

Abstract
Mesenteric cysts, typically benign and asymptomatic, are incidental findings during abdominal investigations for nonspecific symptoms. Their origin is commonly in the mesentery of the small bowel, mesocolon, or retroperitoneum. This paper reports a rare case of a 22-year-old male with a mesenteric cyst presenting as a right lower abdominal mass. Ultrasonography revealed a heterogenous collection, leading to surgical excision. Histopathology unexpectedly revealed an extragonadal yolk sac tumor (YST) originating in the mesentery, a rarity often misdiagnosed as a cyst. YST, primarily found in gonads, is infrequently reported extragonadally. This study contributes to the limited literature on primary peritoneal YST, discussing clinicopathological parameters and presenting a detailed case. The pathogenesis of extragonadal germ cell tumors, including YST, remains debated, with migration and stagnation of germ cells during embryonic development proposed as a prevalent theory. Histopathological examination of extragonadal YST mirrors gonadal YST, featuring various patterns. Immunohistochemistry, crucial for diagnosis, reveals positive expression for SALL-4, glypican-3, PLAP, AFP, and panCK. SALL-4 emerges as the most sensitive marker for extragonadal YST. This case underscores the importance of accurate postoperative histopathology and immunohistochemistry in distinguishing mesenteric YST from cysts, as misdiagnosis can impact prognosis. The rarity of extragonadal YST emphasizes the need for comprehensive understanding and recognition in clinical practice. The study contributes valuable insights into diagnosis and management, shedding light on a challenging aspect of surgical pathology.
Keywords: Excision surgery, Mesenteric cyst, Histopathology, Malignant, Yolk sac tumor
Introduction
Mesenteric cysts are typically uncommon, benign lesions that are often asymptomatic. They are frequently discovered incidentally during investigations for nonspecific abdominal symptoms [1]. Previous studies have reported an incidence of one case per 250,000 admissions. The mesentery of the small bowel, followed by the mesocolon and retroperitoneum, is the most common site of origin for these cysts [2]. They can manifest as single or multiple cysts, either unilocular or multilocular, containing serous, purulent, chylous, or hemorrhagic fluid. Various theories, such as infection, trauma, and inadequate lymphatic flow, have been proposed to explain the pathogenesis of these lesions. Malignant transformation has been documented in only 3% of cases. Surgical resection is the preferred treatment option due to the excellent prognosis and very low risk of recurrence [3].
Case Report
A 22-year-old unmarried male presented at our hospital with a 4-month history of right-sided lower abdominal swelling accompanied by mild pain. The swelling gradually increased in size, and the patient reported no associated fever, nausea, vomiting, bladder/bowel issues, hematemesis, or abdominal trauma. Upon clinical examination, the patient was conscious with stable vital signs. While no ascites was observed, a mobile non-tender mass measuring 8 × 6 cm was palpated in the right lower abdomen. The overlying skin appeared normal with no dilated veins. Digital rectal examination and palpation revealed no abnormal masses or lymphadenopathy. Routine blood investigations yielded normal results.
Whole abdomen ultrasonography revealed a heterogeneous hypoechoic collection with septations in the right iliac fossa, measuring approximately 10 × 6 × 5 cm, suggesting a mesenteric cyst. The bilateral testis was found to be unremarkable. The mass, along with mesenteric fat and a small bowel segment, was excised and sent for histopathology (Fig. 1).
Fig. 1.
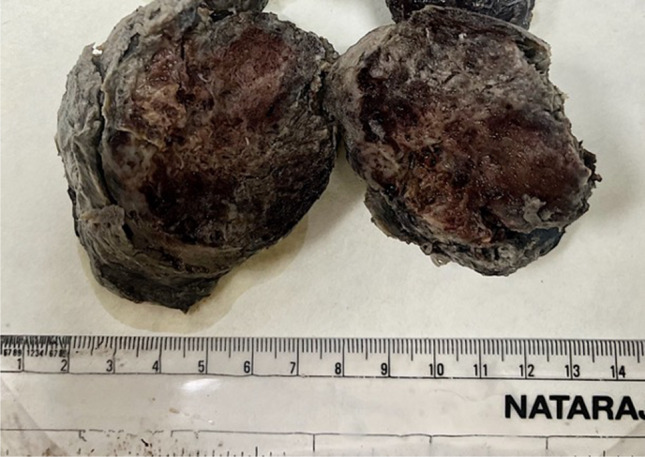
Cut surface of the mass showed a solid cystic lesion with areas of hemorrhage and necrosis
The gross examination of the received specimen showed a grayish-brown mass measuring 12 × 8 × 5 cm. The cut surface exhibited solid features with cystic changes, focal hemorrhage, and necrosis.
Microscopic examination of multiple hematoxylin-and-eosin-stained sections revealed a tumor arranged in nests, sheets, papillae, and a microcystic pattern. Schiller-Duval bodies and areas of necrosis were occasionally identified. Individual cells displayed moderate pleomorphism with vacuolated to eosinophilic cytoplasm, enlarged nuclei, and prominent nucleoli. Atypical mitoses were also observed. The attached bowel segment appeared unremarkable (Fig. 2a–e ).
Fig. 2.

Histopathological and immunohistochemical findings. a–e Hematoxylin-and-eosin-stained sections show a partly encapsulated (a) tumor exhibiting a myriad of patterns including sheets (b), microcystic (c), endodermal sinus (d), and papillae (e) [× 10 magnification]. f–h Hematoxylin-and-eosin-stained sections show tumor cells exhibiting moderate pleomorphism with vacuolated to eosinophilic cytoplasm. Few atypical mitoses are also observed [× 40 magnification]. i–l Immunohistochemistry showing tumor cells positive for SALL-4, AFP, PLAP, and MOC-31 confirming the diagnosis of yolk sac tumor [× 40 magnification]
Immunohistochemistry analysis indicated positive expression for PLAP, SALL-4, and AFP in the tumor cells, with focal positivity for CD-117. However, they were negative for CK7, CK-20, CDX-2, calretinin, vimentin, WT-1, CD-30, inhibin, and HMB-45 (Fig. 2i–l).
Based on the morphological and immunohistochemical findings, a final diagnosis of extragonadal yolk sac tumor arising from the mesentery was established. The patient is currently on a 6-month follow-up with no evidence of disease.
Discussion
Yolk sac tumor (YST) manifests as a malignant germ cell tumor predominantly found in gonads [4]. When occurring outside gonadal sites, particularly in the peritoneum, it constitutes a rare malignancy. Previous reports have documented instances of primary peritoneal YST arising from the omentum and mesentery [5], and the clinicopathological details of such cases are compiled in Table 1.
Table 1.
The clinicopathological features of previously reported cases of extragonadal yolk sac tumor
| Author | Age and sex | Primary site | FIGO stage | Histologic type | Follow-up |
|---|---|---|---|---|---|
| Jones et al. [11] | 2, M | Mesentery | 4 | YST | NED |
| 17, M | Mesentery | NA | YST | NR | |
| Tangour-Bouaicha et al. [12] | 16, F | Mesentery | 4 | YST | NED |
| Park et al. [6] | 45, F | Omentum | NA | YST | NED |
| Xinghui et al. [13] | 3, M | Omentum | NA | YST | NR |
| Geminiani et al. [7] | 46, F | Omentum | NA | YST | NED |
| Kim et al. [14] | 37, F | Omentum | NA | YST | NED |
| Dulger et al. [15] | 19, M | Omentum | NA | YST | Died of cardiac arrest |
| Harano et al. [16] | 35, M | Omentum | NA | YST | NED |
| Present case | 22, M | Mesentery | - | YST | NED |
NR, not reported; NED, no evidence of disease; NA, not available; YST, yolk sac tumor
The etiology and pathogenesis of peritoneal YST, akin to other extragonadal locations, remain subjects of debate. Various theories, such as those concerning the migration and stagnation of germ cells during embryonic development, have been postulated for the pathogenesis of extragonadal germ cell tumors [6, 7]. According to the prevailing theory, primitive gonads migrate from the yolk sac to the posterior peritoneal genital ridge, and the malignant transformation of these displaced germ cells can result in primary extragonadal germ cell tumors.
The International Germ Cell Cancer Collaborative Group (IGCCCG) has proposed a widely accepted classification for treating metastatic germ cell tumors. This classification categorizes patients into groups with good, intermediate, and poor prognoses based on factors such as the primary tumor site, serum lactate dehydrogenase (LDH) levels, pretreatment tumor marker levels (AFP and beta-human chorionic gonadotropin), and disease severity [8].
Histopathological examination reveals that the features of extragonadal YST closely resemble their gonadal counterparts, exhibiting various patterns. The microcystic pattern, characterized by a loose reticular architecture wherein tumor cells form tubular structures with cystic spaces, is the most prevalent. Other patterns include pseudopapillary, glandular, endodermal sinus, hepatoid, and solid [4, 5]. Although Schiller-Duvall bodies are characteristic of YST, they are observed in only 50% of cases [9]. Immunohistochemistry plays a crucial role in confirming YST diagnosis, with positive expressions for SALL-4, glypican-3, PLAP, AFP, and panCK. SALL4, exhibiting 100% sensitivity, emerges as the most sensitive marker for diagnosing extragonadal YST, surpassing the sensitivity of PLAP, AFP, or glypican-3. These antibodies also aid in differentiating between YST and clear cell carcinoma [10].
Conclusion
In summary, this study revealed an unusual manifestation of a yolk sac tumor (YST) originating in the retroperitoneum, initially misdiagnosed as a mesenteric cyst on radiological examination. YST is an exceptionally rare malignant tumor associated with a grim prognosis. Hence, it is crucial to differentiate it accurately from a mesenteric cyst to positively impact patient outcomes. Postoperative histopathology and immunohistochemistry emerge as essential gold standards, playing a pivotal role in diagnosing mesenteric yolk sac tumors and distinguishing them from mesenteric cysts.
Author Contribution
SA and SZ were responsible for reporting the case. All authors contributed equally to the literature review, drafting, and critically revising the final version of the manuscript. All authors approved the final version of the manuscript.
Data Availability
No additional data generated in the case report.
Declarations
Ethics Approval and Consent to Participate
Not applicable because this article does not contain any studies with human or animal subjects.
Consent for Publication
Informed consent was sought from patient regarding participation and publication.
Competing Interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Miliaras S, Trygonis S, Papandoniou A, Kalamaras S, Trygonis C, Kiskinis D. Mesenteric cyst of the descending colon: report of a case. Acta Chir Belg. 2006;106:714–716. doi: 10.1080/00015458.2006.11679990. [DOI] [PubMed] [Google Scholar]
- 2.Saviano MS, Fundarò S, Gelmini R, Begossi G, Perrone S, Farinetti A, et al. Mesenteric cystic neoformation: report of two cases. Surg Today. 1999;29:174–177. doi: 10.1007/BF02482245. [DOI] [PubMed] [Google Scholar]
- 3.Kurtz RJ, Heimann TM, Beck AR, Holt J. Mesenteric and retroperitoneal cysts. Ann Surg. 1986;203:109. doi: 10.1097/00000658-198601000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kurman RJ, Norris HJ. Endodermal sinus tumor of the ovary: a clinical and pathologic analysis of 71 cases. Cancer. 1976;38:2404–2419. doi: 10.1002/1097-0142(197612)38:6<2404::AID-CNCR2820380629>3.0.CO;2-3. [DOI] [PubMed] [Google Scholar]
- 5.Zhou X, Zhao L, Feng X, Pan Z, Bin Y, Zhang S, et al. Relapsed and refractory yolk sac tumor of the peritoneum (mesentery): a case report and literature review. Front Oncol. 2022;12:928234. doi: 10.3389/fonc.2022.928234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Park NH, Ryu SY, Park IA, Kang SB, Lee HP. Primary endodermal sinus tumor of the omentum. Gynecol Oncol. 1999;72:427–430. doi: 10.1006/gyno.1998.5268. [DOI] [PubMed] [Google Scholar]
- 7.Geminiani ML, Panetta A, Pajetta V, Bacci F, Negri L, Maccaferri R, et al. Endodermal sinus tumor of the omentum: case report. Tumori. 2005;91:563–566. doi: 10.1177/030089160509100620. [DOI] [PubMed] [Google Scholar]
- 8.Beyer J, Collette L, Sauve N, Daugaard G, Feldman DR, Tandstad T, et al. Survival and new prognosticators in metastatic seminoma: results from the IGCCCG-update consortium. J Clin Oncol. 2021;39:1553–1562. doi: 10.1200/JCO.20.03292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ronchi A, Cozzolino I, Montella M, Panarese I, Zito Marino F, Rossetti S, et al. Extragonadal germ cell tumors: not just a matter of location. a review about clinical, molecular and pathological features. Cancer Med. 2019;8:6832–40. doi: 10.1002/cam4.2195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cao D, Guo S, Allan RW, Molberg KH, Peng Y. SALL4 is a novel sensitive and specific marker of ovarian primitive germ cell tumors and is particularly useful in distinguishing yolk sac tumor from clear cell carcinoma. Am J Surg Pathol. 2009;33:894–904. doi: 10.1097/PAS.0b013e318198177d. [DOI] [PubMed] [Google Scholar]
- 11.Jones MA, Clement PB, Young RH. Primary yolk sac tumors of the mesentery. A report of two cases. Am J Clin Pathol. 1994;101:42–7. doi: 10.1093/ajcp/101.1.42. [DOI] [PubMed] [Google Scholar]
- 12.Tangour-Bouaicha M, Bel Haj Salah M, Ben Brahim E, Ben Othmène M, Douggaz A, Sassi S, et al. Primary peritoneal yolk sac tumour. A case report. Ann Pathol. 2010;30:378–81. doi: 10.1016/j.annpat.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 13.Xinghui Y, Jing H, Mingju L, Weizhong G. Endodermal sinus tumour of the omentum in a child. Pediatr Radiol. 2004;34:985–987. doi: 10.1007/s00247-004-1240-6. [DOI] [PubMed] [Google Scholar]
- 14.Kim SW, Park JH, Lim MC, Park JY, Yoo CW, Park SY. Primary yolk sac tumor of the omentum: a case report and review of the literature. Arch Gynecol Obstet. 2009;279:189–192. doi: 10.1007/s00404-008-0661-0. [DOI] [PubMed] [Google Scholar]
- 15.Dulger AC, Begenik H, Esen R, Rafet M. Endodermal sinus tumor presented with ascites: a case report. Gastroenterol Res. 2012;5:127–129. doi: 10.4021/gr406w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harano K, Ando M, Sasajima Y, Yunokawa M, Yonemori K, Shimizu C, et al. Primary yolk sac tumor of the omentum: a case report and literature review. Case Rep Oncol. 2012;5:671–675. doi: 10.1159/000337281. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No additional data generated in the case report.