

Abstract
Background: Injuries of the volar ligaments of the wrist are not uncommon, but their arthroscopic treatment presents a significant challenge. The objective of this paper is to introduce a technique for reattaching (in acute injuries) or reinforcing (in chronic injuries) various volar wrist ligaments to the bone, using standard wrist arthroscopic dorsal and volar portals.
Methods: There are three common steps for all the arthroscopic volar capsuloligamentous reattachments or reinforcements
Step 1 – Volar Portal Establishment: volar radial, volar ulnar and volar central portals are used depending on which structure needs to be reattached or reinforced.
Step 2 – Anchor Placement: the anchor is positioned at the site where the ligament has been detached.
Step 3 – Capsuloligamentous Suture and Knotting: a knot pusher is introduced inside the joint from the dorsal portal and advanced inside the volar portal where the threads of the anchor are located. The knot pusher is loaded with the threads and retrieved to the dorsal portal. A 16G Abbocath, loaded with a loop is used to pierce the volar ligaments. The loop of the Abbocath is captured from the dorsal portal and loaded with the threads. Both threads are taken to the volar portal and knotted after releasing the traction. This way the knot is placed out of the wrist and the ligaments are reattached or reinforced to the bone.
Result: This technique has been used to reinforce and reattach the scapholunate and lunotriquetral ligaments and to reattach the radiocarpal ligaments and the Poirier space. Since this procedure has been performed in various conditions and in conjunction with other ligament treatments (such as perilunate injuries, carpal bone fractures, distal radius fractures, and reinforcement or reattachment of the dorsal portions of intrinsic ligaments), specific results are not presented.
Conclusions: The described technique enables the reattachment and reinforcement of most volar ligaments to the bone using standard wrist arthroscopic portals. It can be performed in conjunction with the treatment of the dorsal portion of intrinsic ligaments or other wrist injuries.
Keywords: volar capsuloligamentous suture, wrist arthroscopy, perilunate injuries, scapholunate injury, lunotriquetral injury
The present paper describes a technique to reattach (in acute injuries) or reinforce (in chronic injuries) the various volar ligament(s) of the wrist. This technique can be used in conjunction with other arthroscopic procedures.
This technique can be performed in many different conditions such as perilunate injuries, carpal bone fractures, distal radius fractures, dorsal reinforce, or reattachment, so no specific results are presented.
Indications and Contraindications
The technique described is a universal reattaching or reinforcement technique for the volar ligament(s) of the wrist both in acute (reattachment) and chronic (reinforcement) conditions, such as in distal radius fracture, carpal fractures, perilunate fractures-dislocation, or even in the radiocarpal dislocation. Indications for the usage of the technique are fresh injury of the volar ligament(s) of the wrist and some of the chronic conditions with enough quality of the ligaments for reinforcement that are found in grade IIIA instabilities of scapholunate (SL) interosseous ligament and lunotriquetral (LT) interosseous ligament injuries in the European Wrist Arthroscopy Society (EWAS) classification. 1 The reinforcement of the dorsal portions of the SL and LT ligaments as the grade IIIC of the EWAS classification 1 is also possible to be performed along with the technique described.
The contraindication of the technique in acute injuries is infection and compartment syndrome, as same as open surgeries. In the chronic condition, the contraindications are no remnant of the ligament of the volar wrist ligament and irreducible wrist with manual reduction or finger trap traction. In such cases, the open ligament reconstruction using free tendon graft is considered. 2
Surgical Technique
Preparation, Patient Positioning, Instruments, and Portals
The surgery can be performed under regional or general anesthesia. The patient is positioned in the supine position, and the tourniquet is applied. The elbow is flexed in 90 degrees, and finger traps are set on the long and ring fingers with vertical traction. Any traction tower which allows us to access the volar side of the wrist is preferable. The technique requires two experienced surgeons, one works on the dorsal side and the second on the volar.
Small suture anchors are used to reattach or reinforce the volar wrist ligament(s) to the carpal bone. The lasso to retract the threads is needed (a lasso of a commercial company or a 16-G Abbocath loaded with a thread loop). Finally, a small knot pusher is used to retrieve the threads.
The four common dorsal wrist portals, 3/4, 6R, ulnar midcarpal (MCU) and radial midcarpal (MCR) are used, and to perform volar repairs, additional volar wrist portals as follows are necessary ( Fig. 1 ).
Fig. 1.

Volar portals. ( A ) Volar radial portal. 3 ( B ) Volar central portal. 4 ( C ) Volar ulnar portal. 5
Volar radial (VR) portal 3 : the portal is useful to reattach or reinforce the volar portion of the SL ligament or the radioscaphocapitate ligament.
Volar central (VC) portal 4 : this portal is useful to reattach or reinforce the volar portion of the LT ligament or closure of the Poirier space.
Volar ulnar (VU) portal 5 : this portal is useful to reattach or reinforce the volar portion of the LT ligament as same as the VC portal.
A dry arthroscopy technique popularized by Del Piñal et al 6 is preferable for this repairing technique compared with the conventional wet technique, because of less effusion of the saline.
Common Steps
There are three common steps for all the volar capsuloligamentous reattachment or reinforcement.
Step 1: Volar Portal Estasblishment
The dorsal (either 3–4 or 6R in radiocarpal joint, MCR or MCU for midcarpal joint), VR, VC, or VU portals are used in this step. To create the portals, the transillumination effect of the arthroscope is useful for its precise positioning. In specific acute cases, the area of the detachment of the volar ligaments can be used and it is not necessary to create a “capsular portal.”
Step 2: Anchor Placement
In acute cases, the anchor is introduced to the specific carpal bone to reattach the avulsed ligament under arthroscopically visualization from the dorsal portals. In chronic injuries, if the detachment area is not clear, the anchor can be introduced fluoroscopically.
Step 3: How to Repair: Capsuloligamentous Suture and Knotting
After the anchor setting to the carpal bone, a knot pusher is introduced through the dorsal portal to the volar capsule portal. Once the pusher is out from the joint, the threads of the anchor are introduced into the pusher, and then pulling the knot pusher makes two threads of the anchor retrieved out from the dorsal portal ( Fig. 2 ). The 16G Abbocath catheter with a loop pierces the one side of the ruptured volar ligament, and then it is forwarded to dorsal side through the dorsal portal. The loop introduced the one of the two threads of the suture anchor to again volar, passing through the ruptured volar ligament. This way the first limb of the “U” capsuloligamentous suture is performed ( Fig. 3 ). The same procedure is performed through the other side of the ruptured ligament, and the other thread is introduced into the ligament as the second limb of the “U” capsuloligamentous suture. Finally, both threads are knotted to reattach or to reinforce the ruptured ligament ( Fig. 4 ). When Kirschner wires (K-wires) are needed for dislocated or displaced bones to realign, such as in the perilunate injuries, the fixation should be performed before the insertion of the bone anchor in order to not to harm the threads. Traction also may be removed before the threads be knotted.
Fig. 2.
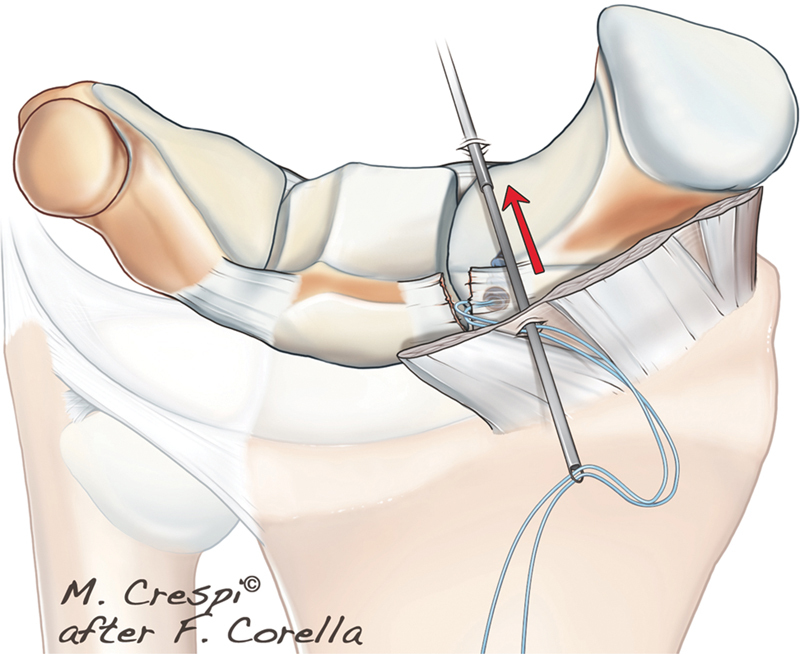
A knot pusher is introduced inside the joint from the dorsal portal located in front of the ligament portion to repair and exit through the volar capsule portal to the volar approach (VR, VC, or VU), where the threads of the anchor are located. The knot pusher is loaded with the two threads and retrieved to the dorsal portal. Adapted from Corella, Heras-Palou, Luchetti. Carpal ligament injuries and instability: FESSH Instructional Course Book 2023. Stuttgart: Thieme; 2023.
Fig. 3.
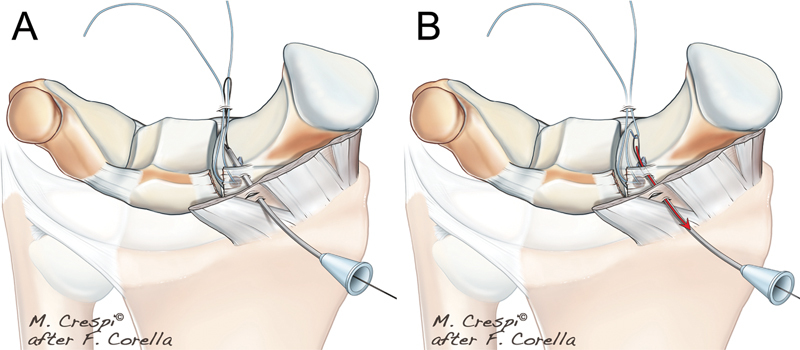
( A ) A 16G Abbocath loaded with a loop is used to pierce the volar ligament. The loop is captured from dorsal (where the threads are located) and is loaded with the first thread. ( B ) The loaded loop taken from the volar portal. Then the first limb of the “U” capsuloligamentous suture is completed. Adapted from Corella, Heras-Palou, Luchetti. Carpal Ligament Injuries and Instability: FESSH Instructional Course Book 2023. Stuttgart: Thieme; 2023.
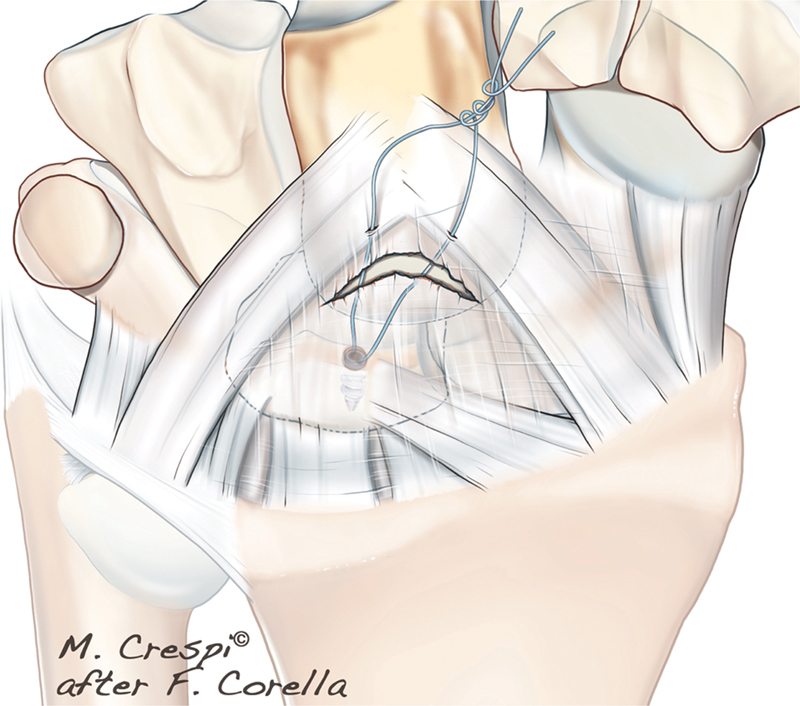
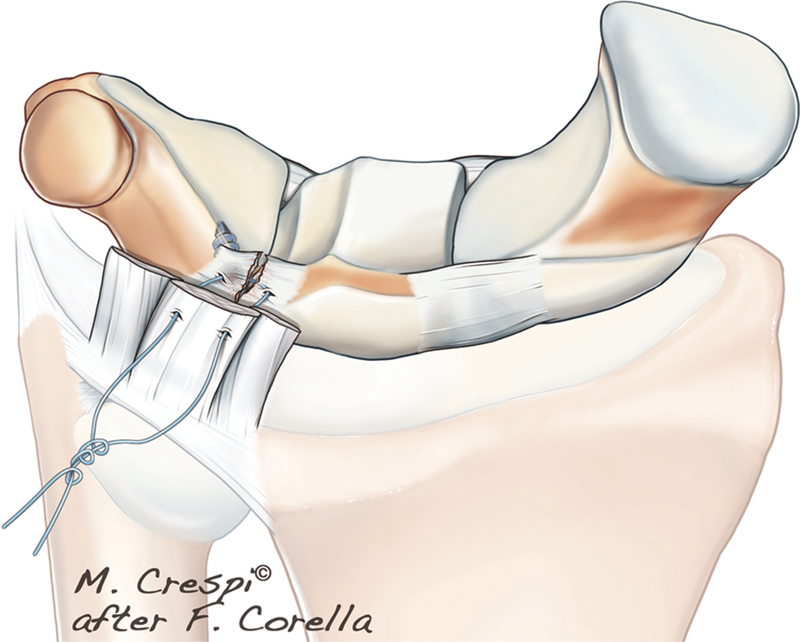
Fig. 4.
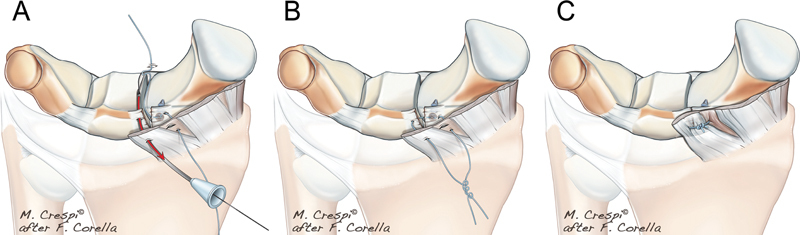
( A ) The 16G loaded Abbocath pierces through the volar ligament again. The second thread is captured in the dorsal portal. ( B ) When two limbs of the suture are in the volar portal, both threads are knotted. ( C ) The knot remains out of the wrist and the captured tissue is reattached or reinforced to the bone. Adapted from, Corella, Heras-Palou, Luchetti. Carpal Ligament Injuries and Instability: FESSH Instructional Course Book 2023. Stuttgart: Thieme; 2023.
Scapholunate Volar Capsuloligament Reinforcement to Bone
This is a relatively common chronic injury without hemorrhagic avulsion injury.
Step 1: The VR portal 3 and the capsular portal are set just over the SL joint viewed from the MCU portal ( Fig. 5 ).
Step 2: The anchor is usually placed on the volar side of the scaphoid. It is easy to place the arthroscope in the MCU portal and the probe in the MCR portal to separate the soft tissues and visualized better the introduction of the anchor. If the K-wire is not easily seen, a fluoroscope can be used to ensure the correct position ( Fig. 6 ).
Step 3: A knot pusher is introduced inside the joint from the MCR portal, through the volar capsular portal and exits through the VR portal approach. The knot pusher is loaded with the two threads and taken to the MCR portal ( Fig. 7 ).
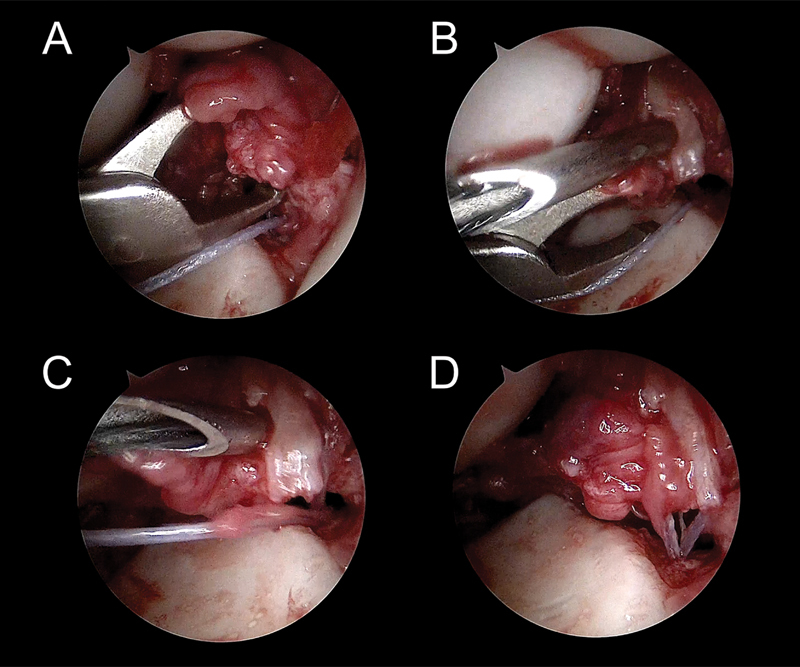
Fig. 5.
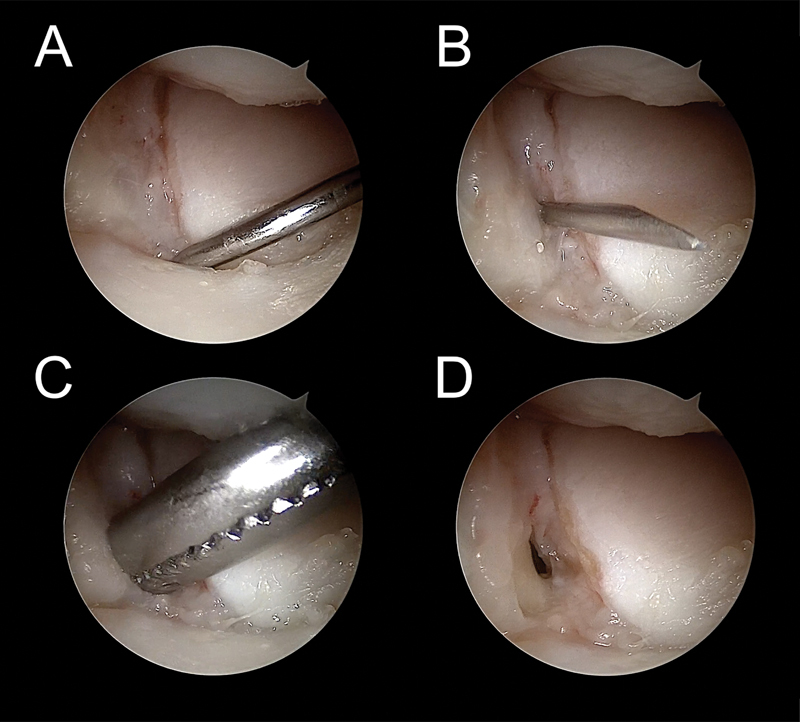
( A ) A probe entering in the volar SL joint explores the volar injury. ( B ) A needle is introduced to locate the position of the capsular portal, just over the SL joint. ( C ) A blunt dissector is used to expand the portal. D. Final aspect and location of the portal in the midcarpal joint.
Fig. 6.
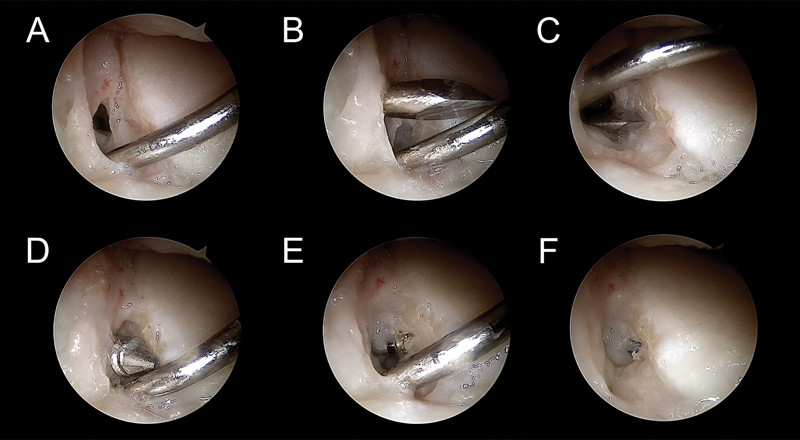
( A ) The arthroscope is in the MCU portal and a probe separates the soft tissues through the MCR portal for better visualization of the anchor insertion. ( B and C ) The hole for the anchor is made at the volar SL ligament insertion. ( D and F ) The anchor is introduced from the VR portal.
Fig. 7.
( A and B ). A knot pusher is introduced form the MCR portal to the VR portal. ( C and D ) The knot pusher is loaded with the threads and taken to the MCR portal.
The Abbocath loaded with the loop is used to pierce the volar capsule and ligaments. Depending on the laxity or type of injury, the position of the suture may be different. In ordinary circumstances, it should go from proximal to distal, exiting one of the limbs of the suture, in the SL joint.
The loop is captured from the MCR portal with a grasper, loaded with the first thread, and retrieved again to the VR portal ( Fig. 8 ).
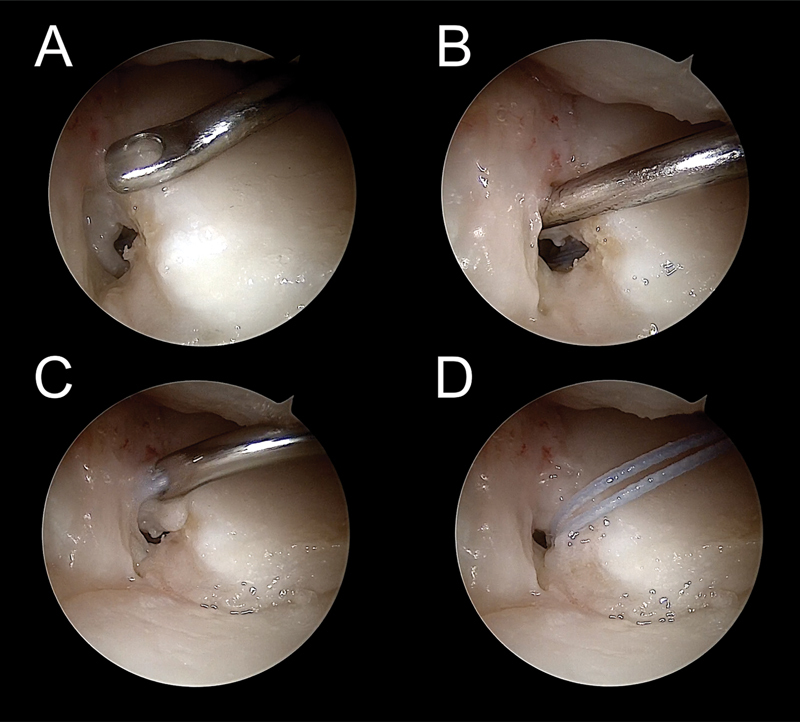
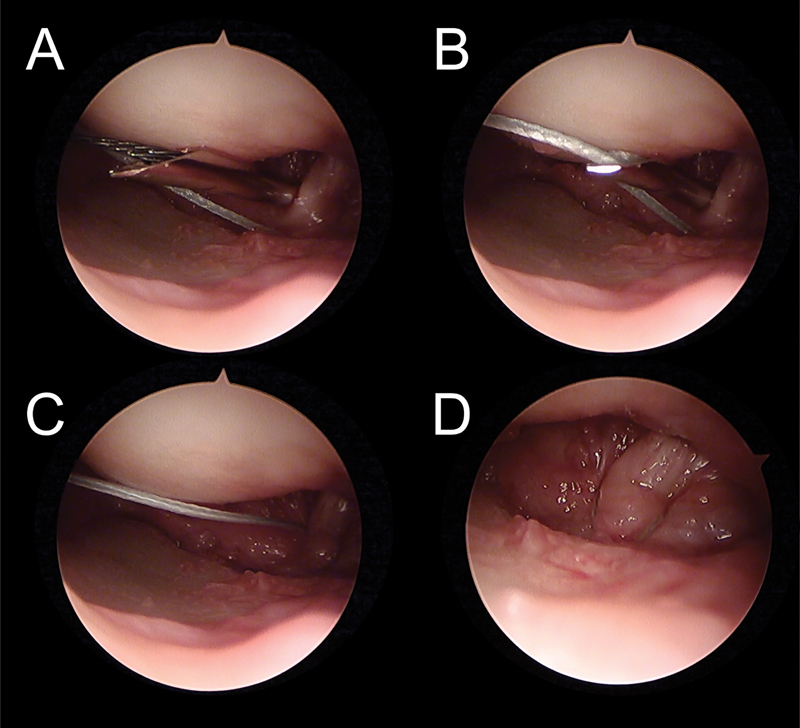
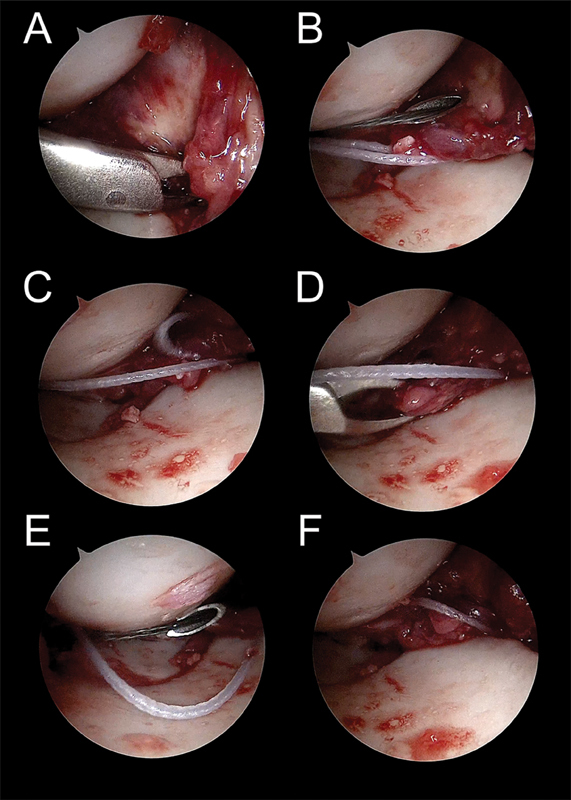
Fig. 8.
( A ) 16G Abbocath loaded with a loop pierces the volar capsule and volar portion of the SL ligament form volar to distal, exiting in the SL joint. ( B and C ) The loop is captured from the MCR portal with a grasper and is loaded with the first thread. ( D and F ) The loop is retrieved again to the VR portal. The first limb of the “U” capsuloligamentous suture is completed.
The same procedure is performed again piercing the capsule and ligament in a more ulnar position, also from proximal to distal, trying to capture as much tissue as possible. Finally, traction is removed, and the two threads are knotted, maintaining the knot out of the join ( Figs. 4 and 9 ).
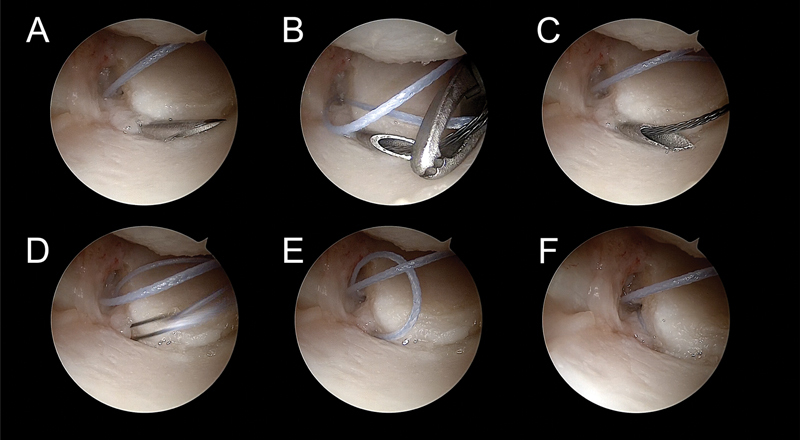
Fig. 9.
( A ) The Abbocath is introduced in a more ulnar position, again from proximal to distal, trying to capture as much tissue as possible. ( B ) The loop is taken to the MCR portal and loaded with the second thread. ( C and D ) The loop and thread are retrieved to the volar side, so the second limb the ”U” capsuloligamentous suture can be done. ( E and F ) The traction is removed, and the two threads are knotted outside of the joint. The tension of the volar SL joint is checked with the probe.
Scapholunate Volar Capsuloligament Reattachment to Bone
The reattachment of the volar portion is indicated in acute injuries. Unfortunately, early diagnoses are uncommon because most patients are identified as suffering from wrist sprains, which delays the performance of an MRI or/and arthroscopy later than 6 to 8 weeks. However, this condition can be found frequently associated with other lesions such as bone fractures (scaphoid, distal radius, etc.) and perilunate injuries.
-
Step 1: As explained before, the best portal to treat SL volar injuries is the VR portal. 3 However, in perilunate injuries, if the VC portal has been used, the reattachment can be performed through it.
The capsular portal is also performed over the SL joint or in perilunate injuries through the space that appears in consequence of the broken capsule and ligaments ( Fig. 10 ).
Step 2: The anchor should be place around the detachment of the volar ligament if it is observed. Sometimes, if there is a midsubstance injury, or the avulsion is not easily identified, the anchor can be placed either in the lunate or scaphoid bones ( Fig. 11 ).
Step 3: The arthroscope is located in the MCU portal. The technique is the same as described in Fig. 12 . The most important difference to note is that the volar capsule and ligament should be pierced in accordance to where the detachment has occurred. This will make the reattachment in a more anatomically appropriate position ( Figs. 13 and 14 ).
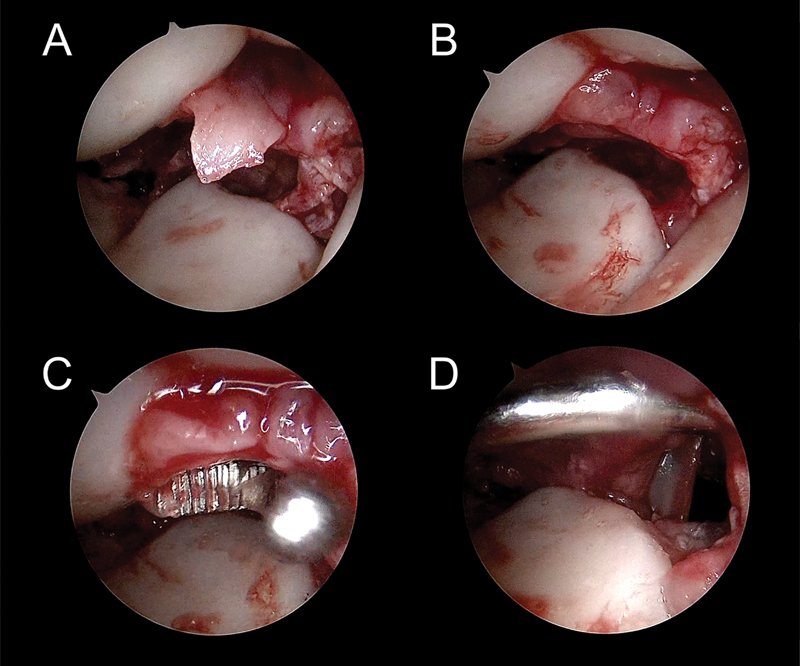
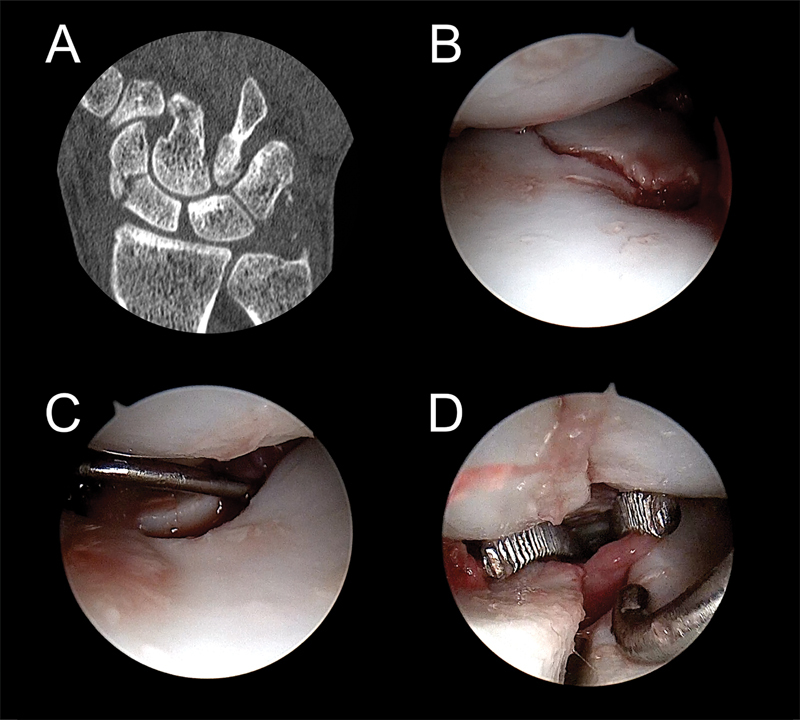
Fig. 10.
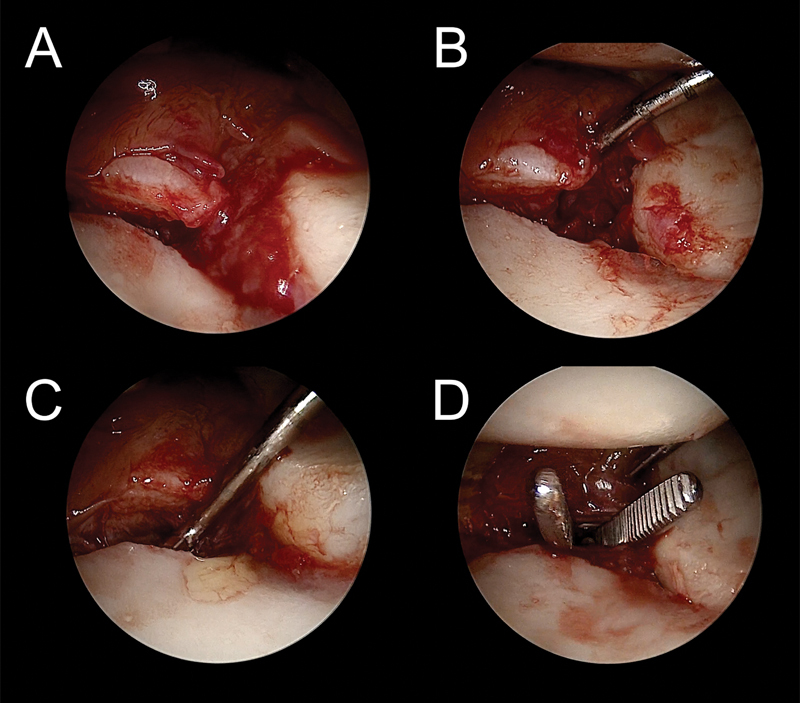
( A–C ) View from the MCU portal. There is an acute injury of the volar portion of the SL ligament, with a small fragment of the volar ulnar corner of the lunate bone. ( D ) The capsular portal is made just over the SL joint, through the tear of the injury.
Fig. 11.
( A ) View from the MCU portal. The hole for the anchor is drilled through the VR portal at the insertion of the ligament on the lunate. ( B and C ) . The anchor is inserted to the bone, then the threads remain in the volar portal.
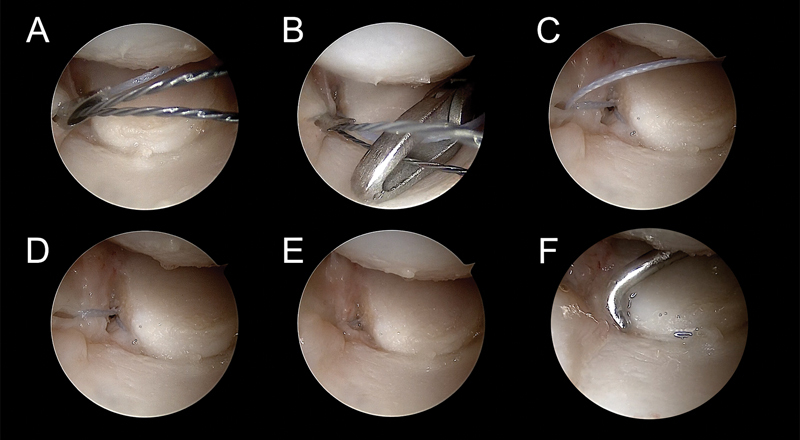
Fig. 12.
( A ) The arthroscope is in the MCU portal. The knot pusher is introduced from the MCR portal. ( B ) It is passed through the VR portal and loaded with the threads of the anchor. ( C ) The threads are retrieved to the MCR portal.
Fig. 13.
( A ) The Abbocath is introduced just over the avulsed fragment. ( B and C ) The loop is captured and taken to the MCR portal, where it is loaded with the first thread. ( D–F ) The loop is recovered to the volar portal along with the first thread, capturing the ulnar portion of the detached ligaments. The first limb of the “U” suture is completed.
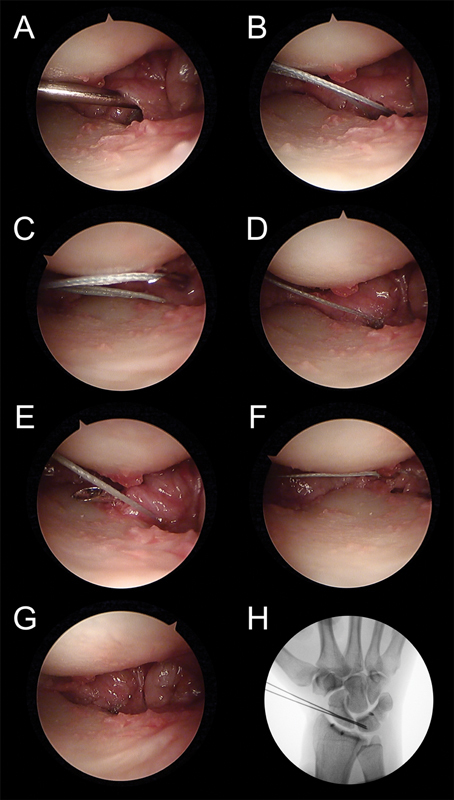
Fig. 14.
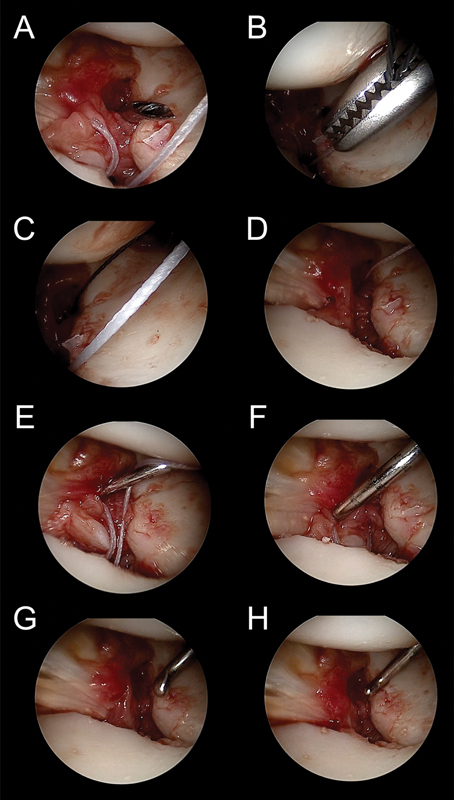
( A ) . The Abbocath pierces the volar ligaments from a more radial position. ( B and C ) The loop is taken to the MCR portal and loaded with the second thread. ( D–F ) The loop and thread are retrieved to the volar portal, so the second limb the “U” is completed. ( G–H ) The two threads are knotted outside of the joint, reattaching the avulsed capsule and ligament to the lunate.
Volar Radiocarpal Ligament Reattachment to Bone
The avulsion of the volar radiocarpal ligaments (radioscaphocapitate, long radiolunate ligament, and short radiolunate ligament) is not a common injury and is found in purely radiocarpal dislocation or dorsal radiocarpal fracture-dislocation.
-
Step 1: If the injury is associated with a distal radius fracture that is going to be fixed with a plate, the volar approach used to fix the fracture and placing the plate can be used for the reattachment. If the injury is a pure radiocarpal dislocation or a small fracture of the radial styloid, the VR portal can be used. 3
As the ligaments are detached from the bone, no capsular portal is needed because the space created between the detached ligament and bone can be used ( Fig. 15 ).
Step 2: Two anchors are usually needed. The position of the anchor and their introduction are visualized directly with the scope placed in the 6R portal ( Fig. 16 ).
Step 3: The arthroscope is maintained in the 6R portal, and the knot pusher is used through the 3/4 portal ( Fig. 16 ). The four sutures should be placed before knotting them; otherwise, it would be more difficult to retrieve the threads as there will be less space between the detached ligaments and bone after knotting the sutures of the first implant. As well, the first knot can be loosened when piercing through the volar ligaments when performing the second suture ( Fig. 17 18 19 ).
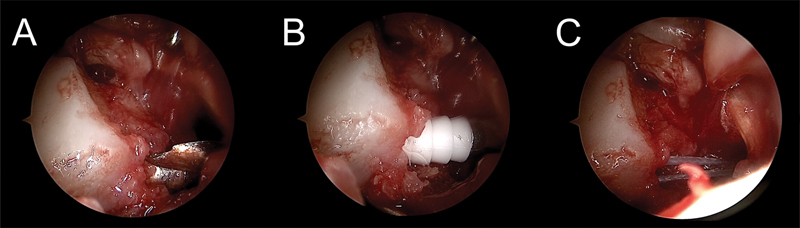
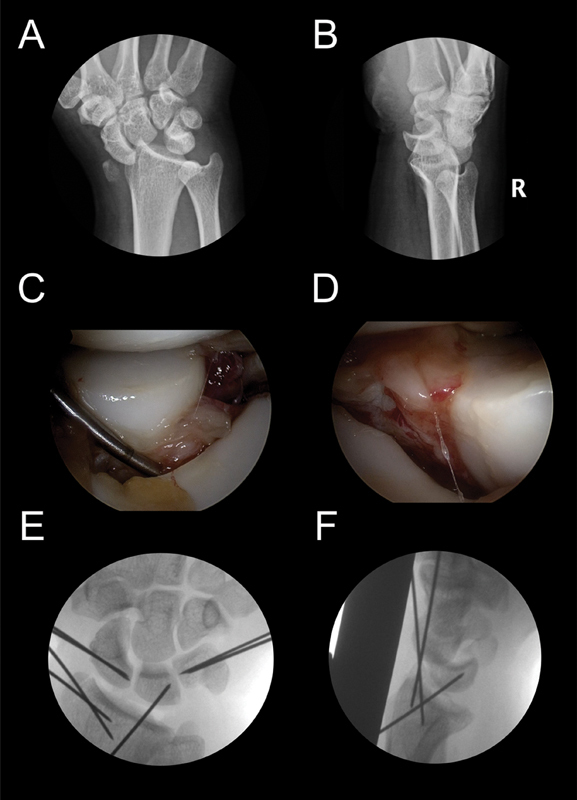
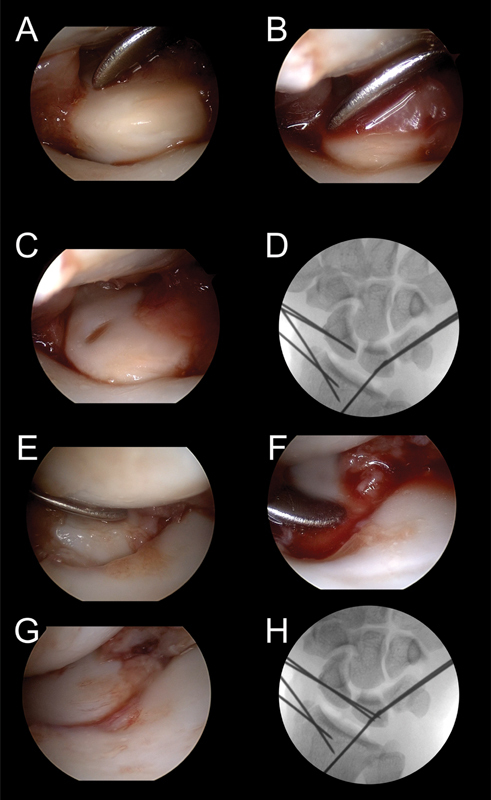
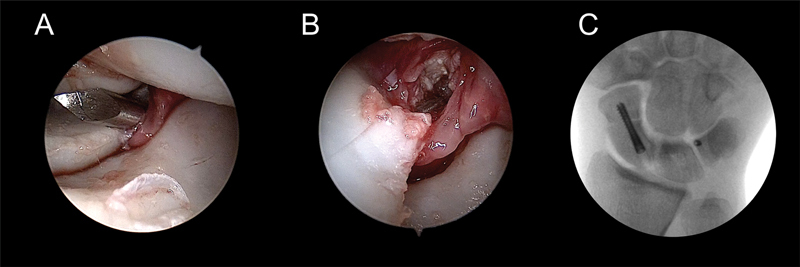
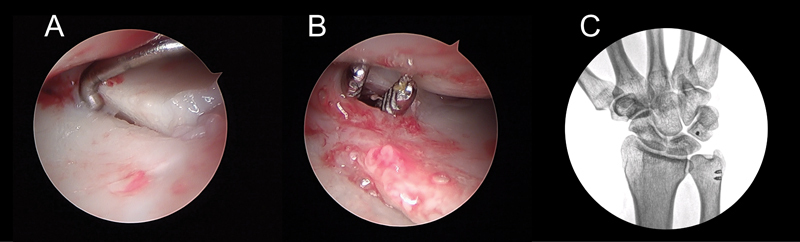
Fig. 15.
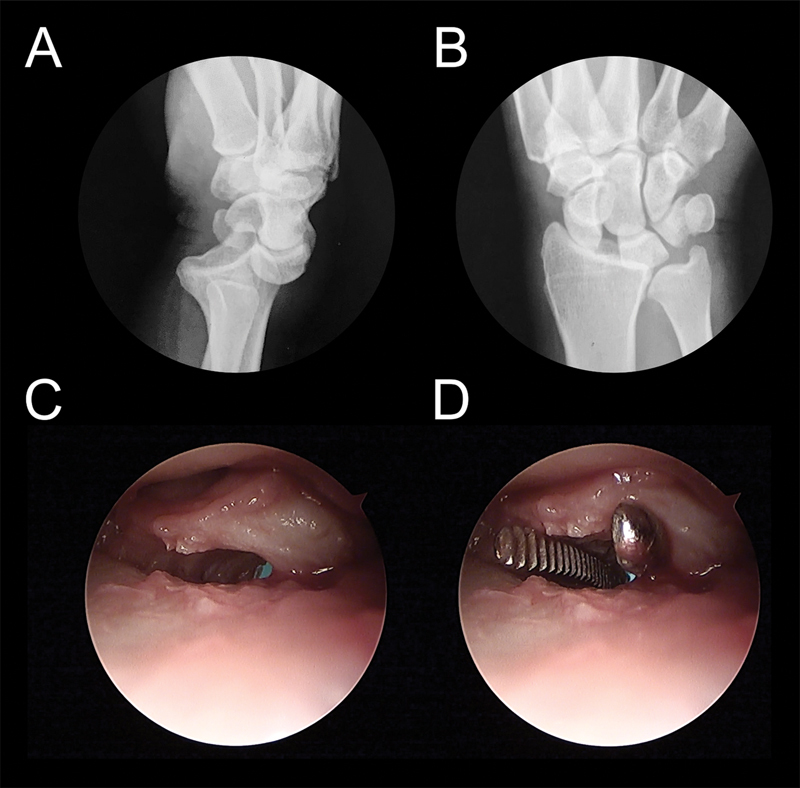
( A and B ) X- rays of a pure radiocarpal dislocation. ( C ) The VR portal is used for the reattachment. ( D ) No capsular portal is needed, because the space between the detached ligament and bone can be used.
Fig. 16.
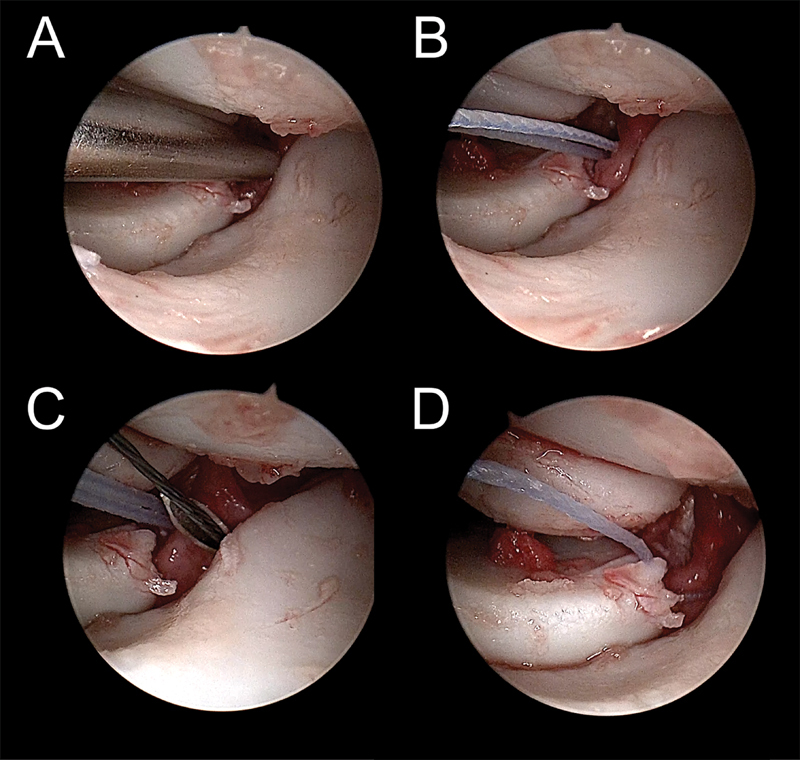
( A ) View from the 6R portal. The hole for the first anchor is drilled through the VR portal in the detached area of the radius. ( B ) The threads remain inside the VR portal. ( C ) The knot pusher is introduced from the 3/4 portal. It is advanced into the VR portal and loaded with the threads of the anchor. ( D ) The threads are retrieved to the 3/4 portal. ( E and F ) The second anchor is placed ulnar to the first one.
Fig. 17.
( A ) The loaded Abbocath pierces the ulnar portion of the volar radiocarpal ligaments (long radiolunate ligament). ( B and C ) The loop is captured and taken to the 3–4 portal, where it is loaded with the first thread. ( D–F ) The loop and thread are recovered to the VR portal. The first limb of the “U” suture of the first anchor is completed.
Fig. 18.
( A and B ) The Abbocath pierces the radiocarpal ligaments in a more radial position. The loop is taken to the 3/4 portal and loaded with the second thread. ( C and D ) The loop and thread are retrieved to the VR portal, so second limb the “U” is completed.
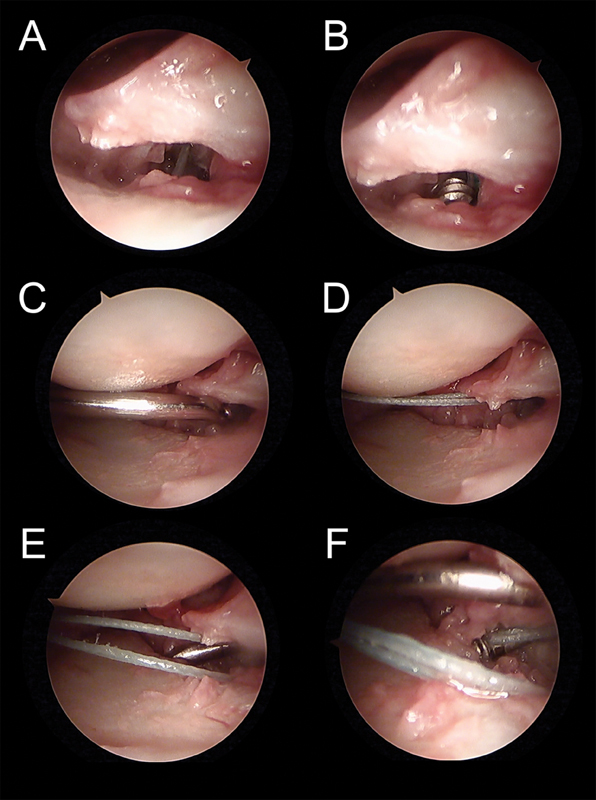
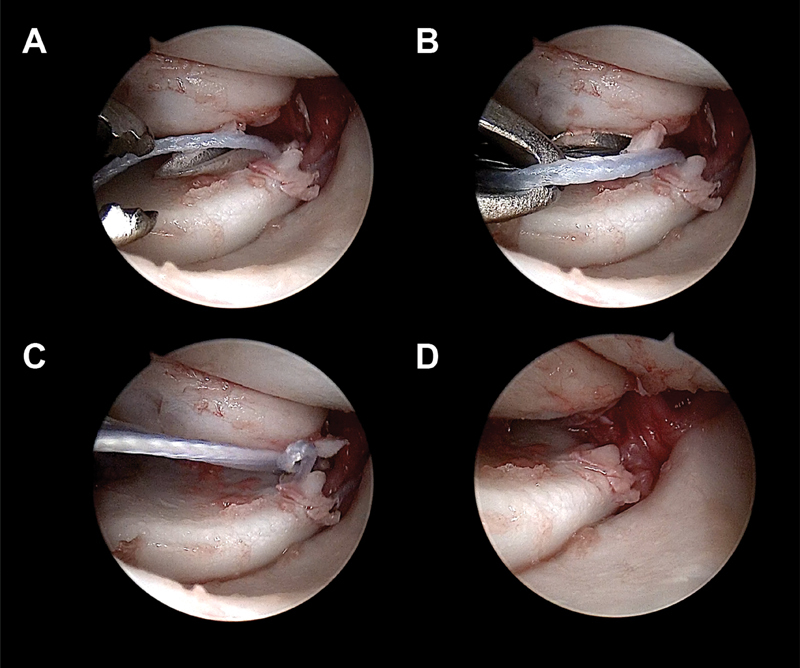
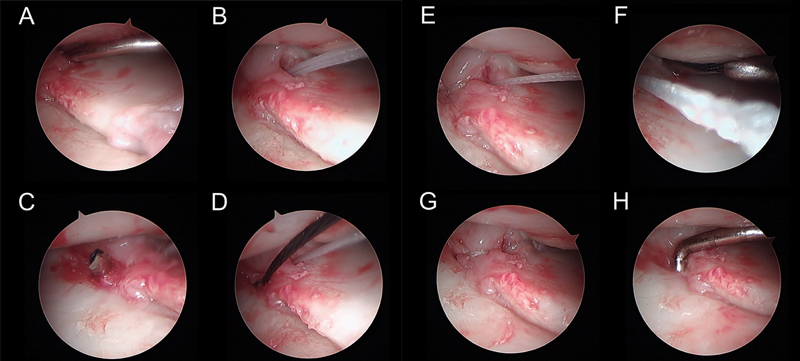
Fig. 19.
( A ) View from the 6R portal of the avulsed radioscaphocapitate ligament. The knot pusher is introduced from the 3/4 portal. It is advanced inside the VR portal and loaded with the threads of the second anchor ( B ) The threads are retrieved to the 3/4 portal. ( C and D ) The Abbocath pierces the ulnar side of the radioscaphocapitate ligament and taken to the 3/4 portal, where it is loaded with the first thread of this implant. The loop and thread are recovered to the VR portal. The first limb of the “U” suture of the second anchor is completed, capturing the ulnar portion of the detached ligament. ( E and F ) The Abbocath pierces the radial part of the ligament and the same procedure is performed to complete the second limb of the “U” suture. ( G ) The four threads are knotted outside of the joint, reattaching the radioscaphocapitate ligament and long radiolunate ligament to the radius. ( H ) X- Ray shows the radial position of the anchors.
The “U” sutures are performed in a horizontal way, trying to capture all the ligaments from the ulnar to the radial side. The knots remain, as in the previous techniques out of the wrist ( Fig. 20 ).
Fig. 20.
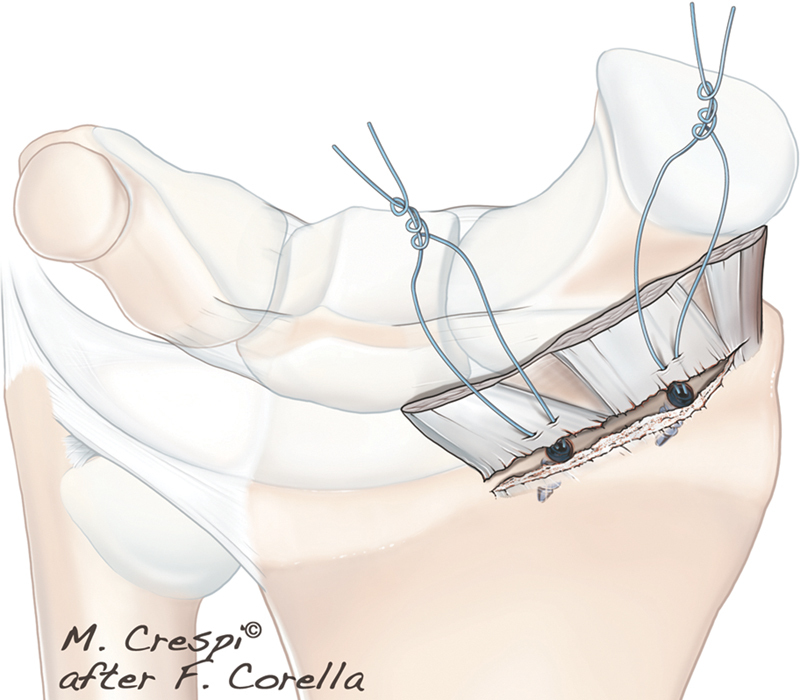
The “U” sutures are performed horizontally with the radiocarpal ligaments from ulnar to radial. The knot remains, as in the previous techniques, outside of the joint.
Traction is released before knotting the sutures and, if necessary, a radiocarpal K-wire is introduced previously to maintain the reduction.
Poirier Space Closure to Bone
In perilunate injuries, the lunate is displaced volar, piercing through the Poirier space. With this technique, the Poirier space and the volar SL and LT ligaments can be repaired through the VC portal.
In this significant instability, the bones must be reduced and stabilized with K-wires; thus the fixation should be done following the placement of the anchors and suture. As it is a complicated procedure that could take some time, the reduction and pinning should be done as fast as possible. We recommend the following technique for the reduction and pinning the bones.
Reduction and pinning the bones in perilunate injuries: The arm is maintained in zenithal traction, and the fluoroscope enters with the C-arm parallel to the floor from the volar side of the wrist. With the suspended hand in pronation or supination, a PA or lateral view are easily obtained.
Two K-wires are introduced under fluoroscopic control into the scaphoid up to the SL joint but without crossing it, and another two in the triquetrum, again up the LT joint. If the lunate is too unstable and the reduction is going to be difficult, another K-wire is introduced from the radius to the lunate, prior to the fixation of the LT or SL joint ( Fig. 21 ).
Fig. 21.
( A and B ) A transstyloid perilunate injury, X-ray view. ( C ) View from the MCU portal of the complete detachment of SL ligament. ( D ) View from the MCR portal of the complete detachment of LT ligament. ( E ) Two K-wires are introduced in the scaphoid up to the SL joint and another two in the triquetrum, again up the LT joint to but not crossing them. ( F ) If the lunate is too unstable, another K-wire is introduced from the radius to the lunate prior to the fixation of the LT or SL joints.
Then, the arthroscope is placed in the MCR portal and a periosteal elevator in the MCU portal. By using this instrument, the gap, rotation, and step-off are reduced. Once a perfect reduction is achieved, the previously placed K-wires are advanced crossing and fixing the joint.
Now, the same maneuver is performed on the opposite site, the arthroscope enters through the MCU portal and the periosteal elevator from the MCR portal, the scaphoid is anatomically reduced, and the K-wires are advanced ( Fig. 22 ).
Fig. 22.
( A ) View from the MCR portal of the LT joint step-off. ( B–D ) With a periosteal elevator introduced from the MCU portal, the anatomical reduction is achieved and the K-wires are advanced crossing and fixing the joint. ( E–H ) The same maneuver is performed on the opposite site, with the arthroscope located in the MCU portal and the periosteal elevator in the MCR portal. The scaphoid is anatomically reduced, and the K-wires are advanced.
If it is a transcaphoperilunate fracture, this reduction is performed in the LT joint first. Once the ulnar side of the wrist is stable, the arthroscope is introduced in the MCU portal, and the arthroscopic reduction of the scaphoid is done.
Step 1: The VC portal is used for this procedure. After performing the approach, as the Poirier space is opened, no capsular portal is needed. For the reattachment only a visualization from the midcarpal joint is needed ( Fig. 23 ).
Step 2: The anchors are placed on the lunate. The introduction of the anchors is directly seen with the arthroscope located in the dorsal portals. The threads exit in the approach of the VC portal ( Fig. 24 ).
Step 3: The arthroscope and knot pusher are introduced from the MCU portal and MCR portal, the threads are recovered to the dorsal side, and the “U” suture is performed in the arcuate ligament in a horizontal manner ( Figs. 25 26 27 28 29 ).
Fig. 23.
( A and B ) View from the MCU portal of the arquate ligament Desinsertion. ( C ) The VC portal is used for this procedure. As the Poirier space is opened, no capsular portal is needed. ( D ) By using the knot pusher the volar portion of the lunate can be seen to facilitate placing the anchor.
Fig. 24.
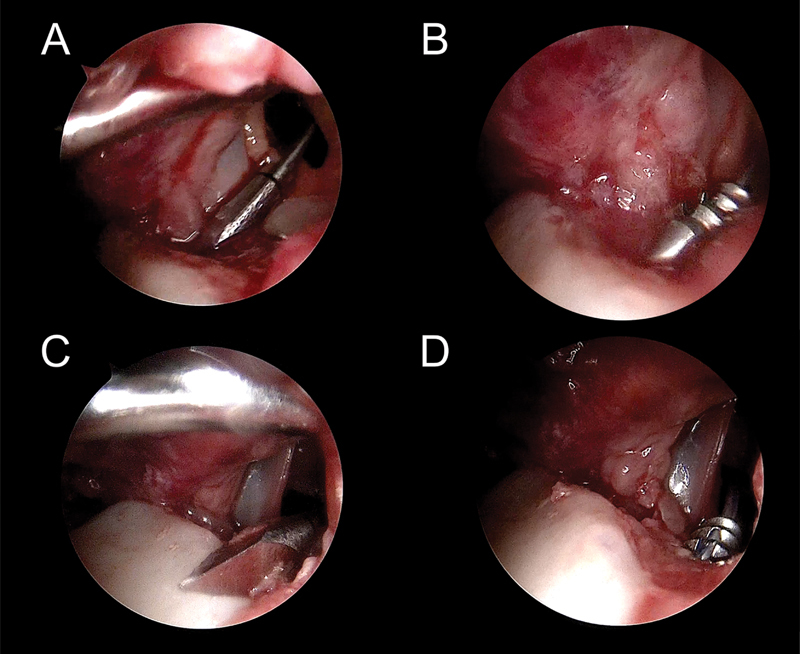
Two anchors are introduced in the lunate through the VC portal. ( A and B ) View from the UCM portal. The first anchor is place in a more radial position. ( C ) The second anchor is separately introduced in a more ulnar position. The four threads remain inside the VC portal.
Fig. 25.
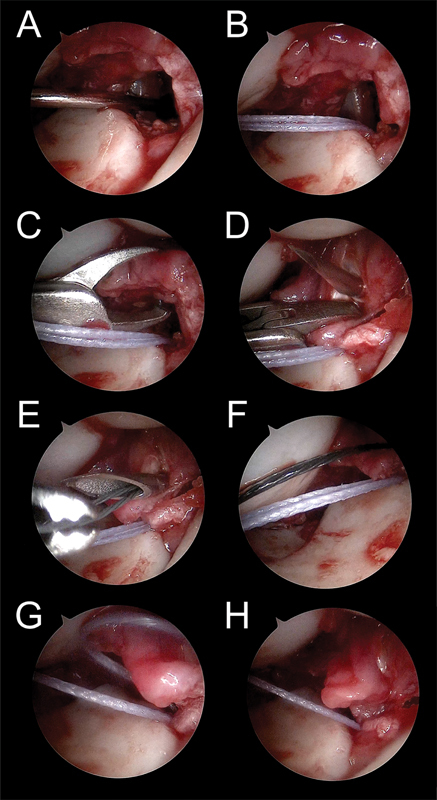
( A and B ) The knot pusher is introduced from the RCM portal. It is advanced inside the VC portal and loaded with the two threads of the first anchor. The threads are retrieved to the RCM portal. ( C and D ) With a grasper the radial portion of the arcuate ligament is capture and pierced with the Abbocath. ( E and F ) The loop is captured and taken to the RCM portal, where it is loaded with the first thread. ( G and H ) The loop and thread are recovered to the VC portal, capturing the ulnar portion of the detached ligaments. The first limb of the “U” suture is completed.
Fig. 26.
The same procedure is performed for the second thread ( A and B ). With the help of the grasper the arcuate ligament is pierced through horizontally ( C and D ). The loop is captured, loaded and taken to the VC portal. The second limb of the “U” suture is completed.
Fig. 27.
The horizontal suture of the second anchor is performed in an ulnar position. ( A–C ) First limb of the “U” suture. ( D–F ) Second limb of the “U” suture.
Fig. 28.
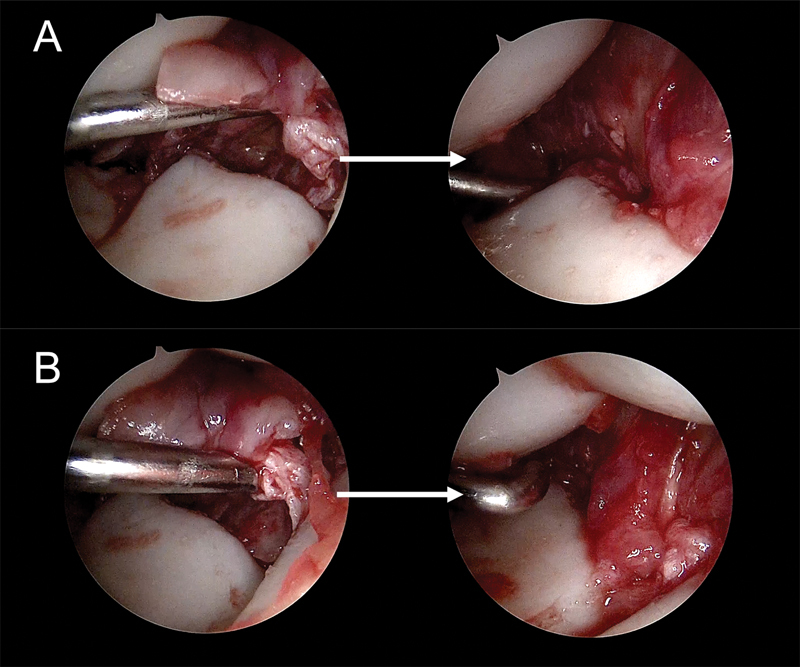
When all the sutures are performed, each anchor are knotted by their respective threads the two threads of each anchor are knotted outside of the joint, reattaching the arcuate ligament. ( A ) Pre- and postview of the radial side of the arcuate ligament. ( B ) Pre- and postview of the ulnar side of the arcuate ligament.
Fig. 29.
The “U” sutures are performed horizontally, trying to capture the arcuate ligament from ulnar to radial. The knot remains, as in the previous techniques, out of the joint, closing the Poirier space.
Lunotriquetral Volar Capsuloligament Reattachment to Bone
Similarly, to SL acute injuries, isolated acute lesions are difficult to diagnose. Normally, they are seen associated with bone fractures. In this technique, the repair of acute LT injures are exposed.
Step 1: The approach of the VU portal or VC portal can be used for the reattachment. The capsular portal is performed over the LT joint or in perilunate injuries through the space that appears consequence of the broken capsule and ligaments ( Fig. 30 ).
Step 2: The anchor is introduced where the detachment has occurred (lunate or triquetrum). As explained before, if K-wires are going to be used, they are placed before introducing the anchor ( Fig. 31 ).
Step 3: The suture is done in the same manner as described earlier ( Figs. 32 33 34 ).
Fig. 30.
( A ) X-ray of a trans-scaphoid perilunate injury. ( B ) Scaphoid fracture, visualized from the MCU portal. ( C ) View from the MCR portal, showing the injury of the volar part of the LT ligament. ( D ) The capsule portal is performed over the LT joint.
Fig. 31.
( A and B ) View from the MCR portal. The anchor is introduced in the triquetrum, the threads remain inside the VU portal. ( C ) X-ray of the scaphoid fixation and the anchor position.
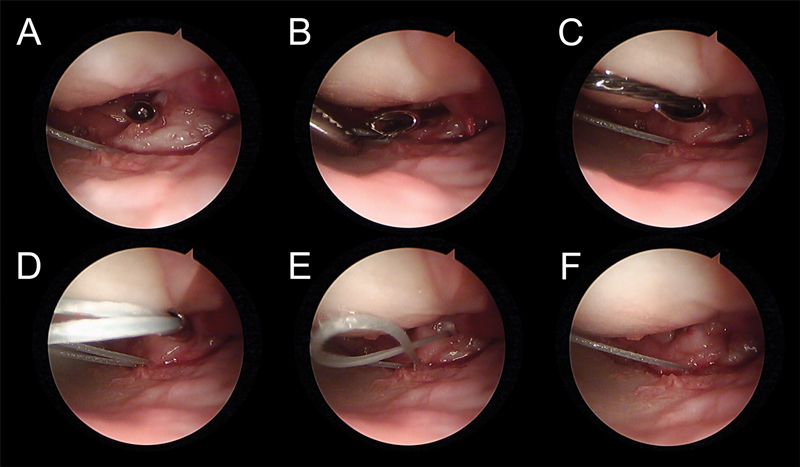
Fig. 32.
( A and B ) The knot pusher is introduced from the UCM portal inside the VU portal. The threads are captured and taken to the UCM portal. ( C ) The Abbocath pierces through the volar capsule and the avulsed LT ligament. ( D ) After retrieving the loaded loop, the first limb of the “U” suture is completed.
Fig. 33.
( A ) The Abbocath is introduced trying to capture as much tissue from the ulnar side of the ligament. ( B ) The loop is captured and loaded with the second thread. ( C ) The loop and thread are recovered to the VU portal, completing the second limb of the “U” suture. ( D ) The two threads are knotted outside of the joint, reattaching the LT ligament and the capsule back to the triquetrum.
Fig. 34.
Volar capsuloligamentous suture of the LT ligament. The sutures pierce through the volar LT ligament and volar capsule along with the ulnocarpal ligaments. The knot remains, as in the previous techniques, outside of the joint.
Lunotriquetral Volar Capsuloligament Reinforcement to Bone
The strongest portion of the LT ligament is the volar portion; therefore, the reinforcement could be done only in the volar side or associated with a reinforcement of the dorsal side.
Step 1: VU portal or VC portal can be used for the reinforcement as explained before ( Fig. 35 ).
Step 2: As usually there is not a clear detachment, the anchor is introduced in the triquetrum bone but can be also placed in the lunate.
Step 3: The suture is done in the same manner as the SL reinforcement ( Fig. 36 ).
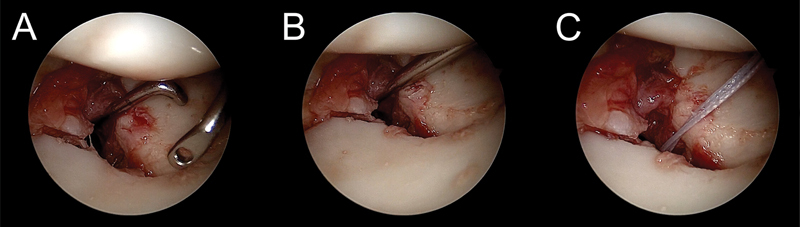
Fig. 35.
( A ) View from the MCR portal. Injury of the volar part of the LT ligament. ( B ) The portal in the capsule is placed just over the LT joint. ( C ) X- ray of the position of the anchor in the triquetrum.
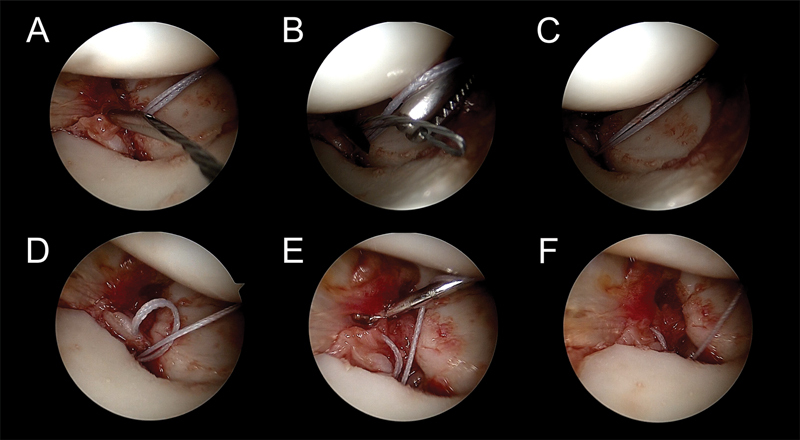
Fig. 36.
( A ) View from the MCR portal. The knot pusher is introduced from the UCM portal and loaded with the threads of the anchor. ( B ) The threads are retrieved to the UCM portal. ( C ) The Abbocath is introduced and pierces the volar capsule and the LT ligament of the radial side. ( D ) The loop is captured and loaded with the first thread. ( E ) The thread is recovered to the VU portal and the first limb of the ”U” suture is completed. ( F and G ) In the same manner, the second limb of the “U” suture is performed on the ulnar side. ( H ) The two threads of the anchor are knotted outside of the joint and the tissue is reinforced to the bone.
Discussion
Already some techniques have been published to perform the reinforcement of the dorsal portion of the SL ligament, the most widespread one is the technique popularized by Mathoulin et al 7 and more recently by Carratalá et al 8 who use an anchor to perform the reinforcement to the bone. However, the injury of the SL goes from volar to dorsal, so many times an isolated rupture of the volar side can be found, (a grade IIIA of the EWAS classification 1 ) or combined with a dorsal injury (a grade IIIC of the EWAS classification 1 ). As far as we know, there is only one arthroscopic technique to perform a volar reinforcement published by del Piñal et al. 9 10 In this technique, an all inside arthroscopic suture of the volar SL ligament and capsule are performed by means of a needle being inserted just ulnar to flexor carpi radialis. The most important difference in the technique presented in this paper is that a bone anchor is used to fix the ligament back to the bone maintaining the knot out of the joint.
Although isolated acute SL ligament injures are diagnosed late, this condition is usually associated with other lesions. In these cases, a repair can be performed. The dorsal portion of the SL ligament is the thickest and the strongest one. 11 12 For this reason, most surgical treatments to repair acute injuries are focused on this portion. Several arthroscopic techniques have been described for the treatment of acute SL ligament injuries such as thermal shrinkage, debridement and reduction, and K-wire fixation. 13 Carratalá et al 8 described an arthroscopic repair of the dorsal portion of the SL ligament using bone anchors associated with a dorsal arthroscopic capsulodesis. As previously mentioned, the only arthroscopic suture of the volar portion of the SL ligament described to date is that described by del Piñal et al, 9 10 this technique is also useful for acute injuries. The presented technique allows a direct repair to the bone of an acute torn volar ligament. It is usually performed along with a dorsal repair (if it is a complete SL injury) and K-wires for stabilizing the SL joint.
In radiocarpal dislocations, there is no standardized surgical treatment because studies have involved only a small number of patients or isolated case reports. 14 In general, there are three recommended principles of treatment: concentric reduction of the radiocarpal joint, identification and treatment of intercarpal injuries, and stable repair of the osseous-ligamentous avulsions. 15 Arthroscopy treatment for radiocarpal dislocations allows a direct visualization of associated bone fractures and ligamentous injuries, to control the reduction and synthesis of fractures as well as to repair ligamentous injuries with the preservation of soft tissues. There are two papers that describe the arthroscopic treatment of a radiocarpal dislocation but none of them perform ligament repair. 16 17 As far as we know, to date, there is no paper describing the arthroscopic repair of the radiocarpal volar ligaments.
The goal of treating any acute carpal dislocation is to obtain an anatomic reduction of carpus. The most widely used method is open reduction, ligament repair, and internal fixation if it is necessary. 18 19 20 21 22 23 A useful alternative to open surgery is arthroscopic reduction and percutaneous fixation, which allows a good visualization of the joint surface and the intra-articular ligaments and avoids adding more damage to the soft tissues. 24 Although several authors have described arthroscopic treatment of these injuries, 24 25 26 27 28 29 30 31 most of them reduce and stabilize the LT and SL joints with percutaneous pinning without repairing the ligaments. 24 26 28 29 Other authors have proposed the dorsal repair of the SL ligament through a miniopen incision with complete tears but they do not mention the repair of volar structures. 27 30 31 del Piñal et al 9 10 proposed performing their arthroscopic volar repair in SL and LT ligament injuries, as well as tears in the Poirier space. In this paper, a technique to repair all the volar structures through the rent of the Poirier space is shown.
Injuries to the LT ligament are less frequent than SL ones. They can appear isolated or associated with a spectrum of injuries, such as radial fractures or perilunate dislocations, and are frequently missed or misdiagnosed. 32 33 There is no consensus about the optimal treatment of LT ligament injuries because most of the surgical treatments are cases series with not enough scientific evidence and mostly are applied in chronic cases. 34 An open repair has been described with complete tears through a dorsal approach using bone anchors or transosseous sutures, 35 36 despite the fact that the thickest and strongest portion of LT ligament is the volar. 37 The arthroscopic treatment of LT ligament injuries include arthroscopic debridement associated or not with K-wire pinning, 38 39 arthroscopic dorsal capsulodesis 40 using the technique described by Mathoulin in SL injuries, 7 and arthroscopic volar capsulodesis by means a plication suture of the ulnocarpal ligaments. 41 As mentioned previously, del Piñal et al 9 10 can be used to repair LT injuries as well.
Footnotes
Conflict of Interest None declared.
References
- 1.Messina J C, Van Overstraeten L, Luchetti R, Fairplay T, Mathoulin C L. The EWAS classification of scapholunate tears: an anatomical arthroscopic study. J Wrist Surg. 2013;2(02):105–109. doi: 10.1055/s-0033-1345265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Luchetti R, Corella F. 1st ed. Thieme; 2023. The “4R” Algorithm of Treatment; pp. 97–102. [Google Scholar]
- 3.Slutsky D J. Wrist arthroscopy through a volar radial portal. Arthroscopy. 2002;18(06):624–630. doi: 10.1053/jars.2002.34106. [DOI] [PubMed] [Google Scholar]
- 4.Corella F, Ocampos M, Cerro M D, Larrainzar-Garijo R, Vázquez T. Volar central portal in wrist arthroscopy. J Wrist Surg. 2016;5(01):80–90. doi: 10.1055/s-0035-1570741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Slutsky D J. The use of a volar ulnar portal in wrist arthroscopy. Arthroscopy. 2004;20(02):158–163. doi: 10.1016/j.arthro.2003.11.015. [DOI] [PubMed] [Google Scholar]
- 6.del Piñal F, García-Bernal F J, Pisani D, Regalado J, Ayala H, Studer A. Dry arthroscopy of the wrist: surgical technique. J Hand Surg Am. 2007;32(01):119–123. doi: 10.1016/j.jhsa.2006.10.012. [DOI] [PubMed] [Google Scholar]
- 7.Mathoulin C L, Dauphin N, Wahegaonkar A L.Arthroscopic dorsal capsuloligamentous repair in chronic scapholunate ligament tears Hand Clin 20112704563–572., xi [DOI] [PubMed] [Google Scholar]
- 8.Carratalá V, Lucas F J, Miranda I, Sánchez Alepuz E, González Jofré C. Arthroscopic scapholunate capsuloligamentous repair: suture with dorsal capsular reinforcement for scapholunate ligament lesion. Arthrosc Tech. 2017;6(01):e113–e120. doi: 10.1016/j.eats.2016.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.del Piñal F, Studer A, Thams C, Glasberg A. An all-inside technique for arthroscopic suturing of the volar scapholunate ligament. J Hand Surg Am. 2011;36(12):2044–2046. doi: 10.1016/j.jhsa.2011.09.021. [DOI] [PubMed] [Google Scholar]
- 10.del Piñal F. Arthroscopic volar capsuloligamentous repair. J Wrist Surg. 2013;2(02):126–128. doi: 10.1055/s-0033-1343016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Berger R A. The gross and histologic anatomy of the scapholunate interosseous ligament. J Hand Surg Am. 1996;21(02):170–178. doi: 10.1016/S0363-5023(96)80096-7. [DOI] [PubMed] [Google Scholar]
- 12.Sokolow C, Saffar P. Anatomy and histology of the scapholunate ligament. Hand Clin. 2001;17(01):77–81. [PubMed] [Google Scholar]
- 13.Bednar J M. Acute scapholunate ligament injuries: arthroscopic treatment. Hand Clin. 2015;31(03):417–423. doi: 10.1016/j.hcl.2015.04.001. [DOI] [PubMed] [Google Scholar]
- 14.Mourikis A, Rebello G, Villafuerte J, Moneim M, Omer G E, Jr, Veitch J.Radiocarpal dislocations: review of the literature with case presentations and a proposed treatment algorithm Orthopedics 20083104386–392., quiz 393–394 [DOI] [PubMed] [Google Scholar]
- 15.Ilyas A M, Mudgal C S. Radiocarpal fracture-dislocations. J Am Acad Orthop Surg. 2008;16(11):647–655. doi: 10.5435/00124635-200811000-00005. [DOI] [PubMed] [Google Scholar]
- 16.Kamal R N, Bariteau J T, Beutel B G, DaSilva M F. Arthroscopic reduction and percutaneous pinning of a radiocarpal dislocation: a case report. J Bone Joint Surg Am. 2011;93(15):e84. doi: 10.2106/JBJS.J.01306. [DOI] [PubMed] [Google Scholar]
- 17.Hardy P, Welby F, Stromboni M, Blin J L, Lortat-Jacob A, Benoit J. Wrist arthroscopy and dislocation of the radiocarpal joint without fracture. Arthroscopy. 1999;15(07):779–783. doi: 10.1016/s0749-8063(99)70014-9. [DOI] [PubMed] [Google Scholar]
- 18.Kremer T, Wendt M, Riedel K, Sauerbier M, Germann G, Bickert B. Open reduction for perilunate injuries—clinical outcome and patient satisfaction. J Hand Surg Am. 2010;35(10):1599–1606. doi: 10.1016/j.jhsa.2010.06.021. [DOI] [PubMed] [Google Scholar]
- 19.Budoff J E. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008;33(08):1424–1432. doi: 10.1016/j.jhsa.2008.07.016. [DOI] [PubMed] [Google Scholar]
- 20.Herzberg G. Perilunate and axial carpal dislocations and fracture-dislocations. J Hand Surg Am. 2008;33(09):1659–1668. doi: 10.1016/j.jhsa.2008.09.013. [DOI] [PubMed] [Google Scholar]
- 21.Herzberg G, Forissier D. Acute dorsal trans-scaphoid perilunate fracture-dislocations: medium-term results. J Hand Surg [Br] 2002;27(06):498–502. doi: 10.1054/jhsb.2002.0774. [DOI] [PubMed] [Google Scholar]
- 22.Cooney W P, Bussey R, Dobyns J H, Linscheid R L. Difficult wrist fractures. Perilunate fracture-dislocations of the wrist. Clin Orthop Relat Res. 1987;214(214):136–147. [PubMed] [Google Scholar]
- 23.Minami A, Kaneda K. Repair and/or reconstruction of scapholunate interosseous ligament in lunate and perilunate dislocations. J Hand Surg Am. 1993;18(06):1099–1106. doi: 10.1016/0363-5023(93)90410-5. [DOI] [PubMed] [Google Scholar]
- 24.Park M J, Ahn J H. Arthroscopically assisted reduction and percutaneous fixation of dorsal perilunate dislocations and fracture-dislocations. Arthroscopy. 2005;21(09):1153. doi: 10.1016/j.arthro.2005.06.010. [DOI] [PubMed] [Google Scholar]
- 25.Liu B, Chen S L, Zhu J, Tian G L. Arthroscopic management of perilunate injuries. Hand Clin. 2017;33(04):709–715. doi: 10.1016/j.hcl.2017.06.002. [DOI] [PubMed] [Google Scholar]
- 26.Kim J P, Lee J S, Park M J. Arthroscopic reduction and percutaneous fixation of perilunate dislocations and fracture-dislocations. Arthroscopy. 2012;28(02):196–20300. doi: 10.1016/j.arthro.2011.08.299. [DOI] [PubMed] [Google Scholar]
- 27.Liu B, Chen S L, Zhu J, Wang Z X, Shen J. Arthroscopically assisted mini-invasive management of perilunate dislocations. J Wrist Surg. 2015;4(02):93–100. doi: 10.1055/s-0035-1550162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jeon I H, Kim H J, Min W K, Cho H S, Kim P T. Arthroscopically assisted percutaneous fixation for trans-scaphoid perilunate fracture dislocation. J Hand Surg Eur Vol. 2010;35(08):664–668. doi: 10.1177/1753193410375781. [DOI] [PubMed] [Google Scholar]
- 29.Oh W T, Choi Y R, Kang H J, Koh I H, Lim K H. Comparative outcome analysis of arthroscopic-assisted versus open reduction and fixation of trans-scaphoid perilunate fracture dislocations. Arthroscopy. 2017;33(01):92–100. doi: 10.1016/j.arthro.2016.07.018. [DOI] [PubMed] [Google Scholar]
- 30.Weil W M, Slade J F, III, Trumble T E. Open and arthroscopic treatment of perilunate injuries. Clin Orthop Relat Res. 2006;445(445):120–132. doi: 10.1097/01.blo.0000205889.11824.03. [DOI] [PubMed] [Google Scholar]
- 31.Herzberg G, Burnier M, Marc A, Merlini L, Izem Y. The role of arthroscopy for treatment of perilunate injuries. J Wrist Surg. 2015;4(02):101–109. doi: 10.1055/s-0035-1550344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mayfield J K, Johnson R P, Kilcoyne R K. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980;5(03):226–241. doi: 10.1016/s0363-5023(80)80007-4. [DOI] [PubMed] [Google Scholar]
- 33.Fowler T P. Intercarpal ligament injuries associated with distal radius fractures. J Am Acad Orthop Surg. 2019;27(20):e893–e901. doi: 10.5435/JAAOS-D-18-00503. [DOI] [PubMed] [Google Scholar]
- 34.van de Grift T C, Ritt M JPF. Management of lunotriquetral instability: a review of the literature. J Hand Surg Eur Vol. 2016;41(01):72–85. doi: 10.1177/1753193415595167. [DOI] [PubMed] [Google Scholar]
- 35.Shin A Y, Weinstein L P, Berger R A, Bishop A T. Treatment of isolated injuries of the lunotriquetral ligament. A comparison of arthrodesis, ligament reconstruction and ligament repair. J Bone Joint Surg Br. 2001;83(07):1023–1028. doi: 10.1302/0301-620x.83b7.11413. [DOI] [PubMed] [Google Scholar]
- 36.Reagan D S, Linscheid R L, Dobyns J H. Lunotriquetral sprains. J Hand Surg Am. 1984;9(04):502–514. doi: 10.1016/s0363-5023(84)80101-x. [DOI] [PubMed] [Google Scholar]
- 37.Ritt M JPF, Bishop A T, Berger R A, Linscheid R L, Berglund L J, An K N. Lunotriquetral ligament properties: a comparison of three anatomic subregions. J Hand Surg Am. 1998;23(03):425–431. doi: 10.1016/S0363-5023(05)80460-5. [DOI] [PubMed] [Google Scholar]
- 38.Badia A, Khanchandani P. The floating lunate: arthroscopic treatment of simultaneous complete tears of the scapholunate and lunotriquetral ligaments. Hand (N Y) 2009;4(03):250–255. doi: 10.1007/s11552-008-9155-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Henry M. Arthroscopic treatment of acute scapholunate and lunotriquetral ligament injuries. Oper Tech Orthop. 2003;13(01):48–55. [Google Scholar]
- 40.Acar M A, Özdemir A, Eravsar E. Arthroscopic dorsal capsulodesis for isolated lunotriquetral interosseous ligament injuries. J Hand Surg Eur Vol. 2021;46(05):510–515. doi: 10.1177/1753193420983687. [DOI] [PubMed] [Google Scholar]
- 41.Moskal M J, Savoie F H, III, Field L D.Arthroscopic capsulodesis of the lunotriquetral joint Clin Sports Med 20012001141–153., ix–x [DOI] [PubMed] [Google Scholar]