model, we tested racial discrimination as a predictor of insomnia, with post-traumatic stress disorder symptoms and romantic partners as perpetuating and protective moderators of this association, respectively. A total of 325 veterans (N = 236 veterans of colour; 12% Asian, 36% Black, 14% Hispanic/Latine) completed questionnaires online from remote locations. Descriptive statistics were used to compare patterns across racial/ethnic groups. Linear regression was used to test moderators of the association between racial discrimination and insomnia severity. Overall, 68% of participants screened positive for insomnia: 90% of Asian; 79% of Hispanic/Latine; 65% of Black; and 58% of White participants. Of those, 74% reported interest in sleep treatment, and 76% of those with partners reported interest in including their partner in treatment. Racial discrimination and post-traumatic stress disorder were correlated with more severe insomnia, while romantic partners were correlated with less severe insomnia. Only post-traumatic stress disorder moderated the association between racial discrimination and insomnia severity. Rates of insomnia were highest among Asian and Hispanic/Latine participants, yet these groups were among the least likely to express interest in sleep treatment. Racial discrimination may exacerbate insomnia symptoms among veterans, but only among those who do not already have disturbed sleep in the context of post-traumatic stress disorder. Romantic partners may serve as a protective factor in insomnia, but do not seem to mitigate the impact of racial discrimination.
Keywords: discrimination, partner, post-traumatic stress disorder, relationships, sleep
1 |. INTRODUCTION
One in three adults in the USA will experience insomnia at some point in their lives (Ohayon, 2011). Insomnia has been associated with higher risk for comorbid conditions, including post-traumatic stress disorder (PTSD), depression, and alcohol use disorder (Byrne et al., 2021) and trajectories of insomnia worsen with age (Kaufmann et al., 2016). Thus, insomnia is a prevalent and persistent public health concern. Unfortunately, insomnia disproportionally affects veterans in comparison to civilian populations (Mysliwiec et al., 2013). In addition to higher rates of insomnia, veterans and military personnel report worse sleep health; for example, shorter sleep duration, worse sleep quality and more daytime sleepiness (Faestel et al., 2013; Samuel et al., 2022). Health disparities also exist across racial/ethnic groups, such that Black, Hispanic/Latine and Asian adults tend to experience worse sleep health than non-Hispanic White individuals (Carnethon et al., 2016; Kaufmann et al., 2016; Petrov & Lichstein, 2016). However, few studies have investigated sleep disparities across racial/ethnic groups of veterans. This study examines rates of insomnia and interest in sleep treatment in a racially diverse sample of veterans. Consistent with the “3P” model of insomnia (Spielman et al., 1987), we propose racial discrimination as an acute precipitating event for insomnia among veterans of colour. We then examine current PTSD as a compounding perpetuator of insomnia severity, and romantic relationships as a protective factor within this population.
Spielman’s “3P” model (Spielman et al., 1987) has been widely adopted to explain the development of insomnia. Consistent with stress-diathesis frameworks, the 3P model posits that Predisposing, Precipitating and Perpetuating factors explain transitions from preclinical sleep to acute and then chronic insomnia (Ellis et al., 2021; Spielman et al., 1987). First, “predisposing” factors (e.g. biology, personality traits) leave some individuals more vulnerable to insomnia than others throughout their lives. In individuals with a predisposition for sleep disturbance, stressful life events (e.g. work demands, deployment) may then trigger or “precipitate” the onset of insomnia. For some people, stress-induced sleep problems resolve with the stressor. However, some people develop thought patterns or habits that then “perpetuate” their sleep problems over time (e.g. spending excessive time in bed, worrying about sleep). These three Ps explain the development and maintenance of insomnia (Bramoweth & Germain, 2013; Ellis et al., 2021; Pruiksma et al., 2018; Spielman et al., 1987). However, in clinical practice, a fourth P is often added to identify the strengths or supportive (“protective”) factors that mitigate the negative impacts of insomnia (Macneil et al., 2012). In prevention and intervention efforts, predisposing and precipitating factors are often not the focus because they tend not to be modifiable; however, perpetuating factors are often targeted because they can be changed (Bramoweth & Germain, 2013). Protective factors are similarly important because they foster resilience and may facilitate recovery.
Racial discrimination is an acute “precipitating” factor for insomnia in diverse racial/ethnic groups. Racial discrimination is defined as differential treatment and/or distribution of resources and opportunities based on someone’s race or ethnicity (Williams, 2018). Day-to-day experiences of discrimination have been recorded in institutional settings and individual interactions (Williams, 2018), making these encounters quite prevalent for people of colour. In one national survey, 61% of adults reported everyday discrimination due to their race or ethnicity (APA, 2016). In civilian populations, racial discrimination acts as a chronic stressor that has been linked to various negative long-term health outcomes, including higher risk for insomnia and PTSD (Cheng et al., 2020; Marshall et al., 2009; Williams, 1999). Race-related stressors have also been linked to higher risk for negative mental health outcomes in veteran populations (Loo et al., 2001; Loo et al., 2005). Thus, racial discrimination may precipitate (and rumination about discrimination may perpetuate) insomnia symptoms in diverse samples of veterans.
In military and veteran samples, one particularly relevant “precipitating” event for insomnia is exposure to trauma (e.g. combat; Bramoweth & Germain, 2013; Pruiksma et al., 2018), and ongoing struggles with PTSD symptoms (e.g. distressing memories, increased arousal) may “perpetuate” sleep difficulties. Trauma exposure has been linked to sleep disturbances and insomnia severity in veteran and civilian samples (Lee & Gabriele, 2018; Xie et al., 2021). In one study, more than half of the trauma-exposed veterans were diagnosed with clinical insomnia, and PTSD symptoms were strongly correlated with insomnia severity (Rosen et al., 2019). However, the impact of trauma on sleep may also vary across racial/ethnic groups. For example, Black and Hispanic/Latina women who reported childhood trauma were more likely than White women with this experience to report short sleep and delayed sleep onset (Gaston et al., 2021). Studies investigating the cause of higher susceptibility to trauma in diverse racial/ethnic groups suggest that race-related adversity during childhood (e.g. racial discrimination, racism, social injustices) may play a role (Bernard et al., 2021; Slopen et al., 2015; Williams, 1999). In particular, racial discrimination has been linked to both race/ethnicity and insomnia severity, with some investigators suggesting it may explain these associations across racial/ethnic civilian groups (Cheng et al., 2020). Other studies also indicate that experiences of racial discrimination may exacerbate risk for both PTSD (Loo et al., 2001; Marshall et al., 2009) and sleep disturbances (Xie et al., 2021).
In contrast to racial discrimination and PTSD, which precipitate and/or perpetuate insomnia symptoms, strong romantic partnerships may play a protective role. Veterans tend to report more interest in seeking treatment if interventions are family-focused (Khaylis et al., 2011), and many indicate that encouragement from friends and family would facilitate treatment-seeking (Warner et al., 2008). Consistent with recommendations to include partners in mental health treatment among veterans (Monk et al., 2018), multiple studies have theorised and tested the impact of romantic partners on sleep patterns (Troxel et al., 2022). Previous work has demonstrated that partners impact not only patients’ sleep (Arpin et al., 2018; Fillo et al., 2017), but also their response to sleep treatment (Ellis et al., 2015). However, few studies have reported veterans’ interest in including partners in sleep treatment, particularly across racial/ethnic groups.
This study aimed to compare rates of insomnia across racial/ethnic groups of veterans. Based on data in civilian samples (Chen et al., 2015; Grandner et al., 2010; Kaufmann et al., 2016), we hypothesised that Black, Hispanic/Latine and Asian veterans would demonstrate higher rates of insomnia than non-Hispanic White veterans. Our previous research found that veterans (as a group) demonstrate the concerning combination of high rates of sleep problems with comparatively low interest in treatment (Miller, Monk, et al., 2022). To inform future research in this area, we examined this discrepancy (rates of sleep problems versus interest in treatment) across racial/ethnic groups. Based on civilian research (Cheng et al., 2020; Xie et al., 2021), we hypothesised that racial discrimination would precipitate insomnia symptoms among veterans of diverse racial backgrounds. We then examined two theoretically relevant factors that might moderate this association: one perpetuating factor (PTSD symptoms) and one protective factor (romantic partners). Specifically, we hypothesised that racial discrimination would be: (a) more strongly associated with insomnia severity among those who also screen positive for current PTSD; and (b) less strongly associated with insomnia severity among those in romantic relationships.
2 |. MATERIALS AND METHODS
2.1 |. Participants and procedure
Eligible participants (N = 325) were adults (> 18 years) who served in the USA military. They were recruited using Qualtrics research panels in April and May 2021 to participate in a parent study examining attitudes toward health-related research among veterans (Miller, Flores, et al., 2022). Qualtrics sent panel members an invitation to participate, and those who clicked on the link and provided informed consent completed the online survey. The parent study aimed to recruit ~75% veterans of colour. All procedures were approved by the Institutional Review Board.
A total of 602 individuals responded to the initial Qualtrics invitation. Consistent with recommendations to ensure data integrity in online samples, data were screened meticulously (Griffin et al., 2021; Meyer et al., 2013). A total of 268 respondents were excluded for the following reasons: 101 only provided demographic data; 118 provided illogical responses (e.g. “hubba”); 13 reported implausible data (e.g. deployed before birth); and 36 failed random responding indicators. An additional four participants declined to disclose race/ethnicity, and five did not complete the Insomnia Severity Index (ISI), resulting in a final analytic sample of 325 participants (66% male, 73% person of colour; Table 1).
TABLE 1.
Participant demographics (N = 325)
| Descriptive variable | Total (N = 325) | Insomnia screen |
χ2/t(df) | |
|---|---|---|---|---|
| Negative (n = 104) | Positive (n = 221) | |||
| Age, M (SD) | 41.5 (14.8) | 44.8 (16.7) | 40.0 (13.6) | 2.52 (168≠)* |
| Gender, n (%) | ||||
| Female | 105 (32%) | 30 (29%) | 75 (71%) | 0.84 (1) |
| Male | 214 (66%) | 73 (34%) | 141 (66%) | 1.29 (1) |
| Non-binary or other | 6(2%) | 1 (17%) | 5 (83%) | 0.66 (1) |
| Sexual orientation, n (%) | ||||
| Straight or heterosexual | 284 (87%) | 98 (35%) | 186 (66%) | 5.74 (1)* |
| Lesbian or gay | 13 (4%) | 3 (23%) | 10 (77%) | 0.52 (1) |
| Bisexual | 19 (6%) | 1(5%) | 18 (95%) | 6.71 (1)* |
| Queer, pansexual or questioning | 7 (2%) | 2 (29%) | 5 (71%) | 0.04 (1) |
| Prefer not to respond | 2 (< 1%) | 0 (0%) | 2 (100%) | - |
| Relationship status | - | - | - | 4.69 (1)* |
| No partner, n (%) | 118 (36%) | 29 (25%) | 89 (75%) | - |
| Partner, n (%) | 207 (64%) | 75 (36%) | 132 (64%) | - |
| CSI, M (SD) | 15.7 (4.6) | 16.5 (4.5) | 15.3 (4.5) | 1.84 (205) |
| Race/Ethnicity, n (%) | ||||
| American Indian or Alaska Native | 18 (6%) | 6 (33%) | 12 (67%) | 0.02 (1) |
| Asian or Asian American | 38 (12%) | 4 (11%) | 34 (90%) | 9.12 (1)* |
| Black or African American | 116 (36%) | 41 (35%) | 75 (65%) | 0.93 (1) |
| Hispanic, Latino/a, or Latine | 47 (14%) | 10 (21%) | 37 (79%) | 2.90 (1) |
| Multiracial or Multi-ethnic | 13 (4%) | 6 (46%) | 7 (54%) | 1.25 (1) |
| Native Hawaiian or Pacific Islander | 4 (1%) | 0(0%) | 4 (100%) | 1.91 (1) |
| White, Caucasian or European | 89 (27%) | 37 (42%) | 52 (58%) | 5.16 (1)* |
| Other | 0 (0%) | 0 (0%) | 0(0%) | - |
| Military affiliation, n (%) | ||||
| Active duty | 68 (21%) | 18 (27%) | 50 (74%) | 1.21 (1) |
| Reserves/guard | 60 (19%) | 17 (28%) | 43 (72%) | 0.46 (1) |
| Separated/discharged/retired | 197 (61%) | 69 (35%) | 128 (65%) | 2.10 (1) |
| Branch of service, n (%) | ||||
| Air Force | 54 (17%) | 18 (33%) | 36 (67%) | 0.05 (1) |
| Army | 168 (52%) | 60 (36%) | 108 (64%) | 2.21 (1) |
| Coast Guard | 19 (6%) | 9 (47%) | 10 (53%) | 2.19 (1) |
| Marines | 42 (13%) | 7 (17%) | 35 (83%) | 5.21 (1)* |
| Navy | 42 (13%) | 10 (24%) | 32 (76%) | 1.49 (1) |
| Symptoms of PTSD, M (SD) | 4.5 (6.3) | 1.3 (3.5) | 6.0 (6.8) | 8.27 (321≠)* |
| Positive PTSD screen, n (%) | 76 (23%) | 4(5%) | 72 (95%) | 32.59 (1)* |
| Military-related trauma, n (%) | 55 (17%) | 3(6%) | 52 (95%) | 21.44 (1)* |
| Racial discrimination, M (SD) | 13.3 (12.8) | 8.1 (9.3) | 15.7 (13.5) | 5.17 (270≠)* |
| Insomnia severity, M (SD) | 12.5 (6.9) | 4.4 (3.1) | 16.3 (4.5) | 27.70 (276≠)* |
| Positive insomnia screen, n (%) | 221 (68%) | - | - | - |
Abbreviations: ≠, equal variance not assumed; CSI, Couples Satisfaction Index; M, mean; N, number; PTSD, post-traumatic stress disorder; SD, standard deviation.
p < 0.05.
2.2 |. Measures
2.2.1 |. Demographics
Participants selected their race from a list (see options in Table 1), and all participants were then asked to specify via open text box the subgroup that best fit their ethnicity (e.g. Creek, Navajo, Chinese, Vietnamese, Haitian). Participants were only asked to specify their gender, not their sex assigned at birth. Demographics variables (with response options) are depicted in Table 1.
2.2.2 |. Racial discrimination
The 9-item Everyday Discrimination Scale (EDS; Williams et al., 1997) prompted participants to identify how often they experience discrimination in their day-to-day lives (e.g. “people act as if they’re better than you are”). Participants in this study were asked to identify discrimination due specifically to their race/ethnicity, which is compatible with the one-stage attribution version of the measure (Shariff-Marco et al., 2011). Participants indicated their responses on a scale from 0 (never) to 5 (almost every day), and a total score (range 0–45) was created by summing their responses. This scale has shown validity in the prediction of future negative emotions, such as anger or distress, and overall discrimination (Gonzales et al., 2016; Krieger et al., 2005; Shariff-Marco et al., 2011). In this sample, internal consistency was good (α = 0.96).
2.2.3 |. Sleep variables
This study included measures of insomnia symptoms, sleep duration, nightmares, bed partners and sleep treatment preferences. The 7-item ISI (Morin et al., 2011) was used to measure insomnia symptoms. Participants responded to questions about problems staying/falling asleep and the level of distress associated with these problems over the past 2 weeks. Total scores ≥ 10 indicate a positive screen for insomnia (Morin et al., 2011), and reliability in this sample was good (α = 0.89). The Pittsburgh Sleep Quality Index (Buysse et al., 1989) “sleep duration” subscale was used to assess hours of sleep per night; specifically, participants were asked to indicate how many hours of actual sleep they got on a typical night in the past month (noting that hours of actual sleep may differ from hours spent in bed). Lifetime history of nightmares was assessed as part of a checklist of potential medical conditions; participants indicated (yes/no) if they had ever experienced nightmares. This item was included as a covariate in regression models. Finally, participants indicated how often they currently share a bed with another person (0 = never, 1 = rarely, 2 = sometimes, 3 = usually, 4 = always).
Veterans’ preferences for sleep treatment were assessed using three different items. Participants responded to the item, “Are you interested in treatment for your sleep?” (yes/no). Participants who reported having a partner (Table 1) were asked two additional questions: “If you were to seek treatment for your sleep, would you want your partner to be involved?” (yes/no), and “Do you think your partner would want to be involved in treatment for your sleep?” (yes/no/I have no idea).
2.2.4 |. PTSD symptoms
Participants were asked if they had ever experienced, witnessed or had to deal with “any event involving actual or threatened death, serious injury, or sexual violence to you or someone else.” Those who said yes were asked if any of those traumatic events were related to their military experience in any way (yes/no), and then asked to complete the 4-item version of the PTSD Checklist for DSM-5 (PCL; Price et al., 2016). Participants rated how troubled they had been by four symptoms of PTSD (having distressing memories, needing to avoid external reminders, having strong negative beliefs, and feeling jumpy or easily startled) in the past month. Responses ranged from 0 (not at all) to 4 (extremely), and were summed to create a symptom severity score ranging from 0 to 16. Scores ≥ 10 indicate a positive screen for PTSD (Price et al., 2016). When compared with the full-scale PCL-5, the 4-item version has demonstrated similar diagnostic utility. It has also shown validity in identifying PTSD in adults and combat veterans (Price et al., 2016). Reliability in this sample was good (α = 0.90).
Although it is not part of the total score, participants with PTSD also indicated how much they had been bothered by “repeated, disturbing dreams” of their traumatic event(s) in the past month. For descriptive purposes, the number of participants in each racial/ethnic group reporting at least moderate distress related to PTSD-related nightmares is depicted in Table 2.
TABLE 2.
Sleep patterns and treatment preferences in the full sample (N = 325), and those who screened positive for insomnia (N = 221)
| Am. Indian/Al. Native | Asian/Asian American | Black or African Am. | Hispanic or Latine | Native haw./Pac. Islander | Multi-racial/multi-ethnic | White | |
|---|---|---|---|---|---|---|---|
| Full sample (N = 325) | n = 18 | n = 38 | n = 116 | n = 47 | n = 4 | n = 13 | n = 89 |
| ISI total score | 12.3 (7.3) | 15.1 (5.3) | 12.2 (7.1) | 14.0 (6.8) | 15.0 (2.6) | 12.6 (9.1) | 11.0 (6.7) |
| ISI ≥ 10 | 12 (67%) | 34 (90%) | 75 (65%) | 37 (79%) | 4 (100%) | 7 (54%) | 52 (58%) |
| Sleep duration | 5.1 (2.5) | 5.2 (1.5) | 5.3 (2.0) | 5.9 (1.4) | 4.6 (1.7) | 4.9 (1.6) | 5.7 (1.7) |
| Lifetime nightmares | 9 (50%) | 21 (55%) | 56 (48%) | 23 (49%) | 1 (25%) | 5 (39%) | 29 (33%) |
| PTSD nightmaresa | 5 (28%) | 11 (29%) | 33 (28%) | 15 (32%) | 1 (25%) | 3 (23%) | 19 (21%) |
| Romantic partner | 7 (39%) | 24 (63%) | 69 (60%) | 28 (60%) | 2 (50%) | 12 (92%) | 65 (73%) |
| Bed partner | |||||||
| Never | 3 (17%) | 2 (5%) | 32 (28%) | 6 (13%) | 1 (25%) | 0 (0%) | 18 (20%) |
| Rarely | 7 (39%) | 7 (18%) | 13 (11%) | 11 (23%) | 2 (50%) | 3 (23%) | 9 (10%) |
| Sometimes | 3 (17%) | 11 (29%) | 23 (20%) | 6 (13%) | 0 (0%) | 1 (8%) | 11 (12%) |
| Usually | 1 (5%) | 6 (16%) | 16 (13%) | 5 (11%) | 0 (0%) | 2 (15%) | 19 (21%) |
| Always | 4 (22%) | 12 (32%) | 32 (28%) | 19 (40%) | 1 (25%) | 7 (54%) | 32 (36%) |
| Insomnia (N = 221) | n = 12 | n = 34 | n = 75 | n = 37 | n = 4 | n =7 | n = 52 |
| Interest in treatment | 8 (67%) | 23 (68%) | 58 (77%) | 25 (68%) | 2 (50%) | 5 (71%) | 42 (81%) |
| + romantic partner | 3/8 (38%) | 14/23 (61%) | 32/58 (55%) | 15/25 (60%) | 1/2 (50%) | 4/5 (80%) | 31/42 (74%) |
| Want partner involvedb | 2/3 (67%) | 10/14 (71%) | 26/32 (81%) | 13/15 (87%) | 1/1 (100%) | 2/4 (50%) | 22/31 (71%) |
| Partner wants to be involvedb | |||||||
| No | 1/3 (33%) | 4/14 (29%) | 6/32 (19%) | 0/15 (0%) | 0/1 (0%) | 1/4 (25%) | 8/31 (26%) |
| Yes | 1/3 (33%) | 8/14 (57%) | 23/32 (72%) | 13/15 (87%) | 1/1 (100%) | 2/4 (50%) | 17/31 (55%) |
| I have no idea | 1/3 (33%) | 2/14 (14%) | 3/32 (9%) | 2/15 (13%) | 0/1 (0%) | 1/4 (25%) | 6/31 (19%) |
Abbreviations: Am, American; Al, Alaska; Haw, Hawaiian; ISI, Insomnia Severity Index; Pac, Pacific; PTSD, post-traumatic stress disorder; Tx, treatment.
Moderately, quite a bit, or extremely bothered by nightmares in the past month.
Only administered to participants with a romantic partner (denominators listed).
2.2.5 |. Relationship variables
Response options for marital status included: (1) never married; (2) engaged to be married; (3) married; (4) domestic partnership or civil union; (5) divorced or separated; and (6) widowed. Response options for relationship status included: (1) single, not dating; (2) casually dating or talking to partners, but no exclusive partner at this time; (3) in a committed relationship with a single, exclusive partner; and (4) in a committed relationship with multiple partners. Participants who indicated that they were married, engaged to be married, or in a committed relationship (with single or multiple partners) were categorised as having a “partner”. For descriptive purposes, those with a partner completed the 4-item Couples Satisfaction Index (CSI), which asks participants to evaluate their romantic relationship (Funk & Rogge, 2007). Participants first ranked the “degree of happiness (all things considered) of your relationship” on a scale from 0 (extremely unhappy) to 6 (perfect). The remaining three items assessed warmth/comfort, reward and satisfaction with their relationship on a scale from 0 (not at all) to 5 (completely). Higher summed scores indicate higher couple satisfaction, with scores below 13.5 indicative of relationship distress. The CSI has demonstrated strong convergent and construct validity (Funk & Rogge, 2007). Reliability in this sample was good (α = 0.85).
2.3 |. Data screening and analysis plan
Data were screened for invalid and missing responses prior to analysis. No outliers were identified, and all outcome variables were normally distributed. Descriptive statistics and analysis of variance were used to characterise rates of insomnia and interest in sleep treatment across racial/ethnic groups. To reduce the likelihood of misrepresentation, these descriptions focused on the racial/ethnic groups with at least 30 participants: Asian, Black, Hispanic and non-Hispanic White. Two separate hierarchical linear regressions were then conducted among all veterans of colour (N = 236). In the hypothesised “perpetuating” model, PTSD screen (0 = PCL total score < 10; 1 = PCL total score ≥ 10) was tested as a moderator of the association between racial discrimination (EDS score) and insomnia severity (ISI score), controlling for romantic partnership. In the hypothesised “protective” model, romantic partner (0 = no, 1 = yes) was examined as a moderator of the association between racial discrimination (EDS score) and insomnia severity (ISI score), controlling for positive PTSD screen (CSI was not used as the moderator because it was only administered to participants who reported having partners; however, results were consistent when using total CSI score as the moderator in place of the “partner” variable). Age and gender (0 = female, non-binary, or other; 1 = male) were included as covariates in both models due to age- and gender-related variations in insomnia and PTSD (given the small number of non-binary and “other” gender participants, we ran models both excluding and including these participants – results did not differ, so all were included; Ford et al., 2015; Marshall et al., 2009). Both models also controlled for lifetime history of nightmares, as nightmares may contribute to sleep disturbance. Regression coefficients were used to estimate effect size. In the case of significant moderation, tests of simple slopes (Cohen et al., 2003) were used to evaluate the association between racial discrimination and insomnia severity at high and low levels of each moderator (i.e. PCL total scores < versus ≥ 10; with versus without romantic partner).
3 |. RESULTS
Descriptive statistics for the full sample and those with and without insomnia are depicted in Table 1, and descriptive statistics across racial/ethnic groups are depicted in Table 2. Overall, 68% of participants screened positive for clinically significant insomnia: 90% of Asian, 79% of Hispanic/Latine, 65% of Black and 58% of White participants. Rates of insomnia were significantly higher among Asian versus White (χ2(1) =11.74, p < 0.001), Asian versus Black (χ2(1) = 8.53, p = 0.004) and Hispanic/Latine versus White participants (χ2(1) = 5.60, p = 0.02). Group differences between White and Black (χ2(1) =0.83, p = 0.36), Asian and Hispanic/Latine (χ2(1) =1.77, p = 0.18), and Black and Hispanic/Latine participants (χ2(1) =3.08, p = 0.08) were not statistically significant.
Of the 221 who screened positive for insomnia, 163 (74%) reported interest in sleep treatment: 68% of Asian, 68% of Hispanic/Latine, 77% of Black and 81% of White participants (Table 2). Group differences in treatment interest were not significant (all p ≥ 0.16). Of the 163 with insomnia who expressed interest in treatment, 100 (61%) had a partner. Satisfaction with partners was high (M = 15.7, SD = 4.6), with 74% scoring below the cut-off for relationship distress. Of those with romantic partners, 76% agreed that they would want their partner involved in sleep treatment and 65% indicated that their partner would want to be involved (rates across race/ethnicity in Table 2).
Linear regression was used to examine positive PTSD screen as a moderator of the association between everyday racial discrimination and insomnia severity among veterans of colour, controlling for age, gender, nightmares and romantic partners. Bivariate correlations are depicted in Table 3, and main effects and interaction terms are presented in Table 4. Racial discrimination and PTSD screen were both significantly associated with insomnia severity; however, this was qualified by a significant interaction (B = −0.19, SE = 0.08, p = 0.01 [95% CI: −0.34, −0.04]). Follow-up tests of simple slopes indicated that racial discrimination was positively associated with insomnia severity among those who screened negative for PTSD (B = 0.18, SE = 0.04, p < 0.001 [95% CI: 0.09, 0.26]), but was not associated with insomnia severity among those who screened positive for PTSD (B = −0.02, SE = 0.07, p = 0.81 [95% CI: −0.14, 0.11]; see Figure 1). In terms of covariates, nightmares were linked to worse insomnia severity, and partners were linked to less insomnia severity within this model. Age and gender were not significantly associated with insomnia severity.
TABLE 3.
Bivariate correlations among veterans of colour (N = 236)
| Age | Male | EDS | PTSD | NM | Partner | |
|---|---|---|---|---|---|---|
| Age | - | |||||
| Male gender | 0.23* | - | ||||
| Racial discrimination (EDS) | −0.25* | −0.07 | − | |||
| Positive PTSD screen | −0.08 | −0.06 | 0.34* | - | ||
| Nightmares (NM) | −0.03 | 0.10 | 0.20* | 0.52* | - | |
| Romantic partner | 0.05 | 0.07 | 0.02 | −0.05 | −0.08 | - |
| Insomnia severity (ISI) | 0.02 | 0.03 | 0.29* | 0.38* | 0.33* | −0.16* |
Abbreviations: EDS, Everyday Discrimination Scale; ISI, Insomnia Severity Index; NM, nightmares; PTSD, post-traumatic stress disorder.
p < 0.05.
TABLE 4.
Main effects and interactions in the prediction of insomnia severity among veterans of colour (n = 236)
| B | SE | P | 95% CI |
||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Perpetuating factor model: PTSD | |||||
| Intercept | 7.55 | 1.75 | < 0.001 | 4.10 | 11.01 |
| Age | 0.05 | 0.04 | 0.16 | −0.02 | 0.13 |
| Male gender (Y/N) | 0.58 | 0.85 | 0.49 | −1.10 | 2.26 |
| Nightmares (Y/N) | 1.93 | 0.95 | 0.04 | 0.06 | 3.81 |
| Romantic partner (Y/N) | −1.68 | 0.82 | 0.04 | −3.31 | −0.06 |
| Discrimination | 0.18 | 0.04 | < 0.001 | 0.09 | 0.26 |
| Positive PTSD screen (Y/N) | 7.28 | 1.87 | < 0.001 | 3.60 | 10.96 |
| Discrimination x PTSD | −0.19 | 0.08 | 0.01 | −0.34 | −0.04 |
| Protective factor model: Romantic partners | |||||
| Intercept | 7.21 | 1.93 | < 0.001 | 3.41 | 11.00 |
| Age | 0.06 | 0.04 | 0.13 | −0.02 | 0.13 |
| Male gender (Y/N) | 0.65 | 0.86 | 0.45 | −1.05 | 2.34 |
| Nightmares (Y/N) | 1.90 | 0.97 | 0.05 | −0.0004 | 3.80 |
| Positive PTSD screen (Y/N) | 3.71 | 1.14 | 0.001 | 1.46 | 5.96 |
| Discrimination | 0.18 | 0.06 | 0.003 | 0.06 | 0.30 |
| Romantic partner (Y/N) | −0.46 | 1.33 | 0.73 | −3.09 | 2.17 |
| Discrimination x partner | −0.10 | 0.07 | 0.18 | −0.24 | 0.04 |
Abbreviations: CI, confidence interval; PTSD, post-traumatic stress disorder; Y/N = yes (coded 1) versus no (coded 0).
FIGURE 1.
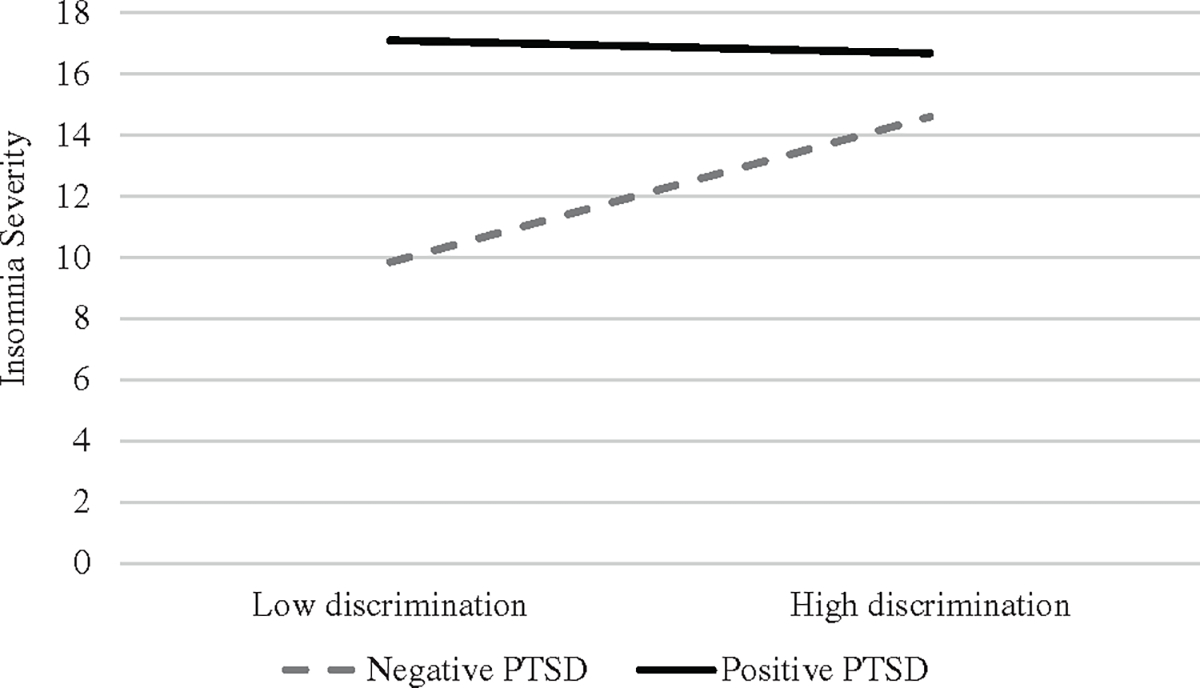
Strength of associations between racial discrimination and insomnia severity in the context of positive versus negative post-traumatic stress disorder (PTSD) screen.
A second linear regression was conducted to test romantic partner as a moderator of the association between everyday racial discrimination and insomnia severity, controlling for age, gender, nightmares and positive PTSD screen (Table 4). Again, racial discrimination was associated with worse insomnia severity (B = 0.18, SD = 0.06, p = 0.003). However, partners were not significantly linked to insomnia severity in this model (B = −0.46, SE = 1.33, p = 0.73), and there was no significant interaction (B = −0.10, SE = 0.07, p = 0.18 [95% CI: −0.24, 0.04]). Nightmares and positive PTSD screen were significant covariates (Table 4).
4 |. DISCUSSION
This study compared insomnia rates across racial/ethnic groups of veterans. Although existing literature has examined racial/ethnic health disparities in insomnia (Chen et al., 2015; Gaston et al., 2021; Grandner et al., 2010; Kaufmann et al., 2016; Lee & Gabriele, 2018; Xie et al., 2021), few have examined these trends in veteran populations. Consistent with findings in civilian populations (Chen et al., 2015; Gaston et al., 2021; Grandner et al., 2010; Kaufmann et al., 2016; Xie et al., 2021), Asian (90%) and Hispanic/Latine (79%) veterans demonstrated the highest rates of insomnia of all racial/ ethnic groups. Unfortunately, they also demonstrated the least interest in sleep treatment (both at 68%). In contrast, White veterans demonstrated relatively low rates of insomnia (58%) and relatively high interest in treatment (80%). Complementing our findings that veterans as a group are least willing to seek treatment for the conditions that are most prevalent in their communities (Miller, Monk, et al., 2022), these data indicate that participants from racial/ethnic groups with the highest need for insomnia treatment are also among the least interested. Given these findings, providers are especially encouraged to screen for sleep problems and offer sleep treatment among veterans of colour, as these minoritised groups may not share sleep issues spontaneously or request sleep treatment unprompted. Though we cannot be certain why rates of insomnia were highest among Asian veterans, Asian Americans are especially at risk for discrimination following the COVID-19 pandemic (Huang & Tsai, 2023), which may explain why they had the greatest rates of insomnia in this sample (data collected in early 2021). Individuals with marginalised racial/ethnic identities may also be more reluctant to seek treatment due to experiences of discrimination in healthcare settings, stigma surrounding mental health, less access to adequate facilities or culturally informed care, or the inability to find providers who understand their racialised experiences (Shim, 2021).
Consistent with hypotheses and previous research (Cheng et al., 2020), racial discrimination was associated with insomnia severity among veterans of colour. However, this association was only significant among those who screened negative for PTSD. We speculate that racial discrimination may not be linked to insomnia severity in the context of PTSD because veterans with PTSD have such high rates of sleep disturbance to begin with (i.e., a ceiling effect). Indeed, in this sample, all but four of those who screened positive for PTSD (95%) also screened positive for insomnia. As such, discrimination may not be linked to insomnia among veterans with PTSD because their sleep is already so disturbed.
In contrast to hypotheses, having a romantic partner did not moderate the association between racial discrimination and insomnia severity. Similarly, although rates of insomnia were higher among those who were not partnered (relative to those who were partnered), having a romantic partner was only linked to lower insomnia severity in one of the two models. This may be due to relatively high relationship satisfaction among all those with partners (regardless of insomnia status). Indeed, three out of four veterans who expressed interest in sleep treatment also expressed interest in involving their partner. This finding aligns with the research on broader mental health treatment preferences among veterans, who report that they would prefer services that are family oriented (Khaylis et al., 2011; Warner et al., 2008). In line with biopsychosocial models, which highlight covariation between relationship functioning and sleep (Troxel et al., 2022), studying and treating sleep as a dyadic (rather than individual) experience may facilitate recovery because partners influence sleep onset, quality and duration as well as response to sleep treatment (Arpin et al., 2018; Ellis et al., 2015; Fillo et al., 2017; Troxel et al., 2022). Extending data pointing to the effectiveness of including partners in sleep interventions, our findings indicate that many veterans – across most racial/ethnic groups – also prefer their partner’s inclusion.
4.1 |. Clinical implications
This study was designed to inform clinical practice. The first and perhaps most important implication is that providers working with veterans can expect at least half of their patients to report clinically relevant sleep disturbance; and these rates are even higher (closer to three out of four) among veterans of colour. Often, veterans’ sleep problems are long-standing and may even predate military service, resulting in the belief that they are intractable. Thus, clinical training in how to screen for and/or diagnose sleep disorders will enhance providers’ abilities to have effective conversations that increase veterans’ intrinsic motivation to engage in available treatments. Even brief interactions (e.g. in primary care settings) can be enhanced by knowing when to provide patients with relevant resources and referrals for evidence-based sleep treatment. The Department of Veterans Affairs and US Department of Defence have published guidelines for the diagnosis and management of insomnia and obstructive sleep apnea (Mysliwiec et al., 2020). Although sleep hygiene and pharmacotherapy are the most frequently offered treatments for insomnia, cognitive behavioural therapies for insomnia (CBT-I) should be offered first (Mysliwiec et al., 2020) and can be delivered effectively inperson, via telehealth (Arnedt et al., 2021) and even by phone (Arnedt et al., 2013). The cognitive and behavioural components of CBT-I have also demonstrated efficacy independently in dismantling studies (Harvey et al., 2014), and the behavioural components alone have demonstrated efficacy in veteran populations (Maguen et al., 2021). Although evidence is weaker, self-help books exist (e.g. Quiet Your Mind and Get to Sleep; Carney & Manber, 2009) and have improved insomnia symptoms in at least one randomised controlled trial (Jernelöv et al., 2012). Mobile apps such as Insomnia Coach (Kuhn et al., 2021) and CBT-I Coach (Miller et al., 2019) have also been developed, and online treatments are available (Bernstein et al., 2017; Ritterband et al., 2017). In line with our findings of veteran preferences for the inclusion of partners, romantic partners can influence the efficacy of CBT-I (Ellis et al., 2015), which further highlights the importance of their consideration (Troxel et al., 2022).
The prevalence of insomnia among veterans with PTSD in this sample was also striking and has clear clinical implications. Sleep disturbance was the rule (not the exception) among veterans with PTSD, meaning the above-mentioned sleep diagnostic and treatment resources are especially needed among veteran providers who specialise in PTSD. Moreover, racial discrimination was linked to insomnia severity among those who screened negative for PTSD, and veterans of colour reported the lowest rates of interest in sleep treatment. Based on these data, targeted outreach and engagement is especially needed in these communities.
4.2 |. Limitations
This work should be reviewed with limitations in mind. First, responses were collected using a single (cross-sectional), retrospective survey. This makes it impossible to know if racial discrimination, PTSD or partners are impacting insomnia severity or vice versa (e.g. perhaps people with insomnia are more vulnerable to symptoms of PTSD). All measures were also self-report, which may contribute to shared method variance and overestimation of parameters (Cole & Maxwell, 2003) and may capture different dimensions of the sleep experience than objective measures (Aili et al., 2017). Future work is needed to replicate these findings using prospective sleep monitoring (e.g. sleep diaries) and objective measures, such as actigraphy. However, we can conclude that these conditions co-occur, and racial discrimination seems to play a stronger role in insomnia outside the context of PTSD. Although the screening measures used in this study have all been validated, it is also important to acknowledge that “screening positive” for insomnia or PTSD is not the same as being diagnosed with chronic insomnia or PTSD via clinical interview with a trained professional, so true rates of Insomnia Disorder and PTSD are uncertain.
Given the plurality of men in this sample, it is also unclear if/how findings would generalise to women; and we did not recruit sufficient numbers of Native American, Alaska Native, Native Hawaiian, Pacific Islander or multiracial/multi-ethnic veterans to draw strong conclusions about these racial/ethnic groups. Given the prevalence of insomnia and PTSD among veterans, we strongly encourage multicultural work examining the unique roles of PTSD and racial discrimination in various racial/ethnic groups. Research examining unique patterns among veterans of various sexual orientations and gender identities is also encouraged to inform and help resolve health disparities in these minoritised groups as well (Carey et al., 2022).
5 |. CONCLUSION
Veterans as a group report high rates of insomnia. However, rates are even higher among veterans of colour, particularly Asian and Hispanic/Latine veterans. Although rates varied across racial/ethnic groups, three out of four veterans expressed interest in sleep treatment, and the majority indicated that they would want their partner involved in treatment. This indicates promise for sleep treatment as a gateway to mental health, but it also means that providers must be trained and prepared to connect veterans with the sleep resources that they need. Everyday experiences of racial discrimination were only associated with more severe symptoms of insomnia outside the context of PTSD, presumably because veterans with PTSD already report such high rates of insomnia. In contrast, partners may be protective against insomnia, but do not seem to mitigate the negative impact of racial discrimination on insomnia severity. Research and clinical training to improve access to sleep treatment among veterans is needed, and targeted outreach is needed for veterans of colour.
FUNDING INFORMATION
Investigator contributions to this project were supported by the National Institute on Alcohol Abuse and Alcoholism (K23AA026895, PI Miller), and the National Institute of Minority Health and Health Disparities Grant K23MD016168 (PI D. L. Bernard). The National Institutes of Health had no role in study design; data collection, analysis or interpretation; manuscript preparation; or the decision to submit for publication. The parent project was registered on Open Science Framework prior to data collection (https://osf.io/dxhj6), and data will be made available upon request.
Footnotes
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest to report. This work has not been previously disseminated.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Aili K, Astrom-Paulsson S, Stoetzer U, Svartengren M, & Hillert L (2017). Reliability of actigraphy and subjective sleep measurements in adults: The design of sleep assessments. Journal of Clinical Sleep Medicine, 13, 39–47. 10.5664/jcsm.6384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- APA. (2016). Stress in America: The impact of discrimination. https://www.apa.org/news/press/releases/stress/2015/impact-of-discrimination.pdf
- Arnedt JT, Conroy DA, Mooney A, Furgal A, Sen A, & Eisenberg D (2021). Telemedicine versus face-to-face delivery of cognitive behavioral therapy for insomnia: A randomized controlled noninferiority trial. Sleep, 44, 1–11. 10.1093/sleep/zsaa136 [DOI] [PubMed] [Google Scholar]
- Arnedt JT, Cuddihy L, Swanson LM, Pickett SM, Aikens J, & Chervin RD (2013). Randomized controlled trial of telephone-delivered cognitive behavioral therapy for chronic insomnia. Sleep, 36, 353–362. 10.5665/sleep.2448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arpin SN, Starkey AR, Mohr CD, Greenhalgh AMD, & Hammer LB (2018). “A well-spent day brings happy sleep”: A dyadic study of capitalization support in military-connected couples. Journal of Family Psychology, 32, 975–985. 10.1037/fam0000469 [DOI] [PubMed] [Google Scholar]
- Bernard DL, Calhoun CD, Banks DE, Halliday CA, Hughes-Halbert C, & Danielson CK (2021). Making the “C-ACE” for a culturally-informed adverse childhood experiences framework to understand the pervasive mental health impact of racism on black youth. Journal of Child & Adolescent Trauma, 14, 233–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein AM, Allexandre D, Bena J, Doyle J, Gendy G, Wang L, Fay S, Mehra R, Moul D, Foldvary-Schaefer N, Roizen MF, & Drerup M (2017). ‘Go! To sleep’: A web-based therapy for insomnia. Telemedicine and e-Health., 23, 590–599. 10.1089/tmj.2016.0208 [DOI] [PubMed] [Google Scholar]
- Bramoweth AD, & Germain A (2013). Deployment-related insomnia in military personnel and veterans. Current Psychiatry Reports, 15, 1–13. 10.1007/s11920-013-0401-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF III, Monk TH, Berman SR, & Kupfer DJ (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28, 193–213. [DOI] [PubMed] [Google Scholar]
- Byrne SP, McCarthy E, DeViva JC, Southwick SM, & Pietrzak RH (2021). Prevalence, risk correlates, and health comorbidities of insomnia in US military veterans: Results from the 2019–2020 National Health and resilience in veterans study. Journal of Clinical Sleep Medicine, 17, 1267–1277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey FR, LeardMann CA, Lehavot K, Jacobson IG, Kolaja CA, Stander VA, Rull RP, & Millennium Cohort Study Team. (2022). Health disparities among lesbian, gay, and bisexual service members and veterans. American Journal of Preventive Medicine, 63, 521–531. 10.1016/j.amepre.2022.04.034 [DOI] [PubMed] [Google Scholar]
- Carnethon MR, de Chavez PJ, Zee PC, Kim KYA, Liu K, Goldberger JJ, Ng J, & Knutson KL (2016). Disparities in sleep characteristics by race/ethnicity in a population-based sample: Chicago area sleep study. Sleep Medicine, 18, 50–55. 10.1016/j.sleep.2015.07.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carney CE, & Manber R (2009). Quiet your mind and get to sleep: Solutions to insomnia for those with depression, anxiety, or chronic pain. New Harbinger Publications. [Google Scholar]
- Chen X, Wang RL, Zee P, Lutsey PL, Javaheri S, Alcántara C, Jackson CL, Williams MA, & Redline S (2015). Racial/ethnic differences in sleep disturbances: The multi-ethnic study of atherosclerosis (MESA). Sleep, 38, 877–888. 10.5665/sleep.4732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng P, Cuellar R, Johnson DA, Kalmbach DA, Joseph CLM, Cuamatzi Castelan A, Sagong C, Casement MD, & Drake CL (2020). Racial discrimination as a mediator of racial disparities in insomnia disorder. Sleep Health, 6, 543–549. 10.1016/j.sleh.2020.07.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed.). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Cole DA, & Maxwell SE (2003). Testing mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology, 112, 558–577. [DOI] [PubMed] [Google Scholar]
- Ellis JG, Deary V, & Troxel WM (2015). The role of perceived partner Alliance on the efficacy of CBT-I: Preliminary findings from the partner Alliance in insomnia research study (PAIRS). Behavioral Sleep Medicine, 13, 64–72. 10.1080/15402002.2013.838768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis JG, Perlis ML, Espie CA, Grandner MA, Bastien CH, Barclay NL, Altena E, & Gardani M (2021). The natural history of insomnia: Predisposing, precipitating, coping, and perpetuating factors over the early developmental course of insomnia. Sleep, 44, 1–10. 10.1093/sleep/zsab095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faestel PM, Littell CT, Vitiello MV, Forsberg CW, & Littman AJ (2013). Perceived insufficient rest or sleep among veterans: Behavioral risk factor surveillance system 2009. Journal of Clinical Sleep Medicine, 9, 577–584. 10.5664/jcsm.2754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fillo J, Holliday SB, DeSantis A, Germain A, Buysse DJ, Matthews KA, & Troxel WM (2017). Observed relationship behaviors and sleep in military veterans and their partners. Annals of Behavioral Medicine, 51, 879–889. 10.1007/s12160-017-9911-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ford ES, Cunningham TJ, Giles WH, & Croft JB (2015). Trends in insomnia and excessive daytime sleepiness among US adults from 2002 to 2012. Sleep Medicine, 16, 372–378. 10.1016/j.sleep.2014.12.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Funk JL, & Rogge RD (2007). Testing the ruler with item response theroy: Increasing precision of measurement for relationship satisfaction with the couples satisfaction index. Journal of Family Psychology, 21, 572–583. 10.1037/0893-3200.21.4.572 [DOI] [PubMed] [Google Scholar]
- Gaston SA, McWhorter KL, Parks CG, D’Aloisio AA, RojoWissar DM, Sandler DP, & Jackson CL (2021). Racial/ethnic disparities in the relationship between traumatic childhood experiences and suboptimal sleep dimensions among adult women: Findings from the sister study. International Journal of Behavioral Medicine, 28, 116–129. 10.1007/s12529-020-09905-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzales KL, Noonan C, Goins RT, Henderson WG, Beals J, Manson SM, Acton KJ, & Roubideaux Y (2016). Assessing the everyday discrimination scale among American Indians and Alaska natives. Psychological Assessment, 28, 51–58. 10.1037/a0039337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grandner MA, Patel NP, Gehrman PR, Xie D, Sha D, Weaver T, & Gooneratne N (2010). Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Medicine, 11, 470–478. 10.1016/j.sleep.2009.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin M, Martino RJ, LoSchiavo C, Comer-Carruthers C, Krause KD, Stults CB, & Halkitis PN (2021). Ensuring survey research data integrity in the era of internet boys. Quality & Quantity, 56, 2841–2852. 10.1007/s11135-021-01252-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harvey A, Bélanger L, Talbot L, Eidelman P, Beaulieu-Bonneau S, Fortier-Brochu E, Ivers H, Lamy M, Hein K, Soehner AM, Mérette C, & Morin CM (2014). Comparative efficacy of behavior therapy, cognitive therapy, and cognitive behavior therapy for chronic insomnia: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 82(4), 670–683. 10.1037/a0036606.supp [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang CY, & Tsai W (2023). Asian American parents’ experiences of stress, discrimination, and mental health during COVID19. Families Systems Health, 41, 68–77. 10.1037/fsh0000715 [DOI] [PubMed] [Google Scholar]
- Jernelöv S, Lekander M, Blom K, Rydh S, Ljotsson B, Axelsson J, & Kaldo V (2012). Efficacy of a behavioral self-help treatment with or without therapist guidance for comorbid and primary insomnia-a randomized controlled trial. BMC Psychiatry, 12, 5. 10.1186/1471-244X-12-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufmann CN, Mojtabai R, Hock RS, Thorpe RJ Jr., Canham SL, Chen LY, Wennberg AMV, Chen-Edinboro LP, & Spira AP (2016). Racial/ethnic differences in insomnia trajectories among U.S. older adults. American Journal of Geriatric Psychiatry, 24, 575–584. 10.1016/j.jagp.2016.02.049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khaylis A, Polusny MA, Erbes CR, Gewirtz A, & Rath M (2011). Posttraumatic stress, family adjustment, and treatment preferences among National Guard soldiers deployed to OEF/OIF. Military Medicine, 176, 126–131. [DOI] [PubMed] [Google Scholar]
- Krieger N, Smith K, Naishadham D, Hartman C, & Barbeau EM (2005). Experiences of discrimination: Validity and reliability of a selfreport measure for population health research on racism and health. Social Science & Medicine, 61, 1576–1596. 10.1016/j.socscimed.2005.03.006 [DOI] [PubMed] [Google Scholar]
- Kuhn E, Miller KE, Puran D, Wielgosz J, YorkWilliams S, Owen JE, Jaworski BK, Hallenbeck HW, McCaslin S, & Taylor KL (2021). A pilot randomized controlled trial of the insomnia coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behavior Therapy, 53, 440–457. 10.1016/j.beth.2021.11.003 [DOI] [PubMed] [Google Scholar]
- Lee AA, & Gabriele JM (2018). Racial differences in the associations of posttraumatic stress and insomnia with body mass index among trauma-exposed veterans. Behavioral Medicine, 44, 263–270. 10.1080/08964289.2017.1292998 [DOI] [PubMed] [Google Scholar]
- Loo CM, Fairbank JA, & Chemtob CM (2005). Adverse race-related events as a risk factor for posttraumatic stress disorder in Asian American Vietnam veterans. The Journal of Nervous and Mental Disease, 193, 455–463. 10.1097/01.nmd.0000168239.51714.e6 [DOI] [PubMed] [Google Scholar]
- Loo CM, Fairbank JA, Scurfield RM, Ruch LO, King DW, Adams LJ, & Chemtob CM (2001). Measuring exposure to racism: Development and validation of a race-related stressor scale (RRSS) for Asian American Vietnam veterans. Psychological Assessment, 13, 503–520. [PubMed] [Google Scholar]
- Macneil CA, Hasty MK, Conus P, & Berk M (2012). Is diagnosis enough to guide interventions in mental health? Using case formulation in clinical practice. BMC Medicine, 10, 1–3. 10.1186/1741-7015-10-111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maguen S, Gloria R, Huggins J, Goldstein LA, Kanady JC, Straus LD, Metzler TJ, Lujan C, & Neylan TC (2021). Brief behavioral treatment for insomnia improves psychosocial functioning in veterans: Results from a randomized controlled trial. Sleep, 12, 1–15. 10.1093/sleep/zsaa205 [DOI] [PubMed] [Google Scholar]
- Marshall GN, Schell TL, & Miles JNV (2009). Ethnic differences in posttraumatic distress: Hispanics’ symptoms differ in kind and degree. Journal of Consulting & Clinical Psychology, 77, 1169–1178. 10.1037/a0017721 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer JF, Faust KA, Faust D, Baker AM, & Cook NE (2013). Careless and random responding on clinical and research measures in the addictions: A concerning problem and investigation of their detection. International Journal of Mental Health and Addiction, 11, 292–306. 10.1007/s11469-012-9410-5 [DOI] [Google Scholar]
- Miller KE, Kuhn E, Owen JE, Taylor K, Yu JS, Weiss BJ, Crowley JJ, & Trockel M (2019). Clinician perceptions related to use of the CBT-I coach mobile app. Behavioral Sleep Medicine, 17, 481–491. 10.1080/15402002.2017.1403326 [DOI] [PubMed] [Google Scholar]
- Miller MB, Flores LY, Dorimé-Williams ML, Williams MS, Martinez LD, Freeman LK, Everson AT, Hall NA, Monk JK, McCrae C, & Borsari B (2022). Motives for and barriers to research participation among racially and ethnically diverse veterans. Military Medicine, 127, e1540–e1546. 10.1093/milmed/usac127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller MB, Monk JK, Flores LY, Everson AT, Martinez LD, Massey K, Blanke EM, Dorimé-Williams ML, Williams MS, McCrae C, & Borsari B (2022). Impact of discrimination and coping on Veterans’ willingness to seek treatment for physical and mental health problems. Psychology of Addictive Behaviors, 37, 209–221. 10.1037/adb0000861 [DOI] [PubMed] [Google Scholar]
- Monk JK, Ruhlmann LM, Nelson Goff BS, & Ogosky BG (2018). Brief systemic programs for promoting mental health and relationship functioning in military couples and families. Journal of Family Therapy Review, 10, 566–586. [Google Scholar]
- Morin CM, Belleville G, Belanger L, & Ivers H (2011). The insomnia severity index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep, 34, 601–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mysliwiec V, Martin JL, Ulmer CS, Chowdhuri S, Brock MS, Spevak C, & Sall J (2020). The management of chronic insomnia disorder and obstructive sleep apnea: Synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense clinical practice guidelines. Annals of Internal Medicine, 172, 325–336. 10.7326/M19-3575 [DOI] [PubMed] [Google Scholar]
- Mysliwiec V, McGraw L, Pierce R, Smith P, Trapp B, & Roth BJ (2013). Sleep disorders and associated medical comorbidities in active duty military personnel. Sleep, 36, 167–174. 10.5665/sleep.2364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohayon MM (2011). Epidemiological overview of sleep disorders in the general population. Sleep Medicine Research, 2, 1–9. [Google Scholar]
- Petrov ME, & Lichstein KL (2016). Differences in sleep between black and white adults: An update and future directions. Sleep Medicine, 18, 74–81. 10.1016/j.sleep.2015.01.011 [DOI] [PubMed] [Google Scholar]
- Price M, Szafranski DD, van Stolk-Cooke K, & Gros DF (2016). Investigation of abbreviated 4 and 8 item versions of the PTSD checklist 5. Psychiatry Research, 239, 124–130. 10.1016/j.psychres.2016.03.014 [DOI] [PubMed] [Google Scholar]
- Pruiksma KE, Fina B, Dietch JR, Dondanville KA, Williams J, Wright EC, Molino A, Hall-Clark B, Nicholson KL, Peterson AL, & Taylor DJ (2018). Special considerations in the adaptation of cognitive behavioral therapy for insomnia with activeduty U.S. army personnel. Cognitive and Behavioral Practice, 25, 515–530. [Google Scholar]
- Ritterband LM, Thorndike FP, Ingersoll KS, Lord HR, Gonder-Frederick L, Frederick C, Quigg MS, Cohn WF, & Morin CM (2017). Effect of a web-based cognitive behavior therapy for insomnia intervention with 1-year follow-up: A randomized clinical trial. JAMA Psychiatry, 74(1), 68–75. 10.1001/jamapsychiatry.2016.3249 [DOI] [PubMed] [Google Scholar]
- Rosen RC, Cikesh B, Fang S, Trachtenberg FL, Seal KH, Magnavita AM, Bovin MJ, Green JD, Bliwise DL, Marx BP, & Keane TM (2019). Posttraumatic stress disorder severity and insomnia-related sleep disturbances: Longitudinal associations in a large, gender-balanced cohort of combat-exposed veterans. Journal of Traumatic Stress, 32, 936–945. 10.1002/jts.22462 [DOI] [PubMed] [Google Scholar]
- Samuel IBH, Breneman CB, Chun T, Hamedi A, Murphy R, & Barrett JP (2022). Compounding effects of traumatic brain injury, military status, and other factors on Pittsburgh sleep quality index: A meta-analysis. Military Medicine., 187, 589–597. 10.1093/milmed/usab377 [DOI] [PubMed] [Google Scholar]
- Shariff-Marco S, Breen N, Landrine H, Reeve BB, Krieger N, Gee GC, Williams DR, Mays VM, Ponce NA, Alegría M, Liu B, Willis G, & Johnson TP (2011). Measuring everyday racial/ethnic discrimination in health surveys. Du Bois Review, 8, 159–177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shim RS (2021). Dismantling structural racism in psychiatry: A path to mental health equity. American Journal of Psychiatry, 178, 592–598. 10.1176/appi.ajp.2021.21060558 [DOI] [PubMed] [Google Scholar]
- Slopen N, Shonkoff JP, Albert MA, Yoshikawa H, Jacobs A, Stoltz R, & Williams DR (2015). Racial disparities in child adversity in the U.S: Interactions with family immigration history and income. American Journal of Preventive Medicine, 50, 47–56. 10.1016/j.amepre.2015.06.013 [DOI] [PubMed] [Google Scholar]
- Spielman AJ, Caruso LS, & Glovinsky PB (1987). A behavioral perspective on insomnia treatment. Psychiatric Clinics of North America, 10(4), 541–553. [PubMed] [Google Scholar]
- Troxel WM, Robles TF, Hall M, & Buysse DJ (2022). Marital quality and the marital bed: Examining the covariation between relationship quality and sleep. Sleep Medicine Reviews, 11, 389–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner CH, Appenzeller GN, Mullen K, Warner CM, & Grieger T (2008). Soldier attitudes toward mental health screening and seeking care upon return from combat. Military Medicine, 173, 563–569. [DOI] [PubMed] [Google Scholar]
- Williams DR (1999). Race, socioeconomic status, and health: The added effects of racism and discrimination. Annals of the New York Academy of Sciences, 896, 173–188. 10.1111/j.1749-6632.1999.tb08114.x [DOI] [PubMed] [Google Scholar]
- Williams DR (2018). Stress and the mental health of populations of color: Advancing our understanding of race-related stressors. Journal of Health and Social Behavior, 59, 466–485. 10.1177/0022146518814251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Yu Y, Jackson JS, & Anderson NB (1997). Racial differences in physical and mental health: Socioeconomic status, stress, and discrimination. Journal of Health Psychology, 2, 335–351. [DOI] [PubMed] [Google Scholar]
- Xie M, Yip T, Cham H, & El-Sheikh M (2021). The impact of daily discrimination on sleep/wake problem trajectories among diverse adolescents. Child Development, 92, 1061–1074. 10.1111/cdev.13605 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.