

Abstract
Purpose of Review:
The purpose of this review is to examine recent literature (2012–2022) on alcohol treatment access and engagement in women in the U.S. and propose future directions for research and clinical practice.
Recent Findings:
A targeted literature review resulted in 27 studies encompassing screening and brief intervention (SBIRT), treatment utilization, treatment engagement, and barriers to treatment. Recent literature demonstrates overall low rates of screening and brief interventions and treatment utilization in the population with women less likely to be screened and utilize alcohol treatment. The magnitude of these gender differences varies with race/ethnicity. Extensive barriers to care include provider knowledge, structural barriers, and attitudinal barriers and these vary with service setting, gender, and race/ethnicity.
Summary:
There is an increasing prevalence of alcohol use and Alcohol Use Disorder (AUD) in women with low rates of screening, brief treatment, treatment, and engagement which have resulted from extensive barriers to care. Possible areas of further inquiry include the impact of race/ethnicity on gender differences, improving provider and system level policies to promote SBIRT and treatment engagement and utilization, further developing digital interventions, and implementation research to investigate factors associated with optimizing effectiveness of gender-responsive and culturally tailored interventions that address the unique needs of women.
Keywords: women, alcohol, alcohol use disorders, gender, gender differences, treatment, drinking
INTRODUCTION
In the United States, the gender gap in the prevalence of alcohol use disorder (AUD) has decreased significantly over the past 35 years. The male to female ratio of AUD in individuals 18 years and older narrowed from 5:1 in the late 1980s 1 to approximately 1.4:1 in 2018, including an estimated 7.3% of men and 5.2% of women 2. Recent data from the National Survey on Drug Use and Health (NSDUH) between 2015–2019 also demonstrate that the magnitude of this male to female ratio of AUD also varies by race and ethnicity 3. During this time frame, the male to female gender prevalence ratios ranged from 1.5:1 – 2.4:1 with the narrowest gender gap among those identifying with 2 or more races (1.5:1) and the widest gap among those identifying as Hispanic/Latino (2.4:1) 3 For those identifying with other races and ethnicities, the gender prevalence ranged between approximately 1.6:1 for individuals identifying as American Indian/Alaskan Native, Hawaiian/Pacific Islander, and Asian; 1.7:1 as White; and 1.9:1 as Black/African American 3. According to the National Epidemiologic Survey on Alcohol and Related Disorders (NESARC), in the United States (U.S.) between 2001–2002 and 2012–2013, there was a 16% increase in the proportion of women who drank alcohol, a 58% increase in women who reported heavy drinking (versus 16% in men), and an 84 % increase in the past-year prevalence of an AUD in women (versus 35% in men) 4. In 2020, 9% of women over age 18 and 17% of women aged 18 to 25 years were reported to have an AUD 5. While alcohol consumption, AUD rates, and related health consequences increased in women and girls in the decades preceding the COVID-19 pandemic, it is additionally concerning that in 2020, women who self-reported greater pandemic-related stress also reported greater alcohol consumption compared with women with lower self-reported pandemic stress 6.
Rising rates of alcohol use, heavy drinking, and AUD pose significant health risks for women and girls 7. Risks for females can occur at lower levels of consumption than for males, including long-term cardiovascular risks, increased risk of breast and other cancers, liver disease including cirrhosis, and dementia, among other adverse health consequences 7. Despite the prevalence and associated health risks, in 2018 only about 7.9% of individuals with AUD had any treatment in the prior year – approximately 7.7% of women and 8.0% of men reported receiving treatment in 2017 8. This is in spite of the widely documented effectiveness of existing behavioral and pharmacologic treatments available for men and women 9. Given the increasing prevalence of alcohol use and AUD in women, existing evidence-based effective treatment for AUD, and the low rates of treatment utilization, we conducted a targeted review of recent literature on women’s access to and engagement in alcohol treatment in the U.S. Our review focused on screening and brief intervention, treatment utilization, engagement in treatment, and treatment barriers.
METHODS
PubMed and PsycINFO databases were used to identify articles related to women’s access to and engagement in treatment and barriers to care for alcohol problems and AUD in the U.S. To examine the most recent literature, we restricted our search to articles published between December 2012 and December 2022. We defined engagement and access to treatment as studies that examined receipt of treatment services, referral to treatment, engagement and adherence to treatment, barriers to treatment, and treatment-seeking beliefs or behaviors. We defined treatment as any intervention for alcohol-related problems, including screening, brief intervention, and referral to treatment (SBIRT), behavioral therapies, medication treatment, and formal peer- or family-based interventions. Combinations of the search terms used to identify relevant articles are listed below (Table 1). Additional studies were found by examining references in relevant articles identified by the search.
Table 1.
Literature Review Search Terms
| Main topic | Search terms |
|---|---|
| AUD | “Alcoholism” OR “Alcohol Dependence” OR “Alcohol Addiction” OR “Chronic Alcoholic Intoxication” OR “Alcohol Abuse” OR “Ethanol Abuse” OR “Alcohol Use Disorder*” OR “Alcohol-Related Disorder*” OR “Alcohol Problem*” |
| Treatment | “Therapeutics” OR “Treatment” OR “Therapy” OR “Pharmacotherapy” OR “Medication” OR “Counseling” |
| Access/Engagement | “Health Services Accessibility” OR “Access” OR “Accessibility” OR “Engagement” |
| Women | “Women” OR “Female” |
Articles were excluded if (1) study participants were under 18 years of age, (2) the article did not include data or results specific to women (studies with mixed gender samples were only included if the authors reported gender-specific analyses related to treatment engagement and access), (3) the article was a review, meta-analysis, case study, or case series, (4) the article was not published in English, or (5) the study was not conducted in the US. If a study examined a mix of alcohol and other drug treatment, results specific to alcohol needed to be reported for inclusion. Quantitative and qualitative research studies were eligible for inclusion. Figure 1 presents the PRISMA flow diagram of studies identified using our search strategy. In total, 27 studies were included.
Fig. 1.
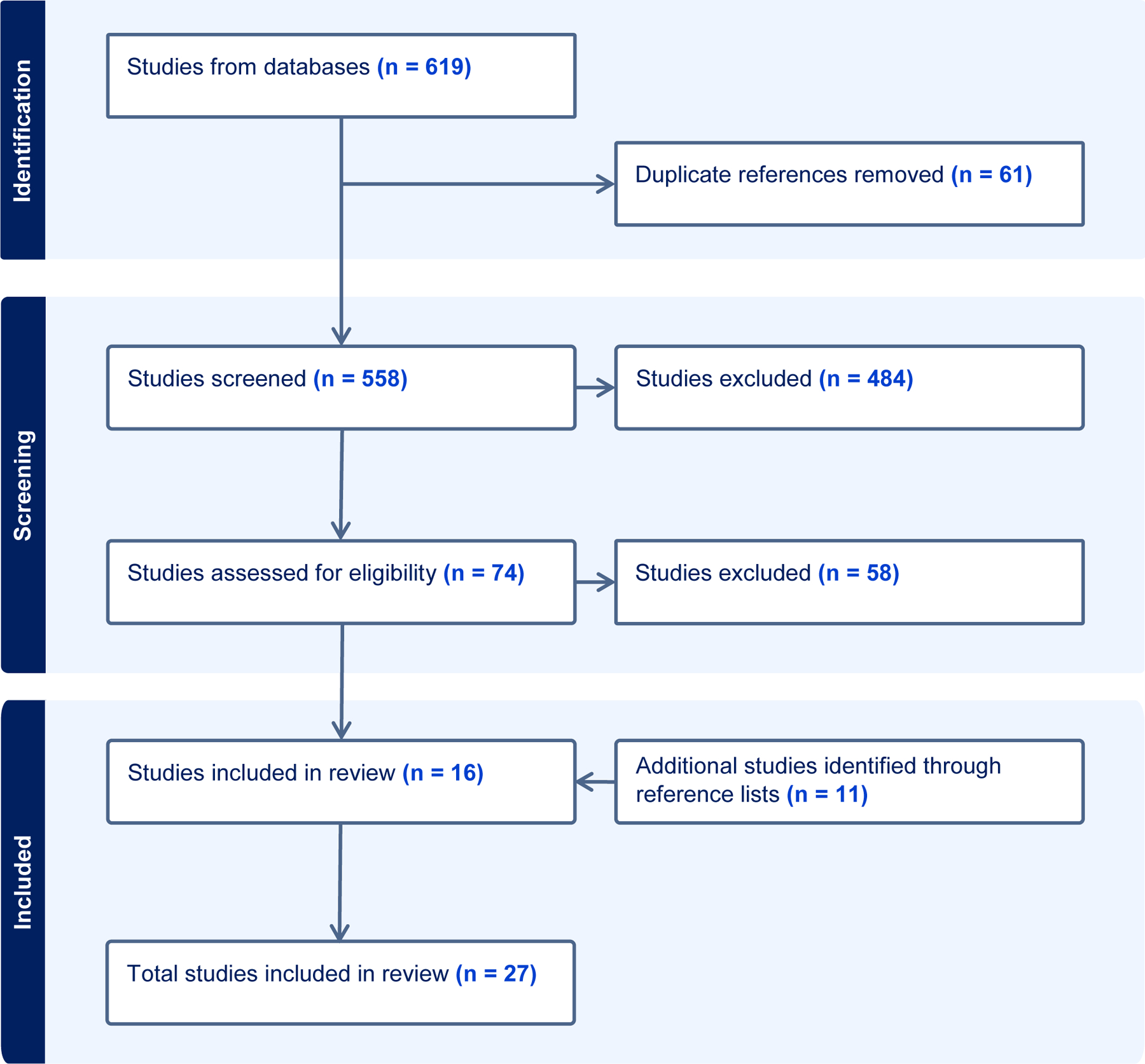
PRISMA flow chart for article selection
In this review, we utilize the Office of Research on Women’s Health definitions of sex and gender 10 with sex defined as a “multidimensional biological construct based on anatomy, physiology, genetics and hormones,” and gender “as a multidimensional construct that encompasses gender identity and expression, as well as social and cultural expectations about status, characteristics and behavior associated with certain sex traits.” We also recognize that “a person’s gender identity (e.g., woman, man, trans man, gender-diverse, nonbinary) is self-identified, may change through their life, and may or may not correspond to a society’s cultural expectations based on their biological sex traits.” 10.However, in summarizing the data reported in each study included in this review, we have utilized the terminology “sex” or “gender” as reported by each study’s data collection and results.
Screening, Brief Intervention, and Referral to Treatment
Universal screening, brief intervention, and referral to treatment (SBIRT) is an evidence-based public health approach aimed at identifying and addressing harmful and hazardous alcohol use 11. Recent recommendations from the United States Preventive Services Task Force (USPSTF) advise screening all adults 18 years or older (including pregnant women) for unhealthy alcohol use in primary care settings 12. These recommendations are based on the USPSTF’s review of the evidence concluding that the use of brief interventions for individuals who screen positive for risky or hazardous drinking is associated with reductions in unhealthy alcohol use 13. We identified five studies that examined receipt of SBIRT and reported analyses by gender 14–16 or utilized women-only samples 17,18.
Analyses of the National Ambulatory Medical Care Survey data from 2014–2016 revealed that overall documented alcohol screening rates were low (documented in 2.6% of 19,213 visits) and patients’ sex was not associated with receipt of screening for unhealthy alcohol use 14. Screening in this study was measured via documentation in the medical record, which may have contributed to the low rates.
In contrast, data compiled from results of the annual NSDUH survey between 2015 and 2019, showed that 76.1% of individuals without an AUD and 87.2% of those with any AUD reported having been screened for alcohol problems in the past year 19. Further examination of the NSDUH data for this same period (2015–2019) revealed gender differences in receipt of screening for older adults (age 65 and older) 15. Results showed that older women who used alcohol in the past year were more likely to report alcohol screening only (i.e., without brief intervention) compared to no alcohol screening. However, older women were less likely to report discussing alcohol with their provider compared to older men (41.9% vs. 50.9%). For those who reported discussing alcohol with their provider, older women had lower rates than older men of being asked about drinking problems (6.8% vs 9.8%), lower likelihood of being advised to reduce alcohol use (3.4% vs. 6.8%), and they were less likely to be given information about alcohol treatment (0.7% vs. 2.0%).
Researchers at the CDC analyzed data from the Behavioral Risk Factor Surveillance System (an annual telephone survey of noninstitutionalized US adults in 23 states and the District of Columbia regarding health-related risk behaviors, chronic health conditions, and use of preventive services) between 2017–2019 to examine receipt of SBIRT for pregnant persons (n=950) and reproductive-aged women (n=28,476) 18. Overall, screening from a healthcare provider for alcohol use was not significantly different among pregnant persons (80%) compared with reproductive-aged women (86%). However, there were significant differences in screening based on patient characteristics. Pregnant persons who did not graduate from high school had lower rates of screening (53.5%) compared to those who did graduate from high school (83.4%) or had some college education (84.5%). For pregnant persons who reported receiving alcohol screening, few (25.3%) reported receiving advice about what level of drinking is harmful, and even fewer (12.3%) reported being advised to reduce or stop drinking.
Examination of data from the Veterans Health Administration (VHA) found that positive alcohol screens post-deployment were associated with linkage to VHA treatment services for men, but not for women 16. Specifically, women with positive alcohol screening scores (≥ 5 on the Alcohol Use Disorder Identification Test - AUDIT-C) were not more likely than women with negative alcohol screening scores to link to VHA services.
In addition to primary care, women’s health clinics are important settings for implementing SBIRT. These settings serve a large volume of women, allowing providers the added benefit of using SBIRT to identify and address risk of alcohol-exposed pregnancy (AEP) 11. Hettema and colleagues 17 examined receipt of SBIRT services in a sample of 199 women receiving women’s health services in public clinics in Virginia between July – October 2012. Although 83% of women in the study reported being asked by their medical provider if they drank alcohol, only 18% of risky drinkers reported being advised to reduce or stop alcohol use. Of participants at risk for AEP, only 50% reported that their provider had discussed risk factors for AEP with them. Of note, 81% of women sampled said they would find it acceptable to be asked about their drinking and the majority expressed favorable attitudes about potentially receiving SBIRT as part of women’s health services.
Taken together, these studies indicate variable rates of screening for women, with reported rates likely influenced by data collection methods (e.g., medical records review, participant surveys) and population (Veterans, women’s clinics, population-based surveys). Once screened, women across most subpopulations appear to have consistently low rates of brief intervention.
Accessing Treatment Services for AUD
Treatment for AUD is delivered in multiple service settings and levels of care 20. In our review of the literature, we found eight studies examining receipt of treatment, all of which utilized mixed-gender samples. 21–28. All studies utilized national population survey data in the U.S. to characterize the odds of treatment receipt among people with AUD. For example, Chartier et al. 22 compared data from two population-based surveys, the 1991–1992 National Longitudinal Alcohol Epidemiologic Survey (NLAES) and the 2001–2002 NESARC. A multivariate analysis of treatment utilization demonstrated that age, alcohol severity, and major depression were correlates of alcohol treatment utilization, but in this model, gender was not significantly associated with AUD treatment receipt in either survey 22.
An analysis of NSDUH data from the 2015–2018 survey years also did not find evidence for a gender difference in treatment receipt 27 but was notably low for women and men. Martin et al. 27 examined past-year treatment receipt among anyone either meeting criteria for a substance use disorder (SUD) or reporting a need for SUD treatment. Bivariate analyses of gender differences in receipt of treatment did not yield any statistically significant gender differences in AUD treatment receipt (7.5% of women and 8.9% of men with AUD received treatment).
In contrast, other studies using NESARC and NSDUH data found gender differences characterized by higher odds of treatment receipt in men than women 21,24–26. A cross-sectional analysis of data collected in the NESARC for 2004–2005 found that among people with AUD, treatment receipt was more common in men than women 25. Women were about half as likely to receive any alcohol treatment and the magnitude of this difference was even more pronounced for accessing specialty services, with men more than twice as likely as women to receive these services. Women were also about 40% less likely than men to utilize 12-step groups 25. This is similar to a longitudinal analysis of NESARC data (using 2001–2002 and 2004–2005 data) that found that men had higher odds of receiving specialty care (but not other types of care) for AUD than women 23. Similarly, Zemore et al. 28 utilized pooled data from the 2000, 2005, and 2010 National Alcohol Surveys and found that lifetime utilization of any alcohol treatment services, specialty alcohol treatment, and Alcoholics Anonymous (AA) was significantly lower for women than men for each treatment type (e.g., 11.1% vs. 16.3% for any services; 6.0% vs. 9.8% for specialty treatment; and 8.7% vs. 10.8% for AA) 28. Alvanzo et al. 21 also utilized data from the NESARC (2001–2002) and found that among adults ages 18–44 with lifetime AUD, women were less likely than men to receive alcohol treatment services in their lifetime and women who did receive treatment were younger at the time of first AUD treatment utilization than men.
When taken together, the majority of the studies reviewed demonstrated evidence for a higher rate of lifetime and past-year AUD treatment receipt in men than women 21,24–26,28, while two found low utilization but no gender difference 22,27. This variance as well as the magnitude of gender difference in receipt of treatment varied depending on the specific epidemiologic survey as well as demographic and clinical characteristics included in statistical models. Studies consistently indicate that the odds of past-year treatment receipt among both men and women with AUD is quite low, with estimates often of 20% or less of this population receiving AUD treatment in any given year 22,25.
Utilization of Medications for Alcohol Use Disorder
While most studies focused on gender differences in alcohol treatment receipt overall, four studies investigated receipt of medication for AUD 29–32. Three medications are approved by the U.S. Food and Drug Administration for treatment of AUD: acamprosate, naltrexone, and disulfiram. Several more medications, including topiramate, are used “off label” for AUD treatment 33. Our review identified three studies that examined AUD medication utilization overall 30–32, and one that examined topiramate specifically 29. Three of these studies conducted analyses by gender 29–31 and one analyzed data from a women-only sample 32.
An examination of electronic medical records from the Community Health Applied Research Network, a national network of 17 community health centers, during the period 2006–2013 (n=572,582), demonstrated very low rates of AUD medication prescriptions (3.2%) among those identified with an AUD. There were no significant gender differences 31.
A retrospective cohort study using VHA data (2009–2012; n=375,777) examined topiramate for AUD and found that while rates of utilization were low overall prescriptions for topiramate increased from approximately 1% to 2% over this period 29. Among the small group given medication, women were more than twice as likely than men to receive topiramate for AUD (OR = 2.5, 95% CI 2.31–2.71) 29.
Additional data from a VHA cohort study of justice-involved women (n=1,535) and men (n=30,478) suggests that justice-involved women with AUD were more likely to receive any form of pharmacotherapy than their male counterparts 30. For this group, 22% of women and 10% of men with a chart diagnosis of AUD received AUD pharmacotherapy (OR = 2.24; 95% CI, 1.82–2.74). These data in combination with Del Re et al. 29 provide evidence that among those being treated at the VHA, women are more likely to receive pharmacotherapy for AUD then men.
Another study focusing on justice-involved women, utilized women’s VHA data from 2014–2017. Taylor et al. 32 found that during the study period, there was a statistically significant increase in pharmacotherapy receipt among all women veterans, from 14% in 2014 to 21% in 2017 (p<.0001). For justice-involved women veterans, there was a significant increase in receipt of pharmacotherapy from 20% in 2014 to 31% in 2017 (p<.0001). Additionally, justice-involved women (OR=1.29, 95% CI 1.15–1.45) and homeless women (OR = 1.35, 95% CI 1.25–1.47) were more likely to receive medication. Those who were 55 or older (OR = 0.74, 95% CI 0.67–0.82) or who were African American (OR = 0.73, 95% Cl 0.68–0.79) had lower odds of receiving pharmacotherapy 32.
These studies show overall low AUD medication treatment utilization but yielded mixed results with respect to significant gender differences 29–31. Additional research on patient, provider, and health systems barriers to medication treatment for both men and women is warranted with the aim of improving AUD medication utilization across genders.
Engagement and Retention in Treatment
Several studies have investigated whether treatment tailored to the needs of women, (referred to in various studies as female-specific treatment 34 may improve alcohol treatment outcomes overall, as well as improve retention and engagement in treatment for women with AUD 34,35. This review identified three studies that examined engagement and retention in female-specific AUD treatment utilizing all-female samples 34–36, and one study examining women’s engagement in conjoint (couples) treatment and mixed conjoint and individual treatment 37.
In a randomized control trial (RCT) of 99 women with AUD, Epstein and colleagues 34 demonstrated that women in a female-specific individual cognitive behavioral therapy (FS-CBT) intervention had a statistically significant increase in abstainers in their social networks in the year following treatment compared to women in gender-neutral CBT (GN-CBT) 34. However, they found no significant differences between treatment conditions in engagement indices (number of sessions completed, therapeutic alliance, client satisfaction, or percentage of assigned homework completed).
In a subsequent study, the FS-CBT intervention was adapted to a group therapy format (G-FS-CBT) 35 and women (N =155) were randomly assigned to the group therapy format (G-FS-CBT) or to the individual FS-CBT format (I-FS-CBT). The study found that G-FS-CBT had a higher initial dropout rate (operationalized by participants who did not attend at least 1 treatment session), and participants in the G-FS-CBT attended significantly fewer sessions compared to those in the I-FS-CBT.
In an earlier study, McCrady et al. 38 found that Alcohol Behavioral Couples Therapy (ABCT) (an efficacious couples’ treatment for heterosexual women with AUD and their male partners) resulted in significantly greater improvements in treatment outcomes compared to individual therapy for women with AUD. However, women in this study reported preferring individual therapy over ABCT 38. McCrady et al. 37 then conducted an RCT comparing ABCT alone to Blended-ABCT (a blend of individual CBT and ABCT) in heterosexual women (N=59) and their male partners. Treatment engagement outcomes (operationalized by women’s treatment attendance, homework completion, and utilization of other treatment services) did not differ significantly between conditions.
In a study assessing treatment engagement in female survivors of intimate partner violence in treatment for posttraumatic stress disorder (PTSD) and AUD, Myers and colleagues 36 examined demographic differences between participants who engaged in treatment (operationalized as attending 25% or more treatment sessions) and those who dropped out. Results showed that women who engaged in treatment were significantly older and had fewer dependents compared to those who dropped out. Of those who engaged in treatment, only 3 of 18 (16.7%) had a dependent (each reporting 1 dependent), whereas 9 of 22 (40.9%) participants who dropped out of treatment had dependents (range: 1–7 dependents). Additionally, greater engagement in treatment was significantly associated with more years of heavy drinking and greater avoidance/numbing PTSD symptoms. Results indicated that having dependents may be a barrier to engagement in treatment in this population. Additionally, it is notable that participants with more severe PTSD and AUD had overall significantly greater engagement in treatment.
Gender-specific interventions for AUD and associated conditions is an emerging area of study. Additional implementation research on the potential for gender-specific interventions to improve access, utilization, and engagement in alcohol treatment, as well as improve a wide range of clinical and functional outcomes is warranted.
Barriers to Treatment
Given the low prevalence of treatment among women with AUD, it is clear there are substantive barriers to accessing and engaging in treatment. In our review of the literature, seven studies examined barriers to treatment, three studies in mixed-gender samples 25,39,40, and four studies conducted in the VHA focused only on women 41–44.
Analysis of data from the 2001–2002 and 2003–2004 NESARC found no significant gender differences in perceived need for alcohol treatment services (4.8% in women vs 4.6% in men, p=0.87) and women endorsed similar numbers and types of barriers as men 25. However, women were twice as likely than men to believe the problem would get better by itself (47% vs 24%, p<0.001). This was the most frequent reason women endorsed for not seeking help. Women were also more likely than men to report that they stopped drinking on their own as a reason not to seek help (23% vs 9%, p<0.002). Furthermore, after controlling for alcohol symptom count, the study demonstrated that women were 3 times likelier than men to think their drinking problem would get better on its own and that they would stop drinking on their own 25.
Verissimo et al. 40 utilized NESARC data (2001–2002) to investigate gender differences in AUD barriers to treatment by racial/ethnic subgroups. This analysis examined structural barriers (e.g., insurance, time, finances), attitudinal barriers (e.g., embarrassed, ashamed), and readiness for change barriers (e.g., stopped on own, not ready to get help). Women were more likely to endorse attitudinal barriers than men and there were no gender differences in structural barriers and readiness to change barriers. When analyzing the data by gender and race/ethnicity a more complex picture emerged. Structural barriers were more likely to be endorsed by people who identified as Latina/Latino than White or African American, with greater likelihood of having structural barriers cited by Latino men than Latina women. For White, African American, and Latina women, attitudinal barriers were more likely to be endorsed compared to men across all three racial/ethnic groups. This study emphasized that financial and structural barriers were among the most cited by both men and women 40. The study also suggests that gender differences in attitudes about women’s alcohol use continue to be barriers for women who are more likely to minimize alcohol problems as a reason not to seek treatment.
Qualitative data from the VHA identified several provider- and clinic-level barriers to connecting women Veterans to alcohol related care. This study used semi-structured interviews of 14 VHA primary care providers in two clinics in Northern California 41. The interviews revealed provider-level and structural barriers to care which included insufficient available resources (e.g., shortage of providers with alcohol-related treatment experience, lack of gender-matched treatment and group therapy, and lack of educational materials), provider decision to prioritize other health needs, insufficient knowledge of care options and/or referral process among providers, time constraints during clinical visits, and the referral process itself. They also identified specific facilitators to alcohol treatment at the VHA such as available resources, provider behavior, and VHA directives. This review focused on women only and, therefore, did not assess gender differences in these barriers.
To understand receptivity to receiving alcohol treatment and disclosing of alcohol use to primary care providers (PCPs) among women veterans with alcohol misuse, qualitative interviews were conducted with 30 women veterans at two VHA facilities between 2012 and 2013 43,44. They found women’s receptivity to alcohol-related care was associated with self-appraisal of severity of alcohol use, availability of gender-specific services, the provider’s presentation of treatment options, and having more severe mental and physical health problems 44. Furthermore, women reported greater willingness to disclose their drinking behavior to a PCP depending on their perception of the PCP’s encouragement of their disclosure and their perceived positive relationship with the PCP 43. Women’s concerns about being labeled as ‘alcoholic’ or having negative self-judgments such as feeling ashamed or embarrassed discouraged disclosure, whereas having health concerns about drinking or other negative consequences of alcohol use such as legal or work-related problems were associated with greater likelihood of disclosing drinking problems to a PCP 43.
Another study conducted focus groups to gather feedback on the feasibility and acceptability of a telephone-delivered shared decision-making protocol for women Veterans with unhealthy drinking, comorbid depression, and/or probable PTSD (N=19) 42. Analyses of these data indicated that the telephone intervention protocol was overall feasible and acceptable. However, a small number of participants identified some potential barriers including the treatment delivery modality (i.e., phone), length of telephone sessions, and the readability of the document used to present treatment options. Of note, this study was conducted prior to the COVID-19 pandemic. These pre-pandemic results indicated that for some women with AUD, the telephone platform might not be optimal. However, since the pandemic onset, telehealth options for treatment of AUD have become more acceptable 45,46 and a replication of this study may be warranted to assess the effectiveness of this delivery platform given these secular changes in telehealth acceptability.
Given the potential morbidity and mortality of alcohol-related liver disease, it is important to identify barriers to alcohol treatment among this subset of patients. In one mixed-methods study, qualitative data was collected for 22 outpatients (10 women, 12 men) with alcohol-related hepatitis or liver cirrhosis, who completed semi-structured interviews 39. In women, five AUD treatment barriers were identified—not wanting treatment, financial or insurance challenges, transportation challenges, social anxiety or discomfort in groups, and stigma. Sample size precluded formal statistical comparisons of these barriers for men and women.
In sum, both attitudinal and structural barriers to treatment utilization for women are common. Barriers to women’s AUD treatment utilization may also be affected by other factors such as race/ethnicity and medical complexity. Attitudinal barriers (e.g., can stop on one’s own, stigma) and certain personal barriers (e.g., having dependents) may suggest possible targets for intervention among sub-groups of women with AUD. Finally, VHA studies show that interventions directed to providers and potential telemedicine interventions may yield improvements in reducing barriers to AUD treatment.
DISCUSSION
This review examined the recent literature on alcohol treatment access and engagement among women in the U.S. with a specific focus on SBIRT, treatment utilization, engagement in treatment, and barriers to treatment. Gender-specific barriers to AUD and other SUD treatment utilization for women in the U.S. have been well documented 47. While treatment-seeking and utilization for most health care conditions in the U.S. are more likely among women than men (e.g., doctor visits, annual physical exams, mental health treatment visits) 7, this does not apply to alcohol treatment.
Despite recommendations for universal screening and brief intervention, most of the recent literature shows that approximately 15%−25% of individuals report not being asked about their alcohol use by their medical provider 18,19. Moreover, documented rates of alcohol screening in the medical record were found to be extremely low 14. Rates of brief intervention following screening were even lower, with evidence consistently showing that compared to men, women were less likely to receive advice about drinking risks and less likely to be linked to treatment services 15,16. Of concern, the proportion of women of reproductive age who received advice about risks for alcohol exposed pregnancy was also low in women’s health clinics 17. This is especially paradoxical given that women in this study reported not minding being asked about their alcohol use or participating in SBIRT 17.
Several barriers to SBIRT have been documented in the literature including lack of provider training and comfort with delivering SBIRT, lack of referral sources, time constraints and competing demands, provider concerns about patients’ receptivity to discussing their alcohol use, and concerns about legal ramifications for pregnant persons reporting alcohol use 11. Similarly, women’s perception of feeling “judged” by their PCP and their provider’s presentation of treatment options were cited as factors in women’s receptivity to alcohol treatment receipt 44. Enhancing provider education in effective approaches to engage women in discussion about their alcohol use is essential in delivering brief interventions and referral to treatment. In addition, the use of digital programs might help alleviate some barriers. Implementation of electronic SBIRT (e-SBIRT) is effective in reducing risky alcohol use and related harms 48. E-SBIRT programs have the potential to eliminate some of the disparities documented in the literature when they are applied universally as part of regular clinical care. Additionally, research is needed on the feasibility and efficacy of tailoring e-SBIRT to gender and/or racial/ethnic subgroups to enhance engagement and outcomes with SBIRT.
Our findings demonstrate low treatment utilization for AUD for both men and women 22, with indication of even lower rates of alcohol treatment utilization for women 21. Several studies in our review point to gender differences in AUD treatment utilization 21,27, pharmacotherapy 32, and barriers to treatment 40 that also vary with race/ethnicity. A compilation of 2015–2019 NSDUH data by gender and race/ethnicity among people age 12 and older 3 found that for people who needed alcohol treatment during these survey years, alcohol treatment utilization was low overall and ranged from 4.4% to 22.4% depending on gender, race, and ethnicity 49. Among White, Black/African American, Asian, and Hispanic/Latino populations, women were less likely to receive alcohol use treatment at any location compared with men (ranging from 3.2% of Asian women to 14.3% of Black/African American women in need of alcohol treatment) 49.. A full review of the complexity of the intersection of gender with race and ethnicity on AUD treatment utilization and barriers to AUD care is beyond the scope of the present review. However, there is a clear need for additional research to understand the intersection of gender, race and ethnicity and access to AUD treatment as well as developing and testing tailored interventions for these populations.
There are a range of barriers to treatment engagement and utilization among women with AUD. While gender-specific treatment for women holds promise, additional research is needed. Epstein et al. 34 found that AUD treatment among women was equally effective in individual female-specific CBT and gender-neutral CBT in improving drinking outcomes and there were no differences in engagement 34. Additionally, female-specific CBT group therapy for AUD did not further improve engagement or retention relative to individual therapy 35. Previous research has demonstrated that gender-specific group therapy for women with SUDs including those with AUD and/or drug use disorders and co-occurring other psychiatric disorders is a feasible and effective component of care for adult women 47,50 and delivery of this gender-responsive component of care in mixed-gender treatment settings is consistent with SAMHSA guidance on supporting women in co-ed settings 51. In a small qualitative study of women Veterans in the VHA, participants indicated greater receptivity to engaging in AUD treatment if gender-specific treatment was available 44. Implementation research utilizing these efficacious gender-responsive treatments could further elucidate the most effective settings and approaches to engage and retain women with AUD in treatment.
Digital interventions may be useful in increasing access and engagement in AUD treatment. One study of an open access web-based program for problem drinkers in the Netherlands demonstrated some support for diminished attrition among women problem drinkers 52. A secondary data analysis of a factorial randomized controlled trial in the United Kingdom of adult drinkers of the “Drink Less” app-based intervention demonstrated that female gender was associated positively with response to follow-up 53. The study by Myers et al. 36 of treatment engagement for women in treatment for AUD and PTSD showed that having dependents at home was negatively correlated with engagement and retention. Digital interventions may be more accessible for women with dependents. Taken together, these studies indicate that digital strategies to reduce drinking and engage in AUD treatment are promising and additional research is warranted. In addition, a recent systematic review by Simpson et al. 54 of 44 randomized controlled trials of online alcohol interventions across multiple countries with relevant trials showed women comprised 51.2% of community recruited samples and 35.8% of clinical samples. It was noted that the prevalence of women with AUD across the relevant countries was 27.1%. The over-representation of women in these RCTs of on-line alcohol intervention trials compared with the AUD prevalence rates may provide additional support that on-line and web-based treatment hold promise in increasing women’s access and engagement in AUD treatment.
Increasing our understanding of barriers to treatment receipt and increasing access to treatment for women with AUD is an essential public health consideration. Furthermore, studies on the impact of other intersectional factors (e.g., sexual orientation, gender, race) are a critically important area for future research to understand the range of barriers to screening, treatment receipt, and engagement among women with a range of alcohol problems. It is incumbent on researchers to ensure representative samples and analyze data accordingly. Understanding these factors could help design interventions that are more responsive to the needs of specific populations by both gender and race/ethnicity. An emerging field that requires additional research is on transgender individuals including those who identify as transgender women 55,56. Better opportunities for individuals to self-identify their gender in epidemiologic surveys and clinical research can inform this field. In addition, this targeted review focused on adults 18 and over and did not include alcohol use in adolescent girls, a topic that needs further review and investigation given rates of drinking and AUD in this population.
Conclusion
Stigma and attitudinal barriers combined with structural barriers including provider lack of education, training, and resources contribute to low AUD treatment utilization overall and among women more specifically 40,41,57. Given the rising rates of alcohol problems and AUD among women and girls in the U.S., this is especially problematic. Implementation research on gender-specific strategies to increase access, engagement, and retention for women with AUD is warranted. Increasing clinician education and incentives to screen and engage women in treatment is critical. Health system emphasis on disseminating resources such as the National Institute on Alcohol Abuse and Alcoholism (NIAAA) Alcohol Treatment Navigator 58 and NIAAA Clinician Resources such as Alcohol Core Resources 59 may assist in overcoming some clinician barriers. More research on gender and culturally responsive treatment approaches, as well as digital interventions are also needed to increase treatment utilization across the spectrum of severity of alcohol problems for women in the U.S.
Acknowledgments:
This work was supported by the National Institute of Drug Abuse, Grant/Award Number: K23DA050780, and the Women’s Mental Health Innovation Fund, McLean Hospital.
Footnotes
Declaration Statement:
The authors have no competing interests to declare that are relevant to the content of this article.
REFERENCES
- 1.Robins LE, Regier DA, eds. Psychiatric Disorders in America: The Epidemiologic Catchment Area Study New York: The Free Press, 1991. [Google Scholar]
- 2.Substance Abuse and Mental Health Services Administration. National Survey on Drug Use and Health, 2018 and 2019, Table 5.4A – Alcohol Use Disorder in Past Year among Persons Aged 12 or Older, by Age Group and Demographic Characteristics: Numbers in Thousands, 2018 and 2019. Center for Behavioral Health Statistics and Quality (https://www.samhsa.gov/data/sites/default/files/reports/rpt29394/NSDUHDetailedTabs2019/NSDUHDetTabsSect5pe2019.htm). (accessed April 30, 2023).
- 3.Center for Behavioral Health Statistics and Quality. Racial/ethnic differences in substance use, substance use disorders, and substance use treatment utilization among people aged 12 or older (2015–2019). Figure 4.5 – Alcohol Use Disorder in the Past Year among People Aged 12 or older, by Race/Ethnicity and Gender: 2015–2019, Annual Averages Rockville, MD: Substance Abuse and Mental Health Services Administration, 2021. (https://www.samhsa.gov/data/sites/default/files/reports/rpt35326/2021NSDUHSUChartbook.pdf ). [Google Scholar]
- 4.Grant BF, Chou SP, Saha TD, et al. Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV Alcohol Use Disorder in the United States, 2001–2002 to 2012–2013: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry 2017;74(9):911–923. DOI: 10.1001/jamapsychiatry.2017.2161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Substance Abuse and Mental Health Services Administration (SAMHSA). 2020 NSDUH Detailed Tables 2020. (https://www.samhsa.gov/data/report/2020-nsduh-detailed-tables).
- 6.Rodriguez LM, Litt DM, Stewart SH. Drinking to cope with the pandemic: The unique associations of COVID-19-related perceived threat and psychological distress to drinking behaviors in American men and women. Addict Behav 2020;110:106532. DOI: 10.1016/j.addbeh.2020.106532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Division of Population Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. Excessive Alcohol Use is a Risk to Women’s Health (https://www.cdc.gov/alcohol/fact-sheets/womens-health.htm). (accessed April 30, 2023).
- 8.Substance Abuse and Mental Health Data Archive (SAMHDA). National Survey on Drug Use and Health 2018 Public Use File Dataset 2018. (https://www.datafiles.samhsa.gov/dataset/national-survey-drug-use-and-health-2018-nsduh-2018-ds0001).
- 9.Ray LAP, Bujarski SP, Grodin EP, et al. State-of-the-art behavioral and pharmacological treatments for alcohol use disorder. Am J Drug Alcohol Abuse 2019;45(2):124–140. DOI: 10.1080/00952990.2018.1528265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.National Institutes of Health, Office of Research on Women’s Health (ORWH). Sex & Gender (https://orwh.od.nih.gov/sex-gender). (accessed April 30, 2023).
- 11.Hammock K, Velasquez MM, Alwan H, von Sternberg K. Alcohol Screening, Brief Intervention, and Referral to Treatment (SBIRT) for Girls and Women. Alcohol Res 2020;40(2):07. DOI: 10.35946/arcr.v40.2.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Curry SJ, Krist AH, Owens DK, et al. Screening and Behavioral Counseling Interventions to Reduce Unhealthy Alcohol Use in Adolescents and Adults: US Preventive Services Task Force Recommendation Statement. Jama 2018;320(18):1899–1909. DOI: 10.1001/jama.2018.16789. [DOI] [PubMed] [Google Scholar]
- 13.O’Connor EA, Perdue LA, Senger CA, et al. Screening and Behavioral Counseling Interventions to Reduce Unhealthy Alcohol Use in Adolescents and Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. Jama 2018;320(18):1910–1928. DOI: 10.1001/jama.2018.12086. [DOI] [PubMed] [Google Scholar]
- 14.Chatterton B, Agnoli A, Schwarz EB, Fenton JJ. Alcohol Screening During US Primary Care Visits, 2014–2016. Journal of general internal medicine 2022;37(15):3848–3852. DOI: 10.1007/s11606-021-07369-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mauro PM, Askari MS, Han BH. Gender differences in any alcohol screening and discussions with providers among older adults in the United States, 2015 to 2019. Alcohol Clin Exp Res 2021;45(9):1812–1820. DOI: 10.1111/acer.14668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vanneman ME, Harris AHS, Chen C, Adams RS, Williams TV, Larson MJ. Postdeployment Behavioral Health Screens and Linkage to the VeteransHealth Administration for Army Reserve Component Members. Psychiatr Serv 2017;68(8):803–809. DOI: 10.1176/appi.ps.201600259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hettema J, Cockrell S, Russo J, et al. Missed Opportunities: Screening and Brief Intervention for Risky Alcohol Use in Women’s Health Settings. J Womens Health (Larchmt) 2015;24(8):648–654. DOI: 10.1089/jwh.2014.4961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Luong J, Board A, Gosdin L, et al. Alcohol Use, Screening, and Brief Intervention Among Pregnant Persons - 24 U.S. Jurisdictions, 2017 and 2019. MMWR Morb Mortal Wkly Rep 2023;72(3):55–62. DOI: 10.15585/mmwr.mm7203a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mintz CM, Hartz SM, Fisher SL, et al. A cascade of care for alcohol use disorder: Using 2015–2019 National Survey on Drug Use and Health data to identify gaps in past 12-month care. Alcohol Clin Exp Res 2021;45(6):1276–1286. DOI: 10.1111/acer.14609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Park-Lee E, Lipari RN, Hedden SL, Kroutil LA, Porter JD. Receipt of Services for Substance Use and Mental Health Issues Among Adults: Results from the 2016 National Survey on Drug Use and Health. Substance Abuse and Mental Health Services Administration (US) (https://www.samhsa.gov/data/sites/default/files/NSDUH-DR-FFR2-2016/NSDUH-DR-FFR2-2016.htm). (accessed April 30, 2023). [PubMed]
- 21.Alvanzo AA, Storr CL, Mojtabai R, et al. Gender and race/ethnicity differences for initiation of alcohol-related service use among persons with alcohol dependence. Drug Alcohol Depend 2014;140:48–55. DOI: 10.1016/j.drugalcdep.2014.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chartier KG, Miller K, Harris TR, Caetano R. A 10-year study of factors associated with alcohol treatment use andnon-use in a U.S. population sample. Drug Alcohol Depend 2016;160:205–211. DOI: 10.1016/j.drugalcdep.2016.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dawson DA, Goldstein RB, Grant BF. Factors associated with first utilization of different types of care for alcohol problems. J Stud Alcohol Drugs 2012;73(4):647–56. DOI: 10.15288/jsad.2012.73.647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Edlund MJ, Booth BM, Han X. Who seeks care where? Utilization of mental health and substance use disorder treatment in two national samples of individuals with alcohol use disorders. J Stud Alcohol Drugs 2012;73(4):635–46. DOI: 10.15288/jsad.2012.73.635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gilbert PA, Pro G, Zemore SE, Mulia N, Brown G. Gender Differences in Use of Alcohol Treatment Services and Reasons for Nonuse in a National Sample. Alcohol Clin Exp Res 2019;43(4):722–731. DOI: 10.1111/acer.13965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kaufmann CN, Chen LY, Crum RM, Mojtabai R. Treatment seeking and barriers to treatment for alcohol use in persons with alcohol use disorders and comorbid mood or anxiety disorders. Soc Psychiatry Psychiatr Epidemiol 2014;49(9):1489–99. DOI: 10.1007/s00127-013-0740-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Martin CE, Parlier-Ahmad AB, Beck L, Scialli A, Terplan M. Need for and Receipt of Substance Use Disorder Treatment Among Adults, by Gender, in the United States. Public Health Rep 2021;137(5):955–963. DOI: 10.1177/00333549211041554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zemore SE, Murphy RD, Mulia N, et al. A moderating role for gender in racial/ethnic disparities in alcohol services utilization: results from the 2000 to 2010 national alcohol surveys. Alcohol Clin Exp Res 2014;38(8):2286–96. DOI: 10.1111/acer.12500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Del Re AC, Gordon AJ, Lembke A, Harris AHS. Prescription of topiramate to treat alcohol use disorders in the Veterans Health Administration. Addict Sci Clin Pract 2013;8(1):12. DOI: 10.1186/1940-0640-8-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Finlay AK, Binswanger IA, Smelson D, et al. Sex differences in mental health and substance use disorders and treatment entry among justice-involved Veterans in the Veterans Health Administration. Med Care 2015;53(4 Suppl 1):S105–11. DOI: 10.1097/mlr.0000000000000271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rieckmann T, Muench J, McBurnie MA, et al. Medication-assisted treatment for substance use disorders within a national community health center research network. Subst Abus 2016;37(4):625–634. DOI: 10.1080/08897077.2016.1189477. [DOI] [PubMed] [Google Scholar]
- 32.Taylor E, Timko C, Harris AHS, Yu M, Finlay AK. Receipt of pharmacotherapy for alcohol use disorder by justice-involved women in the Veterans Health Administration. Addict Sci Clin Pract 2019;14(1):1. DOI: 10.1186/s13722-018-0129-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Knox J, Hasin DS, Larson FRR, Kranzler HR. Prevention, screening, and treatment for heavy drinking and alcohol use disorder. Lancet Psychiatry 2019;6(12):1054–1067. DOI: 10.1016/s2215-0366(19)30213-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Epstein EE, McCrady BS, Hallgren KA, Cook S, Jensen NK, Hildebrandt T. A randomized trial of female-specific cognitive behavior therapy foralcohol dependent women. Psychol Addict Behav 2017;32(1):1–15. DOI: 10.1037/adb0000330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Epstein EE, McCrady BS, Hallgren KA, et al. Individual versus group female-specific cognitive behavior therapy for alcohol use disorder. J Subst Abuse Treat 2018;88:27–43. DOI: 10.1016/j.jsat.2018.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Myers US, Browne KC, Norman SB. Treatment Engagement: Female Survivors of Intimate Partner Violence inTreatment for PTSD and Alcohol Use Disorder. J Dual Diagn 2015;11(3–4):238–247. DOI: 10.1080/15504263.2015.1113762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McCrady BS, Epstein EE, Hallgren KA, Cook S, Jensen NK. Women with alcohol dependence: A randomized trial of couple versus individual plus couple therapy. Psychol Addict Behav 2016;30(3):287–99. DOI: 10.1037/adb0000158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.McCrady BS, Epstein EE, Cook S, Jensen N, Hildebrandt T. A randomized trial of individual and couple behavioral alcohol treatment for women. J Consult Clin Psychol 2009;77(2):243–56. DOI: 10.1037/a0014686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mellinger JL, Scott Winder G, DeJonckheere M, et al. Misconceptions, preferences and barriers to alcohol use disorder treatment in alcohol-related cirrhosis. J Subst Abuse Treat 2018;91:20–27. DOI: 10.1016/j.jsat.2018.05.003. [DOI] [PubMed] [Google Scholar]
- 40.Verissimo ADO, Grella CE. Influence of gender and race/ethnicity on perceived barriers to help-seeking for alcohol or drug problems. J Subst Abuse Treat 2017;75:54–61. DOI: 10.1016/j.jsat.2016.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Abraham TH, Lewis ET, Cucciare MA. Providers’ Perspectives on Barriers and Facilitators to Connecting Women Veterans to Alcohol-Related Care From Primary Care. Mil Med 2017;182(9):e1888–e1894. DOI: 10.7205/MILMED-D-17-00042. [DOI] [PubMed] [Google Scholar]
- 42.Abraham TH, Wright P, White P, Booth BM, Cucciare MA. Feasibility and acceptability of shared decision-making to promote alcohol behavior change among women Veterans: Results from focus groups. J Addict Dis 2017;36(4):252–263. DOI: 10.1080/10550887.2017.1373318. [DOI] [PubMed] [Google Scholar]
- 43.Cucciare MA, Lewis ET, Hoggatt KJ, et al. Factors Affecting Women’s Disclosure of Alcohol Misuse in Primary Care: A Qualitative Study with U.S. Military Veterans. Womens Health Issues 2016;26(2):232–9. DOI: 10.1016/j.whi.2015.07.010. [DOI] [PubMed] [Google Scholar]
- 44.Lewis E, Jamison A, Ghaus S, et al. Receptivity to Alcohol-Related Care among US Women Veterans with Alcohol Misuse. Journal of addictive diseases 2016;35. DOI: 10.1080/10550887.2016.1171670. [DOI] [PubMed]
- 45.Glasner S, Webb J, Michero D, et al. Feasibility, Acceptability, and Preliminary Outcomes of an Integrated Telemedicine Intervention Combining Naltrexone and Cognitive Behavioral Therapy for Alcohol Use Disorder. Telemedicine Reports 2022;3(1):184–190. DOI: 10.1089/tmr.2022.0029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Molfenter T, Roget N, Chaple M, et al. Use of Telehealth in Substance Use Disorder Services During and After COVID-19: Online Survey Study. JMIR Ment Health 2021;8(2):e25835. DOI: 10.2196/25835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Greenfield SF, Brooks AJ, Gordon SM, et al. Substance abuse treatment entry, retention, and outcome in women: a review of the literature. Drug Alcohol Depend 2007;86(1):1–21. DOI: 10.1016/j.drugalcdep.2006.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tansil KA, Esser MB, Sandhu P, et al. Alcohol Electronic Screening and Brief Intervention: A Community Guide Systematic Review. Am J Prev Med 2016;51(5):801–811. DOI: 10.1016/j.amepre.2016.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Center for Behavioral Health Statistics and Quality. Racial/ethnic differences in substance use, substance use disorders, and substance use treatment utilization among people aged 12 or older (2015–2019) Rockville, MD: Substance Abuse and Mental Health Services Administration, 2021. (https://www.samhsa.gov/data/sites/default/files/reports/rpt35326/2021NSDUHSUChartbook.pdf ). [Google Scholar]
- 50.Greenfield SF, Sugarman DE, Freid CM, et al. Group therapy for women with substance use disorders: results from the Women’s Recovery Group Study. Drug Alcohol Depend 2014;142:245–53. DOI: 10.1016/j.drugalcdep.2014.06.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Substance Abuse and Mental Health Services Administration. Guidance Document for Supporting Women in Co-ed Settings Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016. [Google Scholar]
- 52.Postel MG, de Haan HA, ter Huurne ED, van der Palen J, Becker ES, de Jong CA. Attrition in Web-Based Treatment for Problem Drinkers. J Med Internet Res 2011;13(4):e117. (Original Paper). DOI: 10.2196/jmir.1811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Garnett C, Perski O, Tombor I, West R, Michie S, Brown J. Predictors of Engagement, Response to Follow Up, and Extent of Alcohol Reduction in Users of a Smartphone App (Drink Less): Secondary Analysis of a Factorial Randomized Controlled Trial. JMIR Mhealth Uhealth 2018;6(12):e11175. (Original Paper). DOI: 10.2196/11175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Simpson T, Sistad R, Brooks JT, Newberger NG, Livingston NA. Seeking care where they can: A systematic review of global trends in online alcohol treatment utilization among non-veteran and veteran women. Drug Alcohol Depend Rep 2022;5:100116. DOI: 10.1016/j.dadr.2022.100116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Connolly DJ, Davies E, Lynskey M, et al. Differences in Alcohol and Other Drug Use and Dependence Between Transgender and Cisgender Participants from the 2018 Global Drug Survey. LGBT Health 2022;9(8):534–542. DOI: 10.1089/lgbt.2021.0242. [DOI] [PubMed] [Google Scholar]
- 56.Wolfe HL, Biello KB, Reisner SL, Mimiaga MJ, Cahill SR, Hughto JMW. Transgender-related discrimination and substance use, substance use disorder diagnosis and treatment history among transgender adults. Drug Alcohol Depend 2021;223:108711. DOI: 10.1016/j.drugalcdep.2021.108711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sugarman DE, Meyer LE, Reilly ME, Greenfield SF. Women’s and men’s experiences in group therapy for substance use disorders: A qualitative analysis. Am J Addict 2022;31(1):9–21. DOI: 10.1111/ajad.13242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.National Institute on Alcohol Abuse and Alcoholism. NIAAA Alcohol Treatment Navigator (https://alcoholtreatment.niaaa.nih.gov/). (accessed April 30, 2023).
- 59.National Institute on Alcohol Abuse and Alcoholism. The Healthcare Professional’s Core Resource on Alcohol (https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol). (accessed April 30, 2023).