Diagnosis: Pigmented disseminated superficial actinic porokeratosis
Porokeratosis is a benign neoplastic disorder of keratinization characterized by a clonal proliferation of epidermal keratinocytes. The pathway that leads to the abnormal proliferation of keratinocytes is unknown. A variety of causal factors have been proposed, including genetic susceptibility, ultraviolet radiation, viral infections and immunosuppression (1, 2).
Multiple clinical variants of porokeratosis have been described.
Disseminated superficial actinic porokeratosis (DSAP) is the most common type of porokeratosis. DSAP typically occurs in the third or fourth decade of life, with an estimated female to male ratio of 1.8:1 (3). Patients frequently report a history of chronic sun exposure, supporting the role of ultraviolet radiation as one of the main aetiopathogenetic factors.
In recent years, a rare distinct variant of DSAP has been described, which is represented by pigmented disseminated superficial actinic porokeratosis (4–6).
DSAP is clinically characterized by skin-coloured, annular atrophic macules/plaques, 5–10 mm in size, surrounded by a peripheral hyperkeratotic ridge-like border. The distribution of lesions usually involves sun-exposed sites, such as the extensor surfaces of the arms, legs, back and shoulders, with sparing of the palms and soles, whereas facial lesions occur in approximately 15% of patients (4, 5).
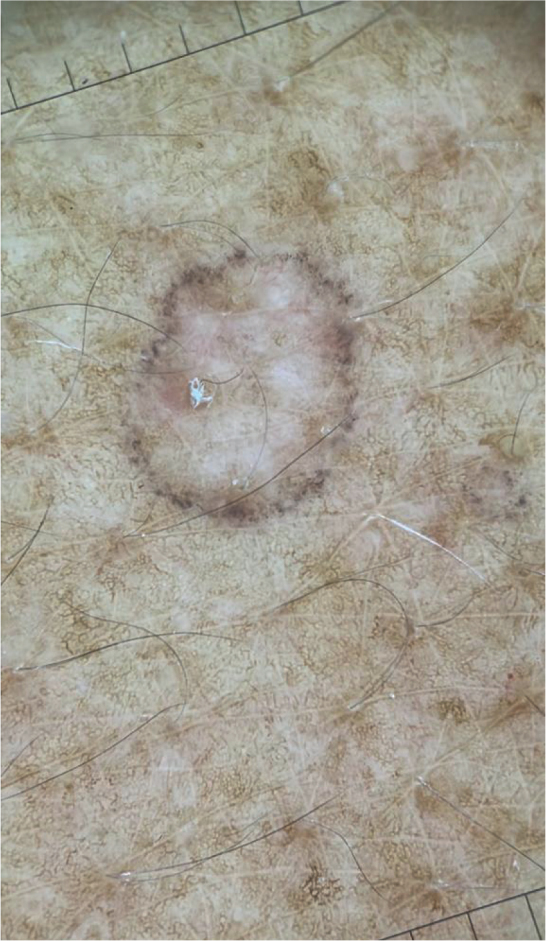
Dermoscopic examination of DSAP reveals a peripheral annular keratin rim with double edge “train tracks”, an atrophic scar-like central area and no obvious melanocytic features (1).
While the pigmented variant of DSAP the “train tracks” border shows with multiple fine grey-black dots (4, 5)
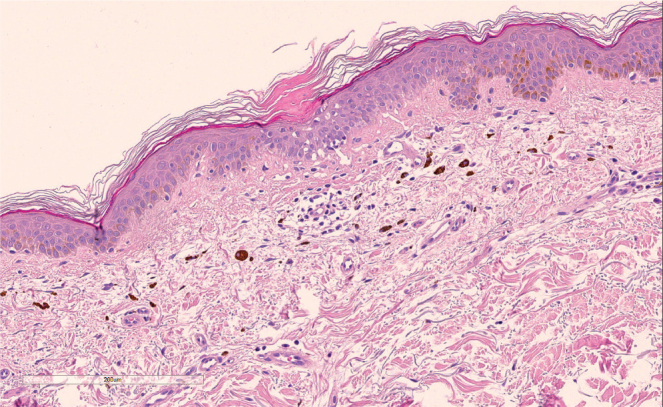
Histopathology of DSAP shows the presence of cornoid lamellae consistent with hyperkeratotic and parakeratotic columns associated with underlying loss of granular layer, in the epidermis, and solar elastosis, melanocyte hyperplasia, pigment incontinence within the superficial dermis below the cornoid lamellae.
Notably, the unusual finding, which support the diagnosis of a pigmented DSAP, as in the current case, was the presence of prominent melanocyte hyperplasia and pigment incontinence (4–6).
Differential diagnosis of DSAP includes other hyperplastic and neoplastic lesions, such as solar lentigo, actinic keratoses, lichenoid keratoses, melanoma, and inflammatory skin disorders such as guttate psoriasis, pityriasis rosea and lichen planus. Particularly, in pigment DSAP differential diagnosis focuses on lichen planus pigmentosus and lichenoid keratoses.
Treatment options for porokeratosis include cryotherapy, 5-fluorouracil, topical retinoids, topical tacrolimus and photodynamic therapy (5).
Due to the possibility of malignant transformation within porokeratosis to squamous cell carcinoma and Bowen’s disease, clinical surveillance with annual skin examinations and sun protection are key elements of the management of porokeratosis (4, 6).
Nevertheless, further observational studies are needed to increase recognition of this particular variant.
REFERENCES
-
1.Zaar O, Polesie S, Navarrete-Dechent C, Errichetti E, Akay BN, Jaimes J, et al. Dermoscopy of porokeratosis: results from a multicentre study of the International Dermoscopy Society. J Eur Acad Dermatol Venereol
2021; 35: 2091–2096.
[DOI] [PubMed] [Google Scholar]
-
2.Vargas-Mora P, Morgado-Carrasco D, Fustà-Novell X. Porokeratosis: A review of its pathophysiology, clinical manifestations, diagnosis, and treatment. Actas Dermosifiliogr (Engl Ed)
2020; 111: 545–560.
[DOI] [PubMed] [Google Scholar]
-
3.Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol
2012; 26: 404–412.
[DOI] [PubMed] [Google Scholar]
-
4.Tan TS, Tallon B. Pigmented porokeratosis. A further variant?
Am J Dermatopathol
2016; 38: 218–221.
[DOI] [PubMed] [Google Scholar]
-
5.Sotoodian B, Mahmood MN, Salopek TG. Clinical and dermoscopic features of pigmented disseminated superficial actinic porokeratosis: case report and literature review. J Cutan Med Surg
2018; 22: 229–231.
[DOI] [PubMed] [Google Scholar]
-
6.Reyna-Rodríguez IL, García-Lozano JA, Ocampo-Candiani J. Pigmented disseminated superficial actinic porokeratosis in dark-skinned patients: Clinical, dermoscopic, and histopathologic features. J Cosmet Dermatol
2021; 20: 3054–3056.
[DOI] [PubMed] [Google Scholar]